10 Manejo Odontologico de La Mujer
13
Dental management of the female patient J OAN O TOMO -C ORGEL The female patient presents with unique therapeutic challenges that vary throughout her lifeÕs continuum. Hormonal influences may appear in oral tissues be- fore other systemic manifestations are apparent. Periodontal tissues can reflect the need to alter con- ventional therapy. Therefore, it is the clinicianÕs responsibility to recognize, customize and vary peri- odontal therapy based on the individual female and the stage of her life cycle (43). This article reviews the clinical management of the female patient during the life cycle from puberty through menopause. The clinician should recognize the periodontal manifestations and ⁄ or intra-oral le- sions caused by systemic diseases. For example, the clinical signs and symptoms of diabetes and auto- immune disorders may be exaggerated by hormonal fluctuations. A thorough review of the patientÕs medical and psychological history is required as part of the periodontal examination. Puberty An exaggerated periodontal tissue response to peri- odontal risk factors may occur during puberty in male subjects and female subjects. In the pubertal female patient, the tissues are likely to present with inflammatory responses as a result of elevated sex- steroid hormone levels, which are irregular until postpubertal hormones stabilize. An enlargement of the gingiva may occur in areas where food debris, materia alba, plaque and calculus are deposited. The inflamed tissues can become erythematous, lobu- lated and retractable. Bleeding may occur easily upon mechanical debridement of the gingival tissues, especially interproximally. During puberty, education of the parent or care- giver is an integral part of successful periodontal therapy. Preventive care, including vigorous imple- mentation of oral hygiene, is vital for maintaining periodontal health. Milder cases of gingivitis in pub- erty respond well to scaling and deplaqueing, along with frequent oral hygiene reinforcement (5). Severe cases of this type of gingivitis may require microbial culture, antimicrobial mouthwashes and local site delivery of an antiseptic. Periodontal maintenance appointments may need to be more frequent when there is an apparent risk of periodontal disease pro- gression (42). The clinician should also recognize that the inci- dence of asthma and ⁄ or mouth breathing may be higher in pubertal female and male subjects. The incidence of asthma also increases after puberty in female subjects. This may cause gingival enlarge- ment, especially in the anterior area of the dentition, possibly as a result of surface dehydration. The cli- nician should recommend meticulous home care and increase the frequency of periodontal maintenance appointments and dental caries evalution. Topical application of an occlusive barrier (lubricant) over the inflamed gingiva after home-care procedures and immediately before bedtime may aid in the reduction of soft-tissue edema. Female adolescents (11–14 years of age) are sus- ceptible to problems associated with eating disorders. The clinician should examine for intra-oral signs and symptoms of anorexia nervosa and bulimia nervosa in a suspect patient. Chronic regurgitation of gastric contents will appear as perimylosis (i.e. smooth ero- sion of enamel and dentin), typically on the lingual surfaces of maxillary anterior teeth, and the duration and frequency of the behavior will determine the degree of perimylosis (9). Also, enlargement of the parotid glands (occasionally sublingual glands) has been estimated to occur in 10–50% of patients who Ôbinge and purgeÕ (36). Therefore, a diminished 219 Periodontology 2000, Vol. 61, 2013, 219–231 Printed in Singapore. All rights reserved Ó 2013 John Wiley & Sons A/S PERIODONTOLOGY 2000
-
Upload
vasiliki-konstantopoulou -
Category
Documents
-
view
218 -
download
0
description
10 Manejo Odontologico de La Mujer
Transcript of 10 Manejo Odontologico de La Mujer

Dental management of thefemale patient
JO A N OT O M O-CO R G E L
The female patient presents with unique therapeutic
challenges that vary throughout her life�s continuum.
Hormonal influences may appear in oral tissues be-
fore other systemic manifestations are apparent.
Periodontal tissues can reflect the need to alter con-
ventional therapy. Therefore, it is the clinician�sresponsibility to recognize, customize and vary peri-
odontal therapy based on the individual female and
the stage of her life cycle (43).
This article reviews the clinical management of the
female patient during the life cycle from puberty
through menopause. The clinician should recognize
the periodontal manifestations and ⁄ or intra-oral le-
sions caused by systemic diseases. For example, the
clinical signs and symptoms of diabetes and auto-
immune disorders may be exaggerated by hormonal
fluctuations. A thorough review of the patient�smedical and psychological history is required as part
of the periodontal examination.
Puberty
An exaggerated periodontal tissue response to peri-
odontal risk factors may occur during puberty in
male subjects and female subjects. In the pubertal
female patient, the tissues are likely to present with
inflammatory responses as a result of elevated sex-
steroid hormone levels, which are irregular until
postpubertal hormones stabilize. An enlargement of
the gingiva may occur in areas where food debris,
materia alba, plaque and calculus are deposited. The
inflamed tissues can become erythematous, lobu-
lated and retractable. Bleeding may occur easily upon
mechanical debridement of the gingival tissues,
especially interproximally.
During puberty, education of the parent or care-
giver is an integral part of successful periodontal
therapy. Preventive care, including vigorous imple-
mentation of oral hygiene, is vital for maintaining
periodontal health. Milder cases of gingivitis in pub-
erty respond well to scaling and deplaqueing, along
with frequent oral hygiene reinforcement (5). Severe
cases of this type of gingivitis may require microbial
culture, antimicrobial mouthwashes and local site
delivery of an antiseptic. Periodontal maintenance
appointments may need to be more frequent when
there is an apparent risk of periodontal disease pro-
gression (42).
The clinician should also recognize that the inci-
dence of asthma and ⁄ or mouth breathing may be
higher in pubertal female and male subjects. The
incidence of asthma also increases after puberty in
female subjects. This may cause gingival enlarge-
ment, especially in the anterior area of the dentition,
possibly as a result of surface dehydration. The cli-
nician should recommend meticulous home care and
increase the frequency of periodontal maintenance
appointments and dental caries evalution. Topical
application of an occlusive barrier (lubricant) over
the inflamed gingiva after home-care procedures and
immediately before bedtime may aid in the reduction
of soft-tissue edema.
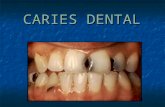
Female adolescents (11–14 years of age) are sus-
ceptible to problems associated with eating disorders.
The clinician should examine for intra-oral signs and
symptoms of anorexia nervosa and bulimia nervosa
in a suspect patient. Chronic regurgitation of gastric
contents will appear as perimylosis (i.e. smooth ero-
sion of enamel and dentin), typically on the lingual
surfaces of maxillary anterior teeth, and the duration
and frequency of the behavior will determine the
degree of perimylosis (9). Also, enlargement of the
parotid glands (occasionally sublingual glands) has
been estimated to occur in 10–50% of patients who
�binge and purge� (36). Therefore, a diminished
219
Periodontology 2000, Vol. 61, 2013, 219–231
Printed in Singapore. All rights reserved
� 2013 John Wiley & Sons A/S
PERIODONTOLOGY 2000

salivary flow rate may also be present, which will
increase oral mucous membrane sensitivity, gingival
erythema and caries susceptibility. Oral healthcare
providers are often the first to recognize eating dis-
orders. After consultation with the patient and ⁄ or
parent, a referral to a physician, psychologist or
nutritional consultant is advised. Patients with diag-
nosed eating disorders also demonstrate an increased
susceptibility to low bone mass. Many will report
cessation of menses, even before significant weight
loss is apparent, as a result of altered endocrine
function, especially low plasma-estrogen levels.
These patients need nutritional and vitamin supple-
mentation, especially calcium and vitamin D. Other
laboratory abnormalities include mild normochromic,
normocytic anemia, mild to moderate leukopenia
and a reduction in the number of polymorphonuclear
leukocytes (57). Blood urea nitrogen and creatinine
are increased in cases of dehydration, frequently
along with a low blood sugar level.
Menstrual cycle
The monthly reproductive cycle can be separated into
two phases (Fig. 1). During the luteal phase (the sec-
ond stage of the menstrual cycle), increased gingival
sensitivity and bleeding have been reported. Women
who present with increased periodontal inflammation
and tenderness should receive periodontal mainte-
nance therapy every 3–4 months. During the luteal
phase, an increased incidence of intra-oral recurrent
aphthous ulcers has also been reported (22), but is
probably independent of hormone levels (37).
The possibility of anemia as a result of iron loss
during menstruation can influence treatment (19,
51). Iron-deficiency-related anemia has been esti-
mated to affect almost 20% of women of childbearing
age, and the possibility of anemia must be considered
for women of reproductive age with lower than
average body weight or with a history of heavy
menstrual flow (51). Severe anemia may result in
angular cheilitis, atrophic glossitis and ⁄ or oral
mucosal atrophy (12). Patients with anemia should
be referred to a physician for appropriate laboratory
tests and treatment.
During the luteal phase, the lower esophageal
sphincter may relax, and thus the gag reflex may well
be heightened more than at other times during the
normal menstrual cycle. As a result, normal intra-oral
procedures can become more difficult. For example,
it may be more difficult for the dental professional to
retract the tongue, place radiographic films or use
aerosols in the mouth. If a patient does present with
oral problems during this state of the cycle, it would
be prudent to schedule surgical therapy until after
menstruation. The relaxed esophageal sphincter may
also make women more susceptible to gastroesoph-
ageal reflux disease, with heartburn, regurgitation
and chest pain, and some patients with severe reflux
disease may develop unexplained coughing, hoarse-
ness, sore throat, gingivitis and asthma (47). Fluoride
therapy is recommended for patients with gastro-
esophageal reflux disease as a result of increased
caries susceptibility and acid erosion (Figs 2 and 3).
The patient should also be advised to use alcohol-free
mouthrinses and to shorten the time intervals be-
tween periodontal ⁄ dental maintenance visits.
The premenstrual syndrome consists of physical
and emotional symptoms that are associated with the
menstrual cycle. The diagnosis of premenstrual syn-
drome is limited to symptoms that develop during
the luteal phase of the menstrual cycle and symp-
toms may be severe enough to impede some aspects
Fig. 1. Monthly female hormonal cycle. Diagramatic
illustration of changes in concentration of the gonado-
tropins (FSH and LH) and ovarian hormones (estrogens
and progesterone) during one reproductive cycle. FSH,
follicle-stimulating hormone; LH, luteinizing hormone.Fig. 2. Acid erosion of maxillary teeth from gastroesoph-
ageal reflux.
220
Otomo-Corgel

of life. Many patients with premenstrual syndrome
also receive antidepressants because of lower levels
of neurotransmitters such as enkephalins, endor-
phins, c-aminobutyric acid and serotonin. Selective
seratonin reuptake inhibitors are often prescribed for
neurotransmitter deficiency. Sertraline is the drug of
choice for premenstrual syndrome (24), but floxetine
is commonly prescribed owing to a reported 70%
response rate in the reduction of depression. Patients
taking fluoxetine have altered absorption, increased
side effects with highly protein-bound drugs (e.g.
aspirin) and an increased half-life of diazepam and
other central nervous system depressants (56). Other
common selective seratonin reuptake inhibitors are
fluvoxamine, paroxetine and citalopram, and an-
tidepressants that may be prescribed are the selective
serotonin and norepinephrine reuptake inhibitors,
tricyclics, trazodone, mirtazapine, nefazodone and
maprotiline. It is important to recognize that an-
tidepressants are associated with an increased inci-
dence of xerostomia. Depression, irritability, mood
swings and difficulty with memory and concentration
may be symptoms of neurotransmitter reduction.
Patients are more sensitive to and less tolerant of
therapeutic procedures while using selective serato-
nin reuptake inhibitors and may have an exaggerated
response to pain.
The premenstrual syndrome patient may be diffi-
cult to treat because of emotional and physiologic
sensitivity. The dentist should treat the gingival and
oral mucosal tissues gently. Gauze pads or cotton
rolls should be moistened with a lubricant, chlorh-
exidine rinse or water before placing them in the
�aphthous ulcer-prone� patient. Careful retraction of
the oral mucosa, cheeks and lips is necessary, espe-
cially in patients prone to aphthous or herpetic
lesions. Because the hypoglycemic threshold is
elevated, the clinician should advise the patient to
have a light snack before her appointment. Seventy
per cent of menstruating women have premenstrual
syndrome symptoms, but only 5% meet the strict
diagnostic criteria of premenstrual syndrome.
Oral contraceptives
Early studies examining the effects of oral contra-
ceptives on the periodontium have shown that the
periodontal response to these agents is similar to that
seen in pregnant women (37). The studies reported
an exaggerated gingival response to local factors.
Inflammation can range from mild edema and ery-
thema to severe inflammation with hemorrhagic or
enlarged gingival tissues (37). More exudate was also
present in inflamed gingival tissues of oral contra-
ceptive users than in pregnant women (63). Some
investigators reported that the inflammation in-
creased with the prolonged use of oral contracep-
tives, but Kalkawarf (31) did not find that duration of
use made a significant difference to inflammation;
however, the brand of contraceptive used resulted in
different gingival responses. It should be noted that
the concentration of female sex hormones in current
oral contraceptives is significantly lower than in the
earlier formulations (1970–1990) and current data
examining contemporary formulations suggest that
oral contraceptives do not have a significant effect on
the inflammatory composition of the periodontium
(45).
Similarly to the early reported effects of oral con-
traceptives on gingival inflammation, studies from
the 1970s found that the salivary composition chan-
ged notably in patients taking oral contraceptives. A
decreased concentration of protein, sialic acid,
hexosamine fucose, hydrogen ions and total electro-
lytes was reported. Salivary flow rates were increased
in one report (35) and were decreased in 30% of
subjects in another report (20). More recent studies
have shown no difference in salivary flow rates
between patients on oral contraceptives versus indi-
viduals not using oral contraceptives (48).
Oral contraceptives have also been reported to
cause a two- to threefold increase in the incidence of
localized osteitis after extraction of mandibular third
molars (52). The higher incidence of osteitis may be
attributed to the effects of oral contraceptives (i.e.
estrogens) on clotting factors. However, others refute
this finding (14), especially in light of the contem-
porary formulation of contraceptives. At this time,
evidence is inconclusive on osteitis after third-molar
extraction in patients on oral contraceptives.
In regard to the skin around the lips, a spotty
melanotic pigmentation of the skin may occur with
Fig. 3. Acid erosion of mandibular teeth from gastro-
esophageal reflux.
221
Therapeutic challenges through female continuum

oral contraceptive use. This suggests a relationship
between the use of oral contraceptives and the
occurrence of gingival melanosis (27), especially in
fair-skinned individuals.
Medical history should include oral contraceptives
under the heading of �medications�, and the dialog
with women of childbearing age should include
questions regarding the use of oral contraceptives.
For those rare patients who are sensitive to the ad-
verse effects of oral contraceptives and exhibit an
exaggerated gingival response while using an oral
contraceptive, treatment should include careful
mechanical debridement and the establishment of an
effective oral hygiene program. Periodontal surgery
may be indicated if the gingival response is inade-
quate after initial scaling and root planing.
Pregnancy
The importance of providing oral health care for
pregnant women is undisputable. Data suggest that
maternal oral health is associated with pregnancy
health, and further research on the nature of this
association is ongoing to determine if there is a
causal relationship (6). Despite conflicting clinical
trial results regarding the effectiveness of periodontal
therapy to improve pregnancy outcomes, preventing
and reducing periodontal inflammation in pregnant
women is safe (29, 41) and reduces the bacterial load.
Early studies indicated that pregnancy was associated
with a subgingival increase in certain bacterial spe-
cies, especially those belonging to the group known
as black-pigmented Bacteroides, and that this in-
crease may play an etiological role in the increased
incidence of gingivitis (37). Recent evidence does not
corroborate these early findings, and several investi-
gators have found little or no association between
periodontal black-pigmented Bacteroides and states
of hormonal surges in women during pregnancy,
puberty or menstruation (33). Pregnancy is also an
opportunity to educate parents on preventive care for
their offspring. Providing counseling to women of
childbearing age regarding the need for periodontal
heath should be offered, especially to individuals who
are planning to become pregnant.
A thorough medical history is an imperative com-
ponent of the periodontal examination, especially in
the pregnant woman. Because of immunologic
alterations, increased blood volume, cardiac consid-
erations and fetal interactions, the clinician must
diligently and consistently monitor the patient�smedical and periodontal status. The medical history
dialog should include previous pregnancy complica-
tions, previous miscarriages and any recent history of
cramping, spotting or pernicious vomiting. The pa-
tient�s obstetrician should be contacted to discuss the
patient�s medical status, periodontal or dental needs
and the proposed treatment.
Establishing a healthy oral environment and
maintaining optimal oral hygiene levels are primary
objectives in the pregnant woman. The periodontal
tissues, which contain hormonal receptors, can be
affected by pregnancy hormones and may reflect an
over-exuberant response, such as pregnancy-associ-
ated pyogenic granulomas (Figs 4 and 5). Pregnant
women with underlying systemic diseases may ex-
hibit exaggerated periodontal responses, as seen in
the periodontitis that occurs in HIV-positive women
during pregnancy (Fig. 6) or excessive gingival
enlargement, pain and bleeding as a result of treat-
ment with cyclosporine medication (Fig. 7). Other
types of gingival pathosis, such as central giant cell
granulomas or underlying systemic diseases that
Fig. 4. Pregnancy granuloma.
Fig. 5. Pregnancy granuloma (courtesy of Dr P War-
shawsky).
222
Otomo-Corgel

resemble pregnancy-associated pyogenic granuloma
must be ruled out for a correct diagnosis. A pre-
ventive periodontal program consisting of nutritional
counseling and rigorous plaque-control measures
should be reinforced. The increased tendency for
gingival inflammation during pregnancy should be
clearly explained to the patient so that acceptable
oral-hygiene techniques may be taught, reinforced
and monitored throughout pregnancy. With ade-
quate home care and periodontal intervention,
inflammation may resolve postpartum. Scaling and
root planing may be performed, whenever necessary,
during pregnancy. Some practitioners avoid the use
of high-alcohol-content antimicrobial rinses in
pregnant women and prefer to recommend the use of
nonalcohol-based oral rinses (42).
The prescription of prenatal fluoride supplements
has been an area of controversy. Although two stud-
ies have claimed beneficial results (24, 25), others
suggest that the clinical efficacy of prenatal fluoride
supplements is uncertain, and that the mechanism
by which prenatal fluoride supplements impart car-
iostasis is unclear (2). As such, the American Dental
Association and The American Academy of Pediatric
Dentistry do not recommend treatment with prenatal
fluoride supplements because of their unproven
efficacy.
Trimester periodontal care
Pregnancy alone is not a reason to defer routine
periodontal therapy. In fact, the pregnant woman is
more susceptible to periodontal inflammation during
this time of her life. The California Dental Association
Foundation, in collaboration with the American
College of Obstetrician and Gynecologists, produced,
in 2010, guidelines that state �prevention, diagnosis,
and treatment of oral diseases, including needed
dental radiographs and use of local anesthesia, is
highly beneficial and can be undertaken during
pregnancy without additional fetal or maternal risk
when compared to the risk of not providing care� (11).
Good oral health and control of oral disease protects
a women�s health and quality of life and has the po-
tential to reduce the transmission of pathogenic
bacteria from mothers to their children (11).
During the first trimester, therapy should include
preventive therapy, creating indiviudalized home-
care instruction. If there is periodontal inflammation,
it is �safe and effective to provide periodontal care to
reduce periodontal disease and periodontal patho-
gens during pregnancy� (11). It is recommended for
the pregnant woman to have a full clinical peri-
odontal examination and to understand the in-
creased susceptiblity to periodontal disease. It is
prudent, however, to avoid elective dental care if
possible during the first trimester and the last half of
the third trimester. The first trimester is the period of
organogenesis, when the fetus is highly susceptible to
environmental influences.
Early in the second trimester (14–20 weeks of ges-
tation) is the safest period for providing routine
dental care (23). The emphasis during this trimester
is to control active disease and eliminate potential
problems that could arise in late pregnancy. Peri-
odontal debridement should be performed during
this trimester. Major elective oral or periodontal
surgery should be postponed until after delivery.
Pyogenic granulomas that develop during pregnancy
(i.e. �pregnancy tumors�) that are painful, interfere
with mastication or continue to bleed or suppurate
after mechanical debridement, may require excision
and biopsy before delivery.
In the last half of the third trimester, a hazard for
premature delivery exists because the uterus is very
Fig. 6. HIV periodontitis in pregnancy.
Fig. 7. Gingival enlargement with cyclosporin treatment
during pregnancy.
223
Therapeutic challenges through female continuum

sensitive to external stimuli. Prolonged chair time
should be avoided because the woman is most
uncomfortable at this time. Furthermore, supine
hypotensive syndrome may occur. In a semi-reclining
or supine position, the great vessels, particularly the
inferior vena cava, are compressed by the gravid
uterus. By interfering with venous return, this com-
pression will cause maternal hypotension, decreased
cardiac output and eventual loss of consciousness.
Supine hypotensive syndrome can usually be reversed
by turning the patient on her left side, thereby
removing pressure on the vena cava and allowing
blood to return from the lower extremities and pelvic
area. A preventive 15 to 24-cm soft wedge (rolled to-
wel) should be placed on the patient�s right side when
she is reclined for clinical treatment (42). A periodontal
maintenance visit should also be performed during the
early- to mid-third trimester as a result of increased
periodontal inflammation associated with pregnancy.
Pre-eclampsia occurs when hypertension is asso-
ciated with proteinuria during pregnancy and is a
challenging condition in the management of the
pregnant woman. The presence of pre-eclampsia is
not a contraindication to dental care (11). Although
maternal periodontal infection has been associated
with a risk for pre-eclampsia, the research results
have been conflicting (28, 50) and further investiga-
tion is warranted (6).
Radiographs
The safety of dental radiography during pregnancy has
been well established, especially when features such
as high-speed film, filtration, collimation and lead
aprons are used. When radiographs are needed for
diagnosis, one of the most important aids for the pa-
tient is the protective lead apron with a thyroid collar
(4). Studies have shown that when an apron is used
during contemporary dental radiography, gonadal
and fetal radiation is virtually immeasurable (7, 38). To
put into perspective the safety of dental radiography,
the number of dental X-ray films needed to reach the
maximum accepted safety limit for radiation to the
fetus would be approximately half a million exposures
(60). With the obvious safety of dental radiography,
X-ray films should be taken when necessary and
appropriate to aid in diagnosis and treatment.
Medications
Drug therapy in the pregnant woman is controversial
because drugs can affect the fetus by diffusion across
the placenta. Presciptions should be kept to as brief a
duration as possible to support the pregnant patient�swellbeing and drugs should only be administered
after careful consideration of potential side effects.
The classification system established by the US Food
and Drug Administration in 1979 to rate fetal risk
levels associated with prescription drugs provides
safety guidelines. The prudent practitioner should
consult references such as Briggs Drugs in Pregnancy
and Lactation (8) and Olin�s Drug Facts and Com-
parisons (18) for information on the US Food and
Drug Administration pregnancy risk associated with
prescription drugs. Ideally, no drug should be
administered during pregnancy, especially in the first
trimester (34). However, it is virtually impossible
always to adhere to this rule. Fortunately, most
commonly used drugs in dental practice can be given
during pregnancy with relative safety, although there
are a few important exceptions. Tables 1, 2 and 3
present general guidelines for the use of anesthetic
and analgesic, antibiotic and sedative-hypnotic
drugs, respectively (5, 57).
Antibiotics, in particular, are often needed in
periodontal therapy. The effect of a particular medi-
cation on the fetus depends on the type of antimi-
crobial, dosage, trimester and duration of the course
of therapy (8, 18). Research regarding subgingival
irrigation and local site delivery in relation to the
developing fetus is limited at the time of writing.
Usually, there is a risk that the drug can enter
breast milk and be transferred to the nursing infant,
in whom drug exposure could have adverse effects
(Tables 4 and 5). Unfortunately, there is minimal
conclusive information on drug dosage in the mother
and level of drug in the breast milk, and the effect on
the infant; however, retrospective clinical studies and
empiric observations, coupled with known pharma-
cologic pathways, allow recommendations to be
made. The amount of drug excreted in breast milk is
usually not more than 1–2% of the maternal dose;
therefore, it is highly unlikely that most drugs have
any pharmacologic significance for the infant (8, 18,
58). When possible, the mother should take pre-
scribed drugs just after breastfeeding and then avoid
nursing for 4 h or more, if possible, to allow the drug
concentration in breast milk to decrease.
Menopause
The patient�s medical history during menopause
requires continual review, and changes in the medi-
cal and oral status should be recorded routinely
and updated. Hormonal changes alter a patient�s
224
Otomo-Corgel

Table 1. Local anesthetic and analgesic administration during pregnancy
Drug Food and Drug
Administration category
Use ⁄ risks during pregnancy
Local anesthetics*
Articaine B Yes; no nerve blocks
Etidocaine B Yes
Lidocaine B Yes
Prilocaine B Yes
Bupivacaine C Use with caution; consult physician
Mepivacaine C Use with caution; consult physician
Procaine C Use with caution; consult physician
Analgesics
Acetaminophen B Yes
Hydrocodone� B Use with caution; consult physician
Ibuprofen B ⁄ D Caution in first and second trimester;
avoid in third trimester
Oxycodone� B Use with caution; consult physician
Aspirin C ⁄ D Caution in first and second trimester;
avoid in third trimester
Codeine� C Use with caution; consult physician
Propoxyphene C Use with caution; consult physician
*Can use vasoconstrictors if necessary.�Avoid prolonged use.
Table 2. Antibiotic administration during pregnancy
Drugs Food and Drug
Administration category
Use during pregnancy Pregnancy risk
Cephalosporins B Yes Limited information
Clindamycin B Yes with caution Drug concentrated in fetal
bone, spleen, lung, liver
Erythromycin B Yes; avoid estolate form Intrahepatic jaundice in
mother
Metronidazole B Avoid Carcinogenic data from
animals
Penicillins B Yes Diarrhea
Ciprofloxacin C Avoid Cartilage erosin
Gentamicin C Caution; consult physician Limited information but
possible ototoxicity
Vancomycin C Caution; consult physician Limited information
Clarithromycin D Avoid; consult physician Adverse effects on pregnancy
outcomes and embryonic;
fetal development in animals
Tetracycline D Avoid Depression of bone growth;
enamel hypoplasia; gray-
brown tooth discoloration
225
Therapeutic challenges through female continuum

systemic, as well as psychologic, wellbeing. The
major cause of death in the menopausal female is
cardiovascular disease (32). The stage for osteope-
nia ⁄ osteoporosis is set at perimenopause. It is
recommended that the patient should be asked when
her last menstrual cycle occurred. If the patient has
had a hysterectomy, the date of the surgery and the
length of postoperative hormone replacement ther-
apy (if prescribed) will allow the clinician to note the
onset of estrogen deprivation. Patients who have not
had a hysterectomy are considered to be menopausal
if there has not been a cycle for one full year. The
median age for menopause is approximately
50 years, with 10% of women becoming menopausal
before 40 years of age and 10% after 60 years.
In women, two stages of primary bone loss occur.
The first stage is rapid trabecular bone loss caused by
estrogen deficiency; it is initiated with the onset of
menopause and continues for approximately 4–
8 years. This stage exhibits high bone resorption and
reduced bone formation. There is a second stage that
occurs in men and women in which slower trabecular
and cortical bone loss occurs as a result of decreased
bone formation.
Because of the possible alterations in oral soft and
osseous tissues during perimenopause and after men-
opause, appropriate questioning regarding hormone
changes should be performed and documented.
There are a myriad of hormone replacement ⁄ estro-
gen replacement therapies available, from prescrip-
tions to holistic approaches, which need to be
assessed. Many medications may alter clotting times,
prolong the effects of other medications and interfere
with absorption or effectiveness of prescription
medications. Estrogen depletion has also been
associated with xerostomia. To compound the prob-
lem of xerostomia, many postmenopausal patients
will be on antidepressants, which also reduce saliva
secretion.
Gingival and mucosal tissue thinning often occurs.
It is generally safe to perform soft-tissue augmenta-
tion procedures if needed. Brushing with an extrasoft
toothbrush using the �toe� or �heel� of the brush may
prevent �scrubbing� the thinning gingiva. Dentifrices
with minimally abrasive particles should be consid-
Table 3. Sedative-hypnotic drug administration duringpregnancy
Drugs Food and Drug
Administration
category
Use during
pregnancy
Barbituates D Avoid
Benzodiazepines D Avoid
Nitrous oxide Not assigned Avoid in first
trimester,
otherwise use
with caution;
consult physician
Table 4. Local anesthetic and analgesic administrationduring breastfeeding
Drug Use during breastfeeding
Local anesthetics
Lidocaine Yes
Mepivacaine Yes
Prilocaine Yes
Bupivacaine Yes
Etidocaine Yes
Procaine Yes
Analgesics
Aspirin Avoid
Acetaminophen Yes
Ibuprofen Yes
Codeine Yes
Hydrocodone No data
Oxycodone Yes
Propoxyphene Yes
Table 5. Antibiotic administration during breastfeeding
Drug(s) Use during breastfeeding
Antibiotics*
Penicillins Yes
Erythromycin Yes
Clindamycin Yes, with caution
Cephalosporins Yes
Tetracycline Avoid
Ciprofloxacin Avoid
Metronidazole Avoid
Gentamicin Avoid
Vancomycin Avoid
Sedative-hypnotics
Benzodiazepines Avoid
Barbiturates Avoid
Nitrous oxide Yes
*Have the risk of diarrhea and sensitization in the mother and infant.
226
Otomo-Corgel

ered. Mouthrinses should have a low alcohol con-
centration. During periodontal maintenance, root
surfaces should be debrided gently with minimal soft
tissue trauma. Oral pain may result from thinning
tissues, xerostomia, inadequate nutritional intake or
hormone depletion (42). In patients with oral symp-
toms who receive hormone replacement therapy,
symptoms may be significantly reduced. Studies
indicate improved periodontal status in women on
hormone replacement therapy or estrogen replace-
ment therapy, as well as increased alveolar bone mass
with associated improved alveolar crestal height, and
reduced clinical attachment loss (13, 46, 53). Consul-
tation with the patient�s physician as to the risks versus
benefits of hormone replacement therapy ⁄ estrogen
replacement therapy and calcium ⁄ vitamin D sup-
plementation for the individual patient may be
needed when periodontal disease occurs.
It has been suggested that the postmenopausal
woman who is susceptible to osteoporosis (e.g. Cau-
casian, Asian, smoker, minimal physical activity, low
calcium intake, thin build or low body weight, genetic
history) may also be more susceptible to periodontal
bone loss (30). Alveolar crestal height loss and max-
illary tooth loss have been associated with decreased
bone mineral density (15, 17, 26, 62); however, studies
evaluating the association of clinical attachment loss
and osteoporosis have produced equivocal results
(21, 39, 44, 49, 61). At the time of writing there were
no overwhelming data to link osteoporosis to peri-
odontal disease, and long-term studies are required
to assess the impact of these chronic problems on
one another (37). Furthermore, there are no scientific
data available to contraindicate the use of osseoin-
tegrated implants in osteoporotic patients, despite
articles indicating osteoporosis as a risk factor.
Bone-sparing drugs
Biphosphonates (e.g. alendronate, risendronte, iban-
dronate and zoledronic acid) are one of the primary
medications prescribed for osteoporosis. Bisphosph-
onate therapy studies have shown a positive effect on
reducing fracture risk, and reports have indicated a
reduction of periodontal disease progression (54, 55).
A rare side effect associated with bisphosphonate use
is osteonecrosis of the jaw. Osteonecrosis of the jaw
associated with bisphosphonates is defined as
exposed or necrotic bone in the maxillofacial region
that is present for at least eight continuous months in
patients who are using (or have used) bisphospho-
nates and have no history of radiation therapy to the
jaws (1, 3).
To date, no data are available regarding success or
failure with periodontal procedures in osteoporotic
versus nonosteoporotic individuals, with or without
bisphosphonate therapy. The best current peri-
odontal therapy is prevention and working in col-
laboration with the treating physician. Radiographic
evaluation of the alveolar bone and a thorough
periodontal examination assessing periodontal
attachment loss is necessary. The medical consulta-
tion conducted by the physician should include the
periodontal status and the periodontal ⁄ implant
treatment plan for the patient, as well as treatment
options. Patients should be asked about the length of
time they have been taking bisphosphonate medica-
tion, if the medication was taken reliably, noted side
effects and the date of the last bone-density scan.
If a patient taking an oral bisphosphonate presents
with osteonecrosis of the jaw, the prescribing physi-
cian needs to be consulted. Current recommenda-
tions for treating patients with osteonecrosis of the
jaw related to oral bisphosphonate use are found in
the 2011 American Dental Association recommen-
dations �Managing the Care of Patients Receiving
Antiresorptive Therapy for Prevention and Treatment
of Osteoporosis� (3). Thorough, but gentle, peri-
odontal debridement should be performed. The pa-
tient may be placed on appropriate antibiotics (as
determined in the medical consultation), stringent
home care and an antimicrobial (chlorhexidine)
mouthrinse. Exposed necrotic, sequestrated bone can
be gently debrided.
In addition to bisphosphonates, clinicians must
also weigh the effect of a myriad of medications that
may induce secondary osteoporosis (Table 6). In
patients taking this type of medication it is advisable
to monitor the patient�s periodontal status closely, to
perform titrated periodontal maintenance care, to
inform the patient about potential risks of hormone
depletion on the oral tissues and to consult the
treating physician.
The National Institutes of Health 1994 Conference
on Optimal Calcium Intake recommended 1,000 mg
of elemental calcium per day for premenopausal
women and 1,200 mg ⁄ day of elemental calcium for
postmenopausal women (Table 7) (40). Vitamin D
uptake has been determined to be suboptimal in 90%
of our elderly population. Currently, recommenda-
tions are 400 IU ⁄ day for premenopausal women and
800 IU ⁄ day for postmenopausal women. The new
consensus, however, is that 800–1,000 IU ⁄ day is the
minimal dose for the elderly, but 1,000-IU pills will
not be adequate for most elderly individuals during
the winter months and many people may consider up
227
Therapeutic challenges through female continuum

to 2,000 IU ⁄ day (16). Many physicians now propose
2,000 IU ⁄ day of vitamin D as the upper allowable
limit. Patients may also be given 50,000 IU ⁄ week of
vitamin D for 4–12 weeks if extremely low serum
levels of vitamin D are noted.
Patients who are prescribed intravenous bis-
phosphonates may be at risk for osteonecrosis of the
jaw. A systematic review by Woo et al. (59) reported
on 368 cases of osteonecrosis of the jaw. The primary
medical diagnoses of multiple myeloma, metastatic
breast cancer and metastatic prostatic cancer con-
stituted 91.5% of the reported cases. Over 94% of the
patients were on intravenous zoledronic acid,
pamidronate, or both. Of the osteonecrosis cases,
60% had received dentoalveolar surgery, but 40% of
cases of osteonecrosis appeared spontaneously, often
in denture wearers, in whom 39% were associated
with exostoses. Osteonecrosis of the jaw was more
common in the mandible (e.g. 65% prevalence) than
in the maxilla (e.g. 26% prevalence) and occurred
only 9% of the time in both mandible and maxilla.
The important predisposing factors for development
of osteonecrosis of the jaw were the type and dose of
the bisphosphonate, plus a history of trauma, dental
surgery or dental infection (59). Patients should have
dental clearance before starting therapy with intra-
venous bisphosphonates, similarly to protocols for
patients anticipating radiation to the head and ⁄ or
neck. Consultation with the treating physician is
important and the physician should be notified about
the status of the periodontal ⁄ dental tissues. Teeth
with a poor or hopeless prognosis should be ex-
tracted. Healthy periodontal tissues should be
established, individualized home-care procedures
developed and the possible oral effects of the medi-
cation should be explained to the patient. The ratio-
nale for closer periodontal monitoring and debride-
ment should also be explained to the patient. Sharp
or irregular bony prominences (e.g. lingual tori,
maxillary tori and the mylohyoid ridge) should be
reduced and removable prostheses should be as-
sessed for accurate fit.
Similarly to patients taking oral bisphosphonates, if
a patient presents with osteonecrosis of the jaw and
with a history of intravenous bisphosphonate therapy
or subcutaneous RANKL inhibitor therapy, the
treating physician should be contacted as soon as
possible. The following recommendations by the
American Academy of Oral and Maxillofacial Surgery
for the various stages of osteonecrosis of the jaw in-
clude informed consent, use of antibacterial mouth-
rinses and, when needed and depending on the
severity of the osteonecrotic lesion, the use of anal-
gesics, antibiotics, gentle debridement of the affected
area and, at times, surgical resection (1).
Surgical resection of lesions associated with
osteonecrosis of the jaw generally is not recom-
mended because more severe sequellae can develop.
However, a recent publication that evaluated surgical
resection of osteonecrosis of the jaw in patients tak-
ing an oral bisphosphonate concluded that resection
Table 6. Medications ⁄ drugs associated with secondaryosteoporosis
Glucocorticoids
Immunosuppressants i.e. cyclosporine A ⁄ tacrolimus
Cytotoxic drugs, i.e. methotrexate
Aromatase inhibitors i.e. anastrozole, exemestane,
letrozole
Lithium
Antisconvulsants, i.e. phenytoin, phenobarbital
Blood thinners i.e. warfarin ⁄ heparin therapy (long term)
Aluminum-containing antacids
Gonadotropin-releasing hormone agonists
Thyroid hormone (in excess)
Proton pump inhibitors (63)
Selective serotonin reuptake inhibitors
Thiazolidenediones i.e. pioglitazone ⁄ roziglitazone
Excessive alcohol
Table 7. Calcium recommendations
Age National academy of
sciences
Calcium intake
recommendations
mg ⁄ day
Birth to 6 months 210
7 months to 1 year 270
1–3 years 500
4–8 years 800
9–18 years 1,300
19–50 years 1,000
51 years or older 1,200
Pregnant ⁄ lactating
14–18 years
1,300
Pregnant ⁄ lactating
19–50 years
1,000
228
Otomo-Corgel

of the osteonecrosis can yield acceptable healing in
the maxilla or mandible (10). In patients with
necrosis after intravenous bisphosphonate therapy,
the healing outcome after surgical resection was
predictably good in the maxilla, but was variable in
the mandible (10). We are just beginning to under-
stand the process of osteonecrosis of the jaw, and
treatment modalities are in their infancy. Additional
research is needed to address the increasing number
of patients who may present to periodontal practices
with osteonecrosis of the jaw.
Conclusions
The female patient presents unique complexities that
vary along her life�s continuum. The cyclic nature of
the female sex hormones is often reflected in the
gingival tissues as initial signs and symptoms. Med-
ical history and dialogs should include thoughtful
investigation of the individual patient�s needs. Hor-
monal fluctuations differ from patient to patient. The
dental professional should explore hormonal stability
and medications associated with hormone regula-
tion. Patients should be educated regarding the
profound effects that sex hormones may play on
periodontal and oral tissues as well as the need for
proper oral self-care and a frequent professional
intervention.
It is apparent that dentists will be treating increasing
numbers of female patients with diseases associated
with longevity. The world population older than
80 years of age is increasing dramatically, with women
assuming the majority in the USA. In 2009, 101.9 mil-
lion octogenarians and older populated the world. By
2050, the projection by the United Nations Depart-
ment of Economic and Social Affairs predict this seg-
ment of the population will rise to 394.7 million.
Clinical periodontal therapy includes an under-
standing of the clinician�s role in the total health and
wellbeing of female patients. Dentists do not treat
localized oral infections without affecting other sys-
tems of the body. Female patients may present with
periodontal and systemic considerations that alter
conventional periodontal therapy.
References
1. American Association of Oral and Maxillofacial Surgeons.
American Association of Oral and Maxillofacial Surgeons
Position Paper on Bisphosphonate-Related Osteonecrosis
of the Jaw. 2009. American Association of Oral and Maxil-
lofacial Surgeons. Available at: http://www.aaoms.org/
docs/position_papers/bronj_update.pdf (accessed March
17, 2011).
2. American Academy of Pediatric Dentistry. Special issue:
reference manual 1994–95. American Academy of Pediatric
Dentistry. Pediatr Dent 1994: 16: 1–96.
3. American Dental Association. Managing the care of pa-
tients receiving antiresorptive therapy for prevention and
treatment of osteoporosis. J Am Dent Assoc 2011: 142:
1243–1251.
4. American Dental Association. The selection of patients for
dental radiographic examinations. 2004. American Dental
Association. Available at:http://www.ada.org/sections/
professionalResources/pdfs/topics_radiography_examina-
tions.pdf (accessed March 17, 2011).
5. American Dental Association Council on Access, Preven-
tion, and Interprofessional Relations. Women�s oral health
issues. Chicago, IL: American Dental Association, 1995.
6. Armitage GC. Bi-directional relationship between preg-
nancy and periodontal disease. Periodontol 2000 2013: 61:
160–176.
7. Bean LR Jr, Devore WD. The effect of protective aprons in
dental roentgenography. Oral Surg Oral Med Oral Pathol
1969: 28: 505–508.
8. Briggs GG, Freeman RK, Yaffe SJ. Drugs in pregnancy and
lactation: a reference guide to fetal and neonatal risk. Bal-
timore, MD: Williams & Wilkins, 1994.
9. Brown S, Bonifazi DZ. An overview of anorexia and bulimia
nervosa, and the impact of eating disorders on the oral
cavity. Compendium 1993: 14: 1594, 1596–1602, 1604–1608.
10. Carlson ER, Basile JD. The role of surgical resection in the
management of bisphosphonate-related osteonecrosis of
the jaws. J Oral Maxillofac Surg 2009: 67: 85–95.
11. California Dental Association. Oral health during preg-
nancy and early childhood: evidence-based guidelines for
health professionals. 2010. CDA Foundation. Available at:
http://www.cdafoundation.org/library/docs/poh_guidelines.
pdf (accessed March 17, 2011).
12. Chi AC, Neville BW, Krayer JW, Gonsalves WC. Oral man-
ifestations of systemic disease. Am Fam Physician 2010: 82:
1381–1388.
13. Civitelli R, Pilgram TK, Dotson M, Muckerman J, Lewan-
dowski N, Armamento-Villareal R, Yokoyama-Crothers N,
Kardaris EE, Hauser J, Cohen S, Hildebolt CF. Alveolar and
postcranial bone density in postmenopausal women
receiving hormone ⁄ estrogen replacement therapy: a ran-
domized, double-blind, placebo-controlled trial. Arch In-
tern Med 2002: 162: 1409–1415.
14. Cohen ME, Simecek JW. Effects of gender-related factors
on the incidence of localized alveolar osteitis. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod 1995: 79: 416–422.
15. Daniell HW. Postmenopausal tooth loss. Contributions to
edentulism by osteoporosis and cigarette smoking. Arch
Intern Med 1983: 143: 1678–1682.
16. Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier
PJ, Vieth R. Estimates of optimal vitamin D status. Osteo-
poros Int 2005: 16: 713–716.
17. Drozdzowska B, Pluskiewicz W, Michno M. Tooth count in
elderly women in relation to their skeletal status. Maturitas
2006: 55: 126–131.
18. Drug facts and comparisons, 65th edn. Baltimore, MD:
Lippincott Williams & Wilkins, 2011.
229
Therapeutic challenges through female continuum

19. Dugdale M. Anemia. Obstet Gynecol Clin North Am 2001:
28: 363–381.
20. el-Ashiry GM, el-Kafrawy AH, Nasr MF, Younis N. Effects of
oral contraceptives on the gingiva. J Periodontol 1971: 42:
273–275.
21. Famili P, Cauley J, Suzuki JB, Weyant R. Longitudinal study
of periodontal disease and edentulism with rates of bone
loss in older women. J Periodontol 2005: 76: 11–15.
22. Ferguson MM, Carter J, Boyle P. An epidemiological study
of factors associated with recurrent aphthae in women.
J Oral Med 1984: 39: 212–217.
23. Gajendra S, Kumar JV. Oral health and pregnancy: a review.
N Y State Dent J 2004: 70: 40–44.
24. Glenn FB. Immunity conveyed by a fluoride supplement
during pregnancy. ASDC J Dent Child 1977: 44: 391–395.
25. Glenn FB, Glenn WD 3rd, Duncan RC. Fluoride tablet
supplementation during pregnancy for caries immunity: a
study of the offspring produced. Am J Obstet Gynecol 1982:
143: 560–564.
26. Gur A, Nas K, Kayhan O, Atay MB, Akyuz G, Sindal D, Aksit
R, Oncel S, Dilsen G, Cevik R, Gunduz OH, Ersoy Y, Altay Z,
Ozturk C, Akkus S, Senocak O, Kavuncu V, Kirnap M,
Tekeoglu I, Erdogan F, Sarac AJ, Demiralp L, Demirkesen A,
Adam M. The relation between tooth loss and bone mass in
postmenopausal osteoporotic women in Turkey: a multi-
center study. J Bone Miner Metab 2003: 21: 43–47.
27. Hertz RS, Beckstead PC, Brown WJ. Epithelial melanosis of
the gingiva possibly resulting from the use of oral contra-
ceptives. J Am Dent Assoc 1980: 100: 713–714.
28. Horton AL, Boggess KA, Moss KL, Beck J, Offenbacher S.
Periodontal disease, oxidative stress, and risk for pre-
eclampsia. J Periodontol 2010: 81: 199–204.
29. Jeffcoat MK, Hauth JC, Geurs NC, Reddy MS, Cliver SP,
Hodgkins PM, Goldenberg RL. Periodontal disease and
preterm birth: results of a pilot intervention study. J Peri-
odontol 2003: 74: 1214–1218.
30. Jeffcoat MK, Lewis CE, Reddy MS, Wang CY, Redford M.
Post-menopausal bone loss and its relationship to oral
bone loss. Periodontol 2000 2000: 23: 94–102.
31. Kalkwarf KL. Effect of oral contraceptive therapy on gin-
gival inflammation in humans. J Periodontol 1978: 49: 560–
563.
32. Krejci CB, Bissada NF. Women�s health issues and their
relationship to periodontitis. J Am Dent Assoc 2002: 133:
323–329.
33. Kumar PS. Sex and the subgingival microbiome: do female
sex steroids affect subgingival bacteria? Periodontol 2000
2013: 61: 103–124.
34. Little JW, Falace D, Miller C, Rhodus NL. (editors).
Pregnancy and breast feeding. Dental management of the
medically compromised patient. St Louis, MO: Mosby
Elsevier, 2008: 268–279.
35. Magnusson I, Ericson T, Hugoson A. The effect of oral
contraceptives on the concentration of some salivary sub-
stances in women. Arch Oral Biol 1975: 20: 119–126.
36. Mandel L, Kaynar A. Bulimia and parotid swelling: a review
and case report. J Oral Maxillofac Surg 1992: 50: 1122–1125.
37. Mariotti A. Sex steroid hormones and cell dynamics in the
periodontium. Crit Rev Oral Biol Med 1994: 5: 27–53.
38. Matteson SR, Joseph LP, Bottomley W, Finger HW, From-
mer HH, Koch RW, Matranga LF, Nowak AJ, Rachlin JA,
Schoenfeld CM. The report of the panel to develop radio-
graphic selection criteria for dental patients. Gen Dent
1991: 39: 264–270.
39. Mohammad AR, Brunsvold M, Bauer R. The strength of
association between systemic postmenopausal osteoporo-
sis and periodontal disease. Int J Prosthodont 1996: 9: 479–
483.
40. National Institutes of Health. NIH Consensus conference.
Optimal calcium intake. NIH Consensus Development
Panel on Optimal Calcium Intake. JAMA 1994: 272: 1942–
1948.
41. Offenbacher S, Lin D, Strauss R, McKaig R, Irving J, Barros
SP, Moss K, Barrow DA, Hefti A, Beck JD. Effects of peri-
odontal therapy during pregnancy on periodontal status,
biologic parameters, and pregnancy outcomes: a pilot
study. J Periodontol 2006: 77: 2011–2024.
42. Otomo-Corgel J. Systemic considerations for female pa-
tients. In: Newman MG, van Winkelhoff AJ editors. Anti-
biotic and antimicrobial use in dental practice. Chicago, IL:
Quintessence Pub. Co., 2001: 636–649.
43. Otomo-Corgel J, Steinberg B. Periodontal medicine and the
female patient. In: Rose LF, Genco R, Cohen D, Mealey B
editors. Periodontal medicine. Hamilton, ON; St. Louis: B.C.
Decker, 2000: 151–166.
44. Pilgram TK, Hildebolt CF, Dotson M, Cohen SC, Hauser JF,
Kardaris E, Civitelli R. Relationships between clinical
attachment level and spine and hip bone mineral density:
data from healthy postmenopausal women. J Periodontol
2002: 73: 298–301.
45. Preshaw PM. Oral contraceptives and the periodontium.
Periodontol 2000 2013: 61: 125–159.
46. Reinhardt RA, Payne JB, Maze CA, Patil KD, Gallagher SJ,
Mattson JS. Influence of estrogen and osteopenia ⁄ osteo-
porosis on clinical periodontitis in postmenopausal
women. J Periodontol 1999: 70: 823–828.
47. Robb-Nicholson C. (editor). Gastroesophageal reflux dis-
ease. Harv Women�s Health Watch 1997: 4: 4.
48. Rockenbach MI, Marinho SA, Veeck EB, Lindemann L,
Shinkai RS. Salivary flow rate, pH, and concentrations of
calcium, phosphate, and sIgA in Brazilian pregnant and
non-pregnant women. Head Face Med 2006: 2: 44.
49. Ronderos M, Jacobs DR, Himes JH, Pihlstrom BL. Associ-
ations of periodontal disease with femoral bone mineral
density and estrogen replacement therapy: cross-sectional
evaluation of US adults from NHANES III. J Clin Period-
ontol 2000: 27: 778–786.
50. Ruma M, Boggess K, Moss K, Jared H, Murtha A, Beck J,
Offenbacher S. Maternal periodontal disease, systemic
inflammation, and risk for preeclampsia. Am J Obstet
Gynecol 2008: 198: 389.e1–389.e5.
51. Schumann K, Ettle T, Szegner B, Elsenhans B, Solomons
NW. On risks and benefits of iron supplementation rec-
ommendations for iron intake revisited. J Trace Elem Med
Biol 2007: 21: 147–168.
52. Sweet JB, Butler DP. Increased incidence of postoperative
localized osteitis in mandibular third molar surgery asso-
ciated with patients using oral contraceptives. Am J Obstet
Gynecol 1977: 127: 518–519.
53. Taguchi A, Sanada M, Suei Y, Ohtsuka M, Nakamoto T, Lee
K, Tsuda M, Ohama K, Tanimoto K, Bollen AM. Effect of
estrogen use on tooth retention, oral bone height, and oral
bone porosity in Japanese postmenopausal women. Men-
opause 2004: 11: 556–562.
230
Otomo-Corgel

54. Takaishi Y. [Treatment of periodontal disease, prevention
and bisphosphonate]. Clin Calcium 2003: 13: 173–176.
55. Takaishi Y, Ikeo T, Miki T, Nishizawa Y, Morii H. Sup-
pression of alveolar bone resorption by etidronate treat-
ment for periodontal disease: 4- to 5-year follow-up of four
patients. J Int Med Res 2003: 31: 575–584.
56. Tuccori M, Testi A, Antonioli L, Fornai M, Montagnani S,
Ghisu N, Colucci R, Corona T, Blandizzi C, Del Tacca M.
Safety concerns associated with the use of serotonin re-
uptake inhibitors and other serotonergic ⁄ noradrenergic
antidepressants during pregnancy: a review. Clin Ther
2009: 31(Pt 1): 1426–1453.
57. Turner M, Aziz SR. Management of the pregnant oral and
maxillofacial surgery patient. J Oral Maxillofac Surg 2002:
60: 1479–1488.
58. Wilson JT, Brown RD, Cherek DR, Dailey JW, Hilman B,
Jobe PC, Manno BR, Manno JE, Redetzki HM, Stewart JJ.
Drug excretion in human breast milk: principles, pharma-
cokinetics and projected consequences. Clin Pharmacoki-
net 1980: 5: 1–66.
59. Woo SB, Hellstein JW, Kalmar JR. Narrative [corrected]
review: bisphosphonates and osteonecrosis of the jaws.
Ann Intern Med 2006: 144: 753–761.
60. Wrzosek T, Einarson A. Dental care during pregnancy. Can
Fam Physician 2009: 55: 598–599.
61. Yoshihara A, Seida Y, Hanada N, Miyazaki H. A longitudinal
study of the relationship between periodontal disease and
bone mineral density in community-dwelling older adults.
J Clin Periodontol 2004: 31: 680–684.
62. Yoshihara A, Seida Y, Hanada N, Nakashima K, Miyazaki H.
The relationship between bone mineral density and the
number of remaining teeth in community-dwelling older
adults. J Oral Rehabil 2005: 32: 735–740.
63. Zachariasen RD. The effect of elevated ovarian hormones
on periodontal health: oral contraceptives and pregnancy.
Women Health 1993: 20: 21–30.
231
Therapeutic challenges through female continuum