AVANCES EN EL CONOCIMIENTO SOBRE EL DAÑO …FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO Uso de...
61
Transcript of AVANCES EN EL CONOCIMIENTO SOBRE EL DAÑO …FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO Uso de...


AVANCES EN EL CONOCIMIENTO
SOBRE EL DAÑO ACUMULADO
EN LUPUS ERITEMATOSO SISTÉMICO Y SU PREVENCIÓN
Dr. José Mª Pego Reigosa, Complejo Hospitalario Universitario de [email protected]
Madrid, 27 de septiembre de 2019

Conflictos de interés
Investigador principal de RELESSER
GSK, Roche, Lilly, UCB y Novartis financiaron la fase transversal de RELESSERLa Sociedad Española de Reumatología y GSK financian la fase longitudinal de RELESSER.

• EVALUACIÓN DEL LUPUS ERITEMATOSO SISTÉMICO
• DEFINICIÓN Y MEDICIÓN DEL DAÑ0
• FACTORES ASOCIADOS A LA PRESENTACIÓN DEL DAÑO
• FÁRMACOS Y DAÑO
• DAÑO Y MORTALIDAD
• NUEVOS DATOS EN RELACIÓN CON EL ACÚMULO DE DAÑO
• PREVENCIÓN DEL DAÑO
AGENDA

OMERACT (Outcome Measures in Rheumatology Clinical Trials)
FDA (Food and Drug Administration)
EULAR (European League Against Rheumatism)
Smolen JS, et al. Randomized clinical trials and longitudinal observational studies in SLE: consensus on a preliminary core set of outcome domains. J Rheumatol 1999;26:504-7. Strand V, et al. Outcome measures to be used in clinical trials in SLE. J Rheumatol 1999;26:490–7FDA. Guidance for Industry Systemic Lupus Erythematosus - Developing Drugs for Treatment. 2005. http://www.fda.gov/cder/guidance/6496dft.pdfBertsias G, et al. Clinical trials in SLE: lessons from the past as we proceed to the future - the EULAR recommendations for themanagement of SLE and the use of end-points in clinical trials. Lupus 2008;17:437-42.
Actividad de la enfermedad
Daño acumulado
Calidad de vida relacionada con la salud (HRQoL)
Efectos adversos

DEFINICIÓN Y CAUSAS DE DAÑO
• CAMBIO IRREVERSIBLE✓ NO RELACIONADO CON INFLAMACIÓN ACTIVA,✓ QUE OCURRE DESDE EL DIAGNÓSTICO DEL LUPUS Y✓ PRESENTE DURANTE ≥ 6 MESES
• NO ES PRECISO QUE LA LESIÓN SEA ATRIBUIBLE AL LES, INCLUYE✓ COMORBILIDAD Y✓ EFECTOS ADVERSOS MEDICAMENTOSOS

Gladman D, et al. The development and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for SLE. Arthritis Rheum 1996;39:363-9.

¿CÓMO SE MIDE EL DAÑO?
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)
• 47 ÍTEMS (12 GRUPOS)
• EPISODIOS REPETIDOS (ACVA, IAM, ONA, ETC.) DEBEN OCURRIRSEPARADOS ≥ 6 MESES PARA PUNTUAR 2
• LA MISMA LESIÓN NO PUEDE PUNTUAR 2

¿CÓMO SE MIDE EL DAÑO?
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)
OCULAR (cualquier ojo, por evaluación clínica)
Catarata, el algún momento
Cambio en la retina u atrofia óptica
1
1
Puntos
NEUROPSIQUIÁTRICO
Deterioro cognitivo o psicosis mayor
Convulsiones que requieren terapia >6 meses
ACVA, en algún momento (puntuar 2 si >1)
Neuropatía craneal o periférica (excluyendo óptica)
Mielitis transversa
1
1
1 ó 2
1
1
RENAL
GFR estimada o medida <50%
Proteinuria ≥ 3,5g/24h
o
Enfermedad renal terminal (independiente de diálisis o trasplante)
1
1
3
PULMONAR
Hipertensión pulmonar (prominencia del VD, P2 reforzado)
Fibrosis pulmonar (física y radiográfica)
Pulmón encogido (Rx)
Fibrosis pleural (Rx)
Infarto pulmonar (Rx)
1
1
1
1
1

CARDIOVASCULAR
Angina o bypass coronario
Infarto de miocardio (puntuar 2 si >1)
Cardiomiopatía (disfunción ventricular)
Enfermedad valvular (soplo diastólico o sistólico >3/6)
Pericarditis durante 6 meses o pericardiectomía
1
1 ó 2
1
1
1
Puntos
VASCULAR PERIFÉRICO
Claudicación durante 6 meses
Pérdida tisular pequeña (pulpejo de los dedos)
Pérdida tisular importante (dedo o extremidad) (puntuar 2 si >1)
Trombosis venosa con tumefacción, ulceración o evidencia clínica de estasis venosa
1
1
1 ó 2
1
GASTROINTESTINAL
Infarto o resección intestinal por debajo de duodeno, resección de bazo, hígado o vesícula de
cualquier causa (puntuar 2 si >1)
Insuficiencia mesentérica
Peritonitis crónica
Estenosis o cirugía gastrointestinal alta
Insuficiencia pancreática que precise sustitución enzimática
1 ó 2
1
1
1
1
MÚSCULOESQUELÉTICO
Atrofia muscular o debilidad
Artritis deformante o erosiva (incluye deformidades reversibles, excluye necrosis avascular)
Osteoporosis con fractura o colapso vertebral (excluye necrosis avascular)
Necrosis avascular (diagnosticada con técnica de imagen) (puntuar 2 si >1)
Osteomielitis (con evidencia microbiológica)
Rotura tendinosa
1
1
1
1 ó 2
1
1
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)
¿CÓMO SE MIDE EL DAÑO?
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)

CUTÁNEO
Alopecia crónica cicatricial
Cicatrices extensas o secuelas de paniculitis (excluyendo cuero cabelludo o pulpejos)
Ulceración cutánea durante >6 meses (excluyendo trombosis)
1
1
1
Puntos
FALLO GONADAL PREMATURO (amenorrea secundaria antes de los 40 años) 1
DIABETES MELLITUS (independientemente del tratamiento) 1
CÁNCER (excluyendo displasia) (puntuar 2 si >1 sitio) 1 ó 2
TOTAL
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)
¿CÓMO SE MIDE EL DAÑO?
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)

SLICC/ACR DAMAGE INDEX
- ES UNA HERRAMIENTA VÁLIDA PARA MEDIR DAÑO EN EL LES
- ES FIABLE, SUS MEDICIONES SON REPRODUCIBLES
- ACONSEJABLE MEDIRLO ANUALMENTE
Gladman D, et al. The development and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for SLE. Arthritis Rheum 1996;39:363-9Gladman DD, et al. The reliability of the SLICC/ACR DI in patients with SLE. Arthritis Rheum 1997;40:809–13 Gladman DD, et al. The SLICC/ACR DI for SLE International Comparison. J Rheumatol 2000;27:373–6
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)
¿CÓMO SE MIDE EL DAÑO?
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)

ESTUDIOS LONGITUDINALES DE COHORTES DE LES HAN MOSTRADO QUE:
-LOS VALORES MEDIOS DE SDI AUMENTAN A LO LARGO DEL TIEMPO
Sutton EJ, et al. The SLICC DI: A systematic literature review. Semin Arthritis Rheum 2013;43: 352–61Pego-Reigosa JM, et al. Relationship between damage clustering and mortality in SLE in early and late stages of the disease: cluster analyses in a large cohort from the Spanish Society of Rheumatology Lupus Registry. Rheumatology 2016;55:1243-50
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)
¿CÓMO SE MIDE EL DAÑO?
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)

ACÚMULO DE DAÑO
Pego-Reigosa JM, et al. Relationship between damage clustering and mortality in SLE in early and late stages of the disease: cluster analyses in a large cohort from the Spanish Society of Rheumatology Lupus Registry. Rheumatology 2016;55:1243-50
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)
¿CÓMO SE MIDE EL DAÑO?
ÍNDICE DE DAÑO (SLICC/ACR DAMAGE INDEX)

• MAYOR EDAD AL DIAGNÓSTICO DEL LES
• ETNIA HISPÁNICA Y AFRICANA
• DAÑO ORGÁNICO PREEXISTENTE
• INFLAMACIÓN CRÓNICA
• HIPERTENSIÓN
• EXPOSICIÓN CRÓNICA A ESTEROIDES
Bruce IN, et al. Factors associated with damage accrual in patients with SLE: Results from the SLICC Inception Cohort. Ann Rheum Dis 2014;74:1706-13 Sutton EJ, et al. The SLICC DI: A systematic literature review. Semin Arthritis Rheum 2013;43:352–61López R, et al. Lupus disease activity and the risk of subsequent organ damage and mortality in a large lupus cohort. Rheumatology 2012;51:491–8Nossent J, et al. Disease activity and damage accrual during the early disease course in a multinational inception cohort of patients with SLE. Lupus 2010;19:949–56Maddison P, et al. The rate and pattern of organ damage in late onset SLE. J Rheumatol 2002;29: 913–7
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO

Mok CC, et al. Predictors and outcome of renal flares after successful cyclophosphamide treatment for diffuse proliferative lupus glomerulonephritis. Arthritis Rheum 2004;50:2559–68Ugarte-Gil MF, et al. The number of flares patients experience impacts on damage accrual in SLE: Data from a multiethnic Latin American cohort. Ann Rheum Dis 2014;74:1019–23
LOS BROTES DE LES CONTRIBUYEN AL
POSTERIOR DAÑO
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO

TANTO EN COHORTES DE INCEPCIÓN COMO PREVALENTES
LOS PACIENTES CON DAÑO TIENEN MAYOR RIESGO DE
ACUMULAR DAÑO ADICIONAL
Bruce IN, et al. Factors associated with damage accrual in patients with SLE: Results from the SLICC Inception Cohort. Ann Rheum Dis2014;74: 1706-13Alarcón GS, et al. SLE in three ethnic groups. XX. Damage as a predictor of further damage. Rheumatology 2004; 43:202–5Becker-Merok A, et al. Damage accumulation in SLE and its relation to disease activity and mortality. J Rheumatol 2006; 33:1570–7 Cardoso C, et al. Initial and accrued damage as predictors of mortality in Brazilian patients with SLE: A cohort study. Lupus 2008;17:1042–8
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO

Prasad R, et al. Anti-dsDNA and anti-Sm antibodies do not predict damage in SLE. Lupus 2006;15:285–91Ravelli A, et al. Assessment of damage in juvenile-onset SLE: A multicenter cohort study. Arthritis Rheum 2003;49:501–7Gladman DD, et al. Accrual of organ damage over time in patients with SLE. J Rheumatol 2003;30:1955–9
EL USO DE GLUCOCORTICOIDES SE RELACIONA FUERTEMENTE
CON VARIAS MANIFESTACIONES DE DAÑO
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO

TERAPIAS en algún momento
ANY TIMEOral corticosteroids 84.6%
Antimalarials 78.8%Azathioprine 31.2%
Cyclophosphamide 21.2%
Mycophenolate mofetil 16.6%Methotrexate 15.8%
i.v. Ig 4.2%Leflunomide 3.5%
Biologics:
- RTX 6.2%- TNF- antagonists 1.8%- Abatacept 0.3%
Plasma exchange 1.5%Splenectomy 1.4%
Pego-Reigosa JM, et al. Lupus 2014
Registry of SLE patients of the Spanish Society of Rheumatology (n 4.000)
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides

Daily dose
< 10 mg 41.5%
10-30 mg 8.6%
> 30 mg 2.3%
TERAPIAS en el momento de la última evaluación del paciente
Pego-Reigosa JM, et al. Lupus 2014
Registry of SLE patients of the Spanish Society of Rheumatology (n 4.000)
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides

FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides

van Staa TP, et al. The epidemiology of corticosteroid-induced osteoporosis: a meta-analysis. Osteoporos Int 2002;13:777-87
FUERTE CORRELACIÓN ENTRE:
• DOSIS ACUMULADA DE GC Y PÉRDIDA DE MASA ÓSEA
• DOSIS DIARIA Y EL RIESGO DE FRACTURA
Dosis de prednisona >5 mg/día o equivalente incrementan
el riesgo de fractura durante el período de tratamiento
OSTEOPOROSIS Y GLUCOCORTICOIDES. UN METAANÁLISIS
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides

Clore JN, Thurby-Hay L. Glucocorticoid-induced hyperglycemia. Endocr Pract 2009;15:469-74Gurwitz JH, et al. Glucocorticoids and the risk for initiation of hypoglycemic therapy. Arch Intern Med 1994;154:97-101
Los GC aumentan el riesgo de hiperglucemia de un modo dosis y tiempo dependiente tanto en diabéticos como en no diabéticos
El riesgo aumentó con el incremento de la dosis diaria media:OR 1,7 para 1-10mg/día de PRD o equivalenteOR 3,0 para 10-20mg/día de PRD o equivalenteOR 5,8 para 20-30mg/día de PRD o equivalenteOR 10,3 para ≥30mg/día de PRD o equivalente
n = 11.855 pacientes que tuvieron que empezar tratamiento para diabetesvs.
11.855 controles
DIABETES Y GLUCOCORTICOIDES
En pacientes que toman corticoides orales, la OR de desarrollar diabetes que requiera tratamiento:
2,3 (IC 95% = 1,9-2,6)
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides
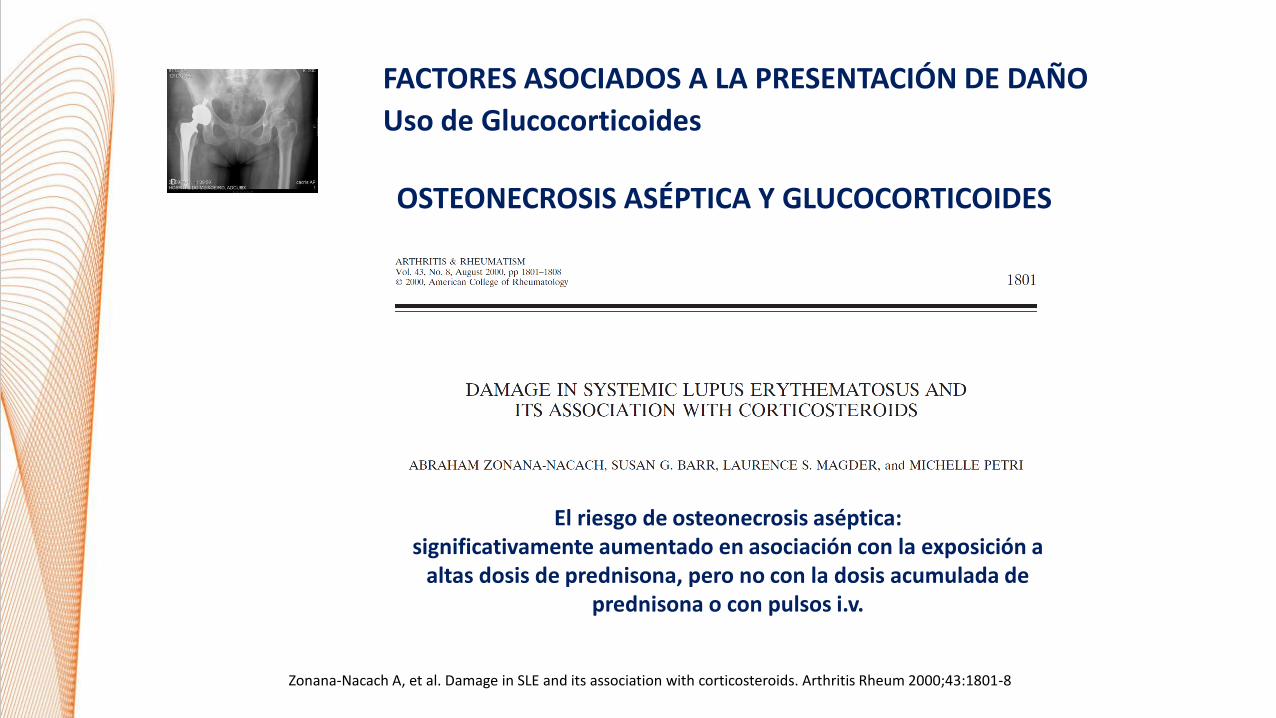
Zonana-Nacach A, et al. Damage in SLE and its association with corticosteroids. Arthritis Rheum 2000;43:1801-8
El riesgo de osteonecrosis aséptica:significativamente aumentado en asociación con la exposición a
altas dosis de prednisona, pero no con la dosis acumulada de prednisona o con pulsos i.v.
OSTEONECROSIS ASÉPTICA Y GLUCOCORTICOIDES
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides

Bruce IN. Rheumatology 2005;44:1492-502.Toloza SMA, et al. Arthritis Rheum 2004;50:3947-57.Manzi S, et al. Arthritis Rheum 1999;42:51-60.Manzi S, et al. Am J Epidemiol 1997;145:408-15.Petri M, et al. Am J Med 1992;93:513-9.Petri MA, et al. Am J Med 1994;96:254-9.Doria A, et al. Ann Rheum Dis 2003;62:107-17.
NO está establecida la dosis y duración del tratamiento GC que marca el punto de corte para un
riesgo cardiovascular aumentado
actividad de LES factores de riesgo C-V
GLUCOCORTICOIDES Y RIESGO CARDIOVASCULAR
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides
Zhang C, et al. J Clin Rheumatol 2009;15:111-6.Haque S, et al. J Rheumatol 2010;37:322-9.Roman MJ, et al. N Engl J Med 2003;349:2399-406.Urowitz MB, et al. J Rheumatol 2007;34:705.Karp I, et al. Arthritis Rheum 2008;59:169-75.Schanberg LE, et al. Arthritis Rheum 2009;60:1496-507.
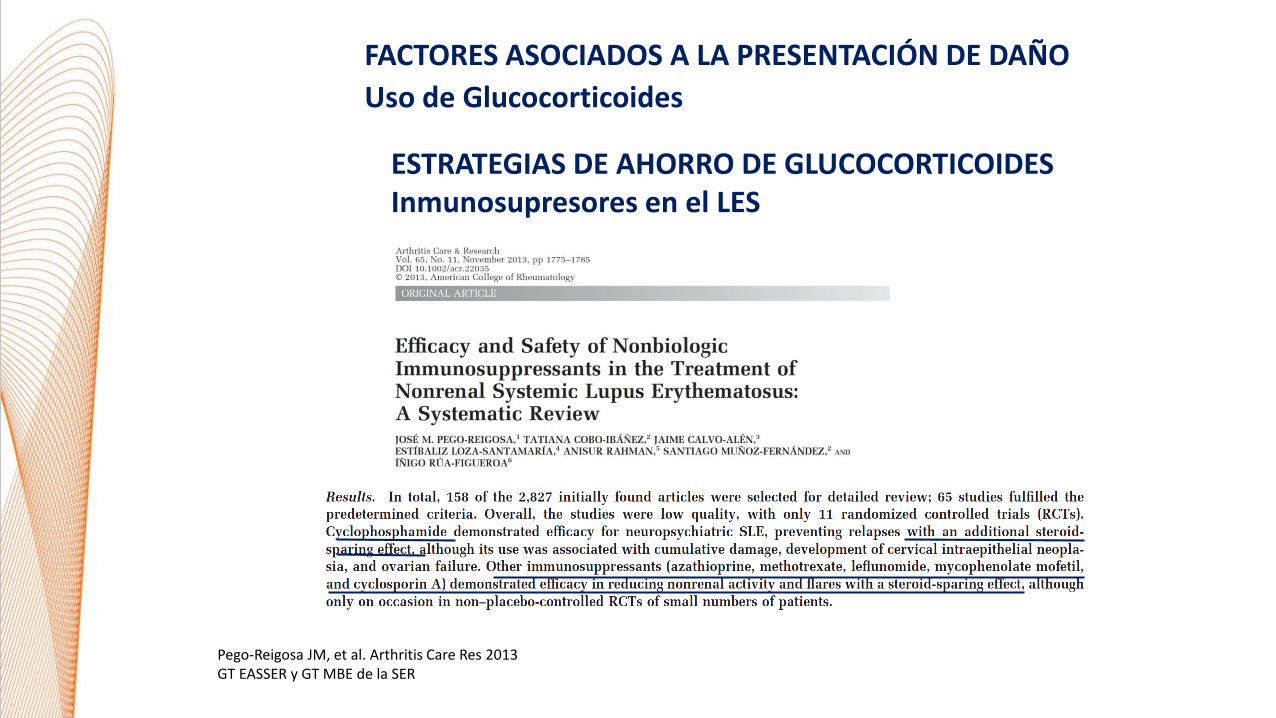
ESTRATEGIAS DE AHORRO DE GLUCOCORTICOIDESInmunosupresores en el LES
Pego-Reigosa JM, et al. Arthritis Care Res 2013GT EASSER y GT MBE de la SER
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides

Cobo-Ibáñez T, et al. Sem Arthritis Rheum 2014GT EASSER y GT MBE de la SER
ESTRATEGIAS DE AHORRO DE GLUCOCORTICOIDESInmunosupresores en el LES
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides

Navarra S, et al.Lancet 2011
ESTRATEGIAS DE AHORRO DE GLUCOCORTICOIDESBelimumab
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Uso de Glucocorticoides

ANTIPALÚDICOS Y DAÑO
Bruce IN, et al. Factors associated with damage accrual in patients with SLE: Results from the SLICC Inception Cohort. Ann Rheum Dis 2014;74:1706–13Fessler BJ, et al. SLE in three ethnic groups: XVI. Association of hydroxychloroquine use with reduced risk of damage accrual. Arthritis Rheum 2005;52:1473–80
• REDUCCIÓN DE BROTES,
• EFECTO AHORRADOR DE GLUCOCORTICOIDES Y
• EFECTOS FAVORABLES SOBRE DIVERSOS FACTORES DE RIESGO METABÓLICOS
El uso de antipalúdicos puede ejercer una protección contra el desarrollo de daño
FACTORES ASOCIADOS A LA PRESENTACIÓN DE DAÑO
Antipalúdicos

EL SDI PREDICE MORTALIDAD
Rahman P, et al. Early damage as measured by the SLICC/ACR DI is a predictor of mortality in SLE. Lupus 2001;10:93–6Nived O, et al. High predictive value of the SDI for survival in SLE. J Rheumatol 2002;29:1398–400Cardoso CR, et al. Initial and accrued damage as predictors of mortality in Brazilian patients with SLE: a cohort study. Lupus 2008;17:1042–8
COHORTE DE INCEPCIÓN; N = 263 PACIENTES CON LES
SEGUIMIENTO > 10 AÑOS
COMPARACIÓN EN LA MORTALIDAD A LOS 10 AÑOS
PACIENTES CON DAÑO EN EL AÑO 1VS
PACIENTES SIN DAÑO EN EL AÑO 1
25% VS. 7.3%.
DAÑO Y MORTALIDAD

Bruce IN, et al. Factors associated with damage accrual in patients with SLE: Results from the SLICC Inception Cohort. Ann Rheum Dis 2014;74:1706–13.
FACTORES ASOCIADOS AL ACÚMULO DE DAÑO (GRUPO SLICC)

Bruce IN, et al. Factors associated with damage accrual in patients with SLE: Results from the SLICC Inception Cohort. Ann Rheum Dis 2014;74:1706–13.
FACTORES ASOCIADOS AL ACÚMULO DE DAÑO (GRUPO SLICC)

Bruce IN, et al. Factors associated with damage accrual in patients with SLE: Results from the SLICC Inception Cohort. Ann Rheum Dis 2014;74:1706–13.
FACTORES ASOCIADOS AL ACÚMULO DE DAÑO (GRUPO SLICC)

Bruce IN, et al. Factors associated with damage accrual in patients with SLE: Results from the SLICC Inception Cohort. Ann Rheum Dis 2014;74:1706–13.
FACTORES ASOCIADOS AL ACÚMULO DE DAÑO (GRUPO SLICC)

PACIENTES CON DAÑO EN EL RECLUTAMIENTO ES MÁS PROBABLE QUETENGAN POSTERIOR ACÚMULO DE DAÑO (SDI 0 VS ≥1; P<0.001)
EDAD, ETNIA USA-AFRICANA, SLEDAI-2K SCORE, USO DE GC E HIPERTENSIÓN SE ASOCIARON A TRANSICIÓN DESDE “NO DAÑO” A “DAÑO” Y A INCREMENTOS EN EL DAÑO YA EXISTENTE
EL USO DE ANTIPALÚDICOS SE ASOCIÓ CON MENORES TASAS DE AUMENTODEL DAÑO PRE-EXISTENTE: 0.63 (0.44-0.89)
DAÑO SE ASOCIÓ CON FUTURA MORTALIDAD: HR (95% CI) 1.46 (1.18-1.81) POR PUNTO SDI
Bruce IN, et al. Factors associated with damage accrual in patients with SLE: Results from the SLICC Inception Cohort. Ann Rheum Dis 2014;74:1706–13.
FACTORES ASOCIADOS AL ACÚMULO DE DAÑO (GRUPO SLICC)

Pego-Reigosa JM, et al. Relationship between damage clustering and mortality in systemic lupus erythematosus in early and late stages of the disease: cluster analyses in a large cohort from the Spanish Society of Rheumatology Lupus Registry. Rheumatology 2016;55:1243-50
ACÚMULO DE DAÑO Y MORTALIDAD EN RELESSER

ACÚMULO DE DAÑO Y MORTALIDAD EN RELESSER
Pego-Reigosa JM, et al. Relationship between damage clustering and mortality in systemic lupus erythematosus in early and late stages of the disease: cluster analyses in a large cohort from the Spanish Society of Rheumatology Lupus Registry. Rheumatology 2016;55:1243-50

ACÚMULO DE DAÑO Y MORTALIDAD EN RELESSER
Pego-Reigosa JM, et al. Relationship between damage clustering and mortality in systemic lupus erythematosus in early and late stages of the disease: cluster analyses in a large cohort from the Spanish Society of Rheumatology Lupus Registry. Rheumatology 2016;55:1243-50

• Los sistemas con daño en fases más tempranas fueron:
– Musculoesquelético: 1.7% (1.2-2.2)
– Neuropsiquiátrico: 1.3% (0.8-1.7)
– Renal: 1.2% (0.8-1.6)
– Cardiovascular: 0.9% (0.6-1.3)
– Cutáneo: 0.8% (0.5-1.2)
CRONOLOGÍA DEL ACÚMULO DE DAÑO EN RELESSER

Número de pacientes con daño de acuerdo con la duración de la enfermedad:
Tiempo desde el diagnóstico del LES
Número de pacientes con daño en al menos 1
dominio
Incidencia acumulada (CI 95%)
1 año 194 7.4% (6.4-8.4)
5 años 464 18.9% (17.3-20.4)
> 10 años 658 29.2% (27.3-31.1)
CRONOLOGÍA DEL ACÚMULO DE DAÑO EN RELESSER

• 7,4% (6,4-8,4)
1 año
• 18,9%
(17,3-20,4)
5 años• 29,2%
(27,3-31,1)
10 años
La tasa de aumento de daño es significativamente mayor (p<0.001) poco
tiempo después del diagnóstico del LES, disminuyendo con el tiempo
Tasa de aumento: 2,9% por año
Tasa de aumento: 2,1% por año
Pego-Reigosa JM, et al. Chronological analysis of damage accrual in patients with SLE: results from the Spanish Registry. Presentado en el 10th European Meeting on SLE (Venecia, Octubre 2016), aceptado en EULAR y ACR Meeting 2016
CRONOLOGÍA DEL ACÚMULO DE DAÑO EN RELESSER

Clin Exp Rheumatol 2017 Jun 12. [Epub ahead of print] Juvenile- and adult-onset SLE: a comparative study in a large cohort from the Spanish Society of Rheumatology Lupus Registry (RELESSER). Torrente-Segarra V; RELESSER Study Group of the SER and the EASSER.
El daño acumulado, particularmente a nivel renal,
es significativamente mayor en el LES juvenil
Creatinine clearance <50%, p = 0,007Proteinuria >3.5g/24hs, p= 0,007Renal failure terminal, p<0,001
DAÑO EN LES JUVENIL.- DATOS DE RELESSER

DAÑO EN LES JUVENIL.- NUEVOS DATOS DE RELESSER
Torrente V, et al. Relationship between damage and mortality in juvenile-onset systemic lupus erythematosus: Cluster analyses in a large cohort from
the Spanish Society of Rheumatology Lupus Registry (RELESSER). Semin Arthritis Rheum. 2019 Jun;48(6):1025-1029.

DAÑO EN LES JUVENIL.- NUEVOS DATOS DE RELESSER
Torrente V, et al. Relationship between damage and mortality in juvenile-onset systemic lupus erythematosus: Cluster analyses in a large cohort from
the Spanish Society of Rheumatology Lupus Registry (RELESSER). Semin Arthritis Rheum. 2019 Jun;48(6):1025-1029.

DAÑO y MORTALIDAD. NUEVOS DATOS
Tejera-Segura B, et al. Rheumatology 2019.

Lupus 2016;25:699–709
BELIMUMAB Y ACÚMULO DE DAÑO

Lupus 2016;25:699–709
BELIMUMAB Y ACÚMULO DE DAÑO

Lupus 2016;25:699–709
BELIMUMAB Y ACÚMULO DE DAÑO

EL EFECTO A LARGO PLAZO DE BELIMUMAB SOBRE EL DAÑO ES MEDIADO:
- POR LA MEJORA EN LA ACTIVIDAD DEL LES Y/O
- POR EL EFECTO AHORRADOR DE CORTICOIDES
LOS PACIENTES CON LES MODERADO-SEVERO TRATADOS CON BELIMUMAB + SOC, A LOS 5-6 AÑOS TUVIERON BAJO ACÚMULO DE DAÑO
LOS PACIENTES CON DAÑO PRE-EXISTENTE, CON TEÓRICO MAYOR RIESGO DE DAÑO ADICIONAL, TAMBIÉN EXPERIMENTARON BAJAS TASAS DE DAÑO
Lupus 2016;25:699–709
BELIMUMAB Y ACÚMULO DE DAÑO

Van Vollenhoven et al. Rheumatology 2019.
BELIMUMAB Y ACÚMULO DE DAÑO.- NUEVOS DATOS

Urowitz MB, et al. Ann Rheum Dis 2019;78:372–379.
BELIMUMAB Y ACÚMULO DE DAÑO.- NUEVOS DATOS

Urowitz MB, et al. Ann Rheum Dis 2019;78:372–379.
BELIMUMAB Y ACÚMULO DE DAÑO.- NUEVOS DATOS

Urowitz MB, et al. Ann Rheum Dis 2019;78:372–379.
BELIMUMAB Y ACÚMULO DE DAÑO.- NUEVOS DATOS

Rheumatology (Oxford). 2017;56:121-8. Both prolonged remission and Lupus Low Disease Activity State are associated with reduced damage accrual in systemic lupus erythematosus. Tsang-A-Sjoe MW, Bultink IE, Heslinga M, Voskuyl AE.
BAJA ACTIVIDAD Y ACÚMULO DE DAÑO

183 pacientes; Mediana follow-up: 5 años
La remisión prolongada >5 años y LLDAS en >50% de las
observaciones se asocian con un riesgo menor de acúmulo de daño
(OR = 0.20, 95% IC: 0.07, 0.53, P = 0.001 y OR = 0.52, 95% IC: 0.28,
0.99, P = 0.046, respectivamente).
Rheumatology (Oxford). 2017;56:121-8. Both prolonged remission and Lupus Low Disease Activity State are associated with reduced damage accrual in systemic lupus erythematosus. Tsang-A-Sjoe MW, Bultink IE, Heslinga M, Voskuyl AE.
BAJA ACTIVIDAD Y ACÚMULO DE DAÑO

ESTADOS DE BAJA ACTIVIDAD O DE REMISIÓN PROLONGADOS
SE ASOCIAN CON MEJORES OUTCOMES (MENOS DAÑO)
Rheumatology (Oxford). 2017;56:121-8. Both prolonged remission and Lupus Low Disease Activity State are associated with reduced damage accrual in systemic lupus erythematosus. Tsang-A-Sjoe MW, Bultink IE, Heslinga M, Voskuyl AE.
BAJA ACTIVIDAD Y ACÚMULO DE DAÑO
ESTRATEGIAS TERAPÉUTICAS ACTIVAS

LOS PACIENTES CON DAÑO:
- ES MÁS PROBABLE QUE DESARROLLEN DAÑO A LO LARGO DEL TIEMPO.
- TIENEN MAYOR RIESGO DE MUERTE.
EL SDI ES FÁCIL DE REALIZAR EN LA PRÁCTICA CLÍNICA DIARIA E IDENTIFICA
PACIENTES CON LES EN RIESGO DE SUFRIR EVENTOS DESFAVORABLES.
LA FORMA MÁS EFECTIVA DE PREVENIR EL DAÑO ES LA ACTUACIÓN SOBRE
LOS FACTORES MODIFICABLES ASOCIADOS AL MISMO.
CONCLUSIONES (1)

1. REDUCIR AL MÁXIMO LA ACTIVIDAD DEL LES.
2. EL CONTROL ESTRICTO DE LA HIPERTENSIÓN Y OTROS FACTORES
DE RIESGO CARDIO-VASCULAR.
CONCLUSIONES (2)

3. PREVENIR LOS EFECTOS (DAÑO) INDUCIDO POR GLUCOCORTICOIDES:
3.1. RECOMENDACIONES: OSTEOPOROSIS INDUCIDA POR GC
3.2. RECOMENDACIONES (EULAR): PREVENCIÓN DE INFECCIONES.
3.3. OPTIMIZAR AL MÁXIMO EL USO DE GLUCOCORTICOIDES.
3.1. REDUCIR/EVITAR SU USO.
3.2. EMPLEO DE BOLOS I.V. SEGUIDOS DE DOSIS MÁS BAJAS.
3.3. NO DEMORAR EN EXCESO EL USO DE INMUNOSUPRESORES Y/O
BIOLÓGICOS
4. EMPLEO DE ANTIPALÚDICOS DESDE EL DIAGNÓSTICO DEL LES.
CONCLUSIONES (3)

RELESSER
Registro Español de Pacientes con LES de la
Sociedad Española de Reumatología
COMPLEJO HOSPITALARIO DE NAVARRA, COMPLEJO HOSPITALARIO DE OURENSE, COMPLEXO HOSPITAL XERAL-CALDE, FUNDACIÓNJIMÉNEZ DÍAZ, HOSPITAL CLÍNICO UNIVERSITARIO SALAMANCA, HOSPITAL COMARCAL DE L'ALT PENEDÉS, HOSPITAL COMARCAL DEMONFORTE, HOSPITAL DE BASURTO, HOSPITAL DE BELLVITGE, HOSPITAL DE CRUCES, HOSPITAL DE GRAN CANARIA DR. NEGRÍN,HOSPITAL DE GUADALAJARA, HOSPITAL DE LA PRINCESA, HOSPITAL DE LEÓN,HOSPITAL DE MARINA BAIXA, HOSPITAL DE VALME,HOSPITAL DO MEIXOEIRO, HOSPITAL DONOSTIA, HOSPITAL DR. PESET, HOSPITAL GENERAL DE ALICANTE, HOSPITAL GENERALUNIVERSITARIO CARLOS HAYA, HOSPITAL GENERAL UNIVERSITARIO GREGORIO MARAÑÓN, HOSPITAL GERMANS TRIAS I PUJOL,HOSPITAL INFANTA SOFÍA, HOSPITAL INSULAR DE GRAN CANARIA, HOSPITAL JEREZ DE LA FRONTERA, HOSPITAL JUAN CANALEJO(CHUAC), HOSPITAL LA PAZ, HOSPITAL MIGUEL SERVET, HOSPITAL PARC TAULÍ, HOSPITAL PRÍNCIPE DE ASTURIAS, HOSPITAL PUERTADE HIERRO, HOSPITAL RAMÓN Y CAJAL, HOSPITAL REINA SOFÍA, HOSPITAL SAN CECILIO, HOSPITAL SIERRALLANA, HOSPITAL SONLLÀTZER DE PALMA DE MALLORCA, HOSPITAL UNIVERSITARIO 12 DE OCTUBRE, HOSPITAL UNIVERSITARIO DE CANARIAS, HOSPITALUNIVERSITARIO MADRID NORTE SANCHINARRO, HOSPITAL VIRGEN DE LA ARRIXACA, HOSPITAL VIRGEN DE LA MACARENA,HOSPITAL MOISÈS BROGGI/HOSPITAL GENERAL, HOSPITAL UNIVERSITARIO MARQUÉS DE VALDECILLA, POVISA-POLICLÍNICA DEVIGO.

AVANCES EN EL CONOCIMIENTO
SOBRE EL DAÑO ACUMULADO
EN LUPUS ERITEMATOSO SISTÉMICO Y SU PREVENCIÓN
Dr. José Mª Pego Reigosa, Complejo Hospitalario Universitario de [email protected]
Madrid, 27 de septiembre de 2019