Cribado de TB en niños - uitb.cat · (e.g., diabetes mellitus, silicosis, cancer of head or neck,...
27
Cribado de TB en niños Antoni Soriano-Arandes Pediatra/Epidemiólogo Unitat de Salut Internacional-Tuberculosis Vall d’Hebron-Drassanes Hospital Universitari Vall Hebron
Transcript of Cribado de TB en niños - uitb.cat · (e.g., diabetes mellitus, silicosis, cancer of head or neck,...
Cribado de TB en niños
Antoni Soriano-Arandes
Pediatra/Epidemiólogo
Unitat de Salut Internacional-Tuberculosis
Vall d’Hebron-Drassanes
Hospital Universitari Vall Hebron
Introducción
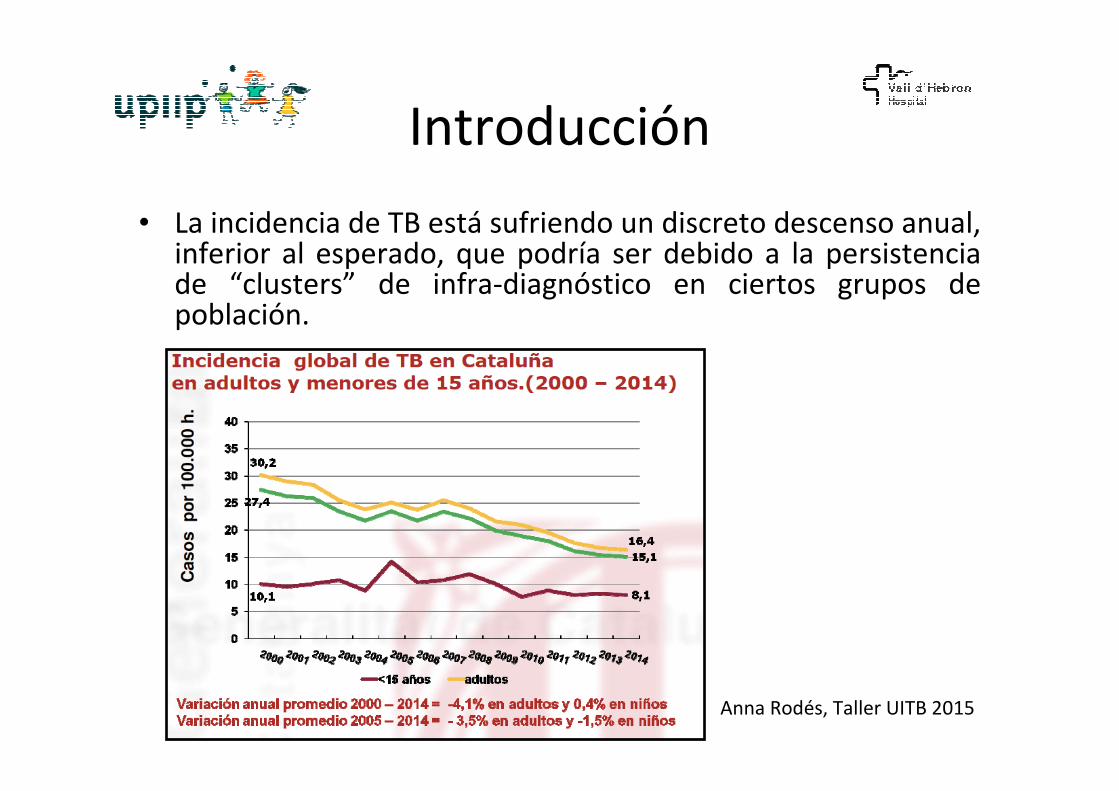
• La incidencia de TB está sufriendo un discreto descenso anual, inferior al esperado, que podría ser debido a la persistencia de “clusters” de infra-diagnóstico en ciertos grupos de población.
Anna Rodés, Taller UITB 2015

Anna Rodés, Taller UITB 2015
TB en edad pediátrica
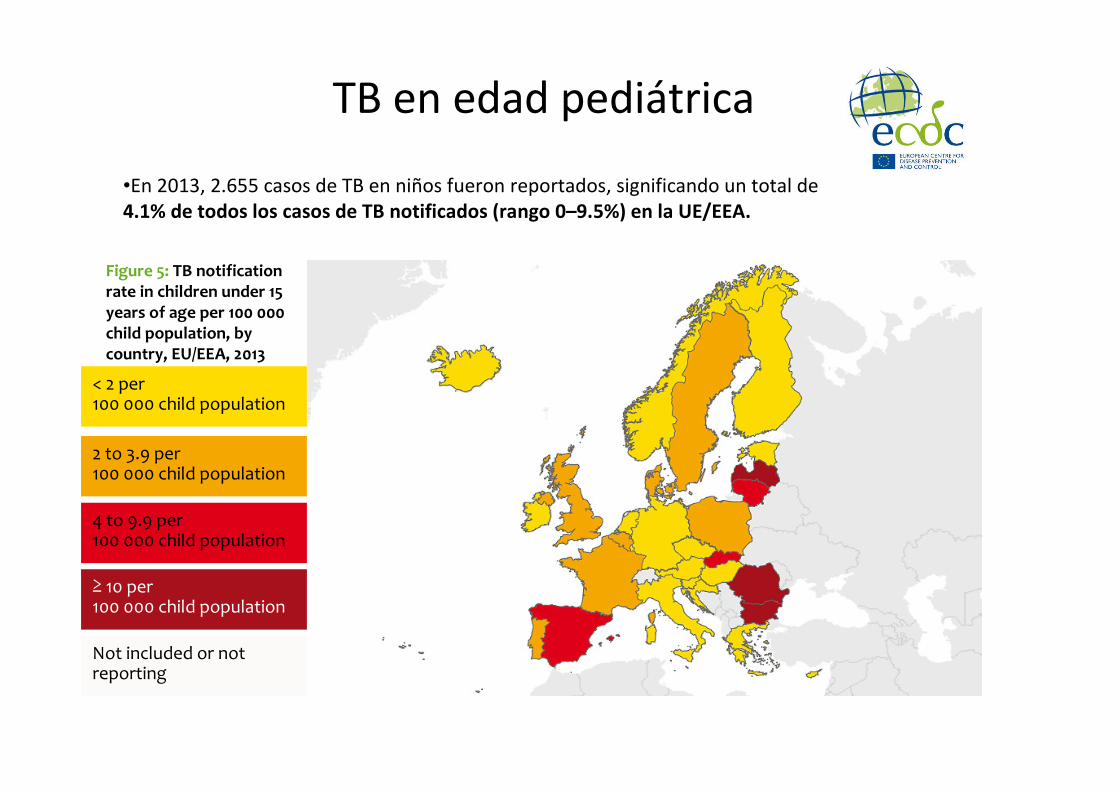
Figure 5: TB notification rate in children under 15 years of age per 100 000child population, by country, EU/EEA, 2013
Not included or not reporting
4 to 9.9 per 100 000 child population
2 to 3.9 per 100 000 child population
≥ 10 per 100 000 child population
< 2 per 100 000 child population
•En 2013, 2.655 casos de TB en niños fueron reportados, significando un total de
4.1% de todos los casos de TB notificados (rango 0–9.5%) en la UE/EEA.

Introducción
• La Organización Mundial de la Salud (OMS) estima que el principal grupo poblacional relacionado con un infra-diagnóstico son los niños pequeños*.
• Por este motivo, sugiere el cribado sistemático de algunos grupos con alto riesgo de TB y/o infección tuberculosa latente, especialmente en entornos epidemiológicos como el nuestro, de incidencia moderada o baja de TB, ya que es claramente coste-efectivo**.
• Se pueden definir 4 grupos de riesgo entre los niños:
– Contactos de casos de TB, – Niños con movilidad internacional, – Niños con inmunosupresión primaria, secundaria o adquirida y – Otros grupos de niños como los convivientes con personas
infectadas por el VIH, grupos con alta pobreza o marginalidad.
*Global Tuberculosis Report WHO 2015. Geneva, World Health Organization, 2015 (WHO/HTM/TB/2015.22).
**Systematic screening for active tuberculosis: principles and recommendations. ISBN 978 92 4 154860 1. WHO 2013.

Objetivos del cribado
• Reducir la morbilidad y mortalidad asociada a la TB con un diagnóstico precoz en grupos de riesgo,
• Reducir los casos de TB en el futuro asociados a la infección tuberculosa latente (ITL) en grupos de riesgo, y
• Establecer un balance entre los potenciales beneficios del cribado y los riesgos y costes que comportan esta actuación.

Epidemiología de la TB
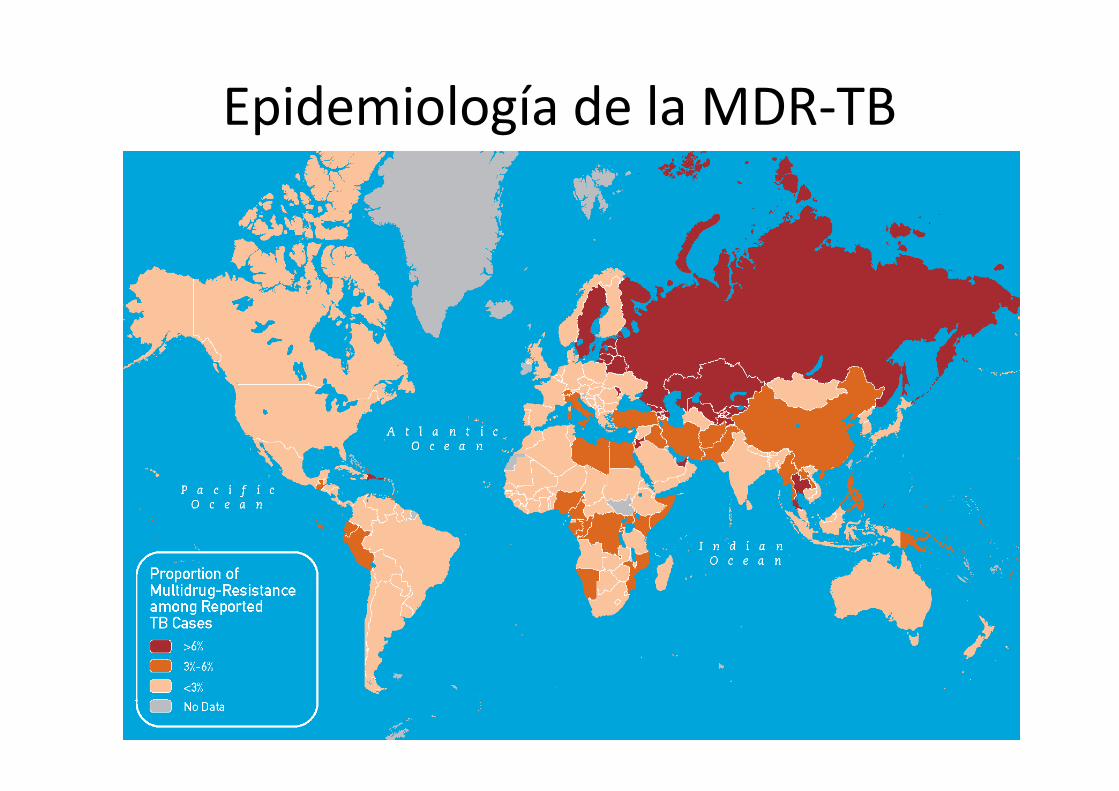
Epidemiología de la MDR-TB

People in high TB burden settings (estimated TB prevalence >100/100,000 in the
general population)

Sample TB Risk Assessment ToolRisk Factor•Recent contact with someone with infectious TB disease
•Foreign-born person from or recent traveler to HBC•Chest radiographs suggesting inactive or past TB
•HIV infection
•Organ transplant recipient
•Immunosuppression secondary to use of prednisone or TNF-α antagonists
•Injection drug user
•Resident or employee of high-risk congregate setting
(e.g., prison, long term care facility, hospital, homeless shelter)
•Medical conditions associated with risk of progressing to TB disease if infected
(e.g., diabetes mellitus, silicosis, cancer of head or neck, Hodgkin’s disease, leukemia,
and end-stage renal disease, intestinal bypass or gastrectomy, chronic malabsorption
syndrome, low body weight [10% or more below ideal for given population])
•Signs and symptoms of TB

TB HBC list
Angola
Bangladesh
Brazil
China
Democratic Peoples Republic of Korea
Democratic Republic of Congo
Ethiopia
India
Indonesia
Kenya
Mozambique
Myanmar
Nigeria
Pakistan
Philippines
Russian Federation
South Africa
Thailand
Tanzania, United Republic of
Viet Nam
Cambodia
Central African Republic
Congo
Lesotho
Liberia
Namibia
Papua New Guinea
Sierra Leone
Zambia
Zimbabwe

Definiciones
• Grupo de riesgo: grupo de personas sospechosas de estar infectadas por Mycobacterium tuberculosis, y que no buscan asistencia sanitaria por la TB propiamente, porque no tienen o no reconocen el riesgo de ITL o los síntomas de la TB,
• Visiting Friends and Relatives (VFR): niños que viven en nuestro entorno (nacidos aquí o no) que viajan alguna vez al país de origen de la familia, donde la incidencia de TB es ≥≥≥≥3 veces superior a la de nuestro país.
• Países de alta incidencia para TB: la incidencia global de TB es ≥ 3 veces superior a la nuestra.
Asia (excepto Japón), América Central y Sudamérica (excepto Chile, Costa Rica y Cuba), África Subsahariana y Norte de África, Este de
Europa incluyendo Rusia.
Tipo de niños en función de les áreas de riesgo para TB:
Niño inmigrante: niño nacido en un país con alta incidencia de TB, que ha
venido a vivir a nuestro país y que en ningún momento ha vuelto a su país
de origen.
VFR viajero (acrónimo del inglés visiting friends and relatives): niños
nacidos en nuestro entorno y que, para visitar familiares y amigos, viajan
alguna vez al país de origen de sus padres, donde la incidencia de TB es como mínimo tres veces superior a la de nuestro país.
VFR inmigrante: niño nacido en un país con alta incidencia de TB, que viaja a
nuestro país para vivir y viaja nuevamente a su país de origen una o más
veces para visitar sus familiares y amigos.
Definiciones

Grupos de riesgo para el cribado en Atención Primaria
• Niños que vienen de o visitan países de alta incidencia: inmigrante, VFR, turista y
emigrante a país de alta incidencia para TB.
• Niños con inmunosupresión primaria, secundaria o adquirida:
– infectados por el VIH,
– tratados con diálisis renal,
– que han recibido corticoides durante un período prolongado (>15mg/día
durante más de un mes),
– diabéticos,
– con enfermedades hematológicas,
– con síndromes de mal absorción crónica,
– con bajo peso, o
– que han estado sometidos a trasplante de órganos.
• Niños de otros grupos de riesgo: que conviven con adultos infectados por VIH,
usuarios de drogas vía parenteral y residentes en instituciones cerradas o en
prisión, con riesgo de pobreza extrema, situaciones de alto riesgo social, y
condiciones de hacinamiento en el domicilio habitual.


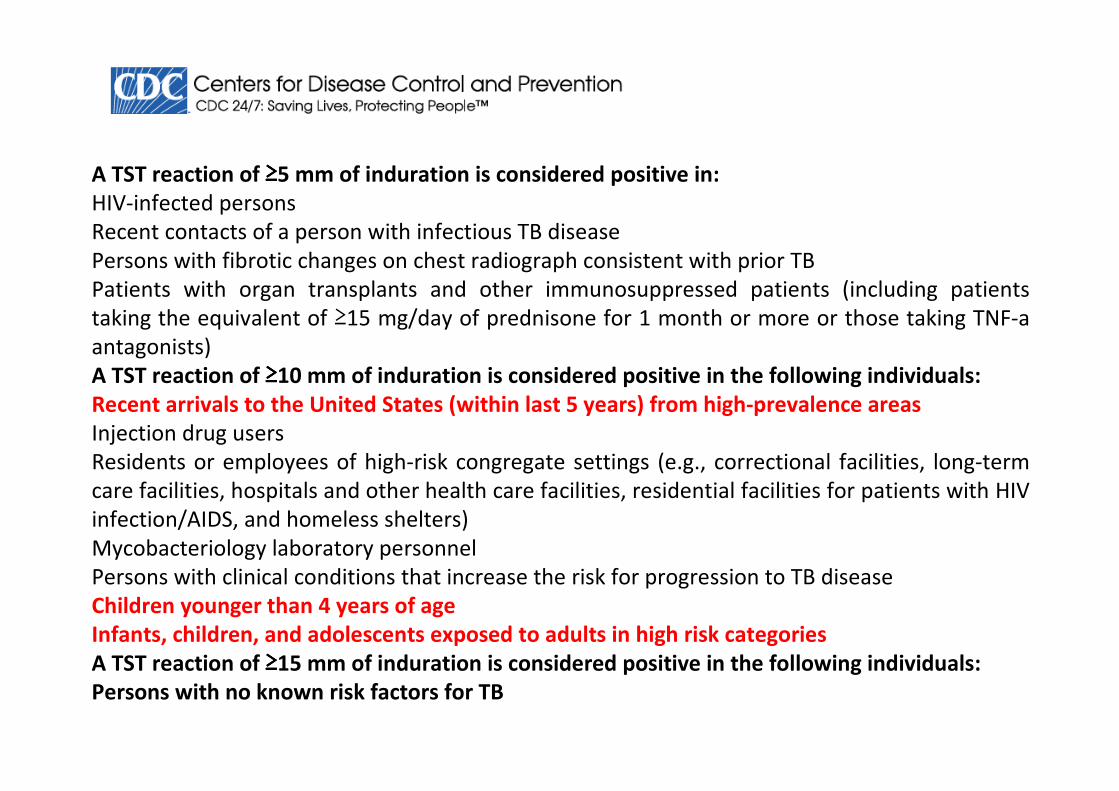
A TST reaction of ≥≥≥≥5 mm of induration is considered positive in:HIV-infected persons
Recent contacts of a person with infectious TB disease
Persons with fibrotic changes on chest radiograph consistent with prior TB
Patients with organ transplants and other immunosuppressed patients (including patients
taking the equivalent of ≥15 mg/day of prednisone for 1 month or more or those taking TNF-a
antagonists)
A TST reaction of ≥≥≥≥10 mm of induration is considered positive in the following individuals:Recent arrivals to the United States (within last 5 years) from high-prevalence areasInjection drug users
Residents or employees of high-risk congregate settings (e.g., correctional facilities, long-term
care facilities, hospitals and other health care facilities, residential facilities for patients with HIV
infection/AIDS, and homeless shelters)
Mycobacteriology laboratory personnel
Persons with clinical conditions that increase the risk for progression to TB disease
Children younger than 4 years of ageInfants, children, and adolescents exposed to adults in high risk categoriesA TST reaction of ≥≥≥≥15 mm of induration is considered positive in the following individuals:Persons with no known risk factors for TB

Selecting a Test to Detect TB Infection
•IGRAs are the preferred method of testing for:• Groups of people who have poor rates of return for TST reading and
interpretation (e.g., homeless persons)
• Persons who have received BCG vaccination
•TST is the preferred method for testing for:• Children under the age of 5 years
•Either TST or IGRA may be used without preference for other groups that are tested
for LTBI.
Certain situations where results from both TST and IGRA may be usefulRoutine testing with both TST and IGRA is not recommended. However, results from both tests
might be useful in the following situations:
•When the initial test is negative and:• The risk for infection, progression to disease, and/or a poor outcome is high (e.g., HIV-
infected persons or children under 5 years of age who are exposed to a person with
infectious TB).
• There is clinical suspicion for TB disease (e.g., signs, symptoms, and/or radiographic
evidence suggestive of TB disease) and confirmation of M. tuberculosis infection is
desired.
• Taking a positive result from a second test as evidence of infection increases detection sensitivity.
Certain situations where results from both TST and IGRA may be usefulRoutine testing with both TST and IGRA is not recommended. However, results from both
tests might be useful in the following situations:
•When the initial test is positive and:• Additional evidence of infection is required to encourage acceptance and
adherence to treatment (e.g., foreign-born health care workers who believe their
positive TST is due to BCG).
• The person has a low risk of both infection and progression from infection to TB disease.
• Requiring a positive result from the second test as evidence of infection increases the likelihood that the test reflects infection. An alternative is to assume, without
additional testing, that the initial result is a false positive or that the risk for disease
does not warrant additional evaluation or treatment, regardless of test results.

Influencia de la BCG
A history of BCG vaccination received in infancy can be ignored in all people aged10 years and older when interpreting an initial TST reaction of 10 mm or greater.
Cribado del niño inmigrante
• Niños de >2 años: realizarlo cuando acuden por primera vez
al CAP.
• Niños de <2 años: como tienen mas revisiones periódicas, 8-
12 semanas después de la primera visita.
Realizar la prueba de la tuberculina• Si PT previa negativa y, después de anamnesis, se
sospecha alto de riesgo de infección, repetirla.
Revisar cicatriz de BCG en brazo o glúteo
Recordar interpretar la PT en cada situación

Algoritmo de cribado
TB/ITBLen AP

¡¡¡MUCHAS
GRACIAS!!!