
Corregidofichas Farmacologicas Zoila y Valenzuela Emg de Pdt.
Upload
chakradhar-reddyCategory
view
165download
0
Technique of Electromyography and Normal EMG

Electromyography
•Needle electromyography refers to methods of studying the electrical activity of muscle
•It serves as additional aid to neurological examination in clinical practice for identifying and characterising disorders of motor unit, including anterior horn cells, peripheral nerves, NM junctions and muscles
•It requires Knowledge and skill

Motor unit•A single motor neuron with all the muscle fibres innervated by it constitutes a motor unit
•It is the functional unit of Motor component of peripheral nervous system
•There are 2 different types of motor units –slow firing fatigue resistant and fast firing fatigable units
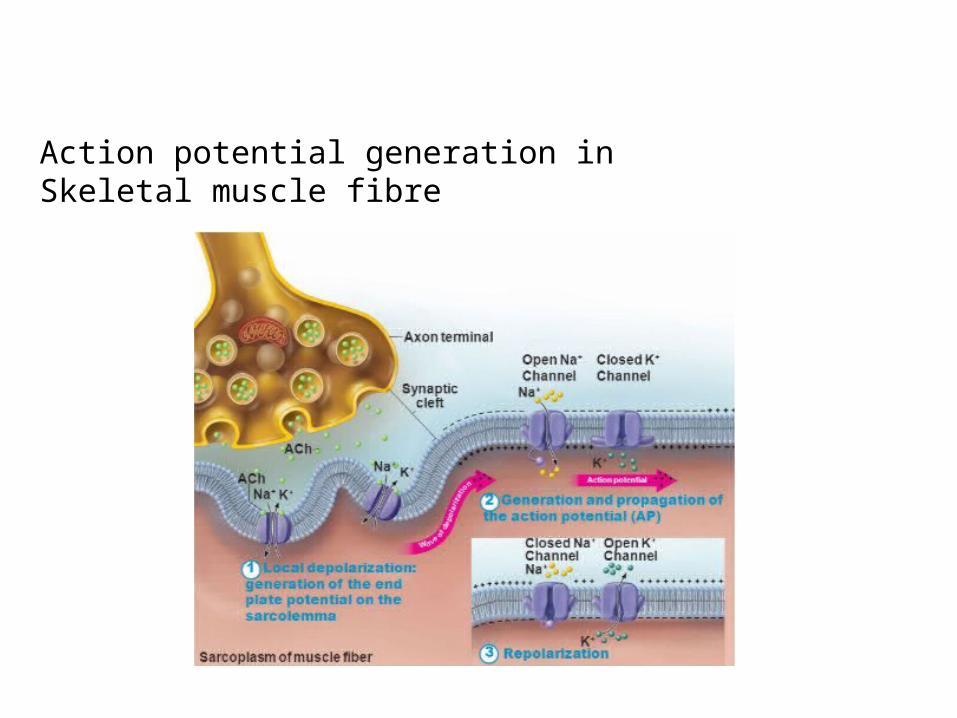
Action potential generation in Skeletal muscle fibre
•Once the Action potential is generated at the End Plate, a depolarising wave travels all along the length of muscle fibre
•Small segment of the muscle fibre act as dipole with positive charge at the advancing end negative charge at the other end resulting an electrical field through the surrounding connective tissue
•The strength of the current decreases in proportion to the square of the distance from the dipole in the skeletal muscle fibre.

•When two electrodes are placed apart in interstitium, due to difference in the distance from the dipole the field strength varies at the two electrodes there by generating a potential difference b/w them
Equipment•Electrodes•Amplifier•Filter•Display method
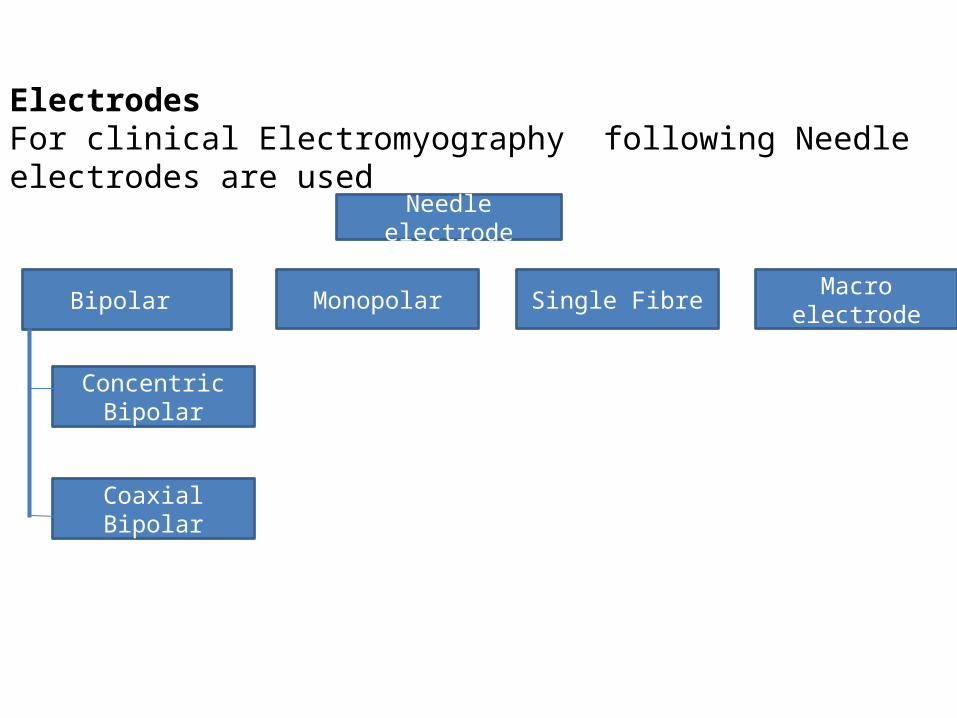
ElectrodesFor clinical Electromyography following Needle electrodes are used
Needle electrode
Concentric Bipolar
Monopolar
Coaxial Bipolar
Single Fibre Macro electrodeBipolar
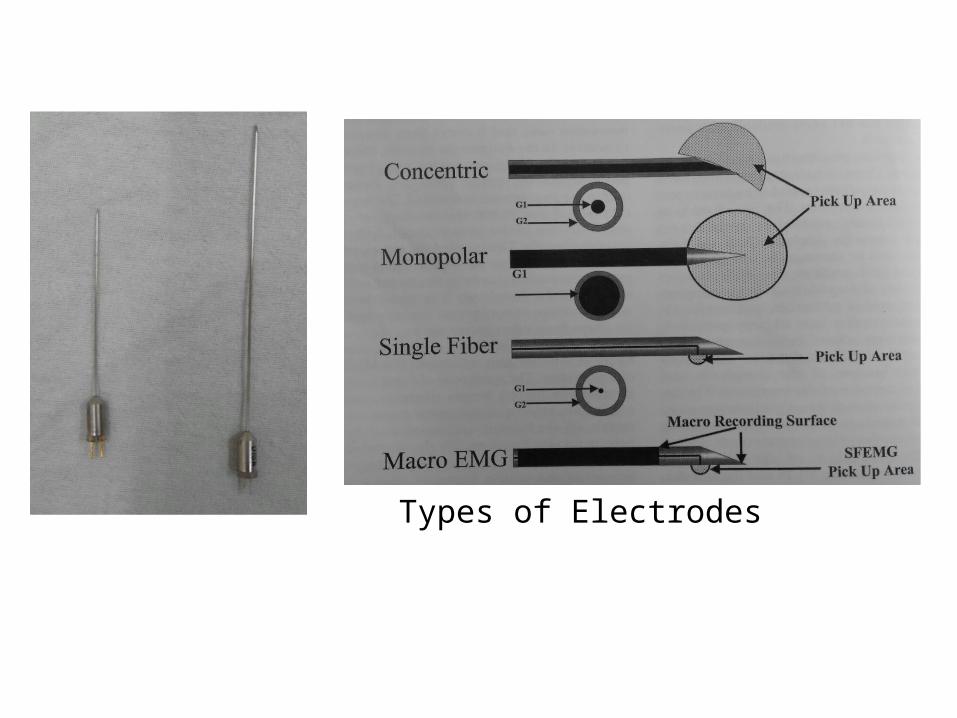
Types of Electrodes
Concentric Bipolar Needle•This electrode consists of a cannula with 2 wires within it•It records the potential difference b/w the two wires, as one acts as active and other as reference•It records from a very localised area, activity from only few muscle fibres is picked up•Amplitudes of MUPs are reduced due to reduced area
Monopolar electrode•Electrode inserted into muscle acts as active electrode, reference electrode is placed over the surface •Due to wide separation of the electrodes the resolution of the low amplitude signals is better, how ever the noise also gets amplified

Single fibre EMG needle•It has smaller leading edge to record from single muscle fibre rather than motor unit •Like concentric bipolar needle it has a cannula with a wire inside it but the wire is bent towards the side of the cannula few mm behind the tip
Macro electrode •It is suited for recording both from the single fibre and motor unit
Amplifiers•Bioelectrical potentials recorded will be in the range of 1μV to 1mV these signals need to be amplified by 1million to thousand times for deflection of 1cm in 1v/cm recording
•Differential amplifiers increases the amplitude of the desired response while rejecting unwanted noise
•Amplifiers ability to reject common signals is knownas its common mode rejection ratio (CMRR). The higherthe CMRR, the better the rejection

Gain •Amplifier gain describes the extent to which the input signal is increased in voltage.
Display sensitivity •Describes the visible waveform and is expressed as volts per division or volts per centimeter•Usually kept at 50-200μV/cm
Filters•They are used to selectively attenuate the noise preserving the signal•Band pass filters extending from 10HZ to 10KHZ is commonly used
Display
•Once the wave form is recorded and processed it is displayed for visual analysis
•As the EMG potentials have distinct auditory characteristics presenting them as audible sounds also helps in differentiating various responses
Preparing the patient•Prior to the test Patient should be briefly explained about the procedure and insertion of needle would cause some discomfort•Wipe the skin over the each puncture site with spirit before needle is inserted•Though most patients tolerate the pain some may require oral analgesic
Selecting the muscle•It is done on the basis of clinical indication•Ideally muscle selected should be superficial, easily palpated, Located away from major blood vessels and nerve trunks

Abductor pollices brevisNeedle insertion:at mid point of 1st metacarpel
Abductor digiti minimiNeedle insertion at mid point of 5th metacarpel
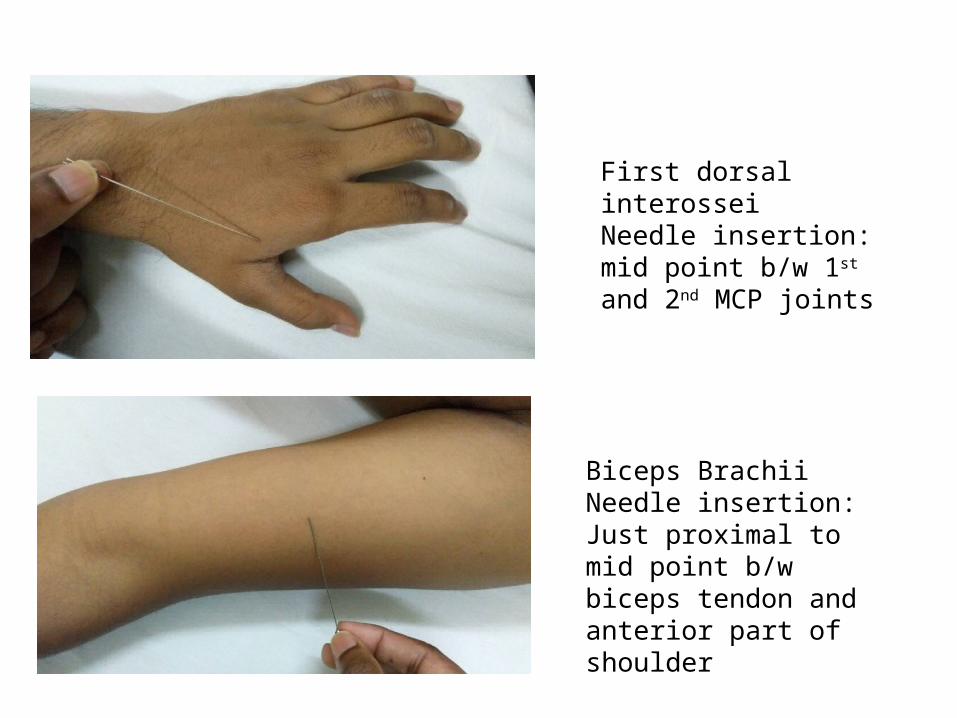
First dorsal interosseiNeedle insertion: mid point b/w 1st and 2nd MCP joints
Biceps BrachiiNeedle insertion: Just proximal to mid point b/w biceps tendon and anterior part of shoulder

Vastus lateralisNeedle insertion: lateral thigh 4 finger breadths proximal to lateral part of knee
Tibialis anteriorNeedle insertion: just lateral to tibial shin at junction of proximal 1/3rd and distal 2/3rd of tibia

Needle insertion•Prior to needle insertion the muscle should be palpated during intermittent contraction to localise its borders•Skin over the puncture site is made taut and needle is inserted smoothly into superficial layers of the muscle•When testing the small muscles needle should be inserted obliquely to increase the needles path
Needle movement•Needle is moved along a straight line in to the muscle in short steps of 0.5-1mm as large movements are more painful•Needle is advanced in 5-30 such steps with brief pause b/w each step

•Once the diameter of the muscle is traversed needle is withdrawn till subcutaneous plain and reinserted from a different angle at same location •All the 4 quadrants should be sampled for achieving good recording
Precautions•For patient with bleeding disorders or those on anticoagulantsINR should be <2Platelet count >20,000•Caution should be taken in patients with skin infection, cellulitis•Patient s with prosthetic heart valves may have risk of infective endocarditis

Findings in Normal EMG
Insertional activity•Burst of high frequency positive or negative spikes occurring during the movement of the needle electrode•It occurs due to stimulation of muscle fibres due to mechanical irritation/injury by the penetrating needle•The level of response depends on magnitude and speed of needle movement•It lasts for about few hundred milliseconds•Though it is a normal response exaggeration/attenuation of this response may suggest pathology
End plate noise•It is frequent irregular low amplitude (10-50μv )negative waveform with duration of 1-2ms•It correspond to miniature end plate potential•It occurs with the release of acetylcholin due to irritation of intramuscular nerve terminals by the needle tip at the end plate region•Sounds like seashell held to the ear•Following botulinum inj analysis of end plate noise helps to evaluate the neuromuscular transmission

End plate spike•It is irregular high amplitude(100-200μv)negative waveform with duration of 3-4ms•It occurs due to stimulation of the single muscle fibre by the tip of the needle at the end plate
Small irregular positive discharges may also occur at the end plate particularly with concentric needles, these are considered to be normal
Fibrillation potentials•These are spontaneous action potentials that arise from single muscle fibre.•Oscillations in resting membrane potential triggering action potential result in fibrillation• Occasionally they may occur in normal healthy muscle•They have regular firing pattern with freq 1-30Hz•Amp litude:20-500μv, Duration of 1-5ms•Pathologically significant when detected in at least three separate sites within the muscle being examined.

FASCICULATION POTENTIALS•They are similar to motor unit action Potentials occurs due to spontaneous activation of the muscle fibres of individual motor units.•Stimulus can originate at any level from anterior horn cell to axon terminal•About 77% of normal individuals can have fasciculations•Association with fibrillations, positive sharp waves suggest pathological fasciculations•Generally Benign fasciculations fire at higher frequency(1-2Hz) than pathological fasciculations(<1Hz), however it is difficult to differentiate benign from pathological

Morphology Frequency Amplitude Duration rhythm Auditory component
End plate noise
Monophasic Negative wave form
20-40Hz 10-50μv 1-2ms Irregular Sea shell held to ear
End plate spike
Biphasic with initial Sharpe negative wave form
5-50Hz 100-200μv 3-4ms Irregular Cracking sound
Positive Sharpe wave
Biphasic with initial positive followed by slow negative
0.5-30Hz 20-200μv 10-15ms Regular Dull pop
Fibrillation Bi/Triphasic with initial positive
1-30HzAvg 13 Hz
20-500μv 1-5ms Regular High pitched ,rain drop on roof
Fasciculation Tri/polyphasic
1-2Hz >300μv 15-20ms Irregular Low pitched popping

Motor Unit Action Potential(MUAP)The motor unit action potential is a compound potential representing the sum of the individual action potentials generated in the few muscle fibres of the unit that are within the pick-up range of the recording electrode
Components:•Amplitude•Duration•Rise time•Phases•Area
Amplitude:•It is measured between the greatest positive and the greatest negative deflections of the potentials.•When recorded by a concentric needle electrode, it isusually between 200 μV and 3 mV
Factors influencing the Amplitude of MUP•Predominantly determined by the action potentials of fibres that lie close to the recording electrode•Slight movement of the electrode has significant effect on amplitude•Temporal dispersion of the individual action potentials also affects to some extent
Rise time of MUP•It is the time lag from the initial positive peak to the subsequent negative peak of the MUP.• It reflects the distance between the recording electrode and the muscle fibres of the motor unit•Rise time less than 500μs indicate appropriate position of the electrode within the motor unit territory
Duration of MUPMeasured from the initial deflection from the base line to the final return to the base line•It indicate the synchrony among various fibres of a motor unit•It is influenced by fibres in the recording region that may extend to about 2-2.5mm radius from the needle•Normally varies from 5-15ms
Area of the MUP •It depends on the number of muscle fibres with in 2mm radius of the recording electrode•Movement of the electrode has significant effect on area•Ratio of amplitude to area is stable and less affected by electrode movement•Helps to differentiate neuropathy from myopathy
Phases of MUPIt is determined by counting the number of base line crossings of MUP plus one•It indicates the synchrony among the individual muscle fibres of a motor unit•Usually MUP has 2-4 phases, when >4 it is called polyphasic•In normal limb muscles about 12 percent may have five or more phases (polyphasic)
Satellite potential•It is a late spike distinct from main potential, that is time locked to the main potential•Generated by muscle fibre in a motor unit that has long nerve terminal, distant end plate region•Latency can rage from 8-32ms•It can occur in both pathologic and normal muscle

Pick up area within a motor unit territory
Motor unit potentials
Physiologic Factors Influencing MUPs•Patient age,Increasing age from infancy to adulthood there is an increase in the mean duration of motor unit action potentials in limb muscles•Intramuscular temperature,As temperature declines Mean duration of motor unit potentials and the number of polyphasic potentials also increase• The site of the recording electrode within the muscle, and Particular muscle under examination
MOTOR UNIT DISCHARGE PATTERNRecruitment•As the force of contraction increases, first the firing rate of the particular active unit increases until it reaches a certain frequency when additional units are recruited•Normal ratio of firing frequency to the number of motor units is 5:1•Maximum firing rate of a motor unit is about 30-50HZ •The order of recruitment depends on Diameter of neuron, synaptic density, Threshold of recruitment, type of motor units•It depends on patients effort, input from cortex, number of active motor units available
Interference•During the maximum contraction of muscle several motor units get activated simultaneously resulting in the over lap of MUPs creating an interference pattern•It gives a simple measure of number of firing units at maximum effort•It is influenced by factors that alter recruitment
Mechanical artefacts during EMGElectrode noise:•It occurs due to generation of potentials by the active metals of electrodes at junction of needle tip and interstitial fluid•This can distort the signal that is being recorded•Using inert metals –stainless steel, platinum this can be minimized
Electrostatic and Electromagnetic interferenceThis occurs from electric appliances- Fans, lamps due to use of AC currentInterference occurs at 50-60Hz It can be minimised by bundling wires of the recording and ground electrode, relocating the wires of appliances, shielding the recording area
Mobile phone use at the recording area also produces artefacts that resemble complex repetitive discharges
Conclusion
•EMG is an important additional aid in evaluating patients with peripheral neuromuscular disorder •It has great sensitivity and specificity•Good recording of various waveforms require high technical skills•Knowledge about various normal and abnormal findings is required for proper interpretation and application of test results
Thank You


















