¿Es seguro el TAR en pacientes con filtrado glomerular
32
¿Es seguro el TAR en pacientes con filtrado glomerular <90 ml/min? Félix Gutiérrez Universidad Miguel Hernández Hospital General Universitario de Elche
Transcript of ¿Es seguro el TAR en pacientes con filtrado glomerular

¿Es seguro el TAR en pacientes
con filtrado glomerular <90
ml/min?
Félix Gutiérrez
Universidad Miguel Hernández
Hospital General Universitario de Elche
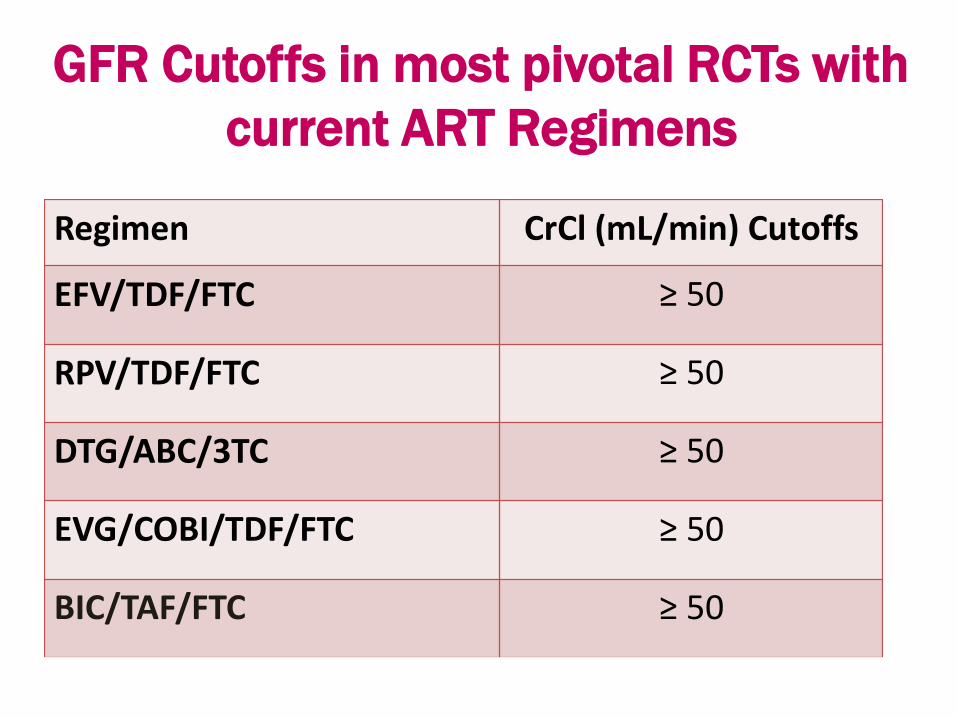
Regimen CrCl (mL/min) Cutoffs
EFV/TDF/FTC ≥ 50
RPV/TDF/FTC ≥ 50
DTG/ABC/3TC ≥ 50
EVG/COBI/TDF/FTC ≥ 50
BIC/TAF/FTC ≥ 50
GFR Cutoffs in most pivotal RCTs with
current ART Regimens

¿Es seguro el TAR en pacientes
con filtrado glomerular
<50ml/min?

¿Es seguro el TAR en pacientes
con filtrado glomerular
<50ml/min?
¿ensayos clínicos?
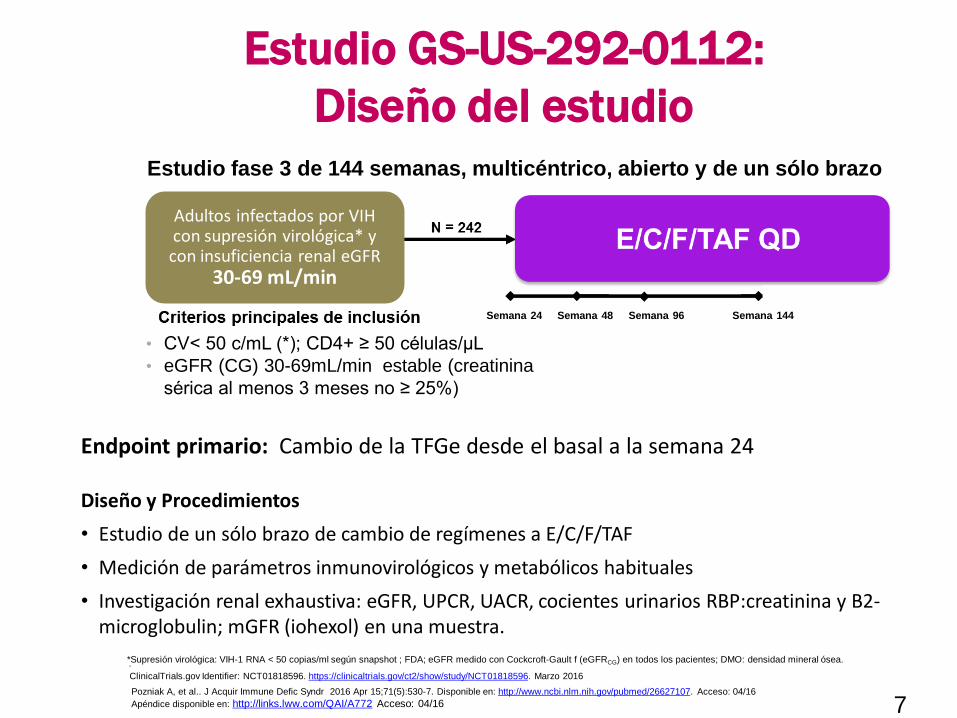
Estudio GS-US-292-0112:
Diseño del estudio
Estudio fase 3 de 144 semanas, multicéntrico, abierto y de un sólo brazo
ClinicalTrials.gov Identifier: NCT01818596. https://clinicaltrials.gov/ct2/show/study/NCT01818596. Marzo 2016
.
7
Adultos infectados por VIH con supresión virológica* y con insuficiencia renal eGFR
30-69 mL/min
Pozniak A, et al.. J Acquir Immune Defic Syndr 2016 Apr 15;71(5):530-7. Disponible en: http://www.ncbi.nlm.nih.gov/pubmed/26627107. Acceso: 04/16
Apéndice disponible en: http://links.lww.com/QAI/A772 Acceso: 04/16
Semana 24 Semana 48 Semana 96 Semana 144
Endpoint primario: Cambio de la TFGe desde el basal a la semana 24
*Supresión virológica: VIH-1 RNA < 50 copias/ml según snapshot ; FDA; eGFR medido con Cockcroft-Gault f (eGFRCG) en todos los pacientes; DMO: densidad mineral ósea.
Diseño y Procedimientos
• Estudio de un sólo brazo de cambio de regímenes a E/C/F/TAF
• Medición de parámetros inmunovirológicos y metabólicos habituales
• Investigación renal exhaustiva: eGFR, UPCR, UACR, cocientes urinarios RBP:creatinina y B2-microglobulin; mGFR (iohexol) en una muestra.
• CV< 50 c/mL (*); CD4+ ≥ 50 células/µL
• eGFR (CG) 30-69mL/min estable (creatinina
sérica al menos 3 meses no ≥ 25%)

Estudio GS-US-292-0112: Características
basales (*)
7%5%Otros
Ninguno
ITINN
42%
8
ABC
22%
TDF
65%
eGFR<50mL/minn=80
eGFR ≥50 mL/minn=162
Mediana edad (rango) 59 (31-82) 58 (24-76)
Edad≥ 65 años, n (%) 25 (31) 38 (23)
Mujeres, n (%) 21(26) 29(18)
Negra o descendencia africana, % 18 19
VIH-1 RNA <50 copias/ml, % 98 98
Mediana recuento CD4, cells/µL 622 635
Pre cambio TDF, % 58 69
Hipertensión, % 50 34
Diabetes, % 15 13
Mediana eGFRCG medio mL/min 43 60
Mediana eGFRCKD – EPI, SCR medio ml/min/1,73 m2* 45 58
Mediana eGFRCKD – EPI, cysC medio ml/min/1,73 m2† 57 77
Proteinuria por tira reactiva, grado 1 o 2%‡ 44 27
Proteinuria significativa (UPCR> 200 mg/g), %§ 56 35
Albuminuria Significativa (UACR ≥ 30 mg/g), %¶ 64 42
(*) N= 242: median age 58 years (range = 24–82 years), including 63 patients >65 year; 21% of
patients were female; median GFRcg 56; 42% of patients had significant proteinuria (UPCR>200
mg/g), 49% had significant albuminuria (UACR>30 mg/g), 39% had hypertension, and 14% were
diabetic.
CG, Cockroft-Gault.
* Ecuación CKD EPI usando la creatinina sérica (FGe CKD-EPI, creatinina).
†Ecuación CKD-EPI con cistatina C (FGe CKD-EPI, cistatina C).
‡Grado 1 (1+ por tira reactiva), grado 2 (2–3+ por tira reactiva); ninguno tiene grado 3 or 4.
¶ Microalbuminuria ≥ 30 mg/g.
UPCR: cociente creatinina proteína en orinaUACR: cociente creatinina albumina en orina
ITIANs
*Algunas terapias incluían >1 tercer agente;
por lo tanto, el total >100%.
ITINN
42%
INSTI
24%
3%
Antagonista CCR5
IP 44%
Tercer agente*
Pozniak A, et al.. J Acquir Immune Defic Syndr 2016 Apr 15;71(5):530-7. Disponible en: http://www.ncbi.nlm.nih.gov/pubmed/26627107.
Acceso: 04/16 Apéndice disponible en: http://links.lww.com/QAI/A772 Acceso: 04/16
0 4 8 1 2 1 6 2 0 2 4 2 8 3 2 3 6 4 0 4 4 4 8
-1 5
-1 0
-5
0
5
1 0
1 5
W e e k s
Me
dia
n (
Q1
,Q3
) e
GF
R C
ha
ng
e
Fr
om
Ba
se
lin
e (
mL
/min
/1.7
3 m
2)
1.81.1
0 4 8 1 2 1 6 2 0 2 4 2 8 3 2 3 6 4 0 4 4 4 8
-1 5
-1 0
-5
0
5
1 0
1 5
W e e k s
Me
dia
n (
Q1
,Q3
) e
GF
R C
ha
ng
e
Fro
m B
as
eli
ne
(m
L/m
in)
0.6
-1.4
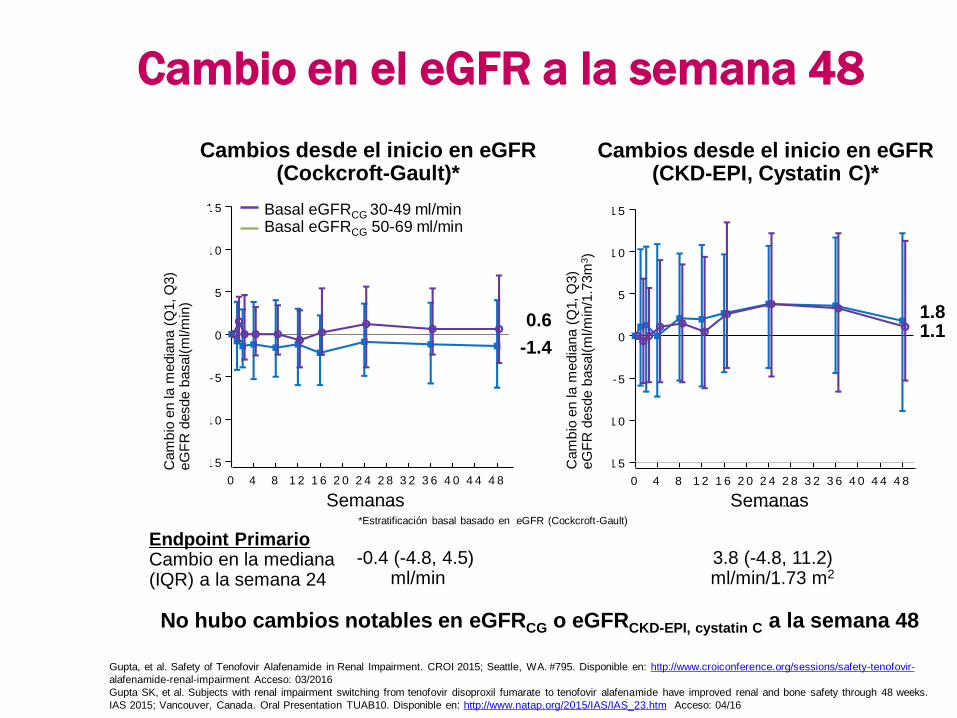
Basal eGFRCG 30-49 ml/minBasal eGFRCG 50-69 ml/min
Cambios desde el inicio en eGFR (Cockcroft-Gault)*
Cambios desde el inicio en eGFR (CKD-EPI, Cystatin C)*
No hubo cambios notables en eGFRCG o eGFRCKD-EPI, cystatin C a la semana 48
3.8 (-4.8, 11.2)ml/min/1.73 m2
Endpoint PrimarioCambio en la mediana (IQR) a la semana 24
Cambio en el eGFR a la semana 48
-0.4 (-4.8, 4.5) ml/min
*Estratificación basal basado en eGFR (Cockcroft-Gault)
Gupta, et al. Safety of Tenofovir Alafenamide in Renal Impairment. CROI 2015; Seattle, WA. #795. Disponible en: http://www.croiconference.org/sessions/safety-tenofovir-
alafenamide-renal-impairment Acceso: 03/2016
Gupta SK, et al. Subjects with renal impairment switching from tenofovir disoproxil fumarate to tenofovir alafenamide have improved renal and bone safety through 48 weeks.
IAS 2015; Vancouver, Canada. Oral Presentation TUAB10. Disponible en: http://www.natap.org/2015/IAS/IAS_23.htm Acceso: 04/16
Cam
bio
en la m
edia
na
(Q1, Q
3)
eG
FR
desde
basal(
ml/m
in)
Cam
bio
en la m
edia
na
(Q1, Q
3)
eG
FR
desde
basal(
ml/m
in/1
.73m
3)
Semanas Semanas

Cambios de la proteinuria desde el inicio hasta la
semana 48 en los pacientes que cambiaron a
E/C/F/TAF
1
0
* Todos los ambios de Total y TDF son estadísticamente significativos; † todos los cambios non-TDF son estadísticamente no significativos
Mejorías significativas en la proteinuria, la albuminuria y la proteinuria tubular desde el inicio hasta la semana 48
Proteínas tubulares
Pozniak A, et al. Switching to Tenofovir Alafenamide, Coformulated With Elvitegravir, Cobicistat, and Emtricitabine, in HIV-Infected Patients With Renal Impairment: 48-Week
Results From a Single-Arm, Multicenter, Open-Label Phase 3 Study. J Acquir Immune Defic Syndr 2016 Apr 15;71(5):530-7. Disponible en:
http://www.ncbi.nlm.nih.gov/pubmed/26627107. Acceso: 04/16
Apéndice disponible en: http://links.lww.com/QAI/A772 Acceso: 04/16
Med
ian
a (
mg
/g)
Med
ian
a (
µg
/g)
UPCR: tasa de creatinina proteína en orina; UACR: tasa de creatinina albumina en orina; RBP:Cr: proteína de unión a retinol; β-2-m: Cr: beta-2 microglobulina
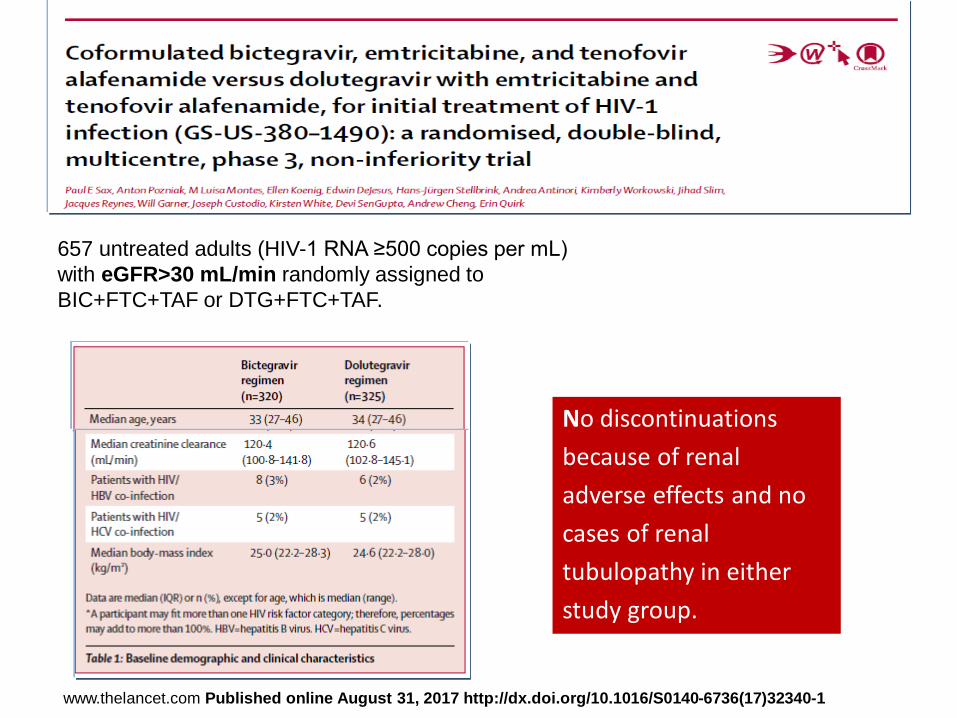
No discontinuations
because of renal
adverse effects and no
cases of renal
tubulopathy in either
study group.
657 untreated adults (HIV-1 RNA ≥500 copies per mL)
with eGFR>30 mL/min randomly assigned to
BIC+FTC+TAF or DTG+FTC+TAF.
www.thelancet.com Published online August 31, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32340-1

¿Es seguro el TAR en pacientes
con filtrado glomerular
<50ml/min?
¿?

¿Cómo emplear el TAR con
seguridad en pacientes con
filtrado glomerular <50ml/min?
• Avoid nephrotoxic agents.
• Make dose adjustment as needed according to package inserts• Avoid using co-formulations of ARV in patients with low
GFR
• In patients undergoing dyalisis: consider both drug adjustment and time of administration regarding the dialysis session.
• Do take into account potential drug-drug interactions (more
common and dangereous in this scenario).
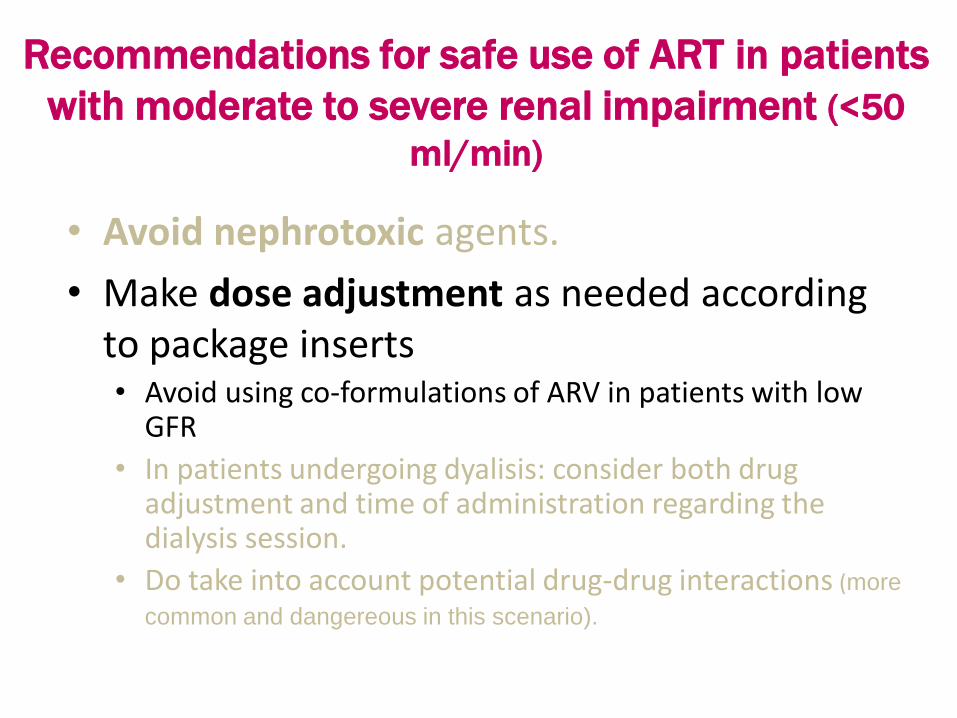
Recommendations for safe use of ART in patients
with moderate to severe renal impairment (<50
ml/min)
• Avoid nephrotoxic agents.
• Make dose adjustment as needed accordingto package inserts• Avoid using co-formulations of ARV in patients with low
GFR
• In patients undergoing dyalisis: consider both drugadjustment and time of administration regarding the dialysis session.
• Do take into account potential drug-drug interactions (more
common and dangereous in this scenario).
Recommendations for safe use of ART in patients
with moderate to severe renal impairment (<50
ml/min)
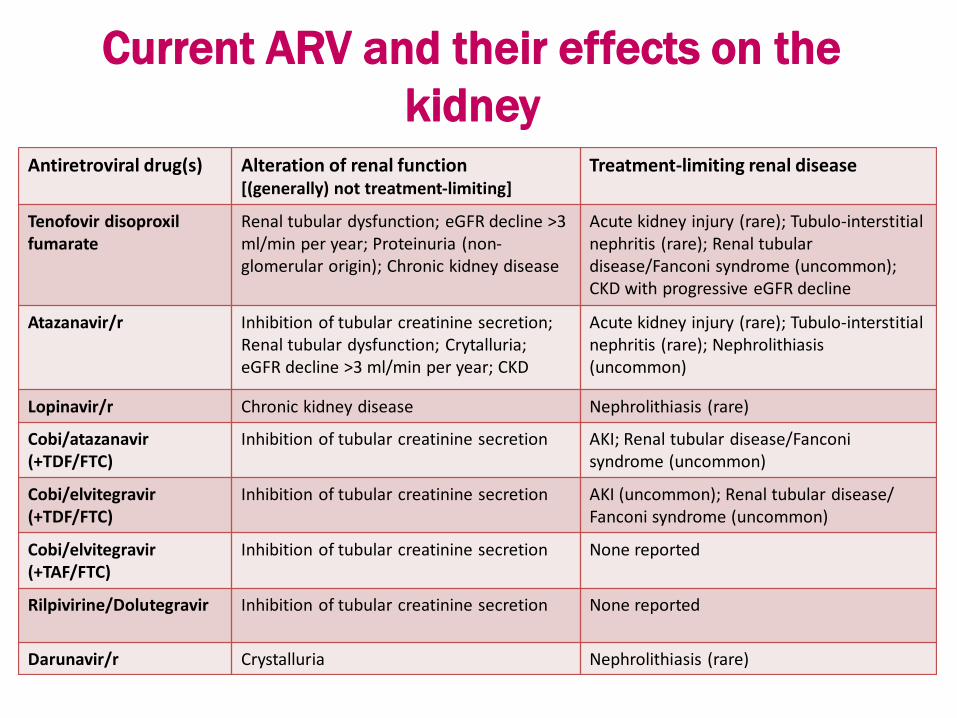
Current ARV and their effects on the
kidneyAntiretroviral drug(s) Alteration of renal function
[(generally) not treatment-limiting]Treatment-limiting renal disease
Tenofovir disoproxilfumarate
Renal tubular dysfunction; eGFR decline >3 ml/min per year; Proteinuria (non-glomerular origin); Chronic kidney disease
Acute kidney injury (rare); Tubulo-interstitial nephritis (rare); Renal tubular disease/Fanconi syndrome (uncommon); CKD with progressive eGFR decline
Atazanavir/r Inhibition of tubular creatinine secretion; Renal tubular dysfunction; Crytalluria; eGFR decline >3 ml/min per year; CKD
Acute kidney injury (rare); Tubulo-interstitial nephritis (rare); Nephrolithiasis (uncommon)
Lopinavir/r Chronic kidney disease Nephrolithiasis (rare)
Cobi/atazanavir(+TDF/FTC)
Inhibition of tubular creatinine secretion AKI; Renal tubular disease/Fanconisyndrome (uncommon)
Cobi/elvitegravir(+TDF/FTC)
Inhibition of tubular creatinine secretion AKI (uncommon); Renal tubular disease/Fanconi syndrome (uncommon)
Cobi/elvitegravir(+TAF/FTC)
Inhibition of tubular creatinine secretion None reported
Rilpivirine/Dolutegravir Inhibition of tubular creatinine secretion None reported
Darunavir/r Crystalluria Nephrolithiasis (rare)

Current ARV and their effects on the
kidneyAntiretroviral drug(s) Alteration of renal function
[(generally) not treatment-limiting]Treatment-limiting renal disease
Tenofovir disoproxilfumarate
Renal tubular dysfunction; eGFR decline >3 ml/min per year; Proteinuria (non-glomerular origin); Chronic kidney disease
Acute kidney injury (rare); Tubulo-interstitial nephritis (rare); Renal tubular disease/Fanconi syndrome (uncommon); CKD with progressive eGFR decline
Atazanavir/r Inhibition of tubular creatinine secretion; Renal tubular dysfunction; Crytalluria; eGFR decline >3 ml/min per year; CKD
Acute kidney injury (rare); Tubulo-interstitial nephritis (rare); Nephrolithiasis (uncommon)
Lopinavir/r Chronic kidney disease Nephrolithiasis (rare)
Cobi/atazanavir(+TDF/FTC)
Inhibition of tubular creatinine secretion AKI; Renal tubular disease/Fanconisyndrome (uncommon)
Cobi/elvitegravir(+TDF/FTC)
Inhibition of tubular creatinine secretion AKI (uncommon); Renal tubular disease/Fanconi syndrome (uncommon)
Cobi/elvitegravir(+TAF/FTC)
Inhibition of tubular creatinine secretion None reported
Rilpivirine/Dolutegravir Inhibition of tubular creatinine secretion None reported
Darunavir/r Crystalluria Nephrolithiasis (rare)

Tenofovir alafenamida (TAF)
Diferencias PK entre TAF y TDF
1.-TAF más estable en plasma que TDF2.-Mayores (x4) concentraciones intracelulares del metabolito activo de TFV (TFV difosfato), lo que permite emplear dosis más bajas 3.- Debido a 1 y 2, la exposición plasmática a TFV es 90% menor, lo que reduce el riesgo de toxicidad renal y ósea.4.- En los ensayos de fase 2 y 3 de TAF+FTC (coadministrado con EVG-c/BIC/DTG/DRV-c/RPV) ha mostrado un “perfil renal” más favorable que TDF y comparable a ABC.
† T1/2 basado en estudios in vitro.

11 randomised head-to-head trials (8111 patients) of TDF versus TAF.
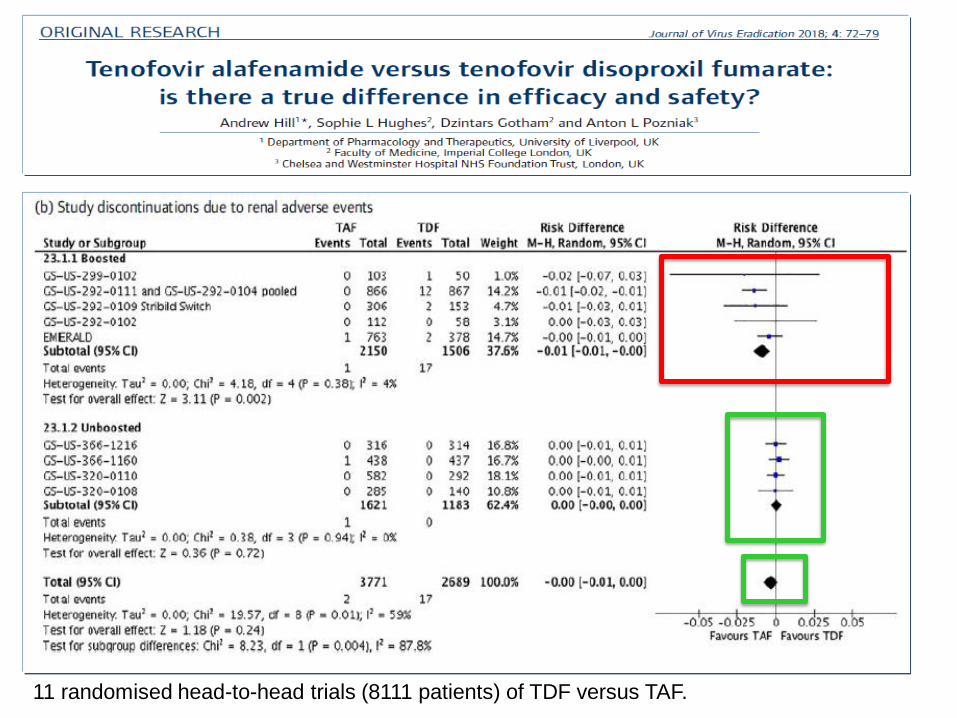
11 randomised head-to-head trials (8111 patients) of TDF versus TAF.
• Avoid nephrotoxic agents.
• Make dose adjustment as needed accordingto package inserts• Avoid using co-formulations of ARV in patients with low
GFR
• In patients undergoing dyalisis: consider both drugadjustment and time of administration regarding the dialysis session.
• Do take into account potential drug-drug interactions (more
common and dangereous in this scenario).
Recommendations for safe use of ART in patients
with moderate to severe renal impairment (<50
ml/min)
• NRTIs
– Require dose adjustment except abacavir
– Eliminated by renal route: should be given
after dyalisis
• Not required for NNRTIs, PIs, InSTI
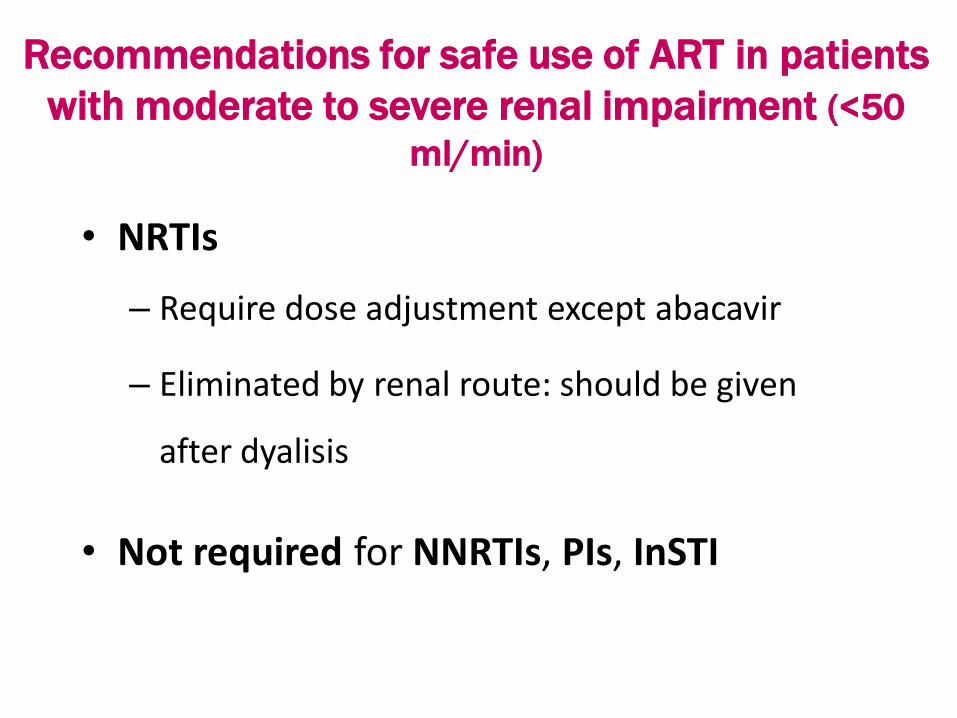
Recommendations for safe use of ART in patients
with moderate to severe renal impairment (<50
ml/min)
• NRTIs
– Require dose adjustment except abacavir
– Eliminated by renal route: should be given
after dyalisis
• Not required for NNRTIs, PIs, raltegravirnor DTG
Recommendations for safe use of ART in patients
with moderate to severe renal impairment (<50
ml/min)

Generic
nameDosage form CrCl 50-30 ml/min CrCl 29-10 ml/min CrCl <10 ml/min
Abacavir
(ABC)
ABC 300 mg
tabletStandard dose
KIVEXA Not recommended
Emtricitabine
(FTC)
FTC 200 mg200 mg every 48
hours
200 mg every 72
hours
200 mg every 96
hours; administer after
dialysis
TRUVADA Not recommended
FTC 200 mg +
TAF 25 mgStandard dose Not recommended
Lamivudine
(3TC)
3TC, 100, 150,
300 mg tablet, 5
mg/ml solution
150 mg daily150 mg stat then 100
mg/d
150 mg stat then 50
mg/d
KIVEXA Not recommended
Tenofovir
Disoproxil
Fumarate
(TDF)
TDF 300 mg
tablet300 mg every 48
hours300 mg 2 days/week 300 mg every 7 days
TRUVADA Not recommended
Tenofovir
Alafenamide
(TAF)
TAF 10 or 25
mg + FTC 200
mg
Standard dose Not recommended
Antiretroviral dose adjustments of NRTIs in
chronic kidney disease according to CrCl

¿Es seguro el TAR en pacientes
con filtrado glomerular
<30ml/min?
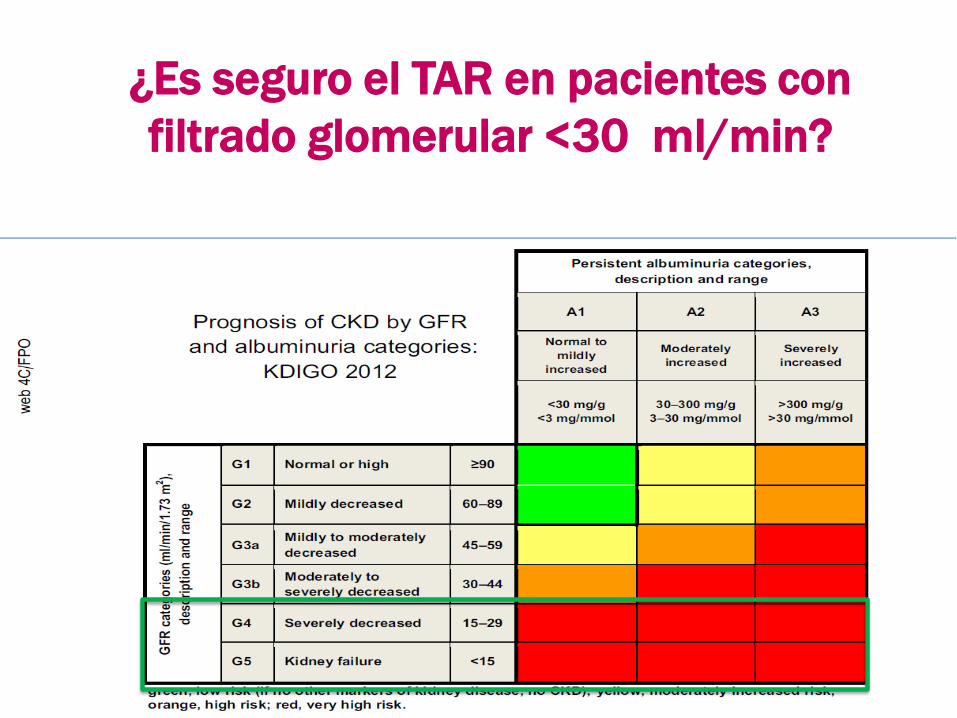
¿Es seguro el TAR en pacientes con
filtrado glomerular <30 ml/min?
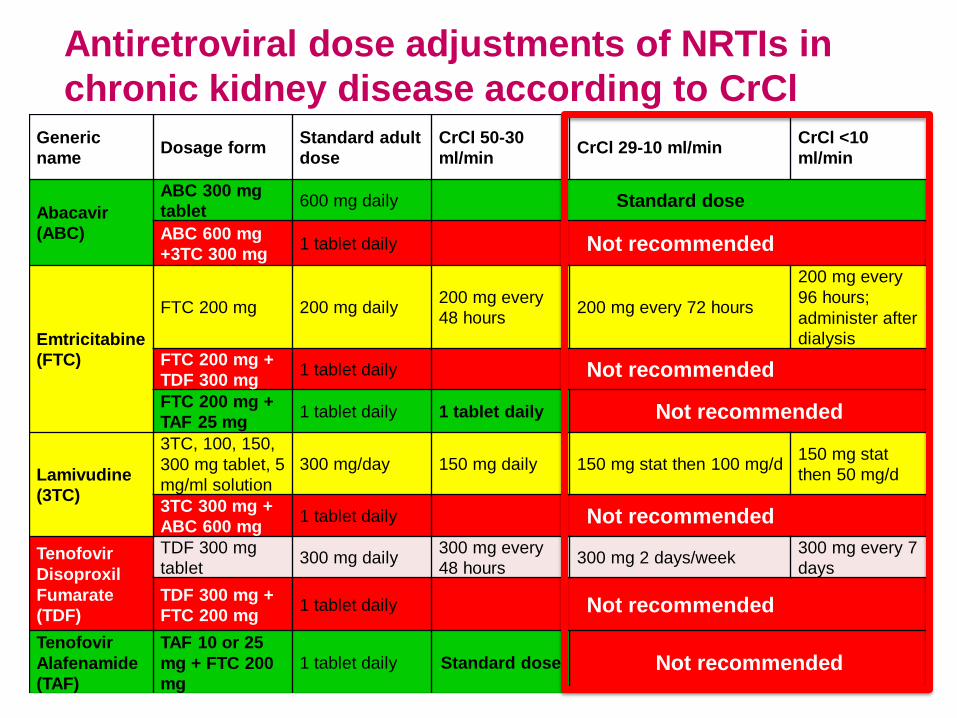
Generic
nameDosage form
Standard adult
dose
CrCl 50-30
ml/minCrCl 29-10 ml/min
CrCl <10
ml/min
Abacavir
(ABC)
ABC 300 mg
tablet600 mg daily Standard dose
ABC 600 mg
+3TC 300 mg1 tablet daily Not recommended
Emtricitabine
(FTC)
FTC 200 mg 200 mg daily200 mg every
48 hours200 mg every 72 hours
200 mg every
96 hours;
administer after
dialysis
FTC 200 mg +
TDF 300 mg1 tablet daily Not recommended
FTC 200 mg +
TAF 25 mg1 tablet daily 1 tablet daily Not recommended
Lamivudine
(3TC)
3TC, 100, 150,
300 mg tablet, 5
mg/ml solution
300 mg/day 150 mg daily 150 mg stat then 100 mg/d150 mg stat
then 50 mg/d
3TC 300 mg +
ABC 600 mg1 tablet daily Not recommended
Tenofovir
Disoproxil
Fumarate
(TDF)
TDF 300 mg
tablet300 mg daily
300 mg every
48 hours300 mg 2 days/week
300 mg every 7
days
TDF 300 mg +
FTC 200 mg1 tablet daily Not recommended
Tenofovir
Alafenamide
(TAF)
TAF 10 or 25
mg + FTC 200
mg
1 tablet daily Standard dose Not recommended
Antiretroviral dose adjustments of NRTIs in
chronic kidney disease according to CrCl
¿TAF en pacientes con filtrado
glomerular <30ml/min?
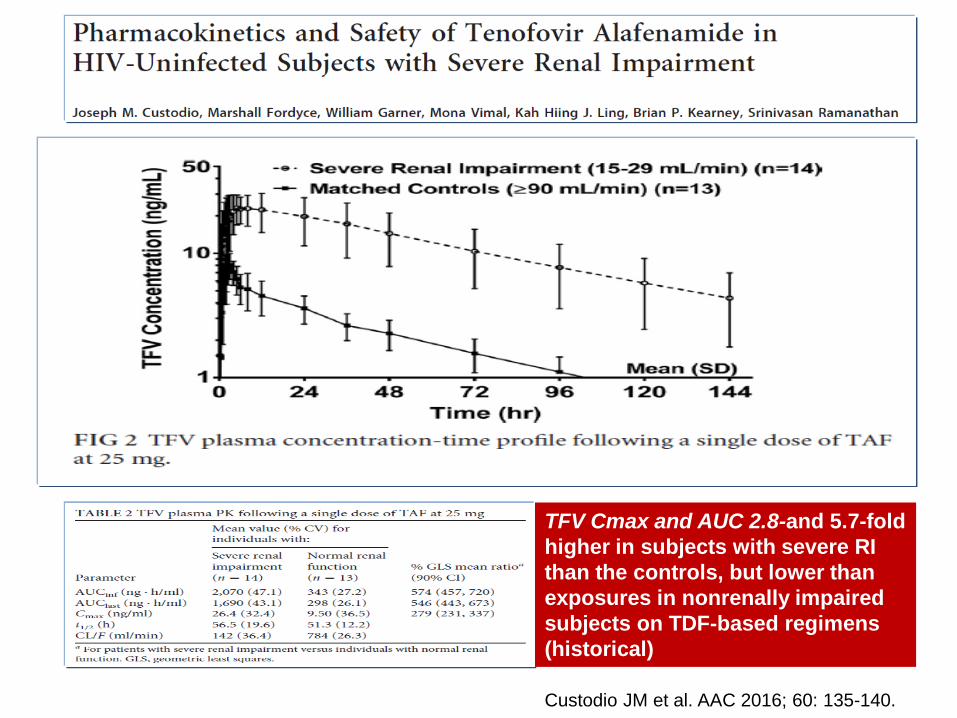
TFV Cmax and AUC 2.8-and 5.7-fold
higher in subjects with severe RI
than the controls, but lower than
exposures in nonrenally impaired
subjects on TDF-based regimens
(historical)
Custodio JM et al. AAC 2016; 60: 135-140.

Entonces, ¿qué pautas de TAR
podemos utilizar con “seguridad”
en pacientes con insuficiencia
renal moderada-severa ?
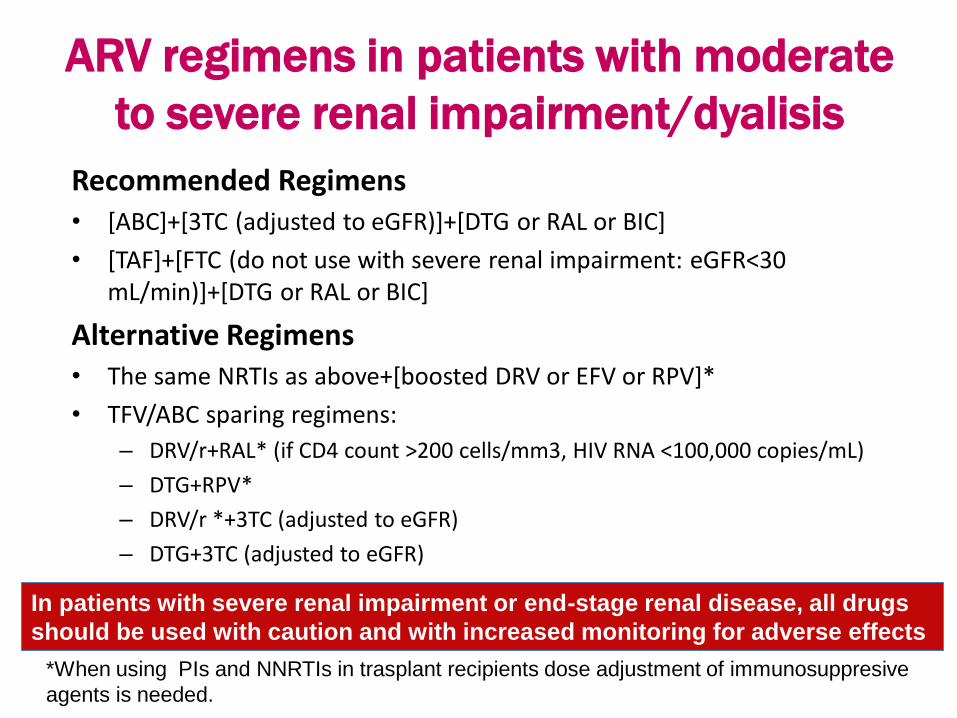
ARV regimens in patients with moderate
to severe renal impairment/dyalisis
Recommended Regimens• [ABC]+[3TC (adjusted to eGFR)]+[DTG or RAL or BIC]
• [TAF]+[FTC (do not use with severe renal impairment: eGFR<30 mL/min)]+[DTG or RAL or BIC]
Alternative Regimens• The same NRTIs as above+[boosted DRV or EFV or RPV]*
• TFV/ABC sparing regimens:
– DRV/r+RAL* (if CD4 count >200 cells/mm3, HIV RNA <100,000 copies/mL)
– DTG+RPV*
– DRV/r *+3TC (adjusted to eGFR)
– DTG+3TC (adjusted to eGFR)
*When using PIs and NNRTIs in trasplant recipients dose adjustment of immunosuppresive
agents is needed.
In patients with severe renal impairment or end-stage renal disease, all drugs
should be used with caution and with increased monitoring for adverse effects
Muchas gracias!!!