FARMACOVIGILANCIA Experiencia Hospital Base Valdivia. Farmacovigilancia Hospital... · 2011, mayo...
40
Taller :“La Farmacovigilancia en el Nuevo Marco Normativo y los Desafíos Futuros”. Instituto de Salud Pública. Santiago, mayo de 2012. FARMACOVIGILANCIA Experiencia Hospital Base Valdivia Ximena Lagos Morales Químico Farmacéutico – Académico Instituto de Farmacia Facultad de Ciencias. Universidad Austral de Chile [email protected]
Transcript of FARMACOVIGILANCIA Experiencia Hospital Base Valdivia. Farmacovigilancia Hospital... · 2011, mayo...

Taller :“La Farmacovigilancia en el Nuevo Marco Normativo y los Desafíos Futuros”. Instituto de Salud Pública. Santiago, mayo de 2012.
FARMACOVIGILANCIA Experiencia Hospital Base
Valdivia
Ximena Lagos Morales
Químico Farmacéutico – Académico Instituto de Farmacia
Facultad de Ciencias. Universidad Austral de Chile
¿Cómo implementamos la
Farmacovigilancia?
1999 2000

Manual de procedimiento FV
SUBDEPARTAMENTO DE FARMACIA – HOSPITAL BASE
VALDIVIA
MANUAL DE PROCEDIMIENTOS UNIDAD DE FARMACIA DE
HOSPITALIZADOS
EDICION: PRIMERA
FECHA: ENE 2009
Página 51 de 80
VIGENCIA: ENE
2014
PROCEDIMIENTO DE FARMACOVIGILANCIA HOSPITALARIA
Elaborado por:
Q.F. Lily Acuña G.
Q.F. Mónica Kyonen L.
FARMACIA DE
HOSPITALIZADOS
Revisado por:
Q.F. Gloria Muñoz
SUBDEPARTAMENTO DE
FARMACIA
Aprobado por:
Dra. Maritza Navarrete
SUBDIRECCION MEDICA
APOYO CLINICO Y
TERAPEUTICO
Fecha: 15 Septiembre 2011 Fecha: 15 Septiembre 2011 Fecha: 15 Septiembre 2011

Paciente con sospecha de RAM
Profesional comunica sospecha a Subdepto.
de Farmacia
Profesional Q.F. notifica sospecha al Centro
Nacional de Farmacovigilancia Q.F. registra RAM
en ficha clínica
Q.F. retroalimenta a profesional notificador
Registro en base de datos y archivo

Actividades de difusión

Disponible en: http://www.redsaf.org/docs/redsaf_boletin_vol01_03b.pdf

Programa de detección de Sospechas de Reacciones Adversas a Medicamentos en pacientes hospitalizados del Hospital Clínico Regional Valdivia: Experiencia
de 6 meses, año 2005.
Costos directos implicados: $ 2.728.015
Actividades de difusión

En prensa: Descripción de las Reacciones Adversas a L-Asparaginasa en Niños en Tratamiento por Leucemia Linfoblástica Aguda, Hospital Base
Valdivia (2000 – 2007)
Descripción de las Reacciones Adversas a L-Asparaginasa en Niños en Tratamiento por Leucemia Linfoblástica
Aguda, Hospital Base Valdivia (2000 – 2007)
Oyedo S., Folatre I.,Kyonen M., Martinez P., Yilorm M., Cea G.
Resultados: Se evaluaron las fichas clínicas de 79 niños entre 1 y 14 años de edad, para 109 sospechas de RAM, calificándose como: definitivas 24 y 33 probables. En estos pacientes, la incidencia de RAM fue 60%. El 35,4% presentó reacciones inmunológicas, con síntomas, desde eritema (55%) a anafilaxia (15,2%) que se detectaron entre la 7a y 12a dosis de ASP (25/33). El 27,5% presentó RAM hemostática, entre ellas disminución de la concentración plasmática de fibrinógeno (95,2%) que fue estadísticamente significativas (p<0,001) Se encontró alteración transitoria de las pruebas de función hepática (2,5%) y gastrointestinal (1,3%) Durante esta década se constató aumento de la frecuencia de RAM mayor a 50%.
En prensa: Evaluación y caracterización de la hiperglicemia en niños portadores de Leucemia Linfoblástica Aguda en tratamiento con
L-asparaginasa Hospital Base Valdivia (2002-2009)
Describir las características de la hiperglicemia asociada al uso de L-asp en niños en tratamiento por LLA.
La incidencia de episodios de hiperglicemia secundarios al tratamiento con L-asp, en niños con LLA, fue de 6.74 %. Las características del sujeto con hiperglicemia fueron:
edad ≥ 9.5 años
con riesgo de obesidad
con antecedentes familiares de DM
con una glicemia promedio de 160 ± 225 mg/dL
con aparición de la RAM durante la etapa de inducción
con administración concomitante de corticoides
Palma P., Kyonen M., Folatre I., Lagos X.

Desarrollo de una Guía Informativa para el funcionamiento de un Sistema de
Farmacovigilancia en la Región de los Ríos.
En Farmacovigilancia, utilicemos el SISTEMA LUPA, para detectar una posible RAM:
L: LEVANTAR LA CABEZA
U: UNIR LOS ESFUERZOS
P: PONER EL OJO
A: ABRIR LAS OREJAS
Figueras A. Reflexiones en
Farmacovigilancia. Sta. Cruz de la Sierra, 19-07-2000

Base de datos
NUMERO RAM SERVICIO
CLINICO
MEDICAMENTO GRUPO
FARMACOLOGICO
(WHO-ART)
ATC CARACTERISTICA
DE LA RAM
PROFESIONAL
NOTIFICADOR
Sencilla Datos para Promoción de la FV
Indicadores
Porcentaje de casos de sospecha de RAM captados por FV pasiva = nº RAM / total egresos hospitalarios
*100
Porcentaje de RAM, por servicio clínico = nº RAM / egresos
hospitalarios según Subdepto. Pediatría y Medicina Adultos.

Número de reportes desde inicios del programa de FV
0
20
40
60
80
100
120
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
N°
rep
ort
es
64
90
46
60
31 44
102 108
52
107
80 64
48

METODOLOGÍA
Estudio de intervención no controlado, consistente en la monitorización prospectiva de la farmacoterapia de pacientes hospitalizados en el Servicio de Medicina Interna del HBV, trabajando en la optimización de la misma, prevención y detección de Problemas Relacionados con Medicamentos (PRM), realización de intervenciones farmacoterapéuticas y posterior registro y evaluación de las mismas a través del SDU.
Participación en visita médica diaria
Seguimiento clínico y farmacoterapéutico
Prevención y detección de PRM
Actuación farmacéutica
Comunicación al profesional involucrado
Documentación y evaluación de las IF
ETAPAS PARA LA MONITORIZACIÓN DE PACIENTES



2011, mayo 26 y 27. I Jornadas de Farmacéuticos Clínicos Asistenciales Hospital Guillermo Grant Benavente. Kyonen López, M.; Lagos Morales, X.; Folatre Briones, I.; Vidal Fernández, D.; Gutiérrez Saldivia, C. PROMOCIÓN DE LAS ACTIVIDADES DE FARMACOVIGILANCIA EN EL ÁREA ASISTENCIAL, EXPERIENCIA EN EL HOSPITAL BASE VALDIVIA. Concepción, Chile.

Kyonen López , M 1a, Lagos Morales, X 2a, , Folatre Briones, I 3b, Vidal Fernández, D 4c , Gutiérrez Saldivia, C 4c
1Subdepartamento de Farmacia, Hospital Base Valdivia.
2Instituto de Farmacia, Facultad de Ciencias. Universidad Austral de Chile. 3Subdepartamento de Pediatría, Hospital Base Valdivia.
4Escuela de Química y Farmacia. Universidad Austral de Chile. a Químico Farmacéutico
b Pediatra C Interna de Química y Farmacia. Universidad Austral de Chile.
1999-2010 N= 850 reportes
1,3 notificaciones de RAM/100.000 atenciones
del HBV anualmente

Casos de los que hemos aprendido…


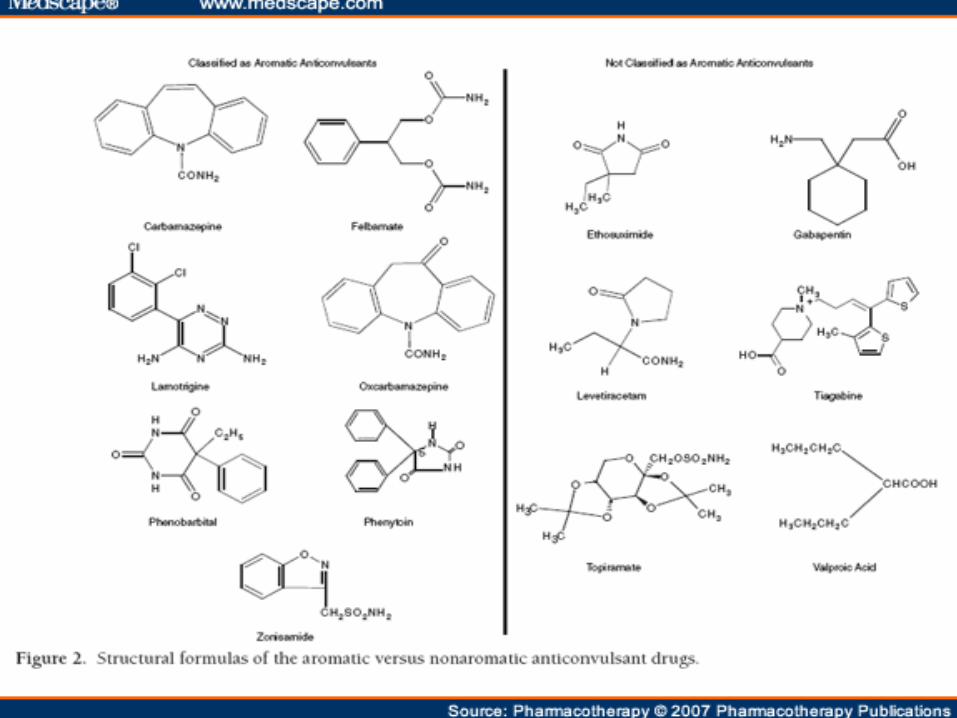
Paciente de 33 años, sexo masculino, manifiesta eritema polimorfo generalizado luego de la exposición a fenitoína 300 mg/día VO, para tratar síndrome convulsivo. La reacción se evidencia en concomitancia con cuadro febril y alteraciones en pruebas hepáticas. El paciente no presentaba tratamiento concomitante con otros medicamentos. Tiene antecedente de tratamiento con fenitoína desde hace 3 semanas. La sospecha de RAM, es notificada desde el HRV por médico tratante y enviada al CENIMEF. Se solicita interconsulta a Neurólogo, quien indica cambio a fenobarbital.
Caso clínico
Anticonvulsant Hypersensitivity Syndrome: Implications for Pharmaceutical Care KarenBeth H Bohan, Tarannum F Mansuri, Natalie M Wilson
Pharmacotherapy. 2007;27(10):1425-1439.


Dasatinib
Thrombocytopenia, Grade 3 or 4 1) Incidence: 22% to 81% (Prod Info SPRYCEL(R)
oral tablets, 2007).
2) Grade 3 or 4 thrombocytopenia occurred in 41%, 71%, 81%, and 78% of patients receiving dasatinib for chronic phase chronic myeloid leukemia (CML) (n=1150), accelerated phase CML (n=502), myeloid blast phase CML (n=280), and lymphoid blast phase CML and Philadelphia chromosome positive (Ph+) acute lymphoblastic leukemia (n=250), respectively (Prod Info SPRYCEL(R) oral tablets, 2007).

Dasatinib
• Pleural effusion
1) Incidence: all grades, 16% to 23%; grade 3 or 4, 2% to 10% (Prod Info SPRYCEL(R) oral tablets, 2007)
2) Pleural effusion (all grades) occurred in 22% of patients with leukemia across all dasatinib studies (n=2182), with grade 3 or 4 occurring in 5% of these patients. Grade 3 or 4 pleural effusion occurred in 4%, 5%, 10%, and 6% of patients with chronic phase chronic myeloid leukemia (CML) (n=1150), accelerated phase CML (n=502), myeloid blast phase CML (n=280), and lymphoid blast phase CML or Philadelphia chromosome positive (Ph+) acute lymphoblastic leukemia (n=250), respectively. Pleural effusion was one of the most frequently-reported serious adverse effects (Prod Info SPRYCEL(R) oral tablets, 2007).


Imipenem
• Seizure
1) Seizures have occurred during imipenem/cilastatin therapy (Lane et al, 1996; Calandra et al, 1985a; Solomkin et al, 1985b; Brotherton & Kelber, 1984a). The incidence of seizures appears to be about 1% to 1.5% (Calandra et al, 1985a). However, the manufacturer indicates an incidence of 0.4% (Prod Info PRIMAXIN(R) IM injection, 2006). Risk factors associated with seizures in patients being treated with imipenem/cilastin include preexisting central nervous system lesions or disorders, renal dysfunction, exceeding the recommended dose, and Pseudomonas aeruginosa infection. The average time to onset of seizures is seven days (Calandra et al, 1988). Imipenem/cilastatin should be used cautiously in patients with impaired renal function; adjusting the dose may not be adequate to prevent seizures (Leo & Ballow, 1991a; Tse et al, 1987); (Fitzsimmons et al, 1987)(Drusano, 1986; Park & Parker, 1986).


L- asparaginasa
• Anaphylaxis 1) Anaphylaxis may occur in the absence of a positive skin test, or during continued maintenance therapy (Prod Info ELSPAR(R) injection, 2006; DeVita et al, 1989). Rash 1) Skin rash has been reported with asparaginase use and may occur in the absence of a positive skin test, or during continued maintenance therapy (Prod Info ELSPAR(R) injection, 2006). Urticaria 1) Urticaria has been reported with asparaginase use and may occur in the absence of a positive skin test, or during continued maintenance therapy (Oettgen et al, 1970; Jaffe et al, 1971; Prod Info ELSPAR(R) injection, 2006).
• Immune hypersensitivity reaction 1) Patients who have received asparaginase as part of a previous treatment regimen have a greater risk of hypersensitivity reactions when the agent is reintroduced at a later time. Desensitization should be instituted prior to administration of full doses to all patients who are found hypersensitive by skin testing or any patient who has received a previous course of the drug (Prod Info Elspar(R), 1999a). 2) Intermittent analysis of antibodies in patients receiving asparaginase may be useful in predicting hypersensitivity. In a clinical study of 35 children receiving asparaginase to treat acute lymphoblastic leukemia, anti-asparaginase antibody levels were higher at all comparable time points in patients with hypersensitivity reactions (n=22) than in control patients (n=13) receiving an identical treatment regimen. Initial reactions occurred after a median of 11.5 doses of E. coli asparaginase, and half of the reacting patients were switched to Erwinia asparaginase. Reactions occurring after Erwinia asparaginase developed after a median of 4 doses. In reacting patients, the median anti-asparaginase antibody levels increased from 0.039 (optical density, 1 to 3200 dilution ratio) at baseline to 0.506 after hypersensitivity reactions (p=0.0002). In non-reacting control patients, these levels increased from 0.011 to 0.032 after 25 doses of asparaginase (p=0.02). After induction, 59% of reacting patients had anti-asparaginase antibody levels that were three times greater than background levels in blood samples from human volunteers, and 91% exhibited these increases after reinduction. Post-induction antibody levels among non-reacting patients did not differ significantly from those of normal control volunteers (Woo et al, 1998). 3) The incidence and clinical characteristics of anaphylactoid reactions to intravenous asparaginase were assessed in 196 patients given E coli asparaginase and 49 patients given Erwinia asparaginase. Twenty-nine of 196 patients (14.8%) given E coli asparaginase had an anaphylactoid reaction, occurring after their first through twelfth doses. The risk of an anaphylactoid reaction to E coli asparaginase was significantly greater in patients who were not receiving concomitant prednisone-vincristine therapy and patients who had a hiatus of at least 1 month between courses. Seven of 49 patients (14%) treated with Erwinia asparaginase had an anaphylactoid reaction; all had been treated with E coli asparaginase earlier (Evans et al, 1982).


Aspirina
• Bronchospasm
1) Aspirin can exacerbate BRONCHOCONSTRICTION in asthmatic patients. Successive rechallenges with aspirin may cause various responses in terms of allergic symptoms (rhinitis, conjunctivitis, asthma) with each rechallenge and aspirin reactivity may disappear (Pleskow et al, 1983)(Slepian et al, 1985).
2) In some patients (11 out of 17), bronchoconstriction is associated with elevations in venous histamine levels. In these patients, symptoms of aspirin hypersensitivity were more common and more severe compared to those patients without an elevation in venous histamine when given aspirin (Szmidt et al, 1981). Elevated prostaglandin F2alpha concentrations fell upon aspirin challenge and appearance of asthma or urticaria in aspirin-sensitive patients. Continued aspirin administration up to 650 mg per day caused tolerance and bronchodilation in 2 of 18 patients. The fall in prostaglandin products as a result of cyclooxygenase inhibition is similar in aspirin-sensitive and control subjects (Asad et al, 1984). The sensitivity to aspirin may be due to different responses to increased lipoxygenase products present secondary to cyclooxygenase inhibition (Bonne et al, 1985; Ameisen et al, 1985; Juergens et al, 1992). Serum levels of acetylsalicylic achieved during airway obstruction are sufficient to inhibit cyclo-oxygenase (Dahlen et al, 1994). In aspirin-sensitive subjects, inhibition of thromboxane synthetase alone, as opposed to cyclooxygenase was not associated with attacks of asthma or impaired pulmonary function tests (Szczeklik et al, 1987; Szczeklik, 1990). Symptoms of bronchial obstruction in aspirin-sensitive patients after aspirin ingestion are not changed by administration of prostacyclin. This would suggest that the generation of leukotrienes, which is suppressed in vitro by prostacyclin, may not occur in vivo, or that leukotrienes are not important in aspirin-induced asthma (Nizankowska et al, 1986). On histopathological examination, sinus tissues from sensitive patients have deposition of immunofluorescent antibody on epithelial basement membrane. Immunoglobulin IgG, IgA, IgM, and IgE are all present (England et al, 1987). 3) Aspirin ingestion has also been reported to improve asthma and pulmonary function tests in some patients (Kordansky et al, 1978) and reverse allergic rhinitis in several subjects (Kumar et al, 1988; Fernandez-Rivas et al, 1992). Six adult patients with bronchial asthma who received single aspirin doses of 0.3 to 1.2 g experienced bronchodilatation with clinical improvement. Asthma in these patients was characterized by a perennial course, onset after flu-like infections, lack of relationship to allergen exposure, negative skin tests to common antigens, and a history of sinusitis. Proper diagnosis is of crucial importance since improvement in asthma secondary to aspirin is rare (Szczeklik & Nizankowska, 1983).
Promoción continua a través de capacitaciones a los
profesionales de la salud.
Integración de alumnos de la escuela de Química y Farmacia de
la UACh bajo supervisión del Q.F asistencial y docente clínico
en las visitas médicas de los servicios clínicos de Medicina y
Pediatría.
Difusión de boletines informativos sobre seguridad de
medicamentos.
Elaboración de respuesta al profesional notificador de una
sospecha de RAM.
Realización de trabajos de investigación farmacoepidemiológica.
Primer curso de capacitación de FV en el HBV: 1 y 2 de Octubre 2012.
EN EL PRESENTE: Farmacovigilancia activa con las siguientes actividades:

Estratificación del riesgo
Detección y priorización de las necesidades farmacoterapéuticas en los pacientes. Diploma Calidad Farmacoterapéutica y Seguridad en el Paciente. Universidad de Valencia. España.
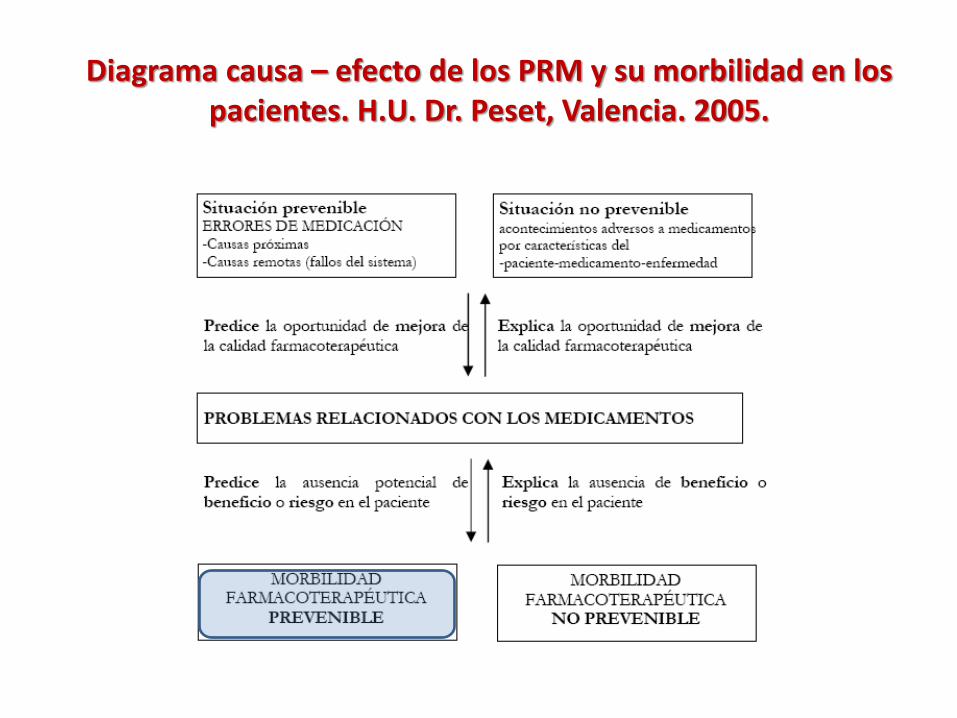
Diagrama causa – efecto de los PRM y su morbilidad en los pacientes. H.U. Dr. Peset, Valencia. 2005.

S-2012-21

11. Evaluación en
base a indicadores de actividad y n° de PRM
prevenidos, detectados y resueltos
1. Identificación del
ingreso hospitalario de pacientes
2. Conocimiento
de su historia clínica
3. Entrevista
con el paciente
4. Seguimiento
farmacoterapéutico
5. Participación en
discusiones clínicas sobre el tratamiento
farmacológico de pacientes
6. Revisión del
informe de epicrisis
7. Educación
farmacoterapéutica
al alta
8. Evaluación de la
satisfacción usuaria
9. Seguimiento vía
telefónica una semana posterior al alta
10. Educación y
seguimiento del paciente
ambulatorio
XLM - 2012

Esta presentación cuenta con la autorización de su autor para ser publicada en la página web del Instituto de Salud
Pública de Chile