ISSN 2219-4665 VISION - PAAO - Pan-American … Mark J. Mannis, MD University of California, Davis...
36
VISION VISION PAN-AMERICA PAN-AMERICA ISSN 2219-4665 Volumen X No.2 Junio 2011 G. Paolo Giuliari MD; Ama Sadaka MD; Peter Y. Chang MD; Alfonso Iovieno MD A BLIND EYE: THE PRICE OF A POOR PHYSICIAN-PATIENT COMMUNICATION A BLIND EYE: THE PRICE OF A POOR PHYSICIAN-PATIENT COMMUNICATION OJO CIEGO: EL PRECIO DE UNA POBRE COMUNICACIÓN MÉDICO-PACIENTE OJO CIEGO: EL PRECIO DE UNA POBRE COMUNICACIÓN MÉDICO-PACIENTE NIVEL DE CONOCIMIENTOS DE PACIENTES GLAUCOMATOSOS SOBRE SU ENFERMEDAD. NIVEL DE CONOCIMIENTOS DE PACIENTES GLAUCOMATOSOS SOBRE SU ENFERMEDAD. CENTRO OFTALMOLÓGICO HOSPITAL UNIVERSITARIO DR. SALVADOR ALLENDE. CENTRO OFTALMOLÓGICO HOSPITAL UNIVERSITARIO DR. SALVADOR ALLENDE. Sexo Total Edad Femenino Masculino No. % No. % No. % 18-29 años 3 4,83 2 5,26 5 5,0 30-39 años 7 11,2 7 18,4 14 14,0 40-49 años 10 16,1 9 23,6 19 19,0 50-59 años 11 17,7 10 26,3 21 21,0 60-69 años 16 25 8 6 15 7 22 22 0 Idalia Triana Casado MD, Ceija Molina Cisneros MD Ramirez-Miranda MD, Armando Gonzal ez-Gomar MD, Susana Muñoz-Sal as BSc EXTERNAL OPHTHALMOMYIASIS DUE TO SHEEP BOTFLY EXTERNAL OPHTHALMOMYIASIS DUE TO SHEEP BOTFLY OESTRUS OVIS OESTRUS OVIS LARVAE LARVAE PROPTOSIS EN EL NEONATO PROPTOSIS EN EL NEONATO Alejandra C. Iurescia MD D MD Juan an D n D. Arias M J. Fernando Arévalo MD FACS, Martin A. Serrano MD, r n A. Serrano MD, Juan n rnando Arévalo MD FACS, Martin A. Serran évalo MD FACS, M s CS u e év t e Ari a o Aré o MD FACS Martin A Serrano MD Jua D FACS Martin A Serrano M s Martin A Serrano MD Juan D Arias M M M MD FACS Martin A Serrano M Fernand FACS Marti é o MD FACS D MD MD MD MD MD MD Juan Juan an n n J. Fernando Arévalo MD FACS, Martin A. Serrano MD, J. Fernando Arévalo MD FACS, Martin A. Serrano MD, . . Fernando Arévalo MD FACS, Martin A. Fernando Arévalo MD FACS, Martin A. Arias Arias Arévalo MD FACS, Martin A. Serrano MD, Juan Arévalo MD FACS, Martin A. Serrano D D D D , Martin A. Serrano MD, , Martin A. Serrano MD, s s a a a a o o a a Se Se a a o MD FACS o MD FACS éva éva o o d d d a a e e v v i i A A n n n n n n A A in in lo MD FAC lo MD FAC A A nan nan o o o o o o o o o D D D D D D D D D D D D D D D D D D D D D a a a a a a a a a a a a a a a a a a e e é é e e A A A A A A A A A A A A é é i i i i J J J J A A A A Arévalo MD F A A é é D LATIN AMERICAN EXPERIENCE IN THE MANAGEMENT OF OPEN LATIN AMERICAN EXPERIENCE IN THE MANAGEMENT OF OPEN GLOBE INJURIES: AN INTERNET BASED SURVEY GLOBE INJURIES: AN INTERNET BASED SURVEY Mário Junqueira Nóbrega MD DIAGNOSIS AND MANAGEMENT OF POSTOPERATIVE ENDOPHTHALMITIS DIAGNOSIS AND MANAGEMENT OF POSTOPERATIVE ENDOPHTHALMITIS
Transcript of ISSN 2219-4665 VISION - PAAO - Pan-American … Mark J. Mannis, MD University of California, Davis...

VISIONVISIONPAN-AMERICAPAN-AMERICA
ISSN 2219-4665
Volumen X No.2 Junio 2011
G. Paolo Giuliari MD; Ama Sadaka MD; Peter Y. Chang MD; Alfonso Iovieno MD
A BLIND EYE: THE PRICE OF A POOR PHYSICIAN-PATIENT COMMUNICATIONA BLIND EYE: THE PRICE OF A POOR PHYSICIAN-PATIENT COMMUNICATION
OJO CIEGO: EL PRECIO DE UNA POBRE COMUNICACIÓN MÉDICO-PACIENTEOJO CIEGO: EL PRECIO DE UNA POBRE COMUNICACIÓN MÉDICO-PACIENTE
NIVEL DE CONOCIMIENTOS DE PACIENTES GLAUCOMATOSOS SOBRE SU ENFERMEDAD. NIVEL DE CONOCIMIENTOS DE PACIENTES GLAUCOMATOSOS SOBRE SU ENFERMEDAD. CENTRO OFTALMOLÓGICO HOSPITAL UNIVERSITARIO DR. SALVADOR ALLENDE.CENTRO OFTALMOLÓGICO HOSPITAL UNIVERSITARIO DR. SALVADOR ALLENDE.
Sexo Total
EdadFemenino Masculino
No. %No. % No. %
18-29 años 3 4,83 2 5,26 5 5,0
30-39 años 7 11,2 7 18,4 14 14,0
40-49 años 10 16,1 9 23,6 19 19,0
50-59 años 11 17,7 10 26,3 21 21,0
60-69 años 16 25 8 6 15 7 22 22 0
Idalia Triana Casado MD, Ceija Molina Cisneros MD
Ramirez-Miranda MD, Armando Gonzalez-Gomar MD, Susana Muñoz-Salas BSc
EXTERNAL OPHTHALMOMYIASIS DUE TO SHEEP BOTFLY EXTERNAL OPHTHALMOMYIASIS DUE TO SHEEP BOTFLY OESTRUS OVISOESTRUS OVIS LARVAE LARVAE
PROPTOSIS EN EL NEONATOPROPTOSIS EN EL NEONATO
Alejandra C. Iurescia MD
DMDJuan an Dn D. Arias MJ. Fernando Arévalo MD FACS, Martin A. Serrano MD, rn A. Serrano MD, Juannrnando Arévalo MD FACS, Martin A. Serranévalo MD FACS, M sCS ue év t e Aria o Aré o MD FACS Martin A Serrano MD JuaD FACS Martin A Serrano M sMartin A Serrano MD Juan D Arias MMMMD FACS Martin A Serrano MFernand FACS Martié o MD FACS DMDMDMDMDMDMDJuan JuananannJ. Fernando Arévalo MD FACS, Martin A. Serrano MD,J. Fernando Arévalo MD FACS, Martin A. Serrano MD, . .Fernando Arévalo MD FACS, Martin A. Fernando Arévalo MD FACS, Martin A. Arias AriasArévalo MD FACS, Martin A. Serrano MD, Juan Arévalo MD FACS, Martin A. Serrano DDD. Arias MD, Martin A. Serrano MD,, Martin A. Serrano MD, ssaaaaooaaSeSeaao MD FACSo MD FACSévaévaoodddaaee vv iiAAnnnnnnAAininlo MD FAClo MD FACAAnannan ooooooooo DDDDDDDDDDDDDDDDDDDDD aaaaaaaaaaaaaaaaaa eeééee AAAAAAAAAAAA éé iiii JJJ. Fernando Arévalo MD FACS, Martin A. Serrano MD,J. Fernando Arévalo MD FACS, Martin A. Serrano MD, AriaAriaAAFACFACArévalAréval AAAAArévalo MD FAArévalo MD FAéé DD
LATIN AMERICAN EXPERIENCE IN THE MANAGEMENT OF OPEN LATIN AMERICAN EXPERIENCE IN THE MANAGEMENT OF OPEN GLOBE INJURIES: AN INTERNET BASED SURVEYGLOBE INJURIES: AN INTERNET BASED SURVEY
Mário Junqueira Nóbrega MD
DIAGNOSIS AND MANAGEMENT OF POSTOPERATIVE ENDOPHTHALMITISDIAGNOSIS AND MANAGEMENT OF POSTOPERATIVE ENDOPHTHALMITIS

1. The AGIS Investigators: The Advanced Glaucoma Intervetion Study - The Relationship Between Control of Intraocular Pressure and Visual Field Deterioration. Am. J. Ophthalmol, 130 (4): 429-40, 2000. 2. Shirakashi, M. et al: Intraocular Pressure-Dependent Progression of VisualField Loss in Advanced Primary Open-Angle Glaucoma: A 15-Year Follow-Up. Ophthalmologica, 207: 1-5, 1993. 3. Mao, LK; Stewart, WC; Shields, MB: Correlation Between Intraocular Pressure Control and Progressive Glaucomatous Damage in Primary Open-Angle Glaucoma. Am.J. Ophthalmol, 111: 51-55, 1991. 4. Higginbotham, EJ et al. One-Year Comparison of Bimatoprost with Timolol in Patients with Glaucoma or Ocular Hypertension. Presented at American Academy Ophthalmology, Nov 11-14, 2001. 5. Gandolfi, S et al. Three-Month Comparison of Bimatoprostand Latanoprost in Patients with Glaucoma and Ocular Hypertension. Adv. Ther, 18 (3): 110-121, 2001. 6. Coleman, AL et al: A 3-Month Comparison of Bimatoprost with Timolol/Dorzolamide in Patients with Glaucoma or Ocular Hypertension. Presented at American Acedemy ofOphthalmol, New Orleans, La, 2001.
Preserva la visión alcanzando las menorespresiones-objetivo en más pacientes
Mejor comodidad posológica:
1 vez al día.
No requiere refrigeración.
Presentación conteniendo 3 ml.
LLLLLumiganumiganumiganumiganumigan® ® ® ® ® (bimatoprost) Forma farmacéutica y prForma farmacéutica y prForma farmacéutica y prForma farmacéutica y prForma farmacéutica y presentación.esentación.esentación.esentación.esentación.Frascos cuenta-gotas conteniendo 5 ml de solución oftalmológica estéril de bimatoprost a 0,03%. USO ADULTO.Composición. Composición. Composición. Composición. Composición. Cada ml contiene: 0,3 mg de bimatoprost. Vehículo: cloreto de sódio, fosfato de sódiohepta-hidratado, ácido cítrico mono-hidratado, ácido clorídrico y/o hidróxido de sódio, cloruro de benzalconio y agua purificada qsp. Indicaciones.Indicaciones.Indicaciones.Indicaciones.Indicaciones. LUMIGAN®®®®® (bimatoprost) es indicado para la reducción de la presión intra-ocular elevada en pacientes con glaucona o hipertensiónocular.Contraindicaciones.Contraindicaciones.Contraindicaciones.Contraindicaciones.Contraindicaciones. LUMIGAN®®®®® (bimatoprost) está contraindicado en pacientes con hipersensibilidad al bimatoprost o cualquier otro componente de la fórmula del producto. Pr Pr Pr Pr Precauciones y Adverecauciones y Adverecauciones y Adverecauciones y Adverecauciones y Advertencias.tencias.tencias.tencias.tencias. Advertencias. Fueron relatados aumento gradual del crescimientode las pestañas en el largo y espesura, y oscurecimiento de las pestañas (en 22% de los pacientes después 3 meses, y 36% después 6 meses de tratamiento), y, oscurecimiento de los párpados (en 1 a <3% de los pacientes después 3 meses y 3 a 10% de los pacientes después6 meses de tratamiento). También fue relatado oscurecimiento del íris en 0,2% de los pacientes tratados durante 3 meses y en 1,1% de los pacientes tratados durante 6 meses. Algunas de esas alteraciones pueden ser permanentes. Pacientes que deben recibir el tratamientode apenas uno de los ojos, deben ser informados a respecto de esas reacciones. PrPrPrPrPrecaucionesecaucionesecaucionesecaucionesecauciones LUMIGAN®®®®® (bimatoprost) no fue estudiado en pacientes con insuficiencia renal o hepática y por lo tanto debe ser utilizado con cautela en tales pacientes.Las lentes de contacto debenser retiradas antes de la instilación de LUMIGAN®®®®® (bimatoprost) y pueden ser recolocadas 15 minutos después. Los pacientes deben ser advertidos de que el producto contiene cloruro de benzalconio, que es absorvido por las lentes hidrofílicas.Si más que un medicamentode uso tópico ocular estuviera siendo utilizado, se debe respetar un intervalo de por lo menos 5 minutos entre las aplicaciones.No está previsto que LUMIGAN®®®®® (bimatoprost) presente influencia sobre la capacidad del paciente conducir vehículos u operar máquinas, sin embargo,así como para cualquier colírio, puede ocurrir visión borrosa transitoria después de la instilación; en estos casos el paciente debe aguardar que la visión se normalice antes de conducir u operar máquinas. Interacciones medicamentosas.Interacciones medicamentosas.Interacciones medicamentosas.Interacciones medicamentosas.Interacciones medicamentosas.Considerando que las concentracionescirculantes sistemicas de bimatoprost son extremadamente bajas después múltiplas instilaciones oculares (menos de 0,2 ng/ml), y, que hay varias vías encimáticas envueltas en la biotransformación de bimatoprost, no son previstas interacciones medicamentosas en humanos.No son conocidas incompatibilidades. R R R R Reacciones adversas.eacciones adversas.eacciones adversas.eacciones adversas.eacciones adversas. LUMIGAN®®®®® (bimatoprost) es bien tolerado, pudiendo causar eventos adversos oculares leves a moderados y no graves.Eventos adversos ocurriendo en 10-40% de los pacientes que recibieron doses únicas diarias, durante3 meses, en orden decreciente de incidencia fueron: hiperenia conjuntival, crecimento de las pestañas y prurito ocular.Eventos adversos ocurriendo en aproximadamente 3 a < 10% de los pacientes, en orden decreciente de incidencia, incluyeron: sequedad ocular, ardor ocular,sensación de cuerpo estraño en el ojo, dolor ocular y distúrbios de la visión.Eventos adversos ocurriendo en 1 a <3% de los pacientes fueron: cefalea, eritema de los párpados, pigmentación de la piel periocular, irritación ocular, secreción ocular, astenopia, conjuntivitis alérgica,lagrimeo, y fotofobia.En menos de 1% de los pacientes fueron relatadas: inflamación intra-ocular, mencionada como iritis y pigmentación del íris, ceratitis puntiforme superficial, alteración de las pruebas de función hepática e infecciones (principalmente resfriados e infeccionesde las vías respiratorias).Con tratamientos de 6 meses de duración fueron observados, además de los eventos adversos relatados más arriba, en aproximadamente 1 a <3% de los pacientes, edema conjuntival, blefaritis y astenia. En tratamientos de asociación con betabloqueador,durante 6 meses, además de los eventos de más arriba, fueron observados en aproximadamente 1 a <3% de los pacientes, erosión de la córnea, y empeoramiento de la acuidad visual. En menos de 1% de los pacientes, blefarospasmo, depresión, retracción de los párpados,hemorragia retiniana y vértigo.La frecuencia y gravedad de los eventos adversos fueron relacionados a la dosis, y, en general, ocurrieron cuando la dosis recomendada no fue seguida.Posología y Administración.Posología y Administración.Posología y Administración.Posología y Administración.Posología y Administración.Aplicar una gota en el ojo afectado, una vez al día, a la noche.La dosis no debe exceder a una dosis única diaria, pues fue demostrado que la administración más frecuente puede disminuir el efecto hipotensor sobre la hipertensión ocular.LUMIGAN®®®®® (bimatoprost) puede ser administrado concomitantemente con otros productos oftálmicostópicos para reducir la hipertensión intra-ocular, respetándose el intervalo de por lo menos 5 minutos entre la administración de los medicamentos. VENTA BAJO PRESCRIPCIÓN MÉDICA.“ESTE PRODUCTO ES UM MEDICAMENTO NUEVO AUNQUE LAS INVESTIGACIONES HAYANINDICADO EFICACIA Y SEGURIDAD, CUANDO CORRECTAMENTE INDICADO, PUEDEN SURGIR REACCIONES ADVERSAS NO PREVISTAS, AÚN NO DESCRIPTAS O CONOCIDAS, EN CASO DE SOSPECHA DE REACCIÓN ADVERSA, EL MÉDICO RESPONSABLE DEBE SER NOTIFICADO.
vs. timolol 4 vs. latanoprost6
Porcentaje de Pacientes quealcanzaron la PIO-Objetivo ≤≤≤≤≤14 21% 9% 17% 2% 19% 9%
Porcentaje de Pacientes quealcanzaron la PIO-Objetivo ≤≤≤≤≤15 31% 16% 24% 9% 29% 14%
dorzolamida/ timolol 5vs.
®®®
Lumigan® alcanza la PIO-objetivo de 14/15 mmHg en un mayor númerode pacientes:
Investigadores de diversos estudios, (AGIS, Shirakashi, Shields)han comprobado que alcanzar y mantener la PIO entre 14 y 15 mmHgreduce la progresión de pérdida del campo visual1,2,3.

PAN-AMERICA
Mark J. Mannis, MDUniversity of California, Davis
Sacramento, CaliforniaEditor-in-Chief
Cristián Luco, MDSantiago, ChileAssociate Editor
Teresa J. BradshawArlington, TexasManaging Editor
Terri L. GrassiArlington, TexasProduction Editor
EDITORIAL BOARD
Eduardo Alfonso, MDMiami, Florida USA
Eduardo Arenas, MDBogotá, Colombia
J. Fernando Arévalo, MDCaracas, Venezuela
José A. Roca Fernández, MDLima, Perú
Denise de Freitas, MDSão Paulo, Brazil
Marian Macsai, MDChicago, Illinois USA
David E. Pelayes, MD PhDBuenos Aires, Argentina
Alfredo Sadun, MDLos Angeles, California USA
Allan Slomovic, MDToronto, Ontario, Canada
Luciene Barbosa de Sousa, MDSão Paulo, Brazil
Lihteh Wu, MDSan José, Costa Rica
Paulo Dantas, MDSão Paulo, Brazil
Chun Cheng Lin Yang, MD MScSan José, Costa Rica
OFFICERS
Cristián Luco MDSantiago, Chile
President, Pan-American Association of Ophthalmology
Nelson R. MarquesSão Paulo, Brazil
Chairman of the Board,Pan-American Ophthalmological Foundation
PRODUCTION STAFF
Director of Printed Matters CLMEliana Barbosa
Graphic Design CLMJuan David Medina / Catalina Lozano Ortega
Databases and Distribution CLMXimena Ortega Bernal
CopyeditingPiedad CamachoVanessa Carmona
PrepressAlejandro Bernal
PAOF INDUSTRY SPONSORS
• Advanced Medical Optics Inc.• Alcon Inc.• Allergan Inc.• Bausch & Lomb Inc.• Carl Zeiss Meditec Inc.
• Johnson & Johnson Vision Care Latin America• Merck & Co Inc.• Novartis International AG.• Santen Inc.
Prepress Creative Latin Media. Printed in Printer Colombiana - Colombia
CREATIVE LATIN MEDIA, LLC.2901 Clint Moore, P.M.B 117 Boca Raton, FL 33496
Tel.: (561) 495 4728 • Fax: (561) 865 1934E-mail: [email protected] • [email protected]
Junio 2011
Special thanks to Ana Carolina Vieira, Enrique Graue Hernandez, Mapy Padilla, Miguel N. Burnier Jr., Dominique de Souza and Cristian Luco for assistance in translation.

MENSAJE DEL EDITOR / MESSAGE FROM THE EDITOR
34 PAN-AMERICA
Del Editor:
Bienvenidos al Congreso Panamericano, aquí en la hermosa Buenos Aires. Este año se distinguirá por muchos nuevos programas y logros de la Asociación Panamericana de Oftalmología. Sin duda alguna, destaca la indexación formal de Visión Pan-America, nuestra publicación científica. En la última década, VPA se ha convertido en una publicación de ciencia clínica de alta calidad, legítima, revisada por pares y basada en las Américas. Representa la única revista verdaderamente panamericana, publicando trabajos en Español, Inglés, Portugués y Francés.
Los invito a que durante el año que viene manden su mejor trabajo, incluyendo revisiones clínicas, re-portes de nuevas técnicas o tratamientos, serie de ca-sos clínicos, investigación básica y reportes de casos para su publicación en la revista. Con una circulación que excede a la de muchas revistas nacionales y de especialidad, VPA es un importante vehículo para el intercambio de información en las Américas.
Esperamos sus contribuciones
From the Editor:
Welcome to the Pan-American Congress here in beautiful Buenos Aires. This year we will mark many new programs and accomplishments for the Pan-Ame-rican Association of Ophthalmology. Not the least of these will be the formal indexing of our scientific pu-blication, Vision Pan-America. Over the past decade, VPA has grown into a legitimate, peer-reviewed pu-blication of high quality clinical science based in the Americas. It represents the only truly pan-American ophthalmology journal, publishing papers in Spanish, English, Portuguese and French.
In the coming year, I urge you to send your best work including clinical reviews, reports of new techni-ques or therapies, clinical case series, basic investi-gation, and case reports for publication in the journal. With a circulation that exceeds many of the specialty and national journals, VPA serves as an important ve-hicle for information exchange in the Americas.
We look forward to your contributions.
Mark Mannis, MD, FACSEditor-en JefeVision Pan-America
EditorialMark J. Mannis, MDEditor en Jefe Vision Pan-America
Mark Mannis, MD, FACSEditor-in-ChiefVision Pan-America

Junio 2011
PAN-AMERICA 35PAN-AMERICA
Do Editor:
Sejam bem-vindos ao Congresso Pan-Americano aqui na linda Buenos Aires. Este ano será marcado por muitos novos programas e realizações na Asso-ciação Pan-Americana de Oftalmologia. Não o menor destes será a indexação formal de nossa revista cientí-fica, Vision Pan-America. Ao longo da última década, VPA tornou-se uma legítima revista revisada por pares de ciências clínicas de alta qualidade, localizada nas Américas. Representa a única revista de Oftalmologia verdadeiramente Pan-Americana, publicando artigos em espanhol, inglês, português e francês.
No próximo ano, solicito a vocês que enviem seus melhores trabalhos, incluindo revisões clínicas, relatos de novas técnicas e terapias, séries de casos clínicos, investigação básica e relatos de casos para publicação neste journal. Com uma circulação que excede aquela de muitas outras revistas nacionais e de especialida-des, a VPA funciona como um importante veículo para o intercâmbio de informações nas Américas.
Aguardamos a sua contribuição.
De l’Éditeur:
Bienvenue au Congrès Pan-Américain dans cette belle ville, Buenos Aires!
Cette année, nous allons marquer beaucoup de nouveaux programmes et les réalisations de l’Asso-ciation Pan-Américaine d’Ophtalmologie. L’indexation officielle de notre publication scientifique Vision Pan-America (VPA) ne sera pas la moindre de nos réa-lisations. Au cours de cette dernière décennie, VPA a grandi et est devenue une légitime «peer reviewed publication», une revue scientifique de haute qualité clinique, basée dans les Amériques. Elle représente le seul véritable journal pan-américain d’ophtalmologie, qui publie des articles en Espagnol, Anglais, Portu-gais et Français.
Pour l’année prochaine, je vous invite, instam-ment, à envoyer vos meilleurs travaux, y compris les examens cliniques, des rapports sur de nouvelles techniques ou thérapies, des séries de cas cliniques, la recherche de base et des rapports de cas à publier dans notre journal.
Avec une circulation qui dépasse de beaucoup la majorité des revues scientifiques de spécialisation et les revues nationales, Vision Pan-America, constitue un véhicule important d’échange d’informations dans les Amériques.
Nous nous réjouissons de vos contributions.
Mark Mannis, MD, FACSEditor-chefeVision Pan-America
Mannis Mark MD FACSRédacteur en chefVIsion Pan-Amérique

MENSAJE DEL PRESIDENTE / MESSAGE FROM THE PRESIDENT
36 PAN-AMERICA
¿Por qué la PAAO es líder de la oftalmología conti-nental? Para ser líder se deben tener algunos elementos que imprimen a un individuo o a una institución las ca-racterísticas de líder.
Hace 70 años fue creada la PAAO por tres oftal-mólogos en una sesión de la Academia Americana de Oftalmología y Otorrinolaringología en Cleveland, Ohio. El doctor Conrad Behrens, el doctor Harry Gradle y el doctor Moacyr Alvaro de Sao Paulo decidieron crear una institución que acercara a los oftalmólogos de habla in-glesa de Estados Unidos con el resto de América his-pana. Los inicios fueron lentos, pero pronto creció a su posición actual de líder de la oftalmología.
Como líder tiene carácter y talento. El carácter lo ha adquirido a medida que evoluciona en el tiempo y el talento es reflejado en su historia y en la capacidad de sus oficiales.
Es líder porque desarrolla un accionar con significa-do en sus cursos y congresos y fomenta el compañeris-mo. Tiene capacidad de plantear un proyecto, planificar-lo y llevarlo a cabo con éxito.
Es líder porque ejerce autoridad. La autoridad invita a una acción, no impone como sí lo hace el “poder”. La autoridad se compromete en la acción y no limita a los demás. La PAAO no tiene poder, sólo la autoridad que emana de su prestigio como institución confiable.
Es líder comprometido con la acción y es auténtico. Esta última característica es de gran trascendencia, ya que es fiel a sus orígenes, no imita a otros con consis-tencia en su acción y sus principios. La PAAO es quien es, ella misma.
También es situacional y se adapta al tiempo y al espacio determinado en cada evento sin abandonar sus principios básicos fundacionales. Hay eventos que se planifican con años de anticipación como los congresos
y cursos. Pero hay situaciones en que no hay tiempo para proyectar y se debe pasar directo a la acción.
Enero 2010, terremoto en Haití: Parte del Comité Ejecutivo estaba en el Curso de Liderazgo en San Fran-cisco. Se lanza la idea “Ayudemos a Haití”. La PAAO se lanza en ayuda de los oftalmólogos de Haití, nuestros hermanos oftalmólogos. Fuimos unas de las primeras ONG en llegar con ayuda. Primero se distribuyeron ali-mentos no perecibles, luego instrumental de examen básico y en una segunda etapa, con dinero donado por la OSWI (Ophthalmological Society of the West Indies), se otorgaron dos becas para oftalmólogos haitianos al curso de liderazgo de la PAAO. Además se consiguió una beca parcial a la India para aprender facoemulsificación y una beca en el Bascom Palmer Institute.
La PAAO es auténtica representante de los oftalmó-logos de las Américas, somos los oftalmólogos de las Américas, sentimos, conocemos y amamos nuestro te-rritorio. No somos una entidad extraña, alienígena, que se quiere aposentar en nuestra tierra, somos america-nos. Confían en nosotros por tener carácter, capacidad, talento y amor para llevar a cabo el mandato de nuestros asociados. Organizamos congresos y cursos, somos ca-paces de responder a las desgracias de las naciones y ahora agregamos la defensa del gremio (Advocacy) ante invasiones de fuera de nuestro territorio como de fuera de nuestra profesión.
La PAAO es líder de la oftalmología continental, cumple y merece ser seguida.
EditorialCristián Luco, MDPresidente PAAO 2009-2011
Dr. Cristián LucoPresidente, PAAO

Junio 2011
PAN-AMERICA 37PAN-AMERICA
Why is the PAAO the leader in continental ophthalmology?
Seventy years ago, three ophthalmologists crea-ted the PAAO in a session at the American Academy of Ophthalmology and Otolaryngology in Cleveland, Ohio. Dr. Conrad Behrens, Dr. Harry Gradle, and Dr. Moacyr Alvaro of Sao Paulo decided to create an institution that would bring together English speaking ophthalmologists with the rest of Latin America. Initial growth was slow, but soon the PAAO grew to assume its current position of leadership in ophthalmology.
Its leadership role stems from character and talent. The character and talent are reflected in the abilities of its officials. Its leadership is reflected in its courses and meetings that promote fellowship. The PAAO does not have the power of authority, but only the authority that emanates from its prestige as a trusted institution. The PAAO has learned to adapt itself to the times without abandoning its basic founding principals. We plan our educational events years in advance, but at the same time, we react to developments in the hemisphere.
Immediately after the earthquake in Haiti, for exam-ple, in January 2010, the PAAO launched the program “Ayudemos a Haiti” to help the ophthalmologists of Haiti. We were among the first non-governmental orga-nizations to arrive with help. First, non-perishable food was distributed, then basic examination instruments, and in a second phase a variety of funding was provided including a donation by the Ophthalmological Society of the West Indies (OSWI), two scholarships for Haitian ophthalmologists to attend the PAAO leadership course, a grant for training in phacoemulsification, and a grant from the Bascom Palmer Eye Institute.
The PAAO is an authentic representation of the ophthalmologists of the Americas. Trust in us to have
the character, ability, talent, and desire to carry out the mandate of our members. We organize both meetings and courses to aid in the education of our constituents, and now we are providing advocacy against invasions from outside our territory and outside our profession. The PAAO is a leader in continental ophthalmology; we hope that it earns your loyalty and support.
Cristián Luco MDPAAO President
REVIEW
38 PAN-AMERICA
Latin American Experience in the Management of Open Globe Injuries: An Internet Based Survey
J. Fernando Arevalo MD FACS1, Martin A. Serrano MD1, Juan D. Arias MD1
1. From the Retina and Vitreous Service, Clinica Oftalmologica Centro Caracas, Caracas, Venezuela
Presented in part at the Joint Meeting of the American Academy of Ophthalmology and the Middle East Africa Council of Ophthalmology, Chicago, IL, October 2010.
The authors have no fi nancial or proprietary interest in any of the products or techniques mentioned in this article.
Supported in part by the Arevalo-Coutinho Foundation for Research in Ophthalmology, Caracas, Venezuela.
Correspondence:
J. Fernando Arevalo MD FACSClinica Oftalmologica Centro CaracasEdif. Centro Caracas PH-1, Av. Panteon, San BernardinoCaracas 1010, VenezuelaPhone: (+58-212) 576-8687. Fax: (+58-212) 576-8815E-mail address: [email protected]
Abstract
Purpose: To evaluate the current preferences and trends of the vitreoretinal surgeons in Latin America re-garding an open globe injury.
Design: Internet based survey.
Participants: The Pan-American Retina & Vitreous Society (PRVS), Venezuelan Society of Ophthalmology (VSO), and the Pan-American Collaborative Retina Stu-dy Group (PACORES) members participated.
Methods: This questionnaire was sent by the principal investigator (JFA) to the PRVS, VSO, and PA-CORES’ web lists with a total of 768 surveys sent. An ocular trauma case scenario was provided with a set of 8 questions related to that case.
Results: Out of the 768 surveys sent, 38 (4.95%) physicians from 38 centers of 26 different cities in 13 countries of Latin America responded. The vast majority of consulted specialists do practice at a large city, and consider that severe ocular trauma cases are somewhat/very common in their locations. Most of the respondent surgeon’s centers have surgical capability, 63% of them have a room staff available 24/7, most of them operate trauma cases, and 56% perform staged surgery. Half of the consulted specialists are satisfied with how eye trauma logistics are handled in their area.
Conclusions: Those who perform the emergency intervention in big city centers have been trained ade-quately, and the responses were received mostly from trauma centers, with facilities outside regular business hours, allowing a complete approach (suturing plus vi-trectomy if needed) of the injured patient. Our results seem to have a response bias as only 1 (2.7%) of the respondents was from a small city, and most of them were from trauma centers. Trauma cases may be referred from small cities to trauma centers in Latin America.
Resumen
Propósito: Evaluar las preferencias y tendencias actuales de los cirujanos de vítreo y retina en América Latina con respecto a un traumatismo ocular abierto.
Diseño: Survey a través de Internet.
Participantes: Los miembros de la Sociedad Panamericana de Retina y Vítreo (SPRV), la Sociedad Venezolana de Oftalmología (SVO), y el Grupo de Es-tudio Panamericano Colaborativo de Retina (PACO-RES) participaron.
Métodos: El cuestionario fue enviado por el inves-tigador principal (JFA) a través de las listas web de la SPRV, SVO y PACORES, con un total de 768 encuestas enviadas. Un escenario de un caso de trauma ocular fue provisto con ocho preguntas referentes a dicho caso.
Resultados: De las 768 encuestas enviadas, res-pondieron 38 (4.95%) médicos de 38 centros de 26 diferentes ciudades en 13 países de Latinoamérica. La vasta mayoría de los especialistas consultados realizan su práctica en grandes ciudades, y consideran que los casos de trauma ocular severo son algo/bastante comu-nes en sus localidades. La mayoría de los centros de los cirujanos que respondieron cuentan con capacidad qui-rúrgica, 63% de éstos tienen un personal de emergencia disponible 24/7, la mayoría opera casos de trauma y el 56% realizan cirugía por estadíos. La mitad de los es-pecialistas consultados están satisfechos con cómo la logística de trauma ocular es manejada en su área.
Conclusiones: Aquellos que realizan intervencio-nes de emergencia en los centros de grandes ciudades han sido entrenados adecuadamente, y las respuestas fueron recibidas mayormente de centros de trauma, con servicio fuera de horario de oficina regular, permitiendo un abordaje completo (sutura más vitrectomía de ser necesario) del paciente traumatizado. Nuestros resulta-

Junio 2011
PAN-AMERICA 39PAN-AMERICA
dos parecen tener un sesgo en las respuestas, ya que sólo 1 (2,7%) de los encuestados que respondieron era de una ciudad pequeña y la mayoría de éstos eran de centros que manejan trauma. Los casos de trauma pudieran ser referidos de las ciudades pequeñas a los centros especializados en trauma en América Latina.
Introduction
Ocular trauma of the posterior segment is a sig-nificant cause of visual loss, with an estimated global incidence of more than 200 000 cases per year.1 The incidence rates of ocular trauma requiring hospitali-zation are reported to be 8.1 per 100 000 persons per year in Scotland,2 12.6 per 100 000 persons per year in Singapore,3 13.2 per 100 000 persons per year in the United States,4 and 15.2 per 100 000 persons per year in Australia.5
Several studies have suggested that the factors that significantly predict visual outcome after open globe injuries are initial visual acuity,6,7 presence of a rela-tive afferent pupillary defect (RAPD),7,8 mechanism of injury,7,9,10 wound location,7,11,12 adnexal trauma,8,13 lens damage,7,12 hyphema,14 vitreous hemorrhage,11,15 and retinal detachment.11,16 Despite extensive advances in surgical techniques and instrumentation over the past few decades,7,17 visual open globe injuries are a common cause of blindness worldwide. Frequent me-chanisms of injury include projectiles, assaults, falls, motor vehicle collisions, sports, and occupational ac-cidents.18 With the advent of microsurgical techniques in the 1960s, surgeons successfully repaired eyes with trauma involving the posterior segment but visual re-sults were often dismal.6,19
Many aspects of vitrectomy surgery for open-globe injuries remain controversial. The general areas include the role and timing of vitrectomy surgery, the use of prophylactic cryotherapy and scleral buckling, prophylactic use of antibiotics and routes of antibiotic administration, vitrectomy versus vitreous tap for trau-matic endophthalmitis, and the concurrent placement of intraocular lenses.15,21,22
Despite a general consensus about many of the indications for the use of vitrectomy in open-globe injuries, the timing of this intervention remains highly controversial. Most surgeons will agree that immediate vitrectomy is indicated for posttraumatic endophthalmi-tis or intraocular foreign body (IOFB) with high risk of infection, but timing of surgery with other scenarios is less clear.23,24 There are arguments with theoretic and experimental rationale for vitrectomy within 3 days of injury,25-29 from 4 to 10 days,30-34 before 2 weeks,11,35-40 and from 15 to 30 days after injury.41,42 Cleary and Ryan43 compared vitrectomy at 1, 14, and 70 days after a standardized injury with intravitreal autologous blood injection known to cause a reproducible tractional re-
tinal detachment. By day 70, most eyes already had a retinal detachment, but prevention of retinal detachment was documented with vitrectomy at both 1 and 14 days post-injury. Whereas there was no significant differen-ce between vitrectomy at 1 and 14 days with regard to its ability to prevent retinal detachment, it was noted that surgery at 1 day was technically more difficult, with increased incidence of vitreorretinal adhesions particu-larly at the vitreous base. By day 14, a posterior vitreous detachment had occurred in many cases and the vi-treous was generally easier to cut.
The objective of the current study was to evaluate the actual preferences and trends of the vitreoretinal sur-geons in Latin America regarding an open globe injury.
Materials and Methods
The American Society of Ocular Trauma (ASOT), in-terested in learning about the Ophthalmology coverage concerns in the hospital emergency room (ER), made a survey for the 2010 ASOT symposium at the annual American Academy of Ophthalmology (AAO) meeting in Chicago, providing an ocular trauma case scenario with a set of questions related to that case. This ques-tionnaire was sent by one of the authors (JFA) to the Pan-American Retina & Vitreous Society (PRVS), Ve-nezuelan Society of Ophthalmology (VSO) and the Pan-American Collaborative Retina Study Group (PACORES) web lists, with a total of 768 surveys sent.
The case and questions presented by the ASOT were:
The Case Scenario:
A 65 year old male presenting to hospital ER af-ter 5 PM following accidental fall with Light Perception vision, limbal rupture with iris prolapse, partial hyphe-ma, luxated crystalline lens, and vitreous hemorrhage. Wound closure, anterior segment reconstruction, and vitrectomy are needed.
The Questions:
1) Where is your practice: Large city (> 250,000), small city (< 250,000), rural area?
1A) How large is the population you/your practice serve?
1B) How common is serious eye injury in this area: very - somewhat - rare?
2) How large is your facility: Solo practice, a group, a city/public or private hospital, a university hospital?
3) Do you have on-site surgical capability?
3A) Is there adequate equipment in the surgical suite to allow complete treatment during after-hours?

REVIEW
40 PAN-AMERICA
3B) Is there trained eye operating room staff avai-lable 24/7, including anesthesia?
4) What do you do with the injured patient?
4A) Refer or operate yourself?
4B) If you refer the patient, where to? University hospital? City hospital or its equivalent? A private surgical center? Would the referral be because your facility is closed/does not offer full services of because you think it is in the patient’s best interest?
4C) If you operate yourself, will you do staged surgery or a comprehensive primary surgery?
4D) If you do staged surgery, how long do you wait until your second (vitrectomy) surgery?
5) Once the patient has been treated by referred physician, will that physician return the patient back to you for follow-up/continual care?
6) Do financial considerations play a role in your decision-making?
7) Is there adequate eye trauma coverage/expertise at your hospital ER - yes or no?
7A) How frequent are you on ER call per month? (how many days/month)
8) In summary, are you satisfied with how “eye trauma logistics” are handled in your area? Do patients receive the best care (optimal for the injury) or the best care based on the circumstances?
The responses were tabulated and presented at the 2010 annual AAO meeting by one of the authors (JFA).
Results
Out of the 768 surveys sent, 38 (4.95%) physicians from 38 centers of 26 different cities in 13 countries of Latin America responded. Thirty-two (84.2%) respon-ded in Spanish, and 6 (15.8%) in English.
To the first question (Figure 1) “Where is your practice: Large city (> 250,000), small city (< 250,000), rural area?”, 37 (97.3%) responded that in a large city, and 1 (2.7%) that in a small city. To question 1A (Figure 2) “How large is the population you/your practice serve?” 3 (7.9%) responded that ≤ 500.000 people, 12 (31.6%) > 500.000 up to 1 mi-llion people, 4 (10.5%) > 1 million up to 2 million people, 16 (42.1%) more than 2 million people, and 3 (7.9%) did not answered. To question 1B (Figure 3) “How common is serious eye injury in this area: very - somewhat - rare?” 13 (34.2%) answered that very common, 20 (52.3%) that somewhat common, and 5 (13.16%) responded that was rare.
Figure 1. The vast majority (37[97.3%]) of consulted specialists do practice at a large city.
Figure 2. When asked about how large was the population served by these surgeons, more than 84% serve a population > 500.000 people.
Figure 3. More than 86% of the consulted specialist considers that severe ocular trauma cases are “Somewhat” and “Very common” in their locations.
Figure 4. To the second question, the percentages about “how large were their facility” was very similar from “solo practice” and “university hospital” as the most common responses (23.7%).
Junio 2011
PAN-AMERICA 41PAN-AMERICA
To question 2 (Figure 4) “How large is your facility: Solo practice, a group, a city/public or private hospital, a university hospital?” 7 (18.4%) responded that a Solo practice, 8 (21%) a Group practice, 4 (10.5%) a City hospital, 9 (23.7%) a Private hospital, 9 (23.7%) a Uni-versity hospital, and 1 (2.6%) did not answered.
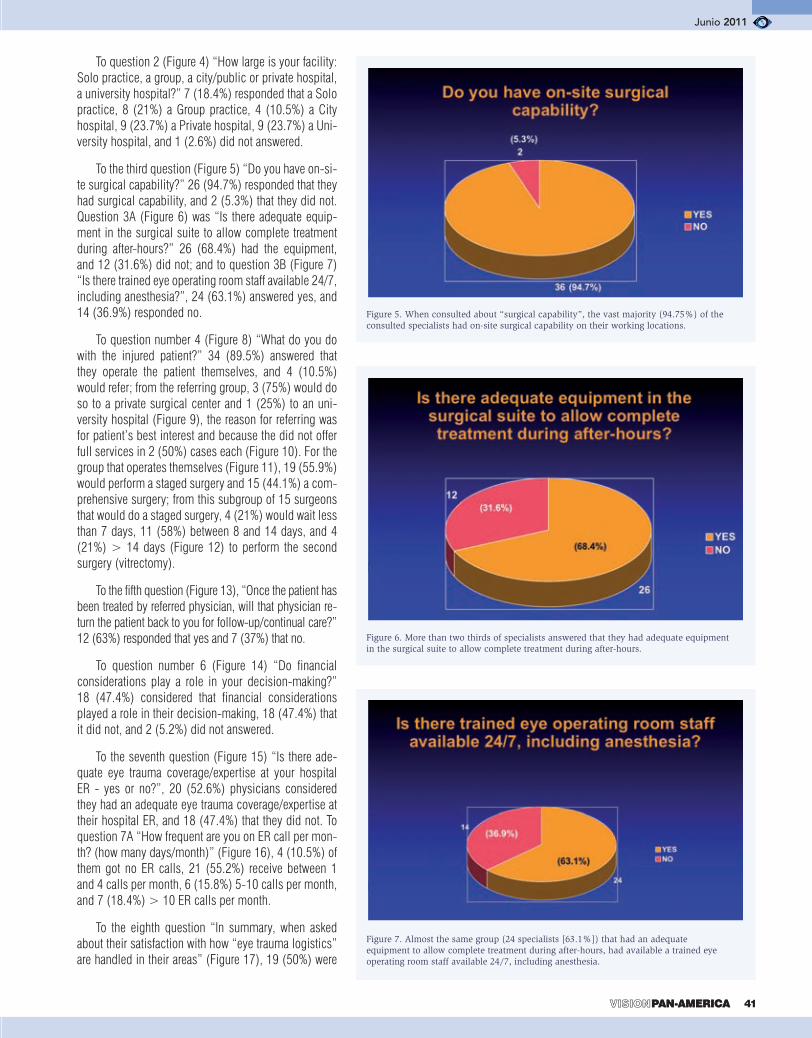
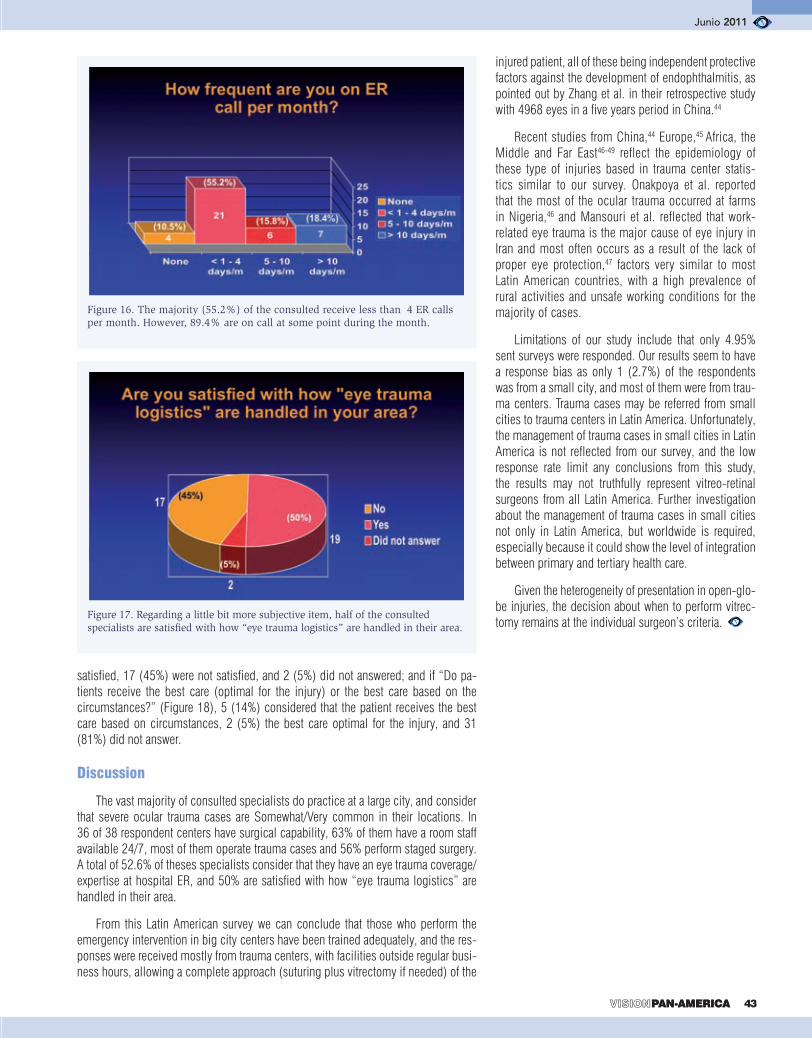
To the third question (Figure 5) “Do you have on-si-te surgical capability?” 26 (94.7%) responded that they had surgical capability, and 2 (5.3%) that they did not. Question 3A (Figure 6) was “Is there adequate equip-ment in the surgical suite to allow complete treatment during after-hours?” 26 (68.4%) had the equipment, and 12 (31.6%) did not; and to question 3B (Figure 7) “Is there trained eye operating room staff available 24/7, including anesthesia?”, 24 (63.1%) answered yes, and 14 (36.9%) responded no.
To question number 4 (Figure 8) “What do you do with the injured patient?” 34 (89.5%) answered that they operate the patient themselves, and 4 (10.5%) would refer; from the referring group, 3 (75%) would do so to a private surgical center and 1 (25%) to an uni-versity hospital (Figure 9), the reason for referring was for patient’s best interest and because the did not offer full services in 2 (50%) cases each (Figure 10). For the group that operates themselves (Figure 11), 19 (55.9%) would perform a staged surgery and 15 (44.1%) a com-prehensive surgery; from this subgroup of 15 surgeons that would do a staged surgery, 4 (21%) would wait less than 7 days, 11 (58%) between 8 and 14 days, and 4 (21%) > 14 days (Figure 12) to perform the second surgery (vitrectomy).
To the fifth question (Figure 13), “Once the patient has been treated by referred physician, will that physician re-turn the patient back to you for follow-up/continual care?” 12 (63%) responded that yes and 7 (37%) that no.
To question number 6 (Figure 14) “Do financial considerations play a role in your decision-making?” 18 (47.4%) considered that financial considerations played a role in their decision-making, 18 (47.4%) that it did not, and 2 (5.2%) did not answered.
To the seventh question (Figure 15) “Is there ade-quate eye trauma coverage/expertise at your hospital ER - yes or no?”, 20 (52.6%) physicians considered they had an adequate eye trauma coverage/expertise at their hospital ER, and 18 (47.4%) that they did not. To question 7A “How frequent are you on ER call per mon-th? (how many days/month)” (Figure 16), 4 (10.5%) of them got no ER calls, 21 (55.2%) receive between 1 and 4 calls per month, 6 (15.8%) 5-10 calls per month, and 7 (18.4%) > 10 ER calls per month.
To the eighth question “In summary, when asked about their satisfaction with how “eye trauma logistics” are handled in their areas” (Figure 17), 19 (50%) were
Figure 5. When consulted about “surgical capability”, the vast majority (94.75%) of the consulted specialists had on-site surgical capability on their working locations.
Figure 6. More than two thirds of specialists answered that they had adequate equipment in the surgical suite to allow complete treatment during after-hours.
Figure 7. Almost the same group (24 specialists [63.1%]) that had an adequate equipment to allow complete treatment during after-hours, had available a trained eye operating room staff available 24/7, including anesthesia.

REVIEW
42 PAN-AMERICA
Figure 9. From those specialists that refer the injured patient, 75% do so to a private surgical center.
Figure 8. When asked about what to do with an injured patient, only a 10.5% refers, the rest (89.5%) operate them.
Figure 11. From those that perform surgery, when asked about “if they perform a staged surgery or a comprehensive primary surgery”, 55.9% perform staged surgery.
Figure 10. Half of the group of specialists that refer the patient would refer because their facility does not offer full services and the other half because they think it is in the patient's best interest.
Figure 13. More than half of the specialists group that refers the patients says that the referred physician returns the patient back to them for follow-up/continual care.
Figure 12. In the group that performs staged surgery, 79% wait up to 14 days for the second (vitrectomy) surgery.
Figure 14. When asked if fi nancial considerations played a role in their decision-making, the answer was splited equally between both groups (yes or no).
Figure 15. There was no a signifi cant difference (52.6% vs. 47.4%) between the specialists that considered that they had an adequate eye trauma coverage/expertise at their hospital ER or not.
Junio 2011
PAN-AMERICA 43PAN-AMERICA
satisfied, 17 (45%) were not satisfied, and 2 (5%) did not answered; and if “Do pa-tients receive the best care (optimal for the injury) or the best care based on the circumstances?” (Figure 18), 5 (14%) considered that the patient receives the best care based on circumstances, 2 (5%) the best care optimal for the injury, and 31 (81%) did not answer.
Discussion
The vast majority of consulted specialists do practice at a large city, and consider that severe ocular trauma cases are Somewhat/Very common in their locations. In 36 of 38 respondent centers have surgical capability, 63% of them have a room staff available 24/7, most of them operate trauma cases and 56% perform staged surgery. A total of 52.6% of theses specialists consider that they have an eye trauma coverage/expertise at hospital ER, and 50% are satisfied with how “eye trauma logistics” are handled in their area.
From this Latin American survey we can conclude that those who perform the emergency intervention in big city centers have been trained adequately, and the res-ponses were received mostly from trauma centers, with facilities outside regular busi-ness hours, allowing a complete approach (suturing plus vitrectomy if needed) of the
Figure 16. The majority (55.2%) of the consulted receive less than 4 ER calls per month. However, 89.4% are on call at some point during the month.
Figure 17. Regarding a little bit more subjective item, half of the consulted specialists are satisfi ed with how “eye trauma logistics” are handled in their area.
injured patient, all of these being independent protective factors against the development of endophthalmitis, as pointed out by Zhang et al. in their retrospective study with 4968 eyes in a five years period in China.44
Recent studies from China,44 Europe,45 Africa, the Middle and Far East46-49 reflect the epidemiology of these type of injuries based in trauma center statis-tics similar to our survey. Onakpoya et al. reported that the most of the ocular trauma occurred at farms in Nigeria,46 and Mansouri et al. reflected that work-related eye trauma is the major cause of eye injury in Iran and most often occurs as a result of the lack of proper eye protection,47 factors very similar to most Latin American countries, with a high prevalence of rural activities and unsafe working conditions for the majority of cases.
Limitations of our study include that only 4.95% sent surveys were responded. Our results seem to have a response bias as only 1 (2.7%) of the respondents was from a small city, and most of them were from trau-ma centers. Trauma cases may be referred from small cities to trauma centers in Latin America. Unfortunately, the management of trauma cases in small cities in Latin America is not reflected from our survey, and the low response rate limit any conclusions from this study, the results may not truthfully represent vitreo-retinal surgeons from all Latin America. Further investigation about the management of trauma cases in small cities not only in Latin America, but worldwide is required, especially because it could show the level of integration between primary and tertiary health care.
Given the heterogeneity of presentation in open-glo-be injuries, the decision about when to perform vitrec-tomy remains at the individual surgeon’s criteria.

REVIEW
44 PAN-AMERICA
REFERENCIAS
1. Negrel AD and Thylefors B. The global impact of eye inju-ries. Ophthalmic Epidemiol 5 (1998), pp. 143–169.
2. Desai P, MacEwen CJ, Baines P. Incidence of cases of ocular trauma admitted to hos-pital and incidence of blind-ing outcome. Br J Ophthalmol 1996; 80: 592–596.
3. Wong TY, Tielsch JM. A population-based study on the incidence of severe ocu-lar trauma in Singapore. Am J Ophthalmol Clin North Am 1999; 128: 345–351.
4. Klopfer J, Tielsch JM, Vitale S. Ocular trauma in the Unit-ed States: eye injuries result-ing in hospitalization, 1984 through 1987. Arch Ophthal-mol 1992; 110: 838–842.
5. Fong LP. Eye injuries in Victoria, Australia. Med J Aust 1995; 162: 64–68.
6. Groessl S, Nanda SK, Mieler WF. Assault-related penetrat-ing ocular injury. Am J Oph-thalmol 1993; 116: 26–33.
7. Pieramici DJ, MacCumber MW, Humayun MU. Open globe injuries. Update on types of injuries and visual results. Ophthalmology 1996; 103: 1798–1803.
8. Rahman I, Maino A, De-vadason D. Open globe in-juries: factors predictive of poor outcome. Eye 2006; 20: 1336–1341.
9. Dunn ES, Jaeger EA, Jef-fers JB. The epidemiology of ruptured globes. Ann Oph-thalmol 1992; 24: 405–410.
10. Gilbert CM, Soong HK, Hirst LW. A two-year pro-spective study of penetrating ocular trauma at the Wilmer Ophthalmological Institute. Ann Ophthalmol 1987; 19: 104–106.
11. Brinton GS, Aaberg TM, Reeser FH. Surgical results in ocular trauma involving the posterior segment. Am J Oph-thalmol 1982; 93: 271–278.
12. Sternberg P, de Juan E, Michels RG. Multivariate analysis of prognostic factors in penetrating ocular injuries.
Am J Ophthalmol 1984; 98: 467–472.
13. Hatton MP, Thakkar MM, Ray S. Orbital and adnexal trauma associated with open globe injuries. Ophthalmol Plastic Reconstr Surg 2002; 18: 458–461.
14. Barr CC. Prognostic fac-tors in corneoscleral lacera-tions. Arch Ophthalmol 1983; 101: 919–924.
15. de Juan E, Sternberg P, Mi-chels RG. Penetrating ocular injuries: types of injuries and visual results. Ophthalmology 1983; 90: 1318–1322.
16. Martin DF, Meredith TA, Topping TM. Perforat-ing (through-and-through) injuries of the globe: surgi-cal results with vitrectomy. Arch Ophthalmol 1991; 109: 951–956.
17. de Bustros S, Michels RG, Glaser, BM. Evolving concepts in the management of posterior segment penetrat-ing ocular injuries. Retina 1990;1:72-75.
18. Koo L, Kapadia MK, Singh RP. Gender differences in etiology and outcome of open globe injuries, J Trauma 2005;59:175–178.
19. Adhikary HP, Taylor P, Fitzmaurice DJ. Prognosis of perforating eye injury. Br J Ophthalmol 1976;60:737–739.
20. Cinotti AA, Maltzman BA. Prognosis and treatment of perforating ocular inju-ries. The John Luhr memo-rial lecture. Ophthalmic Surg 1975;6:54–61.
21. Esmaeli E, Elner SG, Schork MA, Elner VM, Visual outcome and ocular survival after penetrating trauma. A clinicopathologic study. Oph-thalmology 1995;102:393–400.
22. Benson WE, Machemer R, Severe perforating inju-ries treated with pars plana vitrectomy. Am J Ophthalmol 1976;81:728–732.
23. Liggett PE, Gauderman WJ, Moreira CM. Pars plana
vitrectomy for acute retinal detachment in penetrating ocular injuries. Arch Ophthal-mol 1990;108: 1724–1728.
24. Mieler WF, Mittra RA. The role and timing of pars plana vitrectomy in penetrating ocular trauma [editorial].Arch Ophthalmol 1997;115:191–1192.
25. Thompson JT, Parver LM, Enger CL. Infectious en-dophthalmitis after penetrating injuries with retained intraoc-ular foreign bodies. National Eye Trauma System. Ophthal-mology 1993;100:1468–1474.
26. Coleman DJ. Early vitrec-tomy in the management of the severely traumatized eye. Am J Ophthalmol 1982;93:543–551.
27. Coleman DJ. Pars plana vitrectomy. The role of vitrec-tomy in traumatic vitreopathy. Trans Am Acad Ophthalmol Otolaryngol 1976;81:406–413.
28. Coles WH, Haik GM. Vit-rectomy in intraocular trauma. Its rationale and its indications and limitations. Arch Oph-thalmol 1972;87:621–628.
29. de Juan E, Sternberg P Jr, Michels RG. Timing of vitrectomy after penetrating ocular injuries. Ophthalmol-ogy 1984;91:1072–1074.
30. Faulborn J, Atkinson A, Olivier D. Primary vitrectomy as a preventive surgical pro-cedure in the treatment of se-verely injured eyes. Br J Oph-thalmol 1977;61:202–208.
31. Conway BP, Michels RG. Vitrectomy techniques in the management of selected pen-etrating ocular injuries. Oph-thalmology 1978;85,560–583.
32. Gregor Z, Ryan SJ. Com-plete and core vitrectomies in the treatment of experimental posterior penetrating eye in-jury in the rhesus monkey. II. Histologic features. Arch Oph-thalmol 1983;101:446–450.
33. Gregor Z, Ryan SJ. Com-plete and core vitrectomies in the treatment of experimental posterior penetrating eye in-jury in the rhesus monkey. I.
Histologic features. Arch Oph-thalmol 1983;101:441–445.
34. Ramsay RC, Cantrill HL, Knobloch WH. Vitrectomy for double penetrating ocular injuries. Am J Ophthalmol 1985;100;586–589.
35. Ryan SJ, Allen AW. Pars plana vitrectomy in ocular trauma. Am J Ophthalmol 1979;88:483–491.
36. Alfaro DV, Tran VT, Ru-nyan T. Vitrectomy for perfo-rating eye injuries from shot-gun pellets. Am J Ophthalmol 1992;114:81–85.
37. Cupples HP, Whitmore PV, Wertz FD, Mazur DO. Ocular trauma treated by vitreous sur-gery. Retina 1983;3:103–107.
38. Han DP, Mieler WF, Schwartz DM, Abrams GW. Management of traumatic hemorrhagic retinal detach-ment with pars plana vit-rectomy. Arch Ophthalmol 1990;108:1281–1286.
39. Hutton WL, Snyder WB, Vaiser A. Vitrectomy in the treatment of ocular perforat-ing injuries. Am J Ophthalmol 1976;81:733–739.
40. Meredith TA, Gordon PA. Pars plana vitrectomy for severe penetrating injury with posterior segment in-volvement. Am J Ophthalmol 1987;103:549–554.
41. Hermsen V. Vitrectomy in severe ocular trauma. Oph-thalmologica 1984,189:86–92.
42. Vatne HO, Syrdalen P. Vit-rectomy in double penetrating eye injuries. Acta Ophthalmol (Copenh) 1985;63:552–556.
43. Cleary PE, Ryan SJ. Vit-rectomy in penetrating eye injury. Results of a controlled trial of vitrectomy in an ex-perimental posterior penetrat-ing eye injury in the rhesus monkey. Arch Ophthalmol 1981;99:287–292.
44. Zhang Y, Zhang MN, Ji-ang CH, Yao Y, Zhang K. En-dophthalmitis following open globe injury. Br J Ophthalmol 2010;94:111-4.
45. Larque-Daza AB, Peralta-Calvo J, Lopez-Andrade J. Epidemiology of open-globe trauma in the southeast of Spain. Eur J Ophthalmol 2010;20:578-83.
46. Onakpoya OH, Adeoye A, Adeoti CO, Ajite K. Epidemi-ology of ocular trauma among the elderly in a developing country. Ophthalmic Epide-miol 2010;17:315-20.
47. Mansouri MR, Hosseini M, Mohebi M, Alipour F, Mehrdad R. Work-related eye injury: the main cause of ocu-lar trauma in Iran. Eur J Oph-thalmol 2009;20:770-775. [Epub ahead of print]
48. Warrasak S, Euswas A, Hongsakorn S. Posterior seg-ment trauma: types of injuries, result of vitreo-retinal surgery and prophylactic broad encir-cling scleral buckle. J Med Assoc Thai 2005;88:1916-30.
49. Rao LG, Ninan A, Rao KA. Descriptive study on ocu-lar survival, visual outcome and prognostic factors in open globe injuries. Indian J Oph-thalmol 2010; 58:321–323.

Junio 2011
PAN-AMERICA 45PAN-AMERICA
Mário Junqueira Nóbrega, MD1,2,3
1 Sadalla Amin Ghanem Eye Hospital, Joinville (SC), Brazil2 University of Joinville, Joinville (SC), Brazil3 Pan-American Association of Ophthalmology (PAAO), Brazilian Delegate 2009-2011
Correspondence:
Rua Abdon Batista, 146Joinville, SC Brazil 89201-010Email: [email protected]
RESUMO
A endoftalmite pós-operatória é uma infecção in-traocular grave geralmente associada à cirurgia de catarata. Suas causas mais comuns são bactérias gram-positivas e gram-negativas, bactérias anae-róbias e fungos. Nos últimos anos, os resultados do tratamento das endoftalmites melhoraram mas a sua incidência ainda tem aumentado, apesar da adoção de importantes medidas preventivas pré, intra e pós-operatórias. Geralmente, o diagnóstico é clínico mas a avaliação laboratorial de amostras do humor vítreo é essencial para o isolamento do agente causal e para testes de sensibilidade antibiótica. A injeção intravítrea de antibióticos é a principal forma de tratamento e os corticóides também devem ser usados para ajudar a reduzir a inflamação intraocular. A vitrectomia via pars plana também é utilizada no tratamento da endoftalmite pós-operatória, principalmente se a visão é muito baixa ou se não há boa resposta com a terapia intravítrea inicial. O desenvolvimento futuro de novas formas de diagnóstico e tratamento além da observação rigorosa das medidas profiláticas são fundamentais para mel-horar os resultados funcionais e diminuir a incidência desta grave infecção.
ABSTRACT
Postoperative endophthalmitis is a serious and sight-threatening intraocular infection most frequently associated with cataract surgery. The main causes of the infection are gram-positive and gram-negative bacteria, anaerobic bacteria and fungi. Lately, results of therapy for endophthalmitis have improved but its incidence is still increasing despite the adoption of important pre, intra and postoperative preventive measures. Diagno-sis is usually based on clinical findings but laboratory work-up of vitreous specimens is essential for isolation of infecting organisms and antibiotic sensitivity tests.
Intravitreal injection of antibiotics is the mainstay of treatment and steroids must also be used to help re-ducing intraocular inflammation. Pars plana vitrectomy is frequently performed for treatment of postoperative endophthalmitis, especially if vision is severely affected or if there is not a favorable response after initiation of intravitreal therapy. Future development of diagnostic and therapeutic models and rigorous observation of prophylactic standards are critical to optimize functio-nal outcomes and to decrease the incidence of this se-vere infection.
INTRODUCTION
Postoperative endophthalmitis is a serious and sight-threatening intraocular infection most frequently associated with cataract surgery1. Progressive vitritis is the hallmark of the disease that requires prompt diagno-sis and therapy to optimize visual outcome.
Although some important measures have been taken for prevention of endophthalmitis such as immediate preoperative use of povidone-iodine solution for prepa-ration of the conjunctiva, its incidence following cataract surgery have increased over the past years, possibly due to a greater use of clear corneal incisions2,3.
Other predisposing factors that may enhance the risk for developing endophthalmitis are preoperative eviden-ce of chronic blepharitis, conjunctivitis, lacrimal duct obstruction, ocular prosthesis in the fellow orbit, dia-betes mellitus, immunosuppression and intraoperative complications such as posterior capsular tear, vitreous loss and vitreous incarceration in the wound4-8.
Cataract extraction is the most frequent intraocular surgery and approximately 90% of postoperative endo-phthalmitis occur following the surgery; the rate of this complication has ranged from 0.08% to 0.68%9-14.
Diagnosis and Management ofPostoperative Endophthalmitis

REVIEW
46 PAN-AMERICA
Other ocular surgeries can cause endophthalmitis: secondary intraocular lens placement carries the highest risk (0.2-0.37%) while pars plana vitrectomy (PPV) carries the lowest one (0.03-0.08%) 12,15-6.
Some studies show that penetrating keratoplasty, trabeculectomy and glaucoma drainage device implantation have an increased chance for developing endophthal-mitis17-9. Furthermore, intraoperative use of antifibrotic agents seems to predispose to a conjunctival filtering bleb-related endophthalmitis that usually occurs months to years after glaucoma surgery 20-4.
Up to the present days, it has not been observed significant difference in the inci-dence of endophthalmitis between small-gauge (25-gauge and 23-gauge) pars plana vitrectomy (PPV) and 20-gauge PPV 16,25-6.
Also a rising concern for the development of endophthalmitis are intravitreal in-jections, a form of delivering drugs for treatment of several retinal diseases that has progressively been used in the last years. The risk may vary, according to a specific medication or clinical setting, from 0.1% to 0.6% per injection27-31; it seems that intravitreal triamcinolone acetonide injection has a higher risk of causing intraocular infection, probably due to its local immunosuppressive effect 27.
Figure 1 – Acute endophthalmitis six days after phacoemulsifi cation showing a dense hypopyon (A) and one day after pars plana vitrectomy and intravitreal injection of vancomycin and ceftazidime (B).
A
B
ACUTE POSTOPERATIVE ENDOPHTHALMITIS
It is the most common type of endophthalmitis. It occurs days after ocular surgery and it usually mani-fests as a rapidly progressive vision loss associated with red eye, pain, lid swelling and ocular dischar-ge. Slit-lamp examination discloses anterior chamber cells and fibrin, hypopyon and vitreous cells and dense opacities (Figure 1). Its main causative organisms are gram-positive bacteria like Staphylococcus epidermi-dis, Staphylococcus aureus and Streptococcus spe-cies (except Streptococcus pneumoniae). Although gram-negative bacteria are less common, they tend to cause more severe cases of endophthalmitis, with hig-her risk of irreversible vision loss32-3. Some important noninfectious causes of postoperative inflammation must be differentiated such as retained lens particles inside the eye, other forms of uveitis and an intense and early postoperative inflammation due to penetra-tion of toxic substances in the anterior chamber during or after the surgery (toxic anterior segment syndrome – TASS)34-5.
CHRONIC POSTOPERATIVE ENDOPHTHALMITIS
This is a delayed-onset postoperative endophthal-mitis that has been increasingly recognized. It usually manifests 4 to 8 weeks after the surgery as a low-grade indolent inflammation in the anterior chamber, without hypopyon, associated with a white plaque on the lens posterior capsule and a moderate vitreous cellular reaction. Ocular pain or discomfort may not occur. Ini-tially, it responds well to topical corticosteroid therapy but inflammation recurs after steroid taper (Figure 2). Its main causative agents are anaerobic gram-positive bacteria Propionibacterium acnes, nonvirulent forms of Staphylococcus epidermidis and fungi (Candida parap-silosis). Differential diagnosis of delayed-onset endo-phthalmitis include persistent postoperative inflamma-tion, retinal detachment or preexisting uveitis; rarely, sympathetic ophthalmia may be present after surgery to one eye36-7.
FILTERING BLEB-ASSOCIATED ENDOPHTHALMITIS
An acute endophthalmitis may follow a glaucoma filtering surgery due to penetration of microrganisms inside the eye through an avascular and thin bleb. Cli-nical characteristics are the same as those observed in early acute postoperative endophthalmitis but the infection often occurs months to years after the surgery and shows a purulent conjunctival bleb (“blebitis”) (Figure 3). Intraoperative use of antifibrotic agents, such as mitomycin-C, an inferior location to the bleb

Junio 2011
PAN-AMERICA 47PAN-AMERICA
Figure 2 – Chronic endophthalmitis seven months after phacoemulsifi cation and Ahmed glaucoma valve implant (A). There was also a severe cystoid macular edema (B) that disappeared after pars plana vitrectomy, capsulectomy, removal of intraocular lens and Ahmed implant and intravitreal injection of antibiotics (C).
and postoperative laser suture lysis, needling and au-tologous blood injection may increase the likelihood of subsequent infection20-4, 38-9. The use of glaucoma drainage devices may also increase the risk for deve-lopment of endophthalmitis39. As the most common causative organisms found in these cases are more virulent, like Streptococcus and gram-negative spe-cies, visual outcomes are usually poorer than those observed in patients with early-onset postoperative endophthalmitis23.
DIAGNOSIS
In general, diagnosis of postoperative endophthal-mitis is based on clinical findings. Any operated eye that develops inflammation out of proportion to the surgical trauma or has a more extended clinical course than frequently observed is suspected as having intrao-cular infection. In addition, a marked inflammation in an eye with a previous glaucoma surgery showing ble-bitis, has a filtering bleb-related endophthalmitis until proven otherwise. Evidence of retinal vasculitis may be an early sign of bacterial postoperative endophthalmitis and must be investigated even if there are no other sug-gestive clinical features40-1.
If opaque media does not permit ophthalmos-copy, B-scan ultrasound may give important details concerning vitritis and anatomical configuration of retina and choroid.
Laboratory work-up is mandatory whenever endo-phthalmitis is suspected. Vitreous samples are obtained for smears (Gram and Giemsa stains), cultures (blood, chocolate, Sabouraud, thioglycolate) and sensitivity tests. Intravitreal antibiotics must be injected after vi-treous tap and should not be delayed while awaiting microbiology results. If clinical characteristics indica-te chronic postoperative endophthalmitis, additional anaerobic cultures of vitreous must be performed to isolate Propionibacterium acnes. Lately, polymerase chain reaction (PCR) has been suggested to improve sensitivity and rapidity for bacterial endophthalmitis diagnosis42-3.
TREATMENT
Intravitreal injection of antibiotics is the mainstay of treatment of postoperative endophthalmitis. If vision is light perception or worse, vitrectomy is indicated and intravitreal antibiotics are injected at the end of the sur-gery. If vision is better than light perception, vitrectomy is not usually necessary32.
The most common intravitreal antibiotics injected to cover a wide-spectrum of gram-positive and gram-negative bacteria are vancomycin (1.0 mg/0.1 cc) and ceftazidime (2.25 mg/0.1 cc). In ß-lactam sensitive pa-tients, amikacin (400 μg/0.1 cc) is used instead of ce-
A
B
C

REVIEW
48 PAN-AMERICA
ftazidime. If there is a severe intraocular inflammation, intravitreal steroids (e.g., dexametasone 400 μg/0.1 cc) may be also injected. In cases of suspected fungal en-dophthalmitis, intravitreal amphotericin B (5-10 μg) or voriconazole (100 μg) are indicated.
Albeit topical and subconjunctival antibiotics don’t penetrate the vitreous as well as they penetrate the anterior chamber and have not been investigated in a prospective manner, they are often used as adjuvants to intravitreal delivery44-9. The topical use of the fourth-ge-neration fluoroquinolones Gatifloxacin or Moxifloxacin q3h is the main indication. If endophthalmitis occurs in the setting of anterior pathology, one must consider employing Vancomycin (topical 50 mg/mL q1h; sub-conjunctival 25 mg) plus ceftazidime (topical 50 mg/mL q1h; subconjunctival 100 mg) or amikacin (topical 20 mg/mL q1h; subconjunctival 40 mg). Moreover, intensive topical steroids (e.g., prednisolone acetate 1% q1h) and atropine 1% q6-8h are added to antibiotic
therapy. For intraocular fungal infections, topical am-photericin B (0.15-0.5% q1-2h) or voriconazole (1-2% q1- 2h) are used besides intravitreal injections.
Systemic antibiotics are no longer considered for primary treatment of postoperative endophthalmitis. The Endophthalmitis Vitrectomy Study (EVS) showed that there was no difference in visual acuity or media clarity with or without intravenous antibiotics when given in addition to intravitreal antibiotics32. Otherwise, systemic steroids are important adjuvants to reduce intraocular inflammation and must be started at 12 to 24 hours after initiation of intravitreal therapy (e.g., prednisone 60 mg p.o. each morning).
Clinical monitoring is essential and has to be done every 12 hours for the first 3 days. The majority of cases respond well and signs and symptoms begin improving 24 to 48 hours after intravitreal injection of antibiotics. If infection doesn’t stabilize or improve at 36 to 60 hours following the first injection, reinjection is recommended. At this time, culture and sensitivity results are often available and show if intravitreal anti-biotics need to be changed.
Pars plana vitrectomy (PPV) is frequently indicated for postoperative endophthalmitis, especially if vision is severely affected or if the patient doesn’t respond well at 48 to 60 hours after initiation of intravitreal therapy. In cases of chronic endophthalmitis secondary to cataract surgery, PPV is also often performed associated with re-moval of intraocular lens, capsulectomy and intravitreal injection of broad-spectrum antibiotics.
CONCLUSIONS
Postoperative endophthalmitis is a serious and po-tential blinding disease that requires early diagnosis and treatment. Lately, results of therapy for endophthal-mitis have improved but its incidence is still increasing. Probably, a higher number of surgeries such as clear cornea phacoemulsification, secondary intraocular lens placement, filtering procedures with the use of antifibro-tic agents or glaucoma drainage devices, small-gauge PPV and intravitreal injections have been responsible for the elevated rates of intraocular infection. Besides future development of diagnostic methods, to allow immediate identification of infecting organisms, and of antibiotics and delivery systems, with better thera-peutic ratios for intraocular infection and less toxicity, all known prophylactic measures are critical and must be continuously kept in mind by eye healthcare profes-sionals to provide better outcomes and to decrease the incidence of this devastating complication.
Figure 3 – Filtering surgery-related endophthalmitis three years after trabeculectomy showing blebitis and hypopyon (A). Although infection was eliminated with pars plana vitrectomy and intravitreal injection of antibiotics, functional outcome was devastating (no light perception and severe hypotony) (B).
A
B

Junio 2011
PAN-AMERICA 49PAN-AMERICA
REFERENCES
1. Verbraeken H. Treatment of postoperative endophthal-mitis. Ophthalmologica. 1995;209(3):165–171.
2. Cooper BA, Holekamp NM, Bohigian G, Thompson PA. Case-control study of endophthalmitis after cataract surgery comparing scleral tunnel and clear cor-neal wounds. Am J Ophthalmol. 2003;136(2):300–305.
3. Nagaki Y, Hayasaka S, Kadoi C, Matsumoto M, Yanagisawa S, Watanabe K, Watanabe K, Haya-saka Y, Ikeda N, Sato S, Kataoka Y, Togashi M, Abe T. Bacterial endophthalmitis after small-in-cision cataract surgery. effect of incision placement and intraoc-ular lens type. J Cataract Refract Surg. 2003;29(1):20–26.
4. Dortzbach RK, Woog JJ. Choice of procedure. Enucle-ation, evisceration, or prosthetic fi tting over globes. Ophthalmol-ogy. 1985;92(9):1249–1255.
5. Lopez PF, Beldavs RA, al-Ghamdi S, Wilson LA, Wojno TH, Sternberg P Jr, Aaberg TM, Lambert HM. Pneumococcal endophthalmitis associated with nasolacrimal obstruction. Am J Ophthalmol. 1993;116(1):56–62.
6. Miño de Kaspar H, Shriver EM, Nguyen EV, Egbert PR, Singh K, Blumenkranz MS, Ta CN. Risk factors for anti-biotic-resistant conjunctival bacterial fl ora in patients un-dergoing intraocular surgery. Graefes Arch Clin Exp Ophthal-mol. 2003;241(9):730–733.
7. Lalitha P, Rajagopalan J, Prakash K, Ramasamy K, Prajna NV, Srinivasan M. Postcataract endophthalmitis in South India incidence and outcome. Oph-thalmology. 2005;112(11):1884-1889. Epub 2005 Sep 12.
8. Garcia-Sáenz MC, Arias-Puente A, Rodríguez-Caravaca G, Andrés Alba Y, Bañuelos Ba-ñuelos J. Endophthalmitis after cataract surgery: epidemiology, clinical features and antibiotic prophylaxis. Arch Soc Esp Of-talmol. 2010;85(8):263-267.
9. Javitt JC, Street DA, Tielsch JM, Wang Q, Kolb MM, Schien O, Sommer A, Bergner M, Stein-berg EP . National outcomes of cataract extraction. Retinal de-tachment and endophthalmitis after outpatient cataract surgery. Cataract Patient Outcomes Re-search Team. Ophthalmology. 1994;101(1):100–105.
10. Norregaard JC, Thoning H, Bernth-Petersen P, Andersen TF, Javitt JC, Anderson GF. Risk of endophthalmitis after cataract surgery: results from the Inter-national Cataract Surgery Out-
comes study. Br J Ophthalmol. 1997;81(2):102–106.
11. Somani S, Grinbaum A, Slomovic AR. Postoperative endophthalmitis: incidence, predisposing surgery, clinical course and outcome. Can J Oph-thalmol. 1997;32(5):303–310.
12. Aaberg TM Jr, Flynn HW Jr, Schiffman J, Newton J. Noso-comial acute-onset postopera-tive endophthalmitis survey. A 10-year review of incidence and outcomes. Ophthalmology. 1998;105(6):1004–1010.
13. Morlet N, Gatus B, Coroneo M. Patterns of peri-operative prophylaxis for cataract surgery: a survey of Australian ophthal-mologists. Aust N Z J Ophthal-mol. 1998;26(1):5–12.
14. Taban M, Behrens A, New-comb RL, Nobe MY, Saedi G, Sweet PM, McDonnell PJ,. Acute endophthalmitis following cata-ract surgery: a systematic review of the literature. Arch Ophthal-mol. 2005;123(5):613–620.
15. Eifrig CW, Flynn HW Jr, Scott IU, Newton J. Acute-onset postoperative endophthalmitis: review of incidence and vi-sual outcomes (1995-2001). Ophthalmic Surg Lasers. 2002;33(5):373–378.
16. Oshima Y, Kadonosono K, Yamaji H, Inoue M, Yoshida M, Kimura H, Ohii M, Shiraga F, Hamasaki T; Japan Microinci-sion Vitrectomy Surgery Study Group. Multicenter survey with a systematic overview of acute-onset endophthalmitis after transconjunctival microincision vitrectomy surgery. Am J Oph-thalmol. 2010;150(5):716-725.e1. Epub 2010 Aug.16.
17. Ciulla TA, Baker AS. En-dophthalmitis following glau-coma fi ltering surgery. Int Oph-thalmol Clin. 1996;36(3):87–96.
18. Al-Torbak AA, Al-Shahwan S, Al-Jadaan I, Al-Hommadi A, Edward DP. Endophthalmitis associated with the Ahmed glau-coma valve implant. Br J Oph-thalmol. 2005;89(4):454–458.
19. Hassan SS, Wilhelmus KR, Dahl P, Davis GC, Roberts RT, Ross KW, Varnum BH; Medical Review Subcommittee of the Eye Bank Association of America. Infectious disease risk factors of corneal graft donors. Arch Oph-thalmol. 2008;126(2):235–239.
20. Wolner B, Liebmann JM, Sassani JW, Ritch R, Speaker M, Marmor M. Late bleb-related endophthalmitis after trabeculectomy with adjunctive 5-fl uorouracil. Ophthalmology. 1991;98(7):1053–1060.
21. Greenfi eld DS, Suñer IJ,
Miller MP, Kangas TA, Palmberg PF, Flynn HW Jr. Endophthal-mitis after fi ltering surgery with mitomycin. Arch Ophthalmol. 1996;114(8):943–949.
22. Kangas TA, Greenfi eld DS, Flynn HW Jr, Parrish RK 2nd, Palmberg P. Delayed-onset endophthalmitis associ-ated with conjunctival fi lter-ing blebs. Ophthalmology. 1997;104(5):746–752.
23. Song A, Scott IU, Flynn HW Jr, Budenz DL. Delayed-onset bleb-associated endophthalmi-tis: Clinical features and visual acuity outcomes. Ophthalmol-ogy. 2002;109(5):985–991.
24. Sharan S, Trope GE, Chip-man M, Buys YM. Late-onset bleb infections: Prevalence and risk factors. Can J Ophthalmol. 2009;44(3):279–283.
25. Recchia FM, Scott IU, Brown GC, Brown MM, Ho AC, Ip MS. Small-gauge pars plana vitrectomy: a report by the American Academy of Oph-thalmology. Ophthalmology. 2010;117(9):1851–1857.
26. Bahrani HM, Fazelat AA, Thomas M, Hirose T, Kroll AJ, Lou PL, Ryan EA. Endophthal-mitis in the era of small gauge transconjunctival sutureless vitrectomy – meta analysis and review of literature. Semin Oph-thalmol. 2010;25(5-6):275-282.
27. Moshfeghi DM, Kaiser PK, Scott IU, Sears JE, Benz M, Sinesterra JP, Kaiser RS, Bakri SJ, Maturi RK, Belmont J, Beer PM, Murray TG, Quiroz-Mercado H, Mieler WF. Acute endophthalmitis following intra-vitreal triamcinolone acetonide injection. Am J Ophthalmol. 2003;136(5):791–796.
28. Gragoudas ES, Adamis AP, Cunningham ET Jr, Feinsod M, Guyer DR; VEGF Inhibition Study in Ocular Neovascular-ization Clinical Trial Group. Pegaptanib for neovascular age-related macular degeneration. N Engl J Med. 2004;351(27): 2805–2816.
29. Jager RD, Aiello LP, Patel SC, Cunningham ET Jr. Risks of intravitreous injection: a comprehensive review. Retina. 2004;24(5):676–698.
30. Heier JS, Antoszyk AN, Pavan PR, Leff SR, Rosenfeld PJ, Ciulla TA, Dreyer RF, Gen-tile RC, Sy JP, Hantsbarger G, Shams N. Ranibizumab for treat-ment of neovascular age-related macular degeneration: a phase I/II multicenter, controlled, mul-tidose study. Ophthalmology. 2006;113(4):633.e1–4. [Epub 2006 Feb 14].
31. Diago T, McCannel CA,
Bakri SJ, Pulido JS, Edwards AO, Pach JM. Infectious en-dophthalmitis after intravit-real injection of antiangiogenic agents. Retina. 2009;29(5):601-605.
32. Results of the Endophthalm-itis Vitrectomy Study. A random-ized trial of immediate vitrecto-my and of intravenous antibiotics for the treatment of postopera-tive bacterial endophthalmitis. Endophthalmitis Vitrectomy Study Group. Arch Ophthalmol. 1995;113(12):1479–1496.
33. Kernt M, Kampik A. En-dophthalmitis: pathogenesis, clinical presentation, manage-ment and perspectives. Clin Ophthalmol. 2010;4:121-135.
34. Werner L, Sher JH, Taylor JR, Mamalis N, Nash WA, Csor-das JE, Green G, Maziarz EP, Liu XM. Toxic anterior segment syndrome and possible associa-tion with ointment in the ante-rior chamber following cataract surgery. J Cataract Refract Surg. 2006;32(2):227–235.
35. Mamalis N, Edelhauser HF, Dawson DG, Chew J, LeBoyer RM, Werner L. Toxic anterior segment syndrome. J Cataract Refract Surg. 2006;32(2):324–333.
36. Fox GM, Jooneph BC, Flynn HW, Pfl ugfelder SC, Roussel TJ. Delayed-onset pseudophakic endophthalmitis. Am J Ophthal-mol. 1991;111(2):163-173.
37. Aldave AJ, Stein JD, De-ramo VA, Shah GK, Fischer DH, Maguire JI. Treatment strategies for postoperative Propionibacterium acnes en-dophthalmitis. Ophthalmology. 1999;106(12):2395-2401.
38. Higginbotham EJ, Stevens RK, Musch DC, Karp KO, Lich-ter PR, Bergstrom TJ, Skuta GL. Bleb-related endophthal-mitis after trabeculectomy with mitomycin C. Ophthalmology 1996;103(4):650–656.
39. Gedde SJ, Scott IU, Ta-bandeh H, Luu KK, Budenz DL, Greenfi eld DS, Flynn HW Jr. Late endophthalmitis as-sociated with glaucoma drain-age implants. Ophthalmology. 2001;108(7):1323-1327.
40. Packer AJ, Weingeist TA, Abrams GW. Retinal periphlebi-tis as an early sign of bacterial endophthalmitis. Am J Ophthal-mol. 1983;96(1):66–71.
41. Subbiah S, McAvoy CE, Best JL. Retinal vasculitis as an early sign of bacterial post-operative endophthalmitis. Eye (Lond). 2010;24(8):1410-1411.
42. Bispo PJ, Melo GB, Höfl ing-Lima AL, Pignatari AC. Detec-
tion and gram discrimination of bacterial pathogens from aque-ous and vitreous humor using real-time PCR assays. Invest Ophthalmol Vis Sci. 2010;Aug 11. (Epub ahead of print).
43. Sugita S, Shimizu N, Wa-tanabe K, Katayama M, Horie S, Ogawa M, Takase H, Sugamoto Y, Mochizuki M. Diagnosis of bacterial endophthalmitis by broad-range quantitative PCR. Br J Ophthalmol. 2010;Jul 31. [Epub ahead of print].
44. Solomon R, Donnenfeld ED, Perry HD, Snyder RW, Nedrud C, Stein J, Bloom A. Penetra-tion of topically applied gatifl ox-acin 0.3%, moxifl oxacin 0.5%, and ciprofl oxacin 0.3% into the aqueous humor. Ophthalmology. 2005;112(3):466-9.
45. Costello P, Bakri SJ, Beer PM, Singh RJ, Falk NS, Peters GB, Melendez JA. Vitreous pen-etration of topical moxifl oxacin and gatifl oxacin in humans. Retina. 2006;26(2):191-5
46. Iyer MN, Han DP, Yun HJ, Eastwood D, Kim JE, Con-nor TB, Wirostko WJ, Dev S. Subconjunctival antibiotics for acute postcataract extrac-tion endophthalmitis – is it necessary? Am J Ophthalmol. 2004;137(6):1120-1.
47. Roth DB, Flynn HW Jr. Antibiotic selection in the treat-ment of endophthalmitis: the sig-nifi cance of drug combinations and synergy. Surv Ophthalmol. 1997;41(5):395-401.
48. Kresloff MS, Castellarin AA, Zarbin MA. Endophthal-mitis. Surv Ophthalmol. 1998;43(3):193-224.
49. Lemley CA, Han DP. En-dophthalmitis: a review of current evaluation and man-agement. Retina. 2007; 27(6): 662–680.
50. Meredith TA. Vitrectomy for infectious endophthalmitis. In: Ryan SJ, Hinton DR, Schachat AP, Wilkinson CP. Retina. 4th edition. Philadelphia: Elsevier Inc., 2006, p.2255-2275.

CASE REPORT
50 PAN-AMERICA
Summary:
It is necessary to heighten the level of knowledge about glaucoma because of the real danger of blind-ness that it represents, which could minimize serious consequences.
Objective:
To identify the level of knowledge of patients with glaucoma about their illness.
Methods:
A descriptive cross-sectional study was undertaken on the Glaucoma Service of the Ophthalmological Cen-ter of the Dr. Salvador Allende University Hospital, bet-ween January and March of 2010. The cohort included 947 patients with primary open-angle glaucoma who came to the Service during this period, and the sample consisted of the first 100 patients who fulfilled the inclu-sion criteria (willingness to participate in the study and an appropriate level of communication to respond the survey). A survey of the National Eye Health Education Program 2020 Vision was employed (Bethesda, USA). The results were evaluated a based on responses to true or false questions. The percentage method was used for the calculation of the frequencies in each case.
Results:
Women (62.0%) and patients between 50 and 69 years of age (43.0%) predominated. The risk factor most commonly recognized was family history of the illness (94.0%) and the least commonly recognized were racial characteristics (21.0%). The asymptomatic character of the disease was clearly understood (93.0%), but there were incorrect answers on the increase of the intraocular pressure. 87.0% of those interviewed were certain that the illness could only be controlled, but only 9.0% knew visual recovery was not possible. 100.0% erroneously identified
Dra. Idalia Triana Casado1, Dra. Ceija Molina Cisneros2
1 Médico Especialista Segundo Grado de Oftalmología. Máster de Salud Pública1 Profesora Auxiliar de Oftalmología.2 Médico Especialista de Primer Grado de Medicina General Integral y Oftalmología.2 Centro Oftalmológico Hospital Universitario Dr. Salvador Allende, La Habana, Cuba.
Autora para la correspondencia:Dra. Idalia Triana CasadoCentro Oftalmológico, Hospital Universitario Dr. Salvador Allende.Dirección postal: Calzada del Cerro No. 1551 esquina Domínguez, Municipio Cerro, CP 10 400, Ciudad de La Habana, Cuba.Teléfono: 877 6358 (Centro Oftalmológico).Email: [email protected]
« Las autoras declaran que este trabajo no ha sido publicado ni está en vías de consideración para publicación en otra revista. Asimismo, transfi eren los derechos de propiedad del presente trabajo a la Revista Visión Pan-América. Las autoras no tienen interés comercial alguno ni han recibido apoyo económico »
Nivel de conocimientos de pacientes glaucomatosos sobre su enfermedadCentro Oftalmológico Hospital Universitario Dr. Salvador Allende
intraocular pressure as the only diagnostic indicator of the disease. 69.0% demonstrated a mid-level of knowledge about their illness, and 19.0% an appropriate level.
Conclusions:
In the patients evaluated, the mid-level of knowledge prevailed.Words key: perception, risk, glaucoma, knowledge, illness.
Resumen
Es imprescindible elevar el nivel de conocimientos sobre glaucoma por el peligro real de ceguera que representa, lo que podría minimizar sus graves consecuencias.
Objetivo:
Identificar el nivel de conocimientos de enfermos glaucomatosos sobre su enfermedad.
Métodos
Se realizó un estudio descriptivo y transversal en el Servicio de Glaucoma del Centro Oftalmológico del Hospital Universitario Dr. Salvador Allende, entre enero y marzo de 2010. El universo estuvo constituido por los 947 pacientes con glaucoma primario de ángulo abierto que acudieron al Servicio en el periodo y la muestra por los primeros 100 que cumplieron los criterios de inclusión (disposición de participar en el estudio y adecuado nivel de comunicación para responder la encuesta). Se apli-có una encuesta del National Eye Health Education Program 2020 Vision (Bethesda, USA). Los resultados fueron evaluados según el conocimiento demostrado por los pacientes de acuerdo con el tipo de respuesta (cierto o falso). Se utilizó el método porcentual para el cálculo de las frecuencias en cada caso.
Resultados
Predominaron las mujeres (62,0%) y los pacientes entre 50 y 69 años de edad (43,0%). El factor de riesgo más reconocido fue el antecedente familiar de la enfer-medad (94,0%) y las características raciales el menos (21,0%). Fue claramente iden-tificado el carácter asintomático de la enfermedad (93,0%), pero no hubo respuestas correctas sobre el aumento de la presión intraocular. El 87,0% de los encuestados consideró cierto que la enfermedad sólo puede ser controlada y el 9,0% conocía lo referente a la no recuperación visual. El 100,0% valoró erróneamente la presión intraocular como único proceder diagnóstico y el 76,0% correctamente la dilatación pupilar. El 69,0% demostró un nivel medio de conocimientos sobre su enfermedad y el 19,0% un nivel adecuado.

Junio 2011
PAN-AMERICA 51PAN-AMERICA
Conclusiones
En los pacientes evaluados, predominó el nivel me-dio de conocimientos.
Palabras clave: percepción, riesgo, glaucoma, co-nocimientos, enfermedad.
Introducción
El glaucoma primario de ángulo abierto (GPAA) es el tipo más frecuente de neuropatía glaucomatosa. Representa el 60% de todas las formas clínicas.1 Su etiología exacta se desconoce, pero existen factores de riesgo (FR) a tener en cuenta.
Entre los más importantes se encuentra la presión intraocular (PIO), cuya valoración actual se centra en su variabilidad y la posibilidad del nervio óptico de to-lerarla.1, los antecedentes familiares de la enfermedad que parecen aumentar el riesgo entre el 4 y el 16% si el individuo presenta antecedentes familiares de primer grado, la edad, el sexo sobre el que no hay acuerdo uná-nime, aunque parece ser más frecuente en hombres, la diabetes mellitus (DM) y la miopía y las características raciales, en cuanto a lo que existe casi unanimidad de que en las personas de piel no blanca la prevalencia de GPAA es mayor, la aparición más precoz y el curso de la enfermedad más grave.2,5
Estimados consideran que lo padecen entre el 2% y el 4% de la población adulta mayor de 40 años, lo que representa el 90% de todos los casos y que existirán entre 7 y 8 millones de personas con ceguera bilateral en los próximos 25-50 años.6-8
En el contexto geográfico de las Américas, se es-tima que en Estados Unidos aproximadamente dos mi-llones de personas padecen Glaucoma, de los que casi 900.000 tienen un defecto visual crónico significativo y prácticamente 70 000 están legalmente ciegos. En México y Argentina representan la segunda causa de ceguera legal.9,10 En Cuba no existen datos oficiales al respecto. Un estudio de prevalencia realizado en Las Tunas arrojó una incidencia de 1,97% para todos los grupos de edades.11
Desde 2008, el día 12 de marzo se celebra el Día Mundial de la enfermedad, una oportunidad para elevar el nivel de conciencia de la población sobre la enfermedad y realizar iniciativas para su detección precoz.12
El nivel de conocimientos sobre una enfermedad puede considerarse como una medida indirecta de per-cepción de riesgo, si se considera que mientras más conocimientos se posean sobre una enfermedad más elementos se tendrán sobre cómo evitar sus conse-cuencias. En el caso que nos ocupa, estos elementos se comportan en la práctica como condiciones que fa-vorecen una peor evolución hacia la ceguera.
Tabla 1. Frecuencia de pacientes glaucomatosos encuestados, según edad y sexo.
Sexo Total
EdadFemenino Masculino
No. %No. % No. %
18-29 años 3 4,83 2 5,26 5 5,0
30-39 años 7 11,2 7 18,4 14 14,0
40-49 años 10 16,1 9 23,6 19 19,0
50-59 años 11 17,7 10 26,3 21 21,0
60-69 años 16 25,8 6 15,7 22 22,0
70 y más 15 24,1 4 10,5 19 19,0
Total 62 62,0 38 38,0 100 100,0
Tabla 2. Resultados cuantitativos de la aplicación de la encuesta en pacientes glaucomatosos según conocimientos sobre factores de riesgo, síntomas y signos, evolución y procederes diagnósticos del glaucoma.
Variable% de respuestas
correctasRespuesta correcta
Características raciales 21,0 Cierto
Antecedentes familiares positivos
94,0 Cierto
Edad 83,0 Cierto
Dolor ocular 6,0 Falso
Aumento de la PIO 0,0 Falso
Asintomático 93,0 Cierto
Control de la enfermedad
87,0 Cierto
Recuperación visual 9,0 Falso
Medición de la PIO 0,0 Falso
Dilatación pupilar 76,0 Cierto
Tabla 3. Frecuencia de glaucomatosos encuestados según nivel de conocimientos sobre Glaucoma por puntaje obtenido.
Pacientes con respuestas
Características raciales Correctas
Antecedentes familiares positivos
No. %
Entre 9 y 10 (nivel adecuado)
19 19,0
Entre 5 y 8 (nivel medio)
69 69,0
Entre 0 y 4 (nivel bajo) 12 12,0
Por esta razón nos motivamos a realizar este trabajo con los pacientes glauco-matosos que se atienden en nuestro Servicio, con el objetivo de identificar el nivel de conocimientos de los mismos acerca de su enfermedad.
Métodos
Se realizó un estudio descriptivo y transversal en el Servicio de Glaucoma del Hospital Universitario Dr. Salvador Allende, en La Habana, Cuba, entre enero y marzo de 2010, en pacientes con diagnóstico de GPAA, acreditado para la atención oftal-mológica y la docencia de Medicina de pre y posgrado y en él se utiliza la tecnología

CASE REPORT
52 PAN-AMERICA
más moderna de que se dispone en el país para el se-guimiento de estos pacientes.
El universo del estudio estuvo constituido por los 947 pacientes glaucomatosos adultos que acudieron al Servicio en el periodo y la muestra por los primeros 100 de ellos que cumplieron los criterios de inclusión: dis-posición de participar en el estudio y adecuado nivel de comunicación que les permitiera responder la encuesta.
Se aplicó una encuesta internacional publicada por el National Eye Health Education Program 2020 Vision (Bethesda, USA) (Anexo 1),13 adaptada a las caracterís-ticas del tipo de pacientes y a los objetivos del estudio (criterio de expertos). A los pacientes se les presentó el cuestionario por las propias investigadoras, al cual debían responder cierto o falso, reservándose los in-vestigadores la evaluación de las respuestas.
Los resultados fueron analizados de acuerdo con el tipo de respuesta (cierto o falso) y se emplearon los criterios de la encuesta para evaluar el nivel de cono-cimientos según los puntajes obtenidos: entre 9 y 10 respuestas correctas, nivel adecuado de conocimien-tos, entre 8 y 5, medio y menos de 4, bajo.
Las variables analizadas fueron edad y sexo (como características muestrales), conocimiento sobre los FR, signos y síntomas, evolución y procederes diagnósticos y nivel global de conocimientos sobre la enfermedad. Se analizaron las frecuencias absolutas y relativas (por ciento) de los pacientes según sus respuestas.
Aunque se trata de un estudio donde no medió nin-guna intervención sobre los participantes, se obtuvo el consentimiento informado. El protocolo del estudio fue aprobado por el Comité de Ética del Hospital. Los pa-cientes fueron informados de los resultados y se realizó una labor educativa personalizada según los resultados.
ResultadosEntre los pacientes encuestados predominaron las
mujeres (62%) y aquellos entre 50 y 69 años (Tabla 1).
Con relación a los FR de padecer glaucoma, el más reconocido fue el antecedente familiar de la enferme-dad (el 94,0% respondió de forma acertada a la pregun-ta correspondiente de la encuesta), mientras que las características raciales resultó el menos identificado (sólo el 21,0% respondió acertadamente). (Tabla 2)
Como signos y síntomas de glaucoma, el carácter asintomático de la enfermedad fue claramente identifi-cado (93,0% de respuestas correctas). De forma con-tradictoria, sucedió con el aumento de la PIO (100,0% de respuestas incorrectas) y la presencia de dolor ocu-lar (6,0% de respuestas acertadas). (Tabla 2)
Con respecto a la evolución de la enfermedad, el 87,0% de los encuestados consideró cierto que la en-fermedad sólo puede ser controlada, lo contrario se ob-tuvo con relación a la recuperación visual (sólo el 9,0% respondió acertadamente). (Tabla 2)
Sobre los procederes diagnósticos, el 100,0% coincidió en una valoración erró-nea sobre la PIO como único examen necesario y el 76,0% valoró correctamente la importancia de la dilatación pupilar en el examen oftalmológico de un paciente con glaucoma. (Tabla 2)
De forma predominante, los pacientes de la serie demostraron un nivel medio de conocimientos sobre su enfermedad (69,0%), el 19,0% mostró un nivel adecuado y sólo el 12,0% bajo. En general, el 88,0% demostró un nivel aceptable de cono-cimientos, en cuanto a FR de padecer la enfermedad y a la posible evolución a la ceguera. (Tabla 3)
Discusión
Aunque dentro de los objetivos del estudio no se contempló el análisis del nivel de conocimientos por edad y sexo, el predominio en la serie del sexo femenino no coincide con la mayoría de los reportes que plantean que los hombres poseen tasas más altas de glaucoma y de progresión1,2, lo que puede estar en relación con el tamaño de la muestra y con la forma de selección de la misma (limitaciones del estudio), toda vez que resulta conocido que las mujeres demandan más asistencia médica que los hombres.
En la serie, los pacientes demostraron mayor nivel de conocimientos sobre la importancia de los antecedentes familiares de glaucoma y de la edad que en relación con las características raciales, lo que debe tenerse en cuenta por el altísimo grado de mestizaje de la población cubana y la importancia de este FR no sólo de desarrollo de glaucoma, sino también de progresión a la ceguera.14,15
Los estudios de intervención comunitaria utilizan la promoción y la prevención como elementos claves para proporcionar a la población las herramientas cognitivas que garanticen una mayor calidad en lo que a la salud se refiere.16 No existen datos pu-blicados acerca del conocimiento que tiene la población general y los enfermos sobre el glaucoma. Los estudios nacionales e internacionales, son escasos, por lo que los resultados de este estudio son inéditos y no pueden ser ampliamente comparados.
Un estudio realizado en Santiago de Cuba en el año 2008,16 encontró que sólo el 11,1% de ellos conocía los FR de esta enfermedad, cifra que mejoró al 98,9% des-pués de una intervención educativa. Nuestros resultados, sin mediar esta, se acercan más a la última cifra, excepto en lo que a características raciales, presencia de dolor ocular, aumento de la PIO y recuperación visual se refiere, lo que podría deberse al hecho de que en el momento del diagnóstico o cuando el paciente acude por primera vez a nuestro Servicio (si fue diagnosticado en otro lugar), se le explican a él y a los familiares, los aspectos más importantes con relación a esta enfermedad. Las carac-terísticas clínicas de la enfermedad resultaron bien conocidas, lo que no coincide con el estudio antes mencionado.17
Un estudio realizado en la India,18 muestra que la tasa de conocimiento de la en-fermedad es de 18,7%, baja en comparación con las de países desarrollados como el Reino Unido, donde aproximadamente el 50% de las personas con la enfermedad saben que la tienen.19 Si bien nuestro diseño no permite calcular esas tasas, los datos obtenidos ilustran las diferencias entre países de acuerdo con el nivel de desarrollo económico y socio-cultural. En nuestra pequeña serie y con las obvias diferencias de diseño, los resultados se acercan más a los de países desarrollados.
En la serie, la mayoría consideró que la visión perdida era recuperable con el control de la enfermedad, dato no referido en estudios precedentes.
El resultado acerca de los procederes diagnósticos para la detección de la enfer-medad, fue adecuado. Se reconoció la toma de la PIO como uno de los más impor-tantes y lo obtenido en cuanto a la dilatación pupilar, puede estar en relación con el falso concepto de que los glaucomatosos no deben dilatarse la pupila.
Una gran cantidad de organizaciones, iniciativas y programas trabajan para educar y concientizar a los individuos y gobiernos de todo el mundo sobre la enfermedad.

Junio 2011
PAN-AMERICA 53PAN-AMERICA
Ejemplos son el Día Mundial del Glaucoma, copatrocinado por la World Glaucoma Association y por la World Glaucoma Patient Association, Vision 2020, programa conjunto entre la World Health Organization y la International Agency for the Prevention of Blindness y All Eyes on Glaucoma, patrocinado por la transnacional Pfizer.20,21 En el último Congreso Mundial de Glaucoma se discutió respecto a la importancia y alcance de la educación de las personas con glaucoma, lo que ilustra la importancia del tema abordado en el presente trabajo.22
Si bien el enfoque educativo está dando pasos, son insuficientes aún, desde la perspectiva del valor intrínseco que reviste una adecuada conciencia de la enfermedad y su nivel de conocimiento por parte de pacientes y personas en riesgo de enfermar.
Este estudio fue una primera experiencia sobre el tema, en un grupo limitado de personas ya diagnosticadas y supuestamente más informadas que la población gene-ral, pero los resultados obtenidos pueden ser el punto de partida de futuras investiga-ciones con diseños más complejos y abarcadores, por lo que recomendamos diseñar
Haga esta prueba para ver cuánto sabe sobre glaucoma
Millones de estadounidenses corren el riesgo de perder la visión debido al Glaucoma, una de las principales causas de ceguera en los Estados Unidos. ¿Es usted uno de ellos? Si lo es, ¿sabe cómo reducir su riesgo de ceguera? Para determinar cuán-to sabe, responda a las siguientes preguntas: Cierto, falso o no está seguro:
1. El Glaucoma es más común en los afroamericanos que en los blancos.
2. El Glaucoma tiende a ocurrir en miem-bros de la misma familia.
3. Una persona puede tener Glaucoma y no saberlo.
4. Las personas mayores de 60 años tienen más probabilidad de desarrollar el Glaucoma.
5. El dolor en los ojos es a menudo un síntoma de Glaucoma.
6. Se puede controlar el Glaucoma.
7. El Glaucoma es causado por el aumento de la presión en el ojo.
8. Se puede recuperar la visión perdida a causa del Glaucoma.
9. Un examen completo de Glaucoma
consiste únicamente en medir la presión del ojo.
10. Las personas que corren el riesgo de tener Glaucoma deben hacerse un examen de los ojos con dilatación de las pupilas.
Lea las respuestas al dorso para ver cuánto sabe sobre Glaucoma. Si obtuvo entre 9 y 10 respuestas correctas, felicitaciones. Tiene un nivel adecuado de conocimientos sobre su enfermedad. Si tuvo entre 8 y 5, repase las respuestas y asesórese con su médico. Si las respuestas correctas fueron de 4 o menos, su nivel es muy pobre y debe ser asesorado inmediatamente.
Respuestas:1. Cierto. En un estudio financiado por
el Instituto Nacional del Ojo (NEI, por sus siglas en Inglés), investigadores de la Universidad de John Hopkins informaron que es de tres a cuatro veces más probable que el Glaucoma ocurra en afroamericanos que en blancos. Además, es seis veces más probable que el Glaucoma cause ceguera en los afroamericanos que en los blancos.
2. Cierto. Aunque el Glaucoma tiende a ocurrir en miembros de la misma familia, no se ha establecido aún una base hereditaria. Si alguien de su familia inmediata lo padece,
usted debe hacerse un examen completo de los ojos con dilatación de las pupilas cada uno o dos años.
3. Cierto. Generalmente, en las primeras etapas del Glaucoma de Ángulo Abierto, la forma más común de la enfermedad, no aparecen señales de aviso. Sin embargo, a medida que la enfermedad avanza, es posible que la persona note que va perdiendo lentamente su visión lateral.
4. Cierto. Todas las personas de más de 60 años corren mayor riesgo de tener Glau-coma, especialmente las de descendencia mexicana. Otros grupos con mayor riesgo de padecerlo son los afroamericanos de más de 40 años y las personas con familiares que han tenido Glaucoma. Los niños y los bebés también pueden desarrollarlo.
5. Falso. Las personas con Glaucoma generalmente no sienten dolor a causa de la enfermedad.
6. Cierto. Aunque el Glaucoma no tiene cura, generalmente se puede controlar con gotas para los ojos, píldoras, cirugía convencional o cirugía láser. Algunas veces, los médicos recomiendan una combinación de cirugía y medicamentos.
7. Falso. El aumento de la presión dentro del ojo significa que usted corre mayor
riesgo de tener Glaucoma, pero no significa que tenga la enfermedad. Una persona tiene Glaucoma solamente si el nervio óptico está dañado. Si tiene un aumento de presión en el ojo pero no hay daño al nervio óptico, usted no tiene Glaucoma. Siga las recomen-daciones de su médico.
8. Falso. La pérdida de visión por causa del Glaucoma es permanente. Sin embargo, con una detección temprana y un tratamiento oportuno, se puede retrasar o detener el avance de la pérdida de visión. También se puede reducir el riesgo de ceguera.
9. Falso. Aunque es una parte importante del examen de los ojos, medir la presión del ojo por tonometría no es suficiente por sí sola para detectar el Glaucoma. El Glaucoma se detecta más a menudo durante un examen de los ojos con dilatación de las pupilas. lo que permite al médico ver mejor el interior del ojo para determinar si hay signos de Glaucoma. Cuando esté indicado, también debe hacerse un examen del campo visual.
10. Cierto. El examen de los ojos con dila-tación de las pupilas es la mejor manera de diagnosticar el Glaucoma. Las personas que corren mayor riesgo de tener la enfermedad deben ser examinados cada uno o dos años.
REFERENCIAS1. Kanski JJ. Glaucoma. En: Oftal-mología Clínica 5ta ed. Madrid, Har-court, 2005:196-7.
2. Hommer A. Factores de riesgo del glaucoma primario de ángulo abierto (página Web en Internet) 2007. [Citado 2008, enero 20]. Disponible en: http://www.glaucomaworld.net/spagnolo/018/s018a04.html.
3. Boyd L, Benjamín MD, Samuel MD. Últimas innovaciones en los Glauco-mas. Etiología, diagnóstico y tratamien-to. Panamá, Highlights of Ophthalmol-ogy (CD ROM), 2005:56-80.
4. García J. Introducción. Tiempos Médicos. 2005; 615:11-22.
5. Wenreb RN, Khaw PT. Primary Open Glaucoma. Lancet, 2004; 363:1711-20.
6. Glaucoma, causa más frecuente de ceguera (página Web en Internet) 2004.
[Citado 2008, enero 20]. Disponible en: [email protected].
7. Shaarawy T, Flammer J, Haefl iger IO. Reducing intraocular pressure: Is sur-gery better than drugs? En: Shaarawy T, Mermound A. Atlas of glaucoma surgery. New Delhi, Jaypee Brothers Medical Publishers, 2006:1-10.
8. Peris Martínez C, Menezo Rozalen JL. Tonometría y tonografía. En: Mene-zo Rozalen JL, España Gregori E. Téc-nicas exploratorias en Oftalmología. Barcelona, Espaxs Publicaciones Médicas, 2006:263-80.
9. PAC Oftalmología (página Web en Internet) 2004. [Citado 2007, septi-embre 16]. Disponible en: http://www.drscope.com/privados/pac/generales/oftalmología/glaucoma.html.
10. Brechtel Bindel M. Glaucoma Pri-
mario de Ángulo Abierto. Rev Hosp Dr. Gea González, 2003; 4(3):61-8.
11. Labrada Rodríguez YH, Hor-nia Palacios MM, González Hess L, Rodríguez Suárez J. Glaucoma Prima-rio de Ángulo Abierto. Un problema de salud en el municipio Las Tunas. Rev Cub Oftalmol, 2006;19(1).
12. Lupinacci. A, Israel. M. Día Mun-dial del Glaucoma 2010 (página Web en Internet) 2010. [Citado 2010, mayo 12]. Disponible en: www.hospitalaus-tral.edu.ar.
13. Haga esta prueba para ver cuánto sabe sobre Glaucoma (página Web en Internet) [Citado 2010, enero 5]. Di-sponible en: www.nei.nih.gov/health/espanol.
14. Márquez M, Rojas F, Gutiérrez JA, López C. Salud para todos sí es posible
1ª ed. La Habana: Sociedad Cubana de Salud Pública. Sección de Medicina Social, 2005: 42-86.
15. Racette L, Wilson MR, Zangwill LM. Primary open-angle glaucoma in blacks : A review. Surv Ophthalmol, 2003; 48:295-313.
16. Varma R, Ying-Lai M, Francis BA. Prevalence of open-angle glaucoma and ocular hypertension in latinos: The Angeles Latino Eye Study. Ophthalmol, 2004; 111:1439-48.
17. García E. Intervención comunitaria sobre Glaucoma Crónico Simple. Poli-clínico Frank País. Santiago de Cuba 2008. Rev Hab Cienc Med, 2009; 8(3).
18. George R, Vijaya L. First World Glaucoma Day, March 6, 2008: Tack-ling glaucoma challenges in India. In-
dian J Ophthalmol, 2008; 56(2):97-8.
19. Quigley HA, Broman AT. The num-ber of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol, 2006; 90(3):262-7.
20. Nota de prensa: Día Mundial del Glaucoma (página Web en Internet) 2010. [Citado 2010, mayo 18]. Di-sponible en: http://wgday.net/inner.php?pageid=1.
21. Programa Gratuito de Diagnóstico Inicial de Riesgo en Glaucoma (DIRG) (página Web en Internet) 2010. [Citado 2010, mayo 18]. Disponible en: http://www.wgday.net.
22. Taylor HR, Katala S, Muñoz B, Turner V. Increase in mortality asso-ciated with blindness in rural Africa. Bull WHO, 2004; 69(3):335-8.
e implementar en la práctica médico-social, estrategias educativas dirigidas al paciente glaucomatoso y a la población en riesgo, así como evaluar los resultados de las mismas, que a criterio de las autoras, redundarían en mayor prevención de la ceguera por esta causa, cuya única opción hasta el momento, es el diagnóstico pre-coz y el seguimiento adecuado de los enfermos.
Conclusiones
En el grupo de pacientes glaucomatosos encuesta-dos, el nivel de conocimiento sobre su enfermedad, en aspectos como FR, características clínicas, evolución y procederes diagnósticos resultó de nivel medio, por lo que se debe profundizar en esta arista de la conducta médica como una herramienta sanitaria más.

CLINICAL SCIENCES
54 PAN-AMERICA
Proptosis en el neonato
Abstract
Objective: The aim of this work is to consider the most frequent causes of proptosis in newborns and to descri-be its different diagnosis.
Methods: Proptosis newborn babies were evaluated. A complete ocular examination, which included neuro images, was made during a period of 18 months.
Results: Nine proptosic newborn babies, with 100% positive neuro images, get into our institution. The most common pathology was found the vascular mal-formation capilary. This fact made possible to apply the immediate and adequate therapeutic.
Conclusion: Proptosis in newborn babies is a rele-vant and important sign, and a oftalmologic emer-gency. Fast diagnosis and treatment avoid important visual consequences.
Resumen
Objetivo: Considerar las causas más frecuentes de prop-tosis en el neonato y sus diagnósticos diferenciales.
Métodos: Se evaluaron los recién nacidos ingresa-dos con proptosis, se realizó examen ocular completo que incluyó neuro-imágenes, durante el período de 18 meses.
Resultados: Ingresaron 9 neonatos con proptosis, con neuro-imágenes positivas en el 100%, posibilitando la terapéutica inmediata y adecuada.
Conclusión: La proptosis en el neonato es un signo de relevante importancia y una urgencia oftalmológica. El rápido diagnóstico y tratamiento evita importantes se-cuelas visuales.
Introducción
Los tumores primitivos de la órbita son los más frecuentes en la población pediátrica, representados sobre todo por los sarcomas orbitarios y secundaria-mente por los angiomatosos, nerviosos, congénitos y
seudotumores de la órbita. En neonatos, el rabdomio-sarcoma es sumamente infrecuente pasando a ser las malformaciones vasculares la patología más frecuente en este grupo etario.
El objetivo de esta presentación es considerar las causas más frecuentes de proptosis en el neonato y sus diagnósticos diferenciales.
Pacientes y Métodos
Se evaluaron los recién nacidos ingresados con proptosis al Servicio de Oftalmología del Hospital de Pe-diatría “Prof. Dr. Juan P. Garrahan” durante un período de 18 meses, desde marzo de 2007 a septiembre de 2008.
Se realizó examen ocular completo que incluyó ojo externo, función visual acorde a la edad (Fija, Fija y Sigue, Fija Sigue y Mantiene), fondo de ojo con of-talmología binocular indirecta, esquiascopia y se inter-consultó con los Servicios de Clínica Pediátrica, Der-matología, Neurología. Se practicó neuro-imágenes a todos los neonatos ingresados.
Resultados
Ingresaron al Servicio de Oftalmología durante el periodo de 18 meses, 9 neonatos con el signo de Proptosis. Los resultados se incluyen en la Tabla 1. La edad de consulta fue de 1 a 60 días, con una media de 35 días. La edad de aparición de la proptosis tiene una media de 20 días, con un rango de edad de 1 a 40 días. El 66,6% eran de sexo femenino y el 33,3% de sexo masculino. El diagnóstico se realizó combinando la clínica, con las imágenes y en 4 pacientes con biop-sia excisional, 4 presentaron diagnóstico de malforma-ción vascular capilar (44,4%), 2 malformación linfática (22,2%), 1 dermoide orbitario (11,1%), 1 neurinoma plexiforme en paciente con neurofibromatosis, 1 terato-ma. La terapéutica clínica con esteroides se realizó en 3 de los neonatos con angioma a dosis inmunosupresora por un período no menor de 2 meses y no mayor de 6 meses, y en 1 paciente se trató con Propranolol a dosis de 3 mg/día con un estricto control pediátrico y cardiológico en ambas terapéuticas. En los pacientes
Dra. Alejandra C. IuresciaEmail: [email protected]
Institución:
Hospital de Pediatría Juan P. GarrahanBuenos Aires, Argentina

Junio 2011
PAN-AMERICA 55PAN-AMERICA
con malformación linfática se tuvo conducta espectan-te, mientras que en aquellos con diagnóstico de quiste dermoide, neurinoma plexiforme y teratoma se realizó cirugía. El seguimiento fue de 24 meses en el 99.9% de los pacientes y solo el 11,1% a los 20 meses no continuó los controles.
Discusión
Un neonato con proptosis implica un estricto exa-men oftalmológico y clínico.
La causa más frecuente de exoftalmos en recién nacidos es la malformación vascular capilar6, como se demuestra en nuestro trabajo. Del resto de los diagnós-ticos a tener en cuenta el más importante es el sarcoma orbitario. En este grupo etario es infrecuente ésta pa-tología, ya que en la literatura hay dos casos reporta-dos, diagnosticados con biopsia y tratados, los cuales a pesar de su temprana terapéutica no presentaron una buena evolución1. El rabdomiosarcoma se manifiesta a la edad de 5 años, con un rango de 3 meses a 12 años. A pesar de la baja frecuencia del sarcoma en neonatos se debe tener en cuenta como diagnóstico diferencial, principalmente considerando el rápido empeoramiento del estado general del niño, se debe programar la biop-sia para comenzar con el tratamiento; del cual depende la vida del infante.2,3,4,5
La más frecuente patología neonatal que produce proptosis es la malformación vascular capilar, repre-senta al 5% de la patología orbitaria6, correspondien-do en nuestra casuística al 44,4 % de los neonatos. Es una proliferación de células capilares y endoteliales6 que pueden aparecer en el neonato o en el transcur-so de los primeros meses de vida, creciendo activa-mente hasta los 9 meses, más lentamente hasta los 12 meses, a partir del cual comienza el período de regresión. Es una patología benigna pero con un com-portamiento maligno debido a la edad de comienzo y a la localización.7 Cualquiera que sea su presentación clínica, los hemangiomas en el periodo neonatal y los primeros meses de la lactancia requieren una atención cuidadosa, debido a su patrón de crecimiento y la futura aparición de nuevas lesiones.
Las características clínicas y las imágenes llevan al diagnóstico y se debe comenzar el tratamiento ya que en la primera etapa de la enfermedad la proliferación es importante.
La terapéutica se realiza con esteroides a dosis inmunosupresora de 2 mg/kg/d y se desciende al co-menzar la mejoría de la proptosis en forma muy pau-latina8,9. A partir de 2008 hay una nueva alternativa de tratamiento con Propranolol a 3mg/dia.11 Hay varias teorías sobre el efecto terapéutico del propanolol en los hemangiomas las cuales incluyen: la vasoconstric-ción que se ve con el cambio de color junto con el
Malformación Vascular Capilar Tratamiento Corticoide
Malformación congénita: Teratoma

CLINICAL SCIENCES
56 PAN-AMERICA
ablandamiento del hemangioma; la disminución de expresión de genes del factor de crecimiento fibroblástico básico (VEGF) y el factor de crecimiento vascular endotelial (bFGF); e inicio de la apoptosis de las células de capilares endoteliales; sin embargo aún faltan estudios sobre el mecanismo de acción y la evolución de largo plazo con este tratamiento.11
La siguiente patología en frecuencia fue la malformación linfática, la cual se pre-sentó en dos de los neonatos. Es un tumor benigno pero de gran agresividad en la infancia, que se presenta en el 50-60% antes de los 5 años, muchas veces a través de la conjuntiva y los párpados se ve una tumoración azulada.12 Crecen lentamente y se presentan al nacimiento o en la niñez temprana, y a diferencia de los angiomas no se resuelven en forma espontánea. Es frecuente que sangren produciendo en esos momentos una gran proptosis, infrecuente en los recién nacidos, en forma de quistes azulados y oscuros que pueden permanecer mucho tiempo.13 Las hemorragias pue-den producirse con infecciones de la vía respiratoria ó con traumas produciendo un cuadro agudo similar al rabdomiosarcoma. Histopatologicamente se caracteriza por ser un tejido infiltrativo difuso, compuesto por canales lineales endoteliales indistin-guibles de los linfáticos; los folículos linfáticos tienen estromas fibrosos separados de los canales endoteliales y hemorragias intratumorales los cuales comúnmente se denominan quistes de chocolate.14
El tratamiento es quirúrgico, cuando es muy agresivo y/o afecta estructuras no-bles, principalmente el nervio óptico. La respuesta a la radioterapia y corticoides es incierta.15
El quiste dermoide es la patología benigna más frecuente en la órbita en la infan-cia16 En nuestra casuística correspondió solamente al 11%, ya que es congénita pero de crecimiento lento, usualmente con manifestación clínica tardía. Son formaciones quísticas a nivel de las suturas óseas, con restos de ectodermo (glándulas sebáceas, sudorípadas, folículos pilosos), y el interior del quiste esta lleno de secreciones. La terapéutica es la escisión quirúrgica cuando comprime tejidos vecinos o erosiona pared ósea.16,17,18
El teratoma es un raro tumor embrionario compuesto por los derivados de las tres capas embrionarias. Se presenta desde el nacimiento como una proptosis extrema, de rápido crecimiento, de tal manera que produce un estiramiento de la piel palpebral, pudiendo la órbita ensancharse al doble de su tamaño normal, con la subsecuente deformidad facial.19,20,21,22 Las imágenes muestran estructuras multiquísticas que no involucran al sistema nervioso central. El tratamiento quirúrgico es de urgencia para realizar el diagnóstico diferencial con el sarcoma orbitario. La cirugía es dificultosa, se debe tratar de preservar el globo ocular, a pesar de lo cual muchas veces necesita excenteración23,24 lo cual no ha sucedido en el paciente de ésta serie.
diagnostico ojo Edad días Biopsia tratamientoSeguimiento
meses.F S M
1 Angioma OD 20 No Corticoide 24 + - -
2 Linfangioma OI 24 No Espectante 24 + + +
3 Angioma OD 15 Si Corticoide 24 + + +
4 Dermoide OD 25 No Cirugía 24 + + -
5 Teratoma OI 10 Si Cirugía 24 - - -
6 Angioma OI 22 No Corticoide 24 + + -
7 Neurinoma OI 12 Si Cirugía 20 - - -
8 Linfangioma OD 27 Si Espectante 24 + - -
9 Angioma OD 18 no propranolol 24 + - -
Angioma: Malformación Vascular Capilar
Linfangioma: Malformación Vascular Linfática
Neurinoma: Neurinoma Plexiforme
Visión del ojo afectado
F: fi ja
S: sigue
M: mantiene

Junio 2011
PAN-AMERICA 57PAN-AMERICA
REFERENCIAS
1. Spahn B, Nenadov-Beck M. Orbital rhabdomyosarcoma: Clinicopathologic correlation, management and follow-up in two newborns.Orbit. 2001 Jun;20(2):149-156.
2. Crist WM, Anderson JR, Meza JL, Fryer C, Raney RB, Ruymann FB, BrenemanJ, Qual-man SJ, Wiener E, Wharam M, Lobe T, Webber B, Maurer HM, Donaldson SS. Intergroup rhab-domyosarcoma study-IV: results for patients with nonmetastatic disease. J Clin Oncol. 2001 Jun 15;19(12):3091-102.
3. Huh WW, Beverly Raney R. Orbital metastasis in patients with rhabdomyosarcoma: case series and review of the litera-ture. J Pediatr Hematol Oncol. 2006 Oct;28(10):684-7.
4. Shields CL, Shields JA, Ho-navar SG, Demirci H. Clinical spectrum of primary ophthalmic rhabdomyosarcoma. Ophthal-mology. 2001 Dec;108(12):2284-92.
5. Shields CL, Shields JA, Ho-navar SG, Demirci H. Primary ophthalmic rhabdomyosarcoma in 33 patients.Trans Am Oph-thalmol Soc. 2001;99:133-42; discussion 142-3.
6. Abry F, Kehrli P, Speeg-Schatz C. Hemangioma of the eyelids and orbit in children: therapeutic follow-up. J Fr Oph-talmol. 2007 Feb;30(2):170-6
7. Sterker I, Grafe G. Periocular hemangiomas in childhood--func-tional and esthetic results.Strabis-mus. 2004 Jun;12(2):103-10.
8. Delesalle F, Staumont D, Houmany MA, Breviere M, Piette F. Pulse methylpredni-solone therapy for threatening periocular haemangiomas of infancy. Acta Derm Venereol. 2006;86(5):429-32.
9. Schwartz SR, Blei F, Ceisler E, Steele M, Furlan L, Kodsi S. Risk factors for amblyopia in children with capillary heman-giomas of the eyelids and orbit. J AAPOS. 2006 Jun;10(3):262-8.
10. Kavanagh EC, Heran MK, Peleg A, Rootman J Imaging of the natural history of an orbital capillary hemangioma. Orbit 2006 Mar;25(1):69-72.
11. Leauté-Labréze Ch, Dumas RE, Hubiche T, Boralevi F. “Pro-panolol for severe hemangiomas of infancy”. N Engl J Med 2008; 358: 2649-2651.
12. Vachharajani A, Paes B. Orbital lymphangioma with non-contiguous cerebral arte-riovenous malformation, mani-festing with thrombocytopenia (Kasabach-Merritt syndrome) and intracerebral hemorrhage.Acta Paediatr. 2002;91(1):98-9.
13. Gunduz K, Demirel S, Yag-murlu B, Erden E. Correlation of surgical outcome with neu-roimaging fi ndings in periocular
lymphangiomas. Ophthalmol-ogy. 2006 Jul;113(7):1231.e1-8. Epub 2006 May 26.
14. Rizzardi E, Tagliaferro T, Snijders D, Bertuola F, Spolaore F, Simioni P, Maimone P, Pinello L, Mazzarolo M, Barbato A. D-dimer evaluation of hemorrhagic orbital lymphangioma. J Pediatr Ophthalmol Strabismus. 2010 May-Jun;47(3):174-7.
15. Muallem MS, Garzozi HJ. Conservative management of orbital lymphangioma.Pediatr Ophthalmol Strabismus. 2000 Jan-Feb;37(1):41-3.
16. Yen KG, Yen MT. Current trends in the surgical man-agement of orbital dermoid cysts among pediatric ophthal-mologists. J Pediatr Ophthal-mol Strabismus. 2006 Nov-Dec;43(6):337-40; quiz 363-4.
17. Ahuja R, Azar NF. Or-bital dermoids in children. Semin Ophthalmol. 2006 Jul-Sep;21(3):207-11.
18. Sherman RP, Rootman J, Lapointe JS. Orbital dermoids: clinical presentation and man-agement. Br J Ophthalmol. 1984 Sep;68(9):642-52.
19. Gnanaraj L, Skibell BC, Coret-Simon J, Halliday W, Forrest C, DeAngelis DD. Mas-sive congenital orbital teratoma. Ophthal Plast Reconstr Surg. 2005 Nov;21(6):445-
20. Sreenan C, Johnson R, Rus-sell L, Bhargava R, Osiovich H. Congenital orbital teratoma. Am J Perinatol. 1999;16(5):251-5.
21. Bilgic S, Dayanir V, Kiratli H, Gungen Y. Congenital or-bital teratoma: a clinicopatho-logic case report. Ophthal Plast Reconstr Surg. 1997 Jun;13(2):142-6.
22. Lee GA, Sullivan TJ, Tsikleas GP, Davis NG. Congenital orbit-al teratoma. Aust N Z J Ophthal-mol. 1997 Feb;25(1):63-6.
23. Spinelli HM, Criscuolo GR, Tripps M, Buckley PJ. Massive orbital teratoma in newborn.Ann Plast Surg. 1993 Nov;31(5):453-8.
24. Schaal ST, Kampik A, Ha-senfratz G, Boergen KP. Terato-ma orbitae in the neonatal peri-od. Klin Monatsbl Augenheilkd. 1988 Sep;193(3):295-300.
25. Schick U, Bleyen J, Hassler W. Treatment of orbital schwan-nomas and neurofi bromas. Br J Neurosurg. 2003 Dec;17(6):541-5.
26. Korra A, Sheta A. Neurofi -brosarcoma of the orbit (malig-nant change in a plexiform neu-rofi bromatosis). Bull Ophthalmol Soc Egypt. 1972;65(69):481-90.
27. Woog JJ, Albert DM, Solt LC, Hu DN, Wang WJ. Neuro-fi bromatosis of the eyelid and orbit. Int Ophthalmol Clin. 1982
Fall;22(3):157-87.
28. Smolarz-Wojnowska A, Es-sig H, Gellrich NC, Klein CM. Orbital tumours in children and adolescents. Differential diagnostics and clinical symp-toms.Ophthalmologe. 2010 Jun;107(6):543-8.
El neurofibroma plexiforme es un hamartoma que se encuentra directamente re-lacionado con la neurofibromatosis, en nuestra paciente se relacionaba con displasia ósea con una gran proptosis y asociada a glaucoma. Esta asociación debe ser siste-máticamente investigada ya que el 50-60% de los pacientes que padecen neurinoma plexiforme tienen glaucoma homolateral.25,26,27
Otras causas de proptosis, las cuales no fueron incluídas por no presentarse pa-cientes en el tiempo que duró el trabajo, son el neuroblastoma, el mucocele y las craneosinostosis. Estas últimas, en realidad, producen seudo proptosis o exorbitismo y se manifiestan desde el nacimiento.
Conclusión
La proptosis en el neonato es un signo de relevante importancia y una urgencia of-talmológica. El rápido diagnóstico y tratamiento evita importantes secuelas visuales, principalmente la ambliopía. La misma se produciría en estos pacientes por depriva-ción, por el defecto refractivo, menos frecuentemente por estrabismo ó la asociación de estas causas. Los neonatos se encuentran en el período crítico de maduración visual, razón por la cual se deben tratar los errores refractivos tempranamente.
A pesar de no haber reportes estadísticos de proptosis en neonatos, los casos que se presentan en la bibliografía coinciden en considerar a la malformación vas-cular capilar la causa más frecuente, seguida por el quiste dermoide.28 Del resto de las patologías que pueden producir proptosis la más importante a considerar es el rabdomiosarcoma ya que de su detección precoz depende la vida del paciente; a pesar de ser en este grupo etario sumamente infrecuente.

CASE REPORT
58 PAN-AMERICA
Resumen
La infestación de la superficie ocular por larvas de mosca se denomina oftalmomiasis externa. Estas lar-vas se alimentan del tejido huésped causando diferen-tes manifestaciones clínicas. En general, los síntomas oculares se limitan a irritación conjuntival, lo cual puede conllevar al diagnóstico erróneo de conjuntivitis alérgi-ca. La mosca nasal ovina Oestrus ovis es la causa más común de miasis en humanos, siendo el ganado capri-no y ovino los hospederos habituales. El humano es un hospedero ocasional, especialmente donde la crianza de éste ganado es prevalente, las larvas no penetran el globo ocular debido a que no poseen mecanismos de penetración tisular. A pesar de que la oftalmomiasis externa por larvas de Oestrus ovis ocurre usualmente en pastores y granjeros, existen algunos casos aislados en areas urbanas. Nosotros presentamos un caso de oftal-momiasis externa por larvas de Oestrus ovis en el área urbana de la Ciudad de México.
Abstract
External ocular myiasis is an infestation of the eye with Dipterous larvae, which feed on the host tissue and subsequently may cause different clinical pictures. In general, ocular symptoms are limited to conjunctival irritation, which is often misdiagnosed as acute aller-gic conjunctivitis. Oestrus ovis (sheep nasal botfly) is the most common causes of myiasis in humans, with sheep and goats being the normal hosts for the larvae. Man can be an occasional host, especially where live stock herding is prevalent, although the larvae rarely en-ter the ocular tissues since they do not posses the abi-lity to penetrate tissues. Although Oestrus ovis ophthal-momyiasis typically occurs in shepherds and farmers, isolated cases have also been reported in urban areas. We report a case of external ocular myiais caused by O. ovis in the urban area of Mexico City.
External Ophthalmomyiasis Due to Sheep Botfly Oestrus ovis Larvae
Arturo Ramirez-Miranda MD1, Armando Gonzalez-Gomar MD2, Susana Muñoz-Salas BSc3
1 Department of Cornea and Refractive Surgery. 2 Department of Integral Ophthalmology. 3 Department of Microbiology. Instituto De Oftalmología Fundación “Conde De Valenciana” Mexico DF, Mexico.
Presented as a video at the IX Scientifi c-Cultural Meeting of the Mexican Society of Ophthalmology, Guanajuato, Mexico September 2008Supported in part by Fundación “Conde de Valenciana” Mexico DF, Mexico.
Correspondence:Arturo Ramirez-Miranda, MDInstituto De Oftalmología Fundación “Conde De Valenciana”Department of Cornea and Refractive SurgeryChimalpopoca 14, Colonia Obrera, C.P.06800 Mexico DF, MexicoTel: +525555884600 ext. 3710FAX: + 525554421700Email: [email protected]
Introduction
Larvae invading the eye belong to various species. They can cause external conjunctival infection or more serious internal damage depending on their ability to penetrate ocular tissues. Oestrus ovis is the most common species of flies whose larvae cause infestation or myiasis in man. Sheep are the usual host, but man can be an occasional host, typically occuring in shepherds and farmers. Therefore myiasis appears to be fairly common but underestimated in many rural areas1. Ophthalmomyi-asis (infestation of the eye with larvae) has been reported in many parts of the world, although the majority of these reports are limited to one to 3 cases. We describe the clinical manifestations and larvae in the first case report of Oestrus ovis infestation in a patient from an urban area, Mexico City.
Case History
A 40-year-old Mexican male resident of Mexico City presented to an emergency room with conjunctival redness, foreign body sensation, itching, and tearing in both eyes for eight hours. He reported that grass had blown into his eyes while he was cut-ting his lawn. He had a non-contributory medical history, and lives in an urban area. On examination, the corrected visual acuity was 20/20 in each eye, both conjunctivae were injected, and the corneas appeared normal. Multiple translucent 2 millimeter larvae were present under the upper eyelid and the inferior fornix (Figure 1). The fun-dus showed no evidence of intraocular organisms or inflammation. Their mobility did not slow down the instillation of tetracaine, and as we removed them with forceps they were stuck in the conjunctiva. We recovered five larvae in the right eye and four larvae in the left eye, which were stored in saline solution. We prescribed topical antibiotics to avoid infection. The patient returned for a follow-up visit 3 days later, stating that his symptoms resolved 2 hours after removal of the organisms. No larvae were seen after examination. The microbiology department reported that the isolated organisms were Oestrus ovis larvae, based on their spindle shape and paired sharply curved oral hooks, a part of their cephaloskeleton. The larvae measured 1.8-3 mm in length, their surface was covered with spinnules and their bodies were divided into 10 to 11 segments and 23 to 26 terminal hooks arranged in two scallops (Figure 2).
Discussion
Ophthalmomyiasis is due to deposition of fly larvae in the eye. Various spe-cies of flies have been implicated as causing ophthalmomyiasis, including Oestrus ovis, the latrine fly (Fannia), the house fly (Musca domestica), and the cattle botfly
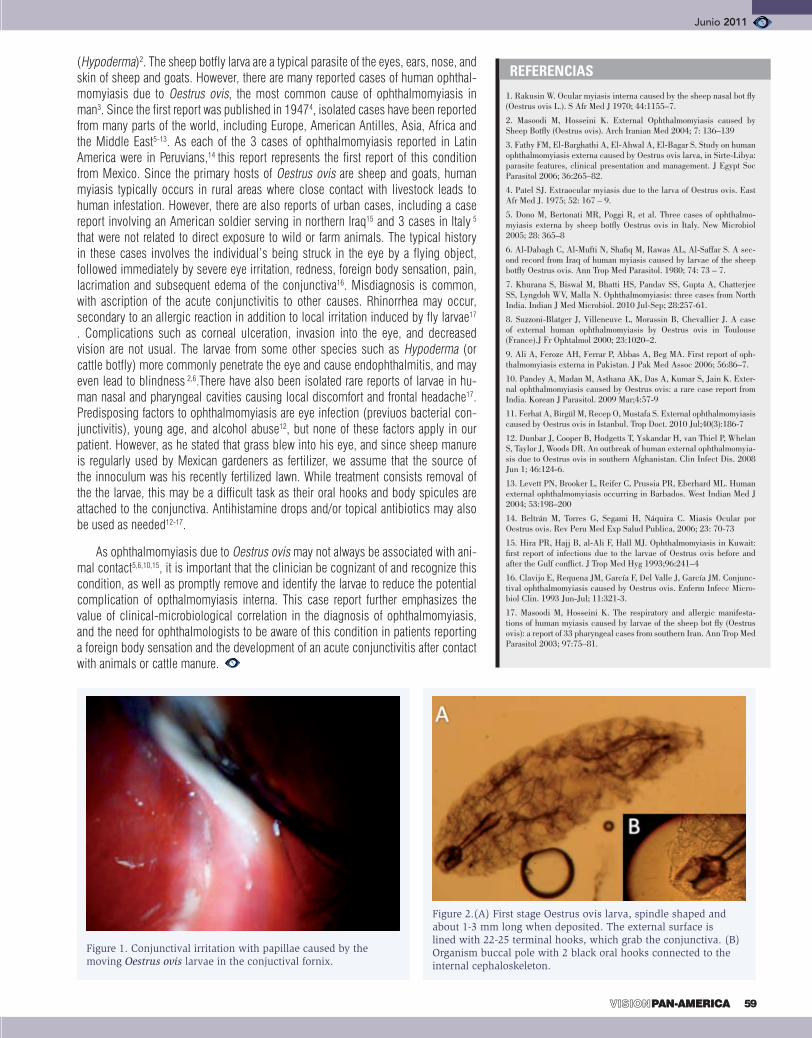
Junio 2011
PAN-AMERICA 59PAN-AMERICA
(Hypoderma)2. The sheep botfly larva are a typical parasite of the eyes, ears, nose, and skin of sheep and goats. However, there are many reported cases of human ophthal-momyiasis due to Oestrus ovis, the most common cause of ophthalmomyiasis in man3. Since the first report was published in 19474, isolated cases have been reported from many parts of the world, including Europe, American Antilles, Asia, Africa and the Middle East5-13. As each of the 3 cases of ophthalmomyiasis reported in Latin America were in Peruvians,14 this report represents the first report of this condition from Mexico. Since the primary hosts of Oestrus ovis are sheep and goats, human myiasis typically occurs in rural areas where close contact with livestock leads to human infestation. However, there are also reports of urban cases, including a case report involving an American soldier serving in northern Iraq15 and 3 cases in Italy 5 that were not related to direct exposure to wild or farm animals. The typical history in these cases involves the individual’s being struck in the eye by a flying object, followed immediately by severe eye irritation, redness, foreign body sensation, pain, lacrimation and subsequent edema of the conjunctiva16. Misdiagnosis is common, with ascription of the acute conjunctivitis to other causes. Rhinorrhea may occur, secondary to an allergic reaction in addition to local irritation induced by fly larvae17 . Complications such as corneal ulceration, invasion into the eye, and decreased vision are not usual. The larvae from some other species such as Hypoderma (or cattle botfly) more commonly penetrate the eye and cause endophthalmitis, and may even lead to blindness 2,6.There have also been isolated rare reports of larvae in hu-man nasal and pharyngeal cavities causing local discomfort and frontal headache17. Predisposing factors to ophthalmomyiasis are eye infection (previuos bacterial con-junctivitis), young age, and alcohol abuse12, but none of these factors apply in our patient. However, as he stated that grass blew into his eye, and since sheep manure is regularly used by Mexican gardeners as fertilizer, we assume that the source of the innoculum was his recently fertilized lawn. While treatment consists removal of the the larvae, this may be a difficult task as their oral hooks and body spicules are attached to the conjunctiva. Antihistamine drops and/or topical antibiotics may also be used as needed12-17.
As ophthalmomyiasis due to Oestrus ovis may not always be associated with ani-mal contact5,6,10,15, it is important that the clinician be cognizant of and recognize this condition, as well as promptly remove and identify the larvae to reduce the potential complication of opthalmomyiasis interna. This case report further emphasizes the value of clinical-microbiological correlation in the diagnosis of ophthalmomyiasis, and the need for ophthalmologists to be aware of this condition in patients reporting a foreign body sensation and the development of an acute conjunctivitis after contact with animals or cattle manure.
REFERENCIAS
1. Rakusin W. Ocular myiasis interna caused by the sheep nasal bot fl y (Oestrus ovis L.). S Afr Med J 1970; 44:1155–7.
2. Masoodi M, Hosseini K. External Ophthalmomyiasis caused by Sheep Botfl y (Oestrus ovis). Arch Iranian Med 2004; 7: 136–139
3. Fathy FM, El-Barghathi A, El-Ahwal A, El-Bagar S. Study on human ophthalmomyiasis externa caused by Oestrus ovis larva, in Sirte-Libya: parasite features, clinical presentation and management. J Egypt Soc Parasitol 2006; 36:265–82.
4. Patel SJ. Extraocular myiasis due to the larva of Oestrus ovis. East Afr Med J. 1975; 52: 167 – 9.
5. Dono M, Bertonati MR, Poggi R, et al. Three cases of ophthalmo-myiasis externa by sheep botfl y Oestrus ovis in Italy. New Microbiol 2005; 28: 365–8
6. Al-Dabagh C, Al-Mufti N, Shafi q M, Rawas AL, Al-Saffar S. A sec-ond record from Iraq of human myiasis caused by larvae of the sheep botfl y Oestrus ovis. Ann Trop Med Parasitol. 1980; 74: 73 – 7.
7. Khurana S, Biswal M, Bhatti HS, Pandav SS, Gupta A, Chatterjee SS, Lyngdoh WV, Malla N. Ophthalmomyiasis: three cases from North India. Indian J Med Microbiol. 2010 Jul-Sep; 28:257-61.
8. Suzzoni-Blatger J, Villeneuve L, Morassin B, Chevallier J. A case of external human ophthalmomyiasis by Oestrus ovis in Toulouse (France).J Fr Ophtalmol 2000; 23:1020–2.
9. Ali A, Feroze AH, Ferrar P, Abbas A, Beg MA. First report of oph-thalmomyiasis externa in Pakistan. J Pak Med Assoc 2006; 56:86–7.
10. Pandey A, Madan M, Asthana AK, Das A, Kumar S, Jain K. Exter-nal ophthalmomyiasis caused by Oestrus ovis: a rare case report from India. Korean J Parasitol. 2009 Mar;4:57-9
11. Ferhat A, Birgül M, Recep O, Mustafa S. External ophthalmomyiasis caused by Oestrus ovis in Istanbul. Trop Doct. 2010 Jul;40(3):186-7
12. Dunbar J, Cooper B, Hodgetts T, Yskandar H, van Thiel P, Whelan S, Taylor J, Woods DR. An outbreak of human external ophthalmomyia-sis due to Oestrus ovis in southern Afghanistan. Clin Infect Dis. 2008 Jun 1; 46:124-6.
13. Levett PN, Brooker L, Reifer C, Prussia PR, Eberhard ML. Human external ophthalmomyiasis occurring in Barbados. West Indian Med J 2004; 53:198–200
14. Beltrán M, Torres G, Segami H, Náquira C. Miasis Ocular por Oestrus ovis. Rev Peru Med Exp Salud Publica, 2006; 23: 70-73
15. Hira PR, Hajj B, al-Ali F, Hall MJ. Ophthalmomyiasis in Kuwait: fi rst report of infections due to the larvae of Oestrus ovis before and after the Gulf confl ict. J Trop Med Hyg 1993;96:241–4
16. Clavijo E, Requena JM, García F, Del Valle J, García JM. Conjunc-tival ophthalmomyiasis caused by Oestrus ovis. Enferm Infecc Micro-biol Clin. 1993 Jun-Jul; 11:321-3.
17. Masoodi M, Hosseini K. The respiratory and allergic manifesta-tions of human myiasis caused by larvae of the sheep bot fl y (Oestrus ovis): a report of 33 pharyngeal cases from southern Iran. Ann Trop Med Parasitol 2003; 97:75–81.
Figure 1. Conjunctival irritation with papillae caused by the moving Oestrus ovis larvae in the conjuctival fornix.
Figure 2.(A) First stage Oestrus ovis larva, spindle shaped and about 1-3 mm long when deposited. The external surface is lined with 22-25 terminal hooks, which grab the conjunctiva. (B) Organism buccal pole with 2 black oral hooks connected to the internal cephaloskeleton.

CASE REPORT
60 PAN-AMERICA
Abstract
In an effort to keep up with the ever rising cost in the current private practice setting, ophthalmology practi-ces are becoming busier, implementing innovative and cost-effective procedures. This has led to a signifi-cant decrease in the amount of time that the physician spends with the patient, which eventually may jeopardi-ze the quality of care.
We recently encountered a case of poor doctor-patient communication in which all ethical principles and limits of patient care were trespassed leaving the patient as a blind victim. We present the case hoping to touch upon every doctor’s conscience to remember the primary role of a physician in educating patients and treating without inflicting harm as a way to offer better and safer quality of health care.
Resumen
En un esfuerzo para soportar los incrementos de los precios en las prácticas médicas privadas, los oftalmó-logos se han visto en la necesidad de incrementar el número de pacientes, al igual que implementar procedi-mientos innovadores de costo beneficio adecuado. Esto ha llevado irremediablemente a disminuir el tiempo que el médico le dedica a cada paciente, lo que puede even-tualmente comprometer la calidad del tratamiento.
Recientemente encontramos uno caso de pobre comunicación médico-paciente, en el que se tras-pasaron los principios éticos llevando al paciente a
G. Paolo Giuliari MD1,3; Ama Sadaka MD2; Peter Y. Chang MD3; Alfonso Iovieno MD1
1 University of Toronto, Department of Ophthalmology and Vision Sciences, Hospital Health Network, Toronto, ON Canada
2 Schepens Eye Research Institute, Boston, MA USA3 Massachusetts Eye Research and Surgery Institution, Cambridge,
MA USA
Corresponding author:Gian Paolo Giuliari MD77 Elm Street, Apt 903Toronto, Ontario M5G1H4Phone: (416) 803-5950Email: [email protected]: silicon oil, vitreo-retinal surgery complications, retinal detachment
No funding support to disclose/no proprietary or fi nancial interest to disclose
Ojo ciego: el precio de una pobre comunicación médico-paciente
A blind eye: The price of poor physician-patient communication
la ceguera irreversible. Presentamos este caso con la esperanza de crear conciencia recordando que el rol primordial del médico es la educación y el tratamiento sin infligir daño al paciente, ofreciendo un mejor y seguro servicio de salud.
Brief Communication
We recently encountered a patient with an uncom-mon but ethically, medically and physically disturbing ocular finding. A 69-year-old gentleman presented to our clinic complaining of a slowly progressive decrease in the visual acuity in his right eye. This was associated with mild to moderate sporadic episodes of pain and redness. His past ocular history was significant for a blunt trauma in the right eye that necessitated an uns-pecified ocular surgery done at another institution three years prior. Although the patient did not remember the exact type of surgery performed, the only fact recalled was that the surgery took approximately three hours. Upon further questioning we were able to predict that he had a vitreo-retinal surgery. Commonly after a retinal detachment surgery, several types of expanding gases such as sulfur hexafluoride (SF6) and perfluoropropane (C3F8), are left in the eye to create a tamponade and increase the chances of retinal re-attachment.1 In the-se cases, the patients are asked to position their head face-down to increase the time and the area of contact between the gas bubble and the detached area of the retina. However, our patient stated that the surgeon did not ask him to maintain any particular body or head position. Hence, several explanations were possible: 1)

Junio 2011
PAN-AMERICA 61PAN-AMERICA
the surgeon did not use any intraocular gas; 2) the surgeon failed to educate the pa-tient properly; 3) the patient had not been compliant with the physician’s instructions; 4) other type of tamponate agents, such as silicon oil, could have been used instead not requiring specific head positioning.2,3
The patient stated that he had “relatively good vision” three months after surgery, being able to function quite well even with his left eye closed. He also revealed that a few months after surgery he moved to another country where eye care access was not easily accessible, hence he did not undergo further follow-up eye examinations. About one year after the surgery, the patient noticed a slowly progressive loss of vision with increasing ocular pain in the right eye, prompting his visit to our clinic.
At the initial visit, he had a visual acuity consistent with hand motion, and an intraocular pressure of 45 mmHg in the right eye. Slit lamp biomicroscopy revealed what appears to be emulsified silicon oil in the anterior chamber at the level of the pupil and a severe brunescent cataract (Fig 1). We performed an ocular ultrasound which also confirmed the presence of silicon oil in the vitreous cavity. At this point, we again inquired about the type of surgery performed, the awareness regarding the substance left in the eye as a vitreous substitute and the need for a second surgical intervention. The patient declared ever being given such information.
Silicone was first introduced in ophthalmology in the 1960s in the form of silico-ne oil for use in retinal reattachment surgery.4 Since its FDA approval in 1996, silicone oil has garnered much popularity among vitreoretinal surgeons in the management of complex rhegmatogenous retinal detachments secondary to severe proliferative vitreoretinopathy, giant retinal tears, viral retinitis, trauma and others.3,5-7 One of the drawbacks of silicone oil is that a second surgery must be done, typically three to six months after the initial surgery, to retrieve it from the eye. If left in the vitreous cavity for a prolonged period, silicone oil can lead to sight-threatening complications such as cataract, band keratopathy, and a progressive drug-resistant glaucoma resulting in permanent optic nerve damage.2,8,9
With the patient’s consent, we subsequently surgically removed the silicone oil, and the cataract. The patient unfortunately did not recover any useful vision in that eye due to significant optic nerve atrophy and retinal ischemia.
This case represents the result of the patient autonomy disrespect and the viola-tion of medical ethics in doing no harm. It is a case where passive rush in ophthal-mology practice, like many other medical practices, where invasive and economically rewarding procedures have made ophthalmologists forget sometimes about the im-portance of educating patients prior to any interventions. Regardless of how busy or time-restricted any physicians’ practice is there is no justification for endangering any patient’s well being. Physicians have been pushed to increase the number of visits and surgical procedures to be able to keep with the ever rising cost of health care, inevitably at the expense of the patient-doctor relation quality. It is very often encountered that post-operative care is over-looked and patients are assumed to know the way to deal with a condition that their physician never took the time to educate them about. This case shows the unfortunate outcome of a situation in which, due to grossly inefficient doctor-patient communication and patient’s low compliance, the potential benefit of a complicated and costly surgery along with useful vision in one eye was irremediably lost.
In a world where reliably safe healthcare expectations remain unfulfilled, we belie-ve and hope that this case touches upon the conscience of physicians and highlights the irreplaceable value of a successful physician’s role: the art of listening, respecting and interacting as means to offer a better and safer quality of health care.
REFERENCIAS
1 Cekic O, Ohji M. Intraocular gas tamponades. Semin.Ophthalmol. 2000;15:3-14.
2 Federman JL, Schubert HD. Complications associated with the use of silicone oil in 150 eyes after retina-vitreous surgery. Ophthalmology 1988;9:870-876.
3 Berker N, Batman C, Ozdamar Y, Eranil S, Aslan O, Zilelioglu O. Long-term outcomes of heavy silicone oil tamponade for complicated retinal detachment. Eur.J.Ophthalmol. 2007;17:797-803.
4 Liesenhoff H. On an improved technic of silicone injec-tion into the vitreous cavity during ablation surgery. Klin.Monbl Augen-heilkd. 1968;152:658-665.
5 McCuen BW,3rd, de Juan E,Jr, Machemer R. Silicone oil in vitreoreti-nal surgery. Part 1: Surgical techniques. Retina 1985;5:189-197.
6 Sodhi A, Leung LS, Do DV, Gower EW, Schein OD, Handa JT. Recent trends in the management of rhegmatogenous retinal detachment. Surv.Ophthalmol. 2008;53:50-67.
7 Herbrig E, Sandner D, Engelmann K. Anatomical and functional re-sults of endotamponade with heavy silicone oil - Densiron 68 - in com-plicated retinal detachment. Ophthalmic Res. 2007;39:198-206.
8 McCuen BW,2nd, de Juan E,Jr, Landers MB,3rd, Machemer R. Sili-cone oil in vitreoretinal surgery. Part 2: Results and complications. Retina 1985;5:198-205.
9 Didier T, Brasseur G, Charlin JF. Retinal detachment with vitreo-retinal proliferation treated by temporary silicone oil tamponade. Long-term results. Bull.Soc.Ophtalmol.Fr. 1990;90:181-2, 185.
Figure 1. External photograph showing emulsifi ed silicone oil in the anterior chamber at the level of the pupil.
PAAO
62 PAN-AMERICA
Nelson R. A. Marques
Chairman of the BoardPan-American Ophthalmological Foundation
New Horizons for the Pan-American
The Pan-American Ophthalmological Foundation (PAOF) Board of Directors has just completed the first half of its term this past May. This seems incredible to me but one year and a half have gone since our appointment in 2009. Consequently it is perfect timing to provide the members of the Pan-American Association of Oph-thalmology (PAAO) with a brief report of our accomplishments so far.
With the strong support of Dr. Cristián Luco from Santiago, Chile, as incumbent PAAO President and Dr Mark J. Mannis as PAAO President-Elect from Sacramento Calif., one of the first things that the Pan-American Foundation did last year was to conduct a search for an external consultant to help us develop a Strategic Plan Proposal for 2010-2013. We were very fortunate to find Michelle Whiting who has facilitated this development, walking the entire PAAO Executive Committee through the whole process. Just for reference, the last Strategic Plan that the Pan-American Association developed was from 1993 and, of course, it was totally outdated. The PAAO and PAOF boards enthusiastically approved the Strategic Plan in our last meetings back in October 2010.
At the same time that we were working on developing our Strategic Plan, we have worked diligently to redefine the branding of the Association and the Foun-dation. The new logos are more contemporary, dynamic and graphically attrac-tive and are now fully implemented in stationery, communication and graphic materials. Our last edition of Vision Pan-America featured the new logo and artwork on its cover page.
The new logo will also be the basis for the new interactive educational Portal. We plan to launch the Portal at our upcoming 29th Pan-American Congress of Oph-thalmology in Buenos Aires, July 6-9, 2011. Members will discover a brand-new world on the Internet when accessing www.PAAO.org. Non members will also have access to a more appealing and contemporary website. Highly interactive the portal features the most modern functionalities in web pages and we hope it will make you “prouder yet of being Pan-American.”
We will keep you informed as we continue to develop this work in progress. The Portal will feature a Forum which we encourage all of you to participate. In our extended development plan of the Portal, education will become more easily acces-sible with online webinars and recorded seminars. Members can create profiles and be able to communicate with each other. They can upload pictures and memories to their profiles. This is indeed a very exciting time.
Following the recommendation of the Strategic Plan, we have spent the last four and a half months in the search of a new Director of Development. This was a long process and we saw a lot of diverse talent and areas of expertise.

Junio 2011
PAN-AMERICA 63PAN-AMERICA
Different professional trajectories were explored, in-terviewed and analyzed. We are glad to report that a very seasoned professional has started at the begin-ning of June and will be introduced to the both the Pan-American Association and Foundation Boards of Directors and Pan-American members when we meet in Buenos Aires in July.
A dedicated professional in the area of Develop-ment will bring more financial resources over time not only to fund new education, grants, exchange pro-grams and blindness prevention programs, but also to hopefully contribute to make our overall financial picture more stable and not so dependent on the Con-gress years.
Please take advantage and enjoy the Tango Show in Buenos Aires on July 8th. The proceeds from ticket sales will help to support our educational programs. For more information please go to our website www.paao.org.
There has been great team work between the leaders of the Pan-American Association and the Foundation who have been totally aligned in terms of priorities and strategies, under the current leadership of Dr. Luco, and as of July, by Dr. Mannis. Teresa and Terri as usual are tireless and totally committed to our causes and goals.
I hope the next 18 months are as exciting, or even more so, than the previous year and half. My goal since my acceptance speech in October 2009 has been to have a more active Foundation focused on de-velopment of resources. We are incessantly following that trail for the greater benefit of the Pan-American Association of Ophthalmology.
See you in Buenos Aires.

Director, J. Fernando Arévalo, MD, FACS (Venezuela)Co-directores, Peter Quiros, MD (USA), Lihteh Wu, MD (Costa Rica)
The Peabody Orlando HotelOrlando, FL, USAMiércoles, 26 de Octubre de 2011(Orlando Ballroom) 8:00 AM - 5:30 PM


PAN-AMERICA4 :