Presentación de PowerPoint - Doctaforum · 2004 ifl (calgb c89804) 2005 folfiri (accord-02) 2005...
37
ESTRATEGIAS DE TRATAMIENTO ADYUVANTE EN CÁNCER DE COLON EDUARDO DÍAZ-RUBIO Hospital Clínico San Carlos MADRID 17 Junio de 2016
Transcript of Presentación de PowerPoint - Doctaforum · 2004 ifl (calgb c89804) 2005 folfiri (accord-02) 2005...

ESTRATEGIAS DE TRATAMIENTO ADYUVANTE EN CÁNCER DE COLON
EDUARDO DÍAZ-RUBIO Hospital Clínico San Carlos
MADRID 17 Junio de 2016

CCR (ESPAÑA)
Todos: 215.534
CCR: 32.240 (15%) 1ª causa
Todos: 102.762
CCR: 14.700 (14%) 2ª causa
Todos: 581.688
CCR: 89.705 (15%) 3ª causa
INCIDENCIA
MORTALIDAD
PREVALENCIA
NECESIDAD DE PROGRESO

SG relativa a 5 años CCR
España 57.1%
Eurocare 5 57% (46.6-61.4)*
US SEER 66%
CON LOS MEDIOS DISPONIBLES ACTUALES HAY POSIBILIDADES DE MEJORA
29 países (Lancet Oncol 2014)

T1
T2
T3
T4 a, b
% Diagnosis of CRC 15% 20-30% 30-40% 20-25%
% Overall Survival at 5 years 85-95% 60-80% 30-60% <5%
Stage I Stage II Stage III (N+) Stage IV
IIB
IIA N0,M0 N0, M0 M1
submucosa
muscularis propia
Pericolorectal tissues
T4a: visceral pt T4b: organs o structures
IIIA:T1-2 N1, T1N2a IIIB:T3-4 N1,T2-3 N2a T1-2 N2b IIIC: T4aN2a, T3-T4N
N1a: 1 N N1b: 2-3 N N1c: deposits* N2a:4-6 N N2b: >6 N
* subserosa, mesentery, or nonperitonealized pericolic or perirectal tissues AJCC (version 7) 2010

SEER population
N=109.953 T3: tejido pericolorrectal T4a: peritoneo visceral T4b: órganos o estructuras

ADJUVANT CT IN CRC (Steps Ahead: 1990-2016)
1990 5FU+Levamisol (Intergrupo) 1994 5FU+Leucovorin (NCCTG,NCIC,NSABP) 2003 CI 5-FU (LV5FU2, PVI5-FU) (André T)
Positive
Positive 2003 FOLFOX (MOSAIC) 2005 FLOX (NSABP C-07) 2004 Oral FU (X-ACT: Cape), (NSABP-C-06: UFT)
Positive 2009 XELOX (XELOXA)
FOLFOX: MOSAIC (NEJM 2004, JCO 2009, JCO 2015) XELOX: XELOXA (JCO 2011) FLOX: NSABP-C-07 (JCO 2007, JCO 2011) ?? > toxicity

ADJUVANT CT IN CRC (Negative results: 1990-2016)
2004 IFL (CALGB C89804) 2005 FOLFIRI (ACCORD-02) 2005 5FU CI+CPT-11 (PETACC3)
Negative
Negative 2009 FOLFOX+BV (NSABP-C-08) (AVANT) 2014 QUASAR-2
Negative 2010 FOLFOX+Cxmab (NCCTG-INT) 2012 PETACC-8 (ESMO)
Bevacizumab: 1) NSABP_ C-08: JCO 2011 2) AVANT: JCO: 2011 3) QUASAR-2 ASCO 2014 Cetuximab: 1) NCCTG 0147: JAMA 2012 2) PETACC-8: Lancet Oncol 2014

Stage III (N+): OS 5 y Adjuvant Treatment
Surgery 50-55%
5FU+LV 60%
5FU IC 65%
Capecitabine 65%
FOLFOX 75%
FLOX 75%
XELOX 71%
1. Clear Benefit (DFS, OS) 2. All pts in good conditions should be treated 3. FOLFOX, XELOX or Capecitabine alone if pts are not candidates for Ox (elderly) 4. Concern: Toxicity 5. Start: 8-12 w after surgery 6. Duration: 6 months (IDEA study)
IIIA:T1-2 N1 IIIB:T3-4 N1 IIIC: N2 (>3)
N1: 1-3, N2>3
CONCLUSIONS


Stage II (N0M0) IIA=T3, IIB=T4a-b QUASAR (FU+LV) Yes (OS: 3.6%)
ACCENT DATA BASE Yes (OS:5.4%)
Meta-analysis (IMPACT: FU+LV) Yes
Cochrane systematic review Yes for DFS
MOSAIC (FOLFOX) NSABP C-07 (FUOX)
No for OX (MOSAIC: trend for DFS, no for OS) (NSABP: 2-3% OS)
Expert opinions Yes in high risk
NCCN Guidelines Yes in high risk
Schedules of CT: FU+LV (Cape), FOLFOX, XELOX

Stage II : High Risk(T3-4,N0)
• T4 (IIB/IIC) (organs) • Intestinal obstruction • Colon perforation • Perineural or lymphatic/vascular invasion • Grade of differentiation G3-G4 • Positive margins • Inadequate number of LN isolated (<12)
ASCO 2004 NCCN GUIDELINES 2016
ESMO GUIDELINES (Ann Oncol 2013)
Different consensus definition

MOSAIC: OS AND STAGE (Anfré T. Dec JCO 2015) 10 years follow-up
overall
71.7% 67.1%
(4.6%)
78.4% 79.5%
67.1% 59%
(8.1%)
Stage II
Stage III N=2.246 pts
NS

Stage II low-risk Stage II high-risk
Stage III N1
Stage III N2
71.4% 65.4% (6%)
59.5 % 46.6 % (12,9%)
André T.- JCO Dec 2015
MOSAIC: OS AND STAGE (JCO 2015) 10 y follow-up
NS NS
NS
N1: 1-3; N2: >4

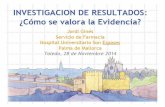
Copyright © American Society of Clinical Oncology
Andre, T. et al. J Clin Oncol; 27:3109-3116 2009
Fig 5. Proportion of patients treated with oxaliplatin plus fluorouracil and leucovorin with grade 1, 2, or 3 peripheral sensory neuropathy during treatment and after follow-up to 4 years
15,4%

Treatment of CRC in the elderly
>85 years old Three or more comorbid diseases One or more geriatric symptoms: - dementia - falling tendency - delirium - incontinence - depression - selft-neglect
Balducci L.- Cancer Control 2000
Elderly pts with Frailty
Should patients, according to the age, treated differently? Sargent (adjuvant meta-analyisis NEJM 2001):
similar benefit with FU+LV (>70 y)
En España el 34% de los pacientes con CCR tienen >80 años >75 años 40%

Slide 16
Presented By Hanna Sanoff at 2015 ASCO Annual Meeting

Slide 17
Presented By Hanna Sanoff at 2015 ASCO Annual Meeting

The Cancer Genome Atlas Network Nature 487, 330-337 (2012) doi:10.1038/nature11252
32 genes somáticos mutados
N= 224 tumores y tejido normal
ACVR2A: activin receptor type 2ª (TGF-B family)
Consorcio Genoma Humano
84% 16%
77%
500-1200 mutaciones
50-100 mutaciones
1. Metilación Promotores (esporádicos) fenotipo metilador en las islas CpG (CIMP) 2. Mutacion Reparadores (Lynch: HNPCC) (MLH1,MLH3,MSH2,MSH3,MSH6, PMS2) (Fenotipo Hipermutador) (MSI) 16%

Stage II-III 5 studies (n=457) (5FU based therapy)
Prognostic and predictive value
untreated pts treated pts
15% dMMR
MSI-H: better prognosis MSI-H: no benefit of CT

Predictive value
Sargent D.- JCO 2010
Stage II (dMMR) Stage III (dMMR)
Stage II (pMMR) Stage III (pMMR)
deleterous
benefit no benefit
no benefit

Prognostic Impact of Defective Mismatch Repair in Stage II/III Colon Cancer: A Pooled Individual Patient Data Analysis of 17 Adjuvant Trials
from the ACCENT Database
D Sargent, Q Shi, G Yothers, S Tejpar, M Bertagnolli, S Thibodeau, T Andre, R Labianca, S Gallinger, SR
Hamilton, G Monges, K Pogue-Geile, S Paik, D Klingbiel, A Roth, E Pavey, G Kim, F Sinicrope for
the ACCENT Collaborative Group
26 randomized studies >37.800 pts MMR: 7.803 (17 trials) ASCO 2014

TTR & OS Stage II, Surgery Alone (N=307)
Time to Recurrence Overall Survival

TTR & OS Stage II, 5-FU Based Rx (N=1155)
Time to Recurrence Overall Survival

Metilaciones en el promotor
Germinales: Lynch
somáticas
MMR-D = MSI-H MMR-P = MSI-L/MSS
mononucleótido monomórfico

1.- Schlicker A: BMC Medical Genomics 2012, 2.- Sadanandam A: Nature Med 2013, 3.- Budinska E: J Pathol 2013, 4.- De Sousa F: Nature Med 2013, 5.- Marisa L: Plos Med 2013, 6.- Roepman P: Int J Cancer 2013, 7.- Perez-Villamil B: BMC Cancer 2012
MSI RAS RAF Wnt Mesen Inmune
Diferentes subtipos

Nature Medicine 2015 SCNA: somatic copy number alterations
N= 4.151 samples (Markov Cluster Algorithm)
Consensus Molecular Subtypes Consortium of 6 independent groups

GENETIC SIGNATURES Platforms Tissue Nº Genes Stage
N Groups
HR
Veridex Paraffine 23 (7) II n=123
2 HR: 6.89
Coloprint (Agendia)
Fresh 18 II n=188
2 HR: 2.5
Oncotype (Genomic Health)
Paraffine 12 (7) III n=1.436
3 HR: 1.38
Almac Fresh 634 II n=215
2 HR: 2.53
Clear pronostic role, but not predictive

Dienstmann R.- JCO 2015 Comentarios: Determinación de MSI: Obligada para estadios II Firmas Genómicas: Posible utilidad estadios II (pronostica) CTC: No son de utilidad en estadios II y III (HCSC: Ann Oncol 2015) ctDNA: Faltan datos

Único con test diagnóstico validado CDX2: Factor transcripcional
2115 muestras de CCR
Análisis bioinformático para buscar marcadores negativamente relacionados con la molécula de adhesión leucocitaria ALCAM/CD16
16 genes candidatos
Universidad de Columbia

Validation data set: N=314
12% 88%


Aspirina y NSAIDs y CCR (escenarios)
1. Prevención de los pólipos adenomatosos esporádicos: Nivel de evidencia 1
2. Prevención del CCR hereditario (APC, HNPCC) (celecoxib aprobado por la FDA 2002 para APC) 3. Prevención del CCR esporádico (Rothwell Lancet 2010, 2012) 4. Tratamiento adyuvante del CCR
TTD: Oviedo 11 Diciembre 2015
Debate Oxford: No se llegó a un consenso

April 2016
Conclusiones e Implicaciones: Hasta tener ensayos randomizados, los estudios observacionales deben ser tenidos en cuenta, y por tanto los pacientes diagnosticados de cáncer deben ser informados del potencial beneficio de la aspirina para que decidan si desean tomarla o no.
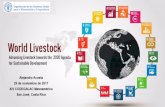
CCR: 9 estudios observacionales (que analizaban mortalidad especifica por CCR) HR: 0.76 (95% CI: 0.66-0.88)
Colon Mama Próstata

Bibbins-Domingo.- Ann Intern Med: April 2016


HR:0.18
HR:0.54
N=161/964 (17%) N=803 (83%)
Liao X.- NEJM 2012
PI3K mutado (pirosecuenciación: exones 9 y 20) en CCR: 17%
Nurses´s Health Study Health Professionals Follow-up Study
riesgo 82%

Conclusiones: Tto Adyuvante C.Colon
• Estadio III: Quimioterapia XELOX, FOLFOX, por 6 meses (¿3 meses?). Mayor beneficio en los N2 vs N1.
• En los pacientes ancianos no está claro el beneficio del oxaliplatino (menor que los <70 años).
• En los estadios II de alto riesgo determinar la MSI es obligado (CDX2?).
• La clasificación molecular pueden tener utilidad y separan grupos que van a ser claves en el futuro. El papel de las firmas genómicas es pronóstico.
• La aspirina ha mostrado su utilidad en estudios observacionales, pero no hay estudios prospectivos randomizados por lo que la decisión debe ser individual.