Presentación de PowerPoint - cirugiacordoba.com.ar · CASO 2: DOBLE AE: BAZO - PELVIS. ... Madoff...
30
Angioembolización simultanea de órganos en la estrategia de tratamiento no operatorio en trauma cerrado de abdomen AUTOR: PAULINA, Eduardo O. RELATOR: VELEZ, Sebastián E. Hospital Municipal de Urgencias
Transcript of Presentación de PowerPoint - cirugiacordoba.com.ar · CASO 2: DOBLE AE: BAZO - PELVIS. ... Madoff...

Angioembolización simultanea de órganos en la estrategia de
tratamiento no operatorio en trauma cerrado de abdomen
AUTOR: PAULINA, Eduardo O.
RELATOR: VELEZ, Sebastián E.
Hospital Municipal de Urgencias

INTRODUCCION

Definición:
Tratamiento no operatorio (TNO) aquel que se
aplica a un órgano o región lesionados con
medidas no quirúrgicas o bien medidas
quirúrgicas minimamente invasivas con el objeto
de evitar los perjuicios de una laparotomía en el
contexto del paciente politraumatizado

Condición para iniciar TNO:
ESTABILIDAD HEMODINAMICA:
Se define por valores normales de constantes vitales, estado acido base, signos clínicos
• Pacientes estables
• Pacientes inestables que responden a la reanimación
• Pacientes inestables que no responden a la reanimación

Con la aplicación del TNO Disminuyó el uso de la laparotomía
Intervenciones hepáticas: <15%
Intervenciones esplénicas: esplenorrafia/Esplenectomias: < 25%
Intervenciones renales: nefrorrafia/Nefrectomias:<5%
Intervenciones en las fx pelvicas packing/ligadura: excepcional
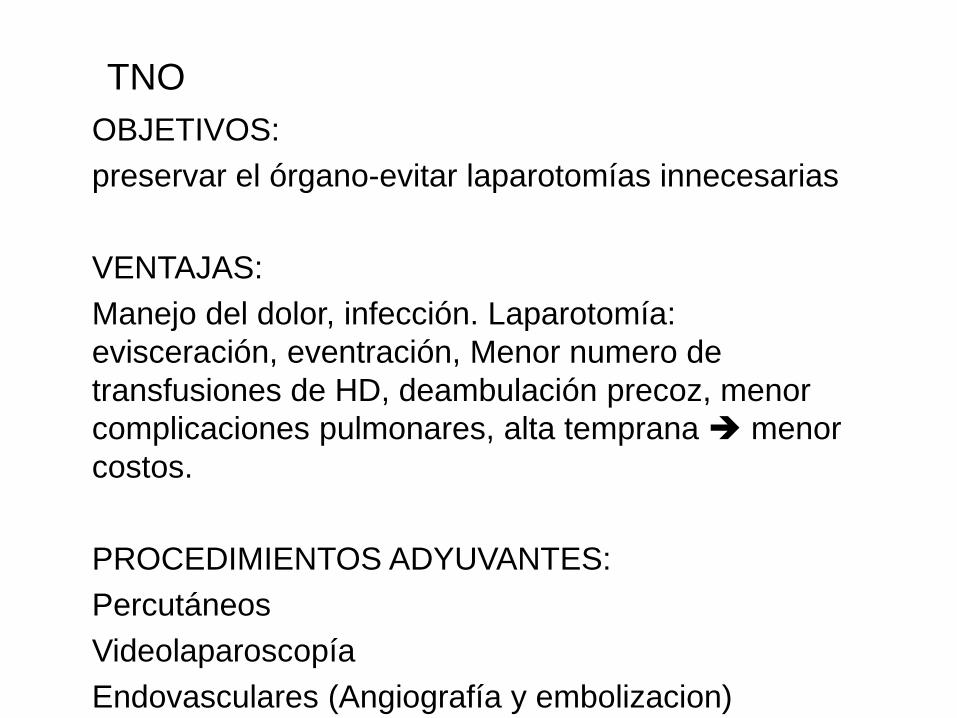
TNO
OBJETIVOS:
preservar el órgano-evitar laparotomías innecesarias
VENTAJAS:
Manejo del dolor, infección. Laparotomía:
evisceración, eventración, Menor numero de
transfusiones de HD, deambulación precoz, menor
complicaciones pulmonares, alta temprana menor
costos.
PROCEDIMIENTOS ADYUVANTES:
Percutáneos
Videolaparoscopía
Endovasculares (Angiografía y embolizacion)

ANGIOGRAFÍA Y EMBOLIZACIÓN:
• Procedimiento endovascular miniinvasivo
OBJETIVO:
• Cohibir el sangrado
• Estabilizar el paciente
INDICACIONES:
• Emergente: sangrado evidente
Fuga del contraste en TC o ANGIO
• Preventivo: signos de peligro o sospecha
FAV, seudoaneurisma, vasoespasmos, lesiones GIII o
mayores, hemoperitoneo extenso
MATERIAL Y METODOS

• Trauma abdominal cerrado con lesiones
demostradas entre2007 2014, que recibieron
AE.
• Indicaciones
Observación de:
• Edad sexo estudios realizados, estado
hemodinámica, ISS, OIS, morbilidad, mortalidad.

TÉCNICA DE AE:
• Punción femoral
• Cateterismo selectivo
• Embolización con micropartículas de esponja de
gelatina absorbible
• Angiografía de control

RESULTADOS

POBLACION
• LAPAROTOMIAS O FALLECIDOS N112
TRAUMA ABDOMINAL CERRADO2007 – 2014
N 393
• TNO CON LESIONES DE BAJO GRADO O FALLO TNO N98
TNO
N281
• no ANGIOGRAFIA (dif. técnica, endoprótesis, Arteria bronquial) N17
ANGIOGRAFIAS
N 183
• FALLOS (esplenectomías, lesión de víscera hueca) N13
AE
N166
• FALLO?? Nefrectomía N1DOBLE AE
N 7

TOTAL DE PACIENTES AE
Total AE n166 AE doble n7
Edad 29 µ 31.5 µ
Sexo 85.5 % M 6 85,7 % M
Shock <2 >3 <2 >3
Estadía 20d µ 19.5 µ
ISS 23 µ 21 µ
OIS >3 >3
Complicaciones 52 31% 22% 4 57% 42%
Fallos 13 7,83% 1??
Mortalidad 4 2,4 µ 0
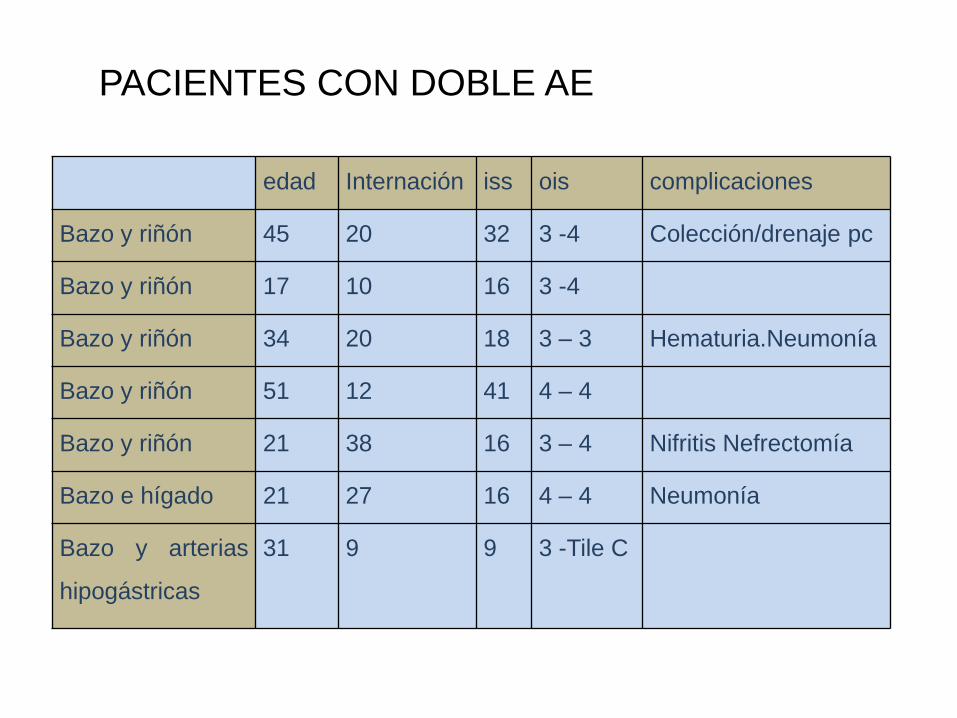
PACIENTES CON DOBLE AE
edad Internación iss ois complicaciones
Bazo y riñón 45 20 32 3 -4 Colección/drenaje pc
Bazo y riñón 17 10 16 3 -4
Bazo y riñón 34 20 18 3 – 3 Hematuria.Neumonía
Bazo y riñón 51 12 41 4 – 4
Bazo y riñón 21 38 16 3 – 4 Nifritis Nefrectomía
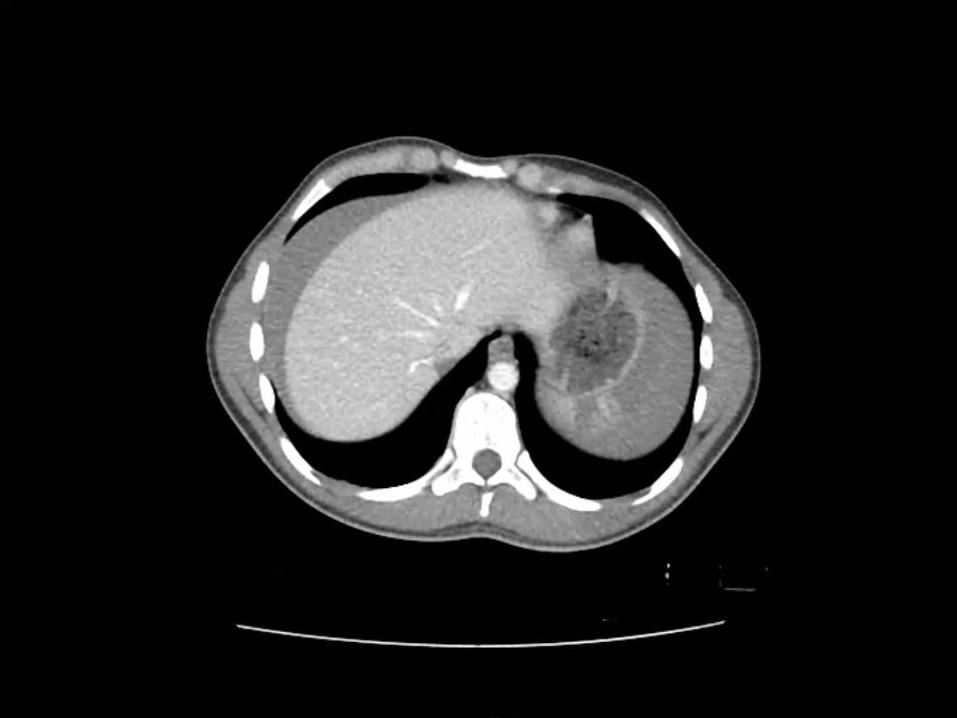
Bazo e hígado 21 27 16 4 – 4 Neumonía
Bazo y arterias
hipogástricas
31 9 9 3 -Tile C
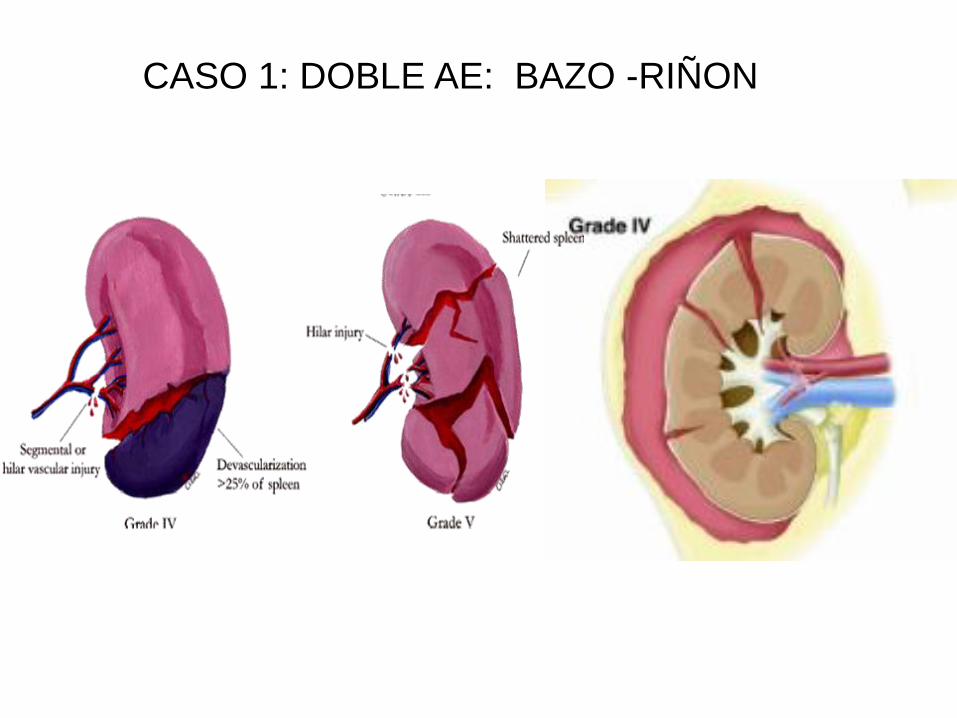
CASO 1: DOBLE AE: BAZO -RIÑON


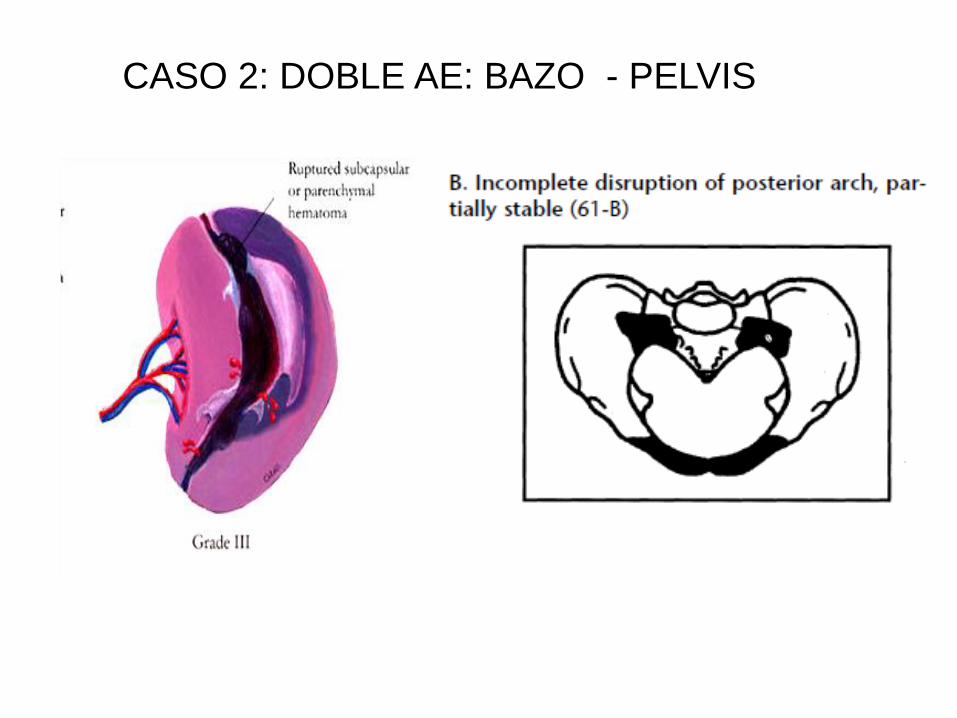
CASO 2: DOBLE AE: BAZO - PELVIS

DISCUSIÓN
• Es necesario un paciente hemodinámicamente normal para este procedimiento ?
• Cuando podemos decir que el procedimiento falló?
• Es posible realizar AE en más de una lesión?

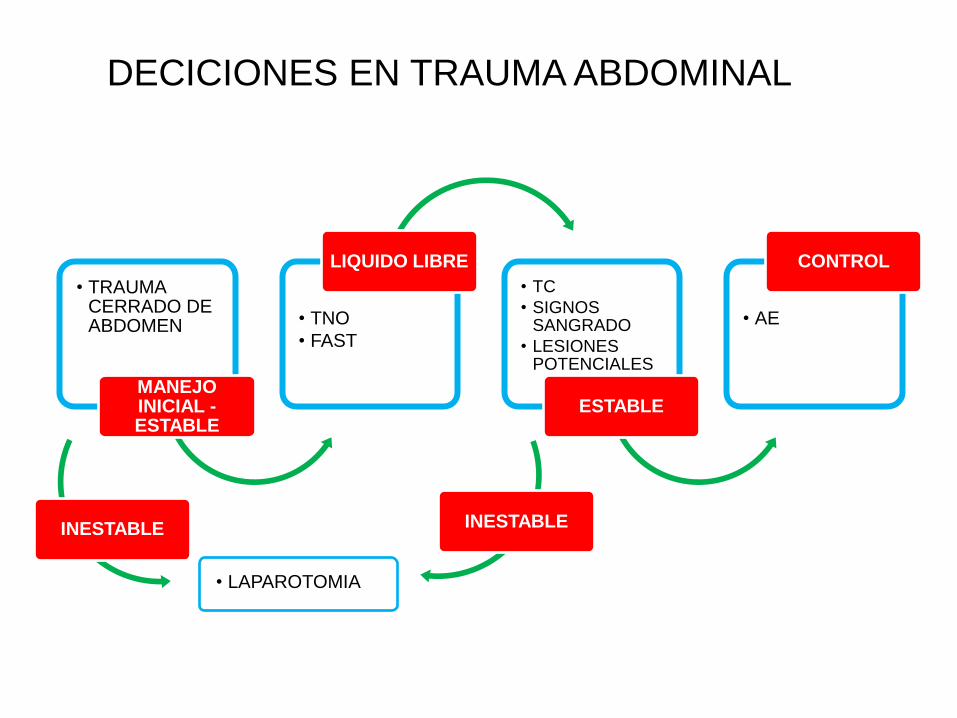
• TRAUMA CERRADO DE ABDOMEN
MANEJO INICIAL -ESTABLE
• TNO
• FAST
LIQUIDO LIBRE
• TC
• SIGNOS SANGRADO
• LESIONES POTENCIALES
ESTABLE
• AE
CONTROL
DECICIONES EN TRAUMA ABDOMINAL
INESTABLE INESTABLE
• LAPAROTOMIA
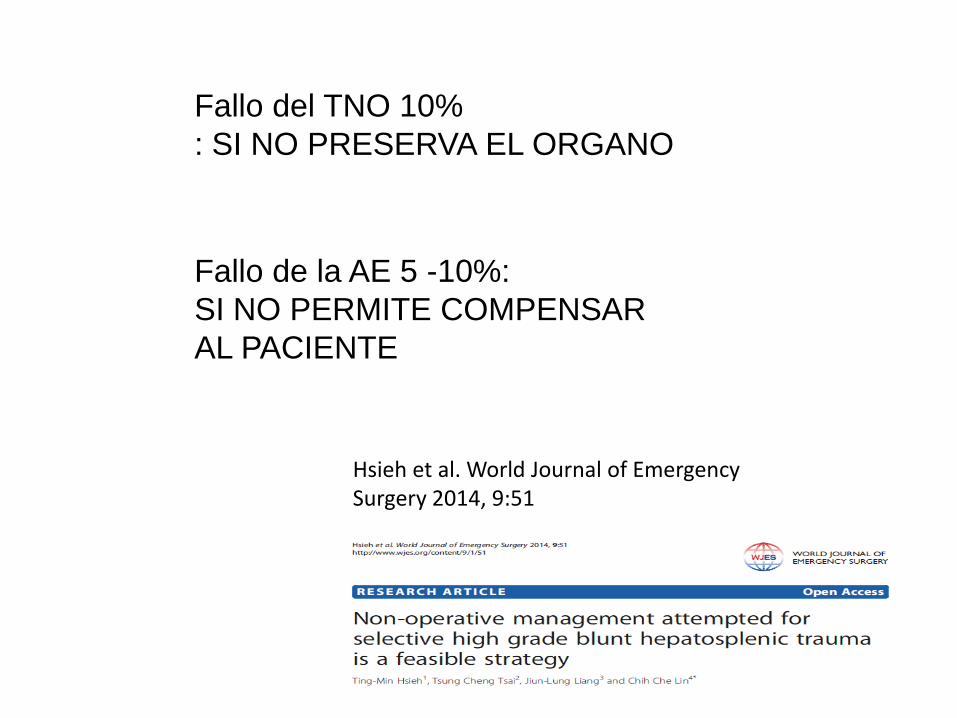
Hsieh et al. World Journal of Emergency Surgery 2014, 9:51
Fallo del TNO 10%
: SI NO PRESERVA EL ORGANO
Fallo de la AE 5 -10%:
SI NO PERMITE COMPENSAR
AL PACIENTE

• hagiwara
41 PAC MAS DE UNA REGION 22 TNO
15 DOS REGIONES PELVIS 13, 7 BAZO, 6 HIGADO, 3 FACIAL, 1 RENAL
4 3 REGIONES 4 BAZO, 3 HIGADO, 2 RENAL

• Inestable a cirugía
• Estable o estabilizado: estudios y procedimientos no invasivos
• Estable o estabilizado: se puede prolongar el procedimiento para realizar mas de una AE y estabilizar y/o evitar laparotomía/preservar organos
CONCLUSION

1Asensio JA, Roldan G, Petrone P, et al. (2003) Operative management and outcomes in 103 AAST-OIS grades IV and V complex hepatic injuries: trauma surgeons still need to
operate, but angioembolization helps. J Trauma 54:647–653, discussion 653–644
2Baker SP, O'Neill B, Haddon W, Jr, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974
Mar;14(3):187–196
3 Cámara H, Canga C., Marcon G. y Martinez G. Embolizacion arterial en trauma abdominopelviano: impacto en la estabilidad hemodinamica. Rev. HUcba 2007; I(4): 5:11.
4Davis KA, Fabian TC, Croce MA, et al.. Improved success in non-operative management of blunt splenic injuries: embolization of splenic artery pseudoaneurysms. J Trauma. 1998;
44: 1008–1015.
5Hagiwara A, Murata A, Matsuda T, et al. (2004) The usefulness of transcatheter arterial embolization for patients with blunt polytrauma showing transient response to fluid
resuscitation. J Trauma 57:271–276, discussion 276–277
6 Hann JM, Biffl W, Knudson M, et al.. Western Trauma Association Multi-Institutional Trials Committee: splenic embolization revisited. J Trauma. 2004; 56: 542–547.
7 Harbrecht BG, Ko SH, Watson GA, et al.. Angiography for blunt splenic trauma does not improve success rate of non-operative management. J Trauma. 2007; 63: 44–49.
8Hoff WS, Holevar M, Nagy KK, Patterson L, Young JS, Practice management guidelines for the evaluation of blunt abdominal trauma: the East practice
management guidelines work group. J Trauma. 2002 Sep;53(3):602-15. Review.
9 Kortbeek J, Turki S,Advanced Trauma Life Support, 8th Edition, The Evidence for Change. J. Trauma. June 2008. Vol 64-6 (1638-1650).
10 Lin WC, Chen YF, Lin CH, Emergent transcatheter arterial embolization in hemodynamically unstable patients with blunt splenic injury. Acad Radiol. 2008 Feb;15(2):201-8.
11Madoff DC, Denys A, Wallace MJ, y col,Splenic arterial interventions: anatomy, indications, technical considerations, and potential complications. Radiographics. 2005 Oct;25 Suppl
1:S191-211.
12Miller PR, Chang MC, Hoth JJ, Prospective trial of angiography and embolization for all grade III to V blunt splenic injuries: nonoperative management success rate is significantly
improved. J Am Coll Surg. 2014 Apr;218(4):644-8.
13Monnin V, Letoublon C, Broux C, Ferretti G . Place of Arterial Embolization in Severe Blunt Hepatic Trauma: A Multidisciplinary Approach Cardiovasc Intervent Radiol (2008)
31:875–882
14Montenegro RB., Alejandre SE. "Manejo conservador de los traumatismos de abdomen". Relato oficial, 78° Congreso Argentino de Cirugía Asociación Argentina de Cirugía.
Publicación extraordinaria. Buenos Aires 2006.
15 Moore EE, Shackford SR, Pachter HL, et al.Organ injury scaling: spleen, liver, and kidney.J Trauma. 1989 Dec;29(12):1664-6.
16Stassen N, Bhullar I, Julius D. Selective nonoperative management of blunt splenic injury: An Eastern Association for the Surgery of Trauma practice management guideline
Trauma Acute Care Surg S294 Volume 73, Number 5, Supplement 4 November 2012 - Volume 73 - Issue 5
17 Tile M Acute Pelvic Fractures: I. Causation and Classification. J Am Acad Orthop Surg. 1996 May;4(3):143-151.
18Ting-Min Hsieh, Tsung Cheng Tsai, Jiun-Lung Liang y col. Non-operative management attempted for selective high grade blunt hepatosplenic trauma is a feasible strategy. Hsieh et
al. World Journal of Emergency Surgery 2014, 9:51
19 Velmahos GC, et al.Técnica embolización transitoria. Am Surg 2000;66: 858-862.
20 Velmahos GC, Zacharias N, Emhoff TA, et al.. Management of the most severely injured spleen.Arch Surg. 2010; 145: 456–460.
21
Velmahos GC, Zacharias N, Emhoff TA, Feeney JM, Hurst JM, Crookes BA, Harrington DT, Gregg SC, Brotman S, Burke PA, Davis KA, Gupta R, Winchell RJ, Desjardins S,
Alouidor R, Gross RI, Rosenblatt MS, Schulz JT, Chang Y: Management of the most severely injured spleen: a multicenter study of the Research Consortium of New England
Centers for Trauma (ReCONECT). Arch Surg 2010, 145(5):456–460
22 Wu SC, et al.. Early selective angioembolization improves success of non-operative management of blunt splenic injury. Am Surg. 2007; 73: 897–902.

OMT:
Dr. Eduardo Paulina
GRACIAS