Ralacion Adreview y Potenciales Ventriculares

of 9
Transcript of Ralacion Adreview y Potenciales Ventriculares
-
7/29/2019 Ralacion Adreview y Potenciales Ventriculares
1/9
ORIGINAL ARTICLE
Relationship between late ventricular potentials
and myocardial 123I-metaiodobenzylguanidine scintigraphy
in patients with dilated cardiomyopathy with mild
to moderate heart failure: results of a prospective study
of sudden death events
Shu Kasama & Takuji Toyama & Yoshiaki Kaneko &
Toshiya Iwasaki & Hiroyuki Sumino & Hisao Kumakura &
Kazutomo Minami & Shuichi Ichikawa &
Naoya Matsumoto & Yuichi Sato &
Masahiko Kurabayashi
Received: 29 November 2011 /Accepted: 15 February 2012 /Published online: 14 March 2012# Springer-Verlag 2012
Abstract
Purpose Late ventricular potentials (LPs) are considered to
be useful for identifying patients with heart failure at risk of
developing ventricular arrhythmias. 123I-metaiodobenzyl-
guanidine (MIBG) scintigraphy, which is used to evaluate
cardiac sympathetic activity, has demonstrated cardiac sym-
pathetic denervation in patients with malignant ventricular
tachyarrhythmias. This study was undertaken to clarify the
relationship between LPs and 123I-MIBG scintigraphy find-
ings in patients with dilated cardiomyopathy (DCM).
Methods A total of 56 patients with DCM were divided into
an LP-positive group (n024) and an LP-negative group (n0
32). During the compensated period, the delayed heart/me-
diastinum count (H/M) ratio, delayed total defect score
(TDS), and washout rate (WR) were determined from 123I-
MIBG images and plasma brain natriuretic peptide (BNP)
concentrations were measured. Left ventricular end-diastolic
volume (LVEDV), left ventricular end-systolic volume
(LVESV), and left ventricular ejection fraction (LVEF) were
simultaneously determined by echocardiography.
Results LVEDV, LVESV, LVEF and plasma BNP concen-
trations were similar in the two groups. However, TDS was
significantly higher (358 vs. 286, p
-
7/29/2019 Ralacion Adreview y Potenciales Ventriculares
2/9
high WR, the incidence of sudden death events was higher
than that in other subgroups of DCM patients.
Keywords123I-MIBG . Late ventricular potentials .
Dilated cardiomyopathy
Introduction
Patients with idiopathic dilated cardiomyopathy (DCM) have
a high incidence of ventricular arrhythmias [1] and are at
increased risk of sudden death from ventricular tachycardia
(VT) and ventricular fibrillation [2]. The histopathological and
electrophysiological characteristics of ventricular arrhythmias
in idiopathic DCM are even less well defined than those of
coronary artery disease. A variety of factors may contribute to
the genesis of ventricular tachyarrhythmias in DCM patients.
Therefore, identification of patients with idiopathic DCM at
risk of malignant ventricular arrhythmias is very important for
optimal medical management.Late ventricular potentials (LPs) detected by signal-
averaged electrocardiography (ECG) in patients with VT are
caused by delayed and fragmented ventricular activation.
These LPs are used to identify patients at risk of life-
threatening arrhythmias, and indicate an increased risk of
malignant ventricular arrhythmias and sudden death in those
with ischaemic heart disease and congestive heart failure [3, 4].
Myocardial imaging with 123I-metaiodobenzylguanidine
(MIBG), an analogue of norepinephrine, is useful for detect-
ing abnormalities of the myocardial adrenergic nervous
system in DCM patients [57]. Cardiac sympathetic nerve
activity evaluated by 123I-MIBG scintigraphy has prognostic
value in these patients [7, 8]. Moreover, recent clinical
studies have suggested that 123I-MIBG imaging predicts
ventricular arrhythmias in patients with heart failure
[9, 10].
In the present study, we clarified the relationship between
LPs and the findings of 123I-MIBG scintigraphy in patients
with mild to moderate heart failure (i.e. patients at low risk
of sudden death events) due to DCM, and determined
whether the presence of LPs and the findings of123I-MIBG
scintigraphy are a reliable sudden death marker in these
patients.
Materials and methods
Patient population
We selected 56 patients with idiopathic DCM (left ventric-
ular ejection fraction, LVEF, 38 ms and
RMS40
-
7/29/2019 Ralacion Adreview y Potenciales Ventriculares
3/9
Twenty-four-hour Holter ECG
Twenty-four-hour Holter ECG monitoring with two leads was
conducted using an ambulatory ECG recorder (DMC-4502;
Nihon Koden, Tokyo, Japan). A modified Lowns classification
[16, 17] was employed to evaluate the severity of ventricular
arrhythmias, including premature ventricular contractions.
Echocardiography
Echocardiography was performed using the standard method
in a blinded manner. Two independent and experienced echo-
cardiographers who had no knowledge of the study, per-
formed all measurements. Left ventricular end-diastolic
volume (LVEDV), left ventricular end-systolic volume
(LVESV), and LVEF were calculated using the modified
method of Simpson [18].
123I-MIBG imaging
The 123I-MIBG imaging method has already been described
in detail [19, 20]. Briefly, 123I-MIBG was obtained from a
commercial source (FUJIFILM RI Pharma, Tokyo, Japan).
At 15 min and 4 h after injection, anterior planar and SPECT
images were obtained with a single-head gamma camera
(Millennium MPR; GE Medical Systems, Waukesha, WI).
The heart/mediastinum count (H/M) ratio was deter-
mined from the anterior planar delayed 123I-MIBG image.
The washout rate (WR) was calculated from early and
delayed planar images. Regional tracer uptake was assessed
semiquantitatively using a five-point scoring system (0 0
normal to 4 0 no uptake) in 17 segments on the delayed
SPECT image as recommended by the American Heart
Association [21]. The total defect score (TDS) was calcu-
lated as the sum of all defect scores.
Plasma BNP concentrations
Blood samples were collected into test tubes containing
EDTA after the subject had rested in the supine position
for at least 30 min. Plasma was separated by centrifugation
and then frozen at84C. Then the plasma BNP was mea-
sured with a specific immunoradiometric assay for human
BNP using a commercially available kit (Shionogi, Osaka,
Japan), as previously reported [22, 23].
Statistical analysis
Statistical analyses were performed using SPSS 16.0 for Win-
dows (SPSS, Chicago, IL). Numerical results are expressed as
means (SD). In all analyses, p
-
7/29/2019 Ralacion Adreview y Potenciales Ventriculares
4/9
difference was not statistically significant. The H/M ratio was
significantly lower in the LP-positive than that in the LP-
negative group (1.570.23 vs. 1.780.20, p
-
7/29/2019 Ralacion Adreview y Potenciales Ventriculares
5/9
the LP-positive and high WR group was significantly higher
than those in the LP-positive and low WR group (p
-
7/29/2019 Ralacion Adreview y Potenciales Ventriculares
6/9
LPs in 43% of their patients with DCM [31]. Similarly, LPswere seen in 24 of our 56 patients (42.9%). Furthermore,
based on Lowns classification, the incidences of ventricular
arrhythmias was significantly higher in the LP-positive than in
the LP-negative group.
Patients with DCM have been found to show impairment of
presynaptic catecholamine reuptake, which can be assessed
using the norepinephrine analogue 123I-MIBG and either planar
scintigraphy or SPECT [58]. Moreover, 123I-MIBG uptake is
reportedly reduced in patients with malignant ventricular
tachyarrhythmias [32, 33]. Schafers et al. reported that patients
with right ventricular outflow tract tachycardia exhibit reduced123I-MIBG uptake in the posterior left ventricular wall, which
indicates presynaptic dysfunction [32]. On the other hand, in
our study, segmental analysis of SPECT images showed im-
paired uptake in the inferior wall in both groups and this wasworse, though not significantly, in the LP-positive group.
Further studies are necessary to clarify the relationship be-
tween segmental denervation and malignant ventricular
tachyarrhythmias.
Yukinaka et al. found that defect scores, as evaluated by123
I-
MIBG scintigraphy after myocardial infarction, were signifi-
cantly greater in LP-positive than in LP-negative patients [34].
In their study, however, perfusion evaluated by99m
Tc perfusion
imaging did not differ between the two groups. Therefore, the
presence of LPs may be more closely related to the denervated
but viable myocardium (i.e. the mismatch area) in patients with
myocardial infarction. In this study, we evaluated the 99mTcperfusion imaging in about half of the patients. However, the
presence of LPs did not relate to the mismatch area (data not
shown). Moreover, there were no relationships between perfu-
sion defects and denervated myocardium in our DCM patients.
Therefore, our findings demonstrate that the mechanisms asso-
ciated with the presence of LPs in patients with myocardial
infarction may be different from those in DCM patients.
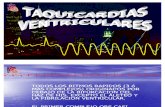
Incidenceofsuddendeath(%)
**
*
**
*:p
-
7/29/2019 Ralacion Adreview y Potenciales Ventriculares
7/9
In our study, 123I-MIBG scintigraphic parameters (TDS,
H/M ratio and WR) overlapped between the LP-positive and
LP-negative groups, and it was difficult to utilize these
parameters. Tamaki et al. reported that WR is the most
powerful predictor of sudden cardiac death in the failing
human heart, and this parameter may be associated with a
change in arrhythmia mechanisms of re-entry, automaticity,
which triggers activity that provokes lethal arrhythmias
[35]. In this study, the difference in WR between the two
groups was more marked than that of both TDS and H/M
ratio, and this parameter was also the most significant factor
predicting sudden death in our DCM patients. Furthermore,
in the LP-positive patients with high WR, the incidence of
sudden death events was higher than in other subgroups, and
this finding was confirmed by logistic regression analysis.
Accordingly, DCM patients who are both LP-positive and
have WR50% should receive with the most careful med-
ical management.
Study limitations
The small number of DCM patients in this study limited the
statistical power. In addition, signal-averaged ECG is
known to be useful for prognostic evaluation of serious
arrhythmic complications in patients with acute myocardial
infarction [13]. However, LPs are not used widely in
patients with nonischaemic congestive cardiomyopathy, as
its positive predictive value has been shown not to be high
enough [36]. Another study has shown that 123I-MIBG
scintigraphy, but not LPs, is a powerful predictor of sudden
cardiac death in patients with cardiomyopathy [35]. Our
findings demonstrate for the first time that LP positivity
together with a high WR could be the incremental predictor
of sudden death in DCM patients, but further studies are
required to confirm this hypothesis in a larger group of
patients. It is still unclear whether the presence of LPs
impairs cardiac sympathetic nerve activity, or whether im-
paired cardiac sympathetic nerve activity leads to the pres-
ence of LPs in patients with nonischaemic heart failure.
Therefore, further studies are necessary to clarify the rela-
tionship between the presence of LPs and impaired123
I-
MIBG uptake.
Conclusion
The TDS, H/M ratio and WR determined by cardiac 123I-
MIBG scintigraphy were worse in LP-positive than in LP-
negative DCM patients. However, echocardiographic
parameters, plasma BNP concentrations and NYHA func-
tional class were similar in the two groups. Furthermore, in
LP-positive patients with high WR, the incidence of sudden
death events was higher than in other subgroups. These
findings indicate that DCM patients who are LP-positive
and have a high WR as evaluated by 123I-MIBG scintigra-
phy must be followed especially carefully during medical
management.
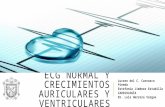
BA
Fig. 5 Delayed anterior planar 1123I-MIBG image (a) and signal-
averaged electrocardiogram (b) from an LP-negative patient. The
delayed H/M ratio and WR, as evaluated by 123I-MIBG, were 1.84%
and 42%, respectively. The f-QRS, LAS40 and RAM40 values were
98 ms, 29 ms and 84 V, respectively
1062 Eur J Nucl Med Mol Imaging (2012) 39:10561064
-
7/29/2019 Ralacion Adreview y Potenciales Ventriculares
8/9
Conflicts of interest None.
References
1. Kjekshus J. Arrhythmias and mortality in congestive heart failure.
Am J Cardiol. 1990;65(19):42I8I.
2. Packer M. Sudden unexpected death in patients with congestiveheart failure: a second frontier. Circulation. 1985;72(4):6815.
3. Ikeda T, Sakata T, Takami M, Kondo N, Tezuka N, Nakae T, et al.
Combined assessment of T-wave alternans and late potentials used
to predict arrhythmic events after myocardial infarction. A pro-
spective study. J Am Coll Cardiol. 2000;35(3):72230.
4. Steinberg JS, Berbari EJ. The signal-averaged electrocardiogram:
update on clinical applications. J Cardiovasc Electrophysiol.
1996;7(10):97288.
5. Henderson EB, Kahn JK, Corbett JR, Jansen DE, Pippin JJ, Kulkarni
P, et al. Abnormal I-123 metaiodobenzylguanidine myocardial wash-
out and distribution may reflect myocardial adrenergic derangement
in patients with congestive cardiomyopathy. Circulation. 1988;78(5
Pt 1):11929.
6. Schofer J, Spielmann R, Schuchert A, Weber K, Schluter M.
Iodine-123 meta-iodobenzylguanidine scintigraphy: a noninvasive
method to demonstrate myocardial adrenergic nervous system
disintegrity in patients with idiopathic dilated cardiomyopathy. J
Am Coll Cardiol. 1988;12(5):12528.
7. Merlet P, Valette H, Dubois-Rande JL, Moyse D, Duboc D, Dove P,
et al. Prognostic value of cardiac metaiodobenzylguanidine imaging
in patients with heart failure. J Nucl Med. 1992;33(4):4717.
8. Nakata T, Wakabayashi T, Kyuma M, Takahashi T, Tsuchihashi K,
Shimamoto K. Cardiac metaiodobenzylguanidine activity can pre-
dict the long-term efficacy of angiotensin-converting enzyme
inhibitors and/or beta-adrenoceptor blockers in patients with heart
failure. Eur J Nucl Med Mol Imaging. 2005;32(2):18694.
9. Akutsu Y, Kaneko K, Kodama Y, Li HL, Kawamura M, Asano T,
et al. The significance of cardiac sympathetic nervous system
abnormality in the long-term prognosis of patients with a history
of ventricular tachyarrhythmia. J Nucl Med. 2009;50(1):617.
10. Boogers MJ, Borleffs CJ, Henneman MM, van Bommel RJ, van
Ramshorst J, Boersma E, et al. Cardiac sympathetic denervation
assessed with 123-iodine metaiodobenzylguanidine imaging predicts
ventricular arrhythmias in implantable cardioverter-defibrillator
patients. J Am Coll Cardiol. 2010;55(24):276977.
11. Yamazaki J, Muto H, Kabano T, Yamashina S, Nanjo S, Inoue A.
Evaluation of beta-blocker therapy in patients with dilated cardiomy-
opathy clinical meaning of iodine 123-metaiodobenzylguanidine
myocardial single-photon emissioncomputed tomography. Am Heart
J. 2001;141(4):64552.
12. Toyama T, Hoshizaki H, Seki R, Isobe N, Adachi H, Naito S, et al.
Efficacy of amiodarone treatment on cardiac symptom, function,
and sympathetic nerve activity in patients with dilated cardiomy-
opathy: comparison with beta-blocker therapy. J Nucl Cardiol.
2004;11(2):13441.
13. Simson MB. Use of signals in the terminal QRS complex to
identify patients with ventricular tachycardia after myocardial in-
farction. Circulation. 1981;64(2):23542.
14. Nalos PC, Gang ES, Mandel WJ, Ladenheim ML, Lass Y, Peter T.
The signal-averaged electrocardiogram as a screening test for induc-
ibility of sustained ventricular tachycardia in high risk patients: a
prospective study. J Am Coll Cardiol. 1987;9(3):53948.
15. Worley SJ, Mark DB, Smith WM, Wolf P, Califf RM, Strauss HC,
et al. Comparison of time domain and frequency domain variables
from the signal-averaged electrocardiogram: a multivariable anal-
ysis. J Am Coll Cardiol. 1988;11(5):104151.
16. Meinertz T, Hofmann T, Kasper W, Treese N, Bechtold H, Stienen
U, et al. Significance of ventricular arrhythmias in idiopathic
dilated cardiomyopathy. Am J Cardiol. 1984;53(7):9027.
17. Schillaci G, Verdecchia P, Borgioni C, Ciucci A, Zampi I,
Battistelli M, et al. Association between persistent pressure
overload and ventricular arrhythmias in essential hypertension.
Hypertension. 1996;28(2):2849.
18. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R,
Feigenbaum H, et al. Recommendations for quantitation of the left
ventricle by two-dimensional echocardiography. American Societyof Echocardiography Committee on Standards, Subcommittee on
Quantitation of Two-Dimensional Echocardiograms. J Am Soc
Echocardiogr. 1989;2(5):35867.
19. Kasama S, Toyama T, Kumakura H, Takayama Y, Ichikawa S,
Suzuki T, et al. Effects of nicorandil on cardiac sympathetic nerve
activity after reperfusion therapy in patients with first anterior
acute myocardial infarction. Eur J Nucl Med Mol Imaging.
2005;32(3):3228.
20. Kasama S, Toyama T, Kumakura H, Takayama Y, Ichikawa S,
Suzuki T, et al. Effect of spironolactone on cardiac sympathetic
nerve activity and left ventricular remodeling in patients with
dilated cardiomyopathy. J Am Coll Cardiol. 2003;41(4):57481.
21. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S,
Laskey WK, et al. Standardized myocardial segmentation and
nomenclature for tomographic imaging of the heart: a statementfor healthcare professionals from the Cardiac Imaging Committee
of the Council on Clinical Cardiology of the American Heart
Association. Circulation. 2002;105(4):53942.
22. Kasama S, Toyama T, Kumakura H, Takayama Y, Ichikawa S,
Suzuki T, et al. Effects of candesartan on cardiac sympathetic nerve
activity in patients with congestive heart failure and preserved left
ventricular ejection fraction. J Am Coll Cardiol. 2005;45(5):6617.
23. Kasama S, Toyama T, Kumakura H, Takayama Y, Ichikawa S,
Suzuki T, et al. Effects of perindopril on cardiac sympathetic nerve
activity in patients with congestive heart failure: comparison with
enalapril. Eur J Nucl Med Mol Imaging. 2005;32(8):96471.
24. Kasama S, Toyama T, Sumino H, Kumakura H, Takayama Y, Minami
K, et al. Serial cardiac 123I-metaiodobenzylguanidine scintigraphic
studiesare more useful for predicting cardiacdeath thanone-time scan
in patients with chronic heart failure: sub-analysis of our previous
report. Nucl Med Commun. 2010;31(9):80713.
25. The CONSENSUS Trial Study Group. Effects of enalapril on
mortality in severe congestive heart failure. Results of the Coop-
erative North Scandinavian Enalapril Survival Study (CONSEN-
SUS). N Engl J Med. 1987;316(23):142935.
26. The SOLVD Investigators. Effect of enalapril on survival in
patients with reduced left ventricular ejection fractions and con-
gestive heart failure. N Engl J Med. 1991;325(5):293302.
27. Cohn JN, Johnson G, Ziesche S, Cobb F, Francis G, Tristani F, et
al. A comparison of enalapril with hydralazine-isosorbide dinitrate
in the treatment of chronic congestive heart failure. N Engl J Med.
1991;325(5):30310.
28. De Maria R, Gavazzi A, Caroli A, Ometto R, Biagini A, Camerini
F. Ventricular arrhythmias in dilated cardiomyopathy as an inde-
pendent prognostic hallmark. Italian Multicenter Cardiomyopathy
Study (SPIC) Group. Am J Cardiol. 1992;69(17):14517.
29. Josephson ME, Horowitz LN, Farshidi A. Continuous local elec-
trical activity. A mechanism of recurrent ventricular tachycardia.
Circulation. 1978;57(4):65965.
30. Poll DS, Marchlinski FE, Falcone RA, Josephson ME, Simson MB.
Abnormal signal-averaged electrocardiograms in patients with non-
ischemic congestive cardiomyopathy: relationship to sustained ven-
tricular tachyarrhythmias. Circulation. 1985;72(6):130813.
31. Denereaz D, Zimmermann M, Adamec R. Significance of ventric-
ular late potentials in non-ischaemic dilated cardiomyopathy. Eur
Heart J. 1992;13(7):895901.
Eur J Nucl Med Mol Imaging (2012) 39:10561064 1063
-
7/29/2019 Ralacion Adreview y Potenciales Ventriculares
9/9
32. Schafers M, Wichter T, Lerch H, Matheja P, Kuwert T, Schafers K,
et al. Cardiac 123I-MIBG uptake in idiopathic ventricular tachy-
cardia and fibrillation. J Nucl Med. 1999;40(1):15.
33. Paul M, Schafers M, Kies P, Acil T, Schafers K, Breithardt G, et al.
Impact of sympathetic innervation on recurrent life-threatening
arrhythmias in the follow-up of patients with idiopathic ventricular
fibrillation. Eur J Nucl Med Mol Imaging. 2006;33(8):86670.
34. Yukinaka M, Nomura M, Ito S, Nakaya Y. Mismatch between
myocardial accumulation of 123I-MIBG and 99mTc-MIBI and
late ventricular potentials in patients after myocardial infarction:association with the development of ventricular arrhythmias. Am
Heart J. 1998;136(5):85967.
35. Tamaki S, Yamada T, Okuyama Y, Morita T, Sanada S, Tsukamoto
Y, et al. Cardiac iodine-123 metaiodobenzylguanidine imaging
predicts sudden cardiac death independentl y of left ventricular
ejection fraction in patients with chronic heart failure and left
ventricular systolic dysfunction: results from a comparative study
with signal-averaged electrocardiogram, heart rate variability, and
QT dispersion. J Am Coll Cardiol. 2009;53(5):42635.
36. Bax JJ, Kraft O, Buxton AE, Fjeld JG, Parzek P, Agostini D, et al.
123I-mIBG scintigraphy to predict inducibility of ventricular
arrhythmias on cardiac electrophysiology testing: a prospectivemulticenter pilot study. Circ Cardiovasc Imaging. 2008;1(2):131
40.
1064 Eur J Nucl Med Mol Imaging (2012) 39:10561064