Situación Actual del Tratamiento Adyuvante en Cáncer de Mama · 12/11/2014 · In Node -negative...
66
Situación Actual del Tratamiento Adyuvante en Cáncer de Mama Luis Manso Hosp. Univ. 12 de Octubre Madrid
Transcript of Situación Actual del Tratamiento Adyuvante en Cáncer de Mama · 12/11/2014 · In Node -negative...

Situación Actual del Tratamiento Adyuvante en Cáncer de Mama
Luis MansoHosp. Univ. 12 de OctubreMadrid

AGENDA
• Factores Pronóstico y Predictivos.
• Quimioterapia.
• Hormonoterapia.
• ¿Se puede evitar la quimioterapia en algunas pacientes?
• Terapia anti-HER2.
• Hábitos de vida.

INTRODUCCIÓN
• El objetivo del tratamiento adyuvante es eliminar la enfermedad micro-metastásica.
Para empezar…
• No dispones de métodos para saber si tiene enfermedad micro-metastásica.
• Como no tiene enfermedad detectable, no puedes medir a corto plazo la eficacia de tu tratamiento.
• Gran parte de tu actividad se concentrará en un ejercicio de estimación de riesgos y probabilidad de mejora.
• Cada vez más tu paciente querrá participar en la gestión del riesgo.
Surg Gynecol Obstet. 1955 Jan;100(1):102-8.The cytologic demonstration and significance of tumor cells in the mesenteric venous blood in patients with colorectal carcinoma.FISHER ER, TURNBULL RB Jr.

Decisiones terapeúticas en el tratamiento adyuvante del cáncer de mama precoz:
En quién puede evitarse el tratamiento?
Qué tratamientoes el mejor?
Factores pronósticos Factores predictivos
INTRODUCCIÓN
ESTIMACIÓN DEL RIESGO: FR. PRONÓSTICOS
Histología
Tamaño
Grado
Ganglios
RRHH
HER 2
TNM
Edad / Estado menopáusico
Co-morbilidad
ESTIMACIÓN DEL RIESGO: FR. PREDICTIVOS
Histología
Tamaño
Grado
Ganglios
RRHH
HER 2
TNM

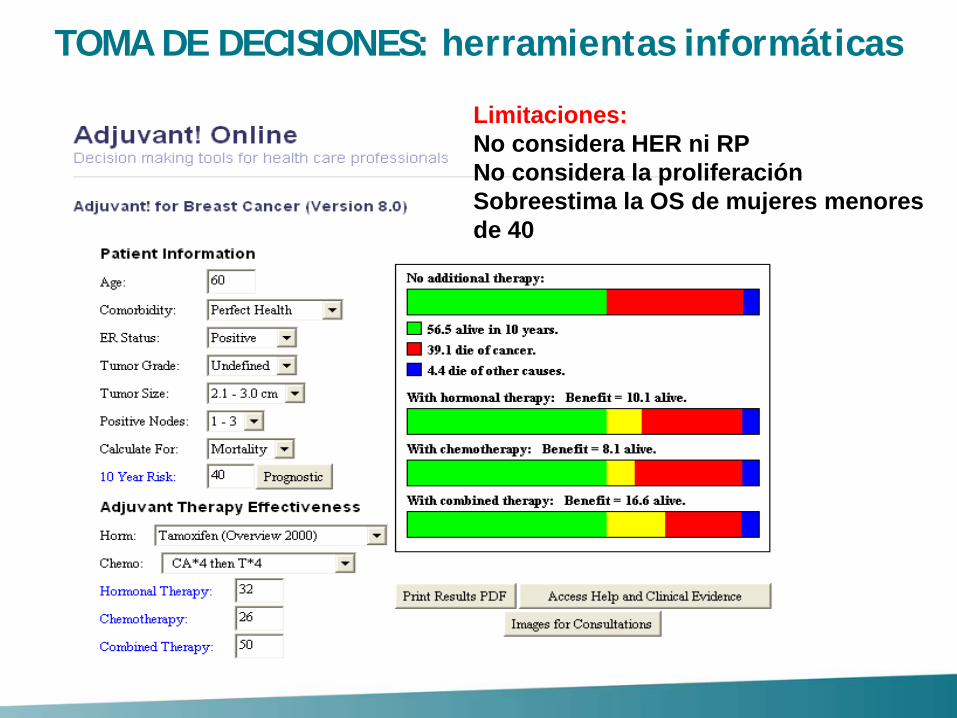
TOMA DE DECISIONES: herramientas informáticas
TOMA DE DECISIONES: herramientas informáticas
Limitaciones:No considera HER ni RPNo considera la proliferaciónSobreestima la OS de mujeres menores de 40

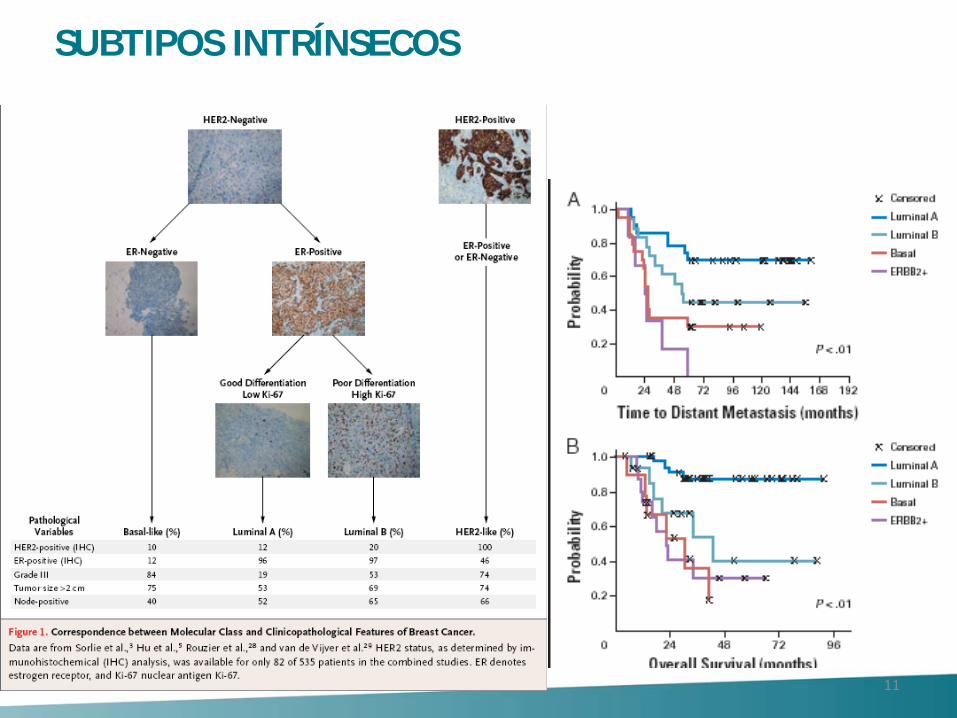
• Perou et al. in 2000 identified tumors with distinct patterns of gene expression that they termed “basal type” and “luminal type” using complementary DNA (cDNA) microarrays to analyze breast-cancer tissue.
• These subgroups differ with respect to the outcome of disease in patients with locally advanced breast cancer.
Molecular portraits of human breast tumoursCharles M. Perou Nature 406, 747-752 (17 August 2000)

11
SUBTIPOS INTRÍNSECOS
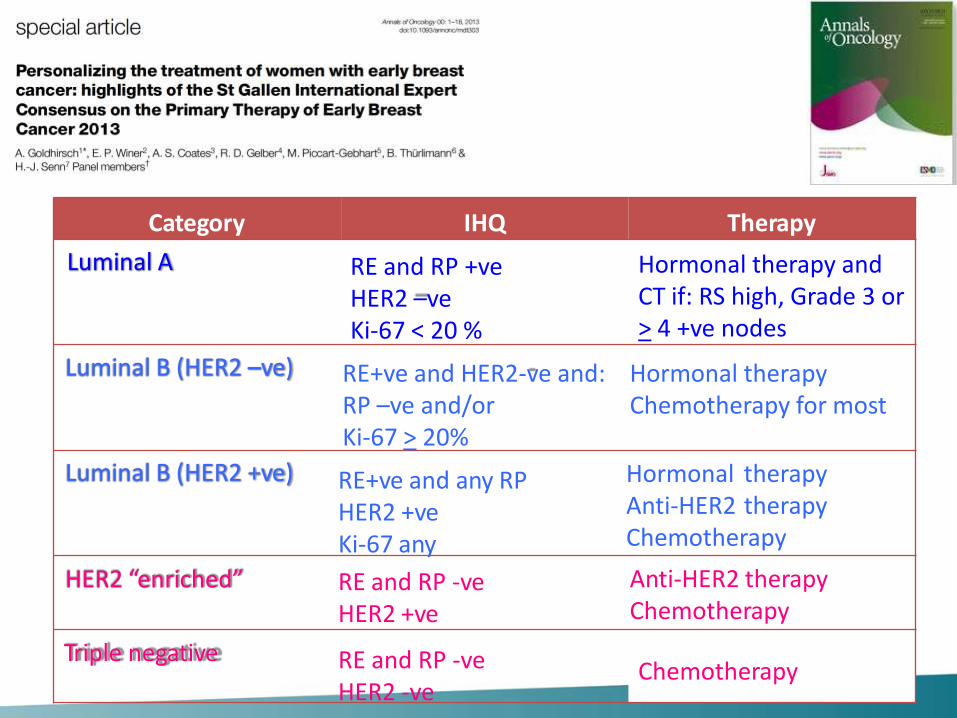
Category IHQ Therapy
RE and RP +ve HER2 –veKi-67 < 20 %
Hormonal therapy and CT if: RS high, Grade 3 or> 4 +ve nodes
RE+ve and HER2-ve and: RP –ve and/orKi-67 > 20%
Hormonal therapy Chemotherapy for most
RE+ve and any RPHER2 +veKi-67 any
Hormonal therapyAnti-HER2 therapyChemotherapy
RE and RP -veHER2 +ve
Anti-HER2 therapyChemotherapy
RE and RP -ve HER2 -ve
Chemotherapy
Luminal B (HER2 –ve)
Luminal A
Luminal B (HER2 +ve)
Triple negative
HER2 “enriched”
Quimioterapia

• Indicada en (casi) todas las pacientes con tumores triple negativo o HER2 positivo, y en la mayoría de pacientes luminal B (Ki-67 elevado y/o RP negativo y/o grado 3).
• Se recomienda usar el mejor esquema de quimioterapia disponible.
CONCEPTOS BÁSICOS

1970-1985 1985-1997 1998?
CMF-like Oral
IV6 meses1 año+/- Prednisona+/- Vincristina
Antraciclinas
Adriamicina Epirubicina Dosis bajas Dosis altas 4-6 ciclos+/- 5-FU
Taxanos
Paclitaxel Docetaxel Concurrente Secuencial
HISTORIA

Courtesy: Martine Piccart
Discordancia en el tratamiento adyuvante
40 expertos internacionales
61 añosPostmenopaúsica
Ca ductal infiltrante grado 2
pT1b (0,9cm) N0 M0
RE – RP – HER2 -
48%
25%
15%
4%8%
0%
10%
20%
30%
40%
50%
60%
NONE CMFx6 ACx4 TAM OTHER

El empleo de poliquimioterapia con antraciclinas por 6 ciclos tipo CAF/FEC versus no quimioterapia reduce el riesgo de muerte en un 36% (RR 0·64, SE 0·09, 2p<0·0001), y es superior a lo obtenido con 4AC (RR 0·78, SE 0·09, 2p=0·01) o CMF estándar (RR 0·76, SE 0·05, 2p<0·0001).

Los esquema que aumentan la duración de quimioterapia añadiendo taxano secuencial a un esquema de antraciclinas igual al brazo control reducen el riesgo de muerte por cáncer de mama en un 14% (RR 0·86, SE 0·04, 2p=0·0005) (Ganancia a 8 años de 2.8%)


Disminución del riesgo de recurrencia con HR entre 0.63 y 0.97, con p significativa en 7/13 estudios. P < 0.00001 en el análsis global
Disminución del riesgo de muerte con HR entre 0.76 y 0.91, P < 0.0001
No diferencias entre paclitaxel y docetaxel, y entre esquemas secuenciales o concomitantes
En administración concomitante no existe significancia estadística en SG. Gran heterogeneidad de los estudios.
No diferencias en el análisis por subgrupos:-Expresión de RE -Afectación nodal -Edad -Estado menopáusico
Laurentiis M et al. J Clin Oncol 2008 26: 44-53
● Indicación adyuvancia con QT individualizada según paciente y subtipo (factores pronósticos y predictivos).
● Taxanos y antraciclinas como estándar de tratamiento.
• La mejor forma de administrar paclitaxel secuencial es semanal y de docetaxel es cada 21 días.
– ECOG 1199. N Engl J Med 2008• No existen diferencias entre esquema secuencial (ACx4->Docx4)
vs concurrente (TACx6)
– BCIRG 005. Eiermann et al. J Clin Oncol 2011
RESUMEN QUIMIOTERAPIA ADYUVANTES
● Un esquema corto tipo ATx4 o TACx4 resulta inferior a un esquema largo tipo ACx4_>Docx4
– NSABP B-30. N Eng J Med 2010
● No factores predictivos de respuesta establecidos a antraciclinas ni a taxanos.
● Ajustar QT por riesgo de efectos secundarios: Toxicidad cardiaca de antraciclinas. Monitorización.
RESUMEN QUIMIOTERAPIA ADYUVANTES

Hormonoterapia

• Bloqueo del receptor: SERM– TAMOXIFENO
• Degradación del receptor:– FULVESTRANT
• Reducción de síntesis:– Inhibidores de aromatasa (postmenopausica)
• Esteroideos: EXEMESTANO• No esteroideos: ANASTROZOL, LETROZOL
– Ablación de función ovárica (premenopaúsicas)• OOFORECTOMÍA, RADIOTERAPIA• ANÁLOGOS LHRH (goserelina, triptorelina)
TRATAMIENTO HORMONAL

Tamoxifeno 20 mg/día 5 años tras tratamiento con QT reduce RIESGO RECURRENCIA 39% a 15 años y RIESGO DE
MUERTE por CM 30% a los 15 años
Recaída 39% Muerte 30%

Even in marginally ER-positive disease (10–19 fmol/mg cytosol protein) the recurrence
reduction was substantial (RR 0·67 [SE 0·08])

Ri. Recaída 25% Ri. Muerte 29%
12894 pts include / Analysis of 6846 ER+ (53%)

Gray et al. ASCO, 2013

Type: Evidence-Based, Evidence Quality: High, Strength of Recommendation:Strong
Tamoxifeno 10 años
IA 5 años
TAM 5 años IA 5 años
TAM 2-3años IA completar 5 años
Adyuvancia en Postmenopausia
IA 2-3 años
Type: Informal consensus, Evidence Quality: Low, Strength of Recommendation: Weak;
TAM completar 5 años
ATACBIG 1.98TEAM
ATLASaTTom
IESITAARNO-95ABSCGBIG 1.98
MA.17
BIG 1.98

Cohorte1:5 años de IA versus 5 años de
tamoxifeno
Cohorte 2: 2-3 años de tamoxifeno seguido de 2-3 años de IA versus 5 años de tamoxifeno
Con la estrategia switch tras 2-3 años existe una marcada reducción del riesgo de recaída (del 40%) en los 3 años siguientes de seguimiento y mejoría discreta de la supervivencia global del 0.7%, estadísticamente significativa, que no se evidencia en el grupo de terapia up front.

↓ Contralateral BC↓ Deep vein thrombosis↓ Endometrial cancer↓ Hot flashes
↑Arthralgia/myalgia(farmacodinamic factor?)
↑ Bone fractures↑ Cardiovascular events
AI
↓Contralateral BC↓Osteoporosis risk↓Myalgia↓Hyperlipidemia
↑ Hot flashes↑ Thromboembolism↑ Endometrial cancer↑ Gynaecologic adverse effects
Tamoxifen
Amir E. J Natl Cancer Inst. 2011 Sep 7;103 (Meta-analysis)
ADYUVANCIA HORMONAL EN PREmenopausicas
• Tamoxifeno 20 mg/día durante 5-10 años es el estándar en pacientes premenopaúsicas RE+.
• En pacientes jóvenes que no quedan amenorreicas tras la quimioterapia se debe valorar la supresión de la función ovárica (meta-análisis. Lancet 2007).
• Aún no está definido el papel de análogos en presencia de tamoxifeno (estudio SOFT confirmará este planteamiento)
Pre-ASCO 2014 / Pre-SABCs 2014
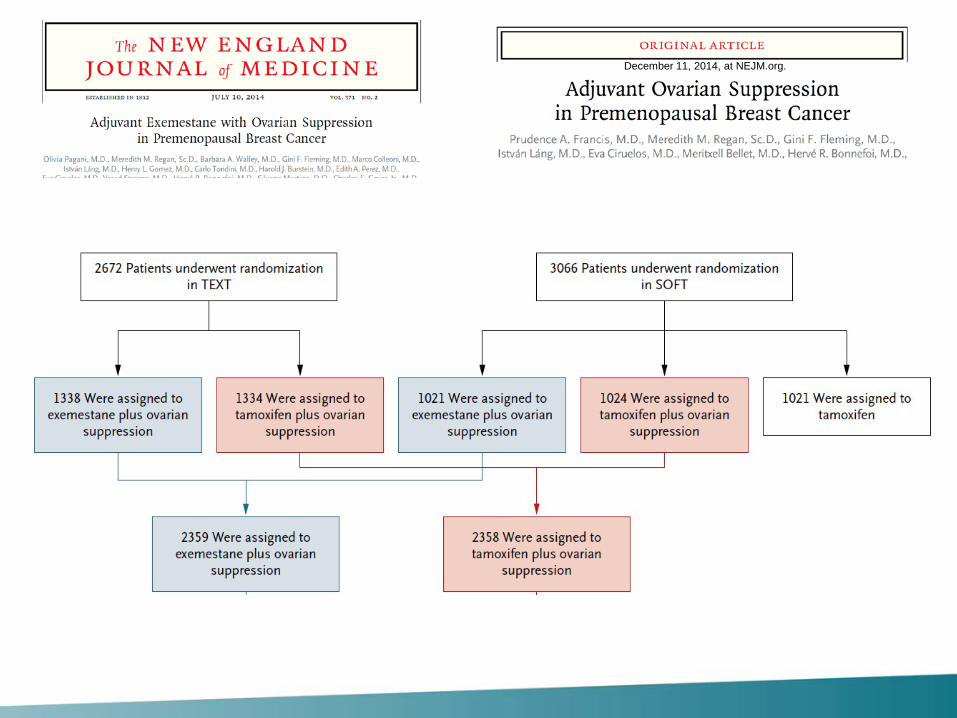
December 11, 2014, at NEJM.org.

95.9 %vs
96.9%
92.8 % vs
88.8%91.1 %
vs87.3%
93.8 %vs
92.0%
NEJM, June 1, 2014

December 11, 2014, at NEJM.org.

ADYUVANCIA HORMONAL EN PREmenopausicas
• Tamoxifeno 20 mg/día durante 5-10 años es el estándar en pacientes premenopaúsicas RE+.
• En pacientes jóvenes (<35 años) y/o no quedan amenorreicas tras la quimioterapia se debe plantear tratamiento con exemestano + análogo
Post-ASCO 2014 / Post-SABCs 2014

Paciente de 59 años postmenopáusica Carcinoma ductal infiltrante grado 2 T1c (17 mm)N0RE 90%; RP 90%; HER2 negativoKi-67 4%
¿Se puede evitar la quimioterapia en pacientes hormono-dependientes?

T1 N0 RE+ Grado 2
Exceso de toxicidad y costes
Courtesy: Peter Ravdin
Necesario tratar 100 casos para beneficiar
sólo a uno

• Genomic Grade• Mamaprint (70-gene)
• Oncotype DX (21-gene)• PAM50 (50-gene)• Rotterdam (76-gene)
• ….• 115 firmas genéticas publicadas (“Meta-analysis”.
Fan….and C. Perou. BMC medical genetics 2011)
¿De qué TEST Riesgo Recaída disponemos?

The three most commonly used molecular
prognostic profiles are:
a 70-gene assay (MammaPrint)
a 21-gene assay (Oncotype DX).
a 50-gene assay (PAM 50)
“Prognostic” and “predictive” tools
¿De qué TEST Riesgo Recaída disponemos?

MRT-PCR. Oncotype DX, analiza 21 genes, 16 de ellos relacionados con el tumor y 5 genes de referencia, calculando un índice de recurrencia (RS), que clasifica a las pacientes en 3 grupos de riesgo: bajo, intermedio y alto.
TAILORx

Van’t Veer publicó por primera vez la identificación mediante análisis de microarrays de un perfil de expresión de 70 genes como factor pronóstico de desarrollo de metástasis en mujeres con cáncer de mama estadio T1-T2, sin afectación nodal al diagnóstico.
Vijver publicó el beneficio de este perfil de expresión génica en mujeres con afectación ganglionar y su superioridad como factor predictivo respecto a criterios clínicos e histológicos clásicos
TRANSBIG validación en estudio retrospectivo

La validación retrospectiva propició el desarrollo de un estudio prospectivo, multicéntrico y randomizado, llamado MINDACT (Microarray In Node-negative and 1-3 node positive Disease may Avoid ChemoTherapy), con reclutamiento de 6600 pacientes con cáncer de mama sin afectación ganglionar
Los factores clinicopatológicossupraestiman el riesgo de recaída, y por tanto, la necesidad de quimioterapia, en un 8.25% de los casos (42% vs. 34%, p<0.0001) respecto a Mammaprint

• The Predictor Analysis of Microarray 50 (PAM50) uses a risk of recurrence (ROR) score generated from the 50-gene PAM50 test that was developed to identify intrinsic breast cancer subtypes.
• ROR is derived from the expression profile of these 50 genes, with special weighting given to a set of proliferation-associated genes and with a function of tumor size added.
• Results from the PAM50 are used to generate the risk of recurrence (ROR) score, which can stratify patients into high, medium, and low subsets.
• The test can be performed on formalin-fixed paraffin-embedded tissue by techniques such as quantitative real-time reverse transcription-PCR (qRT-PCR).
• While not available for use in the US, it is available in the European Union.
Prosigna™ assay

• The ROR was significantly predictive of prognosis among patients with node-negative breast cancer.

HER-2 +3 FISH +
Tratamiento de pacientes HER-2

• The Benefit
• Duration
• Concurrent vs. Sequential
• Cardiac toxicity
• Role of Non-Anthracycline Combination
TRATAMIENTO ADYUVANTE ANTI-HER2

• The Benefit
• Duration
• Concurrent vs. Sequential
• Cardiac toxicity
• Role of Non-Anthracycline Combination
TRATAMIENTO ADYUVANTE ANTI-HER2
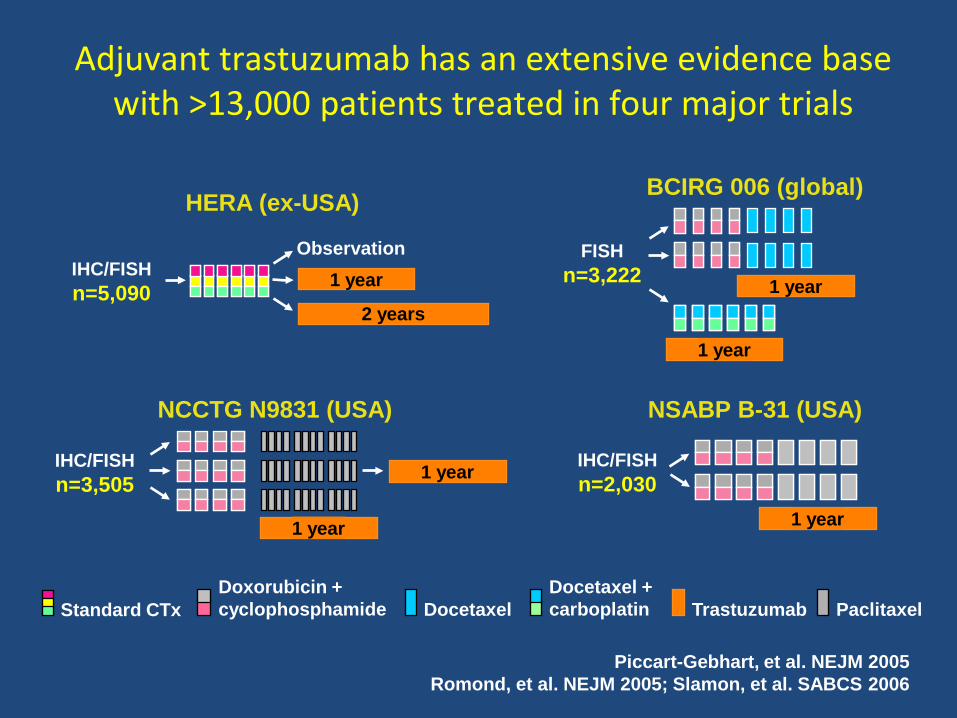
Adjuvant trastuzumab has an extensive evidence base with >13,000 patients treated in four major trials
Piccart-Gebhart, et al. NEJM 2005 Romond, et al. NEJM 2005; Slamon, et al. SABCS 2006
NCCTG N9831 (USA)
BCIRG 006 (global)
NSABP B-31 (USA)
IHC/FISH n=3,505
1 year
FISHn=3,222
IHC/FISH n=2,030
DocetaxelDocetaxel + carboplatin
Doxorubicin + cyclophosphamide TrastuzumabStandard CTx Paclitaxel
HERA (ex-USA)
IHC/FISH n=5,090
Observation
2 years
1 year
1 year 1 year
1 year
1 year

. N Engl J Med. 2005;353: 1659-1672.

Trastuzumab provides DFS benefit irrespective of node involvement
N = node
1–3+ nodes
Favours trastuzumab
Favours no trastuzumab
0 0.5 2.51.0 1.5 2.0
1–3+ nodes≥4+ nodesNot assessed
N9831/B-31 N–
4–9+ nodes>10+ nodes
DCarboH N–N+
N+
BCIRG 006 N–ACDH
N–HERA
HR
Slamon, et al. SABCS 2006 Perez, et al. ASCO 2007; Smith, et al. Lancet 2007
32 % N0
7% N0
29% N0
29% N0

• The Benefit
• Duration
• Concurrent vs. Sequential
• Cardiac toxicity
• Role of Non-Anthracycline Combination
TRATAMIENTO ADYUVANTE ANTI-HER2

M. Piccart et al. SABCS 2012

FinHer (Finland Herceptin)N Enlg J Med 23 Feb 2006 J Clin
Oncol Dec 2009
9 semanas de trastuzumab

Neratinib after adjuvant chemotherapy and trastuzumab in HER2-positive early breast cancer: Primary analysis at 2 years of a phase 3, randomized, placebo-controlled trial (ExteNET).
• The Benefit
• Duration
• Concurrent vs. Sequential
• Cardiac toxicity
• Role of Non-Anthracycline Combination
TRATAMIENTO ADYUVANTE ANTI-HER2


• The Benefit
• Duration
• Concurrent vs. Sequential
• Cardiac toxicity
• Role of Non-Anthracycline Combination
TRATAMIENTO ADYUVANTE ANTI-HER2


Rastogy. ASCO 2007
cardiac toxicity is reversible
B-31 B-9831
Edith Perez. JCO 2008

B-31• Age (> 50)• Anti-hypertensive medication• Basal LVEF < 54• Post-AC LVEF < 54
N9831• Age (> 60)• Anti-hypertensive medication• Basal LVEF < 55
Factors associated to CHF

• The Benefit
• Duration
• Concurrent vs. Sequential
• Cardiac toxicity
• Role of Non-Anthracycline Combination
TRATAMIENTO ADYUVANTE ANTI-HER2



Muchas gracias
• Luis Manso Sánchez– [email protected]
• Servicio Oncología Médica. Hospital Universitario 12 de Octubre, Avd. Córdoba sn 28041 Madrid.




![CAMBIO PASO A PASO HORARIO · node—derechos_pecuniarios.tpl.php C] node—direccion-l.tpl.php C] node—direccion.tpl.php C] node—direction.tpl.php C] node—evento.tpl.php](https://static.fdocuments.es/doc/165x107/5c77371209d3f23a068b779a/cambio-paso-a-paso-horario-nodederechospecuniariostplphp-c-nodedireccion-ltplphp.jpg)