Un Mejor Camino Para Los Beneficios II... · UNA EMPRESA TAN COMO USTED TRABAJAMOS EN BENEFICIO DE...
21
RESUMEN de DOMINION NATIONAL Un Mejor Camino Para Los Beneficios
Transcript of Un Mejor Camino Para Los Beneficios II... · UNA EMPRESA TAN COMO USTED TRABAJAMOS EN BENEFICIO DE...

RESUMEN de DOMINION NATIONAL
Un Mejor Camino Para Los Beneficios

Dominion National reconoce que usted es un persona única y hemos diseñado planes y programas que trabajan para usted. Buscamos una mejor manera de servirle a través de planes personalizados y un servicio excepcional para que pueda centrarse en lo que lo hace extraordinario y satisfecho.
únicaUNA EMPRESA TAN
COMO USTED
TRABAJAMOS EN BENEFICIO DE MÁS DE 875,000 MIEMBROS1, PROPORCIONANDO:
El grupo de compañías Dominion National incluye a Dominion Dental Services, Inc., una entidad emisora autorizada de planes dentales, y a Dominion Dental Services USA, Inc., un administrador autorizado de los beneficios dentales y de la vista. Los planes del cuidado de la vista están asegurados por la Avalon Insurance Company.
DN.SB.S.082417
UN COMPROMISO CON LA SATISFACCION DEL MIEMBRO En una nuestra encuesta de satisfacción del miembro reciente,
el 96% de los encuestados estaban satisfechos con el dominio como su plan dental.2
ACCESO LAS 24 HORAS SIN
COSTO al 888.518.5338Está disponible la información de elegibilidad y reclamos para los
miembros, los administradores de beneficios y dentistas.
ACCESO LA INFORMACIÓN DEL PLAN EN LINEALa aplicación móvil MyDominion y el sitio web
https://DominionMembers.com proporciona a los miembros un acceso fácil a la información de la cuenta y del plan.
Encontrar un Dentista
Ver las Tarjetas de Identificación
Ver la Información del Plan
Calculador de costo dental (solo sitio web)
La aplicación MyDominion se puede descargar a través de nuestro sitio web en DominionNational.com/mobile.
AMPLIAS REDES1
La red Choice PPO ofrece acceso a más de 290,000 odontólogos a nivel nacional.1
Las redes Elite PPO y Elite PPO ePPO proporcionan una flexibilidad sin igual y menores costos fuera de su bolsillo.
La red del Select Plan estilo DHMO es una de las más grandes de la región del Atlántico Medio.3
Una red de visión líder con un directorio de más de 60,000 proveedore.1
Para encontrar un proveedor participante, por favor visite DominionNational.com.
1 Informe de junio de 2017 sobre el demepeno interno de Dominion National. Los dentistas participantes están sujetos a cambio.2 Encuesta de satisfacción del miembro de Dominion National, noviembre de 2016.3 Igual que un plan DHMO con copagos fijos de los miembros, sin límites máximos anuales de dinero, sin periodos de espera, sin deducibles, sin papeleo previo a la
autorización o estimaciones previas al tratamiento y sin formularios de reclamación (excepto en casos de emergencias fuera del área). Encuesta de la red nacional de competitividad de Dominion National, 1 trimestre de 2017. La región atlántica central incluye D.C., Delaware, Maryland, Pennsylvania, y Virginia. Los dentistas participantes están sujetos a cambio.
~

BENEFICIOACCESS ePPO SCHEDULE C2
CHOICE PPO
Dentro de la Red
Fuera de la Red
DIAGNÓSTICO & PREVENTIVO
Exámenes orales Vea la lista de honorarios 100% 100%
Radiografías de aleta de mordida Vea la lista de honorarios 100% 100%
Aplicación de fluoruro para niños Vea la lista de honorarios 100% 100%
Dos (2) limpiezas semestrales de dientes Vea la lista de honorarios 100% 100%
Sellantes Vea la lista de honorarios 100% 100%
RESTAURACIONES BÁSICASEmpastes (amalgama y resina) Vea la lista de honorarios 90% 80%
Extracción de diente brotado Vea la lista de honorarios 90% 80%
PERIODONCIARaspado radicular y terapia Vea la lista de honorarios 90% 80%
ENDODONCIA
Conducto radicular Vea la lista de honorarios 90% 80%
CIRUGÍA BUCALExtracción de dientes impactados Vea la lista de honorarios 90% 80%
RESTAURACIÓN MAYORCoronas y puentes Vea la lista de honorarios 60% 50%
Prótesis Vea la lista de honorarios 60% 50%
Implantes Vea la lista de honorarios 60% 50%
ORTODONCIA Consulte el folleto del Programa de Descuentos para Ortodoncia a fin de
obtener más detalles
Consulte el folleto del Programa de Descuentos para Ortodoncia a fin de
obtener más detalles
LÍMITE DE EDAD PARA ORTODONCIA
MÁXIMO DE ORTODONCIA EN LA VIDA
CARGO POR VISITA AL CONSULTORIO DEL MÉDICO N/A N/A
DEDUCIBLE POR AÑO CALENDARIO (eliminado para el diagnóstico y preventivo)Individual $25 $25
Familiar $75 $75
MÁXIMO ANUAL POR AÑO CALENDARIO $2,000 $2,000
TRANSFERENCIA MÁXIMA ANUAL Hasta $1,500 Hasta $1,500
PERIODOS DE ESPERA Ninguno Ninguno
FORMULARIOS DE RECLAMO Sí Sí
RECIBIR ATENCIÓN DE Access/Elite ePPO dentistaCualquier dentista o Choice PPO dentista
SUBSIDIOS FUERA DE LA RED1 Ninguno 80th
IDENTIFICACIÓN DEL PLAN 3241 2972
ESDC II
OPCIÓN DUALRESUMEN DE BENEFICIOSDominionNational.com
SM
LOS BENEFICIOS DENTALES
1 Dispendios fuera de la Red: Limitación sobre un precio facturado, conforme lo determine el Plan, según el área geográfica donde se incurre en los gastos. Tenga presente que cuando se usan los servicios de la red, los miembros pueden incurrir en cualquier gasto que exceda la cantidad permitida.
Esta póliza incluye limitaciones, exclusiones y términos bajo los cuales puede seguir estando vigente o ser descontinuada. Para conocer los costos y detalles de la cobertura completa, comuníquese con su administrador de beneficios.

El plan de servicios dentales está asegurado por Dominion Dental Services, Inc. d/b/a Dominion National.
t
¿CÓMO ME INSCRIBO?
1. Llene la tarjeta de inscripción adjunta y anote
todos los dependientes que desea que estén
cubiertos.
• Asegúrese de marcar la casilla del plan
adecuado.
2. Devuelva la credencial de inscripción llena a su
Administrador de Beneficios o según se le
instruya.
3. En o antes de su primer día de elegibilidad, se le
enviará una tarjeta de membresía, la descripción
de los beneficios y el certificado de la cobertura.
4. Si tiene alguna pregunta en cuanto a su fecha
de elegibilidad, póngase en contacto con su
Administrador de Beneficios.
¿QUIÉN ES ELEGIBLE?
Usted y sus dependientes son elegibles. Los
dependientes incluyen a su cónyuge e hijos solteros
menores de 26 años. Consulte sus documentos de la
póliza para obtener información adicional en cuanto a
la cobertura de sus dependientes.
¿CÓMO ENCUENTRO A UN DENTISTA PARTICIPANTE?
Para ver una lista completa de los dentistas
participantes, por favor visite DominionNational.com/
find-a-dentist.
¿CÓMO PRESENTO UN RECLAMO DEL PPO PLAN?
Los beneficios le serán pagados a usted o podrán ser
adjudicados directamente a su dentista. Su dentista
podrá usar el formulario estándar de reclamos de la
Asociación Dental Americana. Los reclamos podrán
ser presentados electrónicamente y enviándolos a:
Dominion National, P.O. Box 1126, Elk Grove Village, IL
60009; Or Faxed To: 888.208.8290.
¿PUEDO HACER CAMBIOS EN LÍNEA?
Sí. Dominion provee a los miembros un acceso seguro
en línea a:
• Tarjetas de identificación
• Información sobre el Plan
• Búsqueda de dentistas
• Calculadora del costo de los servicios dentales
• Información de contacto
• Peticiones de servicios de parte del miembro y
correspondencia general
Todos los cambios son confirmados a través de correo
electrónico con devolución a su remitente. Para
obtener más información, visite DominionNational.com.
¿TIENE DOMINION UNA APLICACIÓN MÓVIL?
Sí. La aplicación móvil MyDominion proporciona a los
miembros un acceso fácil a la información de la cuenta
y del plan. Con MyDominion, usted podrá:
• Encontrar un dentista
• Ver tarjetas de identificación
• Ver la información del plan
Para obtener más información, visite DominionNational.
com/mobile.
¿QUÉ PASA SÍ CAMBIO DE EMPLEO?
Sí deja su centro de trabajo actual, tendrá la opción
de convertir su cobertura a un programa de Dominion
alterno usando un método de pago diferente.

ADA CUSTOMARY MEMBERCODE PROCEDURE DESCRIPTION FEE* FEE**
D0100-D0999 DIAGNOSTIC
CLINICAL ORAL EXAMINATIONSD0120 Periodic oral evaluation – established patient (once every 6 months) $45.00 $0.00D0140 Limited oral evaluation – problem focused (not to exceed 3 in 6 months) $65.00 $0.00D0145 Oral evaluation for a patient under three years of age and counseling with primary $60.00 $0.00
caregiver (once every 6 months for child age 3 or under)D0150 Comprehensive oral evaluation – new or established patient for first encounter with the $70.00 $0.00
dentist/dental office (once per 60 months)D0160 Detailed and extensive oral evaluation – problem focused, by report (once per 60 months) $143.00 $0.00D0170 Re-evaluation – limited problem focused (established patient; not a post-op visit; $65.00 $0.00
not to exceed 3 in 6 months)D0180 Comprehensive periodontal evaluation – new or established patient (once per 60 months) $110.00 $0.00
RADIOGRAPHSD0210 Intraoral – complete series including bitewings (once in 60 months) $125.00 $0.00D0220 Intraoral periapical – first film $22.00 $0.00D0230 Intraoral periapical – each additional film $22.00 $0.00D0240 Intraoral occlusal film (2 per 6 months) $30.00 $0.00D0250 Extraoral – first film (2 per 6 months) $45.00 $0.00D0260 Extraoral – each additional film (2 per 6 months) $22.00 $0.00D0270 Bitewing – single film (one series without duplication per 6 months) $22.00 $0.00D0272 Bitewings – two films (one series without duplication per 6 months) $35.00 $0.00D0273 Bitewings – three films (one series without duplication per 6 months) $40.00 $0.00D0274 Bitewings – four films (one series without duplication per 6 months) $60.00 $0.00D0277 Vertical bitewings – 7 to 8 films (one series without duplication per 6 months) $98.00 $0.00D0290 Posterior/anterior or lateral skull and facial bone survey film (when dentally necessary) $85.00 $0.00D0330 Panoramic film (once in 60 months) $125.00 $0.00
TESTS AND EXAMINATIONSD0460 Pulp vitality tests (per visit, not per tooth, for emergencies) $40.00 $0.00
UNSPECIFIED DIAGNOSTIC PROCEDURE, BY REPORTD0999 Chlorhexidine mouth rinse or fluoride toothpaste (twice per year for 2 years; covered only $15.00 $0.00
following scaling and root planing (a deep cleaning) and must be dispensed in the dentist's office.)
D1000-D1999 PREVENTIVE
D1110 $80.00 $0.00D1120
DENTAL PROPHYLAXIS (ROUTINE CLEANING) Prophylaxis – adult, age 14 and over (2 cleanings every 12 months) Prophylaxis – child, under age 14 (2 cleanings every 12 months) $55.00 $0.00
TOPICAL FLUORIDE TREATMENT (once per 6 months)D1203 Topical application of fluoride (excluding prophylaxis), child up to 14th birthday $30.00 $0.00D1204 Topical application of fluoride (excluding prophylaxis), adult up to 19th birthday $36.00 $0.00D1206 Topical application of fluoride varnish up to 19th birthday $30.00 $0.00
OTHER PREVENTIVE SERVICESD1351 Sealant on unrestored permanent molars – per tooth (once per 4 years through age 15, $40.00 $17.00
or up to age 19 when decay in molar)
SPACE MAINTENANCE (passive applicances)D1510 Space maintainer – fixed unilateral (once per quadrant per lifetime for children under $300.00 $95.00
age 14 for replacement of primary or permanent posterior teeth)D1515 Space maintainer – fixed bilateral (once per arch per lifetime for children under age 14 $450.00 $105.00
for replacement of primary or permanent posterior teeth)D1520 Space maintainer – removable unilateral (once per quadrant per lifetime for children under $300.00 $95.00
age 14 for replacement of primary or permanent posterior teeth)D1525 Space maintainer – removable bilateral (once per arch per lifetime for children under $450.00 $115.00
age 14 for replacement of primary or permanent posterior teeth)D1550 Recementation of space maintainer (once per arch or quadrant for children under age 14) $55.00 $30.00D1555 Removal of fixed space maintainer (once per arch or quadrant for children under age 14) $55.00 $30.00
SYMBOL KEY* The listed Customary Fee is for illustrative purposes only. Customary fees may vary by dentist and by geographic area.** Member Fee when performed by a Participating Dentist.Current Dental Terminology © 2009 American Dental Association. All rights reserved.
Access ePPO Member Fee Schedule C2

ADA CUSTOMARY MEMBERCODE PROCEDURE DESCRIPTION FEE* FEE**
SYMBOL KEY* The listed Customary Fee is for illustrative purposes only. Customary fees may vary by dentist and by geographic area.** Member Fee when performed by a Participating Dentist.Current Dental Terminology © 2009 American Dental Association. All rights reserved.
D2000-D2999 RESTORATIVE
AMALGAM RESTORATIONS (includes polishing; one filling per tooth per surface within 24 months)D2140 Amalgam, one surface – primary or permanent $150.00 $20.00D2150 Amalgam, two surfaces – primary or permanent $175.00 $30.00D2160 Amalgam, three surfaces – primary or permanent $220.00 $40.00D2161 Amalgam, four or more surfaces – primary or permanent $252.00 $55.00
RESIN-BASED COMPOSITE RESTORATIONS (includes acid-etch, light cure & resin bonding; one filling per tooth per surface once within 24 month period)
D2330 Resin-based composite – one surface, anterior $150.00 $32.00D2331 Resin-based composite – two surfaces, anterior $190.00 $42.00D2332 Resin-based composite – three surfaces, anterior $220.00 $52.00D2335 Resin-based composite – four or more surfaces or involving incisal angle, anterior $265.00 $100.00D2390 Resin-based composite crown – anterior $300.00 $70.00D2391 Resin-based composite, one surface, posterior $150.00 $45.00D2392 Resin-based composite, two surfaces, posterior $190.00 $55.00D2393 Resin-based composite, three surfaces, posterior $220.00 $65.00D2394 Resin-based composite, four or more surfaces, posterior $265.00 $115.00
INLAY/ONLAY RESTORATIONS (cast/laboratory restorations once every 60 months)D2510 Inlay – metallic – one surface $550.00 $261.00D2520 Inlay – metallic – two surfaces $625.00 $336.00D2530 Inlay – metallic – three or more surfaces $950.00 $375.00D2542 Onlay – metallic – two surfaces (must be 12 or older) $800.00 $355.00D2543 Onlay – metallic – three surfaces (must be 12 or older) $900.00 $375.00D2544 Onlay – metallic – four or more surfaces (must be 12 or older) $1,000.00 $391.00D2610 Inlay – porcelain/ceramic – one surface $625.00 $317.00D2620 Inlay – porcelain/ceramic – two surfaces $880.00 $331.00D2630 Inlay – porcelain/ceramic – three or more surfaces $850.00 $374.00D2642 Onlay – porcelain/ceramic – two surfaces (must be 12 or older) $850.00 $375.00D2643 Onlay – porcelain/ceramic – three surfaces (must be 12 or older) $935.00 $391.00D2644 Onlay – porcelain/ceramic four or more surfaces (must be 12 or older) $1,000.00 $393.00D2650 Inlay – composite/resin – one surface (laboratory processed) $500.00 $317.00D2651 Inlay – composite/resin – two surfaces (laboratory processed) $650.00 $331.00D2652 Inlay – composite/resin – three or more surfaces (laboratory processed) $730.00 $374.00D2662 Onlay – composite/resin – two surfaces (laboratory processed; must be 12 or older) $775.00 $375.00D2663 Onlay – composite/resin – three surfaces (laboratory processed; must be 12 or older) $900.00 $391.00D2664 Onlay – composite/resin – four or more surfaces (laboratory processed; must be 12 or older) $900.00 $393.00
CROWNS – SINGLE RESTORATIONS (once every 60 months except children under age 12)D2710 Crown – resin (indirect) $800.00 $433.00D2712 Crown – 3/4 resin based composite (indirect) does not include facial veneers $800.00 $433.00D2720 Crown – resin with high noble metal $900.00 $465.00D2721 Crown – resin with predominantly base metal $750.00 $450.00D2722 Crown – resin with noble metal $800.00 $450.00D2740 Crown – porcelain/ceramic substrate $1,000.00 $545.00D2750 Crown – porcelain fused to high noble metal $1,000.00 $570.00D2751 Crown – porcelain fused to predominantly base metal $900.00 $520.00D2752 Crown – porcelain fused to noble metal $975.00 $520.00D2780 Crown – 3/4 cast high noble metal $950.00 $393.00D2781 Crown – 3/4 cast predominately base metal $900.00 $368.00D2782 Crown – 3/4 cast noble metal $925.00 $391.00D2783 Crown – 3/4 porcelain/ceramic $990.00 $400.00D2790 Crown – full cast high noble metal $900.00 $507.00D2791 Crown – full cast predominantly base metal $850.00 $455.00D2792 Crown – full cast noble metal $900.00 $473.00D2794 Crown – titanium $1,000.00 $530.00
OTHER RESTORATIVE SERVICESD2910 Recement inlay (after 6 months of initial placement) $85.00 $34.00D2915 Recement cast or prefabricated post and core (once in lifetime) $85.00 $34.00D2920 Recement crown (once every 12 months per tooth after 6 months of initial placement) $85.00 $27.00D2930 Prefabricated stainless steel crown – primary tooth (once every 24 months) $200.00 $90.00
Access ePPO Member Fee Schedule C2

ADA CUSTOMARY MEMBERCODE PROCEDURE DESCRIPTION FEE* FEE**
SYMBOL KEY* The listed Customary Fee is for illustrative purposes only. Customary fees may vary by dentist and by geographic area.** Member Fee when performed by a Participating Dentist.Current Dental Terminology © 2009 American Dental Association. All rights reserved.
D2931 Prefabricated stainless steel crown – permanent tooth (once every 24 months) $225.00 $90.00D2932 Prefabricated resin crown (once every 24 months on anterior primary tooth) $225.00 $66.00D2933 Prefabricated stainless steel crown with resin window. Open face stainless steel crown with $250.00 $84.00
aesthetic resin facing or veneer. (once every 24 months on anterior primary tooth)D2934 Prefabricated esthetic coated stainless steel crown – primary tooth (once every 24 months $250.00 $84.00
on anterior primary tooth)D2940 Sedative filling – once per tooth; excluded when definitive restoration is performed on tooth $80.00 $30.00D2950 Core build-up, including any pins (once per tooth per 60 months) $250.00 $100.00D2951 Pin retention – per tooth, in addition to restoration (once per permanent tooth during same $45.00 $28.00
appointment for restoration)D2952 Post and core in addition to crown, indirectly fabricated (once per tooth, per 60 months) $295.00 $141.00D2953 Each additional indirectly fabricated post, same tooth, indirectly fabricated $190.00 $77.00D2954 Prefabricated post and core in addition to crown (once per tooth per 60 months) $250.00 $105.00D2961 Labial veneer (resin laminate) – laboratory (not covered if considered cosmetic; $700.00 $285.00
once per 60 months)D2962 Labial veneer (porcelain laminate) – laboratory (not covered if considered cosmetic; $990.00 $436.00
once per 60 months)D2970 Temporary crown – fractured tooth, by report (may be covered when treatment is definitive $225.00 $104.00
and no other restoration is planned)D2971 Additional procedures to construct new crown under existing partial denture framework $150.00 $54.00
(once per tooth per 60 months)D2980 Crown repair, by report (once per tooth per 12 months) after 6 months of initial placement $240.00 $85.00
D3000-D3999 ENDODONTICS
PULP CAPPING (excluding final restoration or sedative filling for same tooth)D3110 Pulp cap direct $70.00 $13.00D3120 Pulp cap indirect $55.00 $13.00
PULPOTOMYD3220 Therapeutic pulpotomy (only on primary teeth, excluding final restoration; $175.00 $100.00
once per tooth per lifetime)D3221 Gross pulpal debridement primary and permanent teeth (once per tooth per lifetime) $200.00 $100.00
ENDODONTIC THERAPYD3222 Therapeutic pulpotomy (once per permanent tooth per lifetime for patients under 19 years) $166.00 $100.00D3230 Pulpal therapy (resorbable filling) anterior primary tooth (excluding final restoration and on $200.00 $90.00
primary molar without a permanent successor)D3240 Pulpal therapy (resorbable filling) posterior primary tooth (excluding final restoration and on $250.00 $102.00
primary molar without a permanent successor)
ENDODONTIC THERAPY (includes treatment plan, clinical procedures, and follow-up care)D3310 Anterior (excluding final restoration) retreatment not before 24 months $850.00 $550.00D3320 Bicuspid (excluding final restoration) retreatment not before 24 months $950.00 $640.00D3330 Molar (excluding final restoration) retreatment not before 24 months $1,200.00 $780.00D3331 Treatment of root canal obstruction; non-surgical access $360.00 $127.00D3332 Incomplete endodontic therapy; inoperable, unrestorable or fractured tooth $400.00 $234.00D3333 Internal root repair of perforation defects $305.00 $119.00
ENDODONTIC RETREATMENT (includes complete root canal therapy)D3346 Retreatment of previous root canal therapy, anterior, by report (once per tooth after 24 months) $950.00 $569.00D3347 Retreatment of previous root canal therapy, bicuspid, by report (once per tooth after 24 months) $1,100.00 $658.00D3348 Retreatment of previous root canal therapy, molar, by report (once per tooth after 24 months) $1,275.00 $776.00D3351 Apexification/recalcification – initial visit. (apical closure/calcific repair of perforations, $390.00 $170.00
root resorption, etc.) for permanent teeth and must follow 4–6 months of healing or narrowing of canal
D3352 Apexification/recalcification – interim medication replacement (apical closure/calcific repair $135.00 $83.00 of perforations, root resorption, etc.) for permanent teeth and must follow 4–6 months of healing or narrowing of canal
D3353 Apexification/recalcification – final visit (includes completed root canal therapy – apical $360.00 $179.00closure/calcific repair of perforations, root resorption, etc.)
D3410 Apicoectomy/periradicular surgery – anterior (once per tooth) $1,000.00 $414.00
D2000-D2999 RESTORATIVE – Continued
Access ePPO Member Fee Schedule C2

ADA CUSTOMARY MEMBERCODE PROCEDURE DESCRIPTION FEE* FEE**
SYMBOL KEY* The listed Customary Fee is for illustrative purposes only. Customary fees may vary by dentist and by geographic area.** Member Fee when performed by a Participating Dentist.Current Dental Terminology © 2009 American Dental Association. All rights reserved.
D3421 Apicoectomy/periradicular surgery – bicuspid (first root; once per tooth) $1,100.00 $446.00D3425 Apicoectomy/periradicular surgery – molar (first root; once per tooth) $1,200.00 $543.00D3426 Apicoectomy/periradicular surgery – (each additional root; must be submitted with $250.00 $145.00
D3421 or D3425 on same date of service)D3430 Retrograde filling (one per root up to maximum of 2 retrogrades on a molar) $220.00 $138.00D3450 Root amputation – per root (once per posterior tooth) $425.00 $258.00D3920 Hemisection (including any root removal), not including root canal therapy (once per $325.00 $194.00
posterior tooth)
D4000-D4999 PERIODONTICS (Limited to 2 Quadrants per Date of Service)
SURGICAL SERVICES (includes usual post-operative care)D4210 Gingivectomy or gingivoplasty – 4 or more contiguous teeth or tooth bounded spaces per $550.00 $198.00
quadrant for 5 mm or greater pocketing (once per quadrant per 36 months)D4211 Gingivectomy or gingivoplasty – one to three contiguous teeth or tooth bounded spaces per $175.00 $100.00
quadrant for 5 mm or greater pocketing (once per tooth per 36 months)D4240 Gingival flap procedure, including root planing – four or more contiguous teeth or tooth $700.00 $368.00
bounded spaces per quadrant for 5mm or greater pocketing (once per quadrant per 36 months)
D4241 Gingival flap procedure, including root planning one to three contiguous teeth or tooth $550.00 $221.00 bounded spaces with 5mm or greater pocketing per quadrant (once per tooth per 36 months)
D4249 Clinical crown lengthening – hard tissue (covered when bone removed, once per tooth $740.00 $379.00 per 60 months)
D4260 Osseous surgery (including flap entry and closure) – four or more contiguous teeth $950.00 $600.00 or tooth bounded spaces with 5mm or greater pocketing, once per quadrant per 36 months
D4261 Osseous surgery (including flap and closure) – one to three contiguous teeth or tooth $820.00 $360.00 bounded spaces with 5mm or greater pocketing, once per quadrant per 36 months
D4263 Bone replacement graft – first site in quadrant (once per site per 36 months) $525.00 $230.00D4264 Bone replacement graft – each additional site in quadrant, not to exceed 2 sites in a quadrant $436.00 $134.00
(once per site per 36 months)D4265 Biologic materials to aid in soft and osseous tissue regeneration (once per site per 36 months) $546.00 $194.00D4266 Guided tissue regeneration – resorbable barrier, per site (not to exceed 2 sites in a quadrant $585.00 $341.00
per 36 months)D4267 Guided tissue regeneration – non-resorbable barrier, per site, (includes membrane removal; $606.00 $358.00
not to exceed 2 sites in a quadrant per 36 months)D4270 Pedicle soft tissue graft procedure (once per tooth per 36 months, not to exceed 2 teeth $700.00 $401.00
per 36 months)D4271 Free soft tissue graft procedure (including donor site surgery; once per tooth per 36 months, $800.00 $401.00
not to exceed 2 teeth per 36 months)D4273 Subepithelial connective tissue graft procedures (including donor site surgery; $1,088.00 $626.00
once per tooth per 36 months, not to exceed 2 teeth per 36 months)D4274 Distal or proximal wedge procedure (when not performed in conjunction with surgical $400.00 $194.00
procedures in the same anatomical area; once per site per 36 months)D4275 Soft tissue allograft, per site (once per tooth per 36 months, not to exceed 2 teeth $1,120.00 $405.00
per 36 months)D4276 Combined connective tissue and double pedicle graft (once per tooth per 36 months, $1,190.00 $544.00
not to exceed 2 teeth per 36 months)
NON-SURGICAL SERVICES (includes usual post-operative costs)D4341 Periodontal scaling and root planing – four or more teeth per quadrant with 4 mm pocketing $225.00 $97.00
(once per quadrant per 24 months)D4342 Periodontal scaling and root planing – (once per quad per 24 months; one to three teeth $170.00 $52.00
per quadrant)D4355 Full mouth debridement to enable comprehensive evaluation and diagnosis (once) $125.00 $60.00D4381 Localized delivery of antimicrobial agents via a controlled release vehicle into diseased $65.00 $42.00
crevicular tissue (Once per tooth per 24 months 4 weeks after scaling and root planing)
D3000-D3999 ENDODONTICS – Continued
Access ePPO Member Fee Schedule C2

ADA CUSTOMARY MEMBERCODE PROCEDURE DESCRIPTION FEE* FEE**
SYMBOL KEY* The listed Customary Fee is for illustrative purposes only. Customary fees may vary by dentist and by geographic area.** Member Fee when performed by a Participating Dentist.Current Dental Terminology © 2009 American Dental Association. All rights reserved.
OTHER PERIODONTAL SERVICESD4910 Periodontal maintenance procedures (following active therapy) (once per 3 months following $125.00 $75.00
active periodontal therapy)D4920 Unscheduled dressing change (by someone other than treating dentist) $65.00 $49.00
D5000-D5999 PROSTHODONTICS (removable)
COMPLETE DENTURES (includes routine post-delivery care)D5110 Complete denture – maxillary (once per 60 months) $1,200.00 $560.00D5120 Complete denture – mandibular (once per 60 months) $1,200.00 $560.00D5130 Immediate denture – maxillary (once per lifetime) $1,200.00 $565.00D5140 Immediate denture – mandibular (once per lifetime) $1,200.00 $565.00
PARTIAL DENTURES (includes routine post-delivery care; once per arch per 60 months after 6 months from initial placement)
D5211 Maxillary partial denture – resin base (including any conventional clasps, rests, and teeth) $1,100.00 $375.00D5212 Mandibular partial denture – resin base (including any conventional clasps, rests, and teeth) $1,100.00 $375.00D5213 Maxillary partial denture – case metal framework with resin saddles (including any $1,200.00 $625.00
conventional clasps, rests, and teeth)D5214 Mandibular partial denture – cast metal framework and resin saddles (including any $1,200.00 $625.00
conventional clasps, rests, and teeth)D5225 Maxillary partial denture – flexible base (including any clasps, rests and teeth) $1,200.00 $625.00D5226 Mandibular partial denture – flexible base (including clasps, rests and teeth) $1,200.00 $625.00D5281 Removable unilateral partial denture – one piece cast metal (including clasps and arch) $700.00 $318.00
ADJUSTMENTS TO DENTURES (2 adjustments per denture per 12 months after 6 months from initial placement)
D5410 Adjust complete denture – maxillary $60.00 $20.00D5411 Adjust complete denture – mandibular $60.00 $20.00D5421 Adjust partial denture – maxillary $60.00 $20.00D5422 Adjust partial denture – mandibular $60.00 $20.00
REPAIRS TO COMPLETE DENTURESD5510 Repair broken complete denture base (once per arch per 12 months) $140.00 $59.00D5520 Replace missing or broken teeth (once per tooth per 12 months) $130.00 $65.00
REPAIRS TO PARTIAL DENTURESD5610 Repair resin denture base (once per arch per 12 months) $135.00 $59.00D5620 Repair cast framework (once per arch per 12 months) $165.00 $59.00D5630 Repair or replace broken clasp (once per tooth per 12 months) $175.00 $59.00D5640 Repair broken teeth – per tooth (once per tooth per 12 months) $150.00 $65.00D5650 Add tooth to existing partial denture (once per tooth per 12 months) $150.00 $65.00D5660 Add clasp to existing partial denture (once per tooth per 12 months) $180.00 $70.00D5670 Replace all teeth and acrylic on cast metal framework (maxillary; once in 60 months) $500.00 $245.00D5671 Replace all teeth and acrylic on cast metal framework (mandibular; once in 60 months) $500.00 $245.00
DENTURE REBASE PROCEDURES (once per arch per 36 months after 6 months from insertion)D5710 Rebase complete maxillary denture $350.00 $185.00D5711 Rebase complete mandibular denture $350.00 $185.00D5720 Rebase maxillary partial denture $350.00 $110.00D5721 Rebase mandibular partial denture $350.00 $110.00
DENTURE RELINE PROCEDURES (per arch per 36 months after 6 months from insertion)D5730 Reline complete maxillary denture (chair side) $250.00 $93.00D5731 Reline complete mandibular denture (chair side) $250.00 $93.00D5740 Reline maxillary partial denture (chair side) $220.00 $93.00D5741 Reline mandibular partial denture (chair side) $220.00 $93.00D5750 Reline complete maxillary denture (laboratory) $350.00 $134.00D5751 Reline complete mandibular denture (laboratory) $350.00 $134.00D5760 Reline maxillary partial denture (laboratory) $340.00 $134.00D5761 Reline mandibular partial denture (laboratory) $340.00 $134.00
D4000-D4999 PERIODONTICS (Limited to 2 Quadrants per Date of Service) – Continued
Access ePPO Member Fee Schedule C2

ADA CUSTOMARY MEMBERCODE PROCEDURE DESCRIPTION FEE*** FEE*
SYMBOL KEY* The listed Customary Fee is for illustrative purposes only. Customary fees may vary by dentist and by geographic area.** Member Fee when performed by a Participating Dentist.Current Dental Terminology © 2009 American Dental Association. All rights reserved.
INTERIM PROSTHESISD5820 Interim partial denture – maxillary (for replacement of anterior teeth during healing;
once in 60 months) $500.00 $228.00D5821 Interim partial denture – mandibular (for replacement of anterior teeth during healing;
once in 60 months) $500.00 $228.00D5850 Tissue conditioning (maxillary; up to twice per denture unit per 36 months) $125.00 $41.00D5851 Tissue conditioning (mandibular; up to twice per denture unit per 36 months) $125.00 $41.00D5860 Overdenture – complete, by report (once per arch per 60 months) $900.00 $600.00D5861 Overdenture – partial, by report (once per arch per 60 months) $1,108.00 $565.00
D6000-D6199 IMPLANT SERVICES
D6010 Surgical placement of implant body: endosteal implant (in lieu of 3 unit bridge; for age 16 and older; once per tooth per 60 months) $2,300.00 $1,360.00
IMPLANT SUPPORTED PROSTHETICS (Once per tooth per 60 months)D6056 Prefabricated abutment (includes placement) $650.00 $468.00D6057 Custom abutment (includes placement) $950.00 $560.00D6058 Abutment supported porcelain/ceramic crown $1,600.00 $705.00D6059 Abutment supported porcelain fused to metal crown (high noble) $1,600.00 $665.00D6060 Abutment supported porcelain fused to metal crown (base metal) $1,500.00 $600.00D6061 Abutment supported porcelain fused to metal crown (noble metal) $1,600.00 $640.00D6062 Abutment supported cast metal crown (high noble) $1,400.00 $632.00D6063 Abutment supported cast metal crown (base metal) $1,200.00 $600.00D6064 Abutment supported cast metal crown (noble metal) $1,400.00 $620.00D6065 Implant supported porcelain/ceramic crown $1,400.00 $705.00D6066 Implant supported porcelain fused to metal crown (titanium, titanium alloy, high noble metal) $1,600.00 $665.00D6067 Implant supported metal crown (titanium, titanium alloy, high noble metal) $1,600.00 $665.00D6094 Abutment supported crown (titanium) $1,200.00 $640.00
REPAIRS, RECEMENT, OR REMOVALD6090 Repair implant supported prosthesis, by report (once in 12 months per tooth) $200.00 $76.00D6092 Recement implant/abutment supported crown (once per tooth after 6 months from $150.00 $24.00
initial placement)D6093 Recement implant/abutment supported fixed partial denture (once in 12 months after $150.00 $35.00
6 months from initial placement)D6095 Repair implant abutment, by report (once per year after 24 months of initial placement) $250.00 $140.00D6100 Implant removal, by report (once per tooth) $300.00 $116.00
D6200-D6999 PROSTHODONTICS, FIXED (Each retainer and each pontic constitutes a unit in a fixed partial denture. For age 16 and older. Once per tooth per 60 months, unless otherwise noted.)
FIXED PARTIAL DENTURE PONTICSD6205 Pontic – indirect resin based composite $800.00 $520.00D6210 Pontic – cast high noble $900.00 $510.00D6211 Pontic – cast predominantly base metal $825.00 $463.00D6212 Pontic – cast noble metal $900.00 $473.00D6214 Pontic – titanium $900.00 $520.00D6240 Pontic – porcelain fused to high noble metal $900.00 $570.00D6241 Pontic – porcelain fused to predominantly base metal $850.00 $520.00D6242 Pontic – porcelain fused to noble metal $900.00 $520.00D6245 Pontic – porcelain ceramic substrate $950.00 $500.00D6250 Pontic – resin with high noble metal $900.00 $552.00D6251 Pontic – resin with predominantly base metal $850.00 $442.00D6252 Pontic – resin with noble metal $900.00 $508.00
FIXED PARTIAL DENTURE RETAINERS – INLAYS/ONLAYSD6545 Retainer – cast metal for resin bonded fixed prosthesis $500.00 $251.00D6602 Inlay – cast high noble metal two surfaces $670.00 $344.00D6603 Inlay – cast high noble metal three or more surfaces $825.00 $379.00D6604 Inlay – cast predominantly base metal two surfaces $825.00 $394.00
D5000-D5999 PROSTHODONTICS (removable) – Continued
Access ePPO Member Fee Schedule C2

ADA CUSTOMARY MEMBERCODE PROCEDURE DESCRIPTION FEE* FEE**
SYMBOL KEY* The listed Customary Fee is for illustrative purposes only. Customary fees may vary by dentist and by geographic area.** Member Fee when performed by a Participating Dentist.Current Dental Terminology © 2009 American Dental Association. All rights reserved.
D6605 Inlay – cast predominantly base metal three or more surfaces $825.00 $379.00D6606 Inlay – cast noble metal two surfaces $670.00 $394.00D6607 Inlay – cast noble metal three or more surfaces $700.00 $379.00D6610 Onlay – cast high noble metal two surfaces $970.00 $415.00D6611 Onlay – cast high noble metal three or more surfaces $900.00 $401.00D6612 Onlay – cast predominantly base metal two surfaces $825.00 $415.00D6613 Onlay – cast predominantly base metal three or more surfaces $800.00 $401.00D6614 Onlay – cast noble metal two surfaces $945.00 $415.00D6615 Onlay – cast noble metal three or more surfaces $900.00 $401.00D6624 Inlay – titanium $850.00 $401.00D6634 Onlay – titanium $850.00 $401.00
FIXED PARTIAL DENTURE RETAINERS – CROWNSD6710 Crown – indirect resin based composite $800.00 $502.00D6720 Crown – resin with high noble metal $950.00 $446.00D6721 Crown – resin with predominantly base metal $900.00 $425.00D6722 Crown – resin with noble metal $900.00 $425.00D6740 Crown – porcelain/ceramic $930.00 $506.00D6750 Crown – porcelain fused to high noble $1,000.00 $520.00D6751 Crown – porcelain fused to predominantly base metal $900.00 $475.00D6752 Crown – porcelain fused to noble metal $1,000.00 $475.00D6780 Crown – 3/4 cast high noble metal $830.00 $410.00D6781 Crown – 3/4 cast predominately based metal $800.00 $375.00D6782 Crown – 3/4 cast noble metal $945.00 $404.00D6790 Crown – full cast high noble metal $900.00 $512.00D6791 Crown – full cast predominantly base metal $850.00 $446.00D6792 Crown – full cast noble metal $900.00 $473.00D6793 Provisional retainer crown (If used at least 6 months during multistage care) $350.00 $156.00D6794 Crown – titanium $900.00 $502.00
OTHER FIXED PARTIAL DENTURE SERVICESD6930 Recement fixed bridge (once every 12 months after 6 months from initial placement) $110.00 $50.00D6970 Post and core in addition to fixed partial denture retainer, indirectly fabricated $290.00 $138.00D6972 Prefabricated post and core in addition to bridge retainer $260.00 $116.00D6973 Core build-up for retainer, including any pins (not covered in conjunction with $260.00 $116.00
D6970 and D6972)D6977 Each additional prefabricated post – same tooth $85.00 $64.00D6980 Bridge repair, by report (once every 12 months) $250.00 $100.00D6985 Pediatric partial denture – fixed (once per arch per 60 months) $500.00 $375.00
D7000-D7999 ORAL AND MAXILLOFACIAL SURGERY
D7111 Extraction coronal remnants – deciduous tooth (once per tooth) $115.00 $40.00D7140 Extraction – erupted tooth or exposed roots (elevation and/or forceps removal; $125.00 $50.00
once per tooth)D7210 Surgical removal of erupted tooth requiring elevation of mucoperiosteal flap and removal $260.00 $104.00
of bone and/or section of tooth (once per tooth)D7220 Removal of impacted tooth – soft tissue (once per tooth) $285.00 $130.00D7230 Removal of impacted tooth – partially bony (once per tooth) $350.00 $190.00D7240 Removal of impacted tooth – completely bony (once per tooth) $400.00 $225.00D7241 Removal of impacted tooth – completely bony, with unusual surgical complications (once per tooth) $450.00 $235.00 D7250 Surgical removal of residual tooth roots (once per tooth) $250.00 $120.00D7260 Oroantral fistula closure $850.00 $689.00D7261 Primary closure of a sinus perforation $640.00 $200.00D7270 Tooth reimplantation and/or stabilization of accidentally evulsed or displaced tooth and/or $518.00 $414.00
alveolus (once per tooth)D7285 Biopsy of oral tissue – hard (bone, tooth) $330.00 $253.00D7286 Biopsy of oral tissue – soft $350.00 $259.00D7287 Exfoliative cytological sample collection $160.00 $50.00D7288 Brush biopsy – transepithelial sample collection $90.00 $40.00D7310 Alveoloplasty in conjunction with extractions – per quadrant (once per quadrant per lifetime) $225.00 $201.00
D6200-D6999 PROSTHODONTICS, FIXED (Each retainer and each pontic constitutes a unit in a fixed partial denture. For age 16 and older. Once per tooth per 60 months, unless otherwise noted.) – Continued
Access ePPO Member Fee Schedule C2

ADA CUSTOMARY MEMBERCODE PROCEDURE DESCRIPTION FEE* FEE**
SYMBOL KEY* The listed Customary Fee is for illustrative purposes only. Customary fees may vary by dentist and by geographic area.** Member Fee when performed by a Participating Dentist.Current Dental Terminology © 2009 American Dental Association. All rights reserved.
D7311 Alveoloplasty in conjunction with extractions – one to three teeth or tooth spaces per quadrant $205.00 $132.00 (once per quadrant)
D7320 Alveoloplasty not in conjunction with extractions – four or more teeth or tooth spaces per $465.00 $276.00 quadrant (no extractions performed in a quadrant; once per quadrant)
D7321 Alveoloplasty not in conjunction with extractions – one to three teeth or tooth spaces per $285.00 $228.00 quadrant (once per quadrant)
D7340 Vestibuloplasty – ridge extension (secondary epithelialization) $862.00 $690.00D7350 Vestibuloplasty – ridge extension (including soft tissue grafts, muscle re-attachment, revision $1,575.00 $1,322.00
of soft tissue attachment and management of hypertrophied and hyperplastic tissue)D7960 Frenulectomy (frenectomy or frenotomy) – separate procedure (once per site) $450.00 $322.00D7963 Frenuoplasty (once per site) $402.00 $322.00D7970 Excision of hyperplastic tissue – per arch $402.00 $322.00D7971 Excision of pericoronal gingiva $250.00 $106.00D7980 Sialolithotomy $805.00 $644.00D7981 Excision of salivary gland, by report $2,875.00 $2,300.00D7982 Sialodochoplasty $1,725.00 $1,380.00D7983 Closure of salivary fistula $1,495.00 $1,196.00
D9000-D9999 ADJUNCTIVE GENERAL SERVICES
UNCLASSIFIED TREATMENTD9110 Palliative (emergency) treatment of dental pain – minor procedure (per visit basis, once on $95.00 $35.00
same date; limit 3 times per 12 months)D9120 Fixed partial denture sectioning (once per tooth) $159.00 $35.00
ANESTHESIAD9210 Local anesthesia not in conjunction with operative or surgical procedures $35.00 $14.00D9220 Deep sedation/general anesthesia – up to 30 minutes (covered when administered with $320.00 $160.00
covered surgery)D9221 Deep sedation/general anesthesia – each additional 15 minutes (covered when administered $120.00 $65.00
with covered surgery)D9241 Intravenous conscious sedation/analgesia – up to 30 minutes (covered when administered $320.00 $115.00
with covered surgery)D9242 Intravenous conscious sedation/analgesia – each additional 15 minutes (covered when $120.00 $55.00
administered with covered surgery by licensed dentist in a dental office)D9248 Non-Intravenous conscious sedation $120.00 $89.00D9310 Consultation – diagnostic service provided by dentist or physician other than requesting dentist $46.00 $40.00
or physician (not covered in conjunction with an examination/evaluation)D9940 Occlusal guard, by report (includes adjustments or repairs 6 months after delivery; $270.00 $220.00
once in 60 months when delivered within 36 months following active periodontal treatment)D9942 Repair or reline of an occlusal guard (Only when D9940 has been benefited and after $154.00 $82.00
6 months of initial placement)
PLAN PROVISIONS
1. Referral Forms are not required to see Participating Specialists.2. Recognized and accepted ADA-CDT procedure codes must be used when reporting treatment and assessing member fees. Use of alternative
or new materials must correspond to a recognized ADA-CDT procedure code.3. Procedures "Not Covered" by the Plan may be charged at the Participating Dentist's usual and customary fee(s).4. Dental procedures performed solely for esthetic or cosmetic reasons are not covered services under the Plan, and the patient may be charged
the Participating Dentist's usual and customary fee(s).5. It is recommended that Participating Dentist's contact the Plan, or submit a pre-treatment estimate, prior to providing treatment for services of
$600.00 or more.6. Patient will be liable for all hospital costs in the event dental treatment is provided in a hospital.7. Fluoride Toothpaste is only covered following periodontal surgery and must be dispensed in the dentist's office.8. Recement or repair onlay falls under procedure codes D2920 (Recement crown) or D2980 (Crown repair).9. No benefits are provided for dental services rendered by a non-plan participating dentist, except in the case of an out-of-area emergency or
when the Plan has given the member a referral to a non-plan participating dentist. For these exceptions, the member is responsible for filing claims forms for reimbursement.
D7000-D7999 ORAL AND MAXILLOFACIAL SURGERY – Continued
Access ePPO Member Fee Schedule C2
10. Plan benefits may be verified by contacting the Dominion USA Member Services Department at 800-334-6277.

Access ePPO Member Fee Schedule C2 - additional fees
ADA PROCEDURE MEMBERCODE DESCRIPTION FEE(S)
D3950 Canal prep/fitting of preformed dowel or post ........................................................0D7510 Incision/drainage of abscess - intraoral soft .......................................................175D9215 Local anesthesia ....................................................................................................0D9980 Sterilization surcharge ............................................................................................0
Current Dental Terminology © American Dental Association.

Dental Enrollment CardDENTALSELECT ONE:
I choose the Dominion PPO1
I choose the Dominion ePPO1 I choose the Dominion Select Plan1
VISIONSELECT ONE:
I choose the Avalon vision2 plan
Enrollment Information
Last Name First Name M.I.
Social Security Number Sex M F Birthdate (MM/DD/YY)
Home Address Home Phone
City State ZIP Work Phone
Email Address Hire Date List All Your Eligible Dependents Below
Last Name (if different) First Name M.I.. Sex (M/F)
Birthdate(MM/DD/YY)
Spouse
Child
Child
Child
Child
Child
Child
SELECT PLANProvider Selection
Dental Office Name & Code (As Indicated on Your Dentist Directory)
If I am enrolling in the Select Plan and I am voluntarily paying 100% of the cost of this plan, without employer contribution, I agree to remain in plan a minimum of twelve (12) months. If I cancel before the end of the 12 month period, I may be responsible for the usual, customary and reasonable charges for services received, reduced by the sum of the subscription dues and copayments paid.
I understand and agree that my signature on this enrollment form serves as my legal commitment to the Plan and its terms. Further, this signature represents my authorization for the release of information regarding services provided to me or my covered dependents by providers of dental and/or vision services. Information will be released to Dominion Dental Services, Inc., if enrolled in the dental plan and Avalon Insurance Company if enrolled in vision plan, for the purpose of investigation or evaluation of care in connection with a claim or complaint. Authorization will be limited to the term of coverage of this contract. A copy of this form will be made available to subscriber or their authorized representative upon request.
Signature _______________________________________________________________ Date ______________
Agent/Broker # Group # Group Name Coverage Eff. Date
Dominion Dental Services USA, Inc., P.O. Box 75314 Charlotte, NC 28275-53141The dental plans are underwritten by Dominion Dental Services, Inc.2The vision plans are underwritten by Avalon Insurance Company and administered by Dominion Vision Services.Virginia - Any person who, with the intent to defraud or knowing that s/he is facilitating a fraud against an insurer, submits an application or files a claim containing a false or deceptive st tement may have violated the state law.
Dominion Dental Services, Inc.Arlington, VA
Avalon Insurance CompanyHarrisburg, PA
DDS(VA-ONLY)15DVGR
ESDC II

Dominion National tiene extensas redes que proporcionan acceso a más de 290,000 listas nacionales de dentistas PPO y a una de las redes más grandes del tipo DHMO y de ePPO en la región Atlántica Central.1 Siga las instrucciones que aparecen a continuación para encontrar a un dentista participante.
Vaya a DominionNational.com/find-a-dentist.
Utilice las funciones de búsqueda para encontrar dentistas generales y especialistas cerca de su casa u oficina. Podrá filtrar su búsqueda por ciudad, estado
o código postal, nombre del dentista y el tipo o idioma(s) que se habla.
Para determinar la red correspondiente, en el menú desplegable deberá seleccionar el tipo de plan
“Dominion USA.”
Los miembros de Select Plan (igual que los del plan DHMO)2 deberán seleccionar a un dentista
participante antes de concertar una cita. A excepción de una atención de emergencia fuera del área, usted deberá recibir el tratamiento en el consultorio dental que seleccionó. Los miembros de la familia podrán
usar diferentes dentistas participantes.
CÓMO ELEGIR A SU DENTISTA:• Opción 1: Cree su cuenta en línea a través
del Portal del Miembro de Dominion en https://DominionMembers.com. Una vez que haya ingresado al sistema, simplemente vaya a su “Member Summary” y seleccione la opción “Change Dentist.”
• Opción 2: Llame a Dominion al teléfono 888.518.5338.
SELECT PLAN SOLAMENTE
¿NO PUEDE ENCONTRAR AL DENTISTA DE SU ELECCIÓN? DENOMÍNELOS POR FACTOR A CONSIDERAR EN LA RED DE DOMINION, CONSULTANDO EN LÍNEA DOMINIONNATIONAL.COM/FIND-A-DENTIST Y HACIENDO CLIC EN “NOMINATE YOUR DENTIST.”
1
2
Una vez que haya ingresado en los criterios de búsqueda, haga clic en “Find” y aparecerán sus
resultados. Busque los resultados proporcionando la información de contacto pormenorizada,
que incluya:
• Direcciones de oficina y correo electrónico• Números de teléfono de emergencia y
de oficina• Estatus del dentista (que esté aceptando
nuevos miembros)• Horas de operación• Accesibilidad para discapacitados• Idioma(s) que se habla • Instrucciones de cómo llegar al
consultorio dental
3
1 Dominion National Internal Performance Report, junio de 2017. Los dentistas participantes están sujetos a cambio. La región Atlántica Central incluye D.C., Delaware, Maryland, Pennsylvania y Virginia.2 Igual que un plan DHMO con copagos fijos de los miembros, sin límites máximos anuales de dinero, sin periodos de espera, sin deducibles, sin papeleo previo a la autorización o estimaciones previas al tratamiento y sin formularios de reclamación (excepto en casos de emergencias fuera del área).
El grupo de compañías de Dominion National incluye a Dominion Dental Services, Inc., una entidad emisora autorizada de planes dentales, y a Dominion Dental Services USA, Inc., un administrador autorizado de los beneficios dentales y del cuidado de la vista.
¿CÓMO ENCUENTRO A UN DENTISTA PARTICIPANTE?
DUSA-FPD-S-072617

BENEFICIOS DE TRANSFERENCIAS

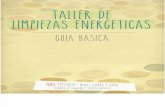
Los beneficios de transferencia agregan valor adicional a su plan dental de Dominion National, permitiéndole trasladar una parte de su máximo beneficio no utilizado año tras año. Tendrá la flexibilidad de ahorrar y planificar procedimientos dentales más costosos, de modo que funcionen mejor para usted. Esta característica viene incluida en su plan de Dominion – la cual le permite tener la certeza de que podrá tener más beneficios en caso de llegar a necesitarlos en el futuro.
Los beneficios de transferencia son fáciles y automáticos.• Un miembro puede ser elegible para transferir
una parte de su máximo anual no usado por beneficio o año calendario1 para servicios de Diagnóstico y Prevención (Clase I), Básicos (Clase II) y Mayores (Clase III). La cantidad de los beneficios de transferencia no puede exceder el máximo del traslado a otro año (consulte la tabla de abajo). La transferencia no se aplica a los beneficios que están sujetos a un máximo de por vida, como la ortodoncia.
• A fin de calificar para los beneficios de transferencia, deberá presentar un reclamo de
al menos un servicio con cobertura de Clase I durante el año del beneficio o año calendario.1 Además, sus reclamos pagados no deberán exceder el umbral de la transferencia anual (vea el gráfico que aparece a continuación).
• Primero se utiliza la cantidad máxima regular anual de dinero. El dinero del beneficio de transferencia, o importes anuales de transferencias, se usan después de que se alcanza el máximo anual.
• Si cancela la inscripción de su plan durante algún período de tiempo por cualquier motivo (por ejemplo, si se casa y se inscribe bajo el plan de su cónyuge), perderá el saldo de la transferencia que le corresponde actualmente.
Cantidades de las transferenciasLas cantidades de las transferencias varían con base en el máximo anual de su beneficio. El monto anual de la transferencia muestra la cantidad que puede transferir al año siguiente y posteriormente, mientras que la transferencia máxima es la cantidad total tope que puede acumular. La siguiente tabla muestra la forma en que se calculan los beneficios de transferencia.
1 Para determinar si su plan es año de beneficio o año calendario, consulte su Resumen de Beneficios o comuníquese con su Administrador de Beneficios.
Máximo AnualUmbral Anual de
Transferencias (Reclamos Pagados)
Monto Anual de Transferencias Transferencia Máxima
$500 – $700 $200 $150 $500
$750 – $950 $300 $200 $500
$1,000 – $1,200 $500 $350 $1,000
$1,250 – $1,450 $600 $450 $1,250
$1,500 – $1,950 $700 $500 $1,250
$2,000 – $2,450 $800 $600 $1,500
$2,500 – $2,950 $900 $700 $1,500
$3,000 o más $1,000 $750 $1,500
Para preguntas, comuníquese con su Administrador de Beneficios o con el Departamento de Servicio a Miembros de Dominion al teléfono 888.518.5338.
APROVECHANDO AL MÁXIMO EL VALOR Y LA FLEXIBILIDAD DE LOS BENEFICIOS
Beneficios deTRANSFERENCIAS
DUSA-RB-S-073117Los planes dentales están asegurados por Dominion Dental Services, Inc. d/b/a Dominion National.

La aplicación móvil MyDominion proporciona a los miembros un acceso fácil a la información de la cuenta y del plan.
Con MyDominion, usted podrá:
La aplicación MyDominion es compatible con iPhone® y Android™ y se puede descargar a través de nuestro sitio web en DominionNational.com/mobile.
APLICACIÓN MÓVIL MyDOMINION
Encontrar un Dentista
Ver las Tarjetas de Identificación
Ver la Información del Plan
t
MA
-MFS
05
1717

PORTAL DEL MIEMBROhttps://DominionMembers.com Acceso a Internet – Tiempo Real, Protegido con Contraseña
Tarjetas de Identificación
Obtenga Información del Plan y de los Certificados de
Cobertura
Calculadora del Costo de los
Servicios Dentales
Correspondencia General
Peticiones de Servicio de los
Miembros
t
PASO 1 Vaya a https://DominionMembers.com.
PASO 2 Seleccione “Create New Account” y llene el formulario de solicitud de ingreso. Dentro de 24 horas recibirá un e-mail de confirmación con su información de ingreso.
Se le indicará que cambie su contraseña. Cambie la contraseña a una que usted recuerde. Las contraseñas deberán tener un mínimo de ocho caracteres, e incluirán al menos una letra mayúscula, un número y un carácter especial (#!$%*).
PASO 4 Regrese al portal e ingrese su contraseña.
PASO 3
FUNCIONES DEL PORTAL
INSTRUCCIONES PARA EL INICIO DE SESIÓN
DN-MP-S-072617

Nondiscrimination and Foreign Language Assistance Notice
The Dominion National family of companies (including insurers Dominion Dental Services, Inc. and Dominion National Insurance Company of New
Jersey) complies with applicable federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex.
Dominion National does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.
Dominion National provides free aids and services to people with disabilities to communicate effectively with us, such as: qualified sign language
interpreters or written information in other formats (large print, audio, accessible electronic format, other formats). Dominion National provides free
language service to people whose primary language is not English, such as: qualified interpreters, and information written in other languages.
If you need these services, contact our Civil Rights Coordinator.
If you believe that Dominion National has failed to provide these services or discriminated in another way on the basis of race, color, national origin,
age, disability, or sex, you can file a grievance with our Civil Rights Coordinator at Dominion National, Attn: Civil Rights Coordinator, 251 18th Street
South, Arlington, VA 22202; call 888.518.5338, fax (703) 518-8849 (Attn: Civil Rights Coordinator), or email at [email protected]. You
can file a grievance by mail, fax, or email. If you need help filing a grievance, our Civil Rights Coordinator is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services, 200 Independence Avenue, SW., Room 509F, HHH Building, Washington, D.C. 20201, 1-800-368-1019, 800-537-7697 (TDD)
Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html.
This notice may have important information about your application or coverage through your health plan. Look for key dates in this notice; you may
need to take action by certain deadlines to keep your health coverage or help with costs. If you, or someone you’re helping, has questions or needs
assistance or information about your health plan or this notice, you have the right to get help in your language at no cost. To talk to an interpreter,
call 888.518.5338.
Spanish: Este aviso puede contener información importante acerca de su solicitud o cobertura a través de su plan de salud. Ponga atención a la fechas importantes en este aviso; es posible que tenga que actuar antes de ciertas fechas límite para mantener su cobertura de salud o con ayuda del costo. Si usted, o alguien a quien usted ayuda, tiene preguntas o necesita asistencia o información acerca de su plan de salud o este aviso, tiene el derecho de obtener ayuda en su idioma sin costo alguno. Para hablar con un intérprete, llame al 888.518.5338.
Chinese: 本通知可能包含有关您的健康计划申请或涵盖范围的重要信息。请注意本通知中的重要日期;您可能需要在具体的
截止期限前采取行动维护您的健康涵盖范围或缴纳费用。如果您自己或者您提供帮助的某个人对您的健康计划或本通知有任
何疑问或者需要获得帮助或信息,您有权免费获得以您的语言提供的帮助。欲与翻译员通话,请拨打电话 888.518.5338。
Korean: 이 안내문에는 귀하의 건강보험을 통한 신청 또는 보장에 관한 중요한 정보가 포함될 수 있습니다. 이 안내문의 주요
날짜를 확인해 주십시오! 건강보험을 유지하거나 비용 지원을 위해 특정 마감일까지 관련 조처를 해야 할 수도 있습니다.
귀하 또는 귀하가 부양하는 사람이 귀하의 건강보험이나 이 안내문에 관하여 문의 사항이 있거나 도움말 또는 정보가 필요할
때는, 무료로 귀하의 언어를 통하여 도움을 받을 권리가 있습니다. 통역사에게 문의하려면 888.518.5338으로 전화해 주십시오.
Vietnamese: Thông báo này có thể chứa những thông tin quan trọng về đơn xin của quý khách hoặc phạm vi bảo hiểm trong chương trình bảo
hiểm sức khỏe của quý khách hàng. Hãy xem những ngày quan trọng trong thông báo này; quý khách có thể cần xử lý trước khi đến hạn cuối để
duy trì bảo hiểm sức khỏe hoặc để giảm chi phí. Nếu quý khách hàng, hoặc người nào đó đang trợ giúp cho quý khách hàng, có câu hỏi hay cần
trợ giúp hay thông tin về chương trình bảo hiểm sức khỏe của quý khách, quý khách có quyền yêu cầu được trợ giúp bằng ngôn ngữ của quý
khách mà không phát sinh chi phí nào. Để kết nối với thông dịch viên, hãy gọi 888.518.5338.
Russian: Данное уведомление может содержать важную информацию по вашей заявке и медицинской страховке. Просмотрите ключевые даты в этом уведомлении – может понадобиться придерживаться некоторых сроков для сохранения медицинской страховки или же внести плату. Если у вас или помогающего вам есть вопросы, а также нужна помощь или информация по медицинской страховке или по данному уведомлению, позвоните на бесплатный телефон. Для соединения с переводчиком, звоните 888.518.5338.

The Dominion National group of companies includes Dominion Dental Services, Inc., a licensed issuer of dental plans, and Dominion Dental Services USA, Inc., a licensed administrator of dental and vision benefits. Vision plans are underwritten by Avalon Insurance Company.
Tagalog: Ang abisong ito ay maaaring may mahalagang impormasyon tungkol sa aplikasyon mo o pagsakop sa pamamagitan ng iyong planong pangkalusugan. Maghanap ng mga pangunahing petsa sa abisong ito; maaaring kailanganin mong kumilos bago ang mga ilang deadline para mapanatili ang pagsakop sa kalusugan mo o makatulong sa mga gastos. Kung ikaw o sinumang tinutulungan mo ay may mga tanong o kailangan ng tulong o impormasyon tungkol sa iyong planong pangkalusugan o sa abisong ito, may karapatan kang humingi ng tulong sa wika mo nang libre. Para makipag-usap sa tagapagsaling-wika, tumawag sa 888.518.5338. Arabic: أوحول طلبك الل بعض المواعيد ال هذا اإلشعار؛ ربما تحتاج إلى اتخاذ إجراء من هائية حول التغطية م خالل خطتك الصحية. ابحث عن التواريخ الرئيسية في ن
إذا كنت تحتاج إلى مساعدة، أو كنت تساعد شخًصا أخر، أو كان لديك أسئلة أو بحاجة إلى المساعدة في سداد التكاليف.للحفاظ على التغطية الصحية الخاصة بك أو المساعدة هذا اإلشعار، فلديك الحق في الحصول على المساعدة بلغتك األم مجاًنا. للتحدث إ لى مترجم فوري، اتصل أو بحاجة للحصول على معلومات حول خطتك الصحية أو حول
الرقم على 888.518.5338 Portuguese: Este aviso pode ter informações importantes sobre a sua aplicação ou cobertura de plano de saúde. Olhe para as datas importantes neste aviso; pode ser necessário tomar medidas em determinados prazos para manter a sua cobertura de saúde ou ajudar com os custos. Se você, ou alguém que você está ajudando, tem dúvidas ou precisa de assistência ou informação sobre seu plano de saúde ou este aviso, você tem o direito de obter ajuda na sua língua sem nenhum custo. Para falar com um intérprete, ligue para 888.518.5338. French: Le présent avis peut avoir information importante concernant votre application ou la couverture à travers de votre plan sanitaire. Regarde pour clef dates dans cet avis ; vous pourries devoir prendre des mesures à certaines dates pour maintenir votre plan sanitaire ou de l’aidé à payer les coûts. Si vous, ou quelqu’un vous les aidez avoir des questions ou il a besoin d’aide ou information concernant votre plan sanitaire ou cet avis, vous avez le droit à obtenir de l’aide dans votre langue à titre gratuit. Pour parler à un interprète, appel 888.518.5338.
Gujarati: આ નોટિસ માાં તમારી અરજી અથવા તમારી આરોગ્ય યોજના મારફતે કવરેજ વવશે મહત્વની જાણકારી હોઈ શકે છે. આ નોટિસ માાં મહત્વ ની તારીખો જુઓ; તમારા આરોગ્ય કવરેજ ને જાળવવા માિે અથવા ખર્ચ બર્ાવવા માિે અમકુ ર્ોક્કસ મદુતો સધુી તમને પગલાાં લેવા પડી શકે છે. જો તમે, અથવા જેની તમે મદદ કરી રહ્યા છો, તેમણે કોઈ સવાલ હોય અથવા સહાય કે તમારી આરોગ્ય યોજના અથવા આ નોટિસ વવશે માટહતી જોઇએ, તો તમને તમારી ભાષા માાં કોઇ પણ ખર્ચ વગર મદદ મેળવવા નુાં અવધકાર છે. દુભાવષયા સાથે વાત કરવા માિે, 888.518.5338ફોન કરો. Italian: Questo avviso potrebbe avere importanti informazioni circa la vostra applicazioni o copertura attraverso il vostro programma di salute. Cercate les principali date in questo avviso; pottrebe essere necessario applicare missuri ritoccando alcune scadenze per mantenere le vostre programma di salute o per contribuire con i costi. Se voi, o qualcuno voi state aiutando, ha quesiti o necessita di assistenza o informazione circa il vostro programma di salute o questo avviso, voi avvere può le diritto per ottenere aiuto in la vostra lingua gratuitamente. Per parlare con un interprete, chiamate 888.518.5338. Polish: To powiadomienie może zawierać ważne informacje na temat Pana/Pani wniosku lub zakresu ubezpieczenia w posiadanym planie. Zalecamy zapoznać się z kluczowymi terminami w tym powiadomieniu; może istnieć konieczność podjęcia działania przed upłynięciem pewnych terminów, aby utrzymać ubezpieczenie zdrowotne lub uzyskać pomoc w kosztach. Jeżeli Pan/Pani lub ktoś, komu Pan/Pani pomaga, ma pytania bądź potrzebuje pomocy lub informacji w sprawie planu ubezpieczenia zdrowotnego albo tego powiadomienia, przysługuje Panu/Pani prawo do nieodpłatnego uzyskania pomocy w ojczystym języku. Aby porozmawiać z tłumaczem ustnym, prosimy zadzwonić pod numer 888.518.5338. French Creole: Avi sila a ka genyen enfòmasyon ki enpòtan konsènan aplikasyon w lan oubyen asirans ou atravè plan lasante w la. Chèche dat enpòtan yo ki nan avi sila a; ou ka gen pou w fè sèten bagay anvan kèk dat limit pou w sa kenbe asirans ou a oubyen pou yo ede w ak kèk depans. Si oumenm, oubyen yon lòt moun w ap ede, genyen kesyon oubyen bezwen èd oswa plis enfòmasyon sou plan lasante w oswa sou avi sila a, ou
genyen dwa pou w resevwa asistans nan lang ou pale a san li pa koute w anyen ditou. Pou w pale ak yon entèprèt, rele 888.518.5338. German: Diese Mitteilung enthält eventuell wichtige Informationen bezüglich Ihres Antrages auf oder Ihres Schutzes durch Ihre Krankenversicherung. Suchen Sie nach Schlüsseldaten in diesem Dokument. Eventuell müssen Sie innerhalb von gewissen Fristen handeln um Ihren Versicherungsschutz zu behalten oder Hilfe mit Kosten zu erhalten. Fall Sie oder jemand, dem/der Sie helfen, Fragen hat oder Hilfe benötigt bezüglich dieser Mitteilung oder der Krankenversicherung, haben Sie Anspruch auf kostenlose Hilfe in Ihrer Sprache. Um mit einem Dolmetscher zu sprechen, rufen Sie an unter 888.518.5338. Amharic: ይህ ማሳሰቢያ፣ ስለማመልከቻዎ ወይም በጤና እቅድዎ አማካኝነት ስለሚያገኙት ሽፋን አስፈላጊ መረጃ ሊይዝ ይችላል፡፡ በዚህ ማሳሰቢያ ላይ የሚገኙትን ወሳኝ ቀናት ይመልከቱ፤ የጤና ሽፋንዎን ይዘው ለመቆየት ወይም በወጪዎች ረገድ እገዛ ለማግኘት፣ እርምጃ ሊወሰድባቸው በሚገቡ በተወሰኑ ቀናቶች ውስጥ እርምጃ መውሰድ ይኖርብዎ ይሆናል፡፡ እርስዎ ወይም እርስዎ የሚረዱት ግለሰብ ስለ ጤና እቅድዎ ጥያቄዎች ካለዎት/ካላቸው ወይም እገዛ አሊያም መረጃ ከፈለጉ እገዛውን ያለምንም ክፍያ
በቋንቋዎ የማግኘት መብት አለዎት፡፡ ከአስተርጓሚ ጋር ለመነጋገር 888.518.5338 ብለው ይደውሉ፡፡