Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF...

of 12
-
Upload
vskywokervs -
Category
Documents
-
view
216 -
download
0
Transcript of Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF...
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
1/12
Chromosomal Syndromesand Genetic DiseaseFrederick W Luthardt, Swedish Hospital Medical Center, Seattle, Washington, USA
Elisabeth Keitges,Dynacare Northwest, Seattle, Washington, USA
The normal human chromosomecomplement consists of 46 chromosomes comprising 22
morphologically different pairs of autosomes and one pair of sex chromosomes. Variation
in either chromosome number or structure frequently results in significant mental
and/or clinical abnormalities. Chromosomal syndromes are associated with specific
chromosomal abnormalities.
Introduction
With the discovery in 1956 that the correct chromosomenumber in humans is 46,the new era of clinical cytogenetics
began its rapid growth. During the next few years, severalmajor chromosomal syndromes with altered numbers ofchromosomes were reported, i.e. Down syndrome (trisomy21), Turner syndrome (45,X) and Klinefelter syndrome(47,XXY). Since then it has been well established thatchromosome abnormalities contribute significantly togenetic disease resulting in reproductive loss, infertility,stillbirths, congenital anomalies, abnormal sexual devel-opment, mental retardation and pathogenesis of malig-nancy. Specific chromosome abnormalities have beenassociated with over 60 identifiable syndromes. They arepresent in at least 50% of spontaneous abortions, 6% ofstillbirths, about 5% of couples with two or more
miscarriages and approximately 0.5% of newborns. Inwomen aged 35 or over, chromosome abnormalities aredetected in about 2% of all pregnancies. Some of theabnormalities and their clinical consequences will bediscussed in the following sections.
Chromosome Abnormalities
Numerical abnormalities
Chromosome abnormalities are classified as either numer-
ical or structural and may involve more than onechromosome. In discussing numerical abnormalities,certain terms need to be clarified. The normal humanchromosome complement consists of 46 chromosomes(diploid) which is double the euploid (haploid) or gametecomplement of 23. Exact multiples of euploid chromosomesets are either diploid or polyploid, i.e. triploid ortetraploid consisting of three or four euploid sets,respectively. Aneuploidy refers to the presence of an extracopy of a specific chromosome, or trisomy, as seen in
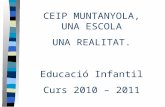
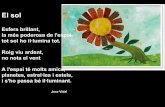
Figure1 (Down syndrome karyotype with trisomy 21), or tthe absence of a single chromosome, or monosomy, as seein Figure 2 (Turner syndrome karyotype with 45,X).
The most common clinically significant chromosomabnormalities involving aneuploidy are frequently detected in newborns (Table 1). Although autosomal and sechromosome trisomies result in clinical abnormalities theare more viable than monosomies, with the exception omonosomy X (45,X Turner syndrome). However, fewethan 5% of 45,X conceptions actually survive to birthAneuploidy is frequently associated with maternal age anconstitutes a significant portion of chromosome abnormalities observed in spontaneous abortions (Table 2) andetected prenatally in fetuses (Table 3).
Polyploidy resulting from triploidy (69 chromosomesor tetraploidy (92 chromosomes) are lethal conditionmost frequently seen in spontaneous abortions and ver
Article Contents
Introductory article
. Introduction
. Chromosome Abnormalities
. Outline of Chromosome Syndromes
. Maternal Age Effects
. Recurrence Risks
. Summary
Figure 1 47,XX,121 female Down syndrome karyotype demonstratin
trisomy 21. (Karyotype prepared by Dave McDonald.)
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
2/12
rarely in newborns with a short survival time. Triploidy ismore common and is related to abnormal events prior to orduring fertilization: most often triploidy results from twohaploid sperm fertilizing a single haploid egg.
Aneuploid and normal diploid cells can occasionallyexist simultaneously in an individual. This condition isknown as mosaicism and involves two or more distinct cellpopulations derived from a single zygote or fertilized egg.Mosaicism can involve either autosomal or sex chromo-somes but most frequently involves sex chromosomes.Mosaicism is seen in approximately 0.2% of fetusesprenatally, 1% of Down syndrome patients, 10% ofKlinefelter syndrome patients and over 30% of patientswith Turner syndrome. The clinical significance of mosai-cism depends upon the proportion and tissue distributionof the aneuploid cells. Chimaerism, in contrast, isdistinguished from mosaicism in that the different celllines are derived from more than one zygote.
Structural abnormalities
Structural rearrangements frequently alter chromosomemorphology. Chromosome morphology is based uponlocation of the centromere or primary constriction that
divides a chromosome into a short arm p and a long armq (Figure 3a). Chromosomes are metacentric when thecentromere is in the middle with short and long arms ofroughly equal length (Figure 3i), submetacentric when thecentromere is closer to one end with short and long arms ofunequal length (Figure 3a), and acrocentric when thecentromere is near one end with very small short arms(Figure 3l). The centromere is essential for correct segrega-tion of chromosomes during cell division.DNA replicationprior to cell division ensures that each chromosome
consists of two identical sister chromatids joined at thcentromere. Chromosomesnormally have one centromerA dicentric chromosome has two centromeres (Figure 3and an acentric chromosome has none. At metaphasewhen chromosomes are typically examined, sister chromatids appear fused as a result of the staining methonecessary to produce the banding patterns essential fochromosome identification (Figures 1 and 2). Each banand subband has an assigned designation that identifies thchromosome arm, region and specific number as publishe
Figure 2 45,X Turner syndrome karyotype demonstrating monosomy X.
(Karyotype prepared by Dave McDonald.)
Table 1 Incidence of chromosomal abnormalities in newborn
Modified from Thompson et al. (1991) Genetics in Medicine, 5th edn
WB Saunders.
Type of abnormality Approximate incidence
Sex chromosome abnormalities in males47,XXY 1/1080 male births47,XYY 1/1080Other 1/1350Total 1/385
Sex chromosome abnormalities in females45,X 1/9600 female births47,XXX 1/960Other 1/2740Total 1/660
Autosomal numerical abnormalities in infantsTrisomy 21 1/800 live birthsTrisomy 18 1/8140Trisomy 13 1/19 000Triploidy 1/57 000Total 1/695
Structural abnormalities in infants (autosomes and sex
chromosomes)Balanced rearrangements
Robertsonian 1/1120 live birthsOther 1/965
Unbalanced rearrangements 1/1675Total 1/395
All chromosome abnormalities
(autosomes and sex chromosomes)
1/160 live births
Table 2 Relative frequencies of different abnormalities ichromosomally abnormal spontaneous abortions
Abnormality Percentage
Trisomies 52
45,X 18
Triploidy 17
Translocations 24
Modified from Harper (1988) PracticalGenetic Counselling, 3rd ednWright.
Chromosomal Syndromes and Genetic Disease
2 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
3/12
by the 1995 International System for Human CytogeneticNomenclature (Figure 3a). Banding patterns are necessaryto identify specific structural rearrangements within orbetween different chromosomes.
Structural rearrangements involve chromosome break-age and reunion within a single chromosome or betweentwo or more different chromosomes resulting in eitherbalanced or unbalanced karyotypes. Rearrangements arebalanced if there is no net change in chromosome material
or unbalanced if there is either a gain (partial trisomy) oloss (partial monosomy) of chromosome material.
The frequency of structural abnormalities varies considerably in different populations. The highest frequencyin spontaneous abortions and the lowest in newborn(Table 4). This reduction can, in part, be explained by fetalosses prior to birth, particularly in those cases witsignificant unbalanced rearrangements.
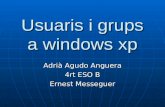
Figure 3 Chromosome structural rearrangements, described in the text. (a) Chromosome arm and numerical banding designations according toISCN (1995). (b) Terminal deletion and (c) interstitial deletion, each with loss of acentric fragment. (d) Pericentric inversion and (e) paracentricinversion, each withrotation of segment between breaks. (f) Direct duplication and (g) inverted duplication. (h) Isochromosome generationfor short an
long arms. (i)Ring chromosome with twoacentricfragments. (j)Insertion of segment from onechromosome into a nonhomologous chromosome.(k) Reciprocal translocation with exchange of segments between nonhomologous chromosomes. (l) Robertsonian translocation between twoacrocentric chromosomes. (Illustration prepared by Dave McDonald.)
Chromosomal Syndromes and Genetic Disease
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
4/12
Unbalanced rearrangements
Unbalanced rearrangements usually result in significantclinical abnormalities due to loss, duplication or both (insome cases) of genetic material. Some examples ofunbalanced rearrangements are deletions, duplications,rings and isochromosomes (Figure 3).
Deletions result in loss of chromosome material from asingle chromosome. Terminal deletions result froma singlebreak within one chromosome arm with loss of materialdistal to the break (Figure 3b). Interstitial deletions involvetwo breaks within the same chromosome arm with loss ofthe material between the breaks (Figure 3c). Ring chromo-somes are formedby breaks occurring in eachchromosomearm with loss of material distal to the breaks and with
subsequent rejoining of the broken ends (Figure 3i). Ringchromosomes vary in size depending upon how muchmaterial has been lost. They are often unstable during celldivision and can, veryrarely, be transmitted fromparent tooffspring.
Duplication of a chromosome segment usually occurs byunequal crossing over between homologous chromosomesor sister chromatids (Figure3f). Duplications can also resultfrom abnormal meiotic segregation in a translocation(Figure 3k,l) or meiotic crossing over in an inversion(Figure 3d,e) carrier. In general, duplications are lessharmful than deletions but they inevitably are associatedwith some clinical abnormalities. The degree of clinical
severity is correlated with size of the duplicated segment.An isochromosome is a chromosome consisting of two
identicalcopiesofonearmandnoneoftheother(Figure3h).In a person with 46 chromosomes, an isochromosomeresults in partial monosomy and partial trisomy. Isochro-mosomes most likely result from exchange betweenhomologues during meiosis, or frombreakage and reunionof sister chromatids near the centromere. Centromeremisdivision during meiosis II is also considered to be a
possible, though less likely, mechanism. Themost commoisochromosome involves the long arm of the X-chromo
some which is frequently seen in individuals with Turnesyndrome. Most X-isochromosomes are actually dicentricInactivation of one centromere makes this abnormachromosome more stable during cell division. Autosomaisochromosomes also occur and most frequently involvacrocentric chromosomes with loss of their short armUnbalanced isochromosomes are always associated witclinical abnormalities owing to their inherent genetimbalance.
Balanced rearrangements
Carriers of balanced chromosomal rearrangements ar
usually clinically normal if no essential chromosommaterial is lost and no genes are damaged by the breakagand reunion process. However, they can produce unbalanced gametes and have an increased risk for chromosomally abnormal offspring. Balanced rearrangemeninclude inversions, insertions, reciprocal translocationand Robertsonian translocations (Figure 3).
Inversions are rearrangements within a single chromosome resulting from two breaks with the interveninsegment being rotated 1808 prior to reconstitutionInversions are classified as either pericentric, which hava single break in each arm (Figure 3d) or paracentric, whichave two breaks in one arm (Figure 3e). Pericentr
inversions frequently produce a change in the relativarm lengths; paracentric inversions do not but can bidentified by changes in the banding pattern of thchromosome arm affected. Inversion carriers are usuallclinically normal but may have an increased risk fooffspring with partial trisomy and monosomy. This because when chromosomes pair during meiosis ainversion loop is formed when the inverted segment pairwith its normal homologue and if an odd number ocrossovers occur, unbalanced recombinant chromosome
Table 4 Frequency of structural chromosome abnormalities in various populations
Data from various sources.
Structural
rearrangement
Spontaneous
abortions (%)
Prenatal
diagnosis (%) Newborn (%)
Balanced24
0.4 0.2
Unbalanced 0.11 0.05
Table 3 Maternal age related frequency of aneuploid fetuses detected prenatally
Modified from Schreinemachers et al. (1982)Human Genetics61: 318324.
Aneuploid rate per 1000
Maternal age range (years) Total number of fetuses Trisomy 21 Trisomy 18 Trisomy 13 XXX XXY XYY
3549 19 672 9.1 2.5 0.6 1.0 1.3 0.5
Chromosomal Syndromes and Genetic Disease
4 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
5/12
are produced. Pericentric inversions can produce recombi-nants with duplication and deficiency of chromosomesegments. The viability of these recombinant products isdependent upon the size of the unbalanced segments.Recombinant chromosomes derived from paracentricinversions are typically acentric or dicentric and usuallyresult in nonviable offspring since these chromosomes are
unstable during cell division.Translocations result from the exchange of chromosome
segments between two or more nonhomologous chromo-somes. There are three types of translocations: reciprocal,Robertsonian and insertional. Reciprocal translocationsare produced by the exchange of broken-off segmentsbetween two different chromosomes (Figure 3k). Carriers ofbalanced reciprocal translocations are usually normal butthey have an increased risk for unbalanced offspring. Theactual risk is associated with segregation of the transloca-tion components, position of breakpoints and centromerelocation. In general, viability is correlated with size of theunbalanced segment. Robertsonian translocations involve
two acrocentric chromosomes that join near their centro-meres, to form a single chromosome (Figure 3l). Frequently,this single chromosome has two centromeres, resulting in adicentric chromosome. Balanced Robertsonian transloca-tion carriers have only 45 chromosomes including thedicentric chromosome. Carriers of balanced Robertsoniantranslocations are usually clinically normal but have anincreased risk of unbalanced offspring. This risk is higherfor female carriers since males frequently have infertilityproblems. An insertional translocation is the result of threebreaks such that a nonreciprocal change occurs when thesegment from one chromosome is inserted into anotherchromosome (Figure 3j). Insertions are relatively rare since
they involve three breaks. Insertion carriers are clinicallynormal but have an increased risk for offspring with partialmonosomy or partial trisomy for the inserted segment.
Outline of Chromosome Syndromes
Common autosomal trisomies
Trisomy 21 (Down syndrome) is one of the best-recognizedand most common chromosome disorders. It is the singlemost common genetic cause for mental retardation. The
incidence of Down syndrome is approximately 1/800newborns. The risk for having a child with trisomy 21Down syndrome increases with maternal age. Clinicalfeatures include mental and growth retardation, charac-teristic facies and other abnormalities described in Table 5.
Approximately 94% of Down syndrome patients havetrisomy 21 (Figure1) resulting from meiotic nondisjunction,the failure of homologous chromosomes or sister chroma-tids to separate during cell division. In about 95% of casestheextra chromosome 21 is of maternal origin, and of these
cases approximately 80% are due to an error durinmeiosis I. About 4% of Down syndrome patients have aunbalanced Robertsonian translocation involving chromosome 21. Approximately 60% of these translocationinvolve the long arm of chromosome 13, 14, or 15 (mosfrequently chromosome 14). About half of these translocations are de novo and half are inherited from a balance
carrier parent (usually the mother). Nearly 40% ounbalanced Robertsonian translocations involve onlchromosomes 21 and 22. Most of these ( 90%) involv21/21 long-arm fusions or isochromosomes and nearly aare de novo. The rare parent who is a balanced 21/2isochromosome carrier has a 100% risk for having a viabloffspring with Down syndrome. Female carriers obalanced 14/21 or 21/22 Robertsonian translocations hava 1015% risk for an unbalanced Down syndrome childMale carriers have a risk of less than 5%. Mosaicisminvolving a mixture of normal diploid cells and trisomy 2cells is present in about 2% of Down syndrome patients.
Trisomy 18 (Edwards syndrome) is the second mos
common autosomal trisomy syndrome. It has a frequencof about 1 in 8000 live births. Clinical features includfailure to thrive, cardiac and kidney problems and othecongenital abnormalities (Table 5). Postnatal survival ipoor and more than 90% die within the first 6 monthsAbout 80% are female. The incidence of trisomy 1increases with maternal age. Very few cases of trisomy 1mosaicism have been reported. Many features characteristic of trisomy 18 have also been reported in patients witunbalanced translocations involving all or most ochromosome 18 long arm. Based upon limited data, threcurrence risk for trisomy 18 is approximately 1%.
Trisomy 13 (Patau syndrome) is the least common of th
major autosomal trisomieswith an estimated incidence ofin 20 000 live births. Owing to severe clinical abnormalitieincluding central nervous system malformations, heardefects, growth retardation and numerous other congental anomalies (Table 5), trisomy 13 patients rarely survivthe newborn period. Trisomy 13 is associated witadvanced maternal age. The extra 13 usually results froma maternal meiotic nondisjunctional error. About 20% ocases have an unbalanced Robertsonian translocatioinvolving chromosome 13. Balanced 13/14 Robertsoniatranslocation carriers have less than 2% risk of having aunbalanced trisomy 13 offspring. Trisomy 13 mosaicismrare and may be associated with less severe clinica
anomalies.
Common sex chromosome abnormalities
Sex chromosome abnormalities have less severe clinicaanomalies than those associated with comparable autosomal imbalances. This difference can be attributed tgenetic inactivation of all but one X-chromosome in thoscases where multiple copies are present, and the relativel
Chromosomal Syndromes and Genetic Disease
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
6/12
low gene content of the Y-chromosome. Sex chromosomeaneuploidy is relatively common, with overall frequency ofabout 1 in 500 live births (Table 1). Some (XXX, XXY,XYY) are relatively frequent in newborns but rare inspontaneous abortions. Monosomy X (Turner syndrome),in contrast, is one of the most common chromosomeabnormalities seen in spontaneous abortions but relativelyrare in newborns.
Turner syndrome (45,X)
The frequency of Turner syndrome is about 1 in 8000newborn females. Clinical features in newborns ofteninclude webbed neck, low hairline, puffy hands and feet,wide spaced nipples and cardiovascular problems. Later inlife, these girls are typically short, sexually immature andinfertile (Table 5). Slightly more than 50% of Turnersyndrome patients have a 45,X karyotype (Figure 2). Theremaining Turner patients have other sex chromosomeabnormalities of the X-chromosome involving isochromo-
somes, short-arm deletions and rings. About 30% ofTurner patients are mosaics consisting of 45,X cells plusother cells with two or more normal X-chromosomes,structurally abnormal X-chromosomes or a Y-chromo-some.
Approximately 9599% of 45,X conceptions fail tosurvive to term and account for about 18% of chromoso-mally abnormal spontaneous abortions. The incidence of45,X is not associated with maternal age. The paternal X-chromosome is missing in about 75% of 45,X patients.
Klinefelter syndrome (47,XXY)
Klinefelter syndrome has a frequency of about 1 in 100newborn males (Table 1). Unlike Turner syndrome, malewith Klinefelter syndrome are not usually detected in thnewborn period. These individuals are generally normal iappearance before puberty. After puberty they arfrequently ascertained in infertility clinics or identified btheir small testes, breast enlargement and tall statur(Table 5). Significant mental retardation is not part of th
syndrome but patients have a higher incidence of educational and emotional problems. Most Klinefelter patienthave a 47,XXY karyotype. At least 10% have mosaicisminvolving normal 46,XY cells plus another population ocells with two or more X chromosomes. Mosaic patienthave more variable clinical features and occasionally mahave relatively normal testicular development.
Cytogenetic and molecular data have indicated tha47,XXY is equally likely to result from a maternal opaternal meiotic nondisjunctional error. Maternally derived cases are associated with maternal age. Variants oKlinefelter syndrome include those patients with morthan two X-chromosomes, multiple X-chromosome mo
saicism and multiple Y-chromosomes. The presence oadditional X-chromosomes (more than two) is associatewith increasing severity of clinical abnormalities includinmental retardation, sexual development and skeletaanomalies.
47,XYY syndrome
Approximately 1 in 1000 newborn males have a 47,XYYkaryotype (Table1). XYYmaleshave no discernible clinica
Table 5 Clinical features of patients with common autosomal or sex chromosome aneuploidy
Syndrome Karyotype Main clinical features
Down Trisomy 21 Short, broad hands with single palmar crease, decreased muscle tone, mental
retardation, broad head with characteristic features, open mouth with large tongue
up-slanting eyes
Edwards Trisomy 18 Multiple congenital malformations of many organs, low-set malformed ears, receding
mandible, small eyes, mouth and nose with general elfin appearance, severe mentaldeficiency, congenital heart defects, horseshoe or double kidney, short sternum,
posterior heel prominence
Patau Trisomy 13 Severe mental deficiency, small eyes, cleft lip and/or palate, extra fingers and toes,
cardiac anomalies, midline brain anomalies, genitourinary abnormalities
Turner 45,X Female with retarded sexual development, usually sterile, short stature, webbing of ski
in neck region, cardiovascular abnormalities, hearing impairment, normal intelligenc
Klinefelter 47,XXY Male, infertile with small testes, may have some breast development, tall, mild menta
deficiency, long limbs, at risk for educational problems
Triple X 47,XXX Female with normal genitalia and fertility, at risk for educational and emotional
problems, early menopause
XXY 47,XYY Tall male with normal physical/sexual development, normal intelligence, increased
tendency for behavioural and psychological problems
Data from various sources.
Chromosomal Syndromes and Genetic Disease
6 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
7/12
features at birth or in infancy. Their mental and physicaldevelopment is normal and they are fertile (Table 5).Although most 47,XYY patients are clinically normal,they tend to be taller than normal and have an increasedtendency for behavioural and learning problems aschildren and young adults. Y-chromosome aneuploidyresults from paternal meiotic nondisjunction and is not
associated with maternal age.
Trisomy X syndrome (47,XXX)
The frequency of 47,XXX in newborn females is about 1 in1000 (Table 1) and is associated with maternal age. MostXXX females are clinically normal with normal gonadalfunction and fertility. However, there is an increased riskfor learning disabilities, reduction in performance IQ,menstrual problems and early menopause (Table 5). Fe-males with more than three X-chromosomes (XXXX andXXXXX) have been reported but, in comparison to47,XXX, are quite rare. These tetra-X and penta-X femalesare all mentally retarded and have more severe clinical
problems.
Autosomal deletion and duplicationsyndromes
Identification of common autosomal deletions requiresprecise chromosomal localization of the missing segment.Chromosome banding patterns make this localizationpossible if the deletion is cytogenetically visible. Detectionof common deletions and also very small deletions notvisible by routine cytogenetic analysis (microdeletions) hasbeen made possible by fluorescence in situ hybridization(FISH) technology. This technique involves hybridizingspecific fluorescently tagged DNA probes to metaphasechromosomes, which are detectable by UV excitation.Absence of a locus-specific fluorescent probe from onehomologue is indicative of a microdeletion.
Several common autosomal deletion syndromes aredescribed in Table 6. The critical region for WolfHirsch-horn syndrome has been assigned to 4p16.3. In 90% ofcases the deletion is de novo and in 10% it is inherited as anunbalanced translocation. The deletion is usually visible
cytogenetically, but occasionally it is too small and caonly be identified molecularly with specific DNA probeutilizing FISH methods. Cri du chat syndrome is one of thearliest deletion syndromes to be described. It has aincidence of about 1 in 50 000 births. The critical region habeen mapped to 5p15.2. About 90% of deletions are dnovo and 10% are derived from an unbalanced familia
translocation. LangerGiedion syndrome is a rare condtion with microcephaly and mental retardation. Thcritical region has been assigned to 8q24.11-q24.13. Acytogenetically visible deletion is seen in about 50% ocases.
More recently, a group of autosomal microdeletions ocontiguous gene syndromes have been identified that hava consistent but complex phenotype associated with a versmall (usually 5 5 Mb) chromosomal deletion. Althougsome microdeletions are cytogenetically visible, the currenmethod is to identify these syndromes by FISH utilizinfluorescently labelled DNA probes specific for the deletesegments. Some of the more common microdeletio
syndromes are described in Table 7. In Williams syndromabout 96% of patients have a deletion for the elastin genwhich produces a protein necessary for elasticity of largblood vessels, skin and other organs. The de novo deletiois of maternal origin in 61% of cases and paternal in 39%Genomic imprinting, the differential expression of alleledepending on the parent of origin, has been reported fothe maternal deletion group of Williams patients since thehad significantly more severe growth retardation anmicrocephaly than the paternal deletion group. Somgenes mapped to the WAGR critical region have alsrevealed genomic imprinting. The incidence for PraderWilli syndrome and Angelman syndrome is approximatel
1 in 10 000 births, respectively. About 60%of PraderWiland Angelman syndrome patients have a cytogeneticallvisible deletion in the same region of chromosome 15FISH analysis identifies a microdeletion in about 70% ocases of both syndromes. DNA polymorphism demonstratedthat in PraderWillisyndrome the deleted15 was opaternal origin and was of maternal origin in Angelmasyndrome patients. These observations suggested that thdifference in clinical features for patients with identica
Table 6 Common autosomal deletions
Syndrome Chromosome region deleted Main clinical features
WolfHirschhorn 4p16.3 Severe growth retardation, midline facial defects, mental retardation
small head, prominent frontal bone between eyebrows, cleft lip/
palate, cardiac defects, wide-spaced eyes, broad nasal bridge
Cri du chat 5p15.2 High-pitched cry, wide-spaced e yes, s mall c hin, s mall h ead, r ound f ac
severe psychomotor and mental retardation
LangerGiedion 8q24.11-q24.13 Small head, mental retardation, sparse hair, bulbous nose, short
stature, multiple cartilaginous growths on bone surfaces
Data from various sources.
Chromosomal Syndromes and Genetic Disease
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
8/12
deletions implies differential expression depending uponparental origin (genomic imprinting). About 30% ofPraderWilli patients have two copies of maternalchromosome 15 and no paternal copy, a condition calleduniparental disomy (UPD). Fewer than 5% of Angelmanpatients have paternal UPD for chromosome 15. A smallproportion (1% PraderWilli and 4% Angelman) have
neither deletions nor UPD but have abnormal methylationpatterns (differential expression of imprinted genes) at lociin 15q11-q13 due to imprinting mutations. At least 20% ofnondeletion, non-UPD 15, normally methylated andcytogenetically normal Angelman patients have othergenetic mutations. A visible cytogenetic deletion is seenin about 50% of MillerDieker syndrome patients. FISHanalysis identifies a microdeletion in 90% of all MillerDieker patients.Hemizygosity for an interstitialdeletion ofchromosome 22q11.2 is associated with variable butoverlapping syndromes known as Catch 22, DiGeorgesyndrome and velocardiofacial syndrome. As a group,these syndromes have an incidence of about 1 in 5000 births
and may account for 5% of all congenital heart defects.Cytogenetic deletions are seen in about 30% of thesepatients. FISH analysis is much more sensitive andidentifies 8590% of patients with microdeletions.
Autosomal duplication syndromes are much less com-mon than autosomal deletion syndromes. Several auto-somal duplication syndromes are described in Table 8.BeckwithWiedeman syndrome has an incidence of 1 in13 700 births. Approximately 85% are de novo and 2028% of these cases are due to paternal UPD for region
11p15.5. Fifteen per cent of cases are familial, due tmaternal carriers with translocations or inversions with breakpoint on 11p. These female carriers are clinicallnormal but their offspring may have clinical effectsuggesting a role for genomic imprinting. Cytogenetiabnormalities are present in 23% of BeckwithWiedeman patients. The most frequent abnormality is duplica
tion of 11p13!p15 resulting from the unbalancesegregation of a paternal translocation or inversion. Dnovo 11p15.5 duplications of paternal originhave also beereported in some patients with BeckwithWiedemasyndrome. Patients with duplication or trisomy fo11p15.5 have a higher incidence of clinical abnormalitiethan those with normal chromosomes. CharcotMarieTooth disease type 1A (CMT1A) is the most commoinherited peripheral neuropathy in humans and has prevalence rate of 1 in2500. In most cases CMT1A patienthave normal chromosomes with duplication of DNAmarkers within 17p11.2!p12. A number of CMT1Apatients have been reported with cytogenetically visibl
duplication of 17p11.2p12, demonstrating that this syndrome is correlated with a gene dosage effect for thchromosome region. Misalignment of homologous chromosomes resulting in unequal crossing over between nonsister chromatids during meiosis is the most likelmechanism for this type ofde novo chromosome duplication. Cat-eye syndrome results from duplication of thproximal portion of the chromosome 22 long arm. Thmost common form of this duplication is a supernumerar(extra) dicentric bisatellited chromosome 22 designated a
Table 7 Autosomal microdeletion syndromes
Syndrome
Chromosome
region Incidence Main clinical features
Williams 7q11.23 1/20000 Cardiac anomalies, mental retardation, characteristic facies, growth
retardation, gregarious disposition, connective-tissue problems
WAGR 11p13 Kidney tumour, absence of iris, genital abnormalities, growth retardatio
PraderWilli 15q11.2 1/10000 Developmental delay, mental retardation, decreased muscle tone, obesity
small genitals, excessive appetite, hypopigmentation
Angelman 15q11.2 1/10 000 Developmental delay, mental retardation, unstable gait,absence ofspeech
hyperactivity, spontaneous laughter, hypopigmentation
MillerDieker 17p13.3 Smooth brain, small head, small chin, growth failure, cardiac abnormalitie
SmithMagenis 17p11.2 1/25000 Flat midface, wide head, broad nasal bridge, short fingers and toes, ment
retardation, hyperactivity, short stature, characteristic behaviouralproblems
Alagille 20p11.23-p12.2 Chronicbile flow suppression, dysmorphic facies, ring-likecornealopacit
vertebral arch defects, narrowing of heart opening
Catch 22 22q11.2 Cardiac defects, abnormal facies, underdeveloped thymus, cleft palate,
decreased calcium in blood
DiGeorge 22q11.2 1/5000 Underdeveloped thymus and parathyroid glands, facial abnormalities,
cardiac defects
Velocardiofacial 22q11.2 Cleft palate, abnormal nose, developmental delay, cardiac abnormalities
Data from various sources.
Chromosomal Syndromes and Genetic Disease
8 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
9/12
inv dup(22)(q11.2). This inverted duplication processrequires breakage at 22q11.2 in each of two sister or non-sister chromatids and produces a chromosome containingtwo copies of the cat-eye syndrome critical region(CESCR) or a total of four copies for the patient. Thesepatients typically have 47 chromosomes owing to thepresence of the supernumerary inv dup(22)(q11.2).
Chromosome instability syndromes
There are several rare inherited syndromes characterizedby increased rates of spontaneous or induced chromoso-mal breakage and predisposition to leukaemia and solidcancers. The most extensively studied of these syndromes,each caused by a different autosomal recessive gene, areBloom syndrome, Fanconi anaemia, ataxia telangiectasiaand xeroderma pigmentosum. These syndromes havedistinctive chromosome aberrations. Bloom syndrome ischaracterized by quadriradial formations, which is theexchange of chromatid segments between two chromo-somes, and a high rate of sister chromatid exchange (SCE)or exchanges betweenhomologous chromosome segments.Fanconi anaemia patients exhibit a high frequency ofchromosome breakage and nonhomologous chromosomeinterchange following exposure to alkylating agents orultraviolet radiation. Their SCE rate is normal.Individualswith ataxia telangiectasia show an increased level ofchromosome breaks and rearrangements and may haveabnormalities involving chromosome 14. These patientshave a normal SCE level. Patients with xerodermapigmentosum do not exhibit spontaneous chromosomebreakage; however, rearrangement, breaks, and increasedSCE rate are observed after exposure to ultravioletradiation.
Maternal Age Effects
Prenatal and live birth risks for trisomy 21 Downsyndrome are well established and are clearly associatedwith maternal age (Table9). In addition to trisomy 21, otherviable autosomal and sex chromosome aneuploidies, i.e.
trisomy 13, trisomy 18, XXX and XXY are also associatewith maternal age (Table 10).
Over 50% of chromosomally abnormal spontaneouabortions are trisomic for various chromosomes and, as group, are more frequently associated with maternal agwhen compared to polyploid and nontrisomic abortionOther chromosomally abnormal spontaneous abortion
with sex chromosome monosomy (45,X), triploidy, tetraploidy and various other structural abnormalities are noassociated with maternal age.
The risk for aneuploidy increases with maternal agprimarily owing to meiotic nondisjunction errors associated with reduced recombination or crossing over prioto the first meiotic division. This relationship has beedemonstrated in Down syndrome patients with trisomy 2Using DNA polymorphisms, the extra chromosome 2was identified to be of maternal origin in over 90% of caseand in approximately 80% of these cases nondisjunctiooccurred during the first meiotic division. A similarelationship implicating a higher frequency of maternanondisjunction errors has also been reported for trisom13, 16, 18, XXX and XXY.
In addition to being associated with various aneuploisyndromes, the maternal age effect has also been observein cases involving structural rearrangements associatewith nondisjunction and segregation errors. Data fromsome balanced translocation carriers indicate that the risfor unbalanced offspring due to 3:1 disjunction increasewith maternal age similarly to the risk pattern for trisom21. A maternal age effect has also been reported for some dnovo structural rearrangements, particularly those invoving bisatellited supernumerary marker chromosomes.
In contrast to maternal age-related risk for aneuploidyyounger women (less than 30 years of age) have aincreased recurrence risk for another trisomy 21 pregnancabove what is normally expected for their age. In womeaged 30 or older, the recurrence risk for trisomy 21 isimilar to their age-related risk. The reason for the higherecurrence risk in younger women is not known. In cases ofamilial Robertsonian translocations involving chromosome 21, the risk for an unbalanced Robertsoniatranslocation Down syndrome is higher for women les
Table 8 Autosomal duplication syndromes
Syndrome
Chromosome
region duplicated Main clinical features
BeckwithWiedemann 11p15.5 Large tongue, tissue and organ overgrowth, mild mental retardation
CharcotMarieTooth
disease type 1A
17p11.2-p12 Decreased reflexes, progressive distal muscular wasting, decreased
muscle tone, sensory neuropathy
Cat-eye 22pter-q11.2 Eye defects, absence of anal opening, skin tags in front of ears,characteristic facies, renal, skeletal and genital anomalies, mental
retardation
Data from various sources.
Chromosomal Syndromes and Genetic Disease
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
10/12
than 30 years of age than for those over 30. In this situation,lack of a maternal age effect can be attributed to knowledgeof being a translocation carrier and the impact of thisknowledge upon the decision to have more children.
Recurrence RisksRecurrence risks for chromosomal abnormalities dependupon the type of abnormality, i.e. numerical or structural,
its origin (de novo or familial) and the sex of the carriepatient. The empirical recurrence risk for trisomy 21 foparents with normal chromosomes is approximately 1%and increases to 2% if the mother is aged 40 or over. Thiindicates that in younger women the recurrence risk iincreased over what is expected for their age, while iwomen 35 years or older the risk is age-related. With th
exception of trisomy 21, the recurrence risk for othespecific aneuploidy or polyploid conditions is rare.
Recurrence risk for unbalanced offspring of carriers witvarious structural rearrangements has been deriveempirically (Table 11). Relatively specific risk estimateare known for more common types of Robertsoniatranslocations. The recurrence risk for an unbalanceRobertsonian translocation Down syndrome child dependent upon which parent is the 14/21 or 21/22 carrieHowever, ifa person is a 21/21 carrier,the recurrence risk100% regardless of which parent is the carrier.For carrierof 13/14 Robertsonian translocation, the risk for aunbalanced trisomy 13 offspring is 12%.
Carriers of balanced rearrangements are usually clincally normal but have an increased risk for producinunbalanced offspring. Risk for unbalanced gametes osegregation products depends upon location of chromosome breakpoints relative to the centromere and crossovefrequency. Since it is difficult theoretically to predict thrate of unbalanced offspring to be expected for anparticular structural rearrangement, risk estimates arbased upon pooling of pregnancy outcome data from atranslocation or inversion carriers (Table 11).
More precise risk figures are available, however, focarriers of t(11;22) translocations since this is probably thmost frequent reciprocal translocation found in human
This translocation is often familial, with reduced fertility imales. Unbalanced probands are nearly always born tcarrier females. The recurrence risk for the unbalance
Table 9 Maternal age incidence of Down syndrome in fetuses
and liveborns
Modified from Thompson et al. (1991) Genetics in Medicine, 5th edn.
WB Saunders.
Incidence
Maternal age (years) At birth
At amniocentesis
(16 weeks)
1519 1/1250
2024 1/1400
2529 1/1100
30 1/900
33 1/625 1/420
34 1/500 1/325
35 1/350 1/250
36 1/275 1/200
37 1/225 1/150
38 1/175 1/120
39 1/140 1/100
40 1/100 1/75
45 and over 1/25 1/20
Table 10 Maternal age and chromosome abnormalities detected at amniocentesis
Modified from Harper (1988) Practical Genetic Counselling, 3rd edn. Wright.
Rate per 1000
Age Trisomy 21 Trisomy 18 Trisomy 13 XXX XXY
All chromosome
anomalies
35 3.9 0.5 0.2 0.6 0.5 8.7
36 5.0 0.7 0.3 0.7 0.6 10.1
37 6.4 1.0 0.4 0.7 0.8 12.238 8.1 1.4 0.5 0.8 1.1 14.8
39 10.4 2.0 0.8 1.2 1.4 18.4
40 13.3 2.8 1.1 1.5 1.8 23.0
41 16.9 3.9 1.5 1.8 2.4 29.0
42 21.6 5.5 2.1 2.4 3.1 29.0
45 44.2 18.0 7.0 62.0
Chromosomal Syndromes and Genetic Disease
10 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
11/12
translocation is approximately 2%. It should also beemphasized that the recurrence risk is substantially higherif the parental rearrangement was originally ascertained
through a liveborn child with an unbalanced chromosomerearrangement, since this identifies unbalanced chromo-some complements that are compatible with survival toterm. In those cases involving a de novo structural
rearrangement, the recurrence risk is generally considereto be negligible.
Summary
Chromosome abnormalities contribute significantly tgenetic disease. This impact is seen in various humapopulations in the effect on the fetus or individual directlor in the ability to produce healthy offspring. Autosomaabnormalities are generally more detrimental than sechromosome abnormalities. Abnormalities involving entire chromosomes or subtle microdeletions can result iclinically abnormal syndromes.
Further Reading
de Grouchy J and Turleau C (1984) Clinical Atlas of Huma
Chromosomes, 2nd edn. New York: Wiley.
Gelehrter TD, Collins FS and Ginsburg D (1998) Principles of Medic
Genetics, 2nd edn. Baltimore, MD: Williams and Wilkins.Harper PS (1988) Practical Genetic Counseling, 3rd edn. Boston, MA
Wright.
Hassold TJ (1986) Chromosome abnormalities in human reproducti
wastage. Trends in Genetics 2: 105110.
Mitelman F (ed.)(1995) An International System for Human Cytogenet
Nomenclature recommendations of the International Standing Commi
tee on Human Cytogenetic Nomenclature, Memphis, Tennessee, USA
October 913, 1994 Basel, Switzerland: Karger.
Nora JJ, Clarke Fraser F, Bear J, Greenberg CR, Patterson D an
Warburton D (1993) Medical Genetics: Principles and Practices, 4t
edn. Philadelphia: Lea and Febiger.
SchreinemachersDM, CrossPK andHook EB(1982) Rates of trisomi
21,18,13 and other chromosome abnormalities in about 20 0
prenatal studies compared with estimated rate in live births. Huma
Genetics 61: 318324.Therman E and Sulsman M (1992) Human Chromosomes: Structur
Behavior and Function, 3rd edn. New York: Springer.
Thompson MW, McInnis RR and Willard HF (1991) Genetics
Medicine, 5th edn. Philadelphia: WB Saunders.
Table 11 Risks of unbalanced offspring for rearrangement
carriers
Type of rearrangement
Percentage
of unbalanced
offspring
Robertsonian translocations
14/21, female 101514/21, male 25
13/14, both sexes 12
21/22, female 1015
21/22, male 12
21/21 both sexes 100
Reciprocal translocations
Pooled, both sexes 612
Ascertained by unbalanced child 20
Ascertained by unbalanced child with
small unbalanced segment
50
Other ascertainment 25
t(11;22)(q23;q11.2) 57Recurrence risk unbalanced t(11;22) 2
Pericentric inversions
Ascertained by unbalanced child 510
Other ascertainment 2
Modified from Nora and Fraser (1993) Medical Genetics: Principlesand Practices, 4th edn. Lea and Febiger.
Chromosomal Syndromes and Genetic Disease
1ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Nature Publishing Group / www.els.net
-
7/27/2019 Web.udl.Es Usuaris e4650869 Docencia Segoncicle Genclin98 Recursos Classe (PDF) RevisionsPDF Chromosyndromes
12/12
Chromosomal Syndromes and Genetic Disease
12 ENCYCLOPEDIA OF LIFE SCIENCES / 2001 N P bli hi G / l