






Idiomas
Páginas
Jurídico

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 1/49
Common antidysrhythmic drugs

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 2/49
Contractile cell Pacemaker
cell

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 3/49

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 4/49

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 5/49

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 6/49
Class II Antiarrhythmics: ß-Blockers
In general all beta-blockers are active at both ß1 and ß2 receptors but to varying degrees
slow SA node impulse formation and depress myocardial
contractility to varying degrees
Effect on ECG is slowing of HR and PR prolongation, withno effect on QRS and QT interval

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 7/49
ß adrenergic receptors and responses tophamacologic manipulation Response toreceptors Location Stimulation Antagonism
ß1Heart Increased HR
and ectopy
Increasedcontractility
Decreased HR
and ectopy
Decreasedcontractility
ß2 Airway (smooth
muscle)
Peripheral
vasculature
Decreased
tone(relaxation)
Decreased
tone(relaxation)
Increased
tone(contraction
)
Increasedtone(contraction)

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 8/49
Class II Antiarrhythmics: ß-Blockers
Relative contraindication include asthma or COPD,advanced CHF, third-trimester pregnancy
Should not be used in pt with bradycardia or greater
than 1o AV block

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 9/49

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 10/49
Indication
Esmolol best suited to control ventricular responserates and break a reentrant circuit in supraventricular
dysrhythmia
Some –blockers decrease morbidity & mortality in
patients with acute myocardial infarction (e.g., metoprolol and
atenolol)
CHF (bisoprolol, carvedilol, and extended-releasemetoprolol)

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 11/49
Esmolol
Action: short-acting drug selectively blocking ß 1-receptors in the myocardium
available only in a parenteral formulation with an
onset of action of 1-4 min, elimination t1/2 9 min
Indications: treatment of supraventricular arrhythmias, including atrial fibrillation/flutter and
sinus tachycardia in acute myocardial ischemia

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 12/49
Esmolol
Dosing and Administration:The loading dose is a 500micrograms/kg bolus over 1 minute, followed by an
infusion at 5micrograms/kg/min for 4 minutes
Adverse Effect: Hypotension is the most common
adverse effect

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 13/49
Labetalol
noncardioselective alpha-adrenergic blocking agentand a selective ß1-adrenergic blocking agent
The alpha-blocking effects > ß1-blocking effects
It is a good choice for treating HT in patients with
myocardial ischemia. It has little effect on cerebral perfusion pressure or
intracranial pressure and can be used in patientswith acute neurologic emergencies
8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 14/49
Propranolol
Noncardioselective ß -blocker without intrinsicsympathomimetic activity
Propranolol slows the sinus rate, depresses AV
conduction, decreases cardiac output
prevents exercise-induced increases in BP, andreduces supine and standing blood pressures
Propranolol also decreases myocardial oxygenconsumption

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 15/49
Propanolol
Propranolol is indicated for a wide variety of supraventricular arrhythmias
include MAT , in particular, those arrhythmias
induced by digoxin or catecholamines; rate control of
atrial flutter or fibrillation with preserved LV function Not commonly use in ED setting because it relatively
long effect
8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 16/49
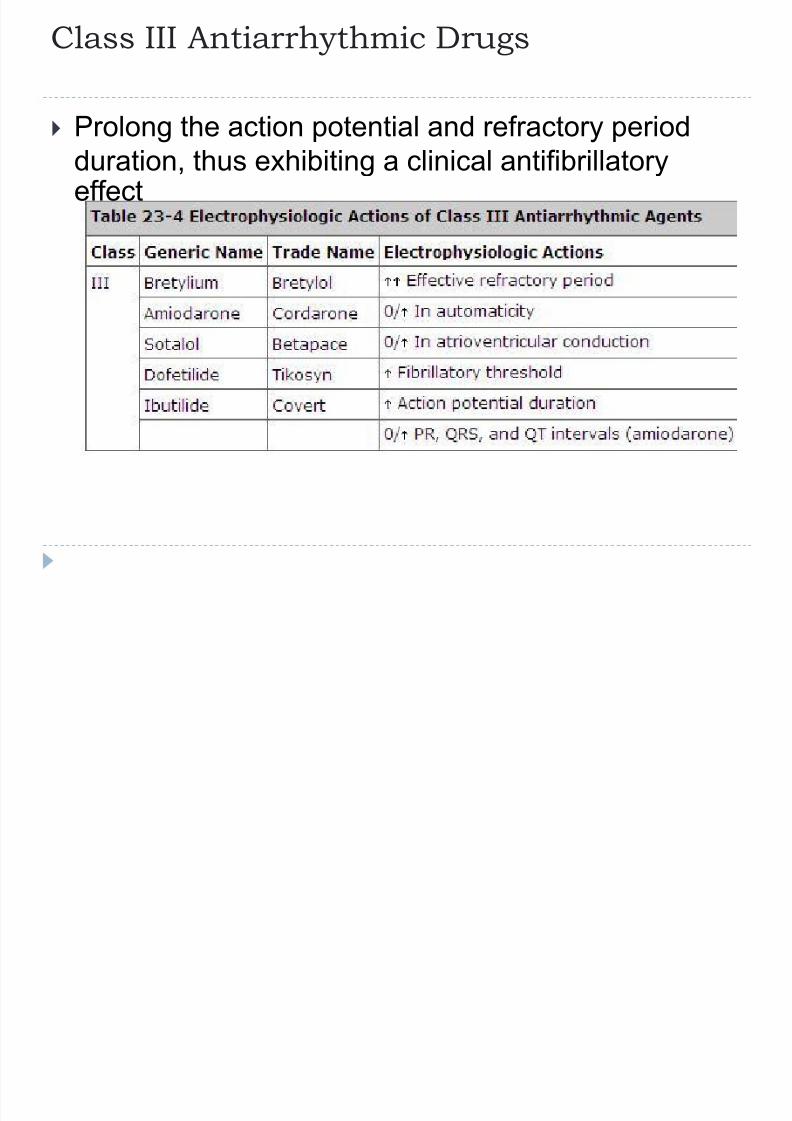
Class III Antiarrhythmic Drugs
Prolong the action potential and refractory periodduration, thus exhibiting a clinical antifibrillatoryeffect

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 17/49
Amiodarone
it also exhibits traits of Class I, II, and IVantiarrhythmics
Amiodarone prolongs the action potential duration
and refractory period ,slow automaticity in
pacemaker cell and slows conduction in the AV node Also displays a noncompetitive blockage of
adrenergic receptors causes smooth musclerelaxation

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 18/49
Amiodarone
When given IV, amiodarone may cause a mild dropin BP and HR
Amiodarone is metabolized in the liver andeliminated by biliary excretion
8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 19/49
Indication
Amiodarone effectively in the suppression andprevention of recurrent Vfib and Vtach, atrial
fibrillation and flutter, and junctional and wide-
complex tachycardias
It is the first-line antiarrhythmic drug in the ACLSpathways for pulseless Vtach and Vfib
it is also indicated to treat atrial arrhythmias in
patients with a significantly ↓ EF (i.e., 40%).

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 20/49
Dose
For Vfib and pulseless Vtach 300-milligram IV bolus, Another 150-milligram bolus
can be given if needed
For stable Vtach or SVT
150 milligrams IV in 100 mL D5W over 10 minutes Follow the loading dose by an infusion at 1 mg/min
for 6 hours, and then 0.5 mg/min thereafter

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 21/49
Amiodarone
For cardioversion of AF the loading dose is 5 to 7 milligrams per kg over 30 -
60 minutes, followed by a continuous infusion of 1.2
-1.8 grams per day until a total dose of 10 grams has
been administered

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 22/49
Adverse Effect Profile
After IV administration, adverse effects are typicallylimited to hypotension and bradycardia

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 23/49
Amiodarone
Long-term oral therapy is associated with thyroid disorders
pulmonary fibrosis
skin discoloration
hepatic dysfunction
corneal infiltrates
Before long-term treatment, patients need baselineophthalmologic and pulmonary function tests
8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 24/49
Amiodarone
Several clinically significant drug interactions increases serum concentrations of many drugs,
including digoxin, procainamide, quinidine,
theophylline
Concurrent use of amiodarone with calcium channelor ß-blockers may potentiate sinus bradycardia,
sinus arrest, and AV block.
Coadministration with simvastatin is associated with
an increased risk of rhabdomyolysis

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 25/49
Ibutilide
An alteranative to IV procainamide for pharmacologic conversion of atrial fibrillation and
atrial flutter in ED
When give in dose of 0.015-0.02 mg/kg
approcimately 50-65% of pt convert to sinus rhythmwithin 20 min
Easier use and a good safety profile offset by higher
cost

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 26/49
Class IV agent: calcium blocker
Block the influx of extracellular calcium through"slow" channels in the cardiac smooth muscle
Verapamil and diltiazem exhibit the most potent
effects on myocardial cell > peripheral vascular
smooth muscle The net result is a slowing of AV nodal conduction
and a prolongation of AV nodal refractoriness

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 27/49
Calcium blocker
effective for rapid conversion of PSVT to NSR and toslow ventricular response in atrial fibrillation or atrial
flutter ( 90% of pt)
Do not use to treat a wide-complex tachyarrhythmia
suggesting an accessory bypass tract (e.g., WPWsyndrome) ), because life-threatening adverseeffects (e.g., Vfib and/or cardiac arrest) may occur

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 28/49
Calcium blocker Adverse effect: hypotension and congestive heart
failure, nausea, vomiting, constipation,
dizziness,nervousness and, pruritus

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 29/49
Diltiazem
Onset 2-3 min after iv administration, peak response
2-7 min, duration 1-3 hr
0.25 mg/kg over 2 min, followed by 0.35 mg/kg 15
min later if the first dose is unsuccessful

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 30/49
Verapamil
The onset of action of verapamil is within 5 minutes,
the peak response is 10 -20 minutes, and the
duration of action is 30 - 60 minutes after IV
administration
the initial dose is 5 to 10 mg(0.1mg/kg )IV bolusgiven over 2 minutes
Reduced to 2.5 to 5.0 mg (0.05mg/kg) in elderly
patients and those with hepatic dysfunction
Check BP immediately before and after verapamiladministration

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 31/49
Verapamil
For the prevention of recurrent PSVT
The dosage is 240 - 480 milligrams/day PO of a
short-acting preparation in four divided doses
long acting is available but not approved for the
treatment of dysrhythmias

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 32/49
Miscellaneous agents Digitalis
Adenosine
Magnesium

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 33/49
Digitalis
Digoxin has three basic actions:
it increases the force, strength, and velocity of
cardiac contractions (positive inotropic effect)
it slows the heart rate (negative chronotropic effect)
it slows conduction velocity through the AV node(negative dromotropic effect)

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 34/49
Digoxin

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 35/49
Digoxin
In therapeutic doses, characteristic ST segment
depress and shortening and T wave inversion
Because it is slow onset and narrow therapeutic
index ,it is not a first line agent for emergencytherapy

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 36/49
Digoxin
Emergently, the first dose iv digoxin dose is 0.5 mg
in adults(Rosen) , 0.25 milligram (Tintinalli)
maximum total dose of 1.5 milligrams
Clinical effect may be seen in 30 min, but the peak
effect is 1.5-2 hr Digoxin is excreted 50-75% unchanged in the urine

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 37/49
Digoxin
The usual oral maintenance dose is 0.125 to 0.375
mg per day
The therapeutic serum digoxin level is 0.8 to 2.0
nanograms/mL
The t1 /2 of digoxin in patients with normal renalfunction is 1.5 -1.8 days and can be extended up to4 - 6 days in patients with renal insufficiency

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 38/49
Digoxin
Side effects of digoxin are enhanced by
hypokalemia, hypomagnesemia, and hypercalcemia,
increased catecholamine
Several drugs can increase serum digoxin levels,
including amiodarone, verapamil, nifedipine,diltiazem, flecainide, quinidine, erythromycin, andtetracycline

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 39/49
Digoxin toxicity
Symptoms of digoxin toxicity
include mental status changes
confusion,
headache, drowsiness
anorexia, nausea,vomiting
Weakness
visual disturbances
Delirium
seizures
Type of arrhythmia can
manifest an increased number of
unifocal or multifocalPVCs
Vtach
junctional tachycardia high-degree AV block
SVT with block
sinus arrest
Atrial fibrillation bradycardia
bidirectional Vtach Vfib

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 40/49
Digoxin toxicity
significant digoxin toxicity itself may produce
hyperkalemia
Lidocaine and phenytoin are antiarrhythmic drugs
that have classically been used in digoxin toxicity,but their efficacy has not been proven

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 41/49
Digoxin toxicity
Digoxin antibody fragments (Digibind, DigiFab) are
indicated for
life-threatening tachyarrhythmia
sinus bradyarrhythmia
severe AV blocks serum potassium >5 mEq/L
Ad i
8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 42/49
Adenosine
is an endogenous nucleoside produced by the
degradation of adenosine triphosphate
Adenosine produces a transient AV nodal block,
which breaks the reentrant circuit of atrial
tachyarrhythmia involving the AV node. Adenosine has no effect on anterograde conduction
over accessory pathways in patients with WPWsyndrome

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 43/49
Adenosine
onset of action of adenosine is 20 to 30 seconds,
with a duration of action lasting approximately 60 to
90 seconds
Adenosine is used for the emergency treatment of
SVT recurrence of the arrhythmia may occur within
minutes after conversion
not effective in converting atrial fibrillation or flutter to
NSR, but it can be used to distinguish these rhythmsfrom other tachyarrhythmias
8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 44/49
Dose
The initial is 6 mg given as a very rapid IV bolus over
1 - 2 seconds directly into the vein or in the most
proximal port of the IV tubing
If the arrhythmia persists, give 12 mg IV rapid bolus
2 minutes later The 12-mg dose can be repeated once, 2 more
minutes later
Follow the bolus dose immediately with a 10- to 20-
mL normal saline flush
8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 45/49
Adenosine
The adverse effects minor and well tolerated, due to
the short half-life
The most common AE include dyspnea, cough,
syncope, vertigo, paresthesias, numbness, nausea,
and metallic taste Cardiovascular AE include facial flushing, headache,
palpitations, retrosternal chest pain, sinusbradyarrhythmia
M i
8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 46/49
Magnesium
directly activating the Na+K+ ATPase pump and
indirectly by calcium channel blockade
It increases membrane potential, prolongs AV
conduction, and increases the absolute refractoryperiod
8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 47/49
Magnesium
The onset is immediate, with a duration of action of
approximately 30 minutes after IV administration
Magnesium is indicated for torsades de pointes and
refractory Vtach/Vfib, regardless of prearrest serum
magnesium levels

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 48/49
Magnesium
The loading dose is
1 - 4 gm in 50 - 100 mL D5W over 20-60 minutes in
patients with spontaneous circulation
1 -2 gm in 10 mL D5W over 1 to 2 minutes in
patients in cardiac arrest. The rate should be reduced or the infusion stopped
temporarily if hypotension develops

8/23/2019 Antiarrhythmia Drug
http://slidepdf.com/reader/full/antiarrhythmia-drug 49/49
Magnesium
Hypotension is the predominant adverse effect but is
surprisingly uncommon, even when a 1- to 2-gram IVbolus dose is given over 1 to 2 minutes
Top Related