






Idiomas
Páginas
Jurídico


Dr. Abel, Calloapaza Pari [email protected]
MR. Cirugía de Tórax y Cardiovascular
HNHU El presente trabajo expresa la opinión personal del autor sobre el tema.


Definición.
Etiología y Epidemiologia.
Cuadro Clínico.
Métodos Diagnósticos.
Opciones terapéuticas.
Pronostico.
Imágenes.

PERICARDITIS CONSTRICTIVA

Constrictive pericarditis is the end stage of an inflammatory
process involving the pericardium.
Libby: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed.

PERICARDITIS CONSTRICTIVA

In the developed world the cause is most commonly: (1 –
3).
idiopathic,
postsurgical, or
radiation injury.
Tuberculosis was the most common cause of constrictive
pericarditis in the developed world before development of
effective drug therapy. It remains important in developing
countries.
1. Troughton RW, Asher CR, Klein AL: Pericarditis. Lancet 2004; 363:717.
2. Hoit BD: Management of effusive and constrictive pericardial heart disease. Circulation 2002; 105:2939.
3. Little WC, Freeman GL: Pericardial disease. Circulation 2006; 113:1622.

Although constriction can follow an initial insult by as little
as several months, it usually takes years to develop.
The end result is dense fibrosis, often calcification, and
adhesions of the parietal and visceral pericardium.
Usually scarring is more or less symmetrical and impedes
filling of all heart chambers.
In a subset of patients the process develops relatively
rapidly and is reversible. This variant is seen most
commonly following cardiac surgery. 1
1. Haley JH, Tajik AJ, Danielson GK, et al: Transient constrictive pericarditis: Causes and
natural history. J Am Coll Cardiol 2004; 43:271.


PERICARDITIS CONSTRICTIVA

The clinical presentation is usually dominated by signs and
symptoms of right-heart failure.
The pathophysiological consequence of pericardial
scarring is markedly restricted filling of the heart. This
results in elevation and equilibration of filling pressures in
all chambers and the systemic and pulmonary veins. In
early diastole the ventricles fill abnormally rapidly because
of markedly elevated atrial pressures and accentuated
early diastolic ventricular suction, the latter related to small
end-systolic volumes. 1. Troughton RW, Asher CR, Klein AL: Pericarditis. Lancet 2004; 363:717.
2. Hoit BD: Management of effusive and constrictive pericardial heart disease. Circulation 2002; 105:2939.
3. Little WC, Freeman GL: Pericardial disease. Circulation 2006; 113:1622.

Systemic venous congestion results in hepatic congestion,
peripheral edema, ascites, and sometimes anasarca and cardiac
cirrhosis. Reduced cardiac output is a consequence of impaired
ventricular filling and causes fatigue, muscle wasting, and weight
loss.
In “pure” constriction, contractile function is preserved, although
ejection fraction can be reduced as a consequence of reduced
preload.
The myocardium is occasionally involved in the chronic inflammation
and fibrosis, leading to true contractile dysfunction that can at times
be quite severe. The latter predicts a poor response to
pericardiectomy.
Libby: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed.

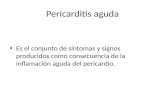
Schematic representation of transvalvular and central venous flow velocities in constrictive
pericarditis. During inspiration the decrease in left ventricular filling results in a leftward
septal shift, allowing augmented flow into the right ventricle. The opposite occurs during
expiration. EA = mitral inflow; HV = hepatic vein; LA = left atrium; LV = left ventricle; PV =
pulmonary venous flow; RA = right atrium; RV = right ventricle.

At a relatively early stage these signs and symptoms include lower
extremity edema, vague abdominal complaints, and some degree of
passive hepatic congestion.
Signs and symptoms ascribable to elevated pulmonary venous
pressures such as exertional dyspnea, cough, and orthopnea may
also appear with progressive disease. Atrial fibrillation and tricuspid
regurgitation, which further exacerbate venous pressure elevation,
may also appear at this stage. In the end stage of constrictive
pericarditis, the effects of a chronically low cardiac output are
prominent including severe fatigue, muscle wasting, and cachexia.
Libby: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed.

El hallazgo semiológico más propio de la pericarditis constrictiva es
el signo de Kussmaul o aumento de la presión venosa yugular
(ingurgitación yugular) durante la inspiración, como
consecuencia de un aumento del retorno venoso, secundario a la
presión negativa intratorácica, pero con restricción al llene
ventricular derecho y sin que haya un aumento simultáneo del gasto
cardíaco. Dado que el corazón está recubierto por una coraza
rígida, la distensibilidad de este se ve muy disminuida y cualquier
aumento de volumen se transmite en forma retrógrada, es por eso
que las yugulares se ingurgitan al inspirar (no como normalmente se
esperaría: al inspirar, las yugulares colapsan)
1. Haley JH, Tajik AJ, Danielson GK, et al: Transient constrictive pericarditis: Causes and
natural history. J Am Coll Cardiol 2004; 43:271.



Medicine.2009; 10(43) :2870-5

Medicine.2009; 10(43) :2870-5

Constrictive pericarditis Doppler schema of respirophasic changes in mitral and tricuspid inflow. Reciprocal
patterns of ventricular filling are assessed on pulsed Doppler examination of mitral (MV) and tricuspid (TV)
inflow. (Courtesy of Bernard E. Bulwer, MD; with permission.)

PERICARDITIS CONSTRICTIVA

No specific ECG findings exist.
Nonspecific T wave abnormalities are often
observed, as well as reduced voltage.
Left atrial abnormality may also be present.
Atrial fibrillation is present in significant numbers of
patients.
Libby: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed.

The cardiac silhouette can be enlarged secondary to a coexisting pericardial
effusion.
Pericardial calcification is seen in a minority of patients and should raise the
suspicion of tuberculous pericarditis, but calcification per se is not diagnostic of
constrictive physiology.
The lateral chest film is useful to detect pericardial calcification along the right
heart border and in the atrioventricular groove.
Isolated calcification of the LV apex or posterior wall suggests ventricular
aneurysm rather than pericardial calcification.
Pleural effusions are occasionally noted and can be a presenting sign of
constrictive pericarditis.
When left heart filling pressures are markedly elevated, pulmonary vascular
congestion and redistribution can be present.
Libby: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed.



Chest radiograph showing marked pericardial calcifications
in a patient with constrictive pericarditis.


CT provides detailed images of the pericardium and is especially
helpful in detecting even minute amounts of pericardial calcification.
Its major disadvantage is the frequent need for iodinated contrast
medium administration to best display findings of pericardial
pathology. The thickness of the normal pericardium measured by CT
is less than 2 mm.
MRI provides a detailed and comprehensive examination of the
pericardium without the need for iodinated contrast or ionizing
radiation. It is somewhat less sensitive for detecting calcification
than CT.
1. Wang ZJ, Reddy GP, Gotway MB, et al: CT and MR imaging of pericardial disease. Radiographics
2003; 23:S167-S180.
2. Oyama N, Oyama N, Komuro K, et al: Computed tomography and magnetic resonance imaging of the
pericardium: Anatomy and pathology. Magn Res Med Sci 2004; 3:145.

CT scan performed during an infusion of contrast material shows enhancement of the soft-tissue-
density pericardium (arrowheads), which is up to 6 mm thick.
Computed Body Tomography by JKT Lee, SS Sagel, and RJ Stanley (Eds) with permission of Raven
Press, New York, ©1989.



Panel A. Echocardiographic transmitral flow pattern with exaggerated respiratory variation in inflow velocities (>25%).
Panel B. Transaxial CT image (slice thickness 3.0 mm) of the heart at mid-ventricular level, demonstrating severe calcification of the pericardium (arrows). In addition, bilateral pleural effusion is seen. AO, descending aorta; PE, pleural effusion.
Panel C. Three-dimensional volume rendering technique reconstruction of the whole chest. Nearly circumferential pericardial calcification is seen (structures of high CT density, such as bone and calcification, are rendered in white colour).
Panel D. Three-dimensional volume rendering technique reconstruction of the heart. To exclude the non-calcified part of the heart, a threshold of 130 Hounsfield units (common threshold for coronary calcification in CT imaging) was chosen.

In mid-diastole, the thickened pericardium
begins to restrict right ventricular filling,
causing a rapid increase in ventricular
pressure. Early changes of septal
flattening and bowing of the
interventricular septum toward the left
ventricle (normally concave in shape
toward the left ventricle during diastolic
filling) are seen. This pressure change
results in diastolic septal dysfunction, the
septal bounce described in
echocardiography.
Frontiers in Bioscience 14, 2688-2703, January 1, 2009


M-mode and two-dimensional echocardiography findings include: Pericardial thickening,
Abrupt displacement of the interventricular septum during early diastole (septal “bounce”), and
Signs of systemic venous congestion such as dilation of hepatic veins and distention of the inferior vena cava with blunted respiratory fluctuation.
Premature pulmonic valve opening as a result of elevated RV early diastolic pressure may also be observed.
Exaggerated septal shifting during respiration is often present. 1
1. Maisch B, Seferovic PM, Ristic AD, et al: Guidelines on the diagnosis and
management of pericardial diseases executive summary; the Task Force on the
Diagnosis and Management of Pericardial Diseases of the European Society of
Cardiology. Eur Heart J 2004; 25:587.

Cardiac catheterization in patients with suspected constrictive
pericarditis provides documentation of the hemodynamics of
constrictive physiology and assists in discriminating between
constrictive pericarditis and restrictive cardiomyopathy.
Although there is limited need for contrast ventriculography,
coronary angiography is used to detect occult coronary artery
disease in those being considered for pericardiectomy. In
addition, on rare occasions external pinching or compression of
the coronary arteries or outflow tract regions by the constricting
pericardium is detected.

Cardiac Catheterization and Angiography

Cardiac Catheterization and Angiography

Cardiac Catheterization and Angiography

Constrictive Pericarditis

Constriction Restriction
Prominent y descent in venous pressure Present Variable
Paradoxical pulse ≈⅓ cases Absent
Pericardial knock Present Absent
Equal right-left side filling pressures Present Left at least 3-5 mm Hg > right
Filling pressures >25 mm Hg Rare Common
Pulmonary artery systolic pressure >60
mm Hg
No Common
“Square root” sign Present Variable
Respiratory variation in left-right
pressures/flows
Exaggerated Normal
Ventricular wall thickness Normal Usually increased
Atrial size Possible LA enlargement Biatrial enlargement
Septal “bounce” Present Absent
Tissue Doppler E′ velocity Increased Reduced
Pericardial thickness Increased Normal
Libby: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed.

Constrictive Pericarditis

Constrictive pericarditis is a progressive disease.
With the exception of patients with transient constrictive
pericarditis, surgical pericardiectomy is the only
definitive treatment.
Libby: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed.

HOSPITAL NACIONAL HIPOLITO UNANUE





Top Related