

Idiomas
Páginas
Jurídico

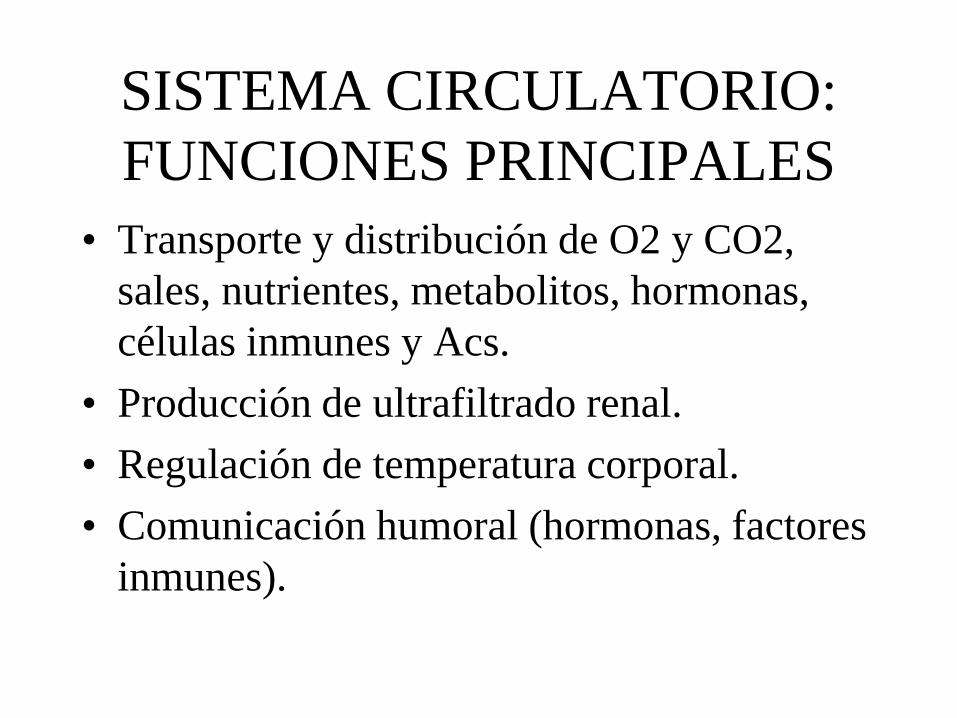
SISTEMA CIRCULATORIO:
FUNCIONES PRINCIPALES
• Transporte y distribución de O2 y CO2,
sales, nutrientes, metabolitos, hormonas,
células inmunes y Acs.
• Producción de ultrafiltrado renal.
• Regulación de temperatura corporal.
• Comunicación humoral (hormonas, factores
inmunes).
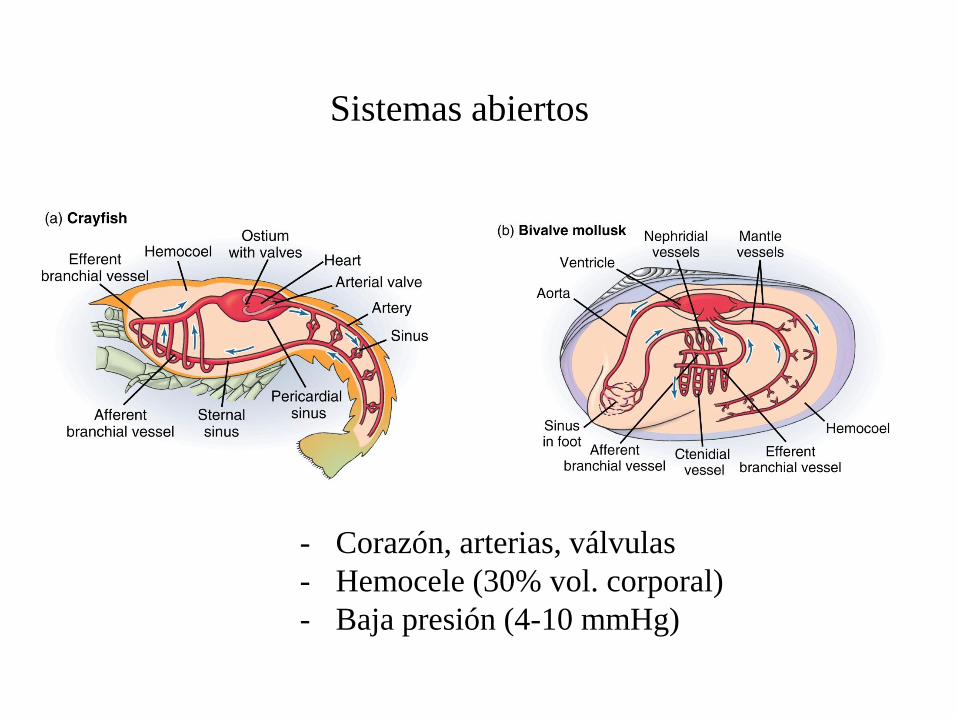
Sistemas abiertos
- Corazón, arterias, válvulas
- Hemocele (30% vol. corporal)
- Baja presión (4-10 mmHg)
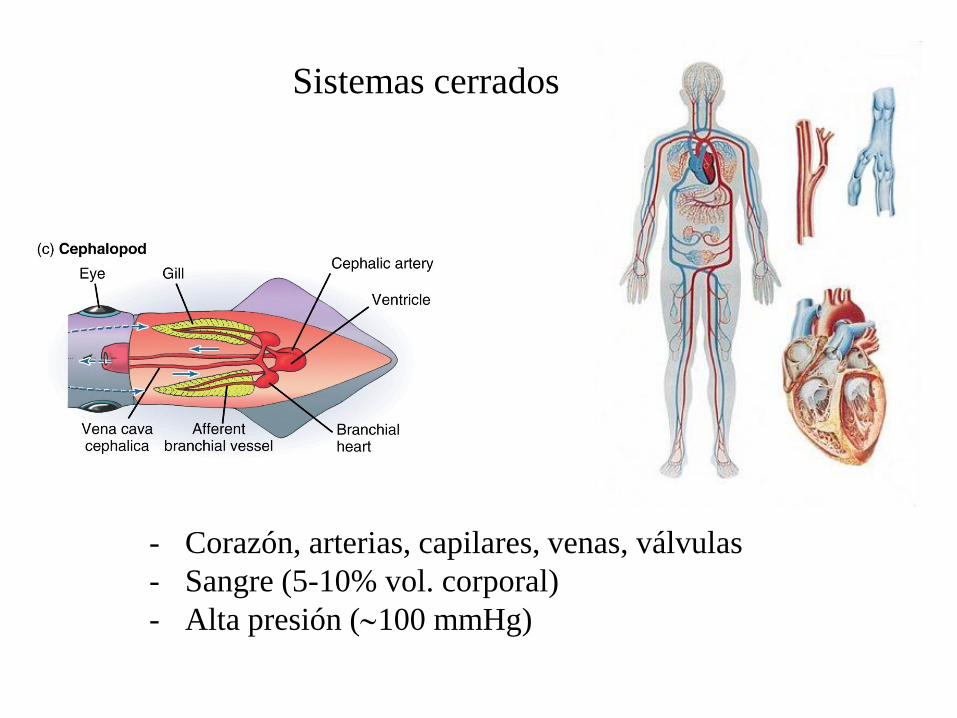
Sistemas cerrados
- Corazón, arterias, capilares, venas, válvulas
- Sangre (5-10% vol. corporal)
- Alta presión (100 mmHg)
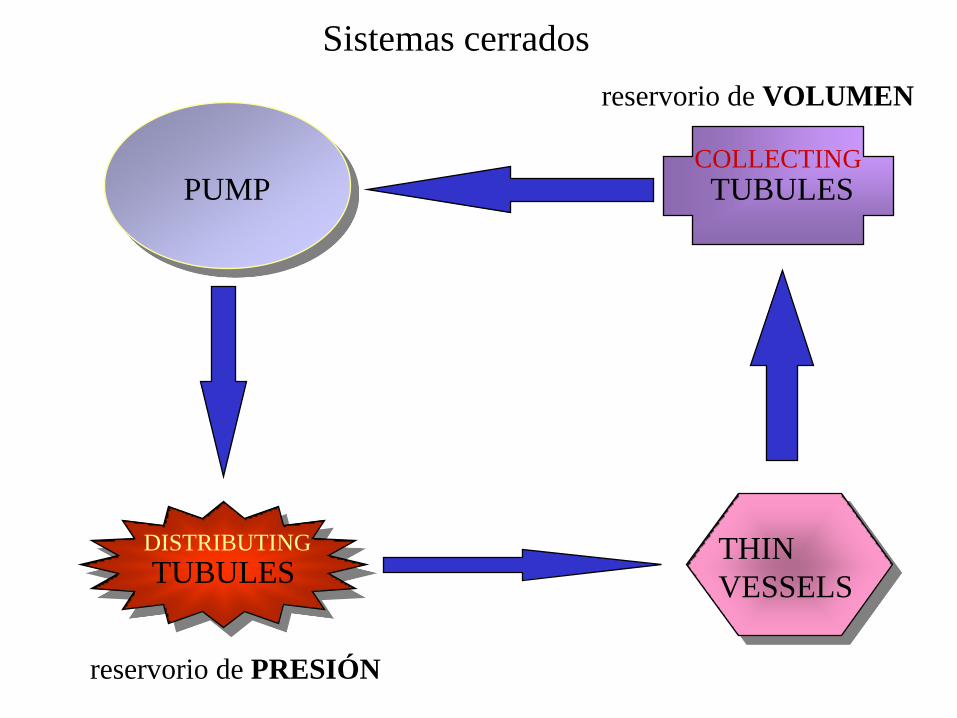
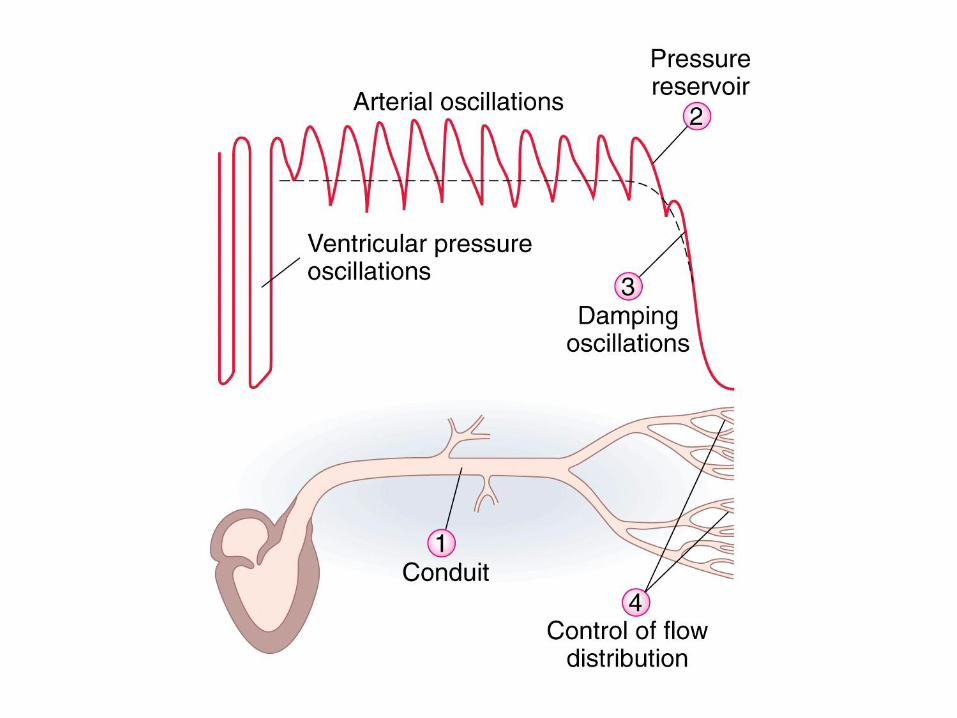
PUMP
DISTRIBUTING
TUBULES THIN
VESSELS
COLLECTING
TUBULES
reservorio de PRESIÓN
reservorio de VOLUMEN
Sistemas cerrados
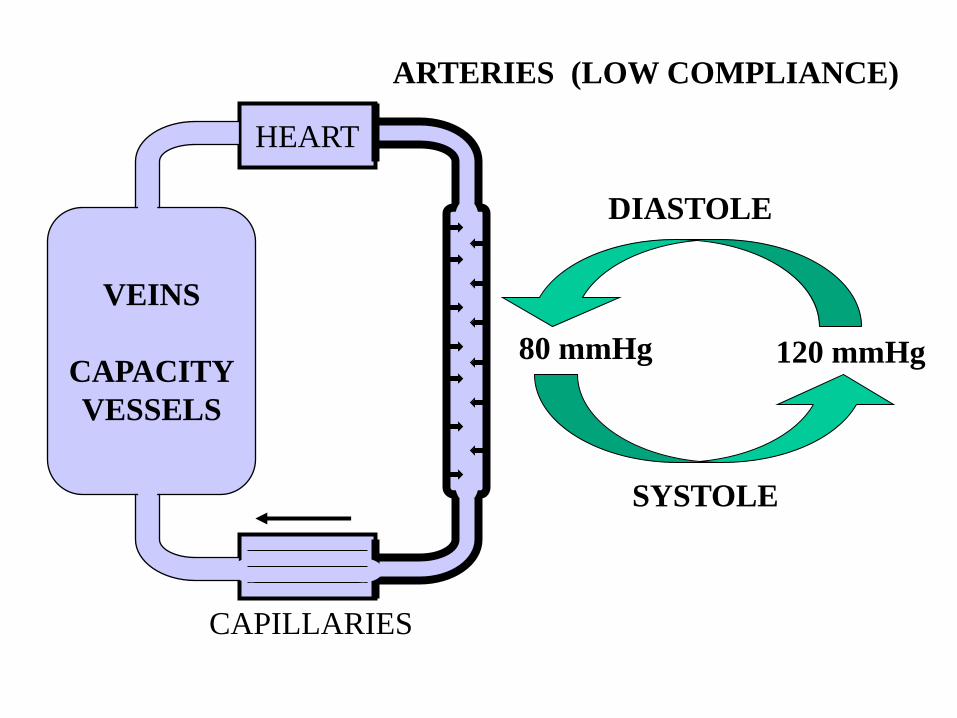
VEINS
CAPACITY
VESSELS
HEART
80 mmHg 120 mmHg
SYSTOLE
DIASTOLE
ARTERIES (LOW COMPLIANCE)
CAPILLARIES
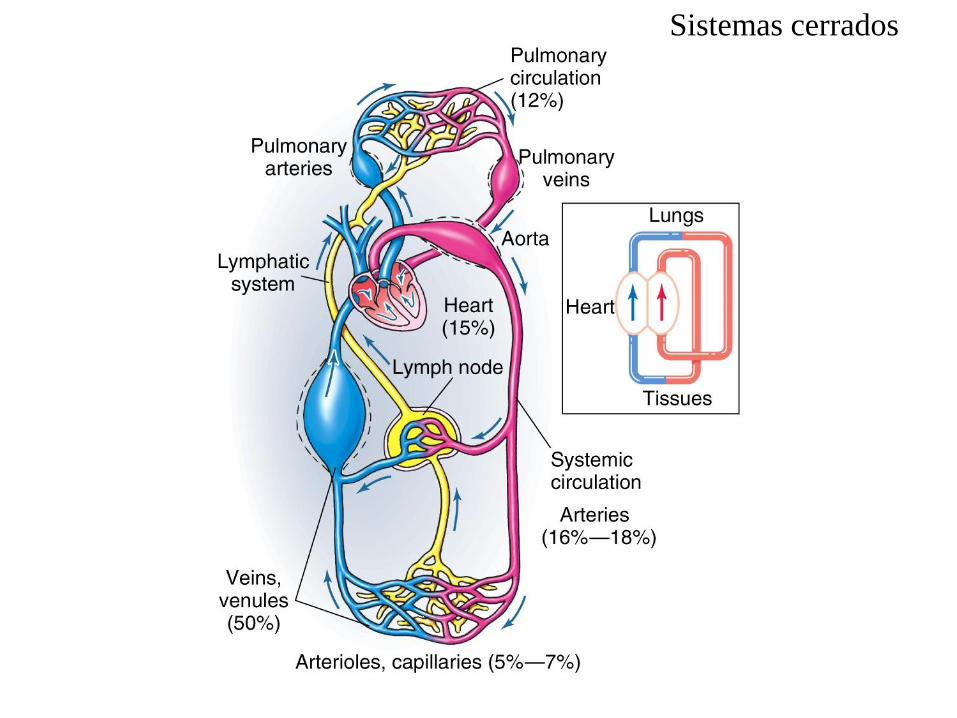
Sistemas cerrados
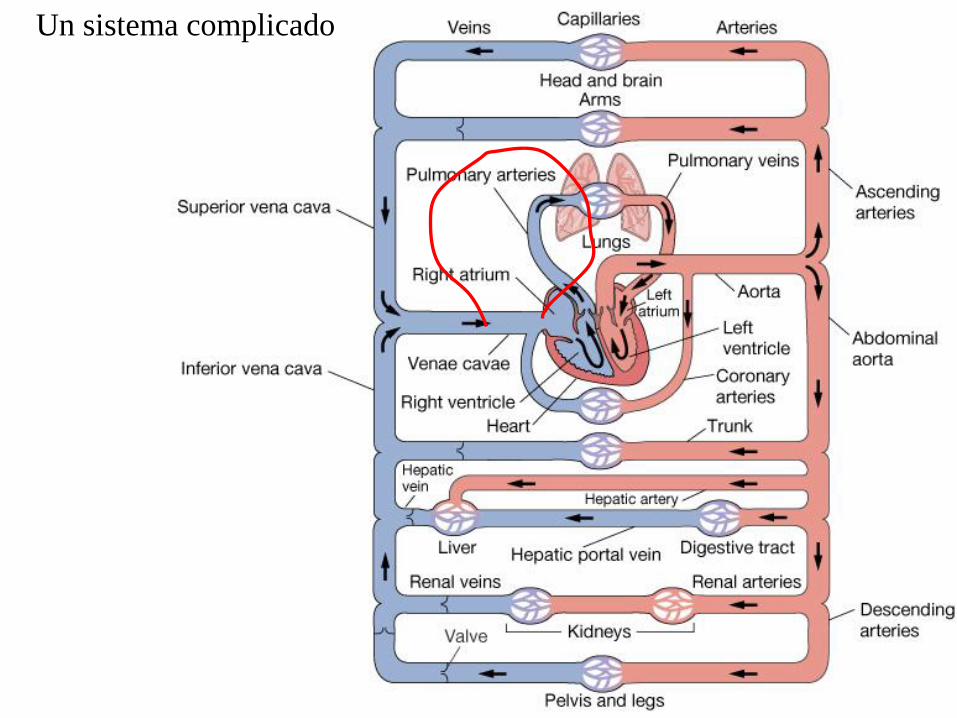
Un sistema complicado
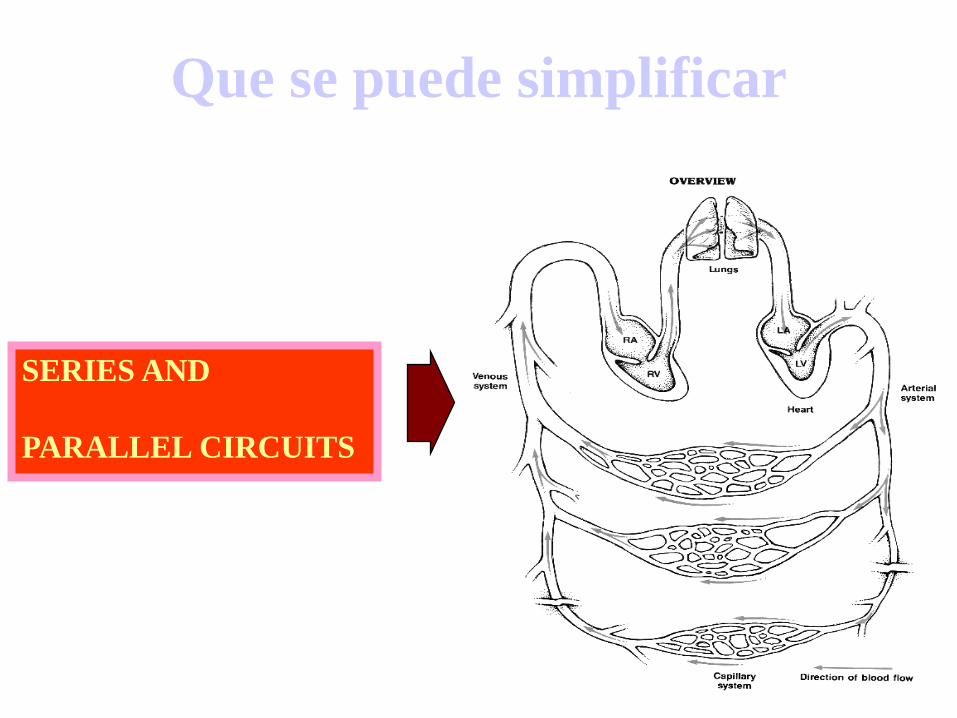
Que se puede simplificar
SERIES AND
PARALLEL CIRCUITS
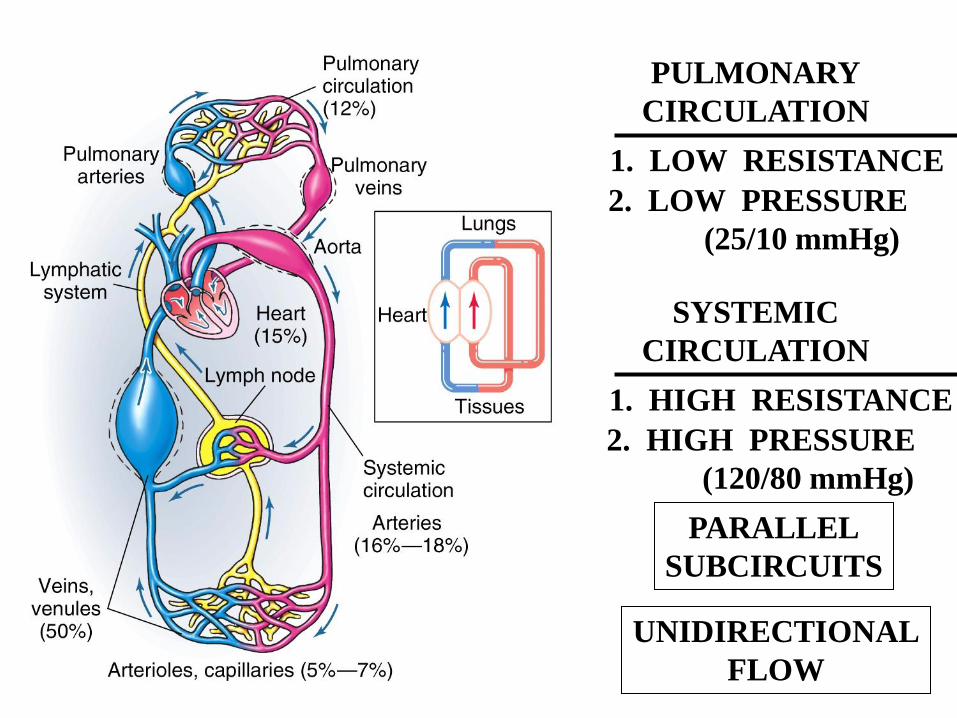
PULMONARY
CIRCULATION
1. LOW RESISTANCE
2. LOW PRESSURE
(25/10 mmHg)
SYSTEMIC
CIRCULATION
1. HIGH RESISTANCE
2. HIGH PRESSURE
(120/80 mmHg)
PARALLEL
SUBCIRCUITS
UNIDIRECTIONAL
FLOW
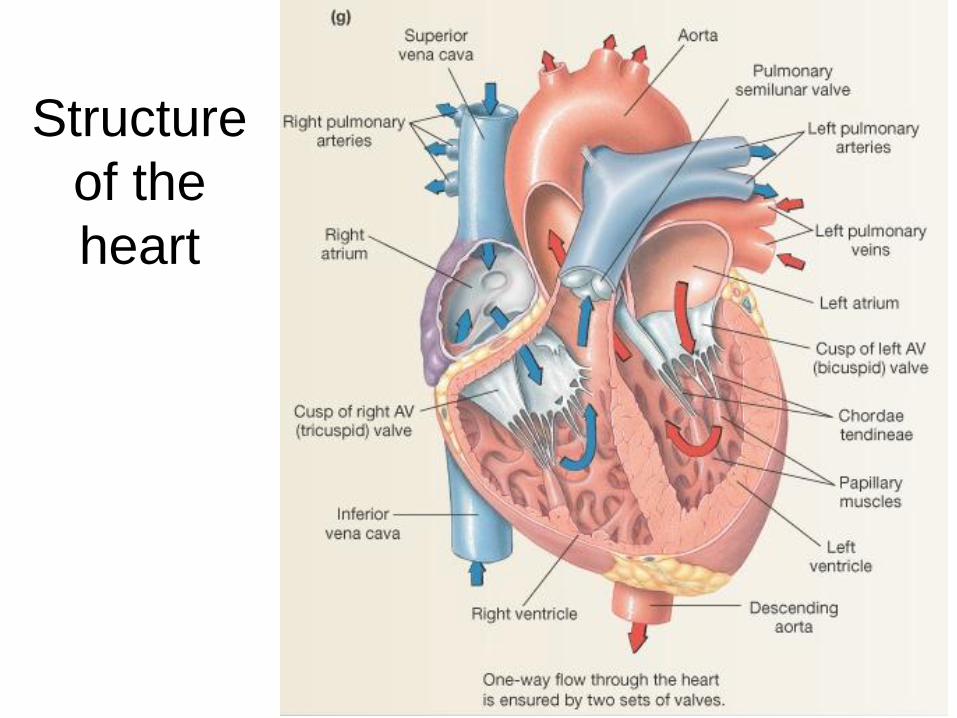
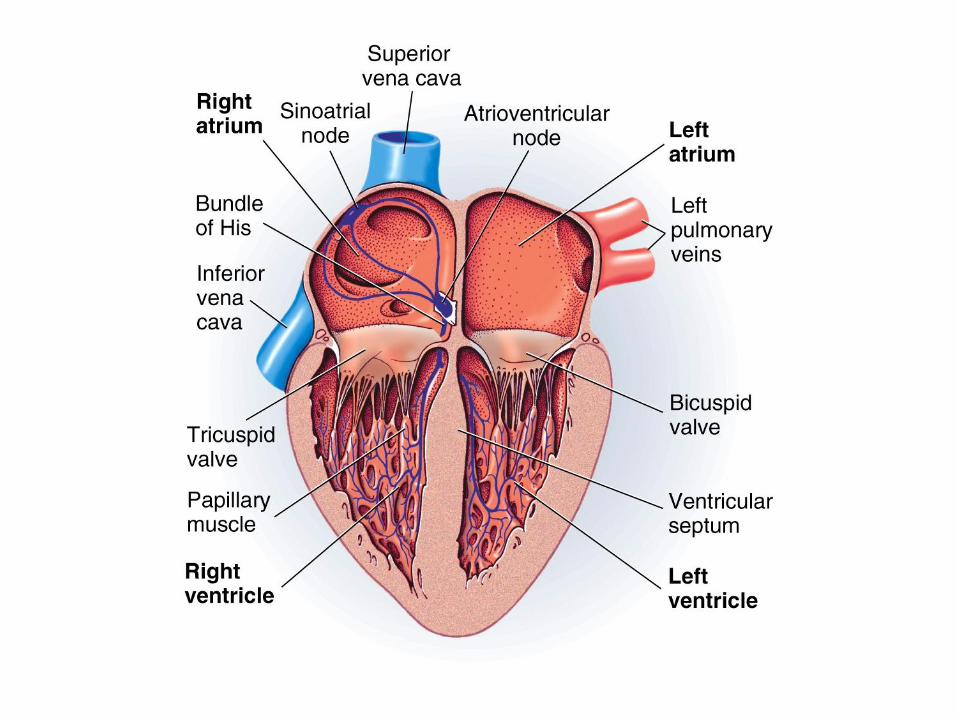
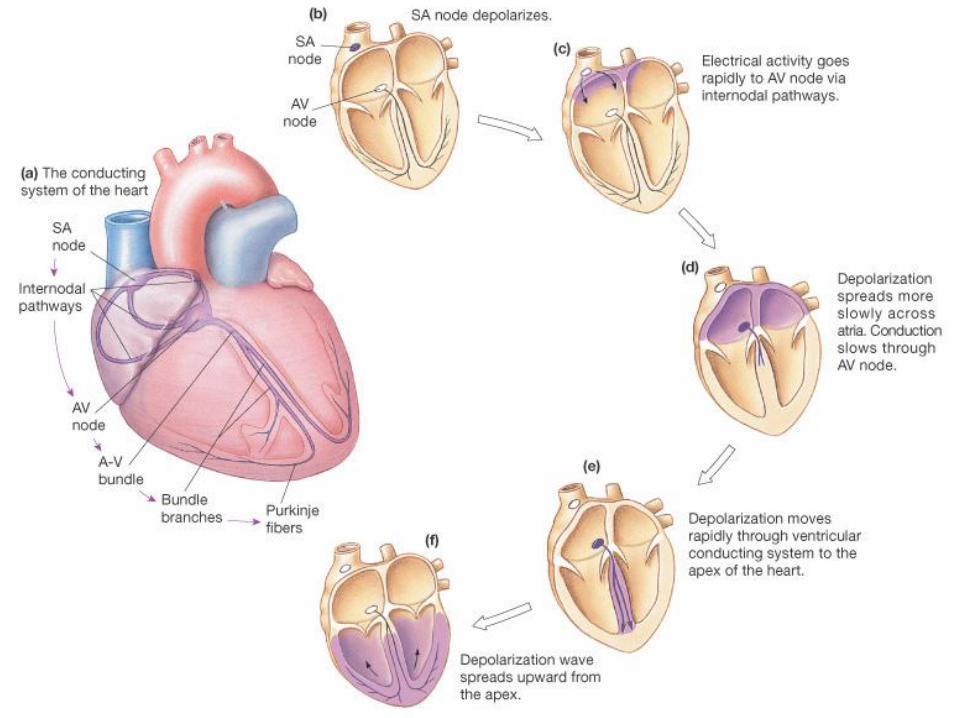
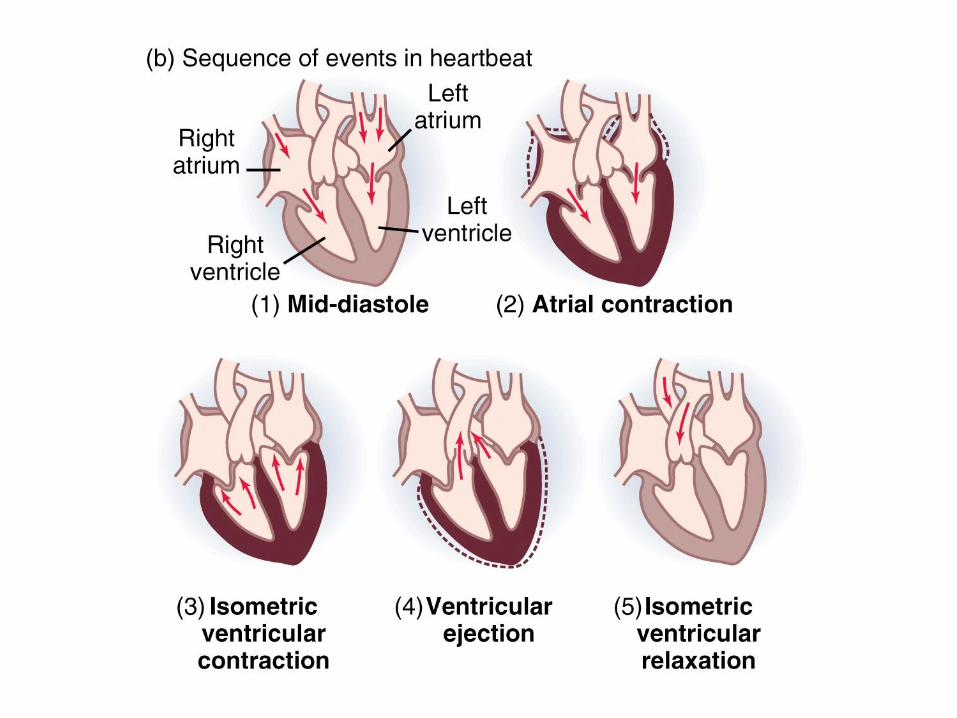
Structure
of the
heart
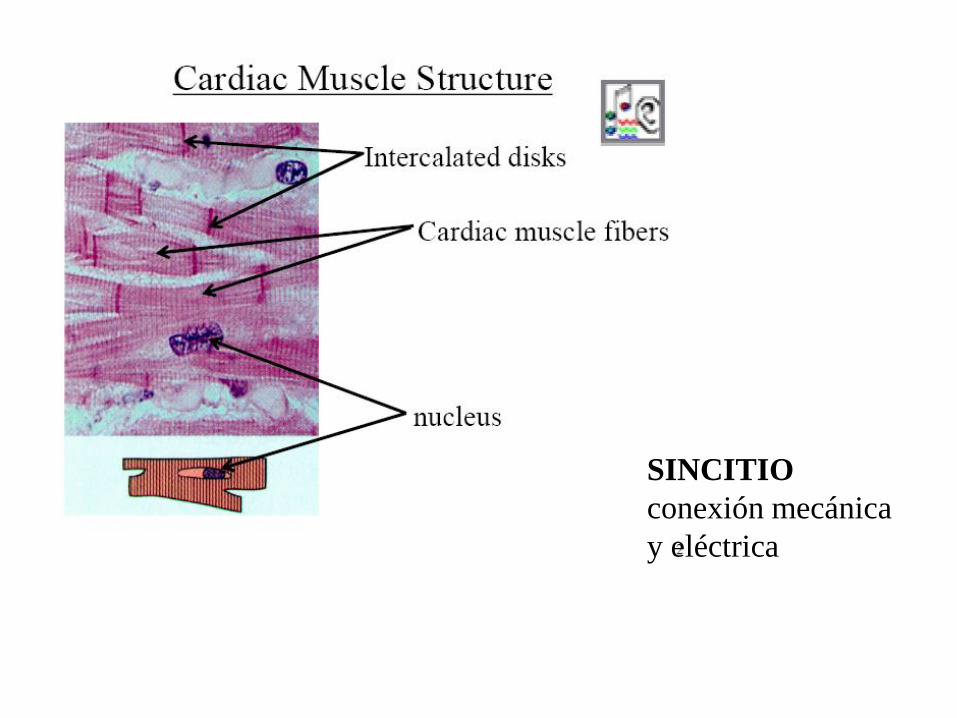
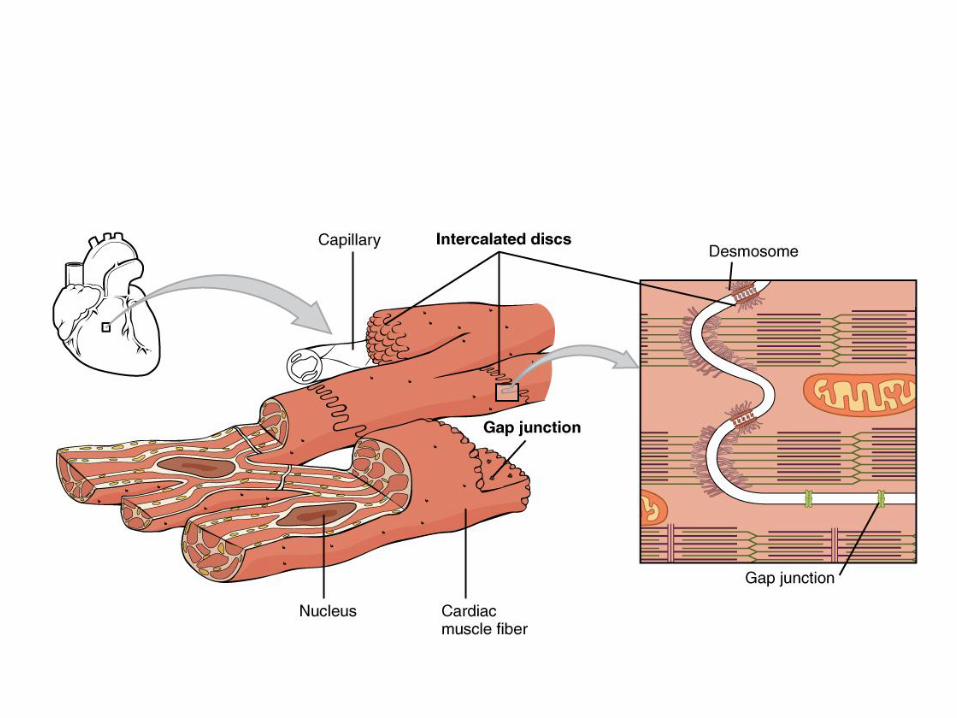
SINCITIO
conexión mecánica
y eléctrica
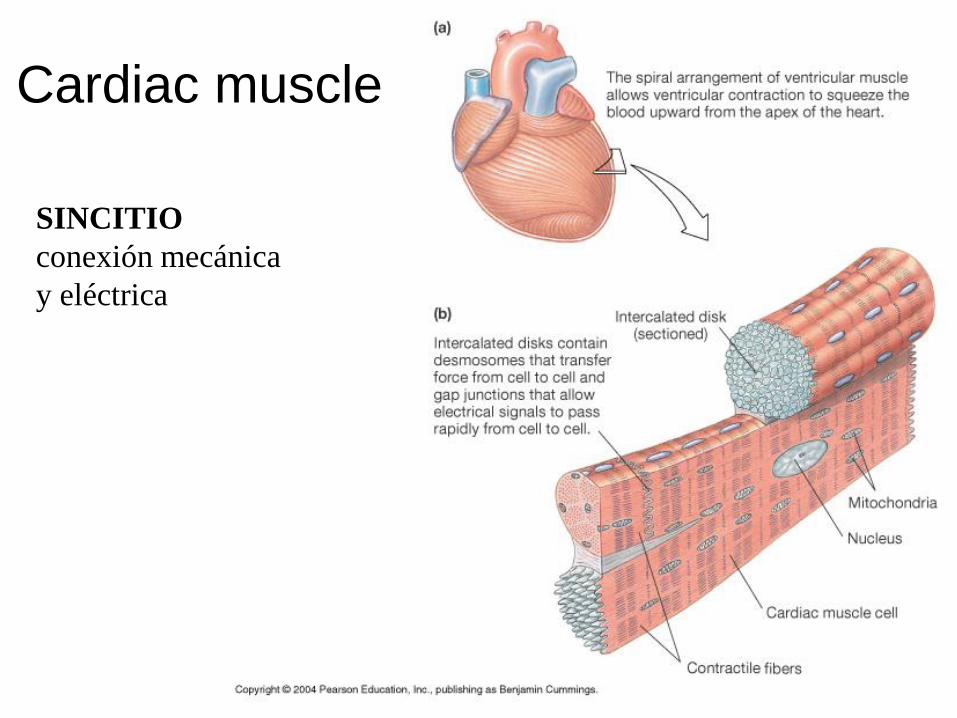
Cardiac muscle
SINCITIO
conexión mecánica
y eléctrica
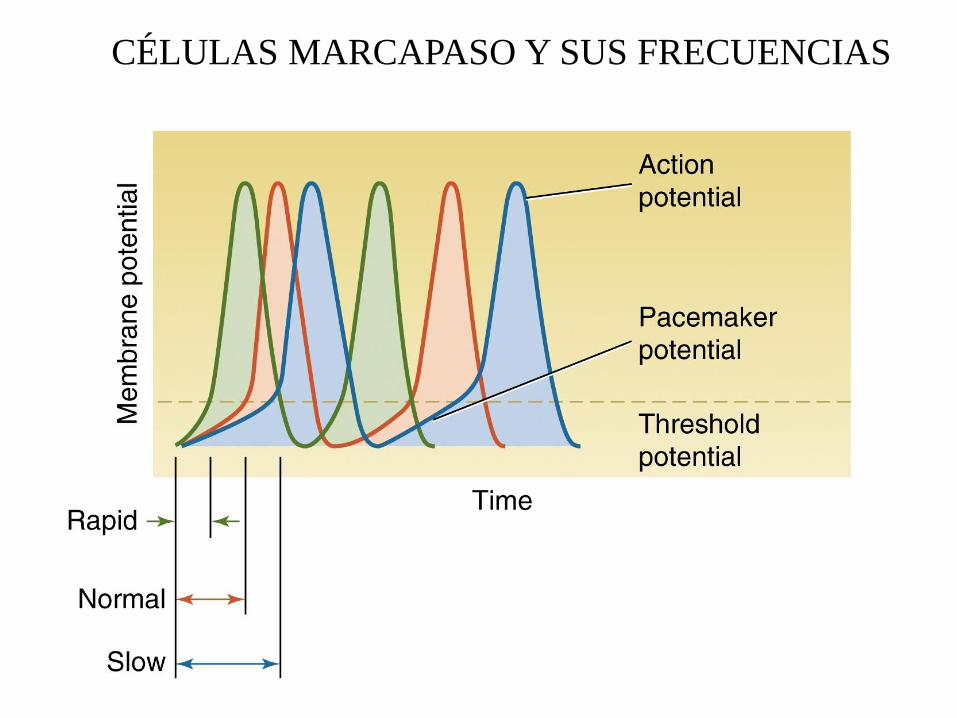
CÉLULAS MARCAPASO Y SUS FRECUENCIAS
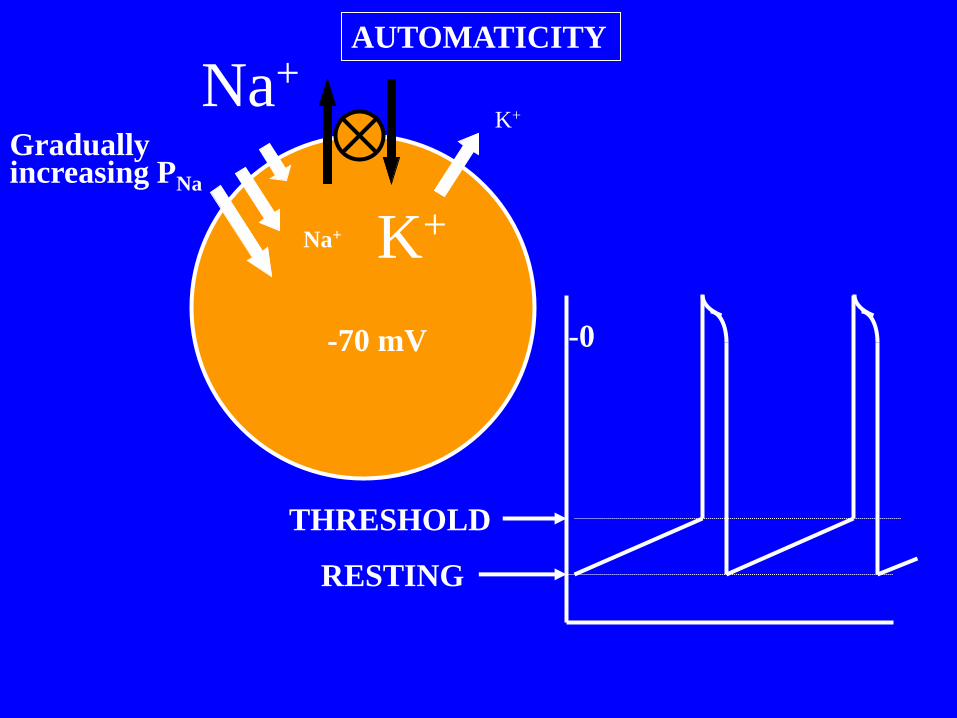
Na+
K+ Na+
K+
-70 mV
RESTING
THRESHOLD
-0
Gradually increasing PNa
AUTOMATICITY

POTENCIAL MARCAPASOS
- Canales de fuga para Na+ (If) abiertos a Vm ~ -60 mV (PNa+ >> PK+)
- Vm ~ -40 mV, despolarización rápida por Ca+ (insensible a TTX)
- Canales de K+ retrasados open to start repolarization and close Ca2+ channels, then
close themselves to allow next pacemaker potential to start.

POTENCIAL DE ACCIÓN CARDÍACO
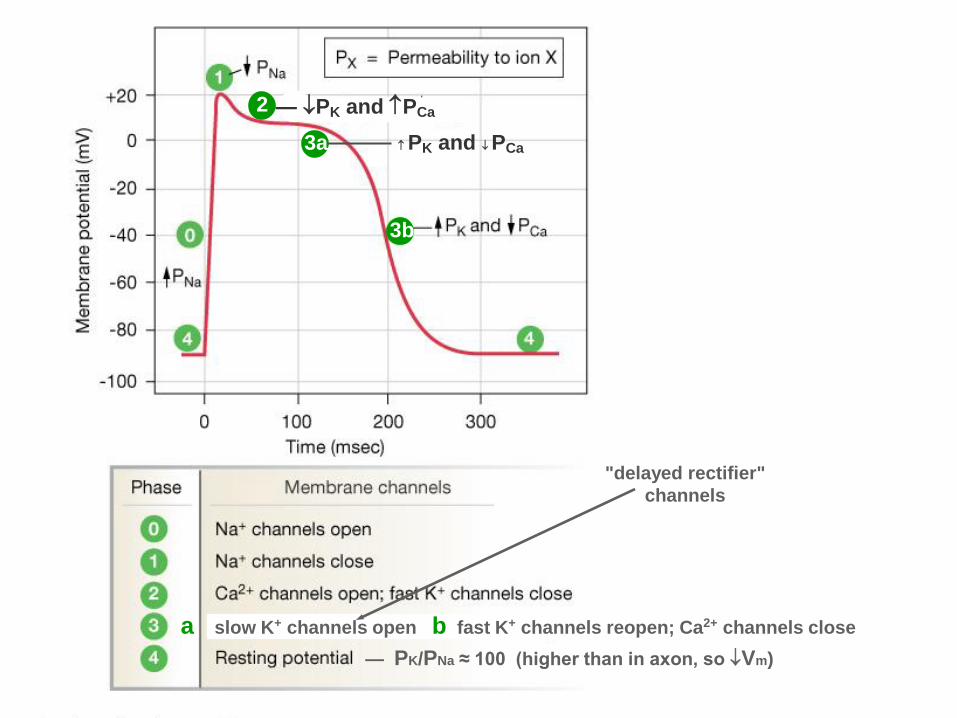
2 — PK and PCa
3a
3b
a slow K+ channels open b fast K+ channels reopen; Ca2+ channels close
PK and PCa
— PK/PNa ≈ 100 (higher than in axon, so Vm)
"delayed rectifier"
channels
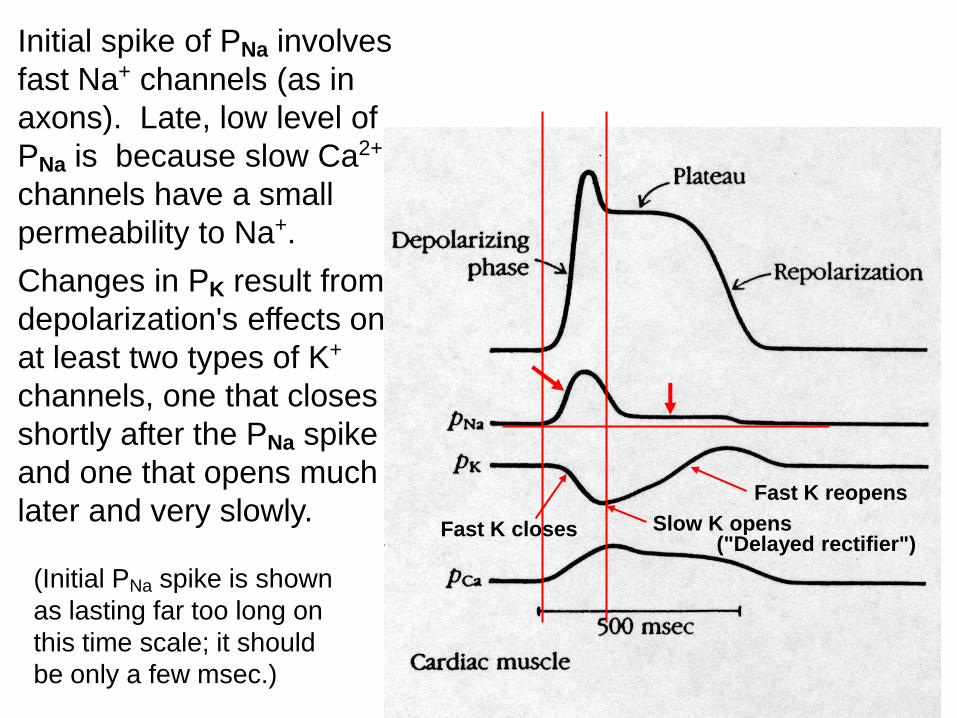
Initial spike of PNa involves
fast Na+ channels (as in
axons). Late, low level of
PNa is because slow Ca2+
channels have a small
permeability to Na+.
(Initial PNa spike is shown
as lasting far too long on
this time scale; it should
be only a few msec.)
Changes in PK result from
depolarization's effects on
at least two types of K+
channels, one that closes
shortly after the PNa spike
and one that opens much
later and very slowly. Fast K closes Slow K opens
Fast K reopens
("Delayed rectifier")
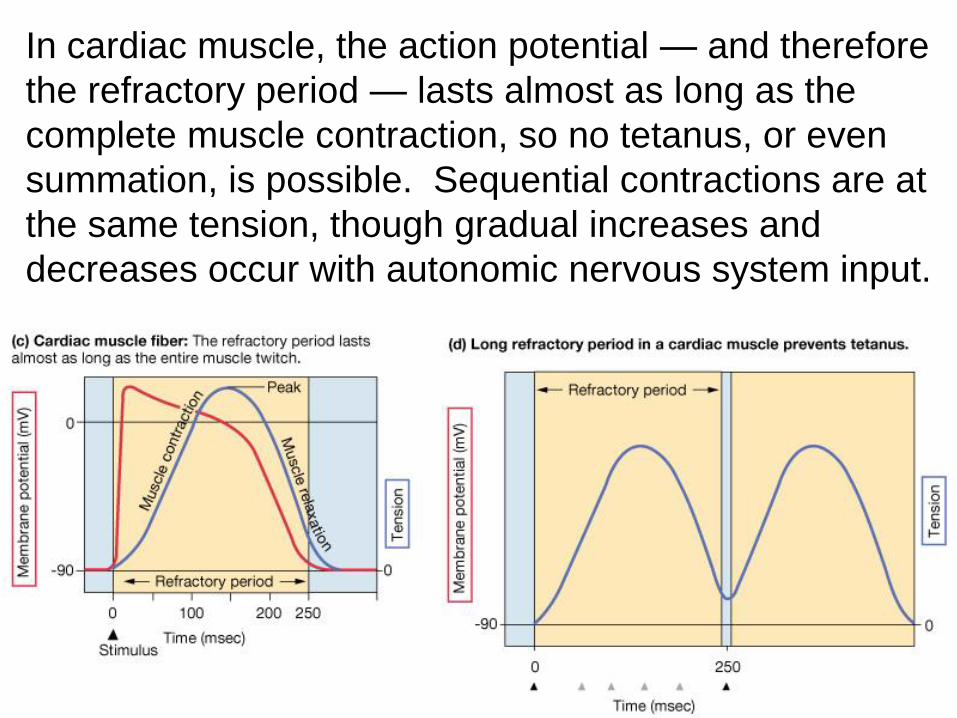
In cardiac muscle, the action potential — and therefore
the refractory period — lasts almost as long as the
complete muscle contraction, so no tetanus, or even
summation, is possible. Sequential contractions are at
the same tension, though gradual increases and
decreases occur with autonomic nervous system input.
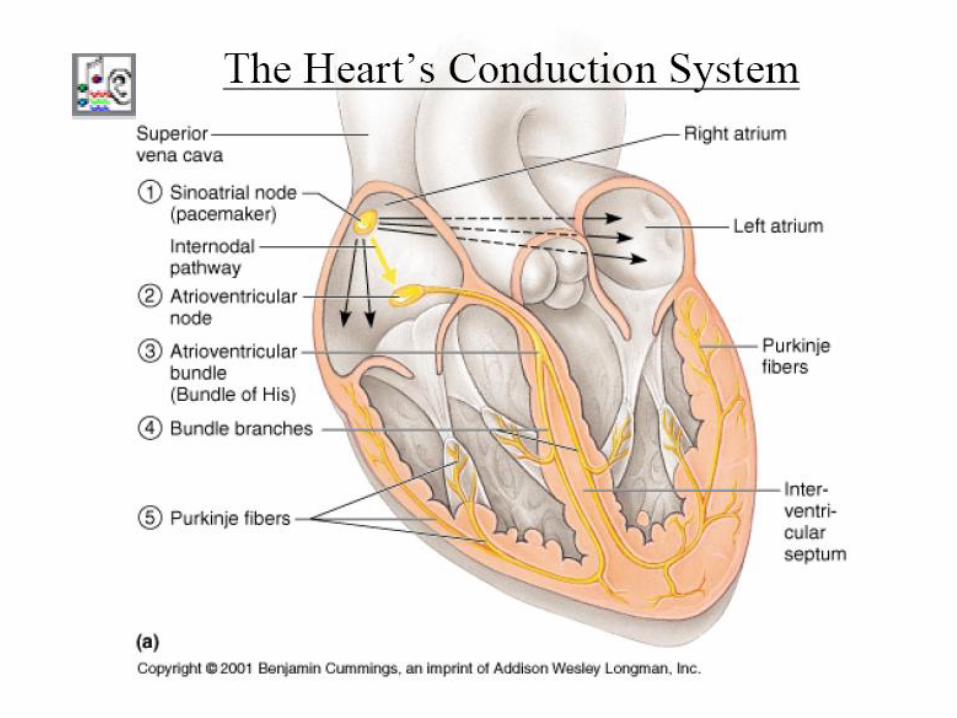
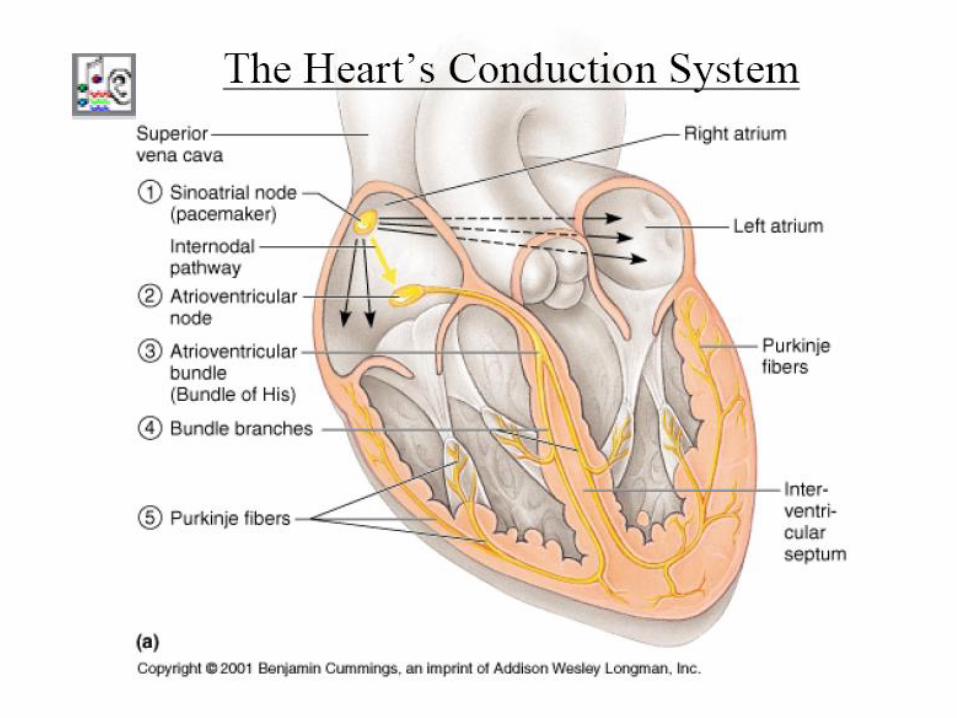
PACEMAKERS (in order of
their inherent velocity)
• Sino-atrial (SA) node (0.8 m/s)
• Atrio-ventricular (AV) node (0.05 m/s)
• Bundle of His (5 m/s)
• Bundle branches (5 m/s)
• Purkinje fibers (5 m/s)
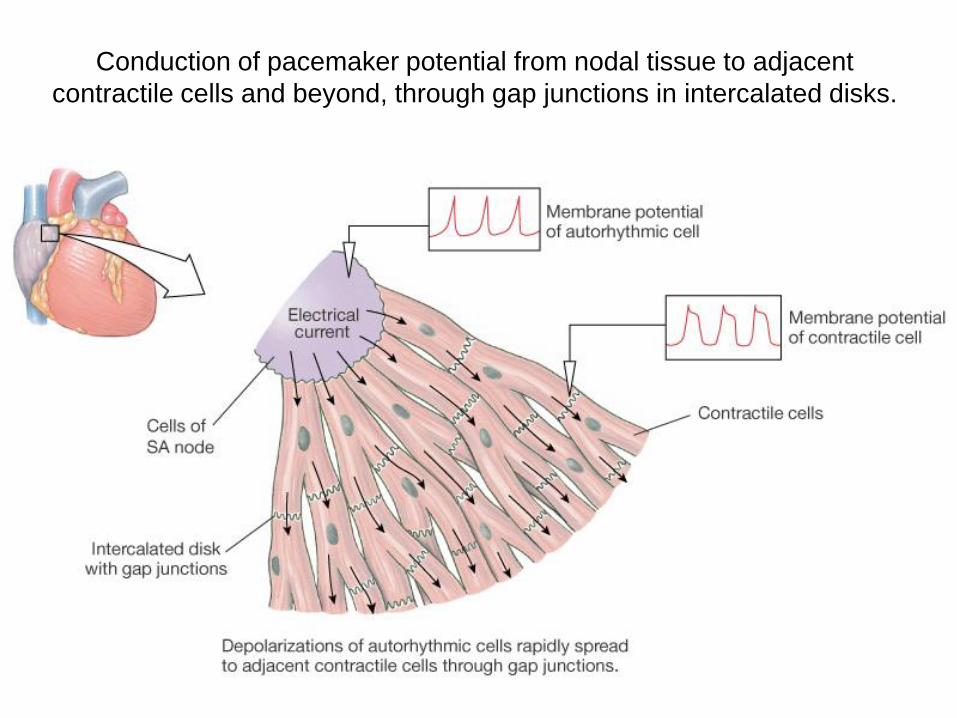
Conduction of pacemaker potential from nodal tissue to adjacent
contractile cells and beyond, through gap junctions in intercalated disks.

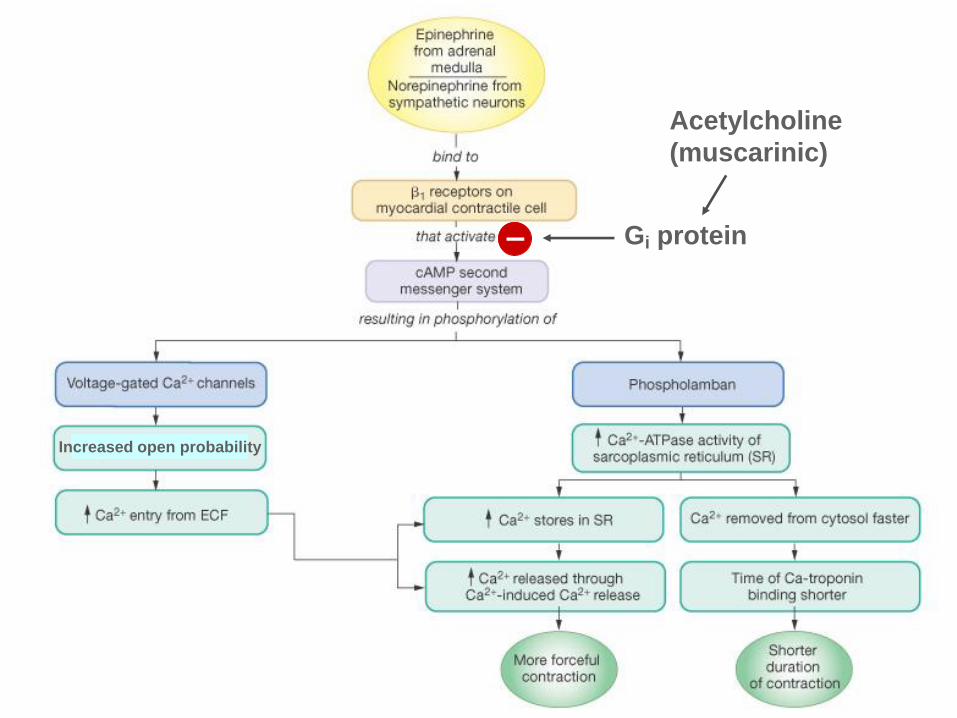
Increased open probability
Acetylcholine
(muscarinic)
Gi protein –
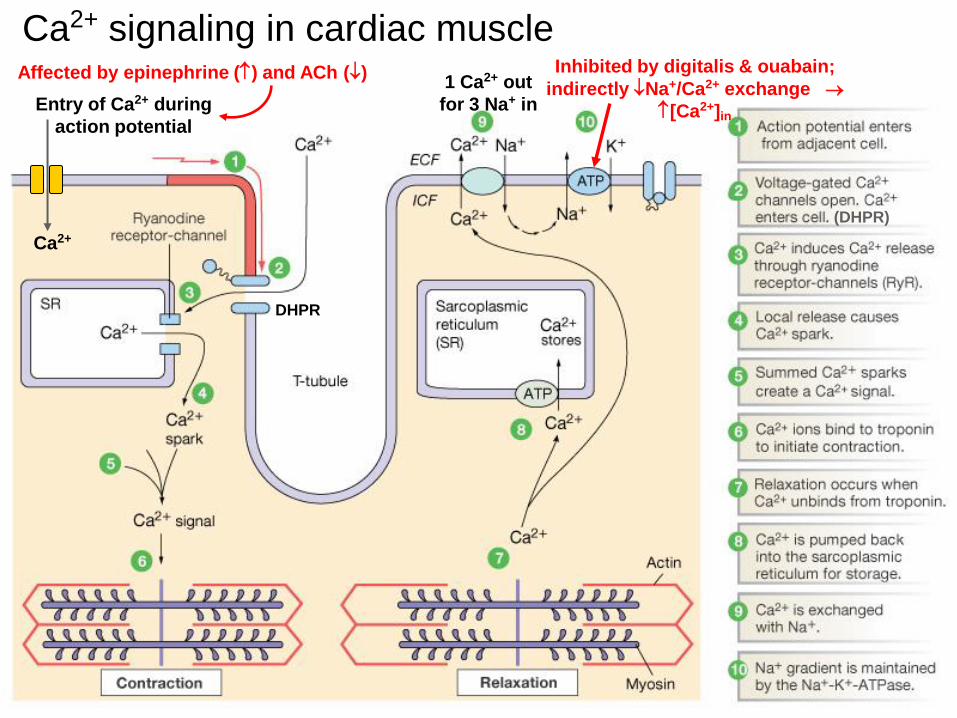
Ca2+ signaling in cardiac muscle
DHPR
(DHPR)
Ca2+
Entry of Ca2+ during
action potential
1 Ca2+ out
for 3 Na+ in
Inhibited by digitalis & ouabain;
indirectly Na+/Ca2+ exchange
[Ca2+]in
Affected by epinephrine () and ACh ()
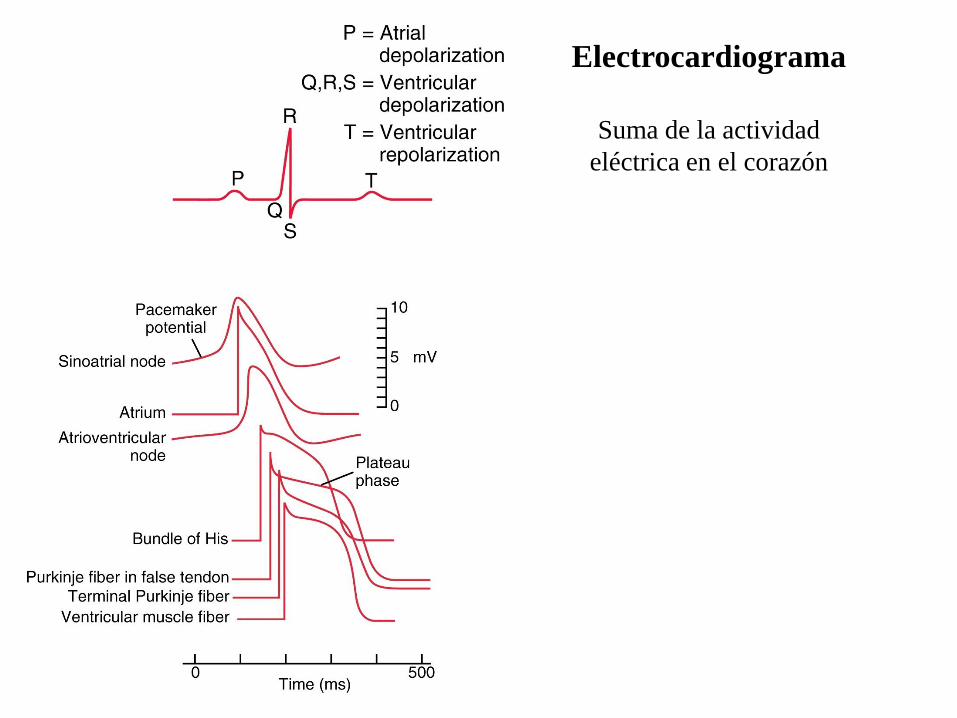
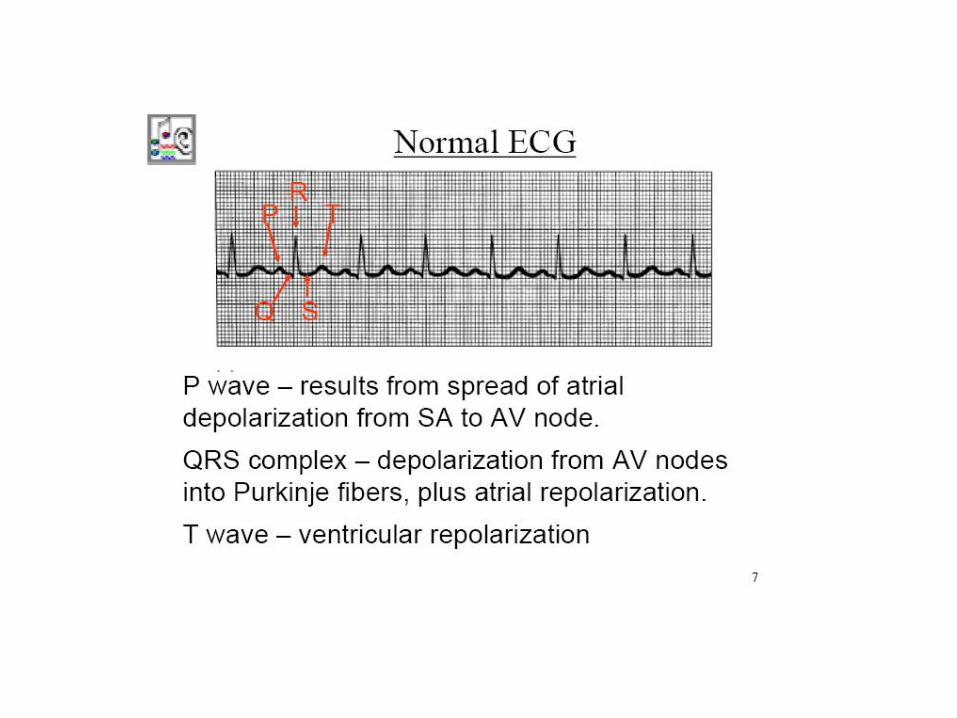
Electrocardiograma
Suma de la actividad
eléctrica en el corazón
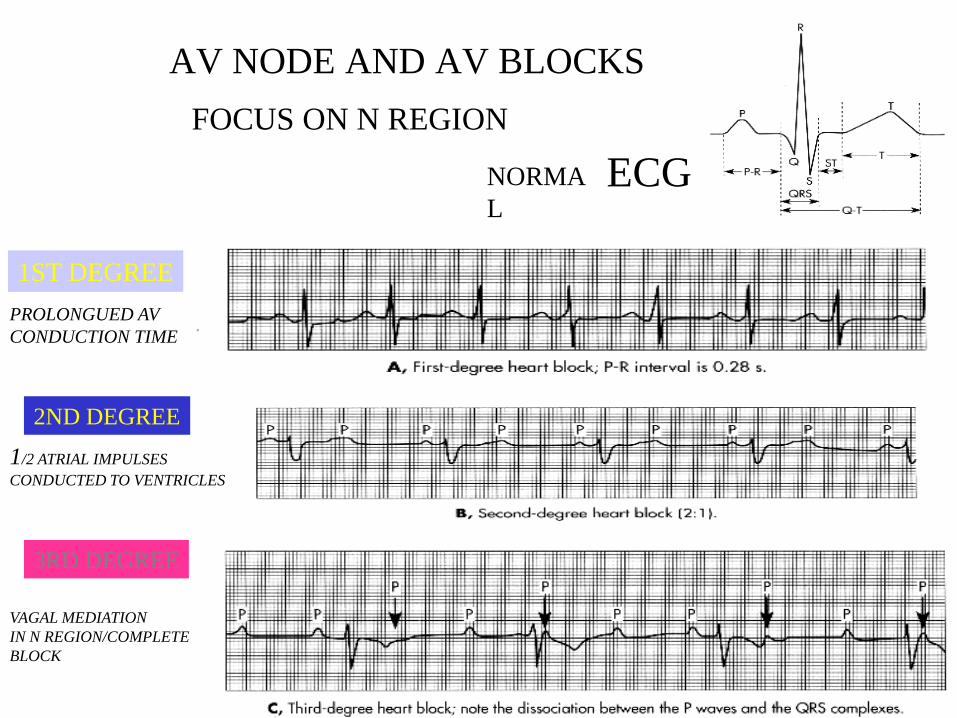
AV NODE AND AV BLOCKS
FOCUS ON N REGION
NORMA
L
ECG
1ST DEGREE
PROLONGUED AV
CONDUCTION TIME
2ND DEGREE
1/2 ATRIAL IMPULSES
CONDUCTED TO VENTRICLES
3RD DEGREE
VAGAL MEDIATION
IN N REGION/COMPLETE
BLOCK
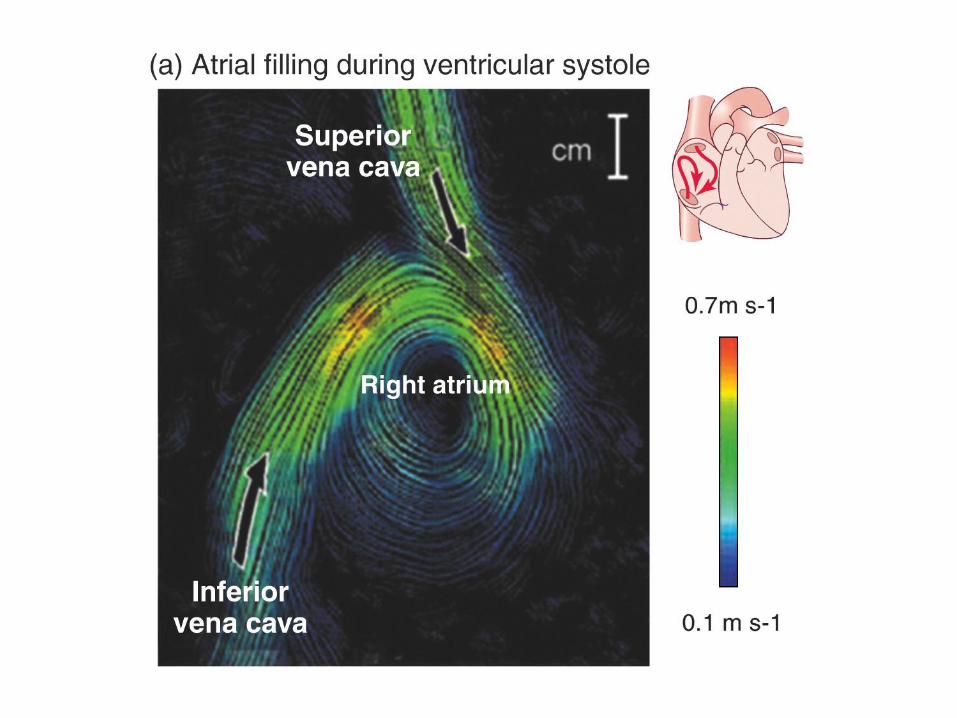
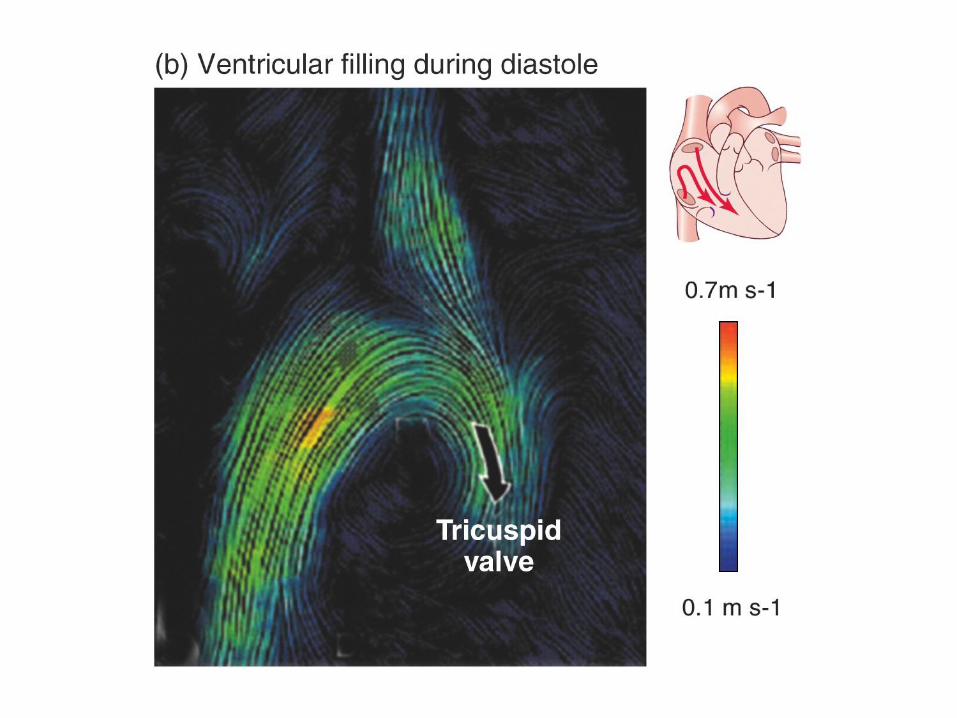
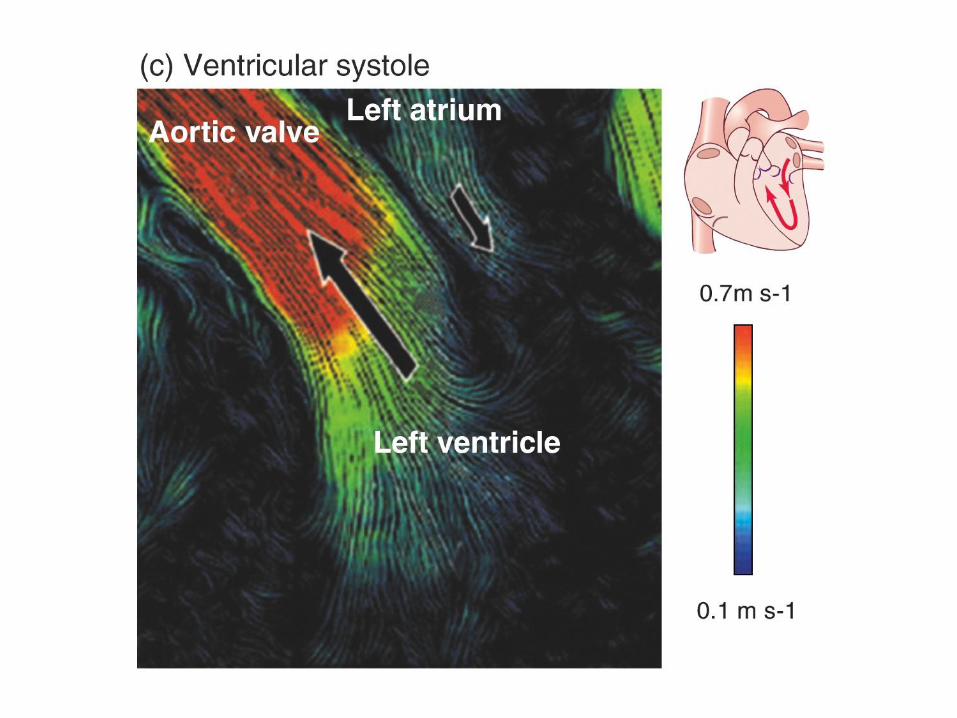
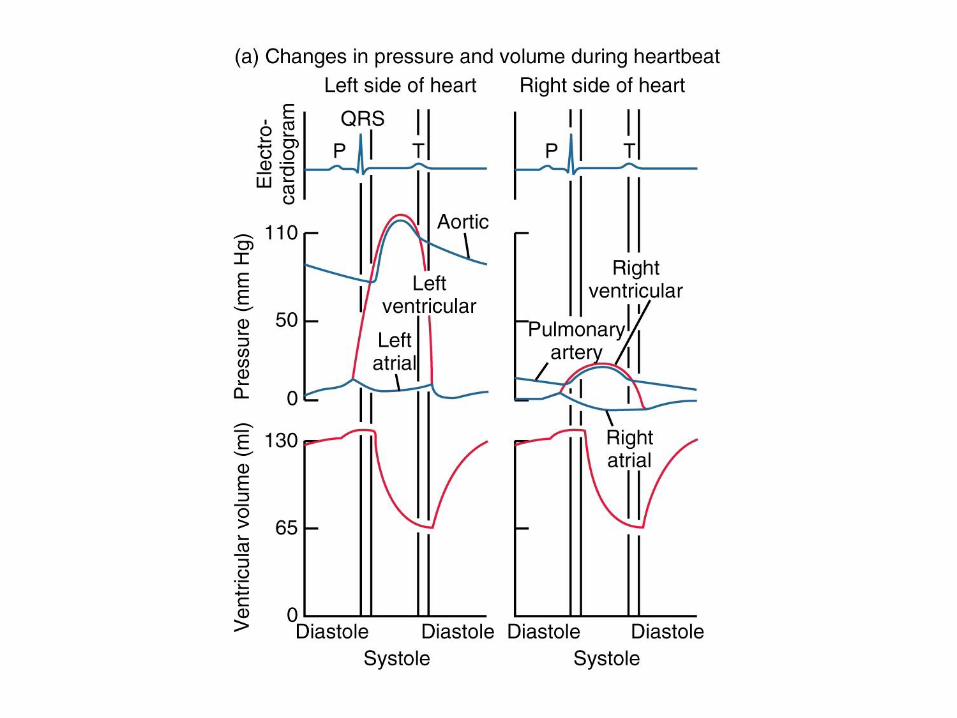
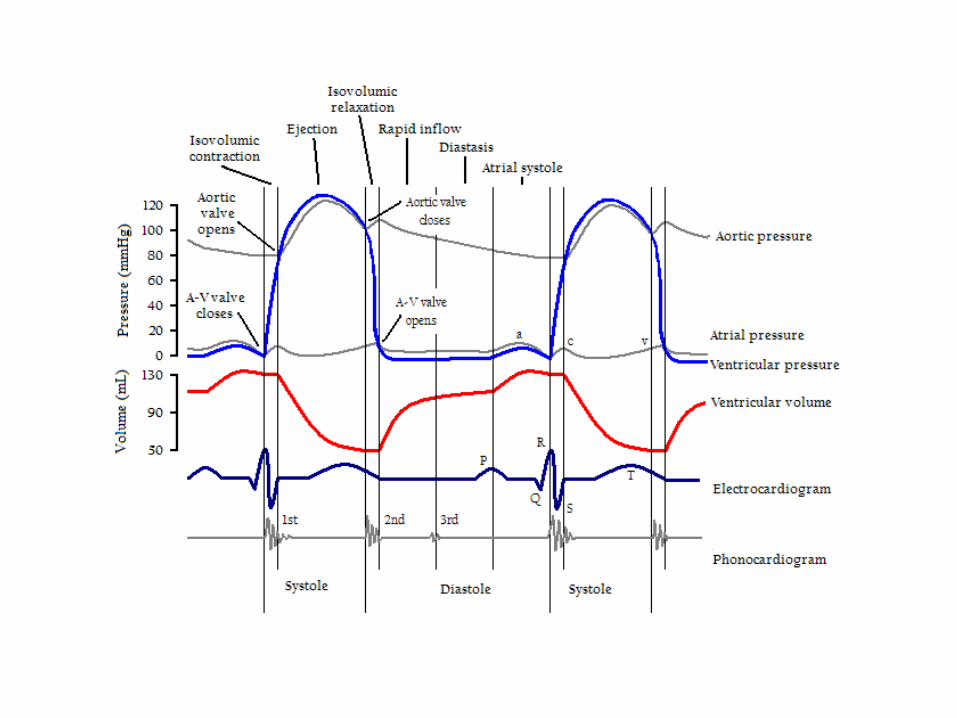
Systole — contraction of ventricles (systolic P = peak pressure
per heartbeat in major systemic arteries)
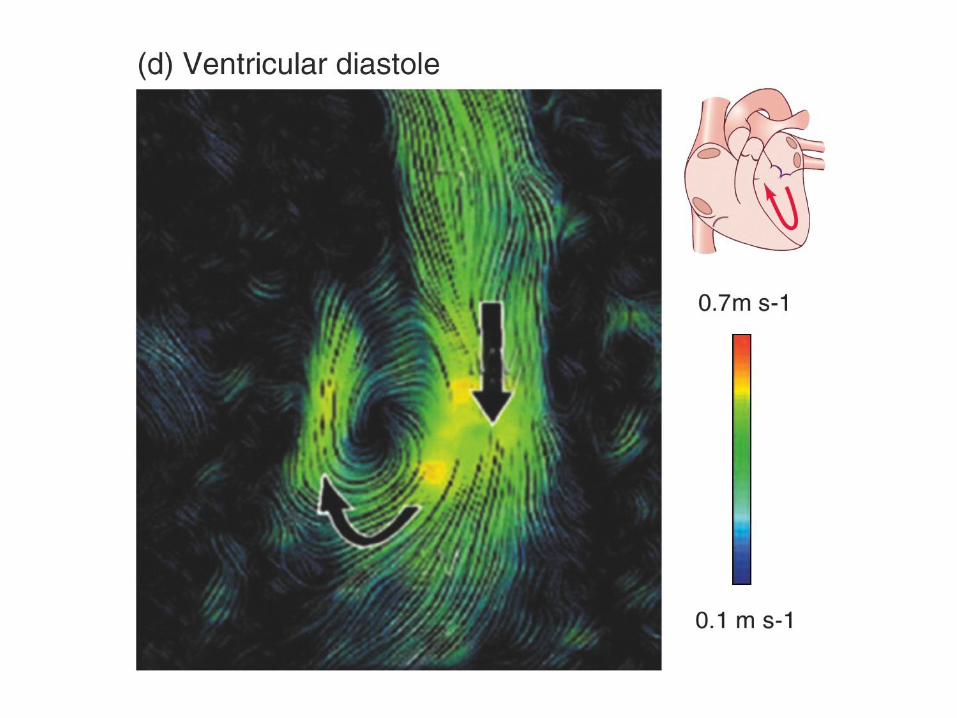
Diastole — relaxed filling of ventricles (diastolic P = lowest pressure
per heartbeat in major systemic arteries)
First heart sound (lub) — sound of atrioventricular valves closing
as ventricles start contracting
Second heart sound (dup) — sound of semilunar valves closing
as ventricles stop contracting and ventricular pressure
drops below pressure in the major arteries
Pulse pressure (PP) — systolic P - diastolic P
Mean arterial pressure (MAP) — diastolic P + 1/3 PP
Stroke volume (SV) — vol. at end of diastole - vol. at end of systole;
usually ~70 ml ( = ~130 ml - ~60 ml )
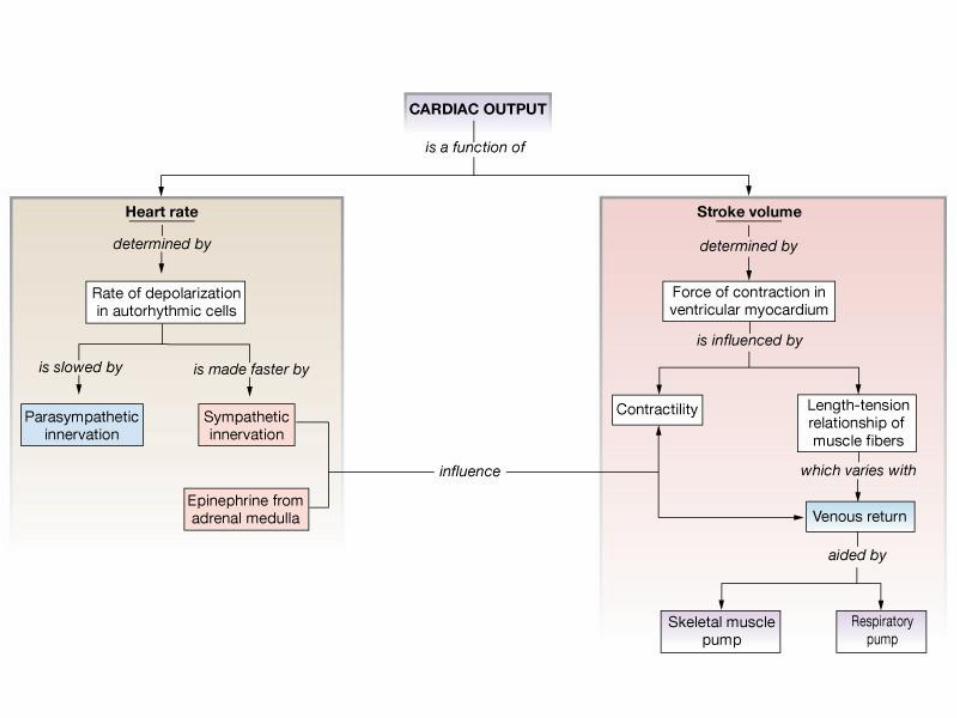
Cardiac output (CO) — heart rate (HR) x SV
CO can increase by a factor of 6 or more, initially due to
HR & SV; at higher CO, increase is mostly due to HR.
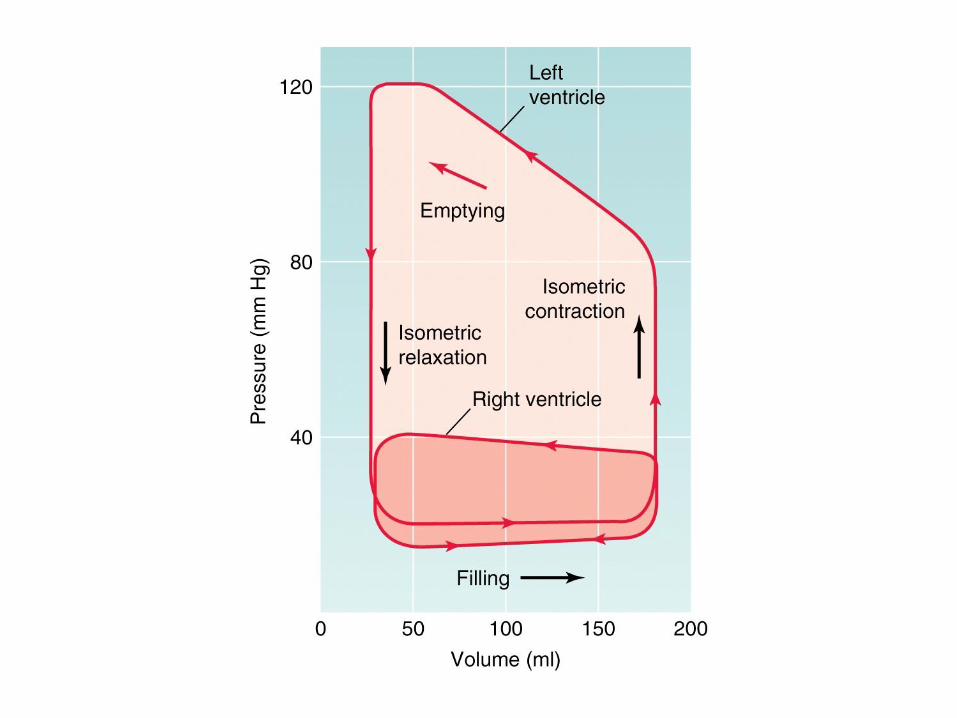
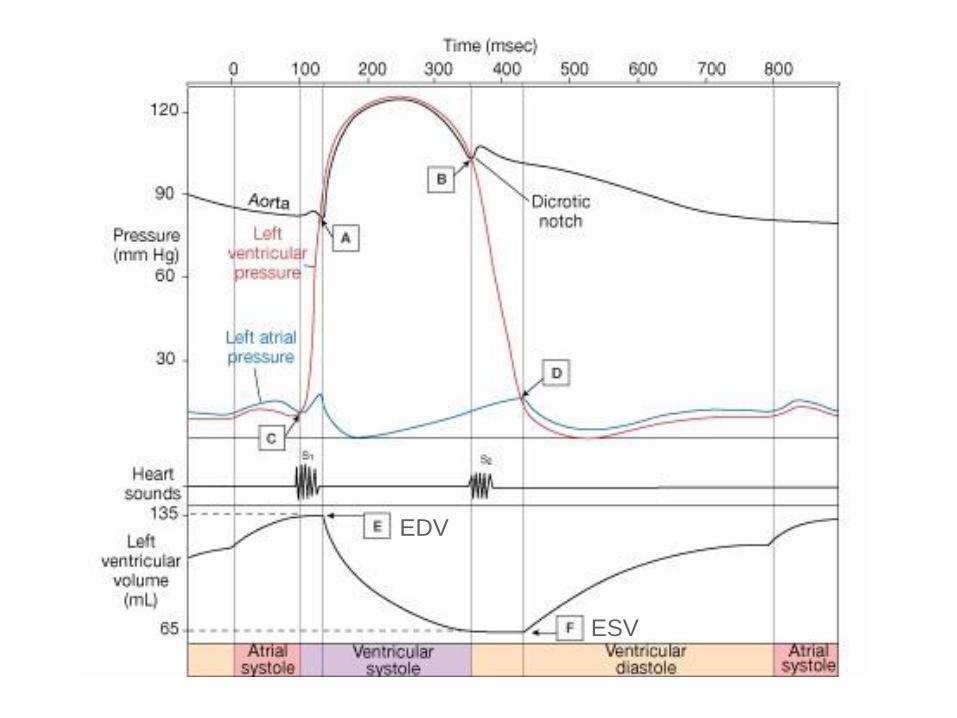
EDV
ESV
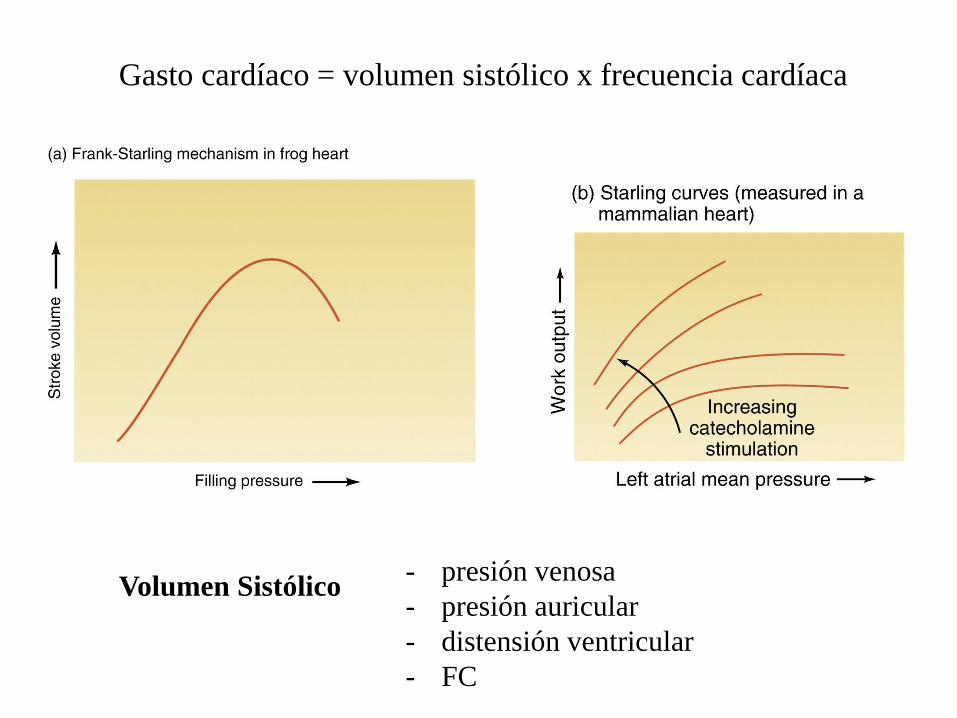
Gasto cardíaco = volumen sistólico x frecuencia cardíaca
Volumen Sistólico - presión venosa
- presión auricular
- distensión ventricular
- FC

Respuesta al ejercicio
- volumen sistólico constante
- estimulación simpática
FC, vel. llenado ventricular
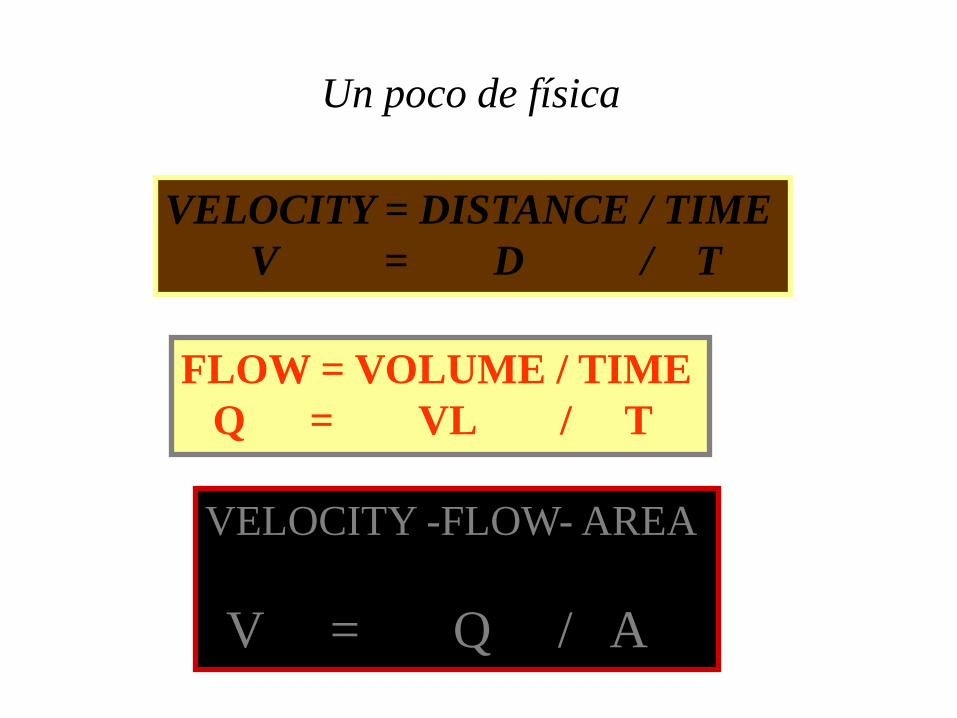
Un poco de física
VELOCITY = DISTANCE / TIME
V = D / T
FLOW = VOLUME / TIME
Q = VL / T
VELOCITY -FLOW- AREA
V = Q / A
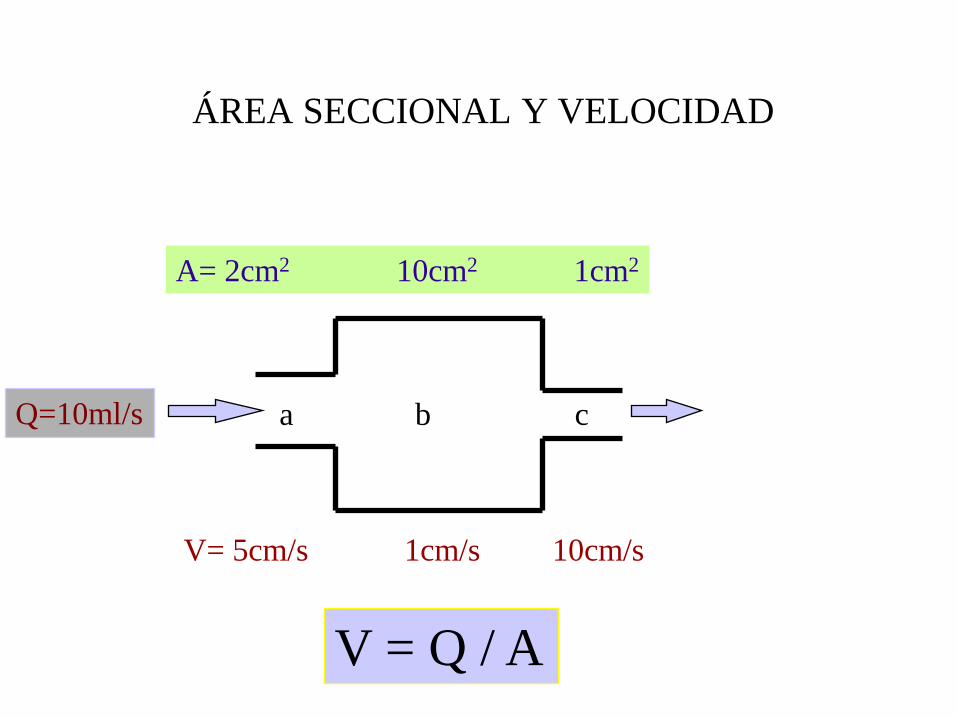
ÁREA SECCIONAL Y VELOCIDAD
Q=10ml/s
A= 2cm2 10cm2 1cm2
V= 5cm/s 1cm/s 10cm/s
V = Q / A
a b c
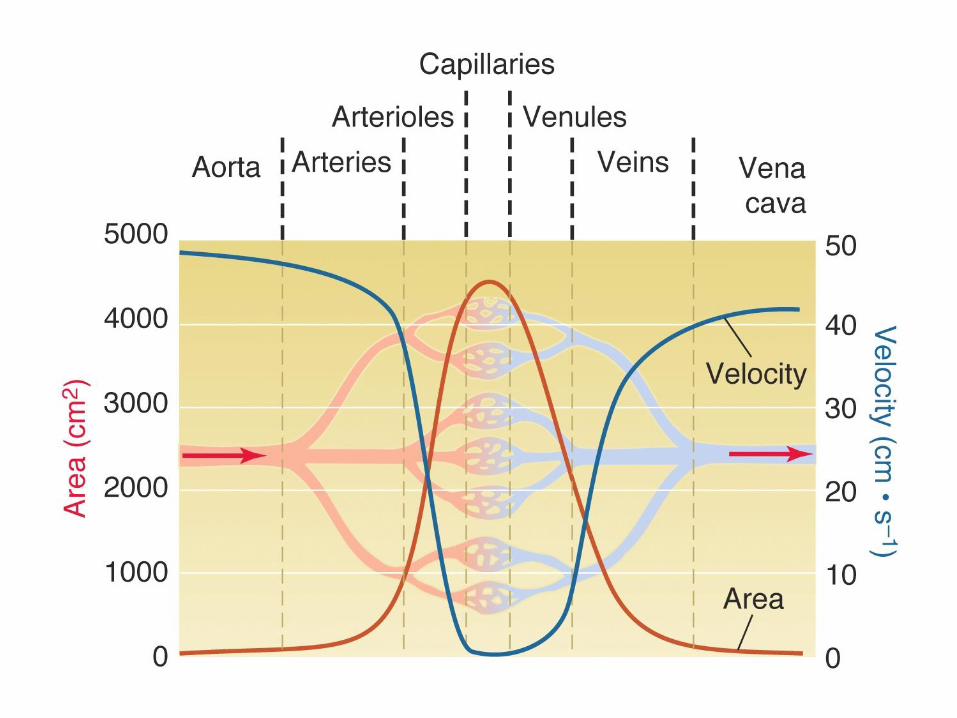
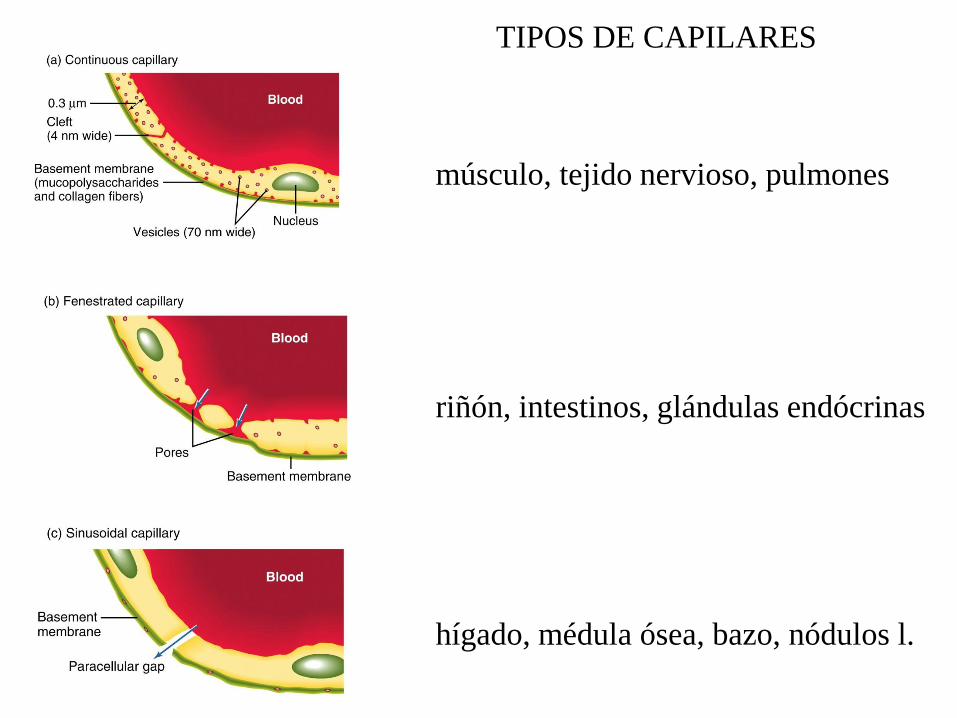
TIPOS DE CAPILARES
músculo, tejido nervioso, pulmones
riñón, intestinos, glándulas endócrinas
hígado, médula ósea, bazo, nódulos l.

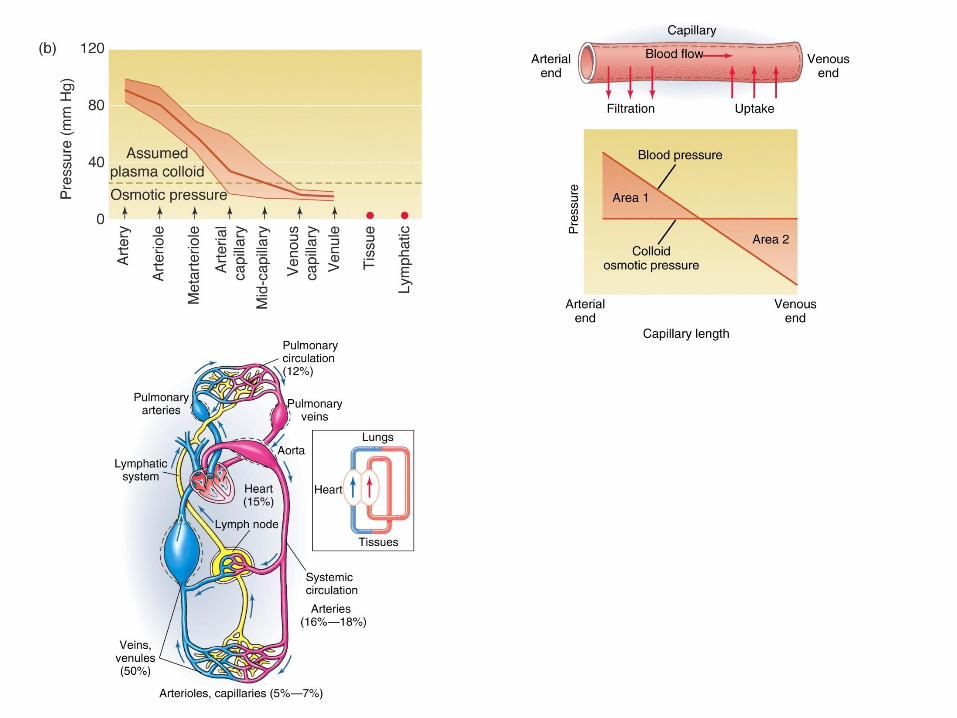
CAPILLARIES
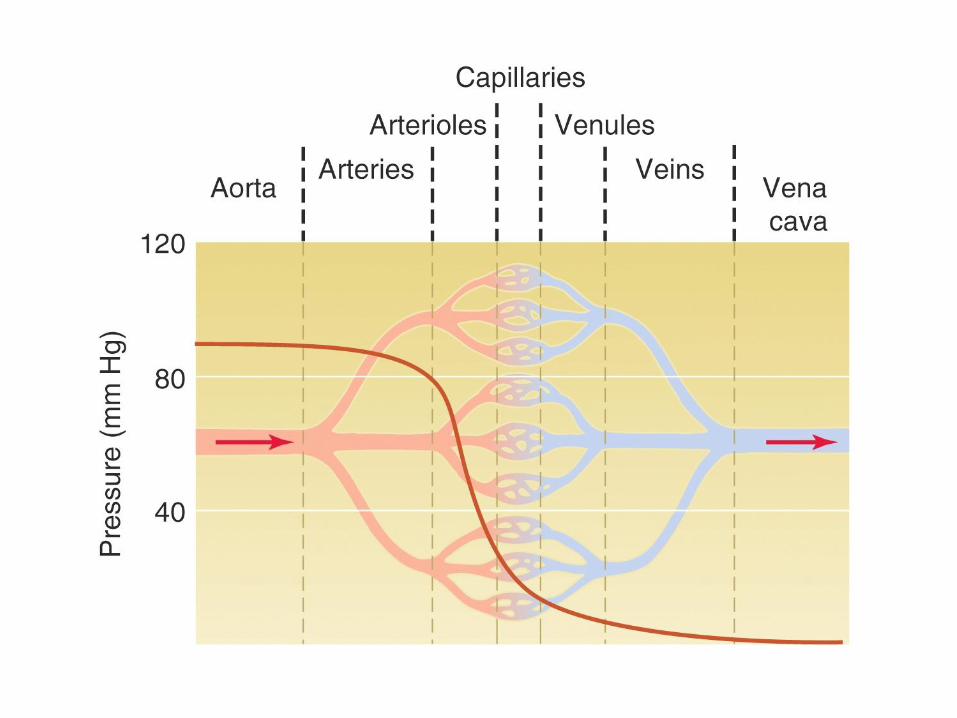
• Pressure inside is 35 to 15 mmHg
• 5% of the blood is in capillaries
• exchange of gases, nutrients, and wastes
• flow is slow and continuous
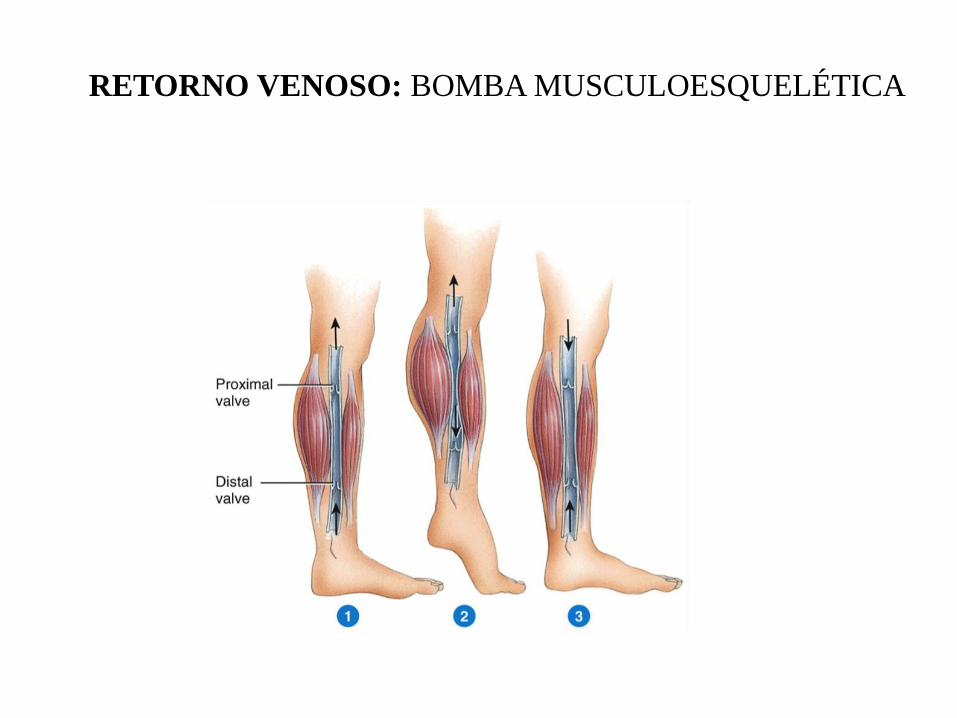
RETORNO VENOSO: BOMBA MUSCULOESQUELÉTICA
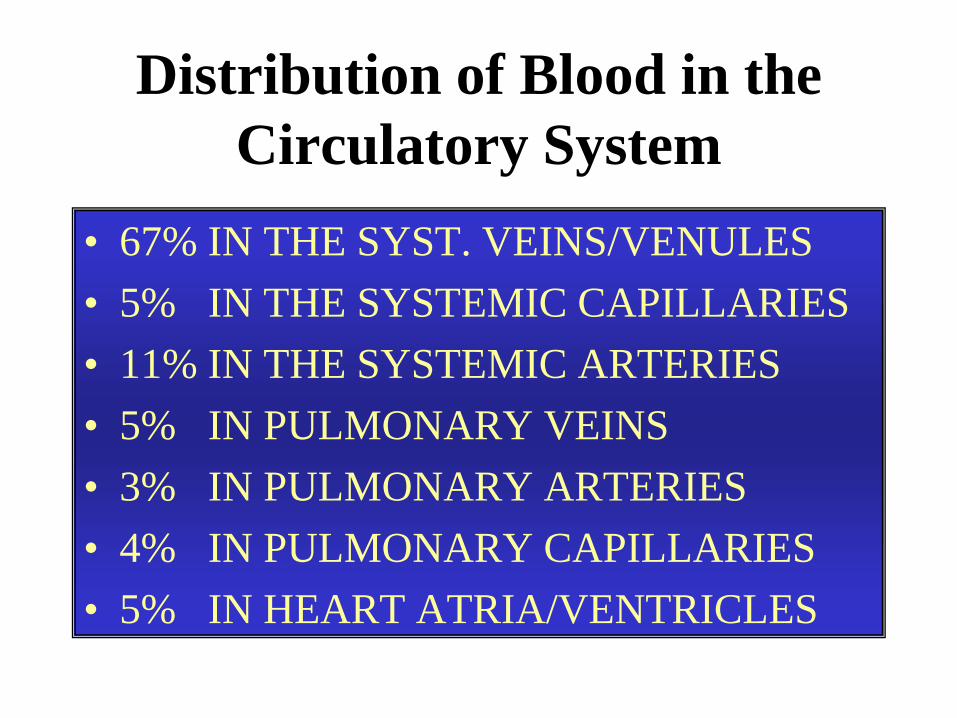
Distribution of Blood in the
Circulatory System
• 67% IN THE SYST. VEINS/VENULES
• 5% IN THE SYSTEMIC CAPILLARIES
• 11% IN THE SYSTEMIC ARTERIES
• 5% IN PULMONARY VEINS
• 3% IN PULMONARY ARTERIES
• 4% IN PULMONARY CAPILLARIES
• 5% IN HEART ATRIA/VENTRICLES

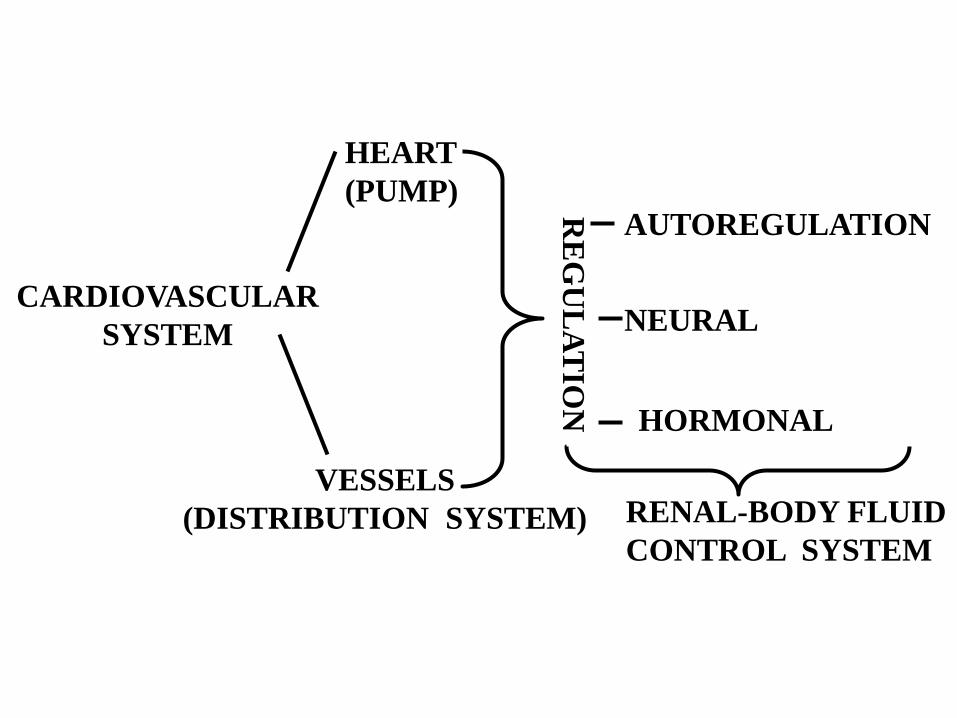
CARDIOVASCULAR
SYSTEM
HEART
(PUMP)
VESSELS
(DISTRIBUTION SYSTEM)
RE
GU
LA
TIO
N
AUTOREGULATION
NEURAL
HORMONAL
RENAL-BODY FLUID
CONTROL SYSTEM
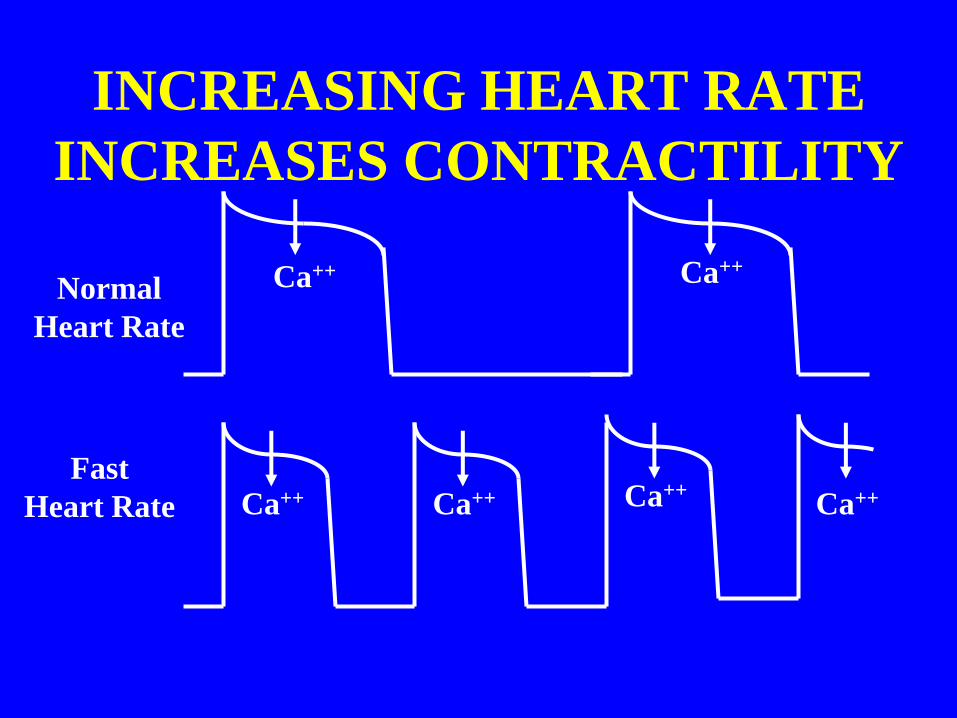
INCREASING HEART RATE
INCREASES CONTRACTILITY
Normal
Heart Rate
Ca++ Ca++
Fast
Heart Rate Ca++ Ca++ Ca++ Ca++
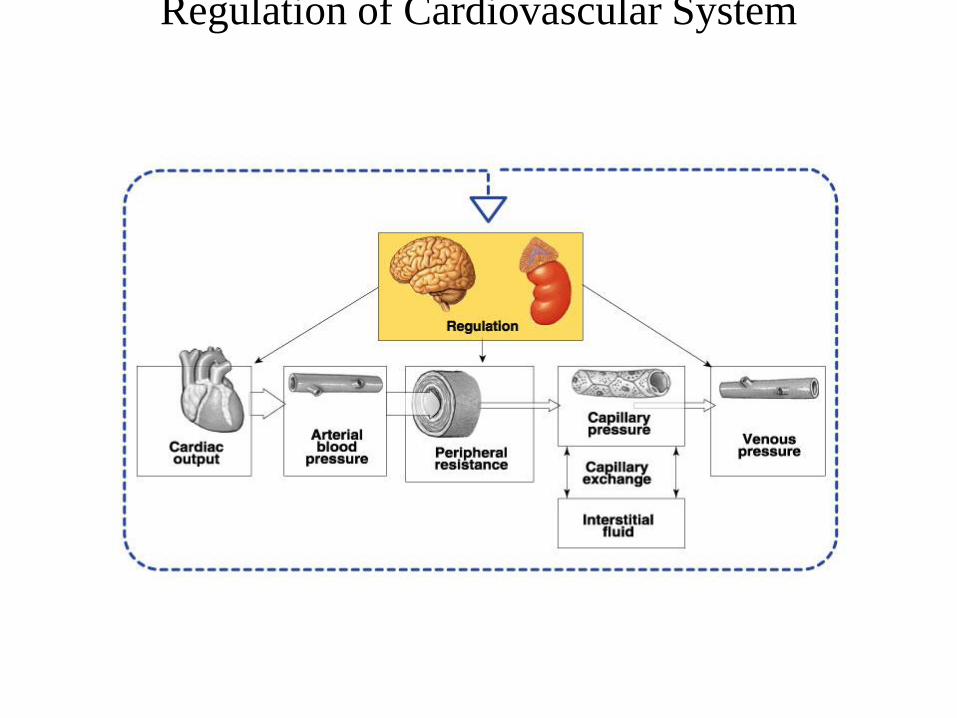
Regulation of Cardiovascular System
Overview-
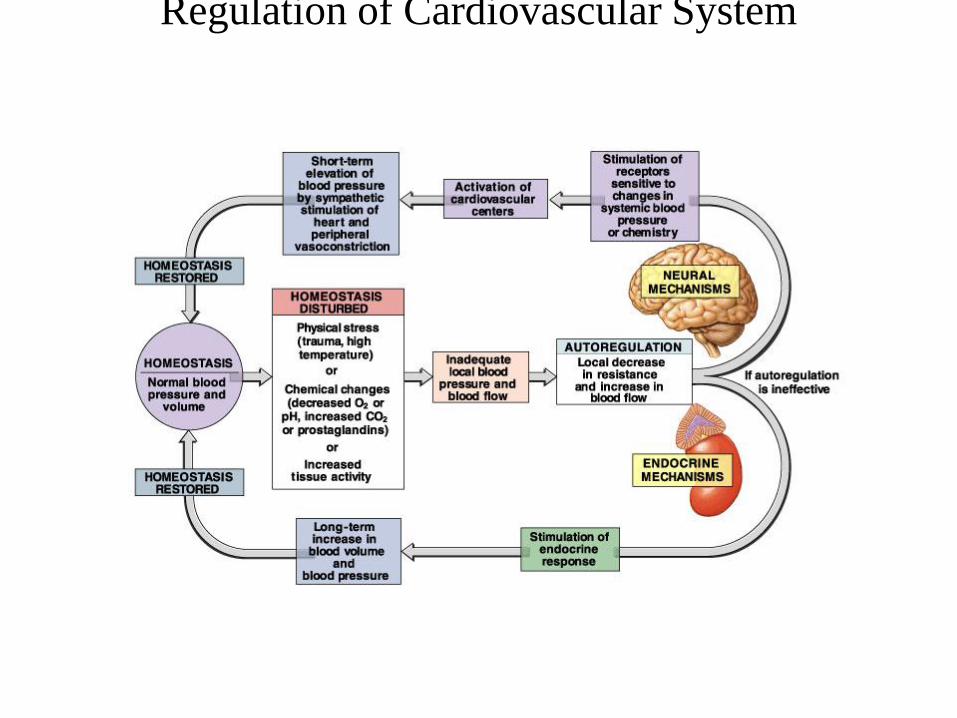
Regulation of Cardiovascular System
Overview-
HORMONAL REGULATION
• Epinephrine & Norepinephrine
– From the adrenal medulla
• Renin-angiotensin-aldosterone
– Renin from the kidney
– Angiotensin, a plasma protein
– Aldosterone from the adrenal cortex
• Vasopressin (Antidiuretic Hormone-ADH)
– ADH from the posterior pituitary
HYPERTENSION (140/90 mmHg)
Secondary Hypertension (10%) [e.g., Pheochromocytoma]
Essential Hypertension (90%) - Normal cardiac output - Cardiac hypertrophy [left ventricle] - “Resetting” of the baroreceptors - Thickening of vascular walls
ARTERIAL PRESSURE-URINARY OUTPUT THEORY Hypertension causes thickening of vascular walls NEUROGENIC THEORY Thickening of vascular walls causes hypertension
TREATMENT: Reduce stress Sympathetic blockers Low sodium diet Diuretics
RESPONSE TO HEMORRHAGE
• Sympathetic tone via baroreceptor reflex
– Heart rate and contractility
– Venoconstriction ( MCP)
– Vasoconstriction ( arterial BP & direct blood to
vital organs)
• Restore Blood Volume
– Capillary fluid shift ( BP favors reabsorption)
– Urinary output ( Arterial BP, ADH, Renin-
Angiotensin-Aldosterone)
• Restore plasma proteins & hematocrit
CARDIAC FAILURE CAUSES: Impairment of electrical activity Muscle damage Valvular defects Cardiomyopathies Result of drugs or toxins
PROBLEM: Maintaining circulation with a weak pump
( Cardiac output & cardiac reserve; RAP)
SOLUTIONS: Sympathetic tone via baroreceptor reflex - Heart rate and contractility
-Venoconstriction ( MCP) -Vasoconstriction ( Arterial BP) Fluid retention ( MCP) -Capillary fluid shift -ADH -Renin-angiotensin-aldosterone
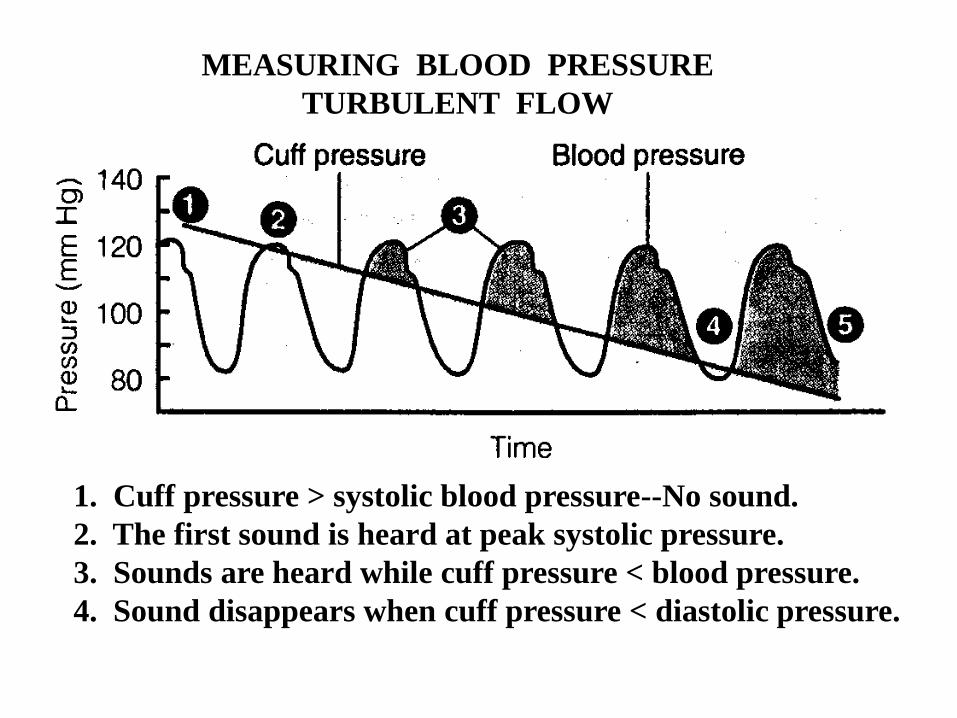
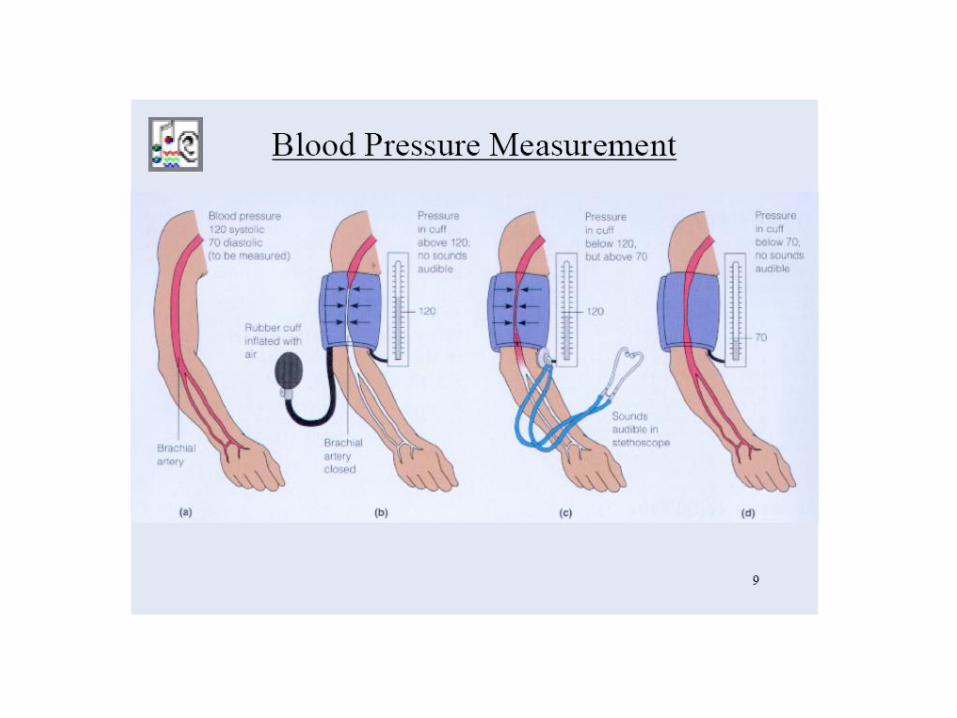
MEASURING BLOOD PRESSURE
TURBULENT FLOW
1. Cuff pressure > systolic blood pressure--No sound.
2. The first sound is heard at peak systolic pressure.
3. Sounds are heard while cuff pressure < blood pressure.
4. Sound disappears when cuff pressure < diastolic pressure.
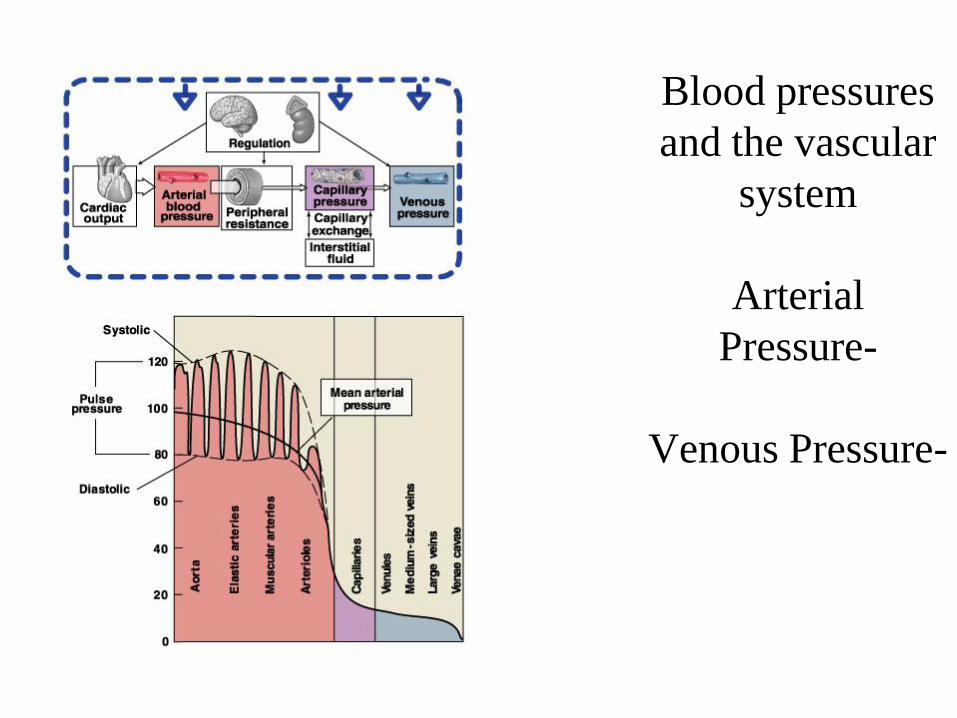
Blood pressures
and the vascular
system
Arterial
Pressure-
Venous Pressure-
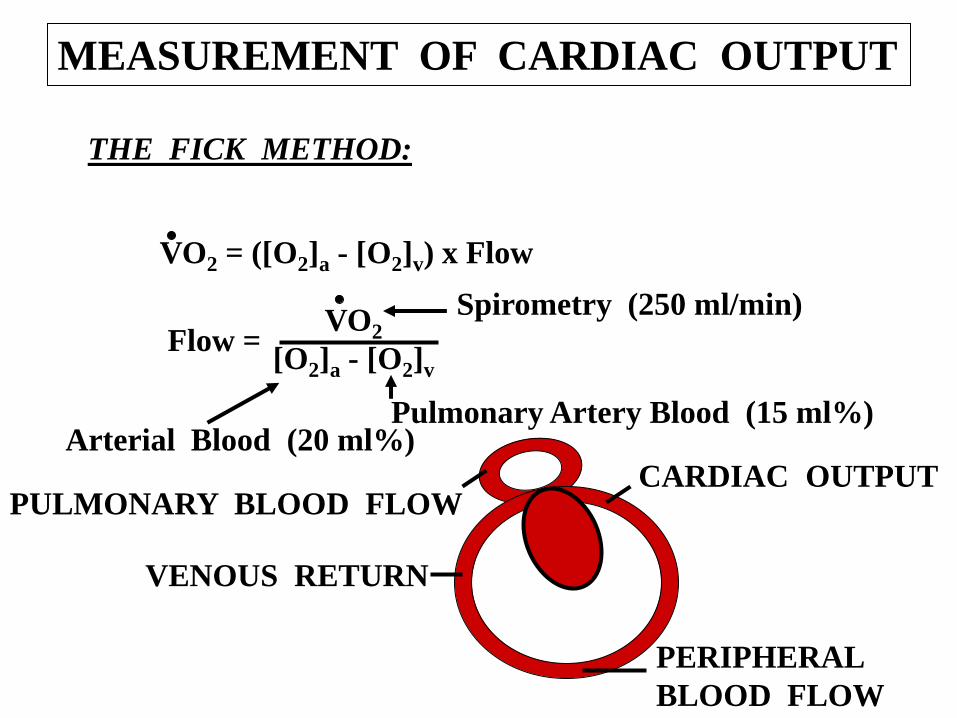
MEASUREMENT OF CARDIAC OUTPUT
THE FICK METHOD:
VO2 = ([O2]a - [O2]v) x Flow
Flow = VO2
[O2]a - [O2]v
Spirometry (250 ml/min)
Arterial Blood (20 ml%) Pulmonary Artery Blood (15 ml%)
CARDIAC OUTPUT
PERIPHERAL
BLOOD FLOW
VENOUS RETURN
PULMONARY BLOOD FLOW
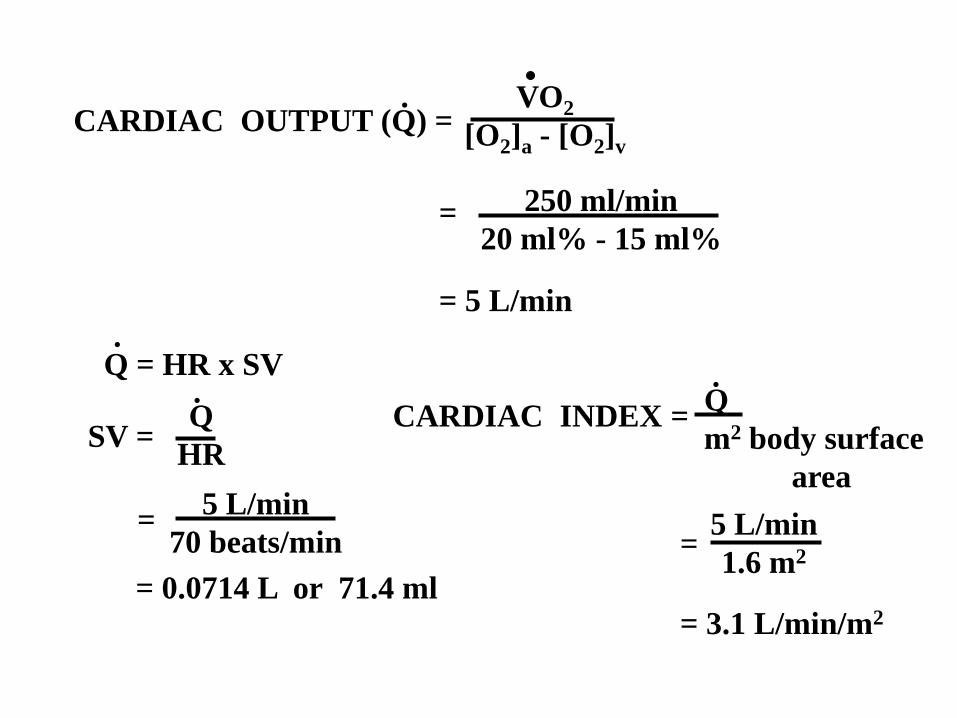
CARDIAC OUTPUT (Q) = VO2
[O2]a - [O2]v
250 ml/min
20 ml% - 15 ml% =
= 5 L/min
.
Q = HR x SV .
SV = Q
HR
.
= 5 L/min
70 beats/min
= 0.0714 L or 71.4 ml
CARDIAC INDEX = Q
m2 body surface
area
.
5 L/min
1.6 m2 =
= 3.1 L/min/m2
Top Related