diposit.ub.edudiposit.ub.edu/dspace/bitstream/2445/103980/1/DVR_TESIS.pdf · Caracterización...
141
Caracterización clínica, bioquímica y de neuroimagen de la enfermedad de Parkinson asociada a mutaciones del gen LRRK2 y de su fase prodrómica Dolores Vilas Rolán ADVERTIMENT. La consulta d’aquesta tesi queda condicionada a l’acceptació de les següents condicions d'ús: La difusió d’aquesta tesi per mitjà del servei TDX ( www.tdx.cat) i a través del Dipòsit Digital de la UB (diposit.ub.edu) ha estat autoritzada pels titulars dels drets de propietat intel·lectual únicament per a usos privats emmarcats en activitats d’investigació i docència. No s’autoritza la seva reproducció amb finalitats de lucre ni la seva difusió i posada a disposició des d’un lloc aliè al servei TDX ni al Dipòsit Digital de la UB. No s’autoritza la presentació del seu contingut en una finestra o marc aliè a TDX o al Dipòsit Digital de la UB (framing). Aquesta reserva de drets afecta tant al resum de presentació de la tesi com als seus continguts. En la utilització o cita de parts de la tesi és obligat indicar el nom de la persona autora. ADVERTENCIA. La consulta de esta tesis queda condicionada a la aceptación de las siguientes condiciones de uso: La difusión de esta tesis por medio del servicio TDR (www.tdx.cat) y a través del Repositorio Digital de la UB (diposit.ub.edu) ha sido autorizada por los titulares de los derechos de propiedad intelectual únicamente para usos privados enmarcados en actividades de investigación y docencia. No se autoriza su reproducción con finalidades de lucro ni su difusión y puesta a disposición desde un sitio ajeno al servicio TDR o al Repositorio Digital de la UB. No se autoriza la presentación de su contenido en una ventana o marco ajeno a TDR o al Repositorio Digital de la UB (framing). Esta reserva de derechos afecta tanto al resumen de presentación de la tesis como a sus contenidos. En la utilización o cita de partes de la tesis es obligado indicar el nombre de la persona autora. WARNING. On having consulted this thesis you’re accepting the following use conditions: Spreading this thesis by the TDX (www.tdx.cat) service and by the UB Digital Repository (diposit.ub.edu) has been authorized by the titular of the intellectual property rights only for private uses placed in investigation and teaching activities. Reproduction with lucrative aims is not authorized nor its spreading and availability from a site foreign to the TDX service or to the UB Digital Repository. Introducing its content in a window or frame foreign to the TDX service or to the UB Digital Repository is not authorized (framing). Those rights affect to the presentation summary of the thesis as well as to its contents. In the using or citation of parts of the thesis it’s obliged to indicate the name of the author.
Transcript of diposit.ub.edudiposit.ub.edu/dspace/bitstream/2445/103980/1/DVR_TESIS.pdf · Caracterización...

Caracterización clínica, bioquímica y de neuroimagen de la enfermedad de Parkinson asociada a mutaciones
del gen LRRK2 y de su fase prodrómica
Dolores Vilas Rolán
ADVERTIMENT. La consulta d’aquesta tesi queda condicionada a l’acceptació de les següents condicions d'ús: La difusió d’aquesta tesi per mitjà del servei TDX (www.tdx.cat) i a través del Dipòsit Digital de la UB (diposit.ub.edu) ha estat autoritzada pels titulars dels drets de propietat intel·lectual únicament per a usos privats emmarcats en activitats d’investigació i docència. No s’autoritza la seva reproducció amb finalitats de lucre ni la seva difusió i posada a disposició des d’un lloc aliè al servei TDX ni al Dipòsit Digital de la UB. No s’autoritza la presentació del seu contingut en una finestra o marc aliè a TDX o al Dipòsit Digital de la UB (framing). Aquesta reserva de drets afecta tant al resum de presentació de la tesi com als seus continguts. En la utilització o cita de parts de la tesi és obligat indicar el nom de la persona autora. ADVERTENCIA. La consulta de esta tesis queda condicionada a la aceptación de las siguientes condiciones de uso: La difusión de esta tesis por medio del servicio TDR (www.tdx.cat) y a través del Repositorio Digital de la UB (diposit.ub.edu) ha sido autorizada por los titulares de los derechos de propiedad intelectual únicamente para usos privados enmarcados en actividades de investigación y docencia. No se autoriza su reproducción con finalidades de lucro ni su difusión y puesta a disposición desde un sitio ajeno al servicio TDR o al Repositorio Digital de la UB. No se autoriza la presentación de su contenido en una ventana o marco ajeno a TDR o al Repositorio Digital de la UB (framing). Esta reserva de derechos afecta tanto al resumen de presentación de la tesis como a sus contenidos. En la utilización o cita de partes de la tesis es obligado indicar el nombre de la persona autora. WARNING. On having consulted this thesis you’re accepting the following use conditions: Spreading this thesis by the TDX (www.tdx.cat) service and by the UB Digital Repository (diposit.ub.edu) has been authorized by the titular of the intellectual property rights only for private uses placed in investigation and teaching activities. Reproduction with lucrative aims is not authorized nor its spreading and availability from a site foreign to the TDX service or to the UB Digital Repository. Introducing its content in a window or frame foreign to the TDX service or to the UB Digital Repository is not authorized (framing). Those rights affect to the presentation summary of the thesis as well as to its contents. In the using or citation of parts of the thesis it’s obliged to indicate the name of the author.

Dolores Vilas Rolán
Caracterización clínica, bioquímica y de neuroimagen de la enfermedad de Parkinson asociada a mutaciones del gen LRRK2 y de su fase prodrómica
2015
TESIS DOCTORAL
TESI
S D
OC
TOR
AL
- D
olor
es V
ilas
Rolá
n20
15


Caracterización clínica, bioquímica y de neuroimagen de la enfermedad de Parkinson asociada a mutaciones del
gen LRRK2 y de su fase prodrómica
Tesis presentada por:
Dolores Vilas Rolánpara obtener el título de doctora por la Universitat de Barcelona
Dirigida por:
Prof. Eduard Tolosa i Sarró
Programa Doctorado MedicinaUniversitat de Barcelona
2015
TESIS DOCTORAL


INFORME DEL DIRECTOR DE LA TESIS
Barcelona, a 2 de Noviembre de 2015
El Dr. Eduard Tolosa i Sarró, Consultor Senior del Servicio de Neurología del Hospital Clínic de
Barcelona y Catedrático de Neurología de la Facultad de Medicina de la UB.
CERTIFICA:
Que la tesis doctoral “Caracterización clínica, bioquímica y de neuroimagen de la enfermedad de
Parkinson asociada a mutaciones del gen LRRK2 y de su fase prodrómica”, presentada por Dolores
Vilas Rolán para optar al grado de Doctor por la Universidad de Barcelona se ha realizado bajo mi
dirección y cumple todos los requisitos necesarios para ser defendida ante el Tribunal de evalua-
ción correspondiente.
Firmado,
Dr. Eduard Tolosa Sarró
Consultor Senior, Unidad de Parkinson y Trastornos del Movimiento
Servicio de Neurología
Hospital Clínic de Barcelona


Aunque esta tesis lleva mi nombre, es fruto del trabajo de muchas personas. Os quiero dar las
gracias a todos: sin vosotros nada de esto hubiera sido posible. En primer lugar, quiero darle las
gracias a mi director de tesis, el Dr. Tolosa. Gracias por confiar en mí, por darme la oportunidad de
trabajar con usted, por enseñarme, por su paciencia (también por su impaciencia), por las infinitas
versiones de cada artículo, por su espíritu infatigable, por transmitirme su energía, por sus ganas
de aprender cosas nuevas. Gracias por haber sido mi maestro.
Quiero dar unas gracias muy especiales a mis compañeras de viaje. Laura Maragall, gracias por
estar siempre, por hacerme las cosas sencillas, por ser mi amiga. Ana Fernández, gracias por
dejarme compartir tu “altar”, por ser tan buena compañera y amiga. Meritxell Santos, gracias por
tu vitalidad, por su inestimable ayuda. Muchas gracias también a Alba, Christine, María, que tanto
me habéis ayudado.
Gracias a todo el equipo de Trastornos del Movimiento. Dra. Martí, Dr. Valldeoriola, Dr. Compta,
Dr. Muñoz, gracias por vuestra confianza y ayuda. He aprendido mucho durante estos años,
muchas gracias. Un agradecimiento muy especial para la Dra. Buongiorno, gracias por tu forma
de ser, por ser “galaico-napolitana” y para Ana Cámara, gracias por estar siempre dispuesta, por
tu gran corazón. Francesca Antonelli, Judith Navarro, Alicia Garrido, aunque hayamos coincidido
menos, ha sido un placer trabajar con vosotras.
Gracias al equipo de la Dra. Junqué, Bárbara, Hugo, habéis sido muy importantes para mí en
esta tesis, gracias por las horas que le habéis dedicado. Muchas gracias también al equipo de
Trastornos del Sueño. Dr. Iranzo, gracias por tu genialidad, por tus risas, por tu apoyo, por los
nachos. Dr. Santamaría, gracias por la inmersión en las parasomnias de Lugo, toda una expe-
riencia. Dr. Gaig, parte fundamental de esta tesis, gracias por dejarme trabajar contigo. Muchas
gracias al equipo de Trastornos del Movimiento de Can Ruti, que sembraron en mí, hace ya unos
cuantos años, “el gusanillo de las neurodegenerativas”. Dr. Álvarez y Dra. Ispierto, muchas gracias
por todo. Nos queda mucho por hacer juntos!
Agradecimientos

Agradecimientos
Ellen Gelpí, te mereces un párrafo aparte. Si no fuera por ti, nada de esto hubiera pasado.
Gracias por abrirme las puertas del Banc de Teixits aquel caluroso verano, por enseñarme los
cuerpos de Lewy, por darme tan buenos consejos. Eres genial.
Quiero dar unas gracias enormes a los pacientes y a sus familiares. Sois un ejemplo de altruismo.
Muchas gracias por vuestra inmensa generosidad.
Para finalizar, quiero dar las gracias a las personas más importantes de mi vida, sin las que esto no
sería posible. Chema, gracias por quererme, por soportarme, por tu apoyo constante, por seguir
ahí a pesar de los fines de semana “sin planes” por culpa de esta tesis. Gracias a la abuela, a mis
padres, a mi hermano, a mi cuñada, a mis sobrinos que, aún en la distancia y casi sin darse cuenta,
han sido tan importantes en esta tesis. Gracias de todo corazón.



Índice
1. PRESENTACIÓN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2. LISTADO DE ABREVIATURAS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
3. INTRODUCCIÓN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
3.1. La enfermedad de Parkinson asociada a mutaciones del gen LRRK2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
3.1.1. Prevalencia de la enfermedad de Parkinson asociada a mutaciones del gen LRRK2 (EP-LRRK2) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
3.1.2. La variable penetrancia de las mutaciones del gen LRRK2 asociadas a la EP . . . . . . . . . . . . . . . . . . . 12
3.1.3. Características clínicas de la EP-LRRK2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
3.1.4. El gen LRRK2: función y mutaciones . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.1.5. Heterogeneidad neuropatológica de la EP-LRRK2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
3.2. La fase premotora del Parkinson asociado a mutaciones del gen LRRK2 . . . . . . . . . . . . . . . . . . . . . . . 16
3.3. Biomarcadores de la enfermedad de Parkinson asociada a mutaciones del gen LRRK2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
3.3.1. Biomarcadores clínicos . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
3.3.2. Biomarcadores de neuroimagen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
3.3.3. Biomarcadores en líquido cefalorraquídeo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
4. HIPÓTESIS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
5. OBJETIVOS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
6. RESULTADOS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
6.1. Trabajo 1: Nonmotor symptoms in LRRK2 G2019S associated Parkinson’s disease . . . . . . . . . . . . . . 35
6.2. Trabajo 2: Clinical and imaging markers in premotor LRRK2 G2019S mutation carriers . . . . . . . . . 47
6.3. Trabajo 3: Reduced thalamo-cortical functional connectivity in asymptomatic LRRK2 mutation carriers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
6.4. Trabajo 4: Cerebrospinal fluid biomarkers and clinical features in leucine-rich repeat kinase 2 (LRRK2) mutation carriers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
7. SÍNTESIS DE RESULTADOS Y DISCUSIÓN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .105
8. CONCLUSIONES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 115
9. BIBLIOGRAFÍA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 119


CAPÍTULO 1
Presentación


3
PRESENTACIÓN 1
Esta tesis doctoral se estructura según las directrices de la normativa para la presentación de
tesis doctorales como compendio de publicaciones aprobada por la Comisión de Doctorado del
Consejo de Gobierno en fecha 24 de Julio de 2008 y modificada el 28 de Abril de 2010, al amparo
del régimen previsto en el RD 99/2011 del 28 de Enero.
La presente memoria se basa en cuatro trabajos que pertenecen a una misma línea de trabajo:
el estudio de la enfermedad de Parkinson asociada a mutaciones del gen LRRK2. En primer lugar,
se ha estudiado la enfermedad de Parkinson asociada a mutaciones del gen LRRK2 desde un
punto de vista clínico, centrándonos en los síntomas no motores. En segundo lugar se ha reali-
zado un estudio a través de la sonografía transcraneal en portadores de la mutación G2019S
del gen LRRK2, tanto pacientes con enfermedad de Parkinson como portadores asintomáticos.
En tercer lugar, evaluamos la conectividad funcional a través de resonancia magnética en porta-
dores asintomáticos de mutaciones del gen LRRK2. Por último, se ha investigado la capacidad de
los biomarcadores en líquido cefalorraquídeo para diferenciar a los portadores de mutaciones del
gen LRRK2 de no portadores.
Los dos primeros trabajos han sido publicados (Nonmotor symptoms in LRRK2 G2019S associated
Parkinson’s disease. PLOSone. FI: 3.234; Clinical and imaging markers in premotor LRRK2 G2019S
mutation carriers. Parkinsonism and related disorders. FI: 3.972). Los otros dos trabajos están en
revisión en dos revistas indexadas.
El presente trabajo de tesis doctoral ha sido parcialmente financiado por la Marató de TV3 y por la
Michael J Fox Foundation for Parkinson’s Research (MJFF).


CAPÍTULO 2
Listado de abreviaturas


7
LISTADO DE ABREVIATURAS 2
Aβ1-42 : Beta-amiloide
aLRRK2: Portadores asintomáticos de mutaciones del gen LRRK2
EP :Enfermedad de Parkinson
EPI: Enfermedad de Parkinson idiopática
EP-LRRK2: Enfermedad de Parkinson asociada a mutaciones del gen LRRK2
LCR: Líquido cefalorraquídeo
LB: Cuerpos de Lewy (Lewy body)
LRRK2: Leucine-rich repeat kinase 2
RM: Resonancia Magnética
RMf: Resonancia Magnética funcional
SN: Sustancia nigra
SNM: Síntomas no motores
STC: Sonografía transcraneal
Tau: Proteína tau
TCSR: Trastorno de conducta del sueño REM
T-tau: Proteína Tau total
p-tau: Proteína Tau fosforilada
α-syn: Alfa-sinucleína


Introducción
CAPÍTULO 3


11
INTRODUCCIÓN 3
3.1. LA ENFERMEDAD DE PARKINSON ASOCIADA A MUTACIONES DEL GEN LRRK2
La etiología de la enfermedad de Parkinson (EP) es desconocida en la mayoría de casos, de ahí el
nombre de enfermedad de Parkinson idiopática (EPI). Sin embargo, nuestro concepto sobre la etio-
logía de la EP ha cambiado drásticamente en los últimos 15 años gracias, en parte, a los importantes
descubrimientos en el campo de la genética. La identificación de genes asociados a formas mono-
génicas de la enfermedad, tanto con un patrón de herencia autosómico dominante (alfa-sinucleína
(SNCA), Leucine-rich repeat kinase 2 (LRRK2), ATXN2, ATXN3, MAPT, GCH1, DCTN1 y VPS35), como rece-
sivo (gen Parkin (PARK2), DJ-1 (PARK7), PTEN induced putative kinase 1 (PINK1), ATP13A2, FBXO7, PANK2 y
PLA2G6), así como los recientes progresos en la definición de loci con riesgo genético para la EP, han
permitido realizar un gran avance en el conocimiento de los mecanismos patogénicos de la EP.
3.1.1. Prevalencia de la enfermedad de Parkinson asociada a mutaciones del gen
LRRK2 (EP-LRRK2)
Las mutaciones en el gen LRRK2, descritas por primera vez en el año 2004 1-2, son la causa más
frecuente de parkinsonismo hereditario y son responsables de una proporción significativa
de casos de EP, tanto familiares como esporádicos. Entre las mutaciones del gen LRRK2 la más
frecuente es la G2019S, con una frecuencia global del 1 % en pacientes con EP esporádica y del
4 % en los casos familiares, aunque estas cifras varían según la población estudiada 3. Así, la preva-
lencia más elevada de esta mutación es en la población árabe del Norte de África (36 % de los
casos de EP familiares y 39 % de los esporádicos) y en los judíos askenazíes (28 % de los familiares
y 10 % de los esporádicos). En Europa, la frecuencia de esta mutación es más elevada en los países
de Sur. La mutación G2019S es rara en Asia (< 0.1 %) 3. La distribución geográfica de esta muta-
ción se puede explicar en parte por el llamado “efecto fundador”. En el 95 % de los casos caucá-
sicos europeos, judíos ashkenazíes y árabes del Norte de África se ha identificado un haplotipo
común. Se hipotetiza que la mutación en estas poblaciones proviene de un ancestro común que
vivió en Oriente medio hace más de 2000 años, en el periodo de las diásporas judías, donde las
poblaciones judías y árabes vivían próximas 4. En cuanto al resto de mutaciones LRRK2 patógenas,
mucho menos frecuentes, destaca la R1441G como la mutación más prevalente en el Norte de
España, especialmente en el País Vasco, donde fue inicialmente identificada.

12
INTRODUCCIÓN3
En España, la prevalencia de mutaciones del gen LRRK2 también presenta una gran variabilidad
según la población estudiada. La prevalencia más elevada de la mutación G2019S se encontró en
Cantabria, siendo del 8.7 % de la población con EP 5, seguida por Cataluña con una prevalencia
del 6.4 % en los casos familiares y del 3.4 % en los esporádicos 6. La R1441G se encontró, en el caso
de Cataluña, en un 0.7 % de los casos de EP. En el País Vasco, la prevalencia de la G2019S fue del
3.82 %, mientras que la de la R1441G fue del 13.16 %. Es importante resaltar que la frecuencia de
la G2019S fue mayor en población no vasca (6.9 %) mientras que la R1441G fue más frecuente en
la población de origen vasco (22.4 %) 5,7, reforzando la importancia del origen étnico a la hora de
determinar la prevalencia de la mutación. En otras regiones como Asturias, Extremadura y Anda-
lucía la prevalencia fue inferior (2.7 %, 2.08 % y 1.7 %, respectivamente) 8-9.
3.1.2. La variable penetrancia de las mutaciones del gen LRRK2 asociadas a la EP
Las mutaciones en el gen LRRK2 tienen una penetrancia variable según los diferentes estudios
y poblaciones. La mutación G2019S presenta una penetrancia incompleta, edad-dependiente.
Hasta el momento el mayor trabajo realizado a este respecto es el de Healy et al. donde se estima
una penetrancia asociada a la edad para la mutación G2019S del 28 % a los 59 años, 51 % a los
69 años y 74 % a los 79 años 3. Estas diferencias en la penetrancia dependen, fundamentalmente,
del diseño del estudio y de la población estudiada. Así, en las poblaciones donde se estudian
formas familiares de EP la penetrancia es más elevada (100 % a los 75 años, 85 % a los 70 años,
75 % a los 79 años y 67 % a los 85 años) 3,10-12 que en las muestras donde se estudian pacientes
con EP independientemente de la historia familiar (37 %, 24 % y 32 % a los 80 años) 13-14. Un estudio
reciente realizado en Cantabria estima que la penetrancia es en torno al 2 % a los 50 años, 12 %
a los 60 años, 26 % a los 70 años y 47 % a los 80 años 5. Esta penetrancia variable de las muta-
ciones del gen LRRK2 dificulta el estudio de marcadores de riesgo de la enfermedad dado que una
proporción de los portadores asintomáticos de mutaciones del gen LRRK2 nunca la desarrollarán.
3.1.3. Características clínicas de la EP-LRRK2
La EP asociada a mutaciones del gen LRRK2 (EP-LRRK2) y la EPI son clínicamente indistinguibles,
aunque se han descrito algunas diferencias 3,6,15. La edad de inicio es similar en ambas, siendo los

13
INTRODUCCIÓN 3
55-60 años la edad de inicio más habitual. Desde el punto de vista motor, tienen un fenotipo muy
parecido, sin embargo, según algunos estudios la EP-LRRK2 presenta una evolución más benigna 16.
Otros datos como un mayor tiempo desde los primeros síntomas hasta la primera caída, un mayor
tiempo en avanzar en el estadio Hoehn y Yahr o en la necesidad de recibir tratamiento dopami-
nérgico apoyan también esta teoría. Aunque algunos estudios apuntan a un predominio del feno-
tipo tremórico en la EP-LRRK2 17-18, otros sugieren que la forma rígido-acinética es más frecuente
en pacientes EP-LRRK2 de inicio precoz 19. También parece ser que la distonía es más frecuente en
la EP-LRRK2 que en las formas idiopáticas (42 % vs 25 %) y que, además, esta distonía aparece en
los primeros años de la enfermedad con más frecuencia (18 %) que en los casos idiopáticos (4 %) 3.
Por otra parte, los síntomas no motores (SNM), frecuentes en la EPI 20, no están bien definidos en la
EP-LRRK2. Algunos estudios muestran que la presencia de SNM es similar a la forma idiopática, con
la excepción de un menor riesgo de deterioro cognitivo e hiposmia 3,16. Así, en el estudio de Healy
et al, un 23 % de los pacientes con EP-LRRK2 tenían deterioro cognitivo mientras que el porcen-
taje ascendía al 70 % en la EPI. También se ha observado una menor presencia de trastorno de
conducta del sueño REM (TCSR) 21 y de disautonomía 22 en la EP-LRRK2 que en la EPI. Sin embargo
existen pocos estudios al respecto, con un número bajo de pacientes y, en ocasiones, sin un
grupo de sujetos control, sin enfermedad de Parkinson. Tampoco se conoce, hasta el momento,
la correlación clínico-patológica de estos SNM.
3.1.4. El gen LRRK2: función y mutaciones
El gen LRRK2, también conocido como PARK8, está localizado en el cromosoma 12 y codifica
una proteína de 2527 aminoácidos llamada Dardarina (con origen en la palabra vasca “dardara”,
que significa temblor). Dicha proteína contiene 6 dominios: ANK (ankyirin-like repeat), LRR (leuci-
ne-rich repeat), ROC (Ras of Complex proteins), COR (C-terminal of ROC), MAPKKK (mitogen-activated
protein kinase kinase kinase) y WD40, en el extremo C-terminal. La proteína LRRK2 tiene actividad
kinasa y GTPasa, jugando un importante papel en las vías de señalización celular. LRRK2 es,
fundamentalmente, una proteína citoplasmática, aunque también se relaciona con organelas de
membrana como la mitocondria, el retículo endoplásmico, el aparato de Golgi y el endosoma.

14
INTRODUCCIÓN3
LRRK2 se ha asociado a diversas funciones celulares y procesos de señalización incluyendo la
función mitocondrial, el tráfico de vesículas, la endocitosis, y la autofagia 23-24. Los estudios con
modelos experimentales, como Drosophila melanogaster y Caenorhabditis elegans y con ratones,
han demostrado que la alteración en la función de LRRK2 conduce a daño axonal y muerte
neuronal, sin embargo, todavía se desconocen los mecanismos subyacentes 23.
Existen al menos siete mutaciones en este gen que se consideran patógenas: p.N1437H,
p.R1441C/G/H, p.Y1699C, pG2019S y p.I2020T 25. La mutación G2019S fue identificada inicialmente
en 2 familias caucásicas, una de origen Norteamericano-británico y otra de origen judío Askenazí 1.
La R1441C fue descrita inicialmente en una familia norteamericana y otra caucásica 2. La Y1699C
se describió inicialmente en una familia británica y otra germano-canadiense 2 y la I2020T fue
descrita en la familia Sagamihara, de origen japonés 26. Recientemente, se han encontrado, además,
variantes de susceptibilidad que aumentan el riesgo de EP, como R1628P, G2385R y S1761R 27.
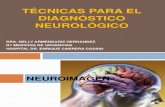
ARM WD40ANK kinaseLRR ROC COR
S910P
S955PConstitutive phosphorylation
PS935
PS973 S1292
N1437H R1628P
G20195R1441G/C/H Y1699C G2385RI202DT
T1343, S1403, T1404, T1410, T1491, T1503
T1967, T1969, T2031, S2032, T2035
T2483
25271
Autophosphorylation sites
Pathogenic mutationsSusceptibility
polymorphism
Figura 1: Estructura del gen LRRK2, mutaciones patógenas y polimorfismos de susceptibilidad (en rojo),
fosforilación constitucional (en verde) y una selección de los sitios de autofosforilación (en negro).
3.1.5. Heterogeneidad neuropatológica de la EP-LRRK2
La EPI se caracteriza por una pérdida de las neuronas dopaminérgicas en la pars compacta de la
SN junto con la presencia de agregados intraneuronales de alfa-sinucleína en forma de cuerpos
de Lewy (LB) y neuritas de Lewy. La primera descripción neuropatológica de la EP-LRRK2 fue en
el año 2004 28. Wszolek y colaboradores describieron 4 casos de EP dentro de una familia de 190
miembros con 22 afectos de EP asociada a mutaciones en el locus PARK8 del cromosoma 12.

15
INTRODUCCIÓN 3
Los 4 casos presentaban una EP con buena respuesta a levodopa, sin embargo los hallazgos de la
autopsia eran heterogéneos: los 4 casos mostraban pérdida neuronal y gliosis en la sustancia nigra
(SN), uno de ellos presentaba además LB en el tronco encefálico, otro tenía LB difusos y en otro se
encontraron ovillos neurofibrilares sin LB. En una revisión reciente sobre la neuropatología de la EP
de causa genética se revisan 49 casos de portadores de mutaciones del gen LRRK2, 28 de ellos eran
portadores de la mutación G2019S y los otros 21 presentaban otras mutaciones (I2020T, R1441C,
Y1699C, R1441G, R1441R, I1371V, R793M, L1165P y N1437H) 29. Analizando de forma global estos casos,
en todos los pacientes con parkinsonismo portadores de la mutación G2019S se encontró pérdida
neuronal en la pars compacta de la SN y en el locus coeruleus. Además, un 79 % de ellos tenían pato-
logía tipo LB, con afectación cortical variable. También se encontraron inclusiones de la proteína Tau,
aunque su presencia fue muy variable, tanto en su distribución como en su severidad. Los portadores
de otras mutaciones diferentes de G2019S presentaron más pérdida neuronal en la pars compacta de
la SN que en el locus coeruleus y sólo en el 43 % de ellos había patología tipo LB.
Recientemente se ha publicado el primer estudio clínico-patológico en una serie de 37 casos de
EP-LRRK2 30. En él encontraron que, entre las diferentes mutaciones, la G2019S fue la más frecuen-
temente asociada a patología tipo LB. El fenotipo predominantemente motor se asoció con la
ausencia de LB, mientras que la presencia de algunos síntomas no motores, como el deterioro
cognitivo, la ansiedad y la hipotensión ortostática se correlacionaron con la presencia de LB. Estos
hallazgos demuestran que los síntomas motores clásicos pueden aparecer en ausencia de LB, y
que, sin embargo, la patología asociada a LB en la EP-LRRK2 puede ser un marcador de un cuadro
clínico más extenso, incluyendo deterioro cognitivo.
En resumen, los hallazgos neuropatológicos en pacientes con mutaciones del gen LRRK2 pueden
variar considerablemente, sobre todo en aquellos pacientes con mutaciones diferentes a la G2019S.
La mayoría de casos de EP asociada a la mutación G2019S presentan inclusiones neuronales de
alfa-sinucleína, al contrario de lo que ocurre en otras mutaciones LRRK2. Esta heterogeneidad en
la patología, con afectación además de diferentes áreas cerebrales, puede suponer además una
heterogeneidad clínica, bioquímica y de neuroimagen en los pacientes con EP-LRRK2.

16
INTRODUCCIÓN3
3.2. LA FASE PREMOTORA DE LA EP-LRRK2
Los estudios de Braak et al. y, posteriormente de otros grupos, han sugerido que los cambios
neuropatológicos de la EP comienzan en estructuras extranígricas e incluso en estructuras fuera
del sistema nervioso central 31. La fase premotora de la EP es bien reconocida en la actualidad.
Diferentes hallazgos clínicos y de neuroimagen sugieren que el inicio del proceso neurodegene-
rativo en la EP comienza mucho tiempo antes del inicio de los síntomas motores 32.
El estudio de esta fase premotora es una de las áreas de investigación más importantes en la
actualidad en la EP. Un mayor conocimiento de esta etapa de la enfermedad nos puede ayudar a
dilucidar cuándo y dónde empieza la EP. También es la fase premotora el momento ideal para la
implementación de ensayos clínicos con fármacos modificadores de la enfermedad. Sin embargo,
estudiar la fase premotora de la EP no es tarea fácil. Varios estudios han encontrado que la pérdida
de olfato 33, el trastorno de conducta de la fase REM del sueño 34 y la depresión 35 pueden preceder
el inicio de los síntomas motores en la EP. Una manera de profundizar en la fase premotora es el
estudio de poblaciones en riesgo de desarrollar EP: hiposmia primaria, trastorno de conducta de
la fase REM del sueño y la EP de causa genética.
En este trabajo nos hemos centrado en la EP-LRRK2, ya que es la causa más frecuente de EP gené-
tica y los portadores asintomáticos de mutaciones del gen LRRK2 son una población en riesgo de
desarrollar EP. Por otra parte, ya que la EP-LRRK2 es clínica y patológicamente similar a la EPI, los
resultados del estudio de la fase premotora de la EP-LRRK2 se podrían generalizar a la EPI.
3.3. BIOMARCADORES DE LA EP-LRRK2
3.3.1. Biomarcadores clínicos
Los portadores asintomáticos de mutaciones del gen LRRK2 (aLRRK2), en riesgo de padecer EP,
son una población adecuada para el estudio de la fase premotora de la EP. No obstante, debemos
tener en cuenta que la penetrancia de las mutaciones en el gen LRRK2 es incompleta, es decir, no
todos los aLRRK2 desarrollarán la enfermedad. Teniendo en cuenta estas dos premisas, la identifi-
cación de características clínicas, bioquímicas o de neuroimagen diferenciales en este grupo de

17
INTRODUCCIÓN 3
sujetos es de gran importancia para un mejor conocimiento de los mecanismos etiopatogénicos
de la EP-LRRK2.
Hasta el momento hay poca literatura sobre este tema. Desde un punto de vista clínico, estudios
recientes han evaluado las posibles diferencias entre los aLRRK2, los familiares no portadores de la
mutación e individuos sanos, con resultados dispares 16,36-37. Recientemente se ha observado que
los aLRRK2 presentan más síntomas no motores que los no portadores de la mutación 38. También
se han encontrado diferencias entre aLRRK2 y no portadores en la identificación de los olores 37,
en la marcha 39 y en ciertos aspectos de la función ejecutiva 40. Sin embargo, otros estudios no
encontraron diferencias entre aLRRK2 y controles 16,41. Es interesante destacar el estudio de Marras
y cols. en el que se observó que los familiares asintomáticos de pacientes con EP-LRRK2, indepen-
dientemente de su estatus genético (portadores o no de una mutación en el gen LRRK2), tenían
una mayor puntuación en escalas motoras como la UPDRS-III, más estreñimiento y una mayor
alteración en la discriminación de los colores 36.
3.3.2. Biomarcadores de neuroimagen
3.3.2.1. Sonografía transcraneal
La sonografía transcraneal (STC) es una técnica de imagen no invasiva, inicialmente desarro-
llada en el diagnóstico de las enfermedades cerebrovasculares, y que, a partir de la mitad de la
década de los noventa, se ha empezado a utilizar para la visualización de estructuras cerebrales
profundas y, más recientemente, se ha aplicado en la EP y otros trastornos del movimiento. Becker
observó, por primera vez en 1995, de forma casual durante la resección de un tumor cerebral
en un paciente con EP, la hiperecogenicidad de la sustancia nigra utilizando la STC 42. A partir de
entonces, múltiples estudios han demostrado su utilidad para el estudio de diferentes estructuras
cerebrales profundas como el tronco encefálico o el sistema ventricular.
La STC ha demostrado, en los últimos años, su utilidad en la evaluación de los Trastornos del Movi-
miento, entre ellos, en la EP. Aproximadamente un 90 % de los pacientes con EPI presentan una hipe-
recogenicidad de la SN 43, mientras que sólo un 10 % de los sujetos sanos presentan dicha alteración 44.

18
INTRODUCCIÓN3
Según estudios recientes, la hiperecogenicidad de la SN se mantiene estable a lo largo del tiempo
y no se asocia con la severidad de la enfermedad 45. Por otra parte, la hiperecogenicidad de la SN
se ha asociado a un riesgo aumentado de desarrollar EP en la población general 46, lo que sugiere
que podría ser un marcador precoz de la enfermedad. En un estudio realizado en 400 sujetos
sanos en el que se detectó hiperecogenicidad de la SN en un 9 %, se observó que algunos de ellos
tenían una alteración de la vía nigroestriatal en la tomografía de emisión de positrones (PET) con
fluorodopa 47. Además, la hiperecogenicidad de la SN también se ha asociado a otros marcadores
prodrómicos de la EP como la hiposmia 48 y el trastorno de conducta del sueño REM 49.
No obstante, hay que tener en cuenta que la hiperecogenicidad de la SN no se observa única-
mente en la EP sino que también se ha descrito en pacientes con otros trastornos del movimiento,
como por ejemplo en la distonía DYT6 50, en la enfermedad de Huntington 51 o en parkinsonismos
atípicos 52.
Otros hallazgos ecográficos han sido menos estudiados, pero han demostrado ser útiles en el
diagnóstico y diagnóstico diferencial de los trastornos del movimiento. La hiperecogenicidad del
núcleo lenticular se ha observado en pacientes con distonía 53 y puede correlacionarse con la
gravedad de la enfermedad de Wilson 54. La hipoecogenicidad de los núcleos del rafe ha sido
descrita en el 70 % de pacientes con depresión y, más recientemente, en pacientes con trastorno
de conducta del sueño REM, sujetos en riesgo de desarrollar EP 55.
Significado de la hiperecogenicidad de la SN
Diferentes estudios de imagen, estudios experimentales en modelos animales y estudios post-
mortem en humanos, apoyan la hipótesis de que la alteración en el depósito de hierro local y
los cambios en la composición celular en la sustancia nigra, condicionan la hiperecogenicidad
de la misma 56. En general, la ecogenicidad de cualquier estructura depende de su impedancia
acústica y de la relación con la de las estructuras adyacentes. Un aumento de la ecogenicidad de
las estructurales cerebrales profundas puede resultar de la composición de los componentes de
las neuronas, de la glía y de las fibras de conexión; por otra parte, el acúmulo de metales pesados

19
INTRODUCCIÓN 3
como el hierro, el cobre o el manganeso, puede producir un aumento de la ecogenicidad. La
hiperecogenicidad de la SN en la EP se ha asociado a un aumento del contenido de hierro y al
daño oxidativo 45.
Sonografía transcraneal en portadores de mutaciones en el gen LRRK2
Existen escasos estudios de sonografía transcraneal en pacientes con EP-LRRK2 y en aLRRK2. En los
pacientes con EP-LRRK2 se ha observado un porcentaje de hiperecogenicidad de la SN similar al
descrito en la EPI 16. Hasta un 85-90 % de los aLRRK2 también presentan este hallazgo ecográfico 16,57,
aunque los estudios al respecto son escasos y los tamaños muestrales limitados.
3.3.2.2. Resonancia magnética estructural y funcional
En los últimos años se han realizado múltiples estudios en pacientes con EP utilizando diferentes
técnicas de resonancia magnética (RM) cerebral, tanto estructural como funcional. Los estudios
de RM estructural han mostrado alteraciones en los pacientes con EP como una reducción en el
volumen de la sustancia gris en determinadas áreas corticales y subcorticales 58, una reducción
en la fracción de anisotropía en las proyecciones nigroestriatales y una atrofia cortical focal 59-61.
En los últimos años, el desarrollo de las técnicas de RM funcional (RMf) han permitido estudiar la
conectividad funcional en la EP. La conectividad funcional relaciona redes neuronales espacial-
mente remotas que muestran cierta interrelación y se apoya principalmente en las técnicas de
RMf tradicional, mediante la cual es posible medir las variaciones en la imagen de la intensidad de
la señal asociadas a los cambios hemodinámicos que acompañan a la activación celular, desenca-
denada por un estímulo determinado a través del contraste dependiente del nivel de oxigenación
en sangre (BOLD, Blood Oxygen Level-Dependent Contrast). Por otra parte, cabe resaltar que además
existe una actividad intrínseca neuronal que corresponde a fluctuaciones espontáneas de baja
frecuencia. Generalmente se trata de un grupo de zonas vinculadas a la organización de la acti-
vidad interna intrínseca del cerebro. La mayoría de los estudios de estas fluctuaciones se llevan
a cabo durante el estado de reposo, es decir, sin aplicar estímulo alguno. Las redes funcionales
generadas bajo tales condiciones se denominan redes ‘resting-state’ (RS). Los resultados derivados

20
INTRODUCCIÓN3
de estudios con RMf apuntan a que la EP está asociada con una alteración en la conectividad
funcional 62. En los pacientes con EP se han observado alteraciones en la conectividad durante la
realización de una determinada tarea 63-64. Los estudios de RS RMf en EP han mostrado resultados
dispares. Por un lado, algunos estudios apuntan a que en la EP existe una disminución en la conec-
tividad funcional entre diferentes áreas cerebrales, como por ejemplo entre el tálamo y la corteza
sensitivo-motora 65 o entre el estriado y el tálamo, mesencéfalo, protuberancia y cerebelo 66.
En pacientes en estadios precoces de la EP, incluso que no recibían aún tratamiento dopaminér-
gico, se ha observado también una reducción en la conectividad funcional entre el caudado y
el tálamo y las cortezas frontal e insular 67 y también en los circuitos corticoestriatal y mesolímbi-
co-estriatal 68. Sin embargo, otros estudios encuentran aumentos en la conectividad funcional 69-70.
Estas discrepancias se pueden explicar en parte por la utilización de diferente metodología
empleada.
RM en la fase premotora de la EPI y otras enfermedades neurodegenerativas
Hasta la fecha no hay estudios publicados que describan los cambios en la conectividad funcional
en las fases preclínicas de la EPI. Sin embargo, se ha descrito una disminución en la conecti-
vidad funcional en estadios preclínicos de otras enfermedades neurodegenerativas como la
enfermedad de Alzheimer o la enfermedad de Huntington. En la enfermedad de Alzheimer se ha
observado una disminución en la conectividad funcional que afecta, principalmente, a regiones
límbicas, como el hipocampo, el parahipocampo, el cingulado anterior y la corteza temporal
medial 71. En portadores de la mutación de la enfermedad de Huntington, en fases preclínicas,
también se ha observado recientemente alteraciones en la conectividad funcional que afecta
fundamentalmente al circuito frontoestriatal, pero también al tálamo, a la ínsula anterior y a los
centros de la memoria 72. Es interesante remarcar que, en la enfermedad de Huntington preclínica,
se ha observado un aumento de la conectividad funcional entre las áreas parietal y atencional
ventral y áreas frontales y subcorticales en aquellos sujetos portadores de la mutación, asintomá-
ticos, pero cercanos al teórico inicio de la enfermedad, mientras que, en los portadores alejados
todavía de la enfermedad, es decir, en fases muy precoces, sólo se han encontrado disminuciones
de la conectividad 72.

21
INTRODUCCIÓN 3
RM en la EP-LRRK2
A día de hoy no existen estudios de RMf en pacientes con EP-LRRK2. Existen, sin embargo, algunos
estudios de RM estructural y funcional en aLRRK2 que han mostrado alteraciones cerebrales en
estos sujetos 16,73-76. Estudios de RM estructural han mostrado que el volumen de sustancia gris
(Gray matter volumen; GMV) en los núcleos caudado y cuneus está aumentado en los aLRRK2 73,77,
mientras que también se ha observado una disminución de dicho volumen en las regiones orbi-
tofrontal y prefrontal 73. En estudios de RMf basados en la realización de tareas (task-based) en
aLRRK2 se encontraron cambios la conectividad cerebral en diferentes áreas cerebrales corticales
y subcorticales 74-75. Sólo hay un estudio que evalúa la conectividad funcional mediante RS RMf
en aLRRK2 76. En este estudio, los aLRRK2 presentaron una interacción disminuida entre la conecti-
vidad de la corteza parietal inferior derecha y el putamen dorsoposterior pero un aumento de la
interacción entre esta área cortical y el putamen ventroanterior.
3.3.3. Biomarcadores en líquido cefalorraquídeo
Las proteínas presentes en el líquido cefalorraquídeo (LCR) se han propuesto como una fuente
potencial de biomarcadores de las enfermedades neurodegenerativas, ya que las proteínas
implicadas en la patología de estas enfermedades probablemente difunden al LCR. La alfa-sinu-
cleína (α-syn) es, potencialmente, la proteína más prometedora ya que podría reflejar la patología
asociada a los cuerpos de Lewy, el distintivo neuropatológico de la EP. Los niveles de α-syn total
en el LCR han sido estudiados en la EPI, encontrando una disminución de los mismos, incluso en
estadios precoces de la enfermedad 78-83, mientras que los niveles de los oligómeros de α-syn
parecen estar aumentados 82,84-86.
Los biomarcadores en LCR de la enfermedad de Alzheimer, beta-amiloide (Aβ1-42) y proteína Tau,
tanto total (T-tau) como en su forma fosforilada (phospho-tau, p-tau), también se han estudiado
en la EP. En cuanto a los niveles de Aβ1-42 algunos estudios encontraron que estaban dismi-
nuidos en la EPI comparado con controles 78,87 mientras que otros estudios no consiguieron
replicar estos resultados 80,88-91. Los estudios sobre la proteína Tau también han mostrado
resultados dispares 78-81,87-93. Las razones para estas discrepancias pueden incluir la diferente

22
INTRODUCCIÓN3
metodología utilizada, incluyendo el procesamiento del LCR, las sondas de biomarcadores utili-
zadas, la diversidad en los criterios de selección del grupo control y el estadio de la EP en los
diferentes estudios. En la EPI los niveles alterados de proteínas en LCR se han correlacionado
con alteraciones cognitivas 77,87,89,94-97.
La información disponible en la actualidad sobre los niveles en LCR de α-syn y de proteínas
asociadas a las enfermedad de Alzheimer en los portadores de mutaciones del gen LRRK2, tanto
pacientes con Parkinson como portadores asintomáticos, es preliminar 98-100. En los aLRRK2 se ha
observado un aumento de los niveles de oligómeros de α-syn en LCR 100. También se ha obser-
vado en estos sujetos una asociación entre la disminución en los niveles de Aβ1-42 y Tau y la dismi-
nución de la función dopaminérgica estriatal 98.
En resumen, en esta introducción hemos querido destacar la importancia del estudio de la fase
premotora de la enfermedad de Parkinson, en nuestro caso centrándonos en la EP asociada a
mutaciones del gen LRRK2 y en los portadores asintomáticos de dichas mutaciones. Sin embargo,
todavía quedan preguntas sin respuesta tales como cuándo y cómo comienza la fase premotora
de la EP-LRRK2 y en qué consiste, cómo es posible identificar aquellos aLRRK2 que van a desarro-
llar la enfermedad, qué implicaciones prácticas podría tener, etc… Con esta tesis pretendemos
aumentar el conocimiento sobre estos y otros aspectos de la EP-LRRK2. En los trabajos que presen-
tamos a continuación estudiamos, desde el punto de vista clínico, bioquímico y de neuroimagen,
la EP-LRRK2 y los aLRRK2.



Hipótesis
CAPÍTULO 4


27
HIPÓTESIS 4
4. HIPÓTESIS
1. La EP-LRRK2 presenta unas características clínicas, bioquímicas y de neuroimagen que la
diferencian del Parkinson idiopático.
2. Existe marcadores clínicos, bioquímicos y de neuroimagen que diferencian a los portadores
asintomáticos de mutaciones en el gen LRRK2 de sujetos no portadores de dichas mutaciones.


Objetivos
CAPÍTULO 5


31
OBJETIVOS 5
5. OBJETIVOS
1. Estudiar las características clínicas, tanto motoras como no motoras, de pacientes con
EP-LRRK2.
2. Evaluar el área de ecogenicidad de la sustancia nigra y otras variables sonográficas en
pacientes con EP-LRRK2 y en portadores asintomáticos de dichas mutaciones.
3. Examinar la conectividad funcional cerebral en estado de reposo y las características estruc-
turales cerebrales en portadores asintomáticos de mutaciones del gen LRRK2.
4. Analizar los niveles de alfa-sinucleína y de proteínas asociadas a la enfermedad de Alzheimer
en líquido cefalorraquídeo, en pacientes con EP-LRRK2 y en aLRRK2.


Resultados
CAPÍTULO 6


35
RESULTADOS 6
Trabajo número 1
Nonmotor symptoms in LRRK2 G2019S associated Parkinson’s disease
Gaig C, Vilas D, Infante J, Sierra M, García-Gorostiaga I, Buongiorno M, Ezquerra M, Martí MJ,
Valldeoriola F, Aguilar M, Calopa M, Hernandez-Vara J, Tolosa E
PLoS One 2014 Oct 17;9(10):e108982.

36
RESULTADOS6
Síntomas no motores en la enfermedad de Parkinson asociada a la mutación G2019S
del gen LRRK2
Introducción: La EPI y la EP-LRRK2 pueden ser clínicamente diferentes dado que el sustrato neuro-
patológico de la EP-LRRK2 es heterogéneo. El rango y la severidad de los síntomas no motores
asociados con las mutaciones del gen LRRK2 no están bien definidos. El objetivo de este trabajo es
evaluar la prevalencia y el tiempo de aparición de los SNM en un grupo de pacientes con EP-LRRK2.
Métodos: Se estudió la presencia de hiposmia y de alteraciones neuropsiquiátricas, disautonó-
micas y del sueño en un grupo de 33 pacientes con EP-LRRK2 portadores de la mutación G2019S,
a través de cuestionarios estandarizados y escalas validadas. Se realizaron las mismas evaluaciones
en 33 pacientes con EPI, apareados por edad, sexo, duración del parkinsonismo y severidad de la
enfermedad y en 33 sujetos sanos.
Resultados: Las puntuaciones en el test de olfacción UPSIT (University of Pennsylvania Smell
Identification Test) fueron mayores en los pacientes con EP-LRRK2 que en los pacientes con EPI
(23.5 ± 6.8 vs 18.4 ± 6.0; p = 0.002) y la hiposmia fue menos frecuente en los EP-LRRK2 que en los
EPI (39.4 % vs 75.8 %; p = 0.01). Las puntuaciones del UPSIT fueron significativamente más elevadas
en mujeres que en varones en los pacientes con EP-LRRK2 (26.9 ± 4.7 vs 19.4 ± 6.8; p< 0.01).
La frecuencia de alteraciones del sueño, neuropsiquiátricas y disautonomía fue similar entre
EP-LRRK2 e EPI. La hiposmia, la depresión, el estreñimiento y el exceso de somnolencia diurna se
presentaban antes del inicio de los síntomas motores clásicos en más del 40 % de los pacientes
con EP-LRRK2 que presentaban estos síntomas en el momento de la exploración.
Conclusión: Las alteraciones neuropsiquiátricas, disautonómicas y del sueño ocurren con la
misma frecuencia en pacientes con EP-LRRK2 portadores de la mutación G2019S que en los
pacientes con EPI, pero el déficit olfactorio es menos frecuente en EP-LRRK2. Como en la EPI, la
hiposmia, la depresión, el estreñimiento y el exceso de somnolencia diurna pueden preceder al
inicio de los síntomas motores clásicos en la enfermedad de Parkinson asociada a la mutación
G2019S del gen LRRK2.

37
RESULTADOS 6
Nonmotor Symptoms in LRRK2 G2019S AssociatedParkinson’s DiseaseCarles Gaig1,2,3., Dolores Vilas1., Jon Infante3,4, Marıa Sierra3,4, Ines Garcıa-Gorostiaga5,
Mariateresa Buongiorno1,2, Mario Ezquerra1,2,3, Maria Jose Martı1,2,3, Francesc Valldeoriola1,2,3,
Miquel Aguilar6, Matilde Calopa7, Jorge Hernandez-Vara8, Eduardo Tolosa1,2,3*
1 Parkinson’s Disease and Movement Disorders Unit, Neurology Service, Institut de Neurociencies Hospital Clınic, University of Barcelona, Barcelona, Spain, 2 Institut
d’investigacions Biomediques August Pi i Sunyer (IDIBAPS), Barcelona, Spain, 3Centro de Investigacion Biomedica en Red de Enfermedades Neurodegenerativas
(CIBERNED), Madrid, Spain, 4Neurology Service, Hospital Universitario Marques de Valdecilla, University of Cantabria (UC), Santander, Spain, 5Neurology Service, Hospital
de Galdakao, Usansolo, Vizcaya, Spain, 6Neurology Service, Hospital Universitari Mutua de Terrasa, Barcelona, Spain, 7Neurology Service, Hospital Universitari de
Bellvitge, Barcelona, Spain, 8Neurology Service, Hospital Universitari Vall D’Hebron, Barcelona, Spain
Abstract
Background: Idiopathic Parkinson’s disease (IPD) and LRRK2-associated PD (LRRK2-PD) might be expected to differ clinicallysince the neuropathological substrate of LRRK2-PD is heterogeneous. The range and severity of extra-nigral nonmotorfeatures associated with LRRK2 mutations is also not well-defined.
Objective: To evaluate the prevalence and time of onset of nonmotor symptoms (NMS) in LRRK2-PD patients.
Methods: The presence of hyposmia and of neuropsychiatric, dysautonomic and sleep disturbances was assessed in 33LRRK2-G2019S-PD patients by standardized questionnaires and validated scales. Thirty-three IPD patients, matched for age,gender, duration of parkinsonism and disease severity and 33 healthy subjects were also evaluated.
Results: University of Pennsylvania Smell Identification Test (UPSIT) scores in LRRK2-G2019S-PD were higher than those inIPD (23.566.8 vs 18.466.0; p = 0.002), and hyposmia was less frequent in G2019S carriers than in IPD (39.4% vs 75.8%;p = 0.01). UPSIT scores were significantly higher in females than in males in LRRK2-PD patients (26.964.7 vs 19.466.8; p,0.01). The frequency of sleep and neuropsychiatric disturbances and of dysautonomic symptoms in LRRK2-G2019S-PD wasnot significantly different from that in IPD. Hyposmia, depression, constipation and excessive daytime sleepiness, werereported to occur before the onset of classical motor symptoms in more than 40% of LRRK2-PD patients in whom thesesymptoms were present at the time of examination.
Conclusion: Neuropsychiatric, dysautonomic and sleep disturbances occur as frequently in patients with LRRK2-G2019S-PDas in IPD but smell loss was less frequent in LRRK2-PD. Like in IPD, disturbances such as hyposmia, depression, constipationand excessive daytime sleepiness may antedate the onset of classical motor symptoms in LRRK2-G2019S-PD.
Citation: Gaig C, Vilas D, Infante J, Sierra M, Garcıa-Gorostiaga I, et al. (2014) Nonmotor Symptoms in LRRK2 G2019S Associated Parkinson’s Disease. PLoSONE 9(10): e108982. doi:10.1371/journal.pone.0108982
Editor: John Duda, Philadelphia VA Medical Center, United States of America
Received March 22, 2014; Accepted September 4, 2014; Published October 17, 2014
Copyright: � 2014 Gaig et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricteduse, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.
Funding: Dr. Tolosa received honoraria for consultancy from Novartis, TEVA, Boehringer Ingelheim, UCB, Solvay, Lundbeck, and TEVA. He also received fundingfor research from Spaniard Network for Research on neurodegenerative Disorders (CIBERNED)- instituto Carlos III (ISCIII), The Michael J. Fox Foundation forParkinson’s Research (MJFF), and Fondo de Investigaciones Sanitarias de la Seguridad Social (FISS). Dr. Infante receives research support from the Fondo deInvestigacion Sanitaria-ISCIII (PI11/00228) and from ‘‘Centro de Investigacion Biomedica en Red de Enfermedades Neurodegenerativas’’ (CIBERNED) (CB06/05/0037). Dr. Sierra receives research support from the Institute for Formation and Research from the Marques de Valdecilla Foundation-IFIMAV (WLA 04/11) andfrom ‘‘Centro de Investigacion Biomedica en Red de Enfermedades Neurodegenerativas’’ (CIBERNED) (CB06/05/0037). Dr. Ezquerra was supported by a MiguelServet contract of the Instituto de Salud Carlos III (ISCIII). Dr. Gaig, Dr. Vilas, Dr. Buongiorno, and Dr. Martı report no disclosures. Dr. Valldeoriola has receivedhonoraria from Medtronic Iberica, Boston Scientific, Abbvie Pharmaceutiocals and UCB pharma for lectures and courses. Dr. Garcıa-Gorostiaga, Dr. Aguilar, Dr.Calopa, and Dr. Hernandez-Vara report no disclosures. The funders had no role in study design, data collection and analysis, decision to publish, or preparation ofthe manuscript.
Competing Interests: Dr. Tolosa received honoraria for consultancy from Novartis, TEVA, Boehringer Ingelheim, UCB, Solvay, Lundbeck, and TEVA, and hereceived funding for research from Spaniard Network for Research on neurodegenerative Disorders (CIBERNED)- instituto Carlos III (ISCIII), The Michael J. FoxFoundation for Parkinson’s Research (MJFF), and Fondo de Investigaciones Sanitarias de la Seguridad Social (FISS). Dr. Infante receives research support from theFondo de Investigacion Sanitaria-ISCIII (PI11/00228) and from ‘‘Centro de Investigacion Biomedica en Red de Enfermedades Neurodegenerativas’’ (CIBERNED)(CB06/05/0037). Dr. Sierra receives research support from the Institute for Formation and Research from the Marques de Valdecilla Foundation-IFIMAV (WLA 04/11) and from ‘‘Centro de Investigacion Biomedica en Red de Enfermedades Neurodegenerativas’’ (CIBERNED) (CB06/05/0037). Dr. Ezquerra was supported by aMiguel Servet contract of the Instituto de Salud Carlos III (ISCIII). Dr. Valldeoriola has received honoraria from Medtronic Iberica, Boston Scientific, AbbviePharmaceutiocals and UCB pharma for lectures and courses. Dr. Gaig, Dr. Vilas, Dr. Buongiorno, Dr. Martı, Dr. Garcıa- Gorostiaga, Dr. Aguilar, Dr. Calopa, and Dr.Hernandez-Vara report no disclosures. This does not alter the authors’ adherence to PLOS ONE policies on sharing data and materials.
* Email: [email protected]
. These authors contributed equally to this work.
PLOS ONE | www.plosone.org 1 October 2014 | Volume 9 | Issue 10 | e108982

38
RESULTADOS6
Introduction
Mutations in the leucine-rich repeat kinase 2 gene (LRRK2) arethe most common cause of inherited parkinsonism and account for
a significant proportion of familial and sporadic Parkinson’s
disease (PD) cases [1–2]. The neuropathological substrate in
LRRK2-PD is in some cases quite different from idiopathic PD
(IPD) and ranges from brainstem or diffuse Lewy body pathology,
to nigral degeneration without distinctive histopathology, and to
progressive supranuclear palsy–like pathology. Age at disease onset
and parkinsonian motor features are similar between LRRK2related PD (LRRK2-PD) and idiopathic PD (IPD) [3] but studies
assessing nonmotor symptoms (NMS) in LRRK2-PD patients are
limited and results at times conflicting [4–6]. Dysautonomia, sleep
and mood disturbances as well as other common NMS occurring
in IPD result, in part, from extra-nigral lesions in the brain and the
peripheral autonomic nervous system [7]. The heterogeneous
neuropathology of LRRK2-PD suggests that the range and
severity of extra-nigral NMS could differ from those encountered
in IPD.
The aim of the present study was to evaluate the prevalence and
estimate the onset of NMS in patients with LRRK2 G2019S PD.
Methods
SubjectsA sample of 1251 PD patients from two regions of Spain,
Catalonia (Hospital Clınic de Barcelona, Hospital Mutua de
Terrassa, Hospital Vall d’Hebron and Hospital de Bellvitge) and
Cantabria (Hospital Marques de Valdecilla, Santander) was
screened for LRRK2 G2019S and codon 1441 (R1441G/C/H)
mutations as previously described [3]. PD was diagnosed
according to UK Parkinson’s Disease Society criteria [8]. LRRK2
G2019S carriers were proposed to participate in this study.
LRRK2-PD patients that met diagnostic criteria for dementia in
PD (PDD) [9] were excluded, to avoid interference of cognitive
impairment in the evaluation of NMS. A group of 33 IPD patients
were recruited as controls among those from the initial sample of
1180 patients that tested negative for LRRK2 mutations. We
selected prospectively on a case by case basis those patients who
matched to the LRRK2 subjects for age, gender, duration of
parkinsonism (from onset of motor symptoms, OMS) and disease
severity (Hoehn and Yahr (H-Y) stage), agreed to participate in the
study, did not fulfil criteria for PDD [9], and had not family
history for PD. We also studied age and gender matched healthy
subjects (HS) without PD, dementia, any other neurological
disorder or a positive family history for PD. Patients, their relatives
as well as medical staff of participating centre recruited volunteers
from their personal relations who were screened for exclusion
criteria and were enrolled as controls for this study. The study was
approved by the Hospital Clinic of Barcelona ethics committee
and the written informed consent was obtained from all study
subjects.
Parkinsonism evaluationInformation about motor symptoms (rest tremor, bradykinesia,
rigidity, postural instability and persistent asymmetry), as well as
development of levodopa-induced motor complications, freezing
of gait and repeated falls during the disease course, was collected
by means of a structured clinical interview. All patients were
assessed through the Unified Parkinson’s Disease Rating Scale
(UPDRS), Schwab & England scale and H-Y stage in On
condition. Medications at the time of the evaluation were also
recorded and levodopa equivalent daily dose (LEDD) calculated
[10].
Nonmotor symptoms evaluationThe presence of the following NMS was assessed: hyposmia;
neuropsychiatric disorders: depression, anxiety, hallucinations andpsychosis; dysautonomic symptoms: constipation and urinary
dysfunction; and sleep disturbances: REM Sleep Behaviour
Disorder (RBD), excessive daytime sleepiness (EDS) and insomnia.
A structured clinical interview was conducted to determine the
presence of each NMS at the time of the evaluation. When a NMS
was present, we asked the patient to estimate when it had been
developed in relation to the OMS (e.g. before, concurrently or
after). Each NMS was also evaluated by using several self-
administered tests. Information on the current use of medications,
such as laxatives, hypnotics or antidepressants to treat some of
these NMS, was also collected.
Smell loss was assessed by asking to the subjects whether they
experienced a loss or change in their ability to smell. The 40-items
University of Pennsylvania Smell Identification Test (UPSIT;
Smell Identification TestTM Sensonics, Spanish version) [11] was
administered. Factors that could impair odor identification, such
as active smoking habit, past-history of significant traumatic head
injury or rhinologic disorders, were also considered. UPSIT scores
obtained previously from 148 HS aged 30 to 85 year-old were used
for comparison with LRRK2-PD and IPD. Since odor identifica-
tion has been shown to decline with age and is better in females
than in males [11–12], these 148 HS were stratified by age (,50
years, n = 36; 50–69 years, n = 76; and $70, n= 36) and gender
(males, n = 73; females, n = 75). Mean and standard deviation (SD)
UPSIT score for each age-gender HS subgroup was calculated.
Hyposmia was considered to be present if the UPSIT score was
lower than the mean–2SD corresponding to the age-gender
matched HS subgroup.
Presence of depression and anxiety at the time of this study were
diagnosed according to DSM-IV criteria [13]. In addition, a
previous history of depression or anxiety was also recorded. The
Hospital Anxiety and Depression scale (HADS) [14] was used to
quantify the symptoms. To assess the presence of hallucinations
and psychosis the NINS-NIMH work group criteria for psychosis
in PD [15] and the Parkinsonian Psychosis Rating Scale (PPRS)
were used [16].
Constipation was diagnosed according to the Rome criteria
[17]. Bowel movements frequency was evaluated. The Bristol
Scale Stool was used to assess whole gut transit time [18]. Urinarydysfunction was assessed by asking for long-lasting complaints of
urinary urgency, frequency, incontinence or incomplete emptying.
The SCOPA-AUT was administered [19].
RBD was considered to be present when a history of
problematic sleep behaviors that were potentially harmful,
disrupted sleep continuity or was annoying to self or bed partner
was present [20]. EDS occurred when the subject could fall asleep
at least twice a day and the total sleeping time during the daytime
was more than 1 hour [21] and insomnia when there were long-
lasting complaints of difficulty in initiating or maintaining sleep.
The Pittsburgh sleep quality index (PSQI), the Epworth sleepiness
scale (ESS) and the Parkinson’s disease sleep scale (PDSS) were
administered [22–24].
Statistical analyses. Categorical variables and the frequency
of each NMS in the different groups were assessed by using the
Chi-square test or the Fisher’s exact test when appropriated. For
continuous variables, the Kruskal-Wallis analysis and the Mann-
Whitney U test were used to compare the means of groups for
Nonmotor Symptoms in LRRK2 Parkinson’s Disease
PLOS ONE | www.plosone.org 2 October 2014 | Volume 9 | Issue 10 | e108982

39
RESULTADOS 6
multiple comparisons and in pairs, respectively. To determine
whether there was a relationship between each NMS and other
variables, the Spearman correlation coefficient was obtained. A
significance level of ,0.05 was used. P-values were also calculated
using the false discovery rate (FDR) correction for multiple
comparisons. The statistical analyses were performed using
commercially available software (SPSS, Version18.0).
Results
General demographic data and parkinsonian motorsymptomsAmong 66 PD patients identified as LRRK2 G2019S carriers,
only 33 were included in the study (22 from Barcelona and 11
from Santander). One LRRK2-PD patient was excluded because
of severe dementia. Of the remaining 32 non-participants, 10
declined to participate, 11 had died when the study was initiated
and 11 had been lost for follow up. Thirty-three IPD patients and
33 HS (22 from Barcelona and 11 from Santander in each group)
were included. Mean age was not statistically different between
LRRK2-PD, IPD and HS (Table 1). Family history for PD was
positive in 20 (60.6%) of LRRK2-PD patients. There were no
significant differences in the features of motor symptoms, or in
dopamine replacement treatment (Table 1).
Nonmotor symptomsOlfaction. Awareness of smell loss occurred in a similar
frequency in both LRRK2-PD and IPD patients (54.5% vs 63.6%;
p= 0.45; Table 2) and more frequently than in HS. Mean UPSIT
scores, though, were significantly different among the three
groups. LRRK2-PD patients had a mean UPSIT score signifi-
cantly higher than IPD patients (23.566.8 vs 18.466.0; p= 0.002)
and lower than HS (29.564.3; p= 0.001) (Figure 1. A). Hyposmia
was present in 13 (39.4%) of G2019S carriers, significantly lower
than in IPD (25 (75.8%); p = 0.01) (Table 2). No significant
differences were found in the frequency of active smoking,
rhinologic pathology or history of head trauma between groups.
Mean UPSIT score in LRRK2-PD cases was significantly
higher in females than in males (26.964.7 vs 19.466.8, p,0.01;
Figure 1.B). Hyposmia was present in only 3 (16.7%) LRRK2-PD
females, in contrast to 10 (66.7%) LRRK2-PD males. Such
significant difference in UPSIT scores by gender was not observed
in IPD patients (18.665.8 males vs 18.266.3 females; p = 0.66) or
HS (28.164.9 males vs 30.763.4 females; p = 0.10). LRRK2-PDfemales were significantly older than LRRK2-PD males (67.868.9
vs 61.1613.3; p = 0.04), but disease duration or severity, and
frequency of active smoking, rhinologic pathology or history of
head trauma, were similar in both genders. Mean UPSIT score in
LRRK2-PD females was significantly higher than in IPD females
(p,0.01) and significantly lower than in HS females (p = 0.01). In
contrast, mean UPSIT score in LRRK2-PD males was similar to
Table 1. General demographic data and parkinsonian motor symptoms in patients with LRRK2 G2019S associated Parkinson’sdisease, idiopathic Parkinson’s disease and healthy subjects.
LRRK2 PD (n=33) IPD (n=33) HS (n=33) P
Age (years)1 64.8611.4 65.1610.0 64.8610.2 0.99"
Sex (male, %) 15 (45.4%) 15 (45.4%) 15 (45.4%) 1.0#
Disease duration (years)1 9.265.7 (2–28) 9.066.1 (1–30) 0.791
Motor symptoms during disease course; n (%)
Rest tremor 29 (87.9%) 27 (81.8%) 0.49#
Action tremor 20 (60.6%) 23 (69.7%) 0.44#
Bradykinesia 33 (100%) 33 (100%) 1.06
Postural instability 16 (48.5%) 11 (33.3%) 0.21#
Repeated falls 9 (27.3%) 7 (21.2%) 0.57#
Freezing of gait 18 (54.6%) 14 (42.4%) 0.32#
Persistent Asymmetry 31 (93.9%) 31 (93.9%) 1.06
Fluctuations 18 (54.5%) 17 (51.5%) 0.80#
Dyskinesias 19 (57.6%) 16 (48.5%) 0.46#
UPDRS part II1 10.367.5 (0–26) 8.364.9 (0–24) 0.481
UPDRS part III1 24.0614.0 (0–62) 19.9612.2 (2–62) 0.161
UPDRS part IVA+IVB1 3.2163.7 (0–13) 2.062.7 (0–10) 0.181
Hoehn & Yahr stage1 2.161.0 (1–4) 1.860.8 (1–4) 0.241
Schwab & England1 82.1614.7 (50–100) 85.8610.3 (60–100) 0.441
Treatment with levodopa; n (%) 31 (93.9%) 30 (90.9%) 1.06
Treatment with dopamine agonists; n (%) 27 (81.8%) 25 (75.8%) 0.55#
Levodopa equivalent daily dose (in mg)1 793.76482.1 (105–2744) 823.06516.4 (0–1770) 0.771
LRRK2 G2019S PD: LRRK2 G2019S related Parkinson’s disease; IPD: Idiopathic Parkinson’s disease; HS: healthy subjects.1Mean 6 Standard deviation (Range)."Kruskal-Wallis analysis;1Mann-Whitney U test;#Chi-square test;6Fisher’s exact test.doi:10.1371/journal.pone.0108982.t001
Nonmotor Symptoms in LRRK2 Parkinson’s Disease
PLOS ONE | www.plosone.org 3 October 2014 | Volume 9 | Issue 10 | e108982

40
RESULTADOS6
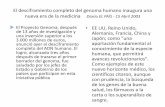
Figure 1. University of Pennsylvania Smell Identification Test (UPSIT) scores. UPSIT scores in LRRK2 G2019S Parkinson’s disease patients,idiopathic Parkinson’s disease patients and healthy controls (Figure 1.A). UPSIT score in each group separated by sex (Figure 1.B). Circles representindividual values, while the bar refers to the mean UPSIT score in each group. IPD: idiopathic Parkinson’s disease; LRRK2-PD: LRRK2 associatedParkinson’s disease, HS: healthy subjects.doi:10.1371/journal.pone.0108982.g001
Nonmotor Symptoms in LRRK2 Parkinson’s Disease
PLOS ONE | www.plosone.org 4 October 2014 | Volume 9 | Issue 10 | e108982

41
RESULTADOS 6
Table
2.Nonmotorsymptomsin
patients
withLRRK2G2019SassociatedParkinson’sdisease,idiopathic
Parkinson’sdiseasean
dhealthysubjects.
LRRK2-PD
(n=33)
IPD
(n=33)
Controls
(n=33)
Threegro
ups
compariso
nFDRp
LRRK2vsIPD
LRRK2vsco
ntrols
IPD
vsco
ntrols
Changein
smellse
nse
18(54.5%)
21(63.6%)
5(15.2%)
0.021*#
0.055
0.45#
0.02*#
0.007*#
UPSIT
Sco
re1
23.566.8
18.466.0
29.564.3
0.001"
0.007
0.0021
0.0011
0.0011
Hyposm
ia2
13(39.4%)
25(75.8%)
1(3.0%)
0.001*#
0.007
0.01#
0.003*#
0.001*#
Histo
ryofdepression
19(57.6%)
12(36.4%)
4(12.1%)
0.024*#
0.055
0.08#
0.006*#
0.02*#
Activedepression
6/19(31.5%)
8/12(66.6%)
1/4
(25.0%)
0.445#
0.703
Antidepressivetreatm
ent
5/19(26.3%)
9/12(75.0%)
1/4
(25.0%)
0.24#
0.45
Histo
ryofanxiety
8(24.2%)
9(27.3%)
5(15.2%)
0.609#
0.794
Currentactiveanxiety
2/8
(25.0%)
6/9
(66.7%)
3/5
(60.0%)
0.559#
0.772
Treatm
entforanxiety
3/8
(37.5%)
2/9
(22.2%)
3/5
(60.0%)
0.642#
0.802
HADSto
tal
10.465.5
10.166.6
8.065.6
0.26"
0.459
HADSdepression
5.262.7
5.063.9
3.062.9
0.001*"
0.007
0.541
0.001*1
0.02*1
HADSanxiety
4.963.6
5.163.8
5.063.5
0.98"
0.985
Hallucinations
3(9%)
5(15%)
NA
0.406
PPRSscore
10.360.5
0.560.9
0.03617
0.018*"
0.055
0.541
0.012*1
0.001*1
Constipation
10(30.3%)
13(39.4%)
9(27.3%)
0.74#
0.853
Bowelmovement(w
eek)
16.562.7
5.661.7
6.562.0
0.13"
0.278
Bristolscale
13.561.1
2.960.9
3.861.1
0.002*"
0.012
0.03*1
0.281
0.001*1
Urinary
dysfunction
17(51.5%)
15(45.5%)
8(24.2%)
0.283#
0.472
SCOPA-A
UT1
16.468.7
13.568.5
10.565.8
0.02*"
0.055
0.171
0.001*1
0.141
G-I
4.363.4
4.163.5
2.162.3
0.024*"
0.055
0.831
0.161
0.02*
1
Urinary
6.464.8
5.463.8
4.963.2
0.56"
0.077
RBD
sympto
ms
7(21.2%)
14(42.4%)
1(3.0%)
0.008*#
0.03
0.11#
0.054#
0.01*
#
Inso
mnia
22(66.7%)
19(57.6%)
20(60.6%)
0.932#
0.985
EDS
6(18.2%)
13(39.4%)
00.003*#
0.013
0.057#
0.02*#
0.001*#
GlobalPSQI1
7.365.4
6.764.8
5.264.7
0.16"
0.32
TotalPDSS1
116.4616.8
116.7622.3
130.163.4
0.001*"
0.007
0.721
0.001*1
0.02*1
ESSSco
re1
8.164.6
9.165.3
5.662.8
0.003*"
0.013
0.461
0.02*1
0.001*1
LRRK2G2019SPD:LRRK2G2019S-relatedParkinson’sdisease;IPD:Idiopathic
Parkinson’sdisease;HS:
healthysubjects.G-I:Gastro-intestinal;RBD:REM
behaviordisorder;ED
S:excessivedaytimesleepiness.
#Chi-squaretest;
6Fisher’sexact
test;
"Kruskal-W
allis
analysis;
1Man
n-W
hitneyUtest;
*Statistically
significan
t:P,0.05;
1Mean
6Stan
darddeviation(Ran
ge);
2Hyp
osm
iawas
arbitrarily
definedas
anUPSITscore
lowerthan
themean
–2SD
UPSITscore
obtainedin
asubsetofhealthysubjectsofthesamegenderan
dsimilarag
e.
doi:10.1371/journal.pone.0108982.t002
Nonmotor Symptoms in LRRK2 Parkinson’s Disease
PLOS ONE | www.plosone.org 5 October 2014 | Volume 9 | Issue 10 | e108982

42
RESULTADOS6
IPD males (p = 0.71), and significantly lower than in HS males (p,0.01). No correlation was found between UPSIT score and disease
duration or severity in LRRK2-PD or IPD patients.
Neuropsychiatric symptoms. Current active depression
and current treatment with antidepressive drugs were more
frequent in IPD than in LRRK2-PD, but these differences were
not statistically significant (Table 2). There were no differences in
the frequency of anxiety disorder between LRRK2-PD, IPD and
HS. Nine IPD patients were under antidepressive treatment but
only 8 had active depression. Similarly, 3 LRRK2-PD patients
were under anxiety treatment but only 2 had active anxiety. These
patients were treated with antidepressants and benzodiazepines
because of past history of depression and anxiety despite
improvement of symptoms. The HADS subscore for depression
was similar between LRRK2-PD and IPD, but higher than HS.
The HADS subscore for anxiety was similar between groups
(Table 2). Hallucinations occurred in similar frequency in
LRRK2-PD and IPD. In all LRRK2 and IPD patients,
hallucinations were visual in nature. Delusions or severe psychosis
did not occur in any LRRK2-PD nor IPD patient.
Dysautonomic symptoms. No significant differences were
found in the presence of constipation between LRRK2-PD, IPD
and HS groups (Table 2). Mean Bristol scale stool score was
significantly higher in LRRK2-PD than in IPD (Table 2). Mean
SCOPA-AUT subscore for gastro-intestinal dysfunction was
similar in LRRK2-PD and IPD. IPD patients, but not LRRK2-PD patients, showed mean SCOPA-AUT subscore for gastro-
intestinal dysfunction significantly higher compared to HS. The
presence of urinary dysfunction was not statistically different
between three groups. No differences in mean SCOPA-AUT
subscore for urinary dysfunction was identified among the three
groups (Table 2).
Sleep disturbances. A trend to an increased frequency of
RBD symptoms in IPD compared to LRRK2-PD was found.
Frequency of insomnia and use of hypnotics were similar among
the three groups. IPD patients had a borderline increased
frequency of EDS compared to LRRK2-PD (Table 2). Mean
Global PSQI, total PDSS and EDSS scores were not significantly
different between LRRK2-PD and IPD. LRRK2-PD and IPD
patients had a mean Global PSQI score that was not significantly
different from HS. In contrast, LRRK2-PD and IPD patients
showed a mean total PDSS significantly lower than HS. Mean
ESS score in LRRK2 and IPD were significantly higher compared
to HS (Table 2).
Estimated onset of NMS in LRRK2-PDLRRK2-PD patients frequently reported that several NMS
occurred before OMS (table 3). Smell loss, depression, constipa-
tion and EDS were reported to develop before OMS in more than
40% of the LRRK2-PD patients in whom these symptoms were
present at the time of examination. Smell loss and depression were
reported to occur at variable time intervals before OMS but
constipation and EDS frequently were estimated to occur more
than 10 years before OMS in most LRRK2-PD (Table 3). In
LRRK2-PD subjects, RBD was reported to occur usually
coincidentally or after OMS. In IPD patients smell loss, depression
and constipation were also reported to appear before OMS, but
EDS and RBD were reported to appear coincidentally or after
OMS in most cases. Anxiety symptoms were reported coinciden-
tally or developing after OMS in most LRRK2-PD cases but more
frequently before OMS in IPD.
Discussion
Our study shows that NMS occur frequently in LRRK2G2019S PD patients, in a frequency similar to a group of IPD
subjects of similar disease duration, severity of motor symptoms,
and dopaminergic treatment. The only NMS that significantly
differed between LRRK2-PD and IPD was smell loss. While
reported awareness of smell loss occurred as frequently in LRRK2-PD as in IPD, UPSIT scores were significantly higher in LRRK2-PD. Hyposmia was present in only 39% of our LRRK2-PDpatients, in contrast to 75% of IPD patients. Also in other studies
the prevalence of abnormal olfaction in LRRK2-PD has been
found to range from 36 to 49%, significantly inferior to IPD (75–
81%) [5].
Reasons for the differences in smell between LRRK2-PD and
IPD encountered in this and other studies remain unclear.
Heterogeneous pathology or less severe involvement of olfactory
structures in LRRK2-PD has been proposed to explain such
differences. In Parkin gene associated PD, absence of smell loss is
common [25] and neuropathological changes are usually limited
to the substantia nigra without LB pathology [26]. One study
involving four LRRK2-PD brains, reported a-synuclein accumu-
lation in the olfactory bulb, olfactory tract, and primary olfactory
cortex providing a pathophysiologic substrate for olfactory deficit6.
Still only 20% of LRRK2 G2019S cases are thought to present
different pathology to that seen in IPD [27], and therefore
neuropathological heterogeneity may not adequately explain the
preservation of the olfactory sense in most LRRK2 patients.
In contrast to previous studies, we found that smell was
particularly preserved in G2019S LRRK2-PD females. Such
difference could suggest a gender effect in the expression of
LRRK2-PD. Gender-related susceptibility factors likely play a role
in PD, a disorder more common in males [28] and female
predominance has been suggested to occur in G2019S LRRK2-PD [29]. One study has also reported an earlier age at disease
onset in women than in men with the G2019S mutation [4].
Neuropsychiatric disorders, dysautonomic symptoms and sleep
disturbances were frequent in LRRK2 G2019S carriers, similarly
to that observed in IPD. Depression, anxiety and hallucinations
were present in our LRRK2 patients at a frequency similar to that
reported in the literature [4,30,31]. Sleep disturbances like RBD,
insomnia and EDS are common in PD and have been reported to
be present frequently in patients carrying the G2019S mutation.
The frequency of RBD symptoms tended to be lower in LRRK2-PD cases than in IPD, although the difference was not statistically
significant. The prevalence of RBD in IPD reported in the
literature varies from 15% to 46% [32]. A recent study has
reported RBD symptoms in only 11% of the LRRK2-PD patients,
compared to 42% of IPD patients [33], suggesting that RBD could
be less frequently present in LRRK2-PD. Frequency of constipa-
tion and urinary dysfunction in our LRRK2 patients was similar to
that reported by others [5,31,33]. In our study the frequency of
constipation was similar between LRRK2 and IPD, but mean
Bristol scale stool score was significantly lower in LRRK2-PD than
in IPD, suggesting that intestinal motility could be less impaired in
LRRK2-PD.
A substantial proportion of our LRRK2-PD patients reported
that several NMS, such as hyposmia, depression, constipation, or
EDS, had been present before OMS. Some NMS have been
evaluated in a limited number of asymptomatic subjects carrying
the LRRK2 G2019S mutation [6,31,34] and hyposmia, depres-
sion and constipation have been found to occur in some non-
manifesting carriers [31,34], although some of these premotor
features were found to be no more frequent in non-manifesting
Nonmotor Symptoms in LRRK2 Parkinson’s Disease
PLOS ONE | www.plosone.org 6 October 2014 | Volume 9 | Issue 10 | e108982

43
RESULTADOS 6
Table 3. Estimated presence of nonmotor symptoms in LRRK2 G2019S Parkinson’s disease patients and idiopathic Parkinson’sdisease patients in relation to onset of motor symptoms.
LRRK2-PD IPD
Loss or change in smell sense; n 18 21
Coincidentally or after OMS (n;%) 8 (44.4%) 8 (38.1%)
Before OMS (n;%) 8 (44.4%) 8 (38.1%)
More than 10 yrs before OMS 2/8 (25%) 4/8 (50%)
Within 10 yrs before OMS 4/8 (50%) 2/8 (25%)
Within 2 yrs before OMS 2/8 (25%) 2/8 (25%)
Unknown 2 (11.1%) 5 (23.8%)
Depression; n 19 12
Coincidentally or after OMS (n;%) 11 (57.9%) 7 (58.3%)
Before OMS (n;%) 8 (42.1%) 5 (41.7%)
More than 10 yrs before OMS 2/8 (25%) 2/5 (40%)
Within 10 yrs before OMS 3/8 (37.5%) 2/5 (40%)
Within 2 yrs before OMS 3/8 (37.5%) 1/5 (20%)
Anxiety symptoms; n 8 9
Coincidentally or after OMS (n;%) 6 (75%) 1 (11.1%)
Before OMS (n;%) 2 (25%) 8 (88.9%)
More than 10 yrs before OMS 0 5/8 (62.5%)
Within 10 yrs before OMS 0 3/8 (37.5%)
Within 2 yrs before OMS 2/2 (100%) 0
Constipation; n 14 15
Coincidentally or after OMS (n;%) 5 (35.7%) 8 (53.3%)
Before OMS (n;%) 9 (64.3%) 7 (46.7%)
More than 10 yrs before OMS 8/9 (88.9%) 7/7 (100%)
Within 10 yrs before OMS 1/9 (11.1%) 0
Within 2 yrs before OMS 0 0
Urinary dysfunction; n 17 15
Coincidentally or after OMS (n;%) 12 (70.6%) 12 (80%)
Before OMS (n;%) 5 (29.4%) 3 (20%)
More than 10 yrs before OMS 0 0
Within 10 yrs before OMS 1/5 (20%) 1/3 (33.3%)
Within 2 yrs before OMS 4/5 (80%) 2/3 (66.6%)
RBD symptoms; n 7 14
Coincidentally or after OMS (n;%) 5 (71.4%) 12 (85.7%)
Before OMS (n;%) 2 (28.6%) 2 (14.3%)
More than 10 yrs before OMS 0 0
Within 10 yrs before OMS K (50%) 0/2 (0.0%)
Within 2 yrs before OMS K (50%) 2/2 (100%)
Insomnia; n 19 22
Coincidentally or after OMS (n;%) 16 (84.2%) 14 (63.6%)
Before OMS (n;%) 3 (15.8%) 8 (36.4%)
More than 10 yrs before OMS 2/3 (66.6%) 6/8 (75%)
Within 10 yrs before OMS 0 0
Within 2 yrs before OMS 1/3 (33.3%) 2/8 (25%)
EDS; n 6 13
Coincidentally or after OMS (n;%) 3 (50%) 12 (92.3%)
Before OMS (n;%) 3 (50%) 1 (7.7%)
More than 10 yrs before OMS 2/3 (66.6%) 1/1 (100%)
Within 10 yrs before OMS 1/3 (33.3%) 0
Within 2 yrs before OMS 0 0
Nonmotor Symptoms in LRRK2 Parkinson’s Disease
PLOS ONE | www.plosone.org 7 October 2014 | Volume 9 | Issue 10 | e108982

44
RESULTADOS6
carriers than in non-carriers. The presence of these symptoms in
the premotor phase, as in the case of IPD, suggests that the
neuropathological changes occur probably in non-dopaminergic
brainstem and peripheral nervous system structures before the
involvement of the substantia nigra, as suggested by Braak [35].
Some limitations of our study should be mentioned. Some
results are based on patient’s responses. More information could
be obtained with objective tests, as occurred in smell evaluation,
where no differences were identified when asked for a loss or
change in smell, while the UPSIT was able to detect significant
differences. Also since the mean disease duration was 9 years, we
acknowledge that the patient’s responses in regards to symptoms
occurring in the presymptomatic phase may not be accurate,but
others studies have reported NMS such as these occurring in the
premotor phase of LRRK2-PD [6,30]. Future prospective studies
in asymptomatic LRRK2 G2019S carriers should clarify this issue.
Finally, cognitive dysfunction which is among the most relevant
and disabling NMS in PD, was not assessed in detail in our study,
but only one patient was excluded for the study because of
dementia. Some studies have suggested that the frequency of
dementia could be lower than usually reported in IPD [5,36].
Cognitive dysfunction in LRRK2 patients deserves additional and
specifically designed studies. One strength of our study, in contrast
to previous ones that usually assessed one or only a few NMS,
include the evaluation of several NMS in the same group of
patients which has given a more global impression of the
contribution of NMS to the clinical picture of LRRK2 associated
PD. In addition, our study includes similar NMS assessments in a
group of healthy subjects for comparison purposes.
In summary, neuropsychiatric, dysautonomic and sleep distur-
bances are equally frequent in non-demented LRRK2 G2019S PD
and IPD. Olfactory dysfunction, however, occurs less often in
LRRK2 G2019S PD, maybe reflecting less involvement of
olfactory structures by the neurodegenerative process. Smell
function seems to be particularly preserved in females with the
G2019S mutation, suggesting a gender effect in the expression of
some LRRK2-PD symptoms. Some NMS may antedate the onset
of PD motor syndrome in substantial number of patients carrying
LRRK2 G2019S mutation, indicating that a premotor phase
similar to that occurring in IPD probably occurs in this genetic
form of PD, and that common physiopathological mechanism
probably underlie the onset and progression of the disease in both
LRRK2 G2019S PD and IPD.
Acknowledgments
The authors are grateful to the patients and the families that participated in
this study.
Author Contributions
Conceived and designed the experiments: CG DV ET. Performed the
experiments: CG DV JI MS IG MAMC JH. Analyzed the data: CG DV JI
MS IG ME MB MM FV ET. Contributed reagents/materials/analysis
tools: CG DV JI MS IG ME MB MM FV ET. Contributed to the writing
of the manuscript: CG DV ET.
References
1. Paisan Ruız C, Jain S, Evans EW, Gilks WP, Simon J, et al. (2004) Cloning of
the gene containing mutations that cause PARK8-linked Parkinson’s disease.
Neuron 44(4): 595–600.
2. Gilks WP, Abou Sleiman PM, Gandhi S, Jain S, Singleton A, et al. (2005) A
common LRRK2 mutation in idiopathic Parkinson’s disease. Lancet 365: 415–
6.
3. Gaig C, Ezquerra M, Marti MJ, Munoz E, Valldeoriola F, et al. (2006) LRRK2
mutations in Spanish patients with Parkinson disease: frequency, clinical
features, and incomplete penetrance. Arch Neurol 63: 377–82.
4. Goldwurm S, Zini M, Di Fonzo A, De Gaspari D, Siri C, et al. (2006) LRRK2
G2019S mutation and Parkinson’s disease: a clinical, neuropsychological and
neuropsychiatric study in a large Italian sample. Parkinsonism Relat Disord 12:
410–9.
5. Healy DG, Falchi M, O’Sullivan SS, Bonifati V, Durr A, et al. (2008)
Phenotype, genotype, and worldwide genetic penetrance of LRRK2-associated
Parkinson’s disease: a case-control study. Lancet Neurol 7: 583–90.
6. Silveira Moriyama L, Guedes LC, Kingsbury A, Ayling H, Shaw K, et al. (2008)
Hyposmia in G2019S LRRK2-related parkinsonism: clinical and pathologic
data. Neurology 71: 1021–6.
7. Simuni T, Sethi K (2008) Nonmotor manifestations of Parkinson’s disease. Ann
Neurol 64: S65–80.
8. Hughes AJ, Daniel SE, Kilford L, Lees AJ (1992) Accuracy of clinical diagnosis
of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases.
J Neurol Neurosurg Psychiatry 55: 181–4.
9. Emre M, Aarsland D, Brown R, Burn DJ, Duyckaerts C, et al. (2007) Clinical
diagnostic criteria for dementia associated with Parkinson’s disease. Mov Disord
22: 1689–707.
10. Moller JC, Korner Y, Dodel RC, Meindorfner C, Stiasny Kolster K, et al. (2005)
Pharmacotherapy of Parkinson’s disease in Germany. J Neurol 252: 926–35.
11. Doty RL, Bromley SM, Stern MB (1995) Olfactory testing as an aid in the
diagnosis of Parkinson’s disease: development of optimal discrimination criteria.
Neurodegeneration 4: 93–7.
12. Doty RL, Shaman P, Applebaum SL, Giberson R, Siksorski L, et al. (1984)
Smell identification ability: changes with age. Science 226: 1441–3.
13. Washington (1994) American Psychiatric Association. Diagnostic and statistical
manual of mental disorders: DSM-IV.
14. Zigmond AS, Snaith RP (1983) The hospital anxiety and depression scale. Acta
Psychiatr Scand 67: 361–70.
15. Ravina B, Marder K, Fernandez HH, Friedman JH, McDonald W, et al. (2007)
Diagnostic criteria for psychosis in Parkinson’s disease: report of an NINDS,
NIMH work group. Mov Disord 22: 1061–8.
16. Friedberg G, Zoldan J, Weizman A, Melamed E (1998) Parkinson Psychosis
Rating Scale: a practical instrument for grading psychosis in Parkinson’s disease.
Clin Neuropharmacol 21: 280–4.
17. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, et al.
(2006) Functional bowel disorders. Gastroenterology 130: 1480–91.
18. Riegler G, Esposito I (2001) Bristol scale stool form. A still valid help in medical
practice and clinical research. Tech Coloproctol 5: 163–4.
19. Visser M, Marinus J, Stiggelbout AM, Van Hilten JJ (2004) Assessment of
autonomic dysfunction in Parkinson’s disease: the SCOPA-AUT. Mov Disord
19: 1306–12.
20. Medicine AASM (2005) International Classification of Sleep Disorders- Second
Edition.
21. Gjerstad MD, Aarsland D, Larsen JP (2002) Development of daytime
somnolence over time in Parkinson’s disease. Neurology 58: 1544–6.
22. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ (1989) The
Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and
research. Psychiatry Res 28: 193–213.
23. Johns MW (1991) A new method for measuring daytime sleepiness: the Epworth
sleepiness scale. Sleep 14: 540–5.
24. Chaudhuri KR, Pal S, DiMarco A, Whately Smith C, Bridgman K, et al. (2002)
The Parkinson’s disease sleep scale: a new instrument for assessing sleep and
nocturnal disability in Parkinson’s disease. J Neurol Neurosurg Psychiatry 73:
629–35.
25. Khan NL, Katzenschlager R, Watt H, Bhatia KP, Wood NW, et al. (2004)
Olfaction differentiates parkin disease from early-onset parkinsonism and
Parkinson disease. Neurology 62: 1224–6.
26. Hayashi S, Wakabayashi K, Ishikawa A, Nagai H, Saito M, et al. (2000) An
autopsy case of autosomal-recessive juvenile parkinsonism with a homozygous
exon 4 deletion in the parkin gene. Mov Disord 15: 884–8.
27. Poulopoulos M, Levy OA, Alcalay RN (2012) The neuropathology of genetic
Parkinson’s disease. Mov Disord 27: 831–42.
28. Wooten GF, Currie LJ, Bovbjerg VE, Lee JK, Patrie J (2004) Are men at greater
risk for Parkinson’s disease than women? J Neurol Neurosurg Psychiatry 75:
637–9.
LRRK2 G2019S PD: LRRK2 G2019S related Parkinson’s disease; IPD: Idiopathic Parkinson’s disease, OMS: onset of motor symptoms, RBD: REM sleep behavior disorder,EDS: excessive daytime sleepiness.doi:10.1371/journal.pone.0108982.t003
Nonmotor Symptoms in LRRK2 Parkinson’s Disease
PLOS ONE | www.plosone.org 8 October 2014 | Volume 9 | Issue 10 | e108982

45
RESULTADOS 6
29. Orr Urtreger A, Shifrin C, Rozovski U, Rosner S, Bercovich D, et al. (2007) The
LRRK2 G2019S mutation in Ashkenazi Jews with Parkinson disease: is there a
gender effect? Neurology 69: 1595–602.
30. Kasten M, Kertelge L, Bruggemann N, van der Vegt J, Schmidt A, et al. (2010)
Nonmotor symptoms in genetic Parkinson disease. Arch Neurol 67: 670–6.
31. Marras C, Schule B, Munhoz RP, Rogaeva E, Langston JW, et al. (2011)
Phenotype in parkinsonian and nonparkinsonian LRRK2 G2019S mutation
carriers. Neurology 77: 325–33.
32. Iranzo A, Santamaria J, Tolosa E (2009) The clinical and pathophysiological
relevance of REM sleep behavior disorder in neurodegenerative diseases. Sleep
Med Rev 13: 385–401.
33. Ruiz Martınez J, Gorostidi A, Goyenechea E, Alzualde A, Poza JJ, et al. (2011)
Olfactory deficits and cardiac 123I–MIBG in Parkinson’s disease related to theLRRK2 R1441G and G2019S mutations. Mov Disord 26: 2026–31.
34. Saunders Pullman R, Stanley K, Wang C, San Luciano M, Shanker V, et al.
(2011) Olfactory dysfunction in LRRK2 G2019S mutation carriers. Neurology77: 319–24.
35. Braak H, Del Tredici K, Rub U, de Vos RA, Jansen Steur EN, et al. (2003)Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol
Aging 24: 197–211.
36. Brockmann K, Groger A, Di Santo A, Liepelt I, Schulte C, et al. (2011) Clinicaland brain imaging characteristics in leucine-rich repeat kinase 2-associated PD
and asymptomatic mutation carriers. Mov Disord 26: 2335–42.
Nonmotor Symptoms in LRRK2 Parkinson’s Disease
PLOS ONE | www.plosone.org 9 October 2014 | Volume 9 | Issue 10 | e108982


47
RESULTADOS 6
Trabajo número 2
Clinical and imaging markers in premotor LRRK2 G2019S mutation carriers
Vilas D, Ispierto L, Álvarez R, Pont-Sunyer C, Martí MJ, Valldeoriola F, Compta Y, de Fabregues O,
Hernández-Vara J, Puente V, Calopa M, Jaumà S, Campdelacreu J, Aguilar M, Quílez P, Casquero P,
Lomeña F, Ríos J, Tolosa E.
Parkinsonism Relat Disord. 2015 Aug 12. pii: S1353-8020(15)00339-9.

48
RESULTADOS6
Marcadores clínicos y de imagen en la fase premotora de los portadores de la
mutación G2019S del gen LRRK2
Introducción: La hiperecogenicidad de la SN se ha propuesto como un marcador de riesgo para
la EP. Los aLRRK2, en riesgo de desarrollar EP, proporcionan una oportunidad para el estudio de
biomarcadores preclínicos. El objetivo de este estudio es evaluar la ecogenicidad de la SN y otros
hallazgos ecográficos en portadores de la mutación G2019S del gen LRRK2 y sus correlaciones
clínicas y con el SPECT con transportador de dopamina (DAT-SPECT).
Métodos: Se realizó una sonografía transcraneal a 26 pacientes con EP G2019S LRRK2, 50 de sus
familiares de primer grado, 31 pacientes con EPI y 26 controles. Se evaluó la ecogenicidad de la SN
y otros hallazgos ecográficos en todos los participantes. Se realizó además un DAT-SPECT a 29 de
los familiares de primer grado.
Resultados: El 75 % de los pacientes con EP-LRRK2 y el 87.5 % de los EPI presentaron hiperecoge-
nicidad de la SN (p = 0.087). Los aLRRK2 presentaron una frecuencia más alta de hiperecogeni-
cidad de la SN que los familiares de primer grado no portadores (58.3 % vs 25 %; p = 0.039) y que
los controles (58.3 % vs 12.5 %; p = 0.002) y una mayor área de ecogenicidad de la SN que los no
portadores (p = 0.003) y que los controles (p < 0.001). El tamaño del tercer ventrículo fue significa-
tivamente menor en la EP-LRRK2 que en la EPI (1.9 mm [1.38; 2.75] vs 3.0 mm [2.3; 5.3]; p = 0.003).
Cuatro de los 5 (80 %) aLRRK2 con una DAT-SPECT anormal y 4 de los 5 (80 %) con trastorno de
conducta del sueño REM tenían también hiperecogenididad de la SN.
Conclusión: La hiperecogenicidad de la SN es frecuente en la EP asociada a la mutación G2019S
del gen LRRK2 y en los aLRRK2. La mayoría de aLRRK2 con un posible marcador subrogado de EP
como un DAT-SPECT anormal o con trastorno de conducta del sueño REM presentan también
hiperecogenicidad de la SN, lo que apoya que este hallazgo ecográfico puede ser un marcador
de EP en esta población asintomática.

49
RESULTADOS 6
Clinical and imaging markers in premotor LRRK2 G2019S mutationcarriers
Dolores Vilas a, Lourdes Ispierto d, Ramiro �Alvarez d, Claustre Pont-Sunyer a,María Jos�e Martí a, b, c, Francesc Valldeoriola a, b, c, Yaroslau Compta a, b, c,Oriol de Fabregues e, Jorge Hern�andez-Vara e, Víctor Puente f, Matilde Calopa g,Serge Jaum�a g, Jaume Campdelacreu g, Miquel Aguilar h, Pilar Quílez h, Pilar Casquero i,Francisco Lome~na j, Jos�e Ríos k, l, Eduardo Tolosa a, b, c, *
a Parkinson's Disease and Movement Disorders Unit, Neurology Service, Institut de Neuroci�encies Hospital Clínic, University of Barcelona, Catalonia, Spainb Institut d'investigacions Biom�ediques August Pi i Sunyer (IDIBAPS), Barcelona, Catalonia, Spainc Centro de Investigaci�on Biom�edica en Red de Enfermedades Neurodegenerativas (CIBERNED), Spaind Neurology Service, Hospital Universitari Germans Trias I Pujol, Badalona, Spaine Neurology Service, Hospital Universitari Vall D'Hebron, Barcelona, Catalonia, Spainf Neurology Service, Hospital Del Mar, Barcelona, Catalonia, Spaing Neurology Service, Hospital Universitari de Bellvitge, Barcelona, Catalonia, Spainh Neurology Service, Hospital Universitari Mutua de Terrasa, Barcelona, Catalonia, Spaini Hospital Mateu Orfila, Ma�o, Menorca, Spainj Nuclear Medicine Service, Hospital Clinic, University of Barcelona, Barcelona, Catalonia, Spaink Biostatistics and Data Management Core Facility, IDIBAPS, (Hospital Clinic), Barcelona, Spainl Biostatistics Unit, Faculty of Medicine, Universitat Aut�onoma de Barcelona, Catalonia, Spain
a r t i c l e i n f o
Article history:Received 3 April 2015Received in revised form4 August 2015Accepted 10 August 2015
Keywords:ParkinsonLRRK2GeneticTranscranial ultrasoundSubstantia nigra
a b s t r a c t
Background: Substantia nigra hyperechogenicity (SNþ) has been proposed as a risk marker of Parkin-son's disease (PD). Asymptomatic LRRK2 mutation carriers (aLRRK2þ), at high risk for developing PD,provide an opportunity for the study of preclinical biomarkers.Objective: To assess SN echogenicity and other echographic features in LRRK2 G2019S carriers and theirclinical and imaging correlates.Methods: Transcranial sonography was performed in 26 LRRK2 G2019S PD patients, 50 first-degreerelatives, 31 idiopathic PD (IPD) patients and 26 controls. SN echogenicity and other echographic fea-tures were assessed in all study subjects. Dopamine transporter imaging (DAT-SPECT) was performed in29 first-degree relatives.Results: 75% of the LRRK2-PD and 87.5% of the IPD showed SNþ (p ¼ 0.087). aLRRK2þ had a higherfrequency of SNþ than non carriers (58.3% vs. 25%, p ¼ 0.039) and controls (58.3% vs. 12.5%; p ¼ 0.002)and had a larger area of SN echogenicity than non carriers (p ¼ 0.030) and controls (p < 0.001). The widthof the third ventricle was significantly lower in LRRK2-PD than in IPD (1.9 mm [1.38; 2.75] vs. 3.0 mm[2.3; 5.3]; p ¼ 0.003). Four out of 5 (80%) of the aLRRK2þ with an abnormal DAT-SPECT and four of the 5(80%) of those with REM sleep behaviour disorder (RBD) had SNþ.Conclusions: SNþ is very frequent in LRRK2-PD and aLRRK2þ. Most aLRRK2 with possible surrogatemarkers of PD such as abnormal DAT-SPECT or RBD, also had SNþ, which supports that this echofeaturemight be a marker of PD in these asymptomatic population.
© 2015 Elsevier Ltd. All rights reserved.
1. Background
Mutations in the leucine-rich repeat kinase 2 gene (LRRK2) arethe most common known cause of inherited Parkinson's disease(PD) [1]. Asymptomatic carriers of LRRK2 mutations (aLRRK2) are
* Corresponding author. Neurology Service, Hospital Clínic Barcelona, C/Villarroel170, 08036 Barcelona, Spain.
E-mail address: [email protected] (E. Tolosa).
Contents lists available at ScienceDirect
Parkinsonism and Related Disorders
journal homepage: www.elsevier .com/locate/parkreldis
http://dx.doi.org/10.1016/j.parkreldis.2015.08.0071353-8020/© 2015 Elsevier Ltd. All rights reserved.
Parkinsonism and Related Disorders 21 (2015) 1170e1176

50
RESULTADOS6
subjects at high risk for developing PD and provide a unique op-portunity to study PD risk biomarkers. One such stable risk markercould be an increased area of echogeniticy in the substantia nigra(SNþ), which has been associated with increased iron content andlinked to oxidative damage [2]. SNþ occurs in more than 90% of PDpatients [3] and in the healthy population is associated with anincreased risk of developing PD [4] but also up to 10% of healthycontrols and patients with other movement disorders (e.g. DYT6dystonia) show this echofeature [5,6]. SNþ is also associated withseveral prodromal markers such as hyposmia [7] and rapid-eye-movement sleep behavior disorder (RBD) [8].
Recent studies have shown that most LRRK2 associated PD(LRRK2-PD) patients have SNþ similarly to idiopathic PD (IPD) cases[9]. Also up to 85e90% of aLRRK2 has been reported to showincreased SN echogenicity [9,10] but the significance of this featureremains unknown. Other forms of genetic parkinsonisms have alsoSN hyperechogenicity [11e13]. Brain echographic features otherthan SN echogenicity have been less studied in LRRK2-PD.
The aim of our study was to assess the echogenicity of the SNand other brain echographic features in LRRK2 mutation carriersand to assess the potential application of these biomarkers aspredictors of PD.
2. Methods
2.1. Selection of patients
In this observational cross-sectional study 26 LRRK2 G2019S PDpatients were studied. Study patients were selected among a cohortof LRRK2 G2019S PD patients already identified at Hospital Clínic deBarcelona and other centers in Catalonia and Menorca that werealive and accessible. PD was diagnosed according to UnitedKingdom Parkinson's Disease Society criteria with the exceptionthat a positive family history was not considered an exclusion cri-terion [14] and the patients were screened for LRRK2 G2019S mu-tations as previously described [15]. For comparison purposes, 31patients with IPD without family history of PD recruited at theMovement Disorders unit of Hospital Clínic de Barcelona were alsostudied. We selected them matched by age to the LRRK2-PDsubjects.
Fifty first-degree relatives of the LRRK2-PD patients included inthe study accepted to participate. Twenty-four of them wereaLRRK2þ. Twenty-six relatives were non mutation carriers(aLRRK2�). Transcranial sonography (TCS) studies were also per-formed in 26 subjects without parkinsonism (healthy controls) ageand sex matched with the aLRRK2þ and unrelated to them. Patientsand their relatives as well as medical staff of participating centersrecruited volunteers from their personal relations who werescreened for exclusion criteria, which included the presence ofsymptoms suggestive of any neurodegenerative disease or a posi-tive family history for PD, and then considered for enrolment in thestudy.
All study participants were clinically evaluated at a single centerby the same researcher team (DV, ET, and CP). Asymptomaticsubjects were blinded to their mutation status.
2.2. Clinical assessment
Demographic data was collected from all study subjects. In PDpatients the age at onset of motor symptoms and age at diagnosis ofPD were collected. Disease durationwas estimated in patients fromthe time of diagnosis to the study date. Patients were assessedthrough the Unified Parkinson's Disease Rating Scale (UPDRS) [16],Schwab & England scale and HoehneYahr stage in On.Medicationsat the time of the evaluation were also recorded and levodopa
equivalent daily dose (LEDD) calculated [17].Smell was assessed by means of the 40-item University of
Pennsylvania Smell Identification Test (UPSIT; Spanish version) andthe patients were classified according to normative values [18].Depression was diagnosed according to DSM-IV criteria [19]. TheHospital Anxiety and Depression scale (HADS) [20] and the BeckDepression Inventory [21] were used to quantify the symptoms.Constipationwas diagnosed according to the Rome criteria [22] andthe SCOPA-AUT was administered [23]. Cognitive function wastested by the Montreal Cognitive Assessment (MOCA) [24]. REMSleep Behaviour Disorder (RBD) was considered to be present ac-cording to the established criteria [25] and the RBD screeningquestionnaire (RBDSQ) [26] was administered.
2.3. Transcranial sonography (TCS)
TCS was performed using a 2.5-MHz transducer with a Phillipsultrasound device (HD15; SO6600146375, Bothell, WA, USA)through the right and left preauricular temporal bone window. Thepenetration depth was 14 cm and the dynamic range 45e55 db. Allparticipants were examined by one experienced sonographer (DV)who store images of the mesencephalic and thalamic planes. Anindependent investigator (LI) blinded to the clinical and geneticstatus of subjects, who had not been involved in the TCS exami-nations, made the measures. We studied the echogenicity of thefollowing regions: SN echogenicity, brainstem raphe echogenicity,lenticular nucleus echogenicity and the third and lateral ventriclessize. Computarized measurements of SN echogenic sizes wereperformed on axial brain parenchyma sonography scans of themesencepahlic brainstem after manually encircling the outercircumference of the SN echogenic area. We selected the larger areaof hyperechogenicity in the SN of each subject. In accordance withpreviously reported cut-off values, SNþ was defined as an area ofechogenic signal �0.20 cm2; on at least one side [27]. The largerarea of each individual was registered (aSNmax). Echogenicity ofthe brainstem raphe was rated as reduced when its structure wasinterrupted or not visible, i.e. isoechogenic compared with theadjacent brain parenchyma [28]. Echogenicity of lentiform nucleiwas classified as hyperechogenic when it was more intense thanthe surrounding white matter [29]. The transverse diameter of thethird ventricle and of the right and left anterior horn weremeasured in the thalamic plane.
2.4. Dopamine transporter (DAT) imaging
Dopamine transporter (DAT) imaging was performed in 29 first-degree relatives of LRRK2-PD patients, 18 of which were aLRRK2þ.DAT SPECT imaging with (123)I-2b-carbomethoxy-3b-(4-iodophenyl)-N-(3-fluoropropyl)-nortropane ((123)I-FP-CIT) wasperformed 4 h after endovenous tracer administration. SPECT im-ages were acquired in a dual-headed gamma camera (E-Cam,Siemens), 64 images/head, with a matrix of 64 x 64. SPECT imageswere classified visually by nuclear medicine physicians (FL) asnormal when a symmetric intense tracer uptake in striatum bothcaudate nucleus and putamen was observed. If a reduction wasobserved in the striatal tracer uptake, either unilateral o bilateral,the DAT-SPECT was considered as abnormal [30].
2.5. Statistical analysis
Quantitative variables were treated as median, interquartilicrange (IQR) and range (maximum, minimum) and analysed usingKruskalleWallis test for overall comparisons and ManneWhitney'sU test for pair-wise comparisons in case of overall comparisonhaving been significant. Qualitative variables were described by
D. Vilas et al. / Parkinsonism and Related Disorders 21 (2015) 1170e1176 1171

51
RESULTADOS 6
absolute and relative frequencies and analysed by Chi2 or Fisher'sExact test. Effects of age in aSNmax in all groups of subjects and sizeof third ventricle in LRRK2-PD and IPD patients were estimatedusing a general lineal model (GLM) with a Dunnett test from youngsubjects as post-hoc analysis. Statistical analyses were performedwith SPSS version 20.0 (IBM, NYC, USA) and a Type I error of 5% wasused in all analyses.
2.6. Standard protocol approvals and patient consents
The study was approved by the Hospital Clínic de BarcelonaEthics Committee (26th July 2012) and a written informed consentwas obtained from all study subjects previous to the study.
3. Results
3.1. Demographic and clinical
Demographic data are summarized in Table 1. Median age ofLRRK2-PD and IPD subjects was 67 [56; 77] and 63 [56; 68]respectively, and 12 (46.2%) of the LRRK2-PD patients and 21 (67.7%)of the IPD were males. Disease duration was not different betweenboth groups (6 years [2; 12] in LRRK2-PD and 5 years [1; 7] in IPD;p ¼ 0.092). UPDRS I, II and III and MOCA scores were also compa-rable between both groups. The levodopa equivalent daily dose(LEDD) was higher in LRRK2-PD patients than IPD patients (859 mg[408; 1377] vs 520 mg [205; 883], p ¼ 0.026). The UPSIT score washigher in LRRK2-PD patients compared to IPD patients (24 [19; 27]vs 19 [17; 22], p ¼ 0.026). Demographic variables in aLRRK2þ werecomparable to aLRRK2� and controls without parkinsonism(Table 1).
3.2. TCS
Six (23.1%) LRRK2-PD and 7 (24.1%) IPD patients had an insuf-ficient bone window that precluded the TCS study (Table 2). Themedian area of the SN echogenicity was not different between bothstudy groups. The aSNmax was similar in the LRRK2-PD and in the
IPD group (0.31 cm2 [0.21; 0.37] vs 0.29 cm2 [0.23; 0.32];p¼ 0.685). Fifteen (75%) of the LRRK2-PD patients and 21 (87.5%) ofthe IPD patients showed SNþ (p ¼ 0.087).
All aLRRK2þ had an adequate bone window and only 2 (7.7%) ofthe aLRRK2� and 2 (7.7%) of the controls had an inadequate tem-poral bone window that precluded the TCS study (Table 3).aLRRK2þ subjects had a larger area of SN echogenicity thanaLRRK2� (0.22 cm2 [0.16; 0.25] vs. 0.16 cm2 [0.1; 0.2]; p ¼ 0.030)and than controls subjects (0.22 cm2 [0.16; 0.25] vs. 0.11 cm2 [0.09;0.15]; p < 0.001). No significantly differences were found in the areaof the SN echogenicity between aLRRK2� and controls. The per-centage of subjects with SNþ was higher in the aLRRK2þ groupthan in aLRRK2� (14 (58.3%) vs. 6 (25%); p ¼ 0.039) and than incontrols (14 (58.3%) vs. 3 (12.5%) in the controls (p ¼ 0.002). Thispercentage was no different between aLRRK2� and controls (6(25%) vs. 3 (12.5%); p ¼ 0.461).
The estimated size of the third ventricle was significantly lowerin LRRK2-PD patients than in the IPD group (1.9 mm [1.38; 2.75] vs.3.0 mm [2.3; 5.3]; p ¼ 0.003). The size of the third ventricleincreased with age in both groups, e.g. LRRK2-PD and IPD. From theage of 60 years onwards the width of the third ventricle wassignificantly higher in IPD patients than in LRRK2-PD patients(eTable 1 in and Fig. 1). No correlation was found between the sizeof the third ventricle and the MOCA scores in the LRRK2-PD group(r ¼ 0.066, p ¼ 0.781) or in the IPD group (r ¼ �0.238, p ¼ 0.455).
Nine (45%) of the LRRK2-PD patients and 7 (33.3%) of the IPDpatients showed hypoechogenicity in the raphe nuclei of thebrainstem (p ¼ 0.53). No differences between the width of thefrontal horn of the lateral ventricles or the echogenicity of thelentiform nuclei were found in both groups (Table 2).
No differences were found among aLRRK2þ, aLRRK2� andcontrols in brainstem raphe echogenicity, and in size of the third orlateral ventricles (Table 3).
3.3. Clinical and imaging markers in aLRRK2þ and aLRRK2� andsubstantia nigra echogenicity
No differences were found in age, gender, motor and nonmotor
Table 1Demographic and clinical data of LRRK2-PD, IPD, first-degree relatives and controls.
LRRK2-PD IPD p-value aLRRK2þ aLRRK2� Controls p-value
26 31 24 26 26
Age 67 [56; 77] (47e89) 63 [56; 68] (47e79) 0.305$ 45 [38; 50] (27e65) 45 [38; 51] (23e77) 45 [40; 60] (27e69) 0.669$
Gender (male), n (%) 12 (46.2%) 21 (67.7%) 0.103& 12 (50%) 11 (42.3%) 6 (32.1%) 0.131&
Age at onset ofmotor symptoms, years
58 [47; 65] (33e82) 58 [50; 65] (40e75) 0.903$ e e e e
Age at onset ofPD diagnosis, years
59 [49; 66] (33e82) 58 [50; 65] (41e75) 0.962$ e e e e
Disease durationsince OMS, years
9 [4; 12] (1e18) 7 [2; 8] (1e11) 0.062$ e e e e
Disease durationsince diagnosis, years
6 [2; 12] (1e18) 5 [1; 7] (1e11) 0.092$ e e e e
UPDRS I score 8 [5; 14] (0e24) 10 [5; 18] (1e23) 0.234$ 3 [0; 5] (0e11) 1 [0; 3] (0e6) 3 [1; 5] (0e5) 0.203$
UPDRS II score 9 [4; 16] (1e35) 10 [2; 12] (1e38) 0.690$ 0 [0; 0] (0e1) 0 [0; 0] (0e2) 0 [0; 0] (0e2) 0.970$
UPDRS III score 14 [9; 31] (2e58) 18 [12; 27] (4e49) 0.535$ 0 [0; 1] (0e4) 0 [0; 0] (0e1) 0 [0; 2] (0e2) 0.059$
UPDRS IV score 0 [0; 6] (0e13) 0 [0; 1] (0e9) 0.205$ e e e e
HY 2 [1,5; 2,5] (1e4) 2 [1,5; 2] (1e2,5) 0.525$ e e e e
SE 90 [80; 90] (20e100) 90 [90; 100] (50e100) 0.067$ e e e e
LEDD 859 [408; 1377] (100e1988) 520 [205; 883] (100e1294) 0.026$ e e e e
UPSIT 24 [19; 27] (4e34) 19 [17; 22] (9e27) 0.026$ 34 [31; 35] (28e38) 34 [31; 35] (27e38) 33 [31; 35] (30e36) 0.728$
MOCA 24 [20; 26] (12e30) 25 [23; 28] (0e30) 0.318$ 28 [26; 29] (23e30) 28 [26; 29] (25e30) 28 [25; 30] (21e30) 0.931$
Results were described by mean median and interquartilic range IQR and range (maximum, minimum) or absolute and relative frequencies for qualitative variables forquantitative or qualitative variables respectively. $: U ManneWhitney test. & Fischer's Exact test. LRRK2-PD: LRRK2 associated Parkinson's disease. IPD: Idiopathic Parkinson'sdisease. aLRRK2þ: asymptomatic carriers of the G2019S LRRK2mutation. aLRRK2�: first-degree relatives non carriers of the G2019Smutation. OMS: onset of motor symptoms.UPDRS: unified Parkinson's disease rating scale. HY: Hoehn and Yahr scale. SE: Schwab and England scale. LEDD: Levodopa equivalent daily dose. UPSIT: University ofPennsylvania Smell Identification Test. MOCA: Montreal Cognitive Assessment.
D. Vilas et al. / Parkinsonism and Related Disorders 21 (2015) 1170e11761172

52
RESULTADOS6
symptoms between aLRRK2þ with and without SNþ (eTable 2).Also the proportion of subjects with an abnormal DAT-SPECT wassimilar in both groups (4/12 (33.3%) vs. 1/6 (16.7%); p ¼ 0.457)(Fig. 2).
Four out of 5 (80%) of the aLRRK2þ subjects with an abnormalDAT-SPECT and four of the 5 (80%) aLRRK2þ with RBD had an SNþ.Only one of the 5 aLRRK2þ with abnormal DAT-SPECT had alsoRBD. Eight out of the 13 (61.5%) with a normal DAT-SPECT and 10 ofthe 18 (55.6%) without RBD also had SNþ (p ¼ 0.298) (eFigure 1).
The aLRRK2�, with and without SNþ, had comparable age, sexand motor symptoms scores. From those, the subjects with SNþhad higher scores in the SCOPA-AUT scale (p ¼ 0.009). None of theaLRRK2� had an abnormal DaT-SPECT. (eTable 3).
4. Discussion
This study shows that most LRRK2-PD patients have increasedSN echogenicity with a detected frequency of SNþ similar to thatencountered in the IPD cases and to that reported previously byothers in LRRK2-PD [3,9,10]. We also found that SNþ is frequent inLRRK2 G2019S asymptomatic carriers.
SNþ is an iron-related risk marker of the vulnerability of the
dopaminergic nigral cells and it is thought to be a stable traitmarker of PD as it antedates the development of classical motorsymptoms, but it does not change thereafter, thus being a potentialPD-risk biomarker in individuals with this feature [2]. LRRK2-PDhas a variable penetrance and not all mutation carriers will developPD in their lifetime. It may be thought that among the group ofasymptomatic LRRK2 carriers, those subjects with SNþ are those inwhom disease will eventually develop. If this were the case, thelower frequency of SNþ in our study population, compared withthe reported frequency by others [10,31], would suggest that feweraLRRK2 carriers will develop PD in our cohort when compared withcohorts with high frequency of SNþ subjects. We have not studiedprevalence of PD in our population but the SNþ frequency values fitwell, in general, with the estimated penetrance of LRRK2-PD incohorts similar to this study [32], suggesting, for example, thatamong carriers only approximately half of subjects will develop PD.
Since an abnormal DAT-SPECT is another suggested surrogatemarker of disease in subjects at high risk for developing PD[7,33e35], if SNþ were a marker of PD development, one wouldexpect such abnormality to be present in aLRRK2þ subjects with anabnormal DaT-SPECT. Four of our 5 cases with an abnormal DAT-SPECT had SNþ and results from Sierra et al.'s study also support
Table 3Ecographic features in aLRRK2þ, aLRRK2� and controls.
aLRRK2þ aLRRK2� Controls p-value Pair-wise
aLRRK2þ vs aLRRK2� aLRRK2þ vs controls aLRRK2� vs controls24 26 26
Inadecuate bonewindow, n (%)
0 (0%) 2 (7.7%) 2 (7.7%) 0.538&
Right SN (cm2) 0.185 [0.15; 0.22](0.1e0.29)
0.125 [0.06; 0.19](0.04e0.45)
0.1 [0.09; 0.14](0.06e0.27)
0.001¥ 0.013$ <0.001$ 0.542$
Left SN (cm2) 0.201 [0.15; 0.23](0.09e0.29)
0.13 [0.08; 0.16](0.01e0.37)
0.105 [0.08; 0.15](0.05e0.25)
<0.001¥ 0.005$ <0.001$ 0.407$
aSNmax (cm2) 0.22 [0.16; 0.25](0.09e0.29)
0.16 [0.1; 0.2](0.06e0.45)
0.11 [0.09; 0.15](0.06e0.27)
<0.001¥ 0.030$ <0.001$ 0.167$
SNþ, n (%) 14 (58.3%) 6 (25%) 3 (12.5%) 0.003¥ 0.039$ 0.002$ 0.461$
Hypoechogenicity of thebrainstem raphe, n (%)
9 (37.5%) 6 (25%) 11 (45.8%) 0.361¥
Third ventricle (mm) 1.57 [1.1; 2.6](0.50e6.48)
1.8 [1.0; 3.39](0.45e6.2)
2.25 [1.5; 4.05](0.90e6.4)
0.113¥
Right frontal horn (mm) 16.8 [15.3; 18.1](14.3e19)
16.28 [15.2; 17.96](10.3e19.8)
15.5 [12.8; 17.35](11.3e19.4)
0.121¥
Left frontal horn (mm) 17.3 [15.9; 18.6](14.4e19.4)
15.7 [15.2; 17.9](13.9e18.43)
16.1 [15.6; 16.4](11.5e19.6)
0.379¥
Lentiform hyperechogenicity 2 (8.3%) 4 (16.7%) 0 (0%) 0.155&
aLRRK2þ: asymptomatic carriers of the G2019S LRRK2 mutation. aLRRK2�: first-degree relatives non carriers of the G2019S mutation. SN: substantia nigra.¥: Kruskall-Wallis test.$: U Mann-Whitney test.&: Fischer's Exact test.
Table 2Ecographic features in LRRK2 G2019S PD and IPD.
LRRK2-PD IPD p-value
26 31
Inadecuate bone window, n (%) 6 (23.1%) 7 (24.1%) 1.000&
Right SN (cm2) 0.255 [0.18; 0.36] (0.1e0.61) 0.255 [0.2; 0.32] (0.116e0.535) 0.969$
Left SN (cm2) 0.3 [0.17; 0.36] (0.1e0.61) 0.234 [0.22; 0.305] (0.114e0.665) 0.546$
aSNmax (cm2) 0.31 [0.21; 0.37] (0.1e0.61) 0.29 [0.23; 0.32] (0.12e0.67) 0.685$
SNþ, n (%) 15 (75%) 21 (95.5%) 0.087&
Hypoechogenicity of the brainstem raphe, n(%) 9 (45%) 7 (33.3%) 0.530&
Third ventricle (mm) 1.9 [1.38; 2.75] (0.4e5.66) 3.0 [2.3; 5.3] (1.3e6.85) 0.003$
Right frontal horn (mm) 16.4 [15.6; 18.4] (14.7e21.2) 16.4 [15.5; 18.3] (10.9e21.5) 0.803$
Left frontal horn (mm) 17.15 [15.35; 18.3] (14.76e22.3) 17.7 [15.8; 18.7] (15e21.1) 0.547$
Lentiform hyperechogenicity, n (%) 1 (5.3%) 0 (0%) 0.463
Results were described by mean median and interquartilic range IQR and range (maximum, minimum) or absolute and relative frequencies for qualitative variables forquantitative or qualitative variables respectively. $: U ManneWhitney test. & Fischer's Exact test. LRRK2-PD: LRRK2 associated Parkinson's disease. IPD: Idiopathic Parkinson'sdisease. SN: substantia nigra.
D. Vilas et al. / Parkinsonism and Related Disorders 21 (2015) 1170e1176 1173

53
RESULTADOS 6
this contention since ninety percent of their aLRRK2þwith reducedstriatal uptake in DAT-SPECT had SNþ. We also found that 66.7% ofaLRRK2 carriers with SNþ had a normal DAT-SPECT. These resultsare similar to those reported previously [10] and in line with theconcept that SNþ is considered a stable statemarker of PD but not amarker indicative of ongoing disease process. Among our aLRRK2þstudy subjects, 80% of those with idiopathic RBD, another markerstrongly associatedwith PD [8], had SNþ. Like the SPECT results thisobservation also supports that SNþ may be a maker of PD in theseasymptomatic population, although this interpretation should betaken cautiously since the diagnosis of RBDwas not confirmed withpolysomnography and since our study is cross-sectional.
We did not find any significant difference in clinical and imagingbiomarkers known to occur in the premotor phase of IPD betweenthose aLRRK2þ subjects with andwithout SNþ. Also possible is thatour aLRRK2þ have not yet reached this threshold of diseasedevelopment in which NMS become manifest, may be because oftheir relatively young age. This finding may possibly reflect that thepremotor phase of LRRK2-PD differs clinically from that of IPD.
In our study 25% of the aLRRK2� had SNþ, a frequency slightlyhigher than that found in controls (12.5%) but lower than that re-ported by others [10]. A positive family history of PD per se in-creases the disease risk [36]. The higher frequency of SNþ inaLRRK2� detected by others supports that other factors, genetic,
Fig. 2. 123I-FP-CIT SPECT images from an asymptomatic 48 years-old man carrier of the G2019S mutation in the LRRK2 gene. A decreased left putamen dopamine transporteruptake was observed. 123I-FP-CIT ¼ 123I-2b-carbomethoxy-3b-(4-iodophenyl)-N-(3-fluoropropyl)-nortropane.
Fig. 1. Third ventricle size in G2019S LRRK2-PD and IPD. The size of the third ventricle increased with age in both groups, e.g. LRRK2-PD and IPD early in LRRK2-PD than IPD group.From the age of 60 years onwards the width of the third ventricle was significantly higher in IPD patients than in LRRK2-PD patients. LRRK2-PD: LRRK2 associated Parkinson'sdisease. IPD: Idiopathic Parkinson's disease.
D. Vilas et al. / Parkinsonism and Related Disorders 21 (2015) 1170e11761174

54
RESULTADOS6
epigenetic or environmental, besides the G2019S mutation, mighthave a role in modifying vulnerability of the nigrostriatal systemand consequently in the number of SNþ on echographic studies.The aLRRK2� subjects with SNþ in this study had higher scores insome dysautonomic scales. These findings should be interpretedcautiously since the number of cases is small and also the differ-ences in the scores of these scales do not seem clinically relevant.
In the present study LRRK2-PD patients had a smaller size of thethird ventricle compared with the IPD patients, especially in sub-jects older than 60 years. In a recent study the size of the thirdventricle wasmentioned to be similar in LRRK2-PD and IPD patients[9]. Higher ventricular size in IPD vs. LRRK2-PD could be explainedby lesser subcortical brain atrophy in LRRK2-PD than in IPD. Lessatrophy in LRRK2-PD might be related to the observation thatLRRK2-PD patients have a more benign course and with lesscognitive impairment than IPD cases [37] and that the neuro-pathological substrate in LRRK2-PD is in some cases different fromIPD with less extensive pathology [38]. These findings should beconfirmed in future studies using both echography and magneticresonance imaging studies in bigger cohorts of subjects.
There are some potential limitations to our study. The samplesizes are small; this could mask or highlight effects due to effect ofextreme values. Also the process of analysis of SN echo images byTCS has intrinsic limitations related to the arbitrary selection ofcutoff points since we have not defined a cut-off value for our ownultrasound device. However, we followed a standard method [27]and also in our study the proportion of parkinsonian patientsshowing abnormal SN hyperechogenicity or brainstem raphehypoechogenicity was in the range of previous studies [39].
In conclusion, our results indicate that hyperechogenicity of theSN is present in most of the LRRK2-PD patients and also in morethan half of the asymptomatic LRRK2 G2019S mutation carriers,suggesting that is an early finding in the premotor stage of theLRRK2-PD. This echofeature could be a risk marker for the devel-opment of parkinsonism in asymptomatic LRRK2mutation carriers.Additional studies in larger cohorts to confirm and extend ourfindings are needed and long-term-follow-up studies in these riskgroups should be performed in order to assess the rate of con-verters to PD. The size of the third ventricle was lower in LRRK2-PDthan in IPD, suggesting a lesser level of subcortical brain atrophy inthis form of genetic PD.
Acknowledgments
The authors are grateful to the patients and the families thatparticipated in this study. We also thank to Dr. A. Chamorro, head ofthe Stroke Unit of Hospital Clínic de Barcelona for kindly provide usthe ultrasound device and the Michael J Fox Foundation and theMarat�o TV3 for support the research. None of the authors of thismanuscript report conflict of interest.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.parkreldis.2015.08.007.
References
[1] C. Paisan-Ruiz, S. Jain, E.W. Evans, et al., Cloning of the gene containing mu-tations that cause PARK8-linked Parkinson's disease, Neuron 44 (4) (2004)595e600.
[2] D. Berg, W. Roggendorf, U. Schroder, et al., Echogenicity of the substantianigra: association with increased iron content and marker for susceptibility tonigrostriatal injury, Arch. Neurol. 59 (6) (2002) 999e1005.
[3] D. Berg, J. Godau, U. Walter, Transcranial sonography in movement disorders,Lancet Neurol. 7 (11) (2008) 1044e1055.
[4] D. Berg, S. Behnke, K. Seppi, et al., Enlarged hyperechogenic substantia nigra as
a risk marker for Parkinson's disease, Mov. Disord. 28 (2) (2013) 216e219.[5] R. Saunders-Pullman, K. Stanley, N. Brüggemann, et al., Substantia nigra
hyperechogenicity in DYT6 dystonia: a pilot study, Park. Relat. Disord. 16 (6)(2010 Jul) 420e422.
[6] D. Berg, G. Becker, B. Zeiler, et al., Vulnerability of the nigrostriatal system asdetected by transcranial ultrasound, Neurology 53 (1999) 1026e1031.
[7] U. Sommer, T. Hummel, K. Cormann, et al., Detection of presymptomaticParkinson's disease: combining smell tests, transcranial sonography, andSPECT, Mov. Disord. 19 (10) (2004) 1196e1202.
[8] A. Iranzo, F. Lomena, H. Stockner, et al., Decreased striatal dopamine trans-porter uptake and substantia nigra hyperechogenicity as risk markers ofsynucleinopathy in patients with idiopathic rapid-eye-movement sleepbehaviour disorder: a prospective study [corrected], Lancet Neurol. 9 (11)(2010) 1070e1077.
[9] K. Brockmann, A. Groger, A. Di Santo, et al., Clinical and brain imaging char-acteristics in leucine-rich repeat kinase 2-associated PD and asymptomaticmutation carriers, Mov. Disord. 26 (13) (2011) 2335e2342.
[10] M. Sierra, P. Sanchez-Juan, M.I. Martinez-Rodriguez, et al., Olfaction and im-aging biomarkers in premotor LRRK2 G2019S-associated Parkinson disease,Neurology 80 (7) (2013) 621e626.
[11] K.J. Schweitzer, T. Brussel, P. Leitner, et al., Transcranial ultrasound in differentmonogenetic subtypes of Parkinson's disease, J. Neurol. 254 (5) (2007)613e616.
[12] U. Walter, C. Klein, R. Hilker, et al., Brain parenchyma sonography detectspreclinical parkinsonism, Mov. Disord. 19 (12) (2004 Dec) 1445e1449.
[13] J.M. Hagenah, B. Becker, N. Brüggemann, et al., Transcranial sonographyfindings in a large family with homozygous and heterozygous PINK1mutations, J. Neurol. Neurosurg. Psychiatry 79 (9) (2008 Sep)1071e1074.
[14] A.J. Hughes, S.E. Daniel, L. Kilford, et al., Accuracy of clinical diagnosis ofidiopathic Parkinson's disease: a clinico-pathological study of 100 cases,J. Neurol. Neurosurg. Psychiatry 55 (3) (1992) 181e184.
[15] C. Gaig, M. Ezquerra, M.J. Marti, et al., LRRK2 mutations in Spanish patientswith Parkinson disease: frequency, clinical features, and incomplete pene-trance, Arch. Neurol. 63 (3) (2006) 377e382.
[16] C.G. Goetz, B.C. Tilley, S.R. Shaftman, et al., Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results, Mov. Disord. 23(15) (2008) 2129e2170.
[17] J.C. Moller, Y. Korner, R.C. Dodel, et al., Pharmacotherapy of Parkinson's dis-ease in Germany, J. Neurol. 252 (8) (2005) 926e935.
[18] R.L. Doty, S.M. Bromley, M.B. Stern, Olfactory testing as an aid in the diagnosisof Parkinson's disease: development of optimal discrimination criteria, Neu-rodegeneration 4 (1) (1995) 93e97.
[19] Diagnostic and Statistical Manual of Mental Disorders: DSM-IV, AmericanPsychiatric Association, Washington, 1994.
[20] A.S. Zigmond, R.P. Snaith, The hospital anxiety and depression scale, ActaPsychiatr. Scand. 67 (6) (1983) 361e370.
[21] A.T. Beck, R.A. Steer, G.K. Brown, Manual for the Beck Depression Inventory,Psychological Corporation, San Antonio, TX, 1996.
[22] G.F. Longstreth, W.G. Thompson, W.D. Chey, et al., Functional bowel disorders,Gastroenterology 130 (5) (2006) 1480e1491.
[23] M. Visser, J. Marinus, A.M. Stiggelbout, et al., Assessment of autonomicdysfunction in Parkinson's disease: the SCOPA-AUT, Mov. Disord. 19 (11)(2004) 1306e1312.
[24] Z.S. Nasreddine, N.A. Phillips, V. Bedirian, et al., The Montreal CognitiveAssessment, MoCA: a brief screening tool for mild cognitive impairment,J. Am. Geriatr. Soc. 53 (4) (2005) 695e699.
[25] Medicine AASM, International Classification of Sleep Disorders, second ed.,2005.
[26] K. Stiasny-Kolster, G. Mayer, S. Schafer, et al., The REM sleep behavior disorderscreening questionnaireea new diagnostic instrument, Mov. Disord. 22 (16)(2007) 2386e2393.
[27] D. Berg, G. Becker, B. Zeiler, et al., Vulnerability of the nigrostriatal system asdetected by transcranial ultrasound, Neurology 53 (5) (1999) 1026e1031.
[28] D. Berg, T. Supprian, E. Hofmann, et al., Depression in Parkinson's disease:brainstem midline alteration on transcranial sonography and magneticresonance imaging, J. Neurol. 246 (12) (1999) 1186e1193.
[29] U. Walter, L. Niehaus, T. Probst, et al., Brain parenchyma sonography dis-criminates Parkinson's disease and atypical parkinsonian syndromes,Neurology 60 (1) (2003) 74e77.
[30] T.S. Benamer, J. Patterson, D.G. Grosset, et al., Accurate differentiation ofparkinsonism and essential tremor using visual assessment of [123I]-FP-CITSPECT imaging: the [123I]-FP-CIT study group, Mov. Disord. 15 (3) (2000)503e510.
[31] N. Bruggemann, J. Hagenah, K. Stanley, et al., Substantia nigra hyper-echogenicity with LRRK2 G2019S mutations, Mov. Disord. 26 (5) (2011)885e888.
[32] M. Sierra, I. Gonzalez-Aramburu, P. Sanchez-Juan, et al., High frequencyand reduced penetrance of LRRK2 G2019S mutation among Parkinson'sdisease patients in Cantabria (Spain), Mov. Disord. 26 (13) (2011)2343e2346.
[33] A. Iranzo, F. Valldeoriola, F. Lomena, et al., Serial dopamine transporter im-aging of nigrostriatal function in patients with idiopathic rapid-eye-movement sleep behaviour disorder: a prospective study, Lancet Neurol. 10
D. Vilas et al. / Parkinsonism and Related Disorders 21 (2015) 1170e1176 1175

55
RESULTADOS 6
(9) (2011) 797e805.[34] A. Winogrodzka, P. Bergmans, J. Booij, et al., [(123)I]beta-CIT SPECT is a useful
method for monitoring dopaminergic degeneration in early stage Parkinson'sdisease, J. Neurol. Neurosurg. Psychiatry 74 (3) (2003) 294e298.
[35] R.B. Postuma, D. Aarsland, P. Barone, et al., Identifying prodromal Parkinson'sdisease: pre-motor disorders in Parkinson's disease, Mov. Disord. 27 (5)(2012) 617e626.
[36] A.J. Noyce, J.P. Bestwick, L. Silveira-Moriyama, et al., Meta-analysis of earlynonmotor features and risk factors for Parkinson disease, Ann. Neurol. 72 (6)
(2012 Dec) 893e901.[37] D.G. Healy, M. Falchi, S.S. O'Sullivan, et al., Phenotype, genotype, and world-
wide genetic penetrance of LRRK2-associated Parkinson's disease: a case-control study, Lancet Neurol. 7 (7) (2008) 583e590.
[38] M. Poulopoulos, O.A. Levy, R.N. Alcalay, The neuropathology of genetic Par-kinson's disease, Mov. Disord. 27 (7) (2012) 831e842.
[39] D. Berg, Transcranial ultrasound as a risk marker for Parkinson's disease, Mov.Disord. 24 (Suppl. 2) (2009) S677eS683.
D. Vilas et al. / Parkinsonism and Related Disorders 21 (2015) 1170e11761176

56
RESULTADOS6
aLRRK2+ n = 24
Abnormal DaT-SPECT 5 (27 .8 %)
Normal DaT-SPECT 13 (72 .2 %)
DaT-SPECT available n = 18
SN+ 4 (80 %)
SN– 1 (20 %)
SN+ 8 (61 .5 %)
SN– 5 (38 .5 %)
Abnormal DaT-SPECT
0 (0 %)
Normal DaT-SPECT 11 (100 %)
SN+ 5 (45 .5 %)
SN– 6 (54 .5 %)
DaT-SPECT available n = 11
aLRRK2– n = 26
eFigure 1: Imaging markers in asymptomatic relatives of LRRK2-PD patients.
aLRRK2+: asymptomatic carriers of the G2019S LRRK2 mutation. aLRRK2–: first-degree relatives non carriers of the
G2019S mutation. SN+: substantia nigra hyperechogenicity. SN–: normal echogenicity of the substantia nigra.
Age (years) LRRK2-PD a p value b IPD a p value b p value c
40 0.122 (0.091; 0.152) Baseline 0.24 (0.088; 0.392) Baseline 0.136
50 0.196 (0.093; 0.298) 0.176 0.269 (0.222; 0.316) 0.724 0.203
60 0.225 (0.156; 0.294) 0.008 0.405 (0.284; 0.526) 0.097 0.011
70-80 0.288 (0.173; 0.402) 0.006 0.493 (0.347; 0.638) 0.019 0.03
eTable 1: Size of the third ventricle and age in EP-LRRK2 and EPI
a Estimation of mean of size of the third ventricle (mm) from GLM model and 95 % CI. b Between LRRK2-PD
vs. IPD subjects. c From younger subjects. LRRK2-PD: LRRK2 associated Parkinson’s disease. IPD: Idiopathic
Parkinson’s disease.

57
RESULTADOS 6
aLRRK2+ SN+ n = 14
aLRRK2+ SN– n = 10
p value
Age, years 41.50 [36.00; 47.25] 47 [43.75; 51] 0.078 a
Male , n(%) 8 (57.1 %) 4 (49 %) 0.408 b
UPDRS I score 2 [0; 4] 4 [0; 7] 0.806 a
UPDRS II score 0 [0; 0] 0 [0; 5] 0.632 a
UPDRS III score 0 [0; 2.5] 1 [0; 1] 0.699 a
Hyposmia, n(%) 1 (7.1 %) 2 (28.6 %) 0.106 b
Depression, n(%) 3 (21.4 %) 3 (33.3 %) 0.526 b
Anxiety, n(%) 5 (38.5 %) 2 (22.2 %) 0.421 b
HADS Total score 7 [2; 12.25] 8 [5; 12] 0.393 a
HADS Depression score 1.5 [0; 5] 2 [1.5; 4.5] 0.521 a
HADS Anxiety score 4 [2; 8] 5 [3.5; 8] 0.310 a
BDI score 2 [0; 9] 5 [3; 10.5] 0.227 a
Constipation, n(%) 0 (0 %) 1 (11.1 %) 0.202 b
SCOPA-GI 1.5 [0; 3] 1 [0; 3] 0.819 a
SCOPA-U 3 [0.75; 5.25] 4 [2.5; 8] 0.162 a
SCOPA-CV 1 [0; 1] 0 [0; 2.5] 0.756 a
SCOPA-T 0 [0; 1.25] 2 [0; 4] 0.116 a
SCOPA-P 1 [0; 2.25] 2 [0; 3] 0.534 a
SCOPA-AUT 8.5 [1.5; 12.5] 10 [7; 20.5] 0.206 a
RBD, n(%) 4 (28.6 %) 1 (10 %) 0.298 b
RBDSQ score 2 [0; 5.5] 2 [0.75; 4.5] 0.953 a
Insomnia, n(%) 3 (21.4 %) 3 (30 %) 0.395 b
Epworth Scale 6 [5; 10] 6 [5; 9] 0.948 a
Abnormal DaT-SPECT, n(%) 4 (33.3 %) 1 (16.7 %) 0.457 b
eTable 2: Demographic and clinical features in aLRRK2+ and substantia nigra echogenicity
Results expressed as median [Percentiles 25th; 75th] for quantitative variables and absolute frequencies
with percentage for qualitative variables. a U Mann-Whitney test. b Fischer’s Exact test.
aLRRK2+: asymptomatic carriers of the G2019S LRRK2 mutation. SN+: substantia nigra hyperechogenicity.
SN-: normal echogenicity of the substantia nigra. UPDRS: unified Parkinson’s disease rating scale, parts I, II and III.
HADS: Hamilton Anxiety and Depression Scale. BDI: Beck Depression Inventory. SCOPA-AUT: Scales for Outcomes
in Parkinson’s disease-Autonomic. GI: Gastrointestinal dysfunction. GU: Urinary dysfunction. CV: Cardiovascular
dysfunction. T: Thermoregulatory dysfunction. P: Pupillomotor dysfunction. RBD: REM sleep behaviour disorder.
DaT-SPECT: Dopamine transporter single-photon emission computed tomography.

58
RESULTADOS6
aLRRK2– SN+ n = 6
aLRRK2– SN– n = 19
p value
Age 46 [34.25; 65.5] 43 [38; 51] 0.679 a
Male , n(%) 2 (33.3 %) 9 (47.4 %) 0.554 b
UPDRS I score 1.5 [0; 4.25] 1 [0; 3] 0.768 a
UPDRS II score 0 [0; 0.5] 0 [0; 0] 0.964 a
UPDRS III score 0 [0; 0.25] 0 [0; 0] 0.960 a
Hyposmia, n(%) 1 (16.7 %) 2 (10.5 %) 0.912 b
Depression, n(%) 0 (0 %) 3 (15.8 %) 0.265 b
Anxiety, n(%) 0 (0 %) 4 (21.1 %) 0.154 b
HADS Total score 5 [3.25; 12.5] 5 [2; 8] 0.639 a
HADS Depression score 2 [0.75; 3.25] 1.39 [0; 1.25] 0.221 a
HADS Anxiety score 3 [2.5; 9.25] 4 [1.75; 6.25] 0.814 a
BDI score 2.5 [0; 7.25] 1.5 [0; 4] 0.579
Constipation, n(%) 1 (16.7 %) 1 (5.3 %) 0.379 b
SCOPA-GI 2 [2; 4.5] 0 [0; 1] 0.002 a
SCOPA-U 2.5 [0.75; 9.75] 1 [0; 3] 0.280 a
SCOPA-CV 1 [0; 1.25] 0 [0; 0] 0.009 a
SCOPA-T 0.5 [0; 2.5] 0 [0; 0] 0.025 a
SCOPA-P 1 [0; 2.25] 0 [0; 2] 0.613 a
SCOPA-AUT 12.5 [5.5; 16] 4 [2; 7] 0.009 a
RBD, n(%) 0 (0 %) 1 (5.3 %) 0.695 b
RBDSQ score 0.5 [0; 1.75] 0.5 [0; 2.25] 0.858 a
Insomnia, n(%) 1 (16.7 %) 3 (15.8 %) 1.000 b
Epworth Scale 6 [4; 8.25] 7 [5; 8] 0.700 a
Abnormal DaT-SPECT, n(%) 0 (0 %) 0 (0 %) 0.141 b
eTable 3: Demographic and clinical features in aLRRK2– and substantia nigra echogenicity
Results expressed as median [Percentiles 25th; 75th] for quantitative variables and absolute frequencies
with percentage for qualitative variables. a U Mann-Whitney test. b Fischer’s Exact test.
aLRRK2–: first-degree relatives non carriers of the G2019S mutation. SN+: substantia nigra hyperechogenicity.
SN-: normal echogenicity of the substantia nigra. UPDRS: unified Parkinson’s disease rating scale, parts I, II and III.
HADS: Hamilton Anxiety and Depression Scale. BDI: Beck Depression Inventory. SCOPA-AUT: Scales for Outcomes
in Parkinson’s disease-Autonomic. GI: Gastrointestinal dysfunction. GU: Urinary dysfunction. CV: Cardiovascular
dysfunction. T: Thermoregulatory dysfunction. P: Pupillomotor dysfunction. RBD: REM sleep behaviour disorder.
DaT-SPECT: Dopamine transporter single-photon emission computed tomography.

59
RESULTADOS 6
Trabajo número 3
Reduced thalamo-cortical functional connectivity in asymptomatic LRRK2 mutation carriers
Dolores Vilas, Bàrbara Segura, Claustre Pont-Sunyer, Yaroslau Compta, Francesc Valldeoriola,
María José Martí, Hugo C. Baggio, María Quintana, Angels Bayés, Jorge Hernández-Vara, Matilde Calopa,
Miquel Aguilar, Carme Junqué, Eduardo Tolosa and the Barcelona LRRK2 Study Group.

60
RESULTADOS6
Disminución en la conectividad funcional tálamo-cortical en portadores asintomáticos
de mutaciones del gen LRRK2
Antecedentes: El estudio de la conectividad funcional por medio de la resonancia magnética
cerebral (RM) en los portadores asintomáticos de mutaciones del gen LRRK2 (aLRRK2) puede
contribuir a la caracterización de la fase preclínica de la EP-LRRK2.
Objetivo: Caracterizar los patrones de RM funcional (RMf) durante el estado de reposo (resting
state) en aLRRK2.
Métodos: Realizamos una RM estructural y funcional a 18 aLRRK2 y a 18 no portadores de la
mutación, todos ellos familiares de primer grado de pacientes con EP-LRRK2. Partiendo de la RMf
(resting state), analizamos la conectividad funcional de los circuitos nigroestriatales y tálamo-es-
triato-corticales. Los datos cerebrales estructurales los analizamos a través de la morfometría
basada en voxels (voxel based morphometry), el grosor cortical y medidas volumétricas.
Resultados: Los aLRRK2 presentaron una disminución en la conectividad funcional entre el tálamo
izquierdo y regiones corticales contralaterales, incluyendo el girus postcentral contralateral,
el girus frontal inferior, el girus temporal medio e inferior y el córtex occipital, comparado con los
no portadores. No encontramos diferencias estructurales entre ambos grupos.
Conclusión: Los aLRRK2 presentaron una disminución en la conectividad funcional en el circuito
tálamo-cortical comparado con los sujetos asintomáticos no portadores. Estos hallazgos apoyan
que las alteraciones de la conectividad funcional preceden el inicio de los síntomas motores
clásicos en esta forma de Parkinson genético.

61
RESULTADOS 6
Abstract
Background: The study of the structural changes and functional connectivity by means of
magnetic resonance imaging (MRI) in asymptomatic LRRK2 mutation carriers could contribute to
the characterization of the preclinical phase of LRRK2 associated PD.
Objective: To characterize MRI functional patterns during resting state in asymptomatic relatives
of LRRK2 associated PD subjects.
Methods: We acquired structural and functional MRI (fMRI) data of 18 asymptomatic LRRK2 carriers
and 18 asymptomatic LRRK2 noncarriers, all first-degree relatives of LRRK2-PD patients. Starting
from fMRI resting state, we analysed the functional connectivity of the nigrostriatal and thala-
mo-striato-cortical circuitry. Structural brain data were analysed by voxel based morphometry,
cortical thickness and volumetric measures.
Results: Asymptomatic LRRK2 mutation carriers had functional connectivity reductions between
the left thalami and contralateral postcentral gyrus, inferior frontal gyrus, middle and inferior
temporal gyrus and occipital cortex compared to LRRK2 noncarriers. No differences in structural
MRI measures were found between subjects in these two groups.
Conclusion: Asymptomatic LRRK2 mutation carriers showed functional connectivity reductions
in thalamo-cortical circuitry compared to noncarriers but no structural abnormalities. These find-
ings support altered brain connectivity preceding the onset of classical motor symptoms in a
genetic form of PD.

62
RESULTADOS6
Background
Mutations in the leucine-rich repeat kinase 2 gene (LRRK2) are the most common known cause of
inherited Parkinson’s disease (PD). Since new therapeutic approaches, such as LRRK2 kinase activity
inhibitors, are moving forward 1, it is important to study the premotor phase of LRRK2 associated
PD (LRRK2-PD) 2. Such treatments when applied in the premotor phases could delay or prevent
the development of the motor syndrome. The study of asymptomatic LRRK2 carriers, a group of
subjects at high risk of developing PD, is a unique opportunity to study premotor LRRK2-PD and
might be crucial for an early disease diagnosis. Already some studies have shown clinical abnor-
malities occurring in asymptomatic LRRK2 carriers 3-8 and Magnetic Resonance Imaging (MRI)
techniques have demonstrated structural and functional abnormalities in these subjects 8-12. From
structural MRI analyses it has been reported gray matter volume (GMV) increases in the caudate
nuclei 9 and in the cuneus 10, and decreases in the right prefrontal and orbitofrontal regions 9.
Task based functional MRI (fMRI) results have shown changes in imagery-related activity in
different cortical and subcortical brain areas 11-12. There is only one study that assessed resting
state (RS) functional connectivity in asymptomatic LRRK2 carriers by means of fMRI 13. In this study,
asymptomatic LRRK2 carriers showed reduced interaction between the connectivity of right
inferior parietal cortex and the dorsoposterior putamen but also an increased interaction of this
cortical area with the ventroanterior putamen.
The aim of the current work was to evaluate whole brain resting-state functional connectivity and
structural brain data in a sample of asymptomatic LRRK2 carriers. We hypothesized that functional
connectivity could be altered in this group of subjects at high risk of developing PD since some
of these subjects may already have subclinical brain dysfunction.

63
RESULTADOS 6
Methods
Participants
Study participants were recruited consecutively between April 2012 and May 2013 among
first-degree relatives of a cohort already identified of LRRK2-PD patients at the Movement Disorders
Unit of Hospital Clínic de Barcelona. Exclusion criteria were presence of parkinsonism, other neuro-
degenerative disorders, and general exclusion criteria for MRI scanning (such as claustrophobia,
pacemaker, and implanted metal parts). Thirty-six first-degree relatives of LRRK2-PD patients, who
came from 17 families, agreed to participate in the study. The presence of a mutation in the LRRK2
gene was assessed as previously described 14. Eighteen were carriers of a mutation in the LRRK2
gene. Among them, thirteen (72.2 %) were carriers of the G2019S, 3 (16.7 %) of the R1441G and
2 (11.1 %) of the R1441C mutations. Participants were not aware of their genetic status at the time
of the study.
Standard protocol approvals and patient consent
The study was approved by the Ethics Committee of Hospital Clínic de Barcelona (May 2012; code 7723)
and a written informed consent was obtained from all study subjects previous to the study.
Clinical assessment
All study participants were clinically evaluated at a single center by the same researcher team (DV, ET,
and CP). Demographic data was collected from all study subjects. Motor symptoms were assessed
through the Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS-III) 15.
None of the participants showed signs of parkinsonism as determined by neurological examina-
tion at the time of the study. Smell was evaluated by means of the 40-items University of Penn-
sylvania Smell Identification Test (UPSIT; Smell Identification TestTMSensonics, Spanish version) 16.
The Hospital Anxiety and Depression scale (HADS) 17 and the Beck Depression Inventory-II 18 were
used to quantify depression and anxiety symptoms. Dysautonomic symptoms were assessed by
means of the SCOPA-AUT scale 19. Global cognitive function was tested by the Mini-Mental State
Examination (MMSE) 20.

64
RESULTADOS6
Statistical analyses of demographic and clinical data
The demographic and clinical data are described by means and standard deviation (SD). Quan-
titative variables were analyzed using Mann-Whitney’s U test for comparisons of two indepen-
dent groups. Qualitative variables were analyzed using Fisher’s exact test. Statistical analyses were
performed with SPSS version 18.0 (SPSS Inc.) with a two-sided Type I error threshold of 5 %. Statis-
tical analyses of MRI studies are detailed in the next section.
MRI acquisition, processing and analyses
Images for all subjects were obtained with a 3T MRI scanner (MAGNETOM Trio, Siemens, Germany),
using an 8-channel head coil. The scanning protocol included a resting-state, 10-min-long functional
gradient-echo echo-planar imaging sequence (300 T2*-weighted volumes, TR = 2 s, TE = 19 ms, flip
angle = 90º, slice thickness = 3 mm, FOV = 240 mm, in which subjects were instructed to keep their
eyes closed, not to think of anything in particular and not to fall asleep), a high-resolution 3D structural
T1-weighted MPRAGE sequence acquired sagitally (TR = 2.3 s, TE = 2.98 ms, 240 slices, FOV = 256 mm;
1 mm isotropic voxel) and a T2-weighted axial FLAIR sequence (TR = 9 s and TE = 96 ms).
Cortical Thickness
Cortical thickness was estimated using the automated FreeSurfer stream (version 5.3; available at:
http://surfer.nmr.harvard.edu). The procedures carried out by FreeSurfer software include removal
of nonbrain data, intensity normalization 21, tessellation of the GM/white matter boundary, auto-
mated topology correction 22-23, and accurate surface deformation to identify tissue borders.
Cortical thickness was calculated as the distance between the white matter and GM surfaces
at each vertex of the reconstructed cortical mantle 24. In our study, results for each subject were
visually inspected to ensure accuracy of registration, skull stripping, segmentation, and cortical
surface reconstruction. Maps were smoothed using a circularly symmetric Gaussian kernel across
the surface with a full width at half maximum (FWHM) of 15 mm. Comparisons between groups
were assessed using a vertex-by-vertex general linear model using Qdec. An initial vertex-wise
threshold was set to p < 0.05 (1.3) to find clusters. To avoid clusters appearing significant purely by
chance (i.e., false positives), MonteCarlo simulation with 10,000 repeats was performed. Results are
reported at cluster-wise probability significance level set at p < 0.05.

65
RESULTADOS 6
Subcortical Volumetry
Total subcortical volumes, as well as thalamus, putamen, caudate, pallidum and estimated
total intracranial volume (eTIV) were obtained automatically via whole-brain segmentation 24.
An analysis of covariance including eTIV was used to compare subcortical volumes between
groups. Significant p values were adjusted using post hoc Bonferroni tests considering the
number of intergroup comparisons.
Voxel based Morphometry
Structural data was analyzed with FSL-VBM 25, a voxel-based morphometry style analysis carried
out with FSL tools. First, nonbrain tissue from structural images was extracted. After segmentation,
GM images were aligned to MNI152 standard space using affine registration. The resulting images
were averaged to create a study-specific template, to which the native GM images were then
non-linearly re-registered. The registered partial volume images were then modulated (to correct
for local expansion or contraction) by dividing by the Jacobian of the warp field. The modulated
segmented images were then smoothed with an isotropic Gaussian kernel with a sigma of 3 mm.
Voxelwise general linear model was applied using non-parametric testing (5,000 permutations).
Significance level was set at p < 0.05, corrected for multiple comparisons using family-wise error
(FWE) control, applied to p value maps obtained from threshold-free cluster enhancement 26.
Processing of fMRI
The preprocessing of resting-state images was performed with FSL (release 5.0.4,
http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FSL) and AFNI (http://afni.nimh.nih.gov/afni). Briefly, it included
removal of the first 5 volumes to allow for T1 saturation effects, skull stripping, grandmean scaling,
and temporal filtering (0.01 - 0.1 Hz). To control for the effect of subject head movement, physio-
logical artifacts, and other nonneural sources of signal variation on the estimation of connectivity,
motion correction and regression of nuisance signals (six motion parameters, cerebrospinal fluid,
and WM) were performed. To remove the effects of images corrupted by motion, a scrubbing
procedure as suggested by Power et al. 27 was applied. Images were then smoothed with a 6-mm
FWHM Gaussian kernel. Resampling resolution was set to 4 mm. Additionally, head motion was

66
RESULTADOS6
calculated as the average Euclidean displacement between consecutive timepoints for rotatory
and translatory motion 28.
Definition of Regions of Interest
Regions of interest (ROI), including thalamus and striatum were created based on the Harvard-Ox-
ford probabilistic subcortical atlas 29 and http://www.cma.mgh.harvard.edu/fsl_atlas.html). Addi-
tionally, 8 mm spherical ROIs centered on peak voxels corresponding to MNI coordinates
11, -16, -12 and -11, -16,-12 were created to study the FC of the substantianigra (SN). Supplementary
Figure 1 displays the ROI segmentation scheme used. To obtain each seed region’s resting-state
functional MRI (fMRI) time series, the mask for each structure was linearly registered to each subject’s
T1-weighted image, and subsequently linearly registered to native functional space using FSL FLIRT.
Functional connectivity analysis
Mean time series was obtained from each seed region (SN, caudate, putamen and thalamus per
hemisphere) by averaging the time series of every voxel contained in it before smoothing, in
native functional space. Subsequently, these time series were correlated with the time series of
every voxel inside the brain, thus producing a Pearson’s r coefficient correlation map. These were
then converted to z maps, using Fisher’s r-to-z transformation. Voxelwise general linear model was
applied using non-parametric testing (5,000 permutations) including all brain voxels. Significance
level was set at p < 0.05, corrected for multiple comparisons using FWE control, applied to p value
maps obtained from threshold-free cluster enhancement 26.
Image analysis was performed by two independent investigators (BS and HB) blinded to the
clinical and genetic status of study subjects.

67
RESULTADOS 6
Results
Demographic and clinical data
Mean age was similar between carriers and noncarriers with a similar range of age (27 to 66 years
and 23 to 67 years, respectively) (Table 1). Years of education were similar in both groups.
No significant differences were found in the scores of the UPDRS I, II or III between both groups.
The UPSIT score was also similar in both groups. No significant differences in scores were found
for other non-motor symptoms.
Functional connectivity
Asymptomatic LRRK2 carriers showed differences in functional connectivity differences compared
to asymptomatic noncarriers. We observed functional connectivity reductions between the left
thalamic seed and contralateral cortical areas, including the postcentral gyrus, inferior frontal gyrus,
middle and inferior temporal gyrus, and occipital cortex (p < 0.05 FWE-corrected) (Table 2, Figure 1
and Supplementary Figure 2). Functional connectivity was also reduced between left caudate and
bilateral precentral and postcentral gyrus (left postcentralgyrus; MNI coordinates = -50, -14, 32;
cluster size = 128 mm3, p = 0.034 and right precentral; MNI coordinates 50, 2, 40: cluster size = 64 mm3
p = 0.049, and Supplementary Figure 3). Using a more liberal threshold of FWE-corrected p < .06,
we observed additional areas showing functional connectivity reduction in the motor cortex
bilaterally (left precentral gyrus: MNI coordinates -50, -10, 32, cluster size = 960 mm3 p = 0.056 FWE
corrected; and right precentral gyrus: MNI coordinates 2, -25, 72, cluster size = 1792 mm3 p = 0.054
FWE-corrected). The right primary somatosensorial cluster described above extended to
premotor and primary motor regions (MNI coordinates 34, -38, 75, cluster size = 321 mm3, p = 0.033
FWE-corrected) (see Supplementary Figure 4). No other significant functional connec-
tivity increases or decreases were found when other seed regions were tested. Carriers and
noncarriers moved similarly in all 3 axes during scanning (rotatory head motion (degrees):
carriers 0.03 ± 0.01, noncarriers 0.03 ± 0.02, p = 0.662; translatory head motion (mm):
carriers 0.07 ± 0.03, noncarriers: 0.06 ± 0.05; p = 0.445).

68
RESULTADOS6
Structural MRI findings
Gray matter volumes (VBM analysis and volumetric measures) and cortical thickness measures did
not differ between groups (Table 3).
Discussion
Asymptomatic LRRK2 carriers, in this study, showed functional connectivity reductions between
the left thalamus and contralateral cortical areas including postcentral gyrus, inferior frontal
gyrus, middle and inferior temporal gyrus and occipital cortex, and also between left caudate
and bilateral sensorimotor cortex. We also observed a potential functional connectivity reduction
between the left thalami and bilateral motor cortex, as well as from primary somatosensorial
regions to primary motor cortex.
These results, in preclinical PD, are in line with previous resting-state fMRI studies in manifest
PD that have found decreased functional connectivity between thalamus and sensorimotor
cortices 30 and between the striatum and thalamus, midbrain, pons and cerebellum 31. Even in
untreated patients in early stages of PD decreased functional connectivity of caudate and thal-
amus with frontal and insular cortices 32 and in mesolimbic-striatal and corticostriatal loops 33
has been observed. In addition our results suggest that decrements in functional connectivity
occur in asymptomatic LRRK2 carriers before structural MRI changes can be detected. There are
no published studies describing connectivity changes in the preclinical phases of idiopathic PD.
Decreases in functional connectivity in preclinical stages have been found in other neurodegen-
erative diseases such as Alzheimer’s, mainly in limbic regions, such as the hippocampus, parahip-
pocampus, anterior cingulate and middle temporal cortex 34. In preclinical Huntington disease
weakened and strengthened connectivity has been observed in the frontostriatal network, but
also included the thalamus, anterior insula, and memory centres 35.
In contrast with previous studies in idiopathic PD 36-37 and in the preclinical phase of LRRK2-PD 11-13
we did not observe functional connectivity increments, which possibly are reflecting compensa-
tory mechanisms. Different methods used in these task-based studies could in part explain the

69
RESULTADOS 6
different results. Another reason for the discrepancy might be that our study subjects could still
be far from the onset of motor symptoms- and we might have detected RS functional connec-
tivity decrements that appear before potential compensatory increments such as those previ-
ously described in PD. Increased connectivity of ventral attention areas and parietal cortex with
frontal cortex, thalamus and cerebellum has been observed in prodromal Huntington disease
near to diagnosis, but not in early stages where only connectivity decreases has been found 35.
We did not find in the asymptomatic carriers volumetric brain changes described in idiopathic
and LRRK2-PD. This finding might support the idea that our study subjects are in very early stages
of the neurodegenerative process and that functional changes precede structural abnormalities.
Other neuroimaging changes such as those occurring in the nigrostriatal pathways assessed by
means of the DAT-SPECT or substantia nigra echogenicity on transcranial sonography have iden-
tified asymptomatic LRRK2 carriers with presumed ongoing disease process 38-39. We did not find
any functional connectivity differences involving the substantia nigra in our study. Functional
connectivity changes linked to involvement of the nigrostriatal pathway may appear later, as the
disease progresses to involve more rostral structures, and possibly cannot be identified in the
premotor phase. Also, the small size of the substantia nigra, alongside the known susceptibility of
brainstem regions to physiological noise 40, may limit the sensitivity of fMRI connectivity assess-
ments in this region.
Small sample size, as well as the inclusion of subjects with different LRRK2 mutations, potentially
with different underlying pathogenic mechanisms should be considered limitations when inter-
preting our results. Also since the age dependent penetrance of LRRK2 mutations is incomplete,
some of our study subjects, like those in previous studies 11-13, may not have any ongoing neuro-
degenerative process at the time we scanned them. Regrettably markers to select those cases
with ongoing neurodegeneration are not available. Another limitation of our study is the lack for
comparison purposes of either healthy controls unrelated to LRRK2-PD patients nor a group of
overt LRRK2-PD patients. The coupled connectivity and structural analyses, along with the strin-
gent adjust for multiple corrections, are strengths to the study.

70
RESULTADOS6
In conclusion, this study showed reduced thalamo-cortical functional connectivity in this specific
cohort of subjects without parkinsonismat risk of developing LRRK2-PD, in the absence of signif-
icant structural changes. Future studies should assess the correlation between the functional
connectivity alterations in fMRI and other risk markers such as nigrostriatal degeneration or hyper-
echogenicity of the substantia nigra in this specific cohort of subjects.
Barcelona LRRK2 study group
Parkinson’s Disease and Movement Disorders Unit, Neurology Service, Institut de Neurociències
Hospital Clínic, University of Barcelona: Eduard Tolosa, María José Martí, Yaroslau Compta, Francesc
Valldeoriola, Dolores Vilas, Claustre Pont-Sunyer. Neurology Service, Hospital Universitari Germans
Trias i Pujol, Badalona: Lourdes Ispierto, Ramiro Álvarez. Neurology Service, Hospital Universitari
Vall D’Hebron, Barcelona: Oriol De Fabregues, Jorge Hernández-Vara. Neurology Service, Hospital
Del Mar, Barcelona: Víctor Puente. Neurology Service, Hospital Universitari de Bellvitge, Barcelona:
Matilde Calopa, Serge Jaumà, Jaume Campdelacreu. Neurology Service, Hospital Universitari
Mutua de Terrasa, Barcelona: Miquel Aguilar, Pilar Quílez. Hospital Mateu Orfila, Maó, Menorca:
Pilar Casquero.
Acknowledgments
The authors are grateful to the patients and the families for their participation in the study.

71
RESULTADOS 6
Asymptomatic LRRK2 carriers
(n = 18)
Asymptomatic noncarriers
(n = 18)p
Age, years 43.33 ± 12.07 44.72 ± 12.48 0.736
Gender, % male 9 (50 %) 7 (38.9 %) 0.584
Mutation, n (%)G20195R1441CR1441G
13 (72.2 %)2 (11.1 %)3 (16.7 %)
NA
Years of education 13.44 ± 5.08 15.28 ± 4.66 0.267
UPDRS I score 2.89 ± 4.52 2.39 ± 3.70 0.719
UPDRS II score 0.22 ± 0.43 0.28 ±0.58 0.744
UPDRS III score 0.39 ± 0.98 0.06 ±0.24 0.169
UPSIT score 32.72 ± 3.74 33.0 ± 3.45 0.818
SCOPA-AUT score 8.44 ± 6.68 7.56 ± 4.88 0.651
HADS total score 8.0 ± 5.69 7.83 ± 6.05 0.933
HADS Anxiety score 5.17 ± 3.26 5.39 ± 3.24 0.839
HADS Depression score 2.83 ± 2.68 2.44 ± 3.37 0.704
BDI score 5.12 ± 6.19 4.06 ± 4.87 0.575
MMSE score 29.17 ± 0.92 29.17 ± 0.99 1.0
Table 1: Demographic and clinical data
Results were described by mean and standard deviation ± SD. Quantitative variables were
analysed using Mann-Whitney`s U test. Qualitative variables were described by absolute
and relative frequencies and analysed by Fisher’s Exact test.
BDI: Beck Depression Inventory-II. HADS: Hamilton Anxiety and Depression Scale.
MMSE: Mini-mental state examination. SCOPA-AUT: Scales for Outcomes in Parkinson’s disease-Au-
tonomic. UPDRS: unified Parkinson’s disease rating scale. UPSIT: University of Pennsylvania Smell
Identification Test.
Topography Volume (mm3) VoxelsMNI coordinates
(x,y,z)p value
Right occipital pole 7104 111 26, -94, -8 0.025
Right postcentralgyrus 6592 103 34, -38, 76 0.033
Right lateral occipital Cortex/cuneus/occipital pole
1024 16 14, -86, 24 0.036
Right inferior frontal gyrus,pars opercularis
960 15 11, 36, 22 0.029
Left inferior temporal gyrus 576 9 -54,-46, -12 0.043
Table 2: Differential left thalamo-cortical connectivity in asymptomatic LRRK2 carriers and noncarriers
Description of clusters of significant between group left thalamo-cortical connectivity differences
(p< 0.05 FWE-corrected). Asymptomatic LRRK2 carriers showed reduced left thalamo-cortical
connectivity compared to noncarriers.

72
RESULTADOS6
Asymptomatic LRRK2 carriers
n = 18
Asymptomatic noncarriers
n = 17t p value
L thalamus 7.37 ± 1.18 7.04 ± 0.94 0.927 0.361
L caudate 3.78 ± 0.65 3.76 ± 0.61 0.100 0.921
L putamen 5.67 ± 1.04 5.44 ± 1.05 0.665 0.511
L pallidum 1.78 ± 0.29 1.75 ± 0.21 0.397 0.694
R thalamus 7.51 ± 0.90 7.08 ± 0.93 1.370 0.180
R caudate 3.74 ± 0.65 3.78 ± 0.60 -0.189 0.852
R putamen 5.31 ± 0.84 4.98 ± 0.90 1.136 0.264
R pallidum 1.51 ± 0.30 1.51 ± 0.20 -0.028 0.978
Table 3: Volumetric measures of the subcortical seed regions.
Volumetric measures of the subcortical seed regions corrected by estimated total intracranial
volume. Results were described by mean and standard deviation (SD) and expressed in cm3.
L = left. R = right.
P
R
R L
z = 56 z = 60
z = 12
y = 12
x = 30
y = 44
A
L
R
R
R L
L
L
Figure 1: Differential left thalamo-cortical connectivity between asymptomatic
LRRK2 carriers and noncarriers
Connectivity differences between asymptomatic LRRK2 carriers and non-carriers(carriers< noncarriers).
Color clusters indicate areas of significant (p< 0.05, FWE correction) differences in left thalamo-cortical
connectivity. The Montreal Neurological Institute coordinates of the slices shown are indicated.
R: right. L: left, A: anterior, P: posterior.

73
RESULTADOS 6
L R
Supplementary Figure 1: Seed regions.
Seed regions overlaid onto the structural Montreal Neurological Institute standard MRI template. For graphical
purposes, original masks were resampled to 1mm resolution
-0 .20
-0 .10
0 .00
0 .10
0 .20
0 .30
Mea
n c
on
nec
tivi
ty
Asymptomatic carriers Noncarriers
Supplementary Figure 2: Mean connectivity in left thalamo-cortical significant
clusters between asymptomatic LRRK2 carriers and noncarriers (carriers< noncarriers)

74
RESULTADOS6
z = 39 z = 32
R LR L
Supplementary Figure 3: Differential left caudate connectivity between asymptomatic
LRRK2 carriers and noncarriers.
Connectivity differences between asymptomatic LRRK2 carriers and noncarriers. (carriers < noncarriers)
Color clusters indicate areas of significant (p< 0.05, family-wise error correction) differences in left caudate-cortical
connectivity. The Montreal Neurological Institute coordinates of the slices shown are indicated.
L: left. R: right.

75
RESULTADOS 6
P A
x = 34
R L
z = 59
R L
z = 40
P A
x = 54
R L
y = -6
R L
y = 44
Supplementary Figure 4: Differential left thalamo-cortical connectivity between
asymptomatic LRRK2 carriers and noncarriers.
Significant connectivity differences between asymptomatic LRRK2 carriers and noncarriers.
(carriers < noncarriers). Color clusters indicate areas of significant (p< 0.06 family-wise error
correction) with a cluster extent threshold of 10 voxels. The Montreal Neurological Institute
coordinates of the slices shown are indicated.
R: right. L: left, A: anterior, P: posterior.

76
RESULTADOS6
References
1. West AB. Ten years and counting: moving leucine-rich repeat kinase 2 inhibitors to the clinic. MovDisord 2015;30(2):180-9.
2. Tolosa E, Gaig C, Santamaria J, Compta Y. Diagnosis and the premotor phase of Parkinson disease. Neurology 2009;72(7 Suppl):S12-20.
3. Healy DG, Falchi M, O’Sullivan SS, et al. Phenotype, genotype, and worldwide genetic penetrance of LRRK2-associated Parkinson’s disease: a case-control study. Lancet Neurol 2008;7(7):583-90.
4. Gaig C, Vilas D, Infante J, et al. Nonmotor symptoms in LRRK2 G2019S associated Parkinson’s disease. PLoS One 2014;9(10):e108982.
5. Marras C, Schule B, Munhoz RP, et al. Phenotype in parkinsonian and nonparkinsonian LRRK2 G2019S muta-tion carriers. Neurology 2011;77(4):325-33.
6. van der Vegt JP, van Nuenen BF, Bloem BR, Klein C, Siebner HR. Imaging the impact of genes on Parkinson’s disease. Neuroscience 2009;164(1):191-204.
7. Adams JR, van Netten H, Schulzer M, et al. PET in LRRK2 mutations: comparison to sporadic Parkinson’s disease and evidence for presymptomatic compensation. Brain 2005;128(Pt 12):2777-85.
8. Sierra M, Sanchez-Juan P, Martinez-Rodriguez MI, et al. Olfaction and imaging biomarkers in premotor LRRK2 G2019S-associated Parkinson disease. Neurology 2013;80(7):621-6.
9. Reetz K, Tadic V, Kasten M, et al. Structural imaging in the presymptomatic stage of genetically determined parkinsonism. NeurobiolDis 2010;39(3):402-8.
10. Brockmann K, Groger A, Di Santo A, et al. Clinical and brain imaging characteristics in leucine-rich repeat kinase 2-associated PD and asymptomatic mutation carriers. MovDisord 2011;26(13):2335-42.
11. Thaler A, Mirelman A, Helmich RC, et al. Neural correlates of executive functions in healthy G2019S LRRK2 mutation carriers. Cortex 2013;49(9):2501-11.
12. van Nuenen BF, Helmich RC, Ferraye M, et al. Cerebral pathological and compensatory mechanisms in the premotor phase of leucine-rich repeat kinase 2 parkinsonism. Brain 2012;135(Pt 12):3687-98.
13. Helmich RC, Thaler A, van Nuenen BF, et al. Reorganization of corticostriatal circuits in healthy G2019S LRRK2 carriers. Neurology 2015;84(4):399-406.
14. Gaig C, Ezquerra M, Marti MJ, Munoz E, Valldeoriola F, Tolosa E. LRRK2 mutations in Spanish patients with Parkinson disease: frequency, clinical features, and incomplete penetrance. Arch Neurol 2006;63(3):377-82.
15. Goetz CG, Tilley BC, Shaftman SR, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. MovDisord 2008;23(15):2129-70.
16. Doty RL, Bromley SM, Stern MB. Olfactory testing as an aid in the diagnosis of Parkinson’s disease: develop-ment of optimal discrimination criteria. Neurodegeneration 1995;4(1):93-7.
17. Zigmond AS, Snaith RP. The hospital anxiety and depression scale.ActaPsychiatrScand 1983;67(6):361-70.
18. Beck AT SRA, & Brown, G.K. TX: Psychological corporation. Manual for the Beck depression Inventory. 1996.

77
RESULTADOS 6
19. Visser M, Marinus J, Stiggelbout AM, Van Hilten JJ. Assessment of autonomic dysfunction in Parkinson’s disease: the SCOPA-AUT. MovDisord 2004;19(11):1306-12.
20. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12(3):189-98.
21. Fischl B, Liu A, Dale AM. Automated manifold surgery: constructing geometrically accurate and topologically correct models of the human cerebral cortex. IEEE Trans Med Imaging 2001;20(1):70-80.
22. Segonne F, Pacheco J, Fischl B. Geometrically accurate topology-correction of cortical surfaces using nonseparating loops. IEEE Trans Med Imaging 2007;26(4):518-29.
23. Dale AM, Fischl B, Sereno MI. Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage 1999;9(2):179-94.
24. Fischl B, Salat DH, Busa E, et al. Whole brain segmentation: automated labeling of neuroanatomical struc-tures in the human brain. Neuron 2002;33(3):341-55.
25. Douaud G, Smith S, Jenkinson M, et al. Anatomically related grey and white matter abnormalities in adoles-cent-onset schizophrenia. Brain 2007;130(Pt 9):2375-86.
26. Winkler AM, Ridgway GR, Webster MA, Smith SM, Nichols TE. Permutation inference for the general linear model.Neuroimage 2014;92:381-97.
27. Power JD, Barnes KA, Snyder AZ, Schlaggar BL, Petersen SE. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. Neuroimage 2012;59(3):2142-54.
28. Liu Y, Liang M, Zhou Y, et al. Disrupted small-world networks in schizophrenia. Brain 2008;131(Pt 4):945-61.
29. Smith SM, Jenkinson M, Woolrich MW, et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 2004;23Suppl 1:S208-19.
30. Sharman M, Valabregue R, Perlbarg V, et al. Parkinson’s disease patients show reduced cortical-subcortical sensorimotor connectivity. MovDisord 2013;28(4):447-54.
31. Hacker CD, Perlmutter JS, Criswell SR, Ances BM, Snyder AZ. Resting state functional connectivity of the stri-atum in Parkinson’s disease. Brain 2012;135(Pt 12):3699-711.
32. Agosta F, Caso F, Stankovic I, et al. Cortico-striatal-thalamic network functional connectivity in hemiparkin-sonism. Neurobiol Aging 2014;35(11):2592-602.
33. Luo C, Song W, Chen Q, et al. Reduced functional connectivity in early-stage drug-naive Parkinson’s disease: a resting-state fMRI study. Neurobiol Aging 2014;35(2):431-41.
34. Sheline YI, Raichle ME, Snyder AZ, et al. Amyloid plaques disrupt resting state default mode network connec-tivity in cognitively normal elderly. Biol Psychiatry 2010;67(6):584-7.
35. Harrington DL, Rubinov M, Durgerian S, et al. PREDICT-HD investigators of the Huntington Study Group, Rao SM. Network topology and functional connectivity disturbances precede the onset of Huntington’s disease.Brain. 2015 Aug;138(Pt 8):2332-46. 36.
36. Baudrexel S, Witte T, Seifried C, et al. Resting state fMRI reveals increased subthalamic nucleus-motor cortex connectivity in Parkinson’s disease. Neuroimage 2011;55(4):1728-38.

78
RESULTADOS6
37. Yu R, Liu B, Wang L, Chen J, Liu X. Enhanced functional connectivity between putamen and supplementary motor area in Parkinson’s disease patients. PLoSOne 2013;8(3):e59717.
38. Sierra M, Sanchez-Juan P, Martinez-Rodriguez MI, et al. Olfaction and imaging biomarkers in premotor LRRK2 G2019S-associated Parkinson disease. Neurology 2013;80(7):621-26.
39. Vilas D, Ispierto L, Alvarez R, et al. Clinical and imaging markers in premotor LRRK2 G2019S mutation carriers. Parkinsonism RelatDisord 2015.
40. Brooks JC, Faull OK, Pattinson KT, Jenkinson M. Physiologicalnoise in brainstem FMRI.Front HumNeurosci. 2013 Oct 4;7:623.

79
RESULTADOS 6
Trabajo número 4
Cerebrospinal fluid biomarkers and clinical features in leucine-rich repeat kinase 2 (LRRK2) mutation carriers
Dolores Vilas, Leslie M Shaw, Peggy Taylor, Daniela Berg, Kathrin Brockmann, Jan Aasly,
Connie Marras, Claustre Pont-Sunyer, José Ríos, Ken Marek, Eduardo Tolosa.

80
RESULTADOS6
Biomarcadores en líquido cefalorraquídeo y rasgos clínicos en portadores de una
mutación en el gen LRRK2
Antecedentes: Las mutaciones en el gen LRRK2 son la causa más frecuente de EP hereditaria. Los
aLRRK2 son sujetos en riesgo de desarrollar EP y suponen una oportunidad única para el estudio
de biomarcadores como predictores de conversión a EP. La información disponible actualmente
sobre los biomarcadores en líquido cefalorraquídeo (LCR) en la EP-LRRK2 y en aLRRK2 es preliminar.
Objetivos: Medir los niveles de α-syn, Aβ1-42, T-tau, y p-tau181 en EP-LRRK2, EPI, aLRRK2 y familiares de
primer grado de pacientes EP-LRRK2, no portadores de la mutación. Correlacionar los rasgos clínicos y
la integridad de la vía nigroestriatal medida por neuroimagen con los biomarcadores de LCR.
Métodos: Analizamos 138 muestras de LCR provenientes del LRRK2 Cohort Consortium de la
Michael J Fox Foundation: 28 EP-LRRK2, 35 EPI, 41 aLRRK2 y 34 familiares no portadores. Todos los
participantes se evaluaron clínicamente. En la mayoría de los participantes se realizó además un
SPECT con transportador de dopamina para evaluar la integridad de la vía nigroestriatal.
Resultados: Los niveles de α-syn fueron similares entre los EP-LRRK2, los aLRRK2 y los familiares
asintomáticos no portadores pero significativamente más elevados que en los pacientes con EPI
(p = 0.041). No encontramos diferencias entre las concentraciones de Aβ1-42, T-tau, y p-tau181 entre
los grupos. Los niveles de α-syn en LCR mostraron una fuerte correlación con los niveles de T-tau,
y p-tau181 en todos los grupos. También se observó una correlación, aunque más débil, entre los
niveles de α-syn y Aβ1-42. Los niveles de T-tau fueron más elevados en el fenotipo de inestabilidad
postural y trastorno de la marcha que en el fenotipo tremórico en los EP-LRRK2; sin embargo, los
niveles de Aβ1-42 fueron más elevados en el fenotipo tremórico en los EPI. No se observaron corre-
laciones entre los biomarcadores en LCR y la captación estriatal en el DAT-SPECT en los aLRRK2.
Conclusión: El perfil de proteínas en LCR es diferente en EP-LRRK2 y en EPI sugiriendo que los
mecanismos fisiopatológicos de EP-LRRK2 Y EPI son diferentes. Los biomarcadores de LCR no han
demostrado ser útiles en la diferenciación de los aLRRK2 con los familiares no portadores de la
mutación.

81
RESULTADOS 6
Abstract
Background: Mutations in the leucine-rich repeat kinase 2 (LRRK2) gene are the most common
cause of inherited Parkinson’s disease (PD). Nonmanifesting carriers of LRRK2 mutations are subjects
at high risk for developing PD. Information available on cerebrospinal fluid (CSF) biomarkers in
LRRK2 carriers remains preliminary.
Objectives: To measure CSF levels of alpha-synuclein, β amyloid1-42, Total-tau, and Phospho-tau181,
in LRRK2-PD, idiopathic PD (IPD), nonmanifesting carriers (NMC) and first-degree relatives of
LRRK2-PD patients without the mutation (nonmanifesting noncarriers; NMNC). To correlate the
clinical features and the integrity of the nigrostriatal pathway assessed by neuroimaging with the
CSF biomarkers.
Methods: 138 CSF samples provided by the Michael J. Fox Foundation LRRK2 Cohort Consortium
were analyzed: 28 LRRK2-PD, 35 IPD, 41 NMC and 34 NMNC. All the participants in the study were
clinically assessed. Most of the participants underwent a dopamine transporter scan to assess the
integrity of the nigrostriatal pathway.
Results: CSF levels of alpha-synuclein were similar in LRRK2-PD, NMC and NMNC but significantly
higher than in IPD (p = 0.041). No differences were found in the concentrations of β amyloid1-42,
Total-tau, and Phospho-tau181 among study groups. CSF alpha-synuclein levels strongly correlated
with Total-tau, and Phospo-tau181 levels in all groups. No significant correlation was found between
the cerebrospinal fluid biomarkers and the striatal binding ratios in nonmanifesting carriers.
Conclusion: CSF protein profile differs in LRRK2-PD and IPD suggesting that pathophysiological
mechanisms different from IPD underlie LRRK2-PD. Cerebrospinal fluid biomarkers did not prove
helpful in differentiating asymptomatic LRRK2 mutation carriers from noncarriers.

82
RESULTADOS6
Background
Mutations in the leucine-rich repeat kinase 2 (LRRK2) gene are the most common cause of
inherited Parkinson’s disease (PD) 1,2. Asymptomatic (nonmanifesting) LRRK2 mutations carriers
(NMC), at high risk for developing PD, provide a unique opportunity for the study of biomarkers
as predictors of PD conversion. There is an urgent need for biomarkers to diagnose LRRK2-PD at
the earliest stage, especially since LRRK2 kinase inhibitors are moving closer to enter clinical trials 3.
Cerebrospinal fluid (CSF) proteins have been proposed as a potentially reliable biomarker
source. Alpha-synuclein (α-syn) is potentially the most promising CSF biomarker since it could
reflect underlying Lewy body pathology, the hallmark of PD. CSF α-syn levels have been assessed
in idiopathic PD (IPD) and a drop in CSF total α-syn was found 4-9 even in early stages of the disease 8,
while levels of oligomeric α-syn appear to be increased 8, 10-12. CSF biomarkers of Alzheimer’s
disease (AD) pathology have also been investigated in PD and CSF amyloid-beta (Aβ1-42) levels
have been reported to be lower in IPD compared to controls in some studies 4, 13 but not others6, 14-17.
Studies measuring CSF total tau (T-tau) and phospho-tau (p-tau181) have also shown variable
results 4-7, 13-19. In IPD abnormal CSF protein levels have been correlated with cognitive distur-
bances 13, 15, 20-24.
Information available on α-syn and AD-type CSF levels in LRRK2 mutation carriers remains prelim-
inary pointing to some degree of abnormalities 25-27. An increment in α-syn oligomers in NMC has
been reported 27. Also in NMC reduced CSF Aβ and tau levels were found to correlate with lower
striatal dopaminergic function 25.
The aim of the present study was to determine CSF levels of α-syn, Aβ1-42, T-tau, and p-tau181,
in LRRK2-PD, IPD, and asymptomatic first-degree relatives of LRRK2-PD. We hypothesized that the
CSF α-syn and AD-type proteins levels might differentiate both forms of PD and also NMC from
noncarriers. A secondary objective was to study whether protein levels could reflect clinical or
imaging abnormalities in NMC.

83
RESULTADOS 6
Methods
Established in 2009, the Michael J. Fox Foundation (MJFF) LRRK2 Cohort Consortium (LCC) brought
together investigators from 22 different sites worldwide (North America, Europe, North Africa,
and Asia) to study individuals with mutations in the LRRK2 gene.
The study cohort comprises four different categories of subjects: subjects who carry a mutation
in the LRRK2 gene and have PD (LRRK2-PD), subjects who carry a mutation in the LRRK2 gene and
do not have a clinical diagnosis of PD (yet) (non-manifesting carriers; NMC), subjects who have
a confirmed clinical diagnosis of PD but do not carry a LRRK2 mutation (IPD), and subjects who
do not carry a mutation in the LRRK2 gene and do not manifest PD at the time of enrollment
(nonmanifesting non-carriers; NMNC). The latter group was comprised primarily of non-carrying
first degree relatives of probands.
All participants in the study were comprehensively assessed for clinical characteristics by the site
investigators. Demographic information, disease severity based on the Unified Parkinson’s disease
Rating Scale rating scale (UPDRS) 28, the Movement Disorder Society-sponsored revision of the
Unified Parkinson’s disease Rating Scale (MDS-UPDRS) 29 and the Hoehn and Yahr (HY) stage 30,
and results of cognitive function tests, were downloaded from the LRRK2 Cohort Consortium
database according to guidelines for data Access and use. For this study, we classified PD as mani-
festing the tremor dominant (TD-PD), postural instability and gait disorder (PIGD-PD), or inter-
mediate (IND-PD) phenotype as previously described 31. Most of the participants underwent a
dopamine transporter (DAT) scan to assess the integrity of the nigrostriatal pathway. The images
obtained at each center were analyzed in an Imaging Core (Institute for Neurodegenerative Disor-
ders, New Haven, Connecticut).
A total of 142 participants in the LRRK2 Cohort Consortium study accepted to undergo a lumbar
puncture to obtain CSF. Four of them were excluded of the analyses because of lack of clinical
data or genetic status. We report here results from analyses of CSF specimens from 138 partici-
pants: 28 LRRK2-PD, 35 IPD, 41 NMC and 34 NMNC.

84
RESULTADOS6
The study was approved by the institutional review board of all participating sites. Written
informed consent was obtained from all participants before inclusion in the study.
CSF sample collection and handling
CSF collection was performed at each study site as described in the Parkinson’s progression
markers initiative (PPMI) biologics manual (http://ppmi-info.org) and previously reported 5. Briefly, all
the lumbar punctures were performed between 8 am and 10 am after an 8-hours fasted. CSF was
collected into siliconize polypropylene tubes, and the first 1 to 2 ml of CSF were sent to the site’s
local laboratory for routine testing for cell count, total protein level, and glucose level. An addi-
tional 15 to 20 ml of CSF was transferred into 15 ml conical polypropylene tubes at room tempera-
ture, mixed gently, centrifuged at 2000g for 10 minutes at room temperature, and transferred into
1.5 ml precooled siliconized polypropylene aliquot tubes followed by immediate freezing on dry
ice. The frozen aliquots of CSF were shipped to the LRRK2 Cohort Consortium biorepository Core
Laboratories on dry ice and then thawed, aliquoted into 0.5-mL siliconized polypropylene tubes,
refrozen once, and stored at –80°C. Coded frozen aliquots from the CSF samples were transferred
to the University of Pennsylvania and to Covance for the studies described here.
Analysis of CSF biomarkers
Measurements of Aβ1-42, T-tau, and p-tau181 were performed in each of 138 CSF aliquots at the
University of Pennsylvania. CSF Aβ1-42, T-tau and p-tau181 were measured using the xMAP-Luminex
platform with INNOBIA AlzBio3 immunoassay kit-based reagents (Fujirebio-Europe, Ghent, Belgium),
as described previously 4. Following the standardized operation protocol (SOP) of the University of
Pennsylvania Biomarker Core laboratory, duplicate 75μL aliquots of standards, aqueous controls
and CSF samples (including two CSF pools, one normal and one abnormal, for quality control) were
analyzed, and a total of 10 runs showed mean variability in the concentration (% CV) of Aβ1-42, T-tau
and p-tau181 in two CSF pools were 5.3 and 9.7 %, 9.4 and 8.0 %, 6.4 and 6.7 % respectively.
CSF α-syn was analyzed at BioLegend using an ELISA assay available commercially from BioLegend
(cat # 844101, formerly SIG-38974-kit). The method of analysis is a sandwich type ELISA that utilizes

85
RESULTADOS 6
a luminescent readout. The reference standards used in the assay ranged from 6.1-1500 pg/ml.
The concentration of α-syn in each sample was determined by interpolation of values against the
standard curve established by the reference standards using a 4-parameter regression. Recombi-
nant α-syn from rPeptide was used as the standard in this assay. Each CSF sample was analyzed
in duplicate at a 1:20 dilution. On each plate 2 CSF samples were included as QC samples. The
QC samples were run in duplicate at 1:10 and 1:20 dilution and the interpolated values, adjusted
for dilution factor, were compared across the plates used in this analysis (eTable 1). Plate accep-
tance criteria were set as: Replicate standard curve calibrators must be less than 15 % CV and QC
samples must read within the established range (mean±1SD).
CSF hemoglobin measurement was included as an assessment of blood contamination in the CSF
because red blood cells are rich in hemoglobin and may affect the analysis. CSF hemoglobin (Hb)
was analyzed at BioLegend using an ELISA assay comprising reagents obtained from Bethyl Labo-
ratories (cat # E80-135). The method of analysis is a sandwich type ELISA that utilizes a colorimetric
readout. The reference standards used in the assay ranged from 7.5-125 ng/ml. The concentration
of hemoglobin in each sample was determined by interpolation of values against the standard
curve established by the reference standards using a 4-parameter regression. Each CSF sample
was analyzed in duplicate at a 1:10 dilution. On each plate 2 CSF samples spiked with hemoglobin
(Fisher cat # 23-666-304) were included as QC samples. The QC samples were run in duplicate at 1:4,
1:20 and 1:100 dilution and the interpolated values, adjusted for dilution factor, were compared
across the plates used in this analysis. (eTable 2). For QC sample 1 the 1:4 and 1:20 dilutions were
averaged and reported. For QC sample 2 the 1:20 and 1:100 dilutions were averaged and reported.
Plate acceptance criteria were set as: Replicate standard curve calibrators must be less than 15 %
CV and QC samples must read within the established range (mean±1SD). The CSF analyses were
performed in a blinded manner. After completion of these CSF biomarker analyses, the code was
opened by someone independent from the labs conducting the work.

86
RESULTADOS6
Statistical Analysis
Quantitative results were described by median and interquartile range [Percentiles 25th, 75th] and
analysed using Kruskall-Wallis test for overall comparisons, and Mann-Whitney U test for pair-wise
comparisons. Qualitative variables were described by absolute and relative frequencies (%) and
analysed by Fisher’s Exact test. In order to not increase the multiplicity in the statistical compar-
isons between groups, this pair-wise comparison was only performed if the overall compar-
ison was statistically significant. To explore the relationship between α-syn levels and other CSF
biomarkers we used a Rho Spearman correlation analysis for the entire sample and stratified by
each group. We assessed the concentrations of the CSF biomarkers among groups based on two
fixed cut-off points for the α-syn levels previouslly described (200 ng/mL and 500 ng/mL) 5 using
Mann-Whitney U test. To evaluate the effect of hemoglobin and age for differences between
groups we used general linear models (GLM) with a nonparametric approach, by rank-transfor-
mation of, alpha-synuclein, Aß, T-tau and p-tau181 as dependent variables and the group as main
factor with hemoglobin level as a covariate. Statistical analysis was performed using SPSS version
20.0 (IBM) and a two-sided Type I error of 5 % was used in all analyses.
Results
Demographic and clinical data
Demographic and general information are summarized in Table 1. Disease duration was longer in
the LRRK2-PD than in the IPD patients (8 [2;13] vs 4 [0;6]; p = 0.008) but age at the onset of motor
symptoms and age at PD diagnosis was similar in both groups. Twenty (71.4 %) LRRK2-PD patients
and 31 (75.6 %) NMC were carriers of the G2019S mutation (Table 1). LRRK2-PD and IPD patients had
similar motor characteristics, except for a higher percentage of fluctuations in LRRK2-PD (Table 2).
The right putamen binding ratio was lower in the NMC than in the noncarriers (2.5 [1.75; 2.87] vs
2.9 [2.77; 3.13], p = 0.008) (Table 2).
CSF protein levels
An influence of the CSF Hb concentration was observed for α-syn levels but not for other
biomarkers (eTable 3). Accordingly, we stratified the subjects based on their CSF Hb levels when

87
RESULTADOS 6
describing results of α-syn assays. We also observed an influence of age in the CSF levels of T-tau
and α-syn, but not in Aβ or p-tau181 (data not shown).
CSF α-syn levels were similar among LRRK2-PD, NMC and NMNC but significantly higher than in
IPD (p = 0.041) (Table 3 and Figure 1). This difference persisted after exclusion of 21 subjects with
CSF Hb levels higher than 500 ng/ml (p = 0.051) but this disappeared if 28 subjects with a CSF Hb
concentration higher than 200 ng/ml (p = 0.089) were excluded. The difference also persisted
taking into account the age influence. There were no differences in CSF Aβ, T-tau and p-tau181
concentrations among groups (Table 3; Figure 1).
α-syn levels correlated with T-tau and p-tau181 levels in all study groups (eTable 4; eFigure 1). The
correlation between CSF α-syn levels and Aβ was also significant in all study groups except in
IPD patients. Those patients with lower levels of Aβ presented higher UPDRS-III scores (r = -0.266,
p = 0.017) and a higher Hoehn and Yahr stage (r = -0.172, p = 0.045) but correlations were weak.
T-tau levels were higher in the PIGD-PD than in the TD-PD in the LRRK2-PD, but Aβ levels were
higher in the TD-PD than in the PIGD-PD in the IPD patients (Table 4). There were no differences in
the CSF biomarkers between PIGD, TD and IND phenotypes when CSF from all PD patients were
analyzed together (LRRK2-PD and IPD). The PIGD-PD group had similar age to the TD-PD group
(61 [53-69] years vs 59.5 [48-65] years; p = 0.289) but was older than the IND-PD group (61 [53-69]
years vs 54 [41-66] years; p = 0.006). The age at diagnosis, education and sex distribution were
similar between PIGD, TD and IND patients.
No significant correlation was found between CSF biomarker levels and striatal binding ratio in
NMC or in noncarriers (eTable 5).
LRRK2 G2019S mutation carriers
After excluding from the analysis those subjects with other mutations different than G2019S,CSF
protein were quantitatively similar across groups but differences were no longer statistically

88
RESULTADOS6
significant (eTable 6). Correlations between α-syn and other CSF biomarkers were similar, except
that in the NMC a correlation between α-syn and Aβ was not observed.
Discussion
To the best of our knowledge this is the first cross-sectional study on CSF biomarkers (α-syn, Aβ,
T-tau, and p-tau181) in a cohort of LRRK2 mutation carriers using highly standardized procedures
for sample collection, CSF protein level analysis and clinical assessments. We found several rele-
vant findings regarding the CSF biomarker concentrations and their relationship with clinical and
imaging data. First, the levels of CSF α-syn in patients with LRRK2-PD, NMC and NMNC were similar
but significantly higher than in the IPD. Second, we observed a correlation between α-syn levels
and CSF proteins related to AD pathology (Aβ, T-tau and p-tau181) in all groups. Third, CSF protein
levels according to the motor phenotype were different in LRRK2-PD and IPD; and finally, CSF
biomarkers did not differentiate NMC from NMNC in this group of asymptomatic subjects.
Recent studies in IPD patients showed a drop in CSF total α-syn 4-9 while levels of oligomeric α-syn
appear to be increased8, 10-12. Lower CSF total α-syn has been reported in early PD compared to
healthy controls as well 8 and also in the PD patients of the Parkinson’s Progression Markers Initia-
tive (PPMI) study, which follows similar methodology in the sample collection and analysis than
the one used in the present study 5. Our results show that α-syn levels in IPD patients are lower
than in LRRK2-PD. This also occurs in the G2019S mutation carriers but with less statistical signifi-
cance, possibly because of the smaller sample size. Interestingly, the CSF α-syn levels in LRRK2-PD
patients are similar to those concentrations reported in the PPMI study in the healthy controls.
Higher α-syn levels in CSF in LRRK2-PD patients may reflect different neuropathological substrate,
with absence of α-syn aggregates in some instances. It is also possible that LRRK2-PD have a lower
synuclein burden in the CNS than IPD patients, reflecting the more benign course of LRRK2-PD
described by some. Both of the groups in the present study, though, had a similar degree of motor
severity. This difference in α-syn level might be important also for future therapeutic strategies.

89
RESULTADOS 6
We did not find differences in other CSF biomarkers (Aβ1-42, T-tau and p-tau181) among the four
groups of subjects studied. Previous studies of AD-type biomarkers in IPD showed controver-
sial results. While some found that CSF Aβ42 levels were significantly lower in IPD compared to
controls 4, 13 other investigations have not found this 6, 14-17. Also studies measuring CSF T-tau and
p-tau levels in IPD have been inconsistent 4-7, 13-19. The reasons for these discrepancies may include
but are not limited to methodological variables including CSF processing, the biomarkers assays
used, diversity in criteria for control selection and stage of PD across the studies. In the present
study the use of highly standardized procedures minimize the preanalytical (sampling collection,
handling, and storage) and analytical variability (analysis execution/sample processing) in CSF
biomarker measurement.
The PIGD motor phenotype has been associated with more rapid cognitive decline and/or more
functional disability in patients with PD compared with the TD-PD phenotype 31-32. A recent study
showed lower levels of Aβ1-42, T-tau, p-tau181 and α-syn in the PIGD-PD patients 5. The present
study did not confirm these findings but found different patterns of CSF protein levels in LRRK2-PD
and IPD according to the motor phenotype.
We observed a correlation between α-syn levels and both species of tau, T and p-tau181, and also with
Aβ1-42, suggesting an interaction between α-syn and AD related proteins. α-syn has been shown to
have complex and dynamic interactions with tau and these two proteins have the tendency to
seed the aggregation for the other 33-34. In the present study the protein correlation was seen in PD
patients but also observed in asymptomatic subjects, supporting the fact that this correlation may
be independent of the disease process. Similar observations have been reported previously 5.
An effective biomarker could aid in identifying the preclinical phase of PD, as it is well recognized
that the pathological processes predates the onset of the classical motor symptoms 35-36. Identifi-
cation by means of a CSF protein marker of those NMC with a high risk for developing PD would
be of great value. We did not observe differences regarding α-syn and AD related CSF proteins
between NMC and NMNC. Since subjects with manifest LRRK2-PD had α-syn levels in a range

90
RESULTADOS6
considered normal it is perhaps not surprising that subjects potentially in earlier disease stages
and with less α-syn pathology fail to show abnormal protein levels in the CSF.
The study is limited by the relatively small size of the subjects studied. The relatively young age
of the NMC, at least ten years younger than the expected age at onset of LRRK2-PD 37, is another
consideration since LRRK2-PD is an age-related condition. Finally we included subjects with
different mutations which might make the interpretation of some of the results challenging since
the pathophysiology of the disease could be different. Although all mutations present in this
cohort of LRRK2-PD patients and NMC are known as pathogenic mutations.
In summary, the CSF protein profile was different between IPD and LRRK2-PD patients with lower
α-syn levels in patients with IPD than in LRRK2-PD patients and than in their first-degree relatives.
We also observed a different CSF protein profile according to the motor phenotype between
LRRK2-PD and in IPD. CSF biomarkers did not differentiate NMC from noncarriers in this cohort
of subjects.
Acknowledgements
We thank our research subjects and family members for their participation in this study. None of
the authors of this manuscript report conflict of interest.
Authors’ roles: Dr. Tolosa and Dr. Vilas had full access to all the data in the study and take respon-
sibility for the integrity of the data and the accuracy of the data analysis. Dr. Vilas: drafting/revising
the manuscript, study concept or design, analysis or interpretation of data, acquisition of data,
statistical analysis. Dr. Shaw, Dr. Taylor, Dr. Pont-Sunyer, Dr. Berg, Dr. Brockmann, Dr Marras, and Dr.
Aasly: drafting/revising the manuscript, analysis and interpretation of data. Dr. Marek: drafting/
revising the manuscript, DaT-SPECT images interpretation. Mr. Ríos: statistical analysis, drafting/
revising the manuscript and interpretation of data. Dr. Tolosa: drafting/revising the manuscript,
study concept or design, analysis or interpretation of data, acquisition of data, study supervision.

91
RESULTADOS 6
The investigators within the LRRK2 Cohort Consortium (LCC) contributed to the design and imple-
mentation of the LCC and/or provided data and/or collected biospecimens, but did not neces-
sarily participate in the analysis or writing of this report.
LCC investigators include:
Beth Israel Medical Center, New York, NY, USA: Rachel Saunders-Pullman, MD, MPH; Deborah
Raymond, MSc; Andres Deik, MD; Matthew James Barrett, MD, MSc; Jose Cabassa, MD; Mark
Groves, MD; Ann L. Hunt, DO; Naomi Lubarr, MD; Marta San Luciano, MD, MSc; Joan Miravite, NP;
Christina Palmese, PhD; Rivka Sachdev, MD; Harini Sarva, MD; Lawrence Severt, MD, PhD; Vicki
Shanker, MD; Matthew Carrington Swan, MD; Jeannie Soto-Valencia, BA; Brooke Johannes, MSc;
Laurie Ozelius, PhD; Robert Ortega, MSc; Susan Bressman, MD.
Columbia University Medical Center, New York, NY, USA: Roy N. Alcalay, MD, MSc; Ming-X Tang,
PhD; Helen Mejia Santana, MSc; Ernest Roos, MD; Martha Orbe-Reilly, MD; Stanley Fahn, MD; Lucien
Cote, MD, Cheryl Waters, MD; Pietro Mazzoni, MD, PhD; Blair Ford, MD; Elan Louis, MD, MSc; Oren
Levy, MD, PhD; Llency Rosado, MD; Diana Ruiz, BSc; Tsvyatko Dorovski, MSc, MBA; Lorraine Clark,
PhD; Karen S Marder, MD, MPH.
Hôpital de la Pitié-Salpétrière, Paris, France: Alexis Brice, MD ; Jean-Christophe Corvol, MD, PhD ;
Florence Cormier, MD ; Anne-Marie Bonnet, MD ; Marie-Laure Welter, MD, PhD ; Valérie Mesnage,
MD; Marie Vidailhet, MD; Emmanuel Roze, MD, PhD; Lucette Lacomblez, MD; David Grabli, MD, PhD.
Hospital Donostia, San Sebastian, Spain: Jose Felix Martí Masso, MD, PhD; Javier Ruiz Martínez,
MD, PhD; Elisabet Mondragon Rezola MD; Ainara Estanga Alustiza, BS; Ana Gorostidi Pagola, PhD.
Hospital Clinic de Barcelona, Barcelona, Spain: Eduardo Tolosa, MD; Claustre Pont-Sunyer MD;
Dolores Vilas Rolán MD; Ruben Fernandez-Santiago, PhD; Maria Quintana, BS; Manel Fernandez,
BS; Laura Maragall, BA.
National Institute of Neurology Tunis, Tunisia: Faycal Hentati, MD; Matthew Farrer, PhD; John
Duda, MD; Matt Read, BS; Lefkos Middleton, MD, FRCP; Rachel Gibson, PhD; Joanne Trinh, BS; Samia
Ben Sassi,,MD; Mourad Zouari, MD; Rim amouri, PhD; Emna Farhat, MD; Fatma Nabli, MD.
Norwegian University of Science of Technology, Trondheim, Norway: Jan Aasly, MD; Bjørg
Johanne Warø, MD; Sigrid Andersen, PhD, MSc.

92
RESULTADOS6
PROGENI Study – Indiana University School of Medicine, Indianapolis, IN, USA: John Bertoni
MD, PhD; Julie Carter RN, MN, ANP; Lawrence Elmer MD, PhD; Nestor Galvez Jimenez, MD; Wayne
Martin, MD; Rajesh Pahwa, MD; Kelly Lyons, PhD; Stephen Reich, MD; Robert Rodnitzky, MD;
Carmen Serrano Ramos, MD; Joanne Wojcieszek, MD.
Tel Aviv Sourasky Medical Center, Tel Aviv, Israel: Anat Mirelman, PhD; Tanya Gurevich, MD; Anat
Bar Shira, PhD; Mali Gana Weisz, PhD; Kira Yasinovsky; Maayan Zalis, DMD; Avner Thaler, MD; Avi
Orr-Urtreger, MD, PhD; Nir Giladi, MD.
The Parkinson Institute, Sunnyvale, CA, USA: Birgitt Schuele, MD; Caroline M. Tanner, MD, PhD J.
William Langston, MD; Samuel M. Goldman, MD, MPH; Joanna Mountain, PhD. Toronto Western
Hospital, Toronto, Canada: Connie Marras MD, PhD, FRCPC; Anthony Lang OC, MD, FRCPC, FAAN,
FCAHS, FRSC; Ekaterina Rogaeva PhD; Tiago Mestre MD; Naomi Visanji PhD; Taneera Ghate MSc;
Jennifer Singerman MD, FRCPC; Amaal Al Dakheel MD; Barbara S Connolly MD, FRCP.
University of Tuebingen, Tuebingen, Germany: Thomas Gasser, MD; Daniela Berg, MD; Kathrin
Brockmann, MD.
23andMe, Inc. Mountain View, CA, USA: Emily Drabant Conley, PhD; Meghan E Mullins, BA; Carrie
Northover, PhD.
Data and biospecimens used in preparation of this article were obtained from the MJFF LRRK2
Cohort Consortium (LCC) (https://www.michaeljfox.org/page.html?lrrk2-cohort-consortium). For
up-to-date information on the study, visit https://www.michaeljfox.org/page.html?lrrk2-cohort-con-
sortium.
The MJFF LRRK2 Cohort Consortium is coordinated and funded by The Michael J. Fox Foundation
for Parkinson’s Research.

93
RESULTADOS 6
Table 1: Demographic and general information.
Results were described by median and interquartile range [Percentiles 25th; 75th] or absolute and
relative frequencies for quantitative or qualitative variables respectively.a Kruskall-Wallis test. b U Mann-Whitney Test . c Fischer’s Exact test.
PD: Parkinson’s disease. LRRK2-PD: LRRK2 associated Parkinson’s disease. IPD: idiopathic Parkinson’s disease.
NMC: asymptomatic carriers. LEDD: levodopa equivalent daily dose. NMC: nonmanifesting carriers.
NMNC: nonmanifesting noncarriers.
p value
LRRK2-PDn = 28
IPDn = 35
NMCn = 41
Noncarriersn = 34
OverallLRRK2-PD
vs IPDNMC
vs NMNC
Age, years 65 [54; 73] 60 [52; 68] 53 [42; 62] 55 [42; 65] 0.009 a 0.842 b 0.565 b
Gender (male), n (%) 13 (46.4 %) 25 (71.4 %) 21 (51.2 %) 15 (44.1 %) 0.095 c
Race 0.325 c
Caucasian 26 (92.9 %) 35 (100 %) 40 (97.6 %) 34 (100 %)
West asian 1 (3.6 %) 0 (0 %) 0 (0 %) 0 (0 %)
Other/NA 1 (3.6 %) 0 (0 %) 1 (2.4 %) 0 (0 %)
Subject Education, years 10 [8; 12] 12 [10; 16] 11 [9; 15] 15 [12; 19] 0.001 a 0.007 b 0.003 b
Age at PD Diagnosis, years 55 [45; 64] 55 [47; 63] 0.842 b
Age at onset, years 55 [46; 64] 52 [44; 62] 0.603 b
Disease duration, years 8 [2; 13] 4 [0; 6] 0.008 b
LEDD 479.5 [300; 1085] 387.5 [100; 700] 0.100 b
Mutation
G2019S 20 (71.4 %) 31 (75.6 %)
R1441G 1 (3.6 %) 1 (2.4 %)
R1441C 0 (0 %) 2 (4.9 %)
N1437H 2 (7.1 %) 4 (9.8 %)
I2020T 1 (3.6 %) 0 (0 %)
C228S 1 (3.6 %) 2 (4.9 %)
R1325Q 1 (3.6 %) 0 (0 %)
Other 2 (7.1 %) 1 (2.4 %)

94
RESULTADOS6
Results were described by median and interquartilic range [Percentiles 25th; 75th] or absolute and relative
frequencies for quantitative or qualitative variables respectively.a Kruskall-Wallis test. b U Mann-Whitney Test. c Fischer’s Exact test.
*Data from the LRRK2-PD patients is only included for comparison purposes.
PD: Parkinson’s disease. LRRK2-PD: LRRK2 associated Parkinson’s disease. IPD: idiopathic Parkinson’s disease
NMC: nonmanifesting carriers. NMNC: nonmanifesting noncarriers. UPDRS: unified Parkinson’s disease rating scale.
MDS-UPDRS: Movement Disorders Society unified Parkinson’s disease rating scale. PIGD-PD: postural instability-gait
disturbance Parkinson’s disease. TD-PD: tremor dominant Parkinson’s disease. IND-PD: intermediate PD. HY: Hoehn and
Yahr scale. SE: Schwab and England scale. DaT-SPECT: Dopamine transporter single-photon emission computed tomo-
graphy. SBR: striatal binding ratio. UPSIT: University of Pennsylvania Smell Identification Test. MOCA: Montreal Cognitive
Assessment. Epworth: Epworth scale. GDS-15: Geriatric depression scale (15 items). RBDSQ: REM sleep behaviour disorder
screening questionnaire. SCOPA-AUT: Scales for Outcomes in Parkinson’s disease-Autonomic. GI: Gastrointestinal dysfunction.
GU: Urinary dysfunction. CV: Cardiovascular dysfunction. T: Thermoregulatory dysfunction. P: Pupillomotor dysfunction.
*UPSIT and MOCA scores were adjusted for age and educational level.
Table 2: Clinical and imaging characteristics
p value
LRRK2-PDn = 28
IPDn = 35
NMCn = 41
NMNCn = 34
OverallLRRK2-PD
vs IPDNMC
vs NMNC
MDS-UPDRS-I 5 [5; 5] n = 1
3 [3; 3] n = 1
3 [0; 5] n = 3
3.5 [2; 6] n = 10 0.870
a
UPDRS_I 1 [1; 3] n = 9
1 [1; 2] n = 23
0 [0; 1] n = 24
1 [0; 2] n = 5 0.035
a0.869
b0.352
b
MDS-UPDRS-II 14 [7.9; 16.7] n = 9
9 [6.8; 11.2] n = 24
0 [0; 4.5] n = 4
0 [0; 0] n = 10 < 0.001
a0.207
b0.635
b
MDS-UPDRS-III 21.5 [16.7; 32.3] n = 17
31.1 [22.7; 37.1] n = 29
0 [0; 16.15] n = 4
0 [0; 1] n = 10 < 0.001
a0.076
b0.945
b
UPDRS IV 3 [0; 6] n = 25
0 [0; 1] n = 33 0.005
b
Motor fluctuations (n, %) 13 (46.4 %) 8 (22.9 %) 0.042 c
Motor phenotype PIGD-PD 20 (71.4 %) 17 (50 %) 0.107TD-PD 6 (21.4 %) 8 (23.5 %)IND-PD 2 (7.1 %) 9 (26.5 %)
HY 0.104 c
I / II 22 (81.5 %) 32 (94.1 %)III 1 (3.7 %) 2 (5.9 %)IV / V 4 (14.8 %) 0 (0 %)
Schwab and England(in ON)
90 [70; 90] n = 23
90 [90; 90] n = 33 0.149
b
DaT-SPECT 4 (14.3 %) 29 (70.7 %) 12 (35.3 %)Right Caudate SBR* 2.94 [2.7; 3.82] 3.55 [2.78; 3.96] 3.58 [3.26; 4.08] 0.440
b
Right Putamen SBR* 1.63 [1.13; 3.08] 2.5 [1.75; 2.87] 2.9 [2.77; 3.13] 0.008 b
Left Caudate SBR* 3.41 [2.82; 4.05] 3.47 [3.07; 3.8] 3.7 [3.2; 4.23] 0.375 b
Left Putamen SBR* 2.15 [1.3; 3.1] 2.36 [1.89; 2.91] 2.74 [2.59; 2.99] 0.074 b
UPSIT* 24 [19; 29] 16 [11; 22] 30.5 [29; 34] 32 [30; 35] < 0.001 a
0.003 b
0.756 b
MoCA* 25 [22; 27] 27 [24; 29] 27 [25.5; 28] 28 [26; 29] 0.013 a
0.020 b
0.456 b
Epworth 7 [3.5; 11] 5 [4; 7] 5 [2; 9] 6 [4; 9] 0.418 a
GDS-15 3 [1; 6] 2 [1; 4] 1 [0; 3] 1 [0; 4] 0.053 a
0.345 b
0.671 b
RBDSQ 3 [1; 5] 4 [2; 7] 2 [1; 4] 2 [1; 3] 0.001 a
0.086 b
0.625 b
SCOPA-AUT 18 [11; 21] 11.5 [6; 17] 6 [2; 9] 7 [4; 11] < 0.001 a
0.040 b
0.224 b
SCOPA-AUT (GI) 3 [1; 8] 2.5 [2; 4] 0 [0; 1] 1 [0; 1] < 0.001 a
0.587 b
0.306 b
SCOPA-AUT (GU) 5.5 [3; 9] 5 [2; 8] 3 [1; 4] 4 [1; 5] 0.001 a
0.136 b
0.187 b
SCOPA-AUT (CV) 0 [0; 1] 0 [0; 1] 0 [0; 1] 0 [0; 1] 0.806 a
SCOPA-AUT (T) 3 [0; 5.5] 0.5 [0; 2] 0 [0; 3] 1 [0; 3] 0.058 a
SCOPA-AUT (P) 0 [0; 1] 0 [0; 0] 0 [0; 1] 0 [0; 0] 0.349 a
SCOPA-AUT (Sex) 0 [0; 1] 1 [0; 3] 0 [0; 0] 0 [0; 2] 0.051 a
0.287 b
0.059 b

95
RESULTADOS 6
p v
alu
e
LRRK
2-PD
n =
28IP
Dn
= 35
NM
Cn
= 41
NM
NC
n =
34O
vera
llLRRK
2-PD
vs IP
D
NM
Cvs
N
MN
C
LRRK
2-PD
vsN
MC
LRRK
2-PD
vsN
MN
C
IPD vs
NM
C
IPD vs
NM
NC
Aβ 1
-42 p
g/m
l25
1.16
[1
98.6
2-93
.34]
217.
62
[168
.02-
284.
51]
251.
81
[214
.88-
293
.01]
279.
37
[228
.47-
300.
07]
0.09
4 a
(0.19
4)
T-ta
u p
g/m
l39
.38
[31.
92-5
6.38
]36
.30
[31.
87-4
6.61
]38
.54
[4.4
3-52
.18]
42.2
9 [3
5.39
-54.
52]
0.38
3 a
(0.5
43)
p-t
au18
1 pg
/ml
27.2
1
[24.
36-3
1.94
]24
.98
[1.3
89-2
9.63
]27
.77
[4.4
1-38
.30]
28.7
0 [2
.19-3
4.97
]0.
217 a
(0
.285
)
α-s
yn p
g/m
l14
75.13
[1
033.
76-1
752.
15]
1015
.85
[852
.99-
1442
.79]
1337
.24
[105
9.05
-192
0.64
]13
64.5
3 [1
039.
97-1
785.
59]
0.04
1 a
(0.0
90)
0.02
7 b
(0.0
37)
0.89
0 b
(0.7
28)
0.75
9 (0
.935
)0.
695
(0.6
92)
0.01
4 (0
.023
)0.
026
α-s
yn p
g/m
l H
b <
200
ng
/mL
1363
.47
[101
3.69
-157
5.14
] n
= 2
2
1015
.85
[852
.99-
1441
.79]
n
= 3
5
1275
.20
[104
5.52
-166
1.23
] n
= 3
0
1369
.34
[101
7.34
-179
4.08
] n
= 2
30.
119
α-s
yn p
g/m
lH
b <
500
ng
/mL
1363
.47
[101
3.69
-157
5.14
] n
= 2
2
1015
.847
[8
52.9
9-14
42.7
9]
n =
35
1354
.52
[107
6.45
-192
0.64
] n
= 3
6
1404
.98
[103
2.43
-186
6.74
] n
= 24
0.05
1
T-ta
u/A
β 1-4
2 0.
16
[0.15
-0.2
2]0.
16
[0.13
-0.2
1]0.
15
[0.1
4-0.
19]
0.16
[0
.14-0
.20]
0.64
6 a
p-t
au18
1/ A
β 1-4
2 0.
11
[0.0
9-0.
14]
0.10
[0
.09-
0.12
]0.
11
[0.0
9-0.
14]
0.10
[0
.09-
0.13
]0.
777 a
p-t
au18
1/T-
tau
0.
67
[0.5
7-0.
76]
0.66
[0
.59-
0.76
]0.
71
[0.6
2-0.
79]
0.66
[0
.59-
0.72
]0.
234 a
CSF
Hb
75.0
0 [7
5.00
-189
.84]
75.0
0 [7
5.00
-75.
00]
75.0
0 [7
5.00
-239
.61]
75.0
0 [7
5.00
-112
8.77
]<
0.00
1 a<
0.00
1 b0.
210 b
Results were described by median and interquartilic range [Percentiles 25th; 75th] or absolute and relative
frequencies for quantitative or qualitative variables respectively. Statistically significant p values are in bold type a Kruskall-Wallis test. b U Mann-Whitney Test. PD: Parkinson’s disease. LRRK2-PD: LRRK2 associated Parkinson’s
disease. IPD: idiopathic Parkinson’s disease NMC: nonmanifesting carriers. NMNC: nonmanifesting noncarriers.
α-syn, Hb < 200 ng/ml: α-syn levels in subjects with a Hb concentration lower than 200 ng/ml. α-syn,
Hb < 500 ng/ml: α-syn levels in subjects with a Hb concentration lower than 500 ng/ml.
Table 3: Comparison of Cerebrospinal Fluid biomarkers among groups

96
RESULTADOS6
LRRK2-PDPIGD-PD
n = 20TD-PD
n = 6IND-PD
n = 2p value
p value PIGD vs TD
α-syn1440.679
[1023.725-2058.970]1491.209
[1067.219-1571.710]1604.850
[1457.548-1752.151]0.782 0.684
Aβ257.093
[201.101-315.101]213.682
[146.998-268.835]235.630
[220.756-250.504]0.347 0.162
Tau45.155
[34.934-59.935]31.780
[23.983-36.838]46.038
[35.347-56.729]0.063 0.021
p-Tau27.798
[24.788-33.859]25.549
[17.294-29.515]26.492
[25.984-27.000]0.269 0.139
IPDPIGD-PD
n = 17TD-PD
n = 8IND-PD
n = 9p value
p value PIGD vs TD
α-syn947.876
[841.738-1365.728]1212.322
[976.079-1695.900]1015.847
[991.567-1635.688]0.521 0.322
Aβ213.182
[168.022-264.697]302.342
[220.123-347.704]169.892
[152.204-210.205]0.008 0.012
Tau35.025
[31.872-46.609]40.863
[32.375-48.340]40.039
[33.594-45.449]0.627 0.522
p-Tau24.617
[21.718-27.477]25.194
[22.248-31.016]25.930
[21.389-35.806]0.736 0.727
All PD cases (LRRK2-PD and IPD)
PIGD-PD n = 37
TD-PD n = 14
IND-PD n = 11
p valuep value
PIGD vs TD
α-syn1208.649
[866.511-1719.482]1216.619
[1067.219-1571.710]1242.823
[991.567-1681.471]0.816 0.961
Aβ247.881
[199.417-289.902]248.923
[216.430-320.174]176.518
[152.204-248.364]0.423 0.131
Tau38.564
[32.614-48.457]35.459
[30.544-45.013]40.039
[33.594-56.729]0.177 0.312
p-Tau27.177
[22.553-31.969]25.261
[21.256-29.593]25.984
[21.389-35.806]0.353 0.565
Table 4: Comparison of CSF biomarkers between motor phenotypes.
PD: Parkinson’s disease. LRRK2-PD: LRRK2 associated Parkinson’s disease. IPD: idiopathic Parkin-
son’s disease. Statistically significant results are in bold type.

97
RESULTADOS 6
0
500
1000
1500
2000
2500
3000
3500
4000
LRRK2-PD LRRK2-PD LRRK2-PDIPD IPD IPDNMC NMC NMCNMNC NMNC NMNC
1A 1B 1C
α-s
yn (p
g/m
L)
10
20
20
20
40
30
60
60
40
80
50
100
100
60
120
120
0
0
0
LRRK2-PD IPD NMC NMNC
1D
p-t
au (p
g/m
L)T-
tau
(pg
/mL)
Aβ 1
-42
(pg
/mL)
Figure 1: Boxplot of CSF biomarkers levels in LRRK2-PD, IPD, NMC and NMNC
Concentrations of the CSF proteins. α-synuclein concentration in all patients (1A), in subjects with a CSF Hb
concentration less than 500 ng/ml (1B) and in subjects with a CSF Hb concentration less than 200 ng/ml (1C);
CSF levels of Aβ, Tau, and p-Tau levels (1D).

98
RESULTADOS6
eTable 1: Quality control of samples in the α-synuclein analysis.
QC: quality control. CSF: cerebrospinal fluid.
Expected performance of QC samples (33 independent analyses)
Actual performance of QC samples in analysis of LRRK2 cohort CSF
QC sample 1 QC sample 2 QC sample 1 QC sample 2
Mean value a-syn (pg/ml) 1074 1324 1107 1350
Standard deviation 133 171 53 101
% CV 12.4 % 12.9 % 5 % 7 %
Expected performance of QC samples (29 independent analyses)
Actual performance of QC samples in analysis of LRRK2 cohort CSF
QC sample 1 QC sample 2 QC sample 1 QC sample 2
Mean value Hb (ng/ml) 294 1769 262 1712
Standard deviation 44.72 256 4.8 69.2
% CV 15.2 % 14.5 % 2 % 4 %
eTable 2: Quality control of samples in the hemoglobin analysis
QC: quality control. CSF: cerebrospinal fluid.
Hemoglobin < 200 ng/mL
Hemoglobin > 200 ng/mL
p value
α-syn1216.62
[973.58; 1671.93]1537.96
[1257.27; 1954.08]0.018 a
Aβ1-42247.65
[197.41; 294.83]268.76
[236.63; 290.24]0.151 a
p-tau18126.55
[22.21; 32.45]28.71
[26.75; 33.35]0.158 a
T-tau38.55
[32.65; 49.45]42.35
[36.21; 55.86]0.153 a
eTable 3: Influence of CSF Hemoglobin levels in the CSF biomarkers concentrations.
Results were described by median and interquartilic range [Percentiles 25th; 75th].a U Mann-Whitney Test
All Subjects*
p value LRRK2-PD* p value IPD* p value NMC* p value NMNC* p value
T-tau 0.864 < 0.001 0.851 < 0.001 0.902 < 0.001 0.876 < 0.001 0.780 < 0.001
p-tau 0.755 < 0.001 0.800 < 0.001 0.756 < 0.001 0.755 < 0.001 0.620 < 0.001
Aβ1-42 0.505 < 0.001 0.551 0.003 0.260 0.132 0.374* 0.016 0.744 < 0.001
eTable 4: Correlations between a-syn levels and T-tau, p-tau and AB in CSF
PD: Parkinson’s disease. LRRK2-PD: LRRK2 associated Parkinson’s disease. IPD: idiopathic Parkinson’s disease
NMC: nonmanifesting carriers. NMNC: nonmanifesting noncarriers. *Spearman correlation.

99
RESULTADOS 6
Right Caudate
p valueRight
Putamenp value
Left Caudate
p valueLeft
Putamenp value
All relativesn = 44
α-syn 0.020 0.898 -0.008 0.958 0.010 0.950 -0.013 0.935
Aβ -0.064 0.681 0.104 0.500 0.038 0.806 0.019 0.904
p-Tau 0.118 0.446 0.137 0.375 0.077 0.618 0.199 0.196
Tau 0.005 0.972 -0.022 0.888 -0.020 0.896 -0.048 0.758
NMCn = 31
α-syn -0.095 0.612 -0.135 0.471 -0.093 0.619 -0.086 0.644
Aβ -0.150 0.421 -0.026 0.891 0.058 0.757 0.006 0.973
p-Tau 0.049 0.794 0.013 0.944 -0.004 0.985 0.193 0.299
Tau -0.116 0.535 -0.259 0.160 -0.138 0.460 -0.191 0.303
NMNCn = 13
α-syn 0.346 0.247 0.190 0.535 0.236 0.437 0.220 0.471
Aβ 0.104 0.734 0.245 0.420 0.005 0.986 0.022 0.943
p-Tau 0.396 0.181 0.385 0.194 0.308 0.306 0.335 0.263
Tau 0.407 0.168 0.360 0.226 0.286 0.344 0.341 0.255
eTable 4: Correlations between a-syn levels and T-tau, p-tau and AB in CSF
Spearman’s rho analyses. NMC: nonmanifesting carriers. NMNC: nonmanifesting noncarriers.
LRRK2 G2019S PD n = 20
IPD n = 35
NMC G2019S n = 31
NMNC n = 34
p value
Aβ1-42 pg/ml254.11
[198.89-301.397]217.62
[168.02-284.51]258.531
[213.04- 302.08]279.37
[228.47-300.07]0.102 a
T-tau pg/ml42.03
[31.71-54.05]36.30
[31.87-46.61]38.01
[33.61-51.83]42.29
[35.39-54.52]0.361 a
p-tau181 pg/ml28.60
[24.33-33.86]24.98
[1.389-29.63]27.73
[24.22-38.33]28.70
[2.19-34.97]0.351 a
α-syn pg/ml1483.17
[1094.28-1892.86]1015.85
[852.99-1442.79]1274.73
[1045.52-1941.29]1364.53
[1039.97-1785.59]0.072 a
T-tau / Aβ1-42 0.16
[0.15-0.18]0.16
[0.13-0.21]0.15
[0.13-0.19]0.16
[0.14-0.20]0.744 a
p-tau181 / Aβ1-42 0.11
[0.09-0.13]0.10
[0.09-0.12]0.10
[0.09-0.14]0.10
[0.09-0.13]0.985 a
p-tau181 / T-tau 0.68
[0.63-0.78]0.66
[0.59-0.76]0.71
[0.62-0.79]0.66
[0.59-0.72]0.477 a
eTable 6: Comparison of Cerebrospinal Fluid biomarkers among groups including only G2019S LRRK2-PD and NMC
Results were described by median and interquartile range [Percentiles 25th; 75th] or absolute and rela-
tive frequencies for quantitative or qualitative variables respectively.
Parkinson’s disease. LRRK2 G2019S PD: LRRK2 G2019S associated Parkinson’s disease. IPD: idiopathic Parkinson’s
disease NMC G2019S: G2019S nonmanifesting carriers. NMNC: nonmanifesting noncarriers. a Kruskall-Wallis test.

100
RESULTADOS6
0
50
100
150
200
500040003000200010000
r = 0 .864 p < .001
T-ta
u (p
g/m
L)
α-syn (pg/mL)
0
25
50
75
500040003000200010000
r = 0 .755 p < .001
p-t
au (p
g/m
L)α-syn (pg/mL)
100
200
300
400
500
500040003000200010000
r = 0 .505 p < .001
Aβ 1
-42
(pg
/mL)
α-syn (pg/mL)
0
50
100
150
200
500040003000200010000
r = 0 .851 p< .001
T-ta
u (p
g/m
L)
α-syn (pg/mL)
0
25
50
75
500040003000200010000
r = 0 .800 p < .001
p-t
au (p
g/m
L)
α-syn (pg/mL)
100
200
300
400
500
500040003000200010000
r = 0 .551 p < .001
Aβ 1
-42
(pg
/mL)
α-syn (pg/mL)
0
50
100
150
200
500040003000200010000
r = 0 .902 p < .001
T-ta
u (p
g/m
L)
α-syn (pg/mL)
0
25
50
75
500040003000200010000
r = 0 .756 p < .001
p-t
au (p
g/m
L)
α-syn (pg/mL)
100
200
300
400
500
500040003000200010000
r = 0 .260 p < 0 .132
Aβ 1
-42
(pg
/mL)
α-syn (pg/mL)
0
50
100
150
200
500040003000200010000
r = 0 .876 p < .001
T-ta
u (p
g/m
L)
α-syn (pg/mL)
0
25
50
75
500040003000200010000
r = 0 .755 p < .001
p-t
au (p
g/m
L)
α-syn (pg/mL)
100
200
300
400
500
500040003000200010000
r = 0 .374 p < 0 .016
Aβ 1
-42
(pg
/mL)
α-syn (pg/mL)
eFigure 1: Correlations between α-syn levels and T-tau, p-tau and AB in CSF.
Correlations between a-syn levels and T-tau, p-tau and AB in CSF.
A, B, C: all subjects; D, E, F: LRRK2-PD; G, H, I: IPD; J, K, L: NMC; M, N, O: NMNC.

101
RESULTADOS 6
References
1. Zimprich A, Biskup S, Leitner P, et al. Mutations in LRRK2 cause autosomal-dominant parkinsonism with pleo-morphic pathology. Neuron 2004;44(4):601-7.
2. Paisan-Ruiz C, Jain S, Evans EW, et al. Cloning of the gene containing mutations that cause PARK8-linked Parkinson’s disease. Neuron 2004;44(4):595-600.
3. Gilligan PJ. Inhibitors of leucine-rich repeat kinase 2 (LRRK2): progress and promise for the treatment of Parkinson’s disease. Curr Top Med Chem. 2015;15(10):927-38.
4. Shi M, Bradner J, Hancock AM, et al. Cerebrospinal fluid biomarkers for Parkinson disease diagnosis and progression. Ann Neurol 2011;69(3):570-80.
5. Kang JH, Irwin DJ, Chen-Plotkin AS, et al. Association of cerebrospinal fluid beta-amyloid 1-42, T-tau, p-tau181, and alpha-synuclein levels with clinical features of drug-naive patients with early Parkinson disease. JAMA Neurol 2013;70(10):1277-87.
6. Hall S, Ohrfelt A, Constantinescu R, et al. Accuracy of a panel of 5 cerebrospinal fluid biomarkers in the differ-ential diagnosis of patients with dementia and/or parkinsonian disorders. Arch Neurol 2012;69(11):1445-52.
7. Mollenhauer B, Locascio JJ, Schulz-Schaeffer W, Sixel-Doring F, Trenkwalder C, Schlossmacher MG. alpha-Sy-nuclein and tau concentrations in cerebrospinal fluid of patients presenting with parkinsonism: a cohort study. Lancet Neurol 2011;10(3):230-40.
8. Mollenhauer B, Trautmann E, Taylor P, et al. Total CSF alpha-synuclein is lower in de novo Parkinson patients than in healthy subjects. Neurosci Lett 2013;532:44-8.
9. Hong Z, Shi M, Chung KA, et al. DJ-1 and alpha-synuclein in human cerebrospinal fluid as biomarkers of Parkinson’s disease. Brain 2010;133(Pt 3):713-26.
10. Tokuda T, Qureshi MM, Ardah MT, et al. Detection of elevated levels of alpha-synuclein oligomers in CSF from patients with Parkinson disease. Neurology 2010;75(20):1766-72.
11. Park MJ, Cheon SM, Bae HR, Kim SH, Kim JW. Elevated levels of alpha-synuclein oligomer in the cerebrospinal fluid of drug-naive patients with Parkinson’s disease. J Clin Neurol 2011;7(4):215-22.
12. Sierks MR, Chatterjee G, McGraw C, Kasturirangan S, Schulz P, Prasad S. CSF levels of oligomeric alpha-synu-clein and beta-amyloid as biomarkers for neurodegenerative disease. Integr Biol (Camb) 2011;3(12):1188-96.
13. Compta Y, Marti MJ, Ibarretxe-Bilbao N, et al. Cerebrospinal tau, phospho-tau, and beta-amyloid and neuro-psychological functions in Parkinson’s disease. Mov Disord 2009;24(15):2203-10.
14. Parnetti L, Chiasserini D, Bellomo G, et al. Cerebrospinal fluid Tau/alpha-synuclein ratio in Parkinson’s disease and degenerative dementias. Mov Disord 2011;26(8):1428-35.
15. Montine TJ, Shi M, Quinn JF, et al. CSF Abeta(42) and tau in Parkinson’s disease with cognitive impairment. Mov Disord 2010;25(15):2682-5.
16. Sussmuth SD, Uttner I, Landwehrmeyer B, et al. Differential pattern of brain-specific CSF proteins tau and amyloid-beta in Parkinsonian syndromes. Mov Disord 2010;25(9):1284-8.
17. Ohrfelt A, Grognet P, Andreasen N, et al. Cerebrospinal fluid alpha-synuclein in neurodegenerative disor-ders-a marker of synapse loss? Neurosci Lett 2009;450(3):332-5.

102
RESULTADOS6
18. Alves G, Bronnick K, Aarsland D, et al. CSF amyloid-beta and tau proteins, and cognitive performance, in early and untreated Parkinson’s disease: the Norwegian ParkWest study. J Neurol Neurosurg Psychiatry 2010;81(10):1080-6.
19. Parnetti L, Tiraboschi P, Lanari A, et al. Cerebrospinal fluid biomarkers in Parkinson’s disease with dementia and dementia with Lewy bodies. Biol Psychiatry 2008;64(10):850-5.
20. Shi M, Zhang J. CSF alpha-synuclein, tau, and amyloid beta in Parkinson’s disease. Lancet Neurol 2011;10(8):681; author’s reply 81-3.
21. Buongiorno M, Compta Y, Marti MJ. Amyloid-beta and tau biomarkers in Parkinson’s disease-dementia. J Neurol Sci 2011;310(1-2):25-30.
22. Compta Y, Pereira JB, Rios J, et al. Combined dementia-risk biomarkers in Parkinson’s disease: a prospective longitudinal study. Parkinsonism Relat Disord 2013;19(8):717-24.
23. Muslimovic D, Post B, Speelman JD, Schmand B. Cognitive profile of patients with newly diagnosed Parkinson disease. Neurology 2005;65(8):1239-45.
24. Aarsland D, Zaccai J, Brayne C. A systematic review of prevalence studies of dementia in Parkinson’s disease. Mov Disord 2005;20(10):1255-63.
25. Aasly JO, Shi M, Sossi V, et al. Cerebrospinal fluid amyloid beta and tau in LRRK2 mutation carriers. Neurology 2012;78(1):55-61.
26. Shi M, Furay AR, Sossi V, et al. DJ-1 and alphaSYN in LRRK2 CSF do not correlate with striatal dopaminergic function. Neurobiol Aging 2012;33(4):836 e5-7.
27. Aasly JO, Johansen KK, Bronstad G, et al. Elevated levels of cerebrospinal fluid alpha-synuclein oligomers in healthy asymptomatic LRRK2 mutation carriers. Front Aging Neurosci 2014;6:248.
28. The Unified Parkinson’s Disease Rating Scale (UPDRS): status and recommendations. Mov Disord 2003;18(7):738-50.
29. Goetz CG, Tilley BC, Shaftman SR, et al. Movement Disorder Society-sponsored revision of the Unified Parkin-son’s Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord 2008;23(15):2129-70.
30. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967;17(5):427-42.
31. Jankovic J, McDermott M, Carter J, et al. Variable expression of Parkinson’s disease: a base-line analysis of the DATATOP cohort. The Parkinson Study Group. Neurology 1990;40(10):1529-34.
32. Williams-Gray CH, Foltynie T, Brayne CE, Robbins TW, Barker RA. Evolution of cognitive dysfunction in an incident Parkinson’s disease cohort. Brain 2007;130(Pt 7):1787-98.
33. Giasson BI, Duda JE, Quinn SM, Zhang B, Trojanowski JQ, Lee VM. Neuronal alpha-synucleinopathy with severe movement disorder in mice expressing A53T human alpha-synuclein. Neuron 2002;34(4):521-33.
34. Waxman EA, Giasson BI. Induction of intracellular tau aggregation is promoted by alpha-synuclein seeds and provides novel insights into the hyperphosphorylation of tau. J Neurosci 2011;31(21):7604-18.
35. Braak H, Ghebremedhin E, Rub U, Bratzke H, Del Tredici K. Stages in the development of Parkinson’s disease-re-lated pathology. Cell Tissue Res 2004;318(1):121-34.

103
RESULTADOS 6
36. Gaig C, Tolosa E. When does Parkinson’s disease begin? Mov Disord. 2009;24 Suppl 2:S656-64.
37. Healy DG, Falchi M, O’Sullivan SS, ET AL. Phenotype, genotype, and worldwide genetic penetrance of LRRK2-associated Parkinson’s disease: a case-control study. Lancet Neurol. 2008 Jul;7(7):583-90.


Síntesis de resultados y discusión
CAPÍTULO 7


107
SÍNTESIS DE RESULTADOS Y DISCUSIÓN 7
Los trabajos presentados como parte de la memoria de esta tesis doctoral pretenden resaltar
la importancia del estudio de los síntomas no motores de la EP asociada a mutaciones del gen
LRRK2 y de su fase premotora.
Quedan por aclarar numerosas preguntas pero los resultados de esta tesis doctoral apuntan hacia
la idea de que la EP-LRRK2, aunque clínicamente similar a la EPI, presenta algunos rasgos dife-
renciales tanto clínicos, como de neuroimagen y bioquímicos. Asimismo los portadores asinto-
máticos de mutaciones del gen LRRK2 presentan alteraciones en la neuroimagen, tanto en la
sonografía transcraneal como en la resonancia magnética funcional, que preceden el inicio de
los síntomas motores en esta población en riesgo de desarrollar EP. A continuación resumimos y
discutimos los resultados más importantes de los cuatro trabajos incluidos en esta tesis doctoral.
En el trabajo número 1 (Nonmotor symptoms in LRRK2 G2019S associated Parkinson’s disease)
estudiamos la prevalencia y el momento de inicio de los SNM en la EP-LRRK2 y lo comparamos
con un grupo de pacientes con EPI de similar edad, sexo, duración y severidad de la EP, así como
con un grupo de sujetos sanos. Encontramos que los SNM, como las alteraciones neuropsiquiá-
tricas, disautonómicas y del sueño, son frecuentes en la EP-LRRK2. La depresión, la ansiedad y las
alucinaciones se observaron en una proporción similar a estudios previos en la EP-LRRK215,36,101.
Los trastornos del sueño, como el trastorno de conducta del sueño REM (TCSR), el insomnio, o el
exceso de somnolencia diurna también se han descrito en pacientes con EP-LRRK2. En un estudio
reciente se observó que sólo el 11 % de los pacientes con EP-LRRK2 presentaban TCSR comparado
con un 42 % en los pacientes con EPI, sugiriendo que el TCSR puede ser menos frecuente en esta
forma genética de EP 102. La frecuencia de estreñimiento y disfunción urinaria en nuestro estudio
fue similar a la reportada por otros 3,36.
En este estudio encontramos, además, que el único SNM que diferencia la EP-LRRK2 y la EPI es
la pérdida de olfato, presente en sólo un 39 % de los pacientes con EP-LRRK2 pero en un 75 %
en los pacientes con EPI. No se conocen las razones que explican esta diferencia. Por un lado
podríamos pensar que la heterogénea neuropatología encontrada en la EP-LRRK2, con una menor

108
SÍNTESIS DE RESULTADOS Y DISCUSIÓN7
afectación de las estructuras olfatorias en este tipo de Parkinson genético son las responsables
de esta diferencia. El hecho de que en el Parkinson asociado a mutaciones del gen Parkin, otro
tipo de Parkinson genético, sea frecuente la ausencia de hiposmia y con unas alteraciones neuro-
patológicas habitualmente limitadas a la SN, sin cuerpos de Lewy, apoyaría esta hipótesis 103-104.
No obstante, sólo un 20 % de los casos de EP-LRRK2 asociados a la mutación G2019S presentan
unos hallazgos patológicos diferentes a la EPI 29, por lo que una neuropatología distinta no expli-
caría totalmente la relativa preservación del sentido del olfato en la mayoría de los EP-LRRK2.
En este primer trabajo encontramos que el olfato está particularmente preservado en las mujeres
con EP-LRRK2. Este hallazgo podría sugerir un efecto de género en la expresión de la EP-LRRK2.
Los factores de susceptibilidad asociados al sexo probablemente jueguen un papel en la EP, enfer-
medad más frecuente en varones 105, mientras que en la EP-LRRK2 asociada a la mutación G2019S
se ha propuesto una predominancia del sexo femenino 106 .
Una proporción importante de pacientes con EP-LRRK2 percibía que varios SNM, como la hiposmia,
la depresión, el estreñimiento o el exceso de somnolencia diurna, estaban presentes antes del
inicio de los síntomas motores. Algunos de estos SNM han sido evaluados en aLRRK2 36-37,107, encon-
trando que la hiposmia, la depresión y el estreñimiento pueden ocurrir en este grupo de sujetos en
riesgo de EP. Esta percepción de que ciertos SNM anteceden el comienzo de los síntomas motores
es similar a lo que ocurre en la EPI y sugiere que estos síntomas pueden caracterizar clínicamente
la fase prodrómica del Parkinson LRRK2. Estos síntomas podrían estar asociados a cambios neuro-
patológicos en estructuras no dopaminérgicas del tronco encefálico y en el sistema nervioso peri-
férico, como sugirió Braak para la EPI 31.
En el trabajo número 2 (Clinical and imaging markers in premotor LRRK2 G2019S muta-
tion carriers) nos planteamos evaluar la ecogenicidad de la sustancia nigra y otras varia-
bles ecográficas en pacientes con EP-LRRK2 y en aLRRK2, portadores de la mutación G2019S.
Con fines comparativos, estudiamos los mismos parámetros en un grupo de pacientes con
EPI, en familiares de primer grado de pacientes con EP-LRRK2 pero no portadores de la muta-
ción, y en un grupo de controles, sujetos sanos sin parentesco con los anteriores grupos.

109
SÍNTESIS DE RESULTADOS Y DISCUSIÓN 7
En este trabajo observamos en los pacientes con EP-LRRK2 una hiperecogenicidad de la SN en una
proporción similar a los pacientes con EPI y similar a la reportada en la literatura en otros casos de
EP-LRRK2 16,57. Observamos también que la hiperecogenicidad de la SN era frecuente en los aLRRK2,
sugiriendo que este hallazgo ecográfico podría ser una marcador de la fase premotora de la EP-LRRK2.
La hiperecogenicidad de la SN, asociada a depósito de hierro, es un marcador de riesgo de la
vulnerabilidad de las células dopaminérgicas de la SN y, además, se mantiene estable a lo largo de
la evolución de la EP, por lo que se piensa que puede ser un buen marcador en sujetos en riesgo
de padecer EP. La EP-LRRK2 tiene una penetrancia variable, de manera que no todos los aLRRK2
desarrollarán la enfermedad. Podríamos pues pensar que, entre los aLRRK2, aquellos con hipere-
cogenicidad de la SN son los que desarrollarán EP.
Por otra parte, teniendo en cuenta que la alteración de la vía nigroestriatal estudiada mediante
un SPECT con transportador de dopamina (DAT-SPECT) es un marcador subrogado de la enfer-
medad en sujetos en riesgo de desarrollar EP 108-109, si la hiperecogenicidad de la SN fuera un
marcador de riesgo de EP, deberíamos encontrar esta alteración ecográfica en los aLRRK2 con un
DAT-SPECT alterado. En nuestra muestra, cuatro de los cinco casos de aLRRK2 con un DAT-SPECT
alterado tenían también hiperecogenicidad de la SN. Los resultados del estudio de Sierra y cols.
están en línea con nuestras observaciones ya que el 90 % de los aLRRK2 con un DAT-SPECT alte-
rado tenían también hiperecogenicidad de la SN. En este segundo trabajo también encontramos
que el 66.7 % de los aLRRK2 con hiperecogenicidad de la SN tenían un DAT-SPECT normal. Este
resultado apoya el concepto de que la hiperecogenicidad de la SN es un marcador estable de la
enfermedad, no un marcador de la evolución de la misma.
No encontramos ninguna diferencia clínica entre los aLRRK2 con y sin hiperecogenicidad de la
SN en este estudio. Esto puede deberse a que este grupo de aLRRK2 todavía no ha alcanzado
el umbral de desarrollo de la enfermedad necesario para manifestar los primeros síntomas no
motores, tal vez debido a su edad relativamente corta. También puede reflejar este hallazgo que
la fase premotora de la EP-LRRK2 es diferente a la de la EPI.

110
SÍNTESIS DE RESULTADOS Y DISCUSIÓN7
Otro hallazgo importante de este trabajo es que el 25 % de los familiares no portadores de la
mutación tienen también hiperecogenicidad de la SN, una frecuencia superior a la encontrada en
los controles (12.5 %). Este hallazgo, observado también por otros autores 57 es de difícil explica-
ción. Otros factores genéticos, epigenéticos o ambientales, acompañantes a la mutación G2019S,
pueden tener un papel en la modificación de la vulnerabilidad del sistema nigroestriatal y, conse-
cuentemente, en una mayor frecuencia de hiperecogenicidad de la SN.
Encontramos además que los pacientes con EP-LRRK2 tenían un tamaño del tercer ventrí-
culo menor que los pacientes con EPI, especialmente aquellos sujetos mayores de 60 años.
Este hallazgo no ha sido reportado con anterioridad en la literatura. El mayor tamaño ventricular
en la EPI podría explicarse por una mayor atrofia subcortical, lo que iría en línea con un curso más
benigno desde el punto de vista cognitivo en la EP-LRRK2 3. También se podría explicar por la
heterogeneidad neuropatológica, como comentamos previamente. Estos hallazgos, no obstante,
deben confirmarse en futuros estudios.
En el trabajo número 3 (Reduced thalamo-cortical functional connectivity in asymptomatic
LRRK2 mutation carriers) nos propusimos estudiar la presencia de alteraciones en la resonancia
magnética cerebral en sujetos aLRRK2 caracterizando los patrones de RMf durante el estado
de reposo en un grupo de aLRRK2, comparándolos con familiares no portadores de la muta-
ción. Encontramos que los aLRRK2 presentaron una disminución en la conectividad funcional
entre el tálamo izquierdo y áreas corticales contralaterales, incluyendo el girus postcentral, el
girus frontal inferior, el girus temporal medio e inferior, y el córtex occipital, y también entre el
caudado izquierdo y el córtex sensitivomotor bilateral. Observamos además una reducción de la
conectividad funcional entre el tálamo izquierdo y el córtex motor bilateral, así como desde las
regiones primarias somatosensoriales y el córtex motor primario. Estos resultados están en línea
con estudios de RMf en pacientes con EP, donde se encontró una disminución de la conectividad
funcional entre el tálamo y el córtex sensitivo-motor 65 y entre el estriado y el tálamo, mesen-
céfalo, protuberancia y cerebelo 66. Incluso se han observado disminuciones de la conectividad
funcional del caudado y tálamo con el córtex frontal e insular, en pacientes en fases muy iniciales

111
SÍNTESIS DE RESULTADOS Y DISCUSIÓN 7
de la EP, antes de iniciar el tratamiento 67 y en las conexiones mesolímbicas y corticoestriatales 68.
Nuestros hallazgos sugieren también que las alteraciones en la conectividad funcional preceden
a los cambios estructurales. En la actualidad no hay estudios publicados sobre la conectividad
funcional en las fases preclínicas de la EPI. Sí hay estudios en fases preclínicas de otras enferme-
dades neurodegenerativas como en la enfermedad de Alzheimer 71 y la enfermedad de Huntin-
gton 72, donde se describen disminuciones en la conectividad funcional cerebral.
Por último, en el trabajo número 4 (Cerebrospinal fluid biomarkers and clinical features in
leucine-rich repeat kinase 2 (LRRK2) mutation carriers) estudiamos los niveles de α-syn y
otras proteínas asociadas a la enfermedad de Alzheimer, como α-syn, Aβ1-42, T-tau, y p-tau181 en
EP-LRRK2, EPI, aLRRK2 y familiares de primer grado de pacientes EP-LRRK2 no portadores de la
mutación. Encontramos que los niveles de α-syn fueron similares entre los pacientes con EP-LRRK2,
los aLRRK2 y los familiares asintomáticos no portadores pero significativamente más elevados que
en los pacientes con EPI. Estudios recientes en EPI, incluso en fases precoces de la enfermedad,
mostraron una disminución en los niveles de α-syn. Esta diferencia que nosotros hemos encon-
trado en los niveles de α-syn entre EP-LRRK2 y EPI puede ser el reflejo de una menor carga de
α-syn a nivel cerebral o de un sustrato neuropatológico diferente. Por otro lado, no encontramos
diferencias entre las concentraciones de Aβ1-42, T-tau, y p-tau181 entre los grupos de estudio. Los
estudios previos en EPI sobre proteínas en LCR asociadas a la enfermedad de Alzheimer mostraron
resultados dispares. Mientras que algunos autores encontraron unos niveles de Aβ1-42 bajos en la
EPI 78,87, otros no pudieron llegar a las mismas conclusiones 88-90. Lo mismo ocurre con los niveles
de T-tau, y p-tau181. Las discrepancias en los resultados se pueden explicar, al menos en parte, por
la diferente metodología empleada, incluyendo el procesamiento del LCR, la técnica empleada y
la diversidad en los criterios de inclusión de los sujetos estudiados.
En este trabajo 4 encontramos una fuerte correlación entre los niveles de α-syn y los niveles de
T-tau, y p-tau181 en todos los grupos, sugiriendo una interacción entre la α-syn y las proteínas
asociadas a la enfermedad de Alzheimer. La α-syn presenta interacciones dinámicas con la
proteína tau y tienen la tendencia a favorecer la agregación de la otra 110-111. Nosotros encontramos

112
SÍNTESIS DE RESULTADOS Y DISCUSIÓN7
esta correlación en los pacientes con EP y también en aLRRK2, sugiriendo que esta interacción
puede ser independiente del proceso que subyace a la enfermedad.
No detectamos diferencias en las proteínas en LCR entre los aLRRK2 y los familiares no porta-
dores de la mutación, lo que sugiere quelas proteínas en LCR no son un buen marcador de la
enfermedad en estos. Son necesarios estudios longitudinales en este grupo concreto de sujetos,
preferiblemente complementados con biomarcadores clínicos, bioquímicos o de neuroimagen
para poder evaluar en mayor profundidad el valor real de estos biomarcadores.
En resumen en esta defensa de tesis doctoral se ha querido ahondar en la caracterización de la
enfermedad de Parkinson asociada a mutaciones del gen LRRK2 tanto en su forma manifiesta o
declarada como en la de los sujetos asintomáticos portadores de mutaciones de este gen.



CAPÍTULO 8
Conclusiones


117
CONCLUSIONES 8
1. Los síntomas no motores son frecuentes en los pacientes con enfermedad de Parkinson
asociada a mutaciones del gen LRRK2. Algunos de ellos, como las alteraciones neuropsi-
quiátricas, disautonómicas y del sueño, se presentan con una frecuencia similar a la de los
pacientes con enfermedad de Parkinson idiopática, mientras que la hiposmia es menos
frecuente en los pacientes con este tipo de Parkinson genético.
2. Los pacientes con enfermedad de Parkinson asociada a la mutación G2019S del gen LRRK2
perciben el comienzo de ciertos síntomas no motores, como hiposmia, depresión, estreñi-
miento y exceso de somnolencia diurna, anterior al inicio de los síntomas motores clásicos.
Estos síntomas no motores podrían caracterizar clínicamente la fase prodrómica de la enfer-
medad de Parkinson asociada a mutaciones del gen LRRK2, al igual que ocurre en la enfer-
medad de Parkinson idiopática.
3. La hiperecogenicidad de la SN es frecuente en los portadores asintomáticos de mutaciones
del gen LRRK2. Este hallazgo ecográfico puede representar un marcador de la enfermedad
en esta población asintomática.
4. Los portadores asintomáticos de una mutación del gen LRRK2 presentan una disminución
en la conectividad funcional en el circuito tálamo-cortical en la resonancia magnética
funcional. Este hallazgo sugiere que, en los sujetos asintomáticos, ocurren cambios en la
conectividad cerebral que anteceden el inicio de los síntomas motores clásicos y la apari-
ción de cambios estructurales.
5. El perfil proteico en LCR, alfa-sinucleína y proteínas asociadas a la enfermedad de Alzheimer,
es diferente en la EP-LRRK2 y en la EPI sugiriendo que los mecanismos fisiopatológicos que
subyacen a ambas patologías son diferentes.
6. Los portadores asintomáticos de una mutación del gen LRRK2 presentan en LCR un perfil
proteico (sinucleína y proteínas asociadas a la enfermedad de Alzheimer) similar a los sujetos
no portadores. Los niveles en LCR de estas proteínas no son pues marcadores de enfer-
medad LRRK2 asintomática.


Bibliografía
CAPÍTULO 9


121
BIBLIOGRAFÍA 9
1. Paisan-Ruiz C, Jain S, Evans EW, Gilks WP, Simon J, van der Brug M, et al. Cloning of the gene containing mutations that cause PARK8-linked Parkinson’s disease. Neuron 2004;44(4):595-600.
2. Zimprich A, Biskup S, Leitner P, Lichtner P, Farrer M, Lincoln S, et al. Mutations in LRRK2 cause autoso-mal-dominant parkinsonism with pleomorphic pathology. Neuron 2004;44(4):601-7.
3. Healy DG, Falchi M, O’Sullivan SS, Bonifati V, Durr A, Bressman S, et al. Phenotype, genotype, and world-wide genetic penetrance of LRRK2-associated Parkinson’s disease: a case-control study. Lancet Neurol 2008;7(7):583-90.
4. Zabetian CP, Hutter CM, Yearout D, Lopez AN, Factor SA, Griffith A, et al. LRRK2 G2019S in families with Parkinson disease who originated from Europe and the Middle East: evidence of two distinct founding events beginning two millennia ago. Am J Hum Genet 2006;79(4):752-8.
5. Sierra M, Gonzalez-Aramburu I, Sanchez-Juan P, Sanchez-Quintana C, Polo JM, Berciano J, et al. High frequency and reduced penetrance of LRRK2 G2019S mutation among Parkinson’s disease patients in Cantabria (Spain). Mov Disord 2011;26(13):2343-6.
6. Gaig C, Ezquerra M, Marti MJ, Munoz E, Valldeoriola F, Tolosa E. LRRK2 mutations in Spanish patients with Parkinson disease: frequency, clinical features, and incomplete penetrance. Arch Neurol 2006;63(3):377-82.
7. Gorostidi A, Ruiz-Martinez J, Lopez de Munain A, Alzualde A, Marti Masso JF. LRRK2 G2019S and R1441G mutations associated with Parkinson’s disease are common in the Basque Country, but relative prevalence is determined by ethnicity. Neurogenetics 2009;10(2):157-9.
8. Mata IF, Ross OA, Kachergus J, Huerta C, Ribacoba R, Moris G, et al. LRRK2 mutations are a common cause of Parkinson’s disease in Spain. Eur J Neurol 2006;13(4):391-4.
9. Moran JM, Castellanos-Pinedo F, Casado-Naranjo I, Duran-Herrera C, Ramirez-Moreno JM, Gomez M, et al. [Genetic screening for the LRRK2, G2019S and R1441 codon mutations in Parkinson’s disease patients from Extremadura, Spain]. Rev Neurol 2010;50(10):591-4.
10. Kachergus J, Mata IF, Hulihan M, Taylor JP, Lincoln S, Aasly J, et al. Identification of a novel LRRK2 mutation linked to autosomal dominant parkinsonism: evidence of a common founder across European populations. Am J Hum Genet 2005;76(4):672-80.
11. Latourelle JC, Sun M, Lew MF, Suchowersky O, Klein C, Golbe LI, et al. The Gly2019Ser mutation in LRRK2 is not fully penetrant in familial Parkinson’s disease: the GenePD study. BMC Med 2008;6:32.
12. Lesage S, Ibanez P, Lohmann E, Pollak P, Tison F, Tazir M, et al. G2019S LRRK2 mutation in French and North African families with Parkinson’s disease. Ann Neurol 2005;58(5):784-7.
13. Clark LN, Wang Y, Karlins E, Saito L, Mejia-Santana H, Harris J, et al. Frequency of LRRK2 mutations in early- and late-onset Parkinson disease. Neurology 2006;67(10):1786-91.
14. Goldwurm S, Zini M, Mariani L, Tesei S, Miceli R, Sironi F, et al. Evaluation of LRRK2 G2019S penetrance: rele-vance for genetic counseling in Parkinson disease. Neurology 2007;68(14):1141-3.
15. Goldwurm S, Zini M, Di Fonzo A, De Gaspari D, Siri C, Simons EJ, et al. LRRK2 G2019S mutation and Parkin-son’s disease: a clinical, neuropsychological and neuropsychiatric study in a large Italian sample. Parkin-sonism Relat Disord 2006;12(7):410-9.
16. Brockmann K, Groger A, Di Santo A, Liepelt I, Schulte C, Klose U, et al. Clinical and brain imaging charac-teristics in leucine-rich repeat kinase 2-associated PD and asymptomatic mutation carriers. Mov Disord 2011;26(13):2335-42.

122
BIBLIOGRAFÍA9
17. Clarimon J, Pagonabarraga J, Paisan-Ruiz C, Campolongo A, Pascual-Sedano B, Marti-Masso JF, et al. Tremor dominant parkinsonism: Clinical description and LRRK2 mutation screening. Mov Disord 2008;23(4):518-23.
18. Haugarvoll K, Uitti RJ, Farrer MJ, Wszolek ZK. LRRK2 gene and tremor-dominant parkinsonism. Arch Neurol 2006;63(9):1346-7.
19. Alcalay RN, Mejia-Santana H, Tang MX, Rosado L, Verbitsky M, Kisselev S, et al. Motor phenotype of LRRK2 G2019S carriers in early-onset Parkinson disease. Arch Neurol 2009;66(12):1517-22.
20. Chaudhuri KR, Odin P, Antonini A, Martinez-Martin P. Parkinson’s disease: the non-motor issues. Parkin-sonism Relat Disord 2011;17(10):717-23.
21. Pont-Sunyer C, Iranzo A, Gaig C, Fernandez-Arcos A, Vilas D, Valldeoriola F, et al. Sleep Disorders in Parkinso-nian and Nonparkinsonian LRRK2 Mutation Carriers. PLoS One 2015;10(7):e0132368.
22. Valldeoriola F, Gaig C, Muxi A, Navales I, Paredes P, Lomena F, et al. 123I-MIBG cardiac uptake and smell iden-tification in parkinsonian patients with LRRK2 mutations. J Neurol 2011;258(6):1126-32.
23. Kumar A, Cookson MR. Role of LRRK2 kinase dysfunction in Parkinson disease. Expert Rev Mol Med 2011;13:e20.
24. Liu GH, Qu J, Suzuki K, Nivet E, Li M, Montserrat N, et al. Progressive degeneration of human neural stem cells caused by pathogenic LRRK2. Nature 2012;491(7425):603-7.
25. Li JQ, Tan L, Yu JT. The role of the LRRK2 gene in Parkinsonism. Mol Neurodegener 2014;9:47.
26. Funayama M, Hasegawa K, Kowa H, Saito M, Tsuji S, Obata F. A new locus for Parkinson’s disease (PARK8) maps to chromosome 12p11.2-q13.1. Ann Neurol 2002;51(3):296-301.
27. Lorenzo-Betancor O, Samaranch L, Ezquerra M, Tolosa E, Lorenzo E, Irigoyen J, et al. LRRK2 haplotype-sharing analysis in Parkinson’s disease reveals a novel p.S1761R mutation. Mov Disord 2012;27(1):146-51.
28. Wszolek ZK, Pfeiffer RF, Tsuboi Y, Uitti RJ, McComb RD, Stoessl AJ, et al. Autosomal dominant parkinsonism associated with variable synuclein and tau pathology. Neurology 2004;62(9):1619-22.
29. Poulopoulos M, Levy OA, Alcalay RN. The neuropathology of genetic Parkinson’s disease. Mov Disord 2012;27(7):831-42.
30. Kalia LV, Lang AE, Hazrati LN, Fujioka S, Wszolek ZK, Dickson DW, et al. Clinical correlations with Lewy body pathology in LRRK2-related Parkinson disease. JAMA Neurol 2015;72(1):100-5.
31. Braak H, Del Tredici K, Rub U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging 2003;24(2):197-211.
32. Tolosa E, Poewe W. Premotor Parkinson disease. Neurology 2009;72(7 Suppl):S1.
33. Ross GW, Petrovitch H, Abbott RD, Tanner CM, Popper J, Masaki K, et al. Association of olfactory dysfunction with risk for future Parkinson’s disease. Ann Neurol 2008;63(2):167-73.
34. Iranzo A, Molinuevo JL, Santamaria J, Serradell M, Marti MJ, Valldeoriola F, et al. Rapid-eye-movement sleep behaviour disorder as an early marker for a neurodegenerative disorder: a descriptive study. Lancet Neurol 2006;5(7):572-7.
35. Shiba M, Bower JH, Maraganore DM, McDonnell SK, Peterson BJ, Ahlskog JE, et al. Anxiety disorders and depressive disorders preceding Parkinson’s disease: a case-control study. Mov Disord 2000;15(4):669-77.

123
BIBLIOGRAFÍA 9
36. Marras C, Schule B, Munhoz RP, Rogaeva E, Langston JW, Kasten M, et al. Phenotype in parkinsonian and nonparkinsonian LRRK2 G2019S mutation carriers. Neurology 2011;77(4):325-33.
37. Saunders-Pullman R, Stanley K, Wang C, San Luciano M, Shanker V, Hunt A, et al. Olfactory dysfunction in LRRK2 G2019S mutation carriers. Neurology 2011;77(4):319-24.
38. Mirelman A, Alcalay RN, Saunders-Pullman R, Yasinovsky K, Thaler A, Gurevich T, et al. Nonmotor symptoms in healthy Ashkenazi Jewish carriers of the G2019S mutation in the LRRK2 gene. Mov Disord 2015;30(7):981-6.
39. Mirelman A, Gurevich T, Giladi N, Bar-Shira A, Orr-Urtreger A, Hausdorff JM. Gait alterations in healthy carriers of the LRRK2 G2019S mutation. Ann Neurol 2011;69(1):193-7.
40. Thaler A, Mirelman A, Gurevich T, Simon E, Orr-Urtreger A, Marder K, et al. Lower cognitive performance in healthy G2019S LRRK2 mutation carriers. Neurology 2012;79(10):1027-32.
41. Lohmann E, Leclere L, De Anna F, Lesage S, Dubois B, Agid Y, et al. A clinical, neuropsychological and olfac-tory evaluation of a large family with LRRK2 mutations. Parkinsonism Relat Disord 2009;15(4):273-6.
42. Becker G, Seufert J, Bogdahn U, Reichmann H, Reiners K. Degeneration of substantia nigra in chronic Parkin-son’s disease visualized by transcranial color-coded real-time sonography. Neurology 1995;45(1):182-4.
43. Berg D, Godau J, Walter U. Transcranial sonography in movement disorders. Lancet Neurol 2008;7(11):1044-55.
44. Berg D, Becker G, Zeiler B, Tucha O, Hofmann E, Preier M, et al. Vulnerability of the nigrostriatal system as detected by transcranial ultrasound. Neurology 1999;53(5):1026-31.
45. Berg D, Roggendorf W, Schroder U, Klein R, Tatschner T, Benz P, et al. Echogenicity of the substantia nigra: association with increased iron content and marker for susceptibility to nigrostriatal injury. Arch Neurol 2002;59(6):999-1005.
46. Berg D, Behnke S, Seppi K, Godau J, Lerche S, Mahlknecht P, et al. Enlarged hyperechogenic substantia nigra as a risk marker for Parkinson’s disease. Mov Disord 2013;28(2):216-9.
47. Berg D, Merz B, Reiners K, Naumann M, Becker G. Five-year follow-up study of hyperechogenicity of the substantia nigra in Parkinson’s disease. Mov Disord 2005;20(3):383-5.
48. Sommer U, Hummel T, Cormann K, Mueller A, Frasnelli J, Kropp J, et al. Detection of presymptomatic Parkin-son’s disease: combining smell tests, transcranial sonography, and SPECT. Mov Disord 2004;19(10):1196-202.
49. Iranzo A, Lomena F, Stockner H, Valldeoriola F, Vilaseca I, Salamero M, et al. Decreased striatal dopamine transporter uptake and substantia nigra hyperechogenicity as risk markers of synucleinopathy in patients with idiopathic rapid-eye-movement sleep behaviour disorder: a prospective study [corrected]. Lancet Neurol 2010;9(11):1070-7.
50. Saunders-Pullman R, Stanley K, Bruggemann N, Raymond D, San Luciano M, Wang C, et al. Substantia nigra hyperechogenicity in DYT6 dystonia: a pilot study. Parkinsonism Relat Disord 2010;16(6):420-2.
51. Lambeck J, Niesen WD, Reinhard M, Weiller C, Dose M, Zucker B. Substantia nigra hyperechogenicity in hypokinetic Huntington’s disease patients. J Neurol 2015;262(3):711-7.
52. Kostic VS, Mijajlovic M, Smajlovic D, Lukic MJ, Tomic A, Svetel M. Transcranial brain sonography findings in two main variants of progressive supranuclear palsy. Eur J Neurol 2013;20(3):552-7.
53. Walter U, Buttkus F, Benecke R, Grossmann A, Dressler D, Altenmuller E. Sonographic alteration of lenticular nucleus in focal task-specific dystonia of musicians. Neurodegener Dis 2012;9(2):99-103.

124
BIBLIOGRAFÍA9
54. Walter U, Skowronska M, Litwin T, Szpak GM, Jablonka-Salach K, Skoloudik D, et al. Lenticular nucleus hyperecho-genicity in Wilson’s disease reflects local copper, but not iron accumulation. J Neural Transm 2014;121(10):1273-9.
55. Vilas D, Iranzo A, Pont-Sunyer C, Serradell M, Gaig C, Santamaria J, et al. Brainstem raphe and substantia nigra echogenicity in idiopathic REM sleep behavior disorder with comorbid depression. J Neurol 2015;262(7):1665-72.
56. Berg D, Grote C, Rausch WD, Maurer M, Wesemann W, Riederer P, et al. Iron accumulation in the substantia nigra in rats visualized by ultrasound. Ultrasound Med Biol 1999;25(6):901-4.
57. Sierra M, Sanchez-Juan P, Martinez-Rodriguez MI, Gonzalez-Aramburu I, Garcia-Gorostiaga I, Quirce MR, et al. Olfaction and imaging biomarkers in premotor LRRK2 G2019S-associated Parkinson disease. Neurology 2013;80(7):621-6.
58. Pereira JB, Ibarretxe-Bilbao N, Marti MJ, Compta Y, Junque C, Bargallo N, et al. Assessment of cortical degen-eration in patients with Parkinson’s disease by voxel-based morphometry, cortical folding, and cortical thickness. Hum Brain Mapp 2012;33(11):2521-34.
59. Yoshikawa K, Nakata Y, Yamada K, Nakagawa M. Early pathological changes in the parkinsonian brain demonstrated by diffusion tensor MRI. J Neurol Neurosurg Psychiatry 2004;75(3):481-4.
60. Vaillancourt DE, Spraker MB, Prodoehl J, Abraham I, Corcos DM, Zhou XJ, et al. High-resolution diffusion tensor imaging in the substantia nigra of de novo Parkinson disease. Neurology 2009;72(16):1378-84.
61. Segura B, Baggio HC, Marti MJ, Valldeoriola F, Compta Y, Garcia-Diaz AI, et al. Cortical thinning associated with mild cognitive impairment in Parkinson’s disease. Mov Disord 2014;29(12):1495-503.
62. Biswal B, Yetkin FZ, Haughton VM, Hyde JS. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn Reson Med 1995;34(4):537-41.
63. Helmich RC, Aarts E, de Lange FP, Bloem BR, Toni I. Increased dependence of action selection on recent motor history in Parkinson’s disease. J Neurosci 2009;29(19):6105-13.
64. Helmich RC, Bloem BR, Toni I. Motor imagery evokes increased somatosensory activity in Parkinson’s disease patients with tremor. Hum Brain Mapp 2012;33(8):1763-79.
65. Sharman M, Valabregue R, Perlbarg V, Marrakchi-Kacem L, Vidailhet M, Benali H, et al. Parkinson’s disease patients show reduced cortical-subcortical sensorimotor connectivity. Mov Disord 2013;28(4):447-54.
66. Hacker CD, Perlmutter JS, Criswell SR, Ances BM, Snyder AZ. Resting state functional connectivity of the striatum in Parkinson’s disease. Brain 2012;135(Pt 12):3699-711.
67. Agosta F, Caso F, Stankovic I, Inuggi A, Petrovic I, Svetel M, et al. Cortico-striatal-thalamic network functional connectivity in hemiparkinsonism. Neurobiol Aging 2014;35(11):2592-602.
68. Luo C, Song W, Chen Q, Zheng Z, Chen K, Cao B, et al. Reduced functional connectivity in early-stage drug-naive Parkinson’s disease: a resting-state fMRI study. Neurobiol Aging 2014;35(2):431-41.
69. Baudrexel S, Witte T, Seifried C, von Wegner F, Beissner F, Klein JC, et al. Resting state fMRI reveals increased subthalamic nucleus-motor cortex connectivity in Parkinson’s disease. Neuroimage 2011;55(4):1728-38.
70. Yu R, Liu B, Wang L, Chen J, Liu X. Enhanced functional connectivity between putamen and supplementary motor area in Parkinson’s disease patients. PLoS One 2013;8(3):e59717.
71. Sheline YI, Raichle ME, Snyder AZ, Morris JC, Head D, Wang S, et al. Amyloid plaques disrupt resting state default mode network connectivity in cognitively normal elderly. Biol Psychiatry 2010;67(6):584-7.

125
BIBLIOGRAFÍA 9
72. Harrington DL, Rubinov M, Durgerian S, Mourany L, Reece C, Koenig K, et al. Network topology and func-tional connectivity disturbances precede the onset of Huntington’s disease. Brain 2015;138(Pt 8):2332-46.
73. Reetz K, Tadic V, Kasten M, Bruggemann N, Schmidt A, Hagenah J, et al. Structural imaging in the presymp-tomatic stage of genetically determined parkinsonism. Neurobiol Dis 2010;39(3):402-8.
74. Thaler A, Mirelman A, Helmich RC, van Nuenen BF, Rosenberg-Katz K, Gurevich T, et al. Neural correlates of executive functions in healthy G2019S LRRK2 mutation carriers. Cortex 2013;49(9):2501-11.
75. van Nuenen BF, Helmich RC, Ferraye M, Thaler A, Hendler T, Orr-Urtreger A, et al. Cerebral pathological and compensatory mechanisms in the premotor phase of leucine-rich repeat kinase 2 parkinsonism. Brain 2012;135(Pt 12):3687-98.
76. Helmich RC, Thaler A, van Nuenen BF, Gurevich T, Mirelman A, Marder KS, et al. Reorganization of corticostri-atal circuits in healthy G2019S LRRK2 carriers. Neurology 2015;84(4):399-406.
77. Buongiorno M, Compta Y, Marti MJ. Amyloid-beta and tau biomarkers in Parkinson’s disease-dementia. J Neurol Sci 2011;310(1-2):25-30.
78. Shi M, Bradner J, Hancock AM, Chung KA, Quinn JF, Peskind ER, et al. Cerebrospinal fluid biomarkers for Parkinson disease diagnosis and progression. Ann Neurol 2011;69(3):570-80.
79. Kang JH, Irwin DJ, Chen-Plotkin AS, Siderowf A, Caspell C, Coffey CS, et al. Association of cerebrospinal fluid beta-amyloid 1-42, T-tau, p-tau181, and alpha-synuclein levels with clinical features of drug-naive patients with early Parkinson disease. JAMA Neurol 2013;70(10):1277-87.
80. Hall S, Ohrfelt A, Constantinescu R, Andreasson U, Surova Y, Bostrom F, et al. Accuracy of a panel of 5 cere-brospinal fluid biomarkers in the differential diagnosis of patients with dementia and/or parkinsonian disor-ders. Arch Neurol 2012;69(11):1445-52.
81. Mollenhauer B, Locascio JJ, Schulz-Schaeffer W, Sixel-Doring F, Trenkwalder C, Schlossmacher MG. alpha-Sy-nuclein and tau concentrations in cerebrospinal fluid of patients presenting with parkinsonism: a cohort study. Lancet Neurol 2011;10(3):230-40.
82. Mollenhauer B, Trautmann E, Taylor P, Manninger P, Sixel-Doring F, Ebentheuer J, et al. Total CSF alpha-synu-clein is lower in de novo Parkinson patients than in healthy subjects. Neurosci Lett 2013;532:44-8.
83. Hong Z, Shi M, Chung KA, Quinn JF, Peskind ER, Galasko D, et al. DJ-1 and alpha-synuclein in human cere-brospinal fluid as biomarkers of Parkinson’s disease. Brain 2010;133(Pt 3):713-26.
84. Tokuda T, Qureshi MM, Ardah MT, Varghese S, Shehab SA, Kasai T, et al. Detection of elevated levels of alpha-synuclein oligomers in CSF from patients with Parkinson disease. Neurology 2010;75(20):1766-72.
85. Sierks MR, Chatterjee G, McGraw C, Kasturirangan S, Schulz P, Prasad S. CSF levels of oligomeric alpha-synu-clein and beta-amyloid as biomarkers for neurodegenerative disease. Integr Biol (Camb) 2011;3(12):1188-96.
86. Park MJ, Cheon SM, Bae HR, Kim SH, Kim JW. Elevated levels of alpha-synuclein oligomer in the cerebro-spinal fluid of drug-naive patients with Parkinson’s disease. J Clin Neurol 2011;7(4):215-22.
87. Compta Y, Marti MJ, Ibarretxe-Bilbao N, Junque C, Valldeoriola F, Munoz E, et al. Cerebrospinal tau, phospho-tau, and beta-amyloid and neuropsychological functions in Parkinson’s disease. Mov Disord 2009;24(15):2203-10.
88. Parnetti L, Chiasserini D, Bellomo G, Giannandrea D, De Carlo C, Qureshi MM, et al. Cerebrospinal fluid Tau/alpha-synuclein ratio in Parkinson’s disease and degenerative dementias. Mov Disord 2011;26(8):1428-35.

126
BIBLIOGRAFÍA9
89. Montine TJ, Shi M, Quinn JF, Peskind ER, Craft S, Ginghina C, et al. CSF Abeta(42) and tau in Parkinson’s disease with cognitive impairment. Mov Disord 2010;25(15):2682-5.
90. Sussmuth SD, Uttner I, Landwehrmeyer B, Pinkhardt EH, Brettschneider J, Petzold A, et al. Differential pattern of brain-specific CSF proteins tau and amyloid-beta in Parkinsonian syndromes. Mov Disord 2010;25(9):1284-8.
91. Ohrfelt A, Grognet P, Andreasen N, Wallin A, Vanmechelen E, Blennow K, et al. Cerebrospinal fluid alpha-sy-nuclein in neurodegenerative disorders-a marker of synapse loss? Neurosci Lett 2009;450(3):332-5.
92. Alves G, Bronnick K, Aarsland D, Blennow K, Zetterberg H, Ballard C, et al. CSF amyloid-beta and tau proteins, and cognitive performance, in early and untreated Parkinson’s disease: the Norwegian ParkWest study. J Neurol Neurosurg Psychiatry 2010;81(10):1080-6.
93. Parnetti L, Tiraboschi P, Lanari A, Peducci M, Padiglioni C, D’Amore C, et al. Cerebrospinal fluid biomarkers in Parkinson’s disease with dementia and dementia with Lewy bodies. Biol Psychiatry 2008;64(10):850-5.
94. Shi M, Zhang J. CSF alpha-synuclein, tau, and amyloid beta in Parkinson’s disease. Lancet Neurol 2011;10(8):681; author’s reply 81-3.
95. Compta Y, Pereira JB, Rios J, Ibarretxe-Bilbao N, Junque C, Bargallo N, et al. Combined dementia-risk biomarkers in Parkinson’s disease: a prospective longitudinal study. Parkinsonism Relat Disord 2013;19(8):717-24.
96. Muslimovic D, Post B, Speelman JD, Schmand B. Cognitive profile of patients with newly diagnosed Parkinson disease. Neurology 2005;65(8):1239-45.
97. Aarsland D, Zaccai J, Brayne C. A systematic review of prevalence studies of dementia in Parkinson’s disease. Mov Disord 2005;20(10):1255-63.
98. Aasly JO, Shi M, Sossi V, Stewart T, Johansen KK, Wszolek ZK, et al. Cerebrospinal fluid amyloid beta and tau in LRRK2 mutation carriers. Neurology 2012;78(1):55-61.
99. Shi M, Furay AR, Sossi V, Aasly JO, Armaly J, Wang Y, et al. DJ-1 and alphaSYN in LRRK2 CSF do not correlate with striatal dopaminergic function. Neurobiol Aging 2012;33(4):836 e5-7.
100. Aasly JO, Johansen KK, Bronstad G, Waro BJ, Majbour NK, Varghese S, et al. Elevated levels of cerebrospinal fluid alpha-synuclein oligomers in healthy asymptomatic LRRK2 mutation carriers. Front Aging Neurosci 2014;6:248.
101. Kasten M, Kertelge L, Bruggemann N, van der Vegt J, Schmidt A, Tadic V, et al. Nonmotor symptoms in genetic Parkinson disease. Arch Neurol 2010;67(6):670-6.
102. Ruiz-Martinez J, Gorostidi A, Goyenechea E, Alzualde A, Poza JJ, Rodriguez F, et al. Olfactory deficits and cardiac 123I-MIBG in Parkinson’s disease related to the LRRK2 R1441G and G2019S mutations. Mov Disord 2011;26(11):2026-31.
103. Khan NL, Katzenschlager R, Watt H, Bhatia KP, Wood NW, Quinn N, et al. Olfaction differentiates parkin disease from early-onset parkinsonism and Parkinson disease. Neurology 2004;62(7):1224-6.
104. Hayashi S, Wakabayashi K, Ishikawa A, Nagai H, Saito M, Maruyama M, et al. An autopsy case of autoso-mal-recessive juvenile parkinsonism with a homozygous exon 4 deletion in the parkin gene. Mov Disord 2000;15(5):884-8.
105. Wooten GF, Currie LJ, Bovbjerg VE, Lee JK, Patrie J. Are men at greater risk for Parkinson’s disease than women? J Neurol Neurosurg Psychiatry 2004;75(4):637-9.
106. Orr-Urtreger A, Shifrin C, Rozovski U, Rosner S, Bercovich D, Gurevich T, et al. The LRRK2 G2019S mutation in Ashkenazi Jews with Parkinson disease: is there a gender effect? Neurology 2007;69(16):1595-602.

127
BIBLIOGRAFÍA 9
107. Silveira-Moriyama L, Guedes LC, Kingsbury A, Ayling H, Shaw K, Barbosa ER, et al. Hyposmia in G2019S LRRK2-related parkinsonism: clinical and pathologic data. Neurology 2008;71(13):1021-6.
108. Iranzo A, Valldeoriola F, Lomena F, Molinuevo JL, Serradell M, Salamero M, et al. Serial dopamine transporter imaging of nigrostriatal function in patients with idiopathic rapid-eye-movement sleep behaviour disorder: a prospective study. Lancet Neurol 2011;10(9):797-805.
109. Postuma RB, Aarsland D, Barone P, Burn DJ, Hawkes CH, Oertel W, et al. Identifying prodromal Parkinson’s disease: pre-motor disorders in Parkinson’s disease. Mov Disord 2012;27(5):617-26.
110. Giasson BI, Duda JE, Quinn SM, Zhang B, Trojanowski JQ, Lee VM. Neuronal alpha-synucleinopathy with severe movement disorder in mice expressing A53T human alpha-synuclein. Neuron 2002;34(4):521-33.
111. Waxman EA, Giasson BI. Induction of intracellular tau aggregation is promoted by alpha-synuclein seeds and provides novel insights into the hyperphosphorylation of tau. J Neurosci 2011;31(21):7604-18.