
CÁNCER DE PRÓSTATA RESISTENTE A LA CASTRACIÓN CON ...HISTORIA NATURAL DEL CÁNCER DE PRÓSTATA...
56
CÁNCER DE PRÓSTATA RESISTENTE A LA CASTRACIÓN CON METÁSTASIS ÓSEAS SINTOMÁTICAS Joan Carles Jefe de Sección. Profesor Asociado Oncología UIC Director del Programa de GU, SNC y Sarcomas Hospital Universitario Vall d’Hebron Barcelona
Transcript of CÁNCER DE PRÓSTATA RESISTENTE A LA CASTRACIÓN CON ...HISTORIA NATURAL DEL CÁNCER DE PRÓSTATA...

CÁNCER DE PRÓSTATA RESISTENTE A LA
CASTRACIÓN CON METÁSTASIS ÓSEAS
SINTOMÁTICAS
Joan Carles
Jefe de Sección. Profesor Asociado Oncología UIC
Director del Programa de GU, SNC y Sarcomas
Hospital Universitario Vall d’Hebron
Barcelona

Resistente a la castración Sensible a la castración
HISTORIA NATURAL DEL CÁNCER DE PRÓSTATA
Sintomático ASINTOMÁTICO
No metástasis
Terapia local
Deprivación de andrógenos
Quimioterapia
Postquimioterapia
Death
Desde el punto de vista del tratamiento hormonal existen dos tipos de pacientes: 1. Cáncer de próstata sensible a terapia hormonal 2. Cáncer de próstata resistente a la castración
Metástasis

Tannock et al, NEJM 2004; 351(15): 1502-12 Petrylak et al, NEJM 2004; 351(15): 1513-20
DOCETAXEL IS STANDARD IN FIRST-LINE CPRC
Docetaxel 3 w
Docetaxel
weekly

Intensidad dolor SM (meses) 1-año, % 2-años, % 3-años,%
Mínimo/ninguno PSA-DT > 45 días PSA-DT < 45 días
21.4 32.4 16.5
75 86 72
43 62 33
29 45 25
Leve 15.0 56 20 11
Moderado/ severo 13.1 52 20 4
Oudard S, et al. BJUI 2009
Supervivencia en el CPRC según la intensidad del dolor

90% of patients with mCRPC
have bone metastases
The pelvis, vertebral column,
ribs, and femur are common
sites of bone metastases
Visceral metastases are much
less common and may occur
in the liver, lungs or brain
~70 %
bone
lymph nodes
~20%
bone
visceral
5–10%
lymph node
only
< 5%
visceral only
de Bono et al. Lancet 2010;376:1147. de Bono et al. New Engl J Med 2011;364:1995. Ryan et al. J Clin Oncol 2012;30(suppl.):abstr LBA4518. de Bono et al. J Clin Oncol 2012;30(suppl.):abstr 4519.
Bone is the Most Common Site of Metastases in Prostate Cancer Patients
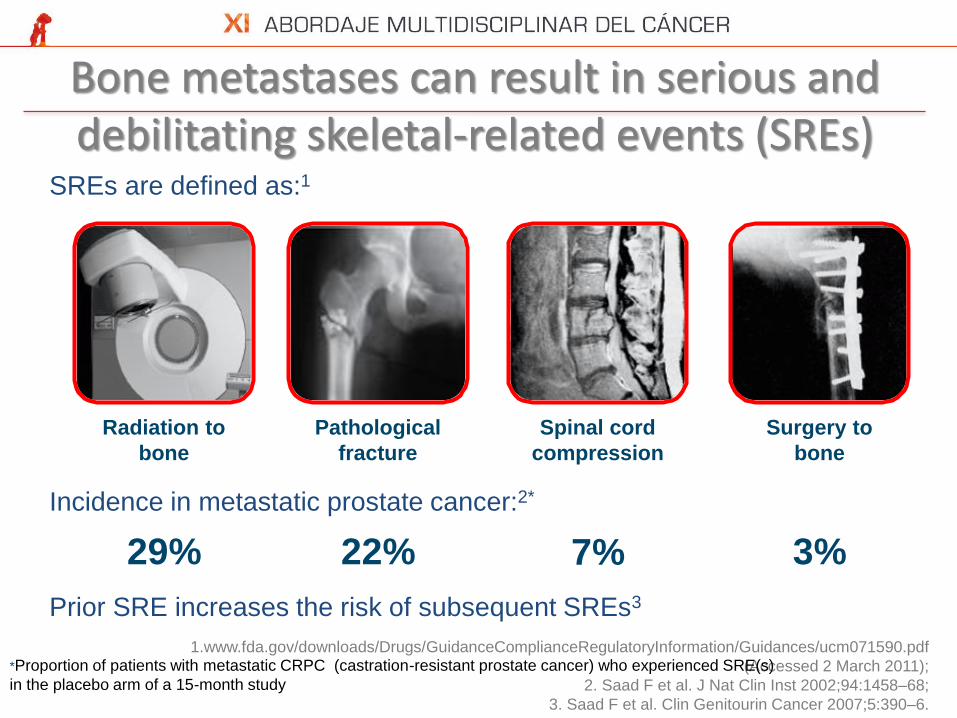
SREs are defined as:1
Incidence in metastatic prostate cancer:2*
Prior SRE increases the risk of subsequent SREs3
1.www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm071590.pdf
(Accessed 2 March 2011);
2. Saad F et al. J Nat Clin Inst 2002;94:1458–68;
3. Saad F et al. Clin Genitourin Cancer 2007;5:390–6.
Pathological
fracture
Radiation to
bone
Surgery to
bone
Spinal cord
compression
29% 3% 7% 22%
*Proportion of patients with metastatic CRPC (castration-resistant prostate cancer) who experienced SRE(s)
in the placebo arm of a 15-month study
Bone metastases can result in serious and debilitating skeletal-related events (SREs)
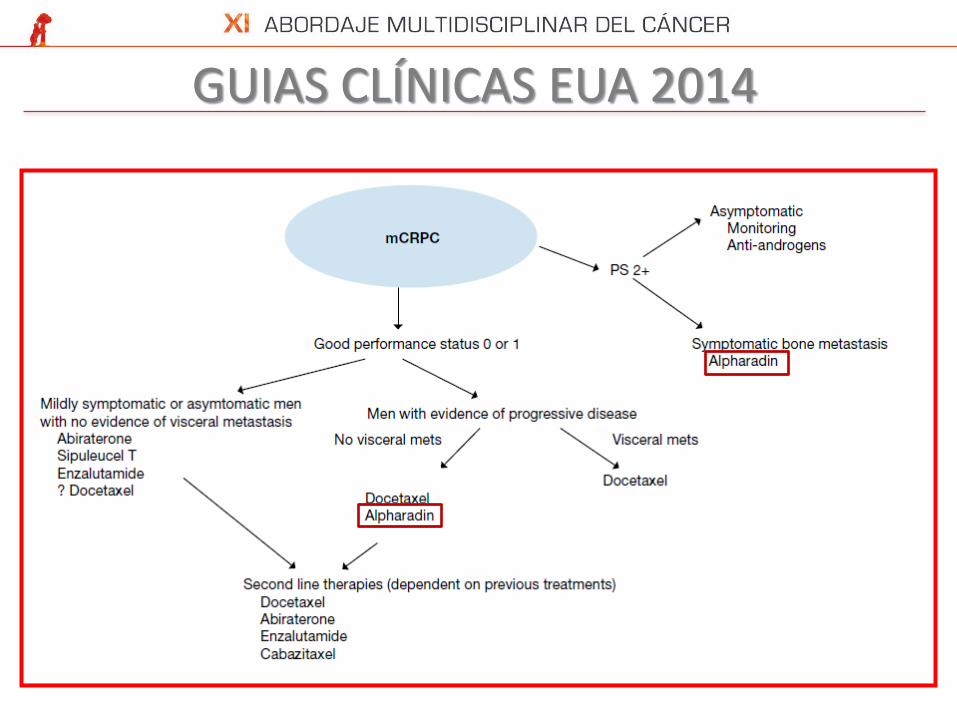
GUIAS CLÍNICAS EUA 2014

PREGUNTA 1

Radium-223 Targets Bone Metastases A natural bone-seeker1 because
it is a ‘calcium mimetic’2
Naturally targets new bone growth in and around bone metastases
Half-life: 11.4 days3
Shelf life: 28 days3
No long-lived radioactive waste products after decay2
Radium-223 is excreted by the small intestine
Ca
Sr
Ba
Ra
1. Henriksen et al. Can Res 2002;62:3120. 2. Nilsson et al. Presented at: American Society
for Radiation Oncology annual meeting 2010: Poster 2385, 3,- Xofigo® (radium Ra 223
dichloride) solution for injection Summary of Product Characteristics (SmPC). Berlin,
Germany: Bayer Pharma AG, 4,- . Nilsson S, et al. Int J Radiat Oncol Biol Phys. 2010;
78(3 suppl):S375-S376.

Características Físicas α β
Radionúclidos Radio-223 Estroncio-89, Samario-153
Tamaño
Masa de la partícula 7000 1
Energía inicial(MeV) 5–9 0.05–2.3
Penetración en tejidos (μm) 40–100 50–12,000
LET (KeV/μm) 60–300 0.1–1.0
Carga +2 –1
Pares de iones/μm 2000–7000 5–20
Lesiones en DNA para muerte celular 1–4 > 1000
Semin Nucl Med 2008;38:358
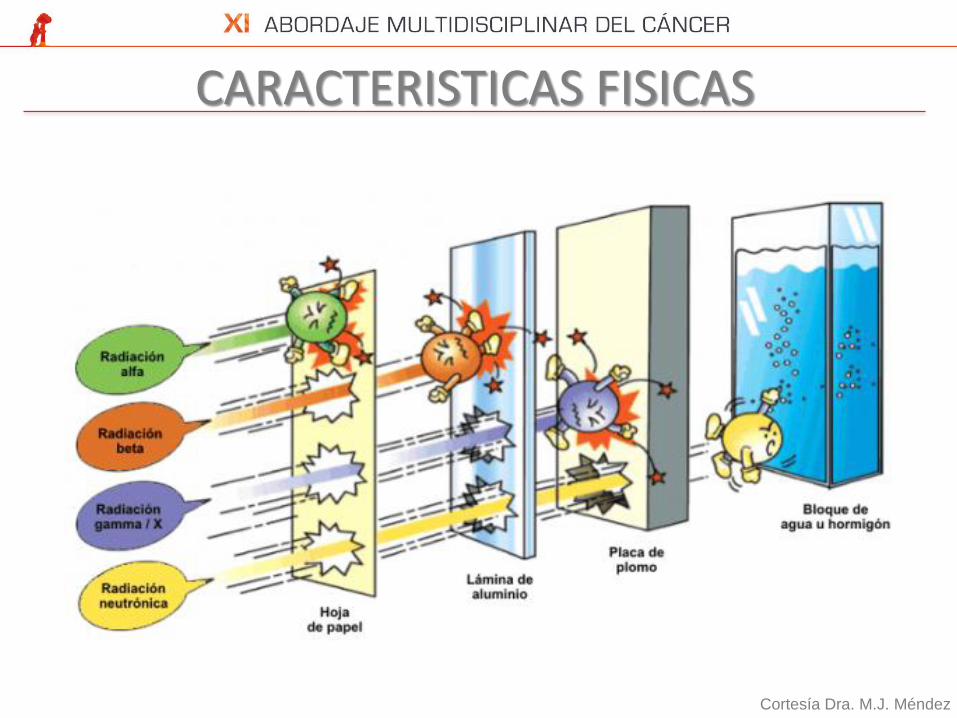
CARACTERISTICAS FISICAS
Cortesía Dra. M.J. Méndez

Beta particle emission
Alpha particle emission
Non-reparable double-strand DNA breaks
Single-strand DNA breaks are
not lethal
Potent Anti-tumour Effects of Radium-223
Radium-223 selectively targets bone, specifically bone metastases
It emits high-energy ionizing alpha particles which cause lethal,
double-strand DNA breaks in adjacent cells
This results in a highly localized anti-tumor effect in bone metastases
Parker C, et al. N Engl J Med. 2013;369(3):213-23.

Short range of alpha emitter
reduces bone marrow exposure
Alpha Emitter Versus Beta Emitters
1
3
Long range of beta emitters
may increase bone marrow exposure
and associated toxicities
Alpha Emitter
(OS benefit + pain palliation)
Beta Emitters
(Pain palliation only)
Marrow
Bone
Radium-223
Marrow
Bone
Strontium-89
and
Samarium-153
1. Henriksen G, et al. Cancer Res. 2002;62:3120-3125. 2. Brechbiel MW. Dalton Trans. 2007;43:4918-4928.
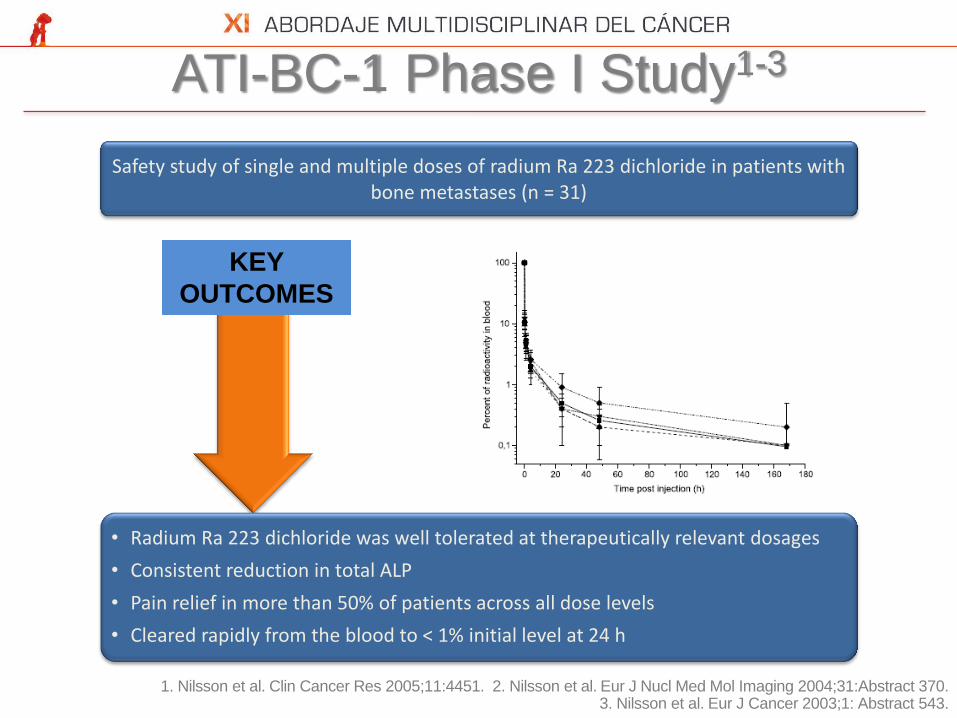
ATI-BC-1 Phase I Study1-3
ALP, alkaline phosphatase 1. Nilsson et al. Clin Cancer Res 2005;11:4451. 2. Nilsson et al. Eur J Nucl Med Mol Imaging 2004;31:Abstract 370.
3. Nilsson et al. Eur J Cancer 2003;1: Abstract 543.
Safety study of single and multiple doses of radium Ra 223 dichloride in patients with bone metastases (n = 31)
• Radium Ra 223 dichloride was well tolerated at therapeutically relevant dosages
• Consistent reduction in total ALP
• Pain relief in more than 50% of patients across all dose levels
• Cleared rapidly from the blood to < 1% initial level at 24 h
KEY
OUTCOMES

BC1-05 Phase I Study1
1. Lewington et al. Presented at ASCO Genitourinary Cancers Symposium 2010: Poster 216.
Study assessing the biodistribution, dosimetry and pharmacokinetics of radium Ra 223 dichloride (2 x 100 kBq/kg) in CRPC and bone metastases (n = 6)
• Rapidly taken up by bone/bone metastases
• Excreted through the GI tract and small intestine
• Spares kidney – radiation dose low
• Radium Ra 223 dichloride was well tolerated and favorable alterations in bone turnover markers
KEY
OUTCOMES
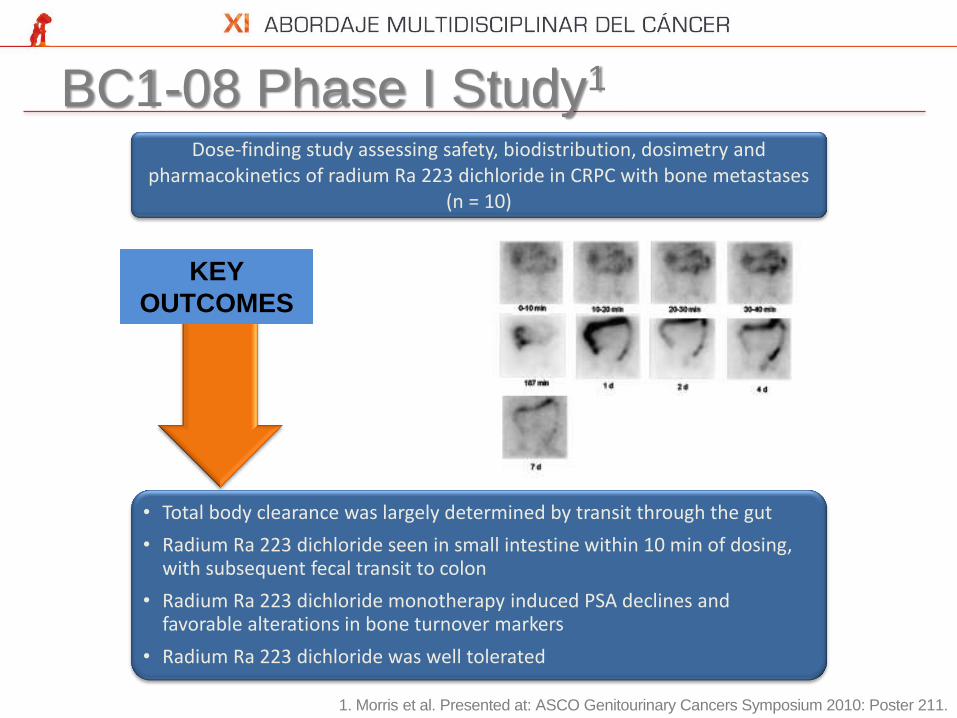
BC1-08 Phase I Study1
1. Morris et al. Presented at: ASCO Genitourinary Cancers Symposium 2010: Poster 211.
Dose-finding study assessing safety, biodistribution, dosimetry and pharmacokinetics of radium Ra 223 dichloride in CRPC with bone metastases
(n = 10)
• Total body clearance was largely determined by transit through the gut
• Radium Ra 223 dichloride seen in small intestine within 10 min of dosing, with subsequent fecal transit to colon
• Radium Ra 223 dichloride monotherapy induced PSA declines and favorable alterations in bone turnover markers
• Radium Ra 223 dichloride was well tolerated
KEY
OUTCOMES
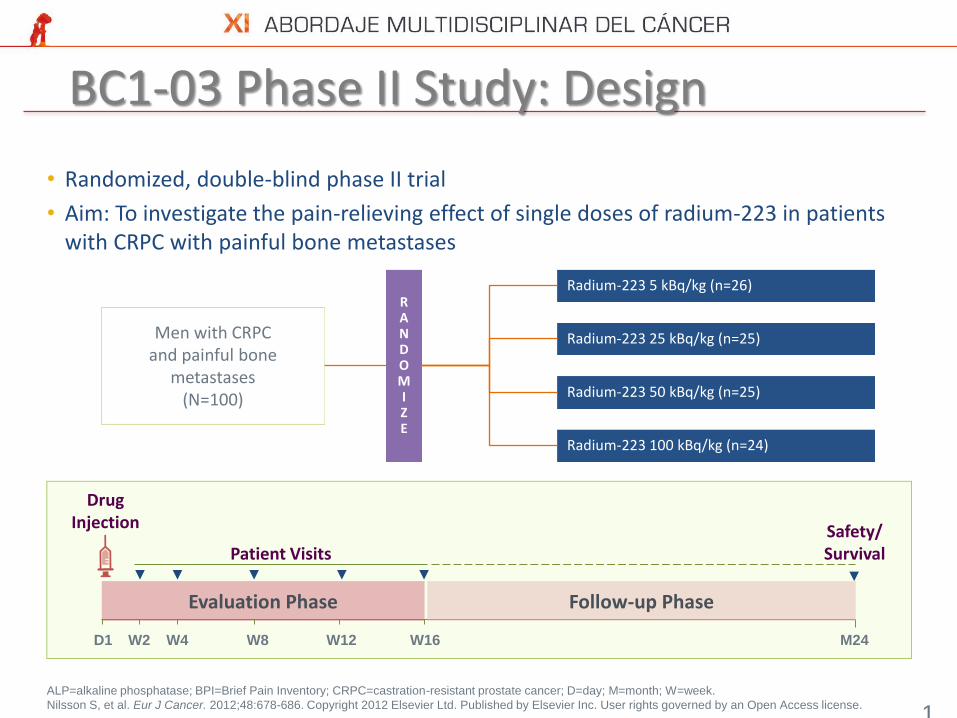
BC1-03 Phase II Study: Design
1
7
ALP=alkaline phosphatase; BPI=Brief Pain Inventory; CRPC=castration-resistant prostate cancer; D=day; M=month; W=week.
Nilsson S, et al. Eur J Cancer. 2012;48:678-686. Copyright 2012 Elsevier Ltd. Published by Elsevier Inc. User rights governed by an Open Access license.
• Randomized, double-blind phase II trial
• Aim: To investigate the pain-relieving effect of single doses of radium-223 in patients with CRPC with painful bone metastases
Evaluation Phase
M24 D1
Follow-up Phase
Drug Injection
Patient Visits
W2 W4 W8 W12 W16
Safety/ Survival
Men with CRPC and painful bone
metastases (N=100)
Radium-223 5 kBq/kg (n=26)
Radium-223 50 kBq/kg (n=25)
R A N D O M I Z E
Radium-223 25 kBq/kg (n=25)
Radium-223 100 kBq/kg (n=24)

CRPC with painful bone metastases (n = 100)
Single doses: 5, 25, 50 or 100 kBq/kg
• A significant dose-dependent pain response was observed with Radium Ra 223 dichloride
• Radium Ra 223 dichloride was well tolerated
• Hematologic toxicity was generally mild
BC1-03 Phase II Study1
1. Nilsson et al. Eur J Cancer 2012;48(5):678
KEY
OUTCOMES
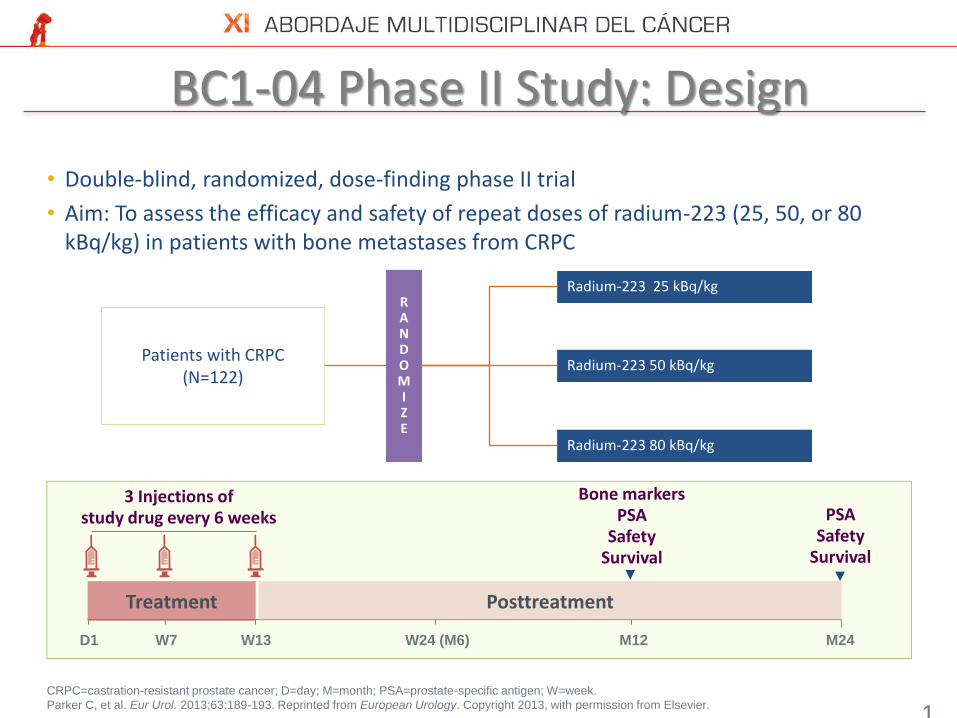
BC1-04 Phase II Study: Design
1
9
CRPC=castration-resistant prostate cancer; D=day; M=month; PSA=prostate-specific antigen; W=week.
Parker C, et al. Eur Urol. 2013;63:189-193. Reprinted from European Urology. Copyright 2013, with permission from Elsevier.
• Double-blind, randomized, dose-finding phase II trial
• Aim: To assess the efficacy and safety of repeat doses of radium-223 (25, 50, or 80 kBq/kg) in patients with bone metastases from CRPC
Patients with CRPC (N=122)
Radium-223 25 kBq/kg
Radium-223 50 kBq/kg
R A N D O M I Z E
Radium-223 80 kBq/kg
Treatment
M24 D1
Posttreatment
3 Injections of study drug every 6 weeks
W7 W13 W24 (M6)
PSA Safety
Survival
M12
Bone markers PSA
Safety Survival

CRPC with bone metastases (n = 122)
Multiple doses: 3 × 25, 50 or 80 kBq/kg at 6-week intervals
• Bone-ALP response in > 60% of patients receiving 50 or 80 kBq/kg
• Radium Ra 223 dichloride was well tolerated
• No evidence of a dose-limiting effect
• No grade 3/4 neutropenia was observed
BC1-04 Phase II Study1
KEY
OUTCOMES
ALP, alkaline phosphatase 1. Parker et al. Eur J Can Suppl 2009;7:406:Abstract 7003.

BC1-02 Phase IIb Study1,2:Radium Ra 223
• Compared with placebo, Radium Ra 223 dichloride significantly reduced PSA, ALP, other bone markers
• Well tolerated with little hematologic toxicity • Median survival was 40% longer in the radium Ra 223 dichloride group vs. the
placebo group2
CRPC with bone metastases requiring EBRT (n = 64) Multiple doses: 4 × 50 kBq/kg or placebo at 4-week intervals
Radium Ra 223 dichloride
Placebo
Median OS, months
15.0 (65 weeks)
10.7 (46 weeks)
Hazard ratio 0.48
95% CI 0.581–0.832
P 0.017
1.00
0.75
0.50
0.25
0.00 0 20 40 60 80 100 120
Time (weeks)
Radium Ra 223 dichloride
Placebo
Pro
po
rtio
n s
urv
ivin
g
ALP, alkaline phosphatase; EBRT, external beam radiation therapy; PSA, prostate-specific antigen
1. Nilsson et al. Lancet Oncol 2007;8:587. 2. Nilsson et al. Eur J Cancer Suppl 2009;7:412 P-7018.
KEY
OUTCOMES

Introduction to ALSYMPCA
Based on the positive results from the randomized Phase II trial, the
decision was taken to proceed with a Phase III trial
ALSYMPCA (ALpharadin* in SYMptomatic Prostate CAncer)
ALSYMPCA was an international multicenter, double-blind,
randomized, placebo-controlled Phase III trial conducted in >
900 patients with symptomatic CRPC and bone metastases
The primary endpoint was overall survival
*Radium Ra 223 dichloride was formerly known as ‘Alpharadin’.

PREGUNTA 2

Phase III ALSYMPCA Trial Design
Primary endpoints: overall survival Secondary endpoints: time to first SRE, time to total ALP progression, total ALP response, total ALP normalization, time to PSA progression, safety and HRQoL
*Plus best standard of care.
Parker et al. J Clin Oncol 2012;30(suppl.):abstr LBA4512. Presented at ASCO 2012. www.clinicaltrials.gov. NCT00699751.
R 2:1
Radium Ra 223 Dichloride* 50 kBq/kg
Saline* (placebo)
FOLLOW-UP PHASE TREATMENT PHASE 6 injections at 4-week intervals
M36 M16 M24 M12 M0 M28 M6 M20 M32 M8 M10
Month
Stratification factors •Total ALP < 220 U/L vs. ≥ 220 U/L •Bisphosphonate use (Yes vs. No) •Prior docetaxel (Yes vs. No) Key inclusion criteria •Confirmed symptomatic CRPC •≥ 2 bone metastases •No known visceral metastases •Post-docetaxel or unfit for docetaxel
Assessments
n = 921 Metastatic
CRPC

ALSYMPCA Analyses
Planned interim analysis (IA)
314 events from 809 patients randomized at the time of the IA: cut-off October 2010
3 June 2011: the Independent Data Monitoring Committee (IDMC) recommended stopping the trial early, because of evidence of a significant treatment benefit
Updated analysis
528 events from all 921 patients randomized to the study
Updated analysis conducted prior to placebo patients crossing over to radium Ra 223 dichloride and when all patients had completed study drug treatment: cut-off July 2011.
Data first announced in Feb 2012
Q1
2012
Q4
2011
Q3
2011
Q2
2011
Q1
2011
Q4
2010
Q3
2010
Q2
2010
Q1
2010
Q4
2009
Q3
2009
Q2
2009
Q1
2009
Q4
2008
Q3
2008
Q2
2008
DATA CUTOFF LPFV IDMC FPFV
UPDATED ANALYSI
S
CROSSOV
ER

ALSYMPCA: Patient Demographics and Baseline Characteristics
Parameter Radium Ra 223
dichloride (n = 614) Placebo (n = 307)
Age, years Mean
70.2
70.8
Ethnicity, n (%) Caucasian
575 (94)
290 (95)
Baseline ECOG score, n (%) ≤ 1 2
536 (87) 76 (12)
265 (86) 40 (13)
Extent of disease, n (%) < 6 metastases 6–20 metastases > 20 metastases/superscan
100 (16) 262 (43) 249 (41)
38 (12)
147 (48) 121 (40)
WHO ladder, cancer pain index ≥ 2, n (%)
345 (56)
168 (55)
ITT analysis; n = 921 Parker et al. NEJM 2013;369:213-23

ALSYMPCA: Patient Baseline Characteristics
Parameter Median (min, max)
Radium Ra 223 dichloride (n = 614)
Placebo (n = 307)
Hemoglobin, g/dL 12.2 (8.5–15.7) 12.1 (8.5–16.4)
Albumin, g/L 40 (24–53) 40 (23–50)
Total ALP, µg/L 211 (32–6431) 223 (29–4805)
LDH, U/L 315 (76–2171) 336 (132–3856)
PSA, µg/L 146 (3.8–6026) 173 (1.5–14500)
Current bisphosphonates Yes, n (%)
250 (40.7)
124 (40.4)
Prior docetaxel Yes, n (%)
352 (57.3)
174 (56.7)
ITT analysis; n = 921 Parker et al. NEJM 2013;369:213-23

ALSYMPCA: Radium Ra 223 Dichloride Significantly Improved Overall Survival
Radium Ra 223 dichloride
Placebo
Median OS (months) 14.9 11.3
Hazard ratio 0.695
95% CI 0.581–0.832
P < 0.0001
Radium Ra 223 dichloride
Placebo
Month
Ra 223 614 578 504 369 274 178 105 60 41 18 7 1 0 0
Placebo 307 288 228 157 103 67 39 24 14 7 4 2 1 0 Parker et al. NEJM 2013;369:213-23
Median OS Δ: 3.6 months
Overall survival: time from date of randomization to the date of death

ALSYMPCA: Survival Benefit Across Patient Subgroups
Parker et al. NEJM 2013;369:213-23
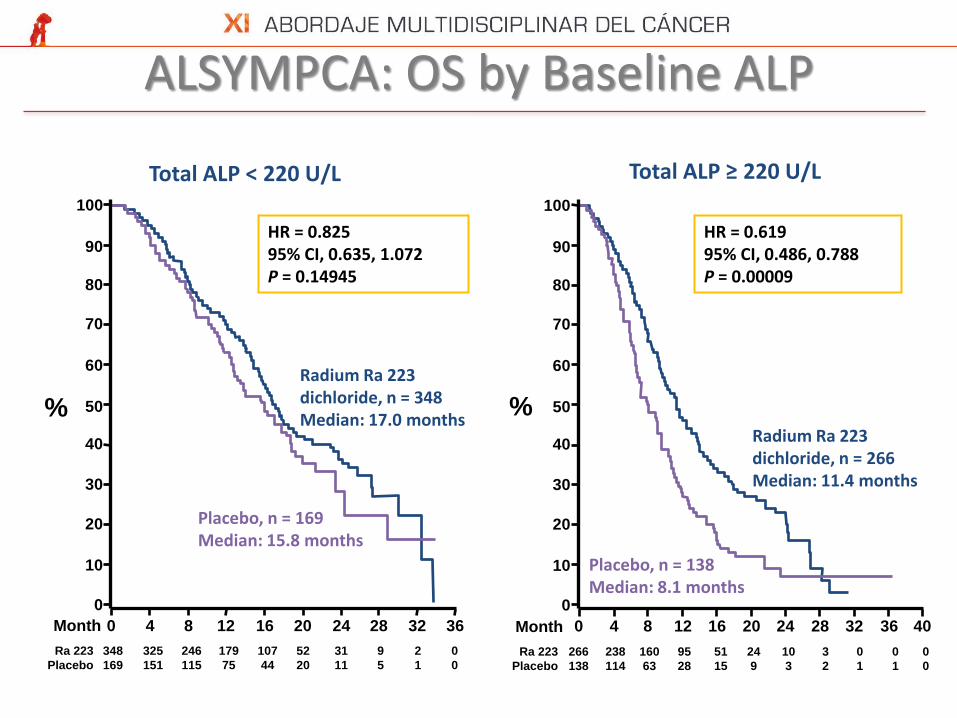
ALSYMPCA: OS by Baseline ALP
Total ALP < 220 U/L Total ALP ≥ 220 U/L
Radium Ra 223 dichloride, n = 348 Median: 17.0 months
Placebo, n = 169 Median: 15.8 months
HR = 0.825 95% CI, 0.635, 1.072 P = 0.14945
Radium Ra 223 dichloride, n = 266 Median: 11.4 months
Placebo, n = 138 Median: 8.1 months
HR = 0.619 95% CI, 0.486, 0.788 P = 0.00009
Ra 223 266 238 160 95 51 24 10 3 0 0 0
Placebo 138 114 63 28 15 9 3 2 1 1 0
100
90
80
70
60
50
40
30
20
10
0
0 4 8 12 16 20 24 28 32 36 40
Ra 223 348 325 246 179 107 52 31 9 2 0
Placebo 169 151 115 75 44 20 11 5 1 0
100
90
80
70
60
50
40
30
20
10
0
0 4 8 12 16 20 24 28 32 36
% %
Month Month

Current bisphosphonate use NO current bisphosphonate use
Radium Ra 223 dichloride, n = 250 Median: 15.3 months
Placebo, n = 124 Median: 11.5 months
HR = 0.699 95% CI, 0.525, 0.931 P = 0.01378
Radium Ra 223 dichloride, n = 364 Median: 14.5 months
Placebo, n = 183 Median: 11.0 months
HR = 0.736 95% CI, 0.587, 0.923 P = 0.00775
ALSYMPCA: OS by Bisphosphonate Use
Ra 223 364 331 235 159 97 50 27 6 0 0 0
Placebo 183 155 102 58 33 16 10 6 2 1 0
100
90
80
70
60
50
40
30
20
10
0
0 4 8 12 16 20 24 28 32 36 40
Ra 223 250 232 171 115 61 26 14 6 2 0
Placebo 124 110 76 45 26 13 4 1 0 0
100
90
80
70
60
50
40
30
20
10
0
0 4 8 12 16 20 24 28 32 36
% %
Month Month
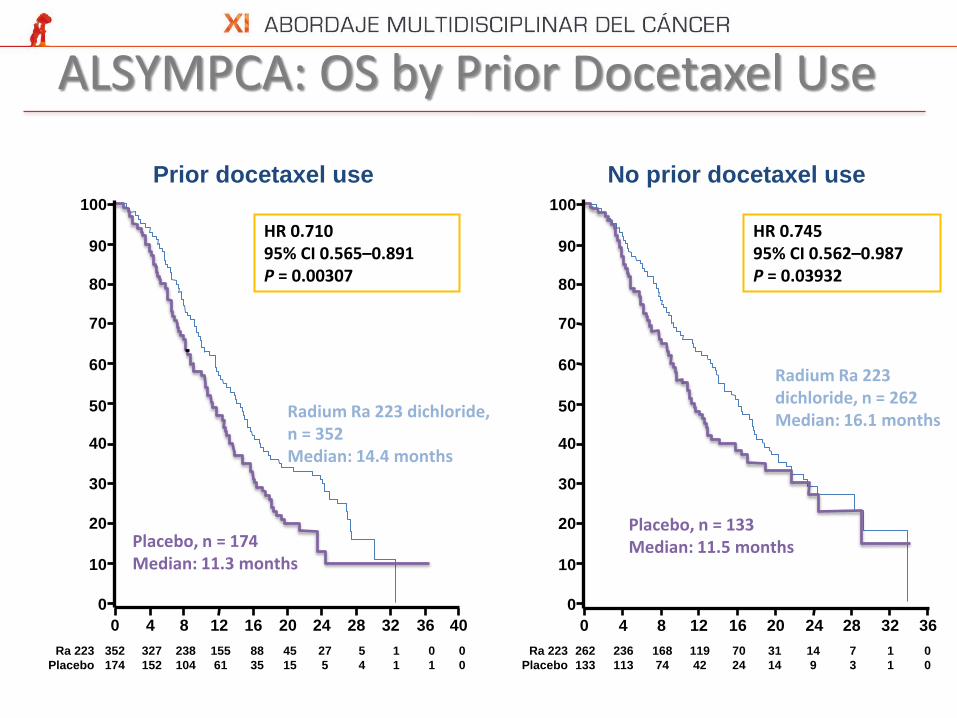
ALSYMPCA: OS by Prior Docetaxel Use
Prior docetaxel use No prior docetaxel use
Ra 223 352 327 238 155 88 45 27 5 1 0 0
Placebo 174 152 104 61 35 15 5 4 1 1 0
Radium Ra 223 dichloride, n = 352 Median: 14.4 months
Placebo, n = 174 Median: 11.3 months
HR 0.710 95% CI 0.565–0.891 P = 0.00307
Radium Ra 223 dichloride, n = 262 Median: 16.1 months
Placebo, n = 133 Median: 11.5 months
HR 0.745 95% CI 0.562–0.987 P = 0.03932
100
90
80
70
60
50
40
30
20
10
0
0 4 8 12 16 20 24 28 32 36 40 Month
%
Ra 223 262 236 168 119 70 31 14 7 1 0
Placebo 133 113 74 42 24 14 9 3 1 0
100
90
80
70
60
50
40
30
20
10
0
0 4 8 12 16 20 24 28 32 36

Month 0 3 6 9 12 15 18 21 24 27 30
Ra 223 614 496 342 199 129 63 31 8 8 1 0
Placebo 307 211 117 56 36 20 9 7 4 1 0
ALSYMPCA Pre-crossover Analysis Time To First SRE
0
10
20
30
40
50
60
70
80
90
100
%
Radium Ra 223 dichloride
Placebo
Median OS (months) 15.6 9.8
Hazard ratio 0.658
95% CI 0.52–0.83
P 0.00037
Radium Ra 223 dichloride
Placebo
Parker et al. NEJM 2013;369:213-23

Radium Ra 223 dichloride, n (%)
Placebo n (%)
P
Total ALP response 30% reduction 50% reduction
233 (47) 135 (27)
7 (3)
2 (< 1)
< 0.001 < 0.001
Total ALP normalization* 109 (34) 2 (1) < 0.001
Confirmed PSA response** 28 (6) 4 (2) 0.032
*In patients who had elevated total ALP at baseline. **≥ 50% reduction from baseline confirmed by a second value ≥ 4 weeks later, by end of treatment. This was not an endpoint in
ALSYMPCA.
Hazard ratio (95% CI) P
Time to total ALP progression 0.167
(0.129–0.217) < 0.00001
Time to PSA progression 0.643
(0.539–0.768) < 0.00001
Parker et al. NEJM 2013;369:213-23
ALSYMPCA: Secondary Endpoints: ALP and PSA

Phase III ALSYMPCA: FACT-P QoL Responder Analysis
P = 0.012 P = 0.111 P = 0.538 P = 0.004 P = 0.077
*For each subscale, MID = 3. Assessment at week 16 and/or week 24.
Parker et al. Presented at ESMO 2012 Poster 898PD

ALSYMPCA: Grade 3/4 AEs Were Lower With Radium Ra 223 Dichloride Than Placebo
*Safety population comprised patients who received at least 1 dose; 1
patient in the placebo group received one injection of radium Ra 223
dichloride (Week 0) and is included in the radium Ra 223 dichloride safety
analysis.
Parker et al. J Clin Oncol 30, 2012 (suppl; abstr
LBA4512). Data on file, Bayer HealthCare
Pharmaceuticals

ALSYMPCA: Adverse Events
Patients with adverse events (AEs), n (%)
Parker et al. NEJM 2013;369:213-23 .

Conclusions from ALSYMPCA
In CRPC patients with bone metastases
Radium Ra 223 dichloride significantly prolonged overall survival
14.9 months vs. 11.3 months placebo
(P = 0.00007; HR 0.695, 95% CI 0.581–0.832)
Radium Ra 223 dichloride significantly prolonged time to first SRE
12.2 months vs. 6.7 months placebo
(P < 0.0001; HR = 0.64 [95% CI: 0.52–0.78])
Radium Ra 223 dichloride was very well tolerated
Radium Ra 223 dichloride may provide a new standard
of care for the treatment of CRPC patients with bone
metastases

PREGUNTA 3

936P | Safety of Cytotoxic Chemotherapy Following Radium-223
Key Results:
• The proportion of patients treated with CT after completing study drug was 15% in the
radium-223 group and 18% in the placebo group
• In patients receiving CT after study drug, death and its causality were similar between the
treatment groups
Table 6: Number of Deaths and Causality [from Poster]
Parameter Radium-223 (n=93) Placebo (n=54)
During Chemotherapy Administration
Deaths on chemotherapy, % 14 15
Causality: PC and skeletal mets (± other mets) PC with other mets (or mets not specified) Cerebral hemorrhage due to trauma Cardiopulmonary failure
10 3 1 0
13 0 0 2
30 Days After Chemotherapy Administration
Deaths within 30 days after chemotherapy, n % 6 4
Causality: PC and skeletal mets (± other mets) Bronchopneumonia Respiratory failure + pulmonary edema
4 1 0
4 1 0
Mets, metastases; PC, prostate cancer.
Sartor O, et al. Presented at: ESMO, Sept. 28–Oct 2, 2012, Vienna, Austria; Poster 936P.

[TITLE]
Presented By Sten Nilsson, MD, PhD at 2014 Genitourinary Cancers Symposium
Presented By Sten Nilsson, MD, PhD at 2014 Genitourinary Cancers Symposium

Presented By Sten Nilsson, MD, PhD at 2014 Genitourinary Cancers Symposium

[TITLE]
Presented By Sten Nilsson, MD, PhD at 2014 Genitourinary Cancers Symposium

[TITLE]
Presented By Sten Nilsson, MD, PhD at 2014 Genitourinary Cancers Symposium

[TITLE]
Presented By Sten Nilsson, MD, PhD at 2014 Genitourinary Cancers Symposium

[TITLE]
Presented By Sten Nilsson, MD, PhD at 2014 Genitourinary Cancers Symposium

[TITLE]
Presented By Sten Nilsson, MD, PhD at 2014 Genitourinary Cancers Symposium

Estudios Actualmente en Marcha
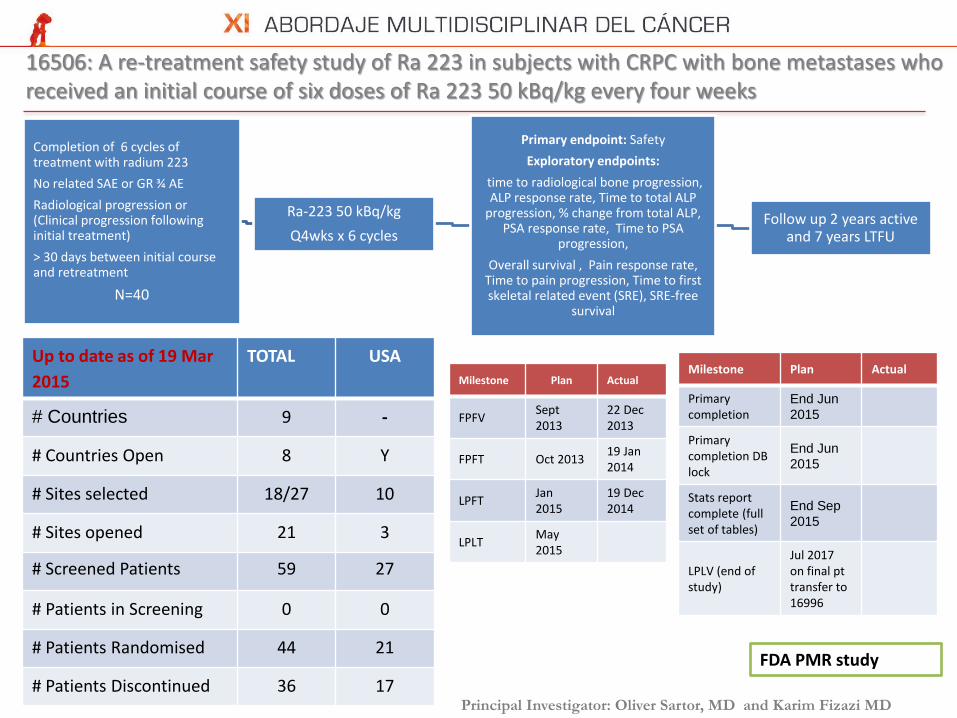
16506: A re-treatment safety study of Ra 223 in subjects with CRPC with bone metastases who received an initial course of six doses of Ra 223 50 kBq/kg every four weeks
Completion of 6 cycles of treatment with radium 223
No related SAE or GR ¾ AE
Radiological progression or (Clinical progression following initial treatment)
> 30 days between initial course and retreatment
N=40
Ra-223 50 kBq/kg
Q4wks x 6 cycles
Primary endpoint: Safety
Exploratory endpoints:
time to radiological bone progression, ALP response rate, Time to total ALP
progression, % change from total ALP, PSA response rate, Time to PSA
progression,
Overall survival , Pain response rate, Time to pain progression, Time to first skeletal related event (SRE), SRE-free
survival
Follow up 2 years active and 7 years LTFU
Milestone Plan Actual
FPFV Sept 2013
22 Dec 2013
FPFT Oct 2013 19 Jan 2014
LPFT Jan 2015
19 Dec 2014
LPLT May 2015
Principal Investigator: Oliver Sartor, MD and Karim Fizazi MD
FDA PMR study
Milestone Plan Actual
Primary completion
End Jun
2015
Primary completion DB lock
End Jun
2015
Stats report complete (full set of tables)
End Sep
2015
LPLV (end of study)
Jul 2017 on final pt transfer to 16996
Up to date as of 19 Mar
2015
TOTAL USA
# Countries 9 -
# Countries Open 8 Y
# Sites selected 18/27 10
# Sites opened 21 3
# Screened Patients 59 27
# Patients in Screening 0 0
# Patients Randomised 44 21
# Patients Discontinued 36 17

16507: A three arm randomized open-label Phase II study of Ra 223 50 kBq/kg vs 80 kBq/kg, and vs 50kBq/kg in an extended dosing schedule in subjects with castration-resistant prostate cancer metastatic to
the bone
ALSYMPCA population
N=360
Ran
do
miz
ed, 1
:1:1
Radium 223 50 KBq/Kg
q4wks X 6 inj
Radium 223 80 KBq/Kg
q4wks X 6 inj
Primary endpoint: SRE FS
Secondary endpoints:
Safety,
OS,
pain response,
time to pain progressions
Time to first SRE
rPFS
Follow up 2 years active and 7 years LTFU
Radium 223 50 KBq/Kg
q4wks X 12 inj
Mile-stone
Plan Actual
FPFV Mar 14 10 Mar 14
FPFT Apr 14 10 Apr 14
LPFT Sep 15
LPLT Sep 16
Principal Investigator: M. Hussain, MD and C. Sternberg, MD
FDA PMC study
Milestone Plan Actual
Primary completion
Jul 2017
Primary completion DB lock
Aug 2017
Stats report complete (full set of tables)
Oct 2017
LPLV (end of study)
Feb 2018 (when last pt transfers to 16996 study
Up to date as of 19 Mar
2015
TOTAL USA
# Countries 17 -
# Countries Open 13 Y
# Sites selected 95 13
# Sites opened 55 13
# Screened Patients 303 64
# Patients in Screening 19 5
# Patients Randomised 209 40
# Patients Discontinued 70 4

16544: A randomized phase IIa study of quantified bone scan response following treatment with Ra 223 alone or in combination with abiraterone acetate or enzalutamide in subjects with CRPC who have bone
metastases
ALSYMPCA population
N=66
Ran
do
miz
ed, 1
:1:1
Ra-223 50 kBq/kgQ4wks x 6 cycles
Ra-223 50 kBq/kgQ4wks x 6 cycles plus abiraterone
1’endpoint
BSLA response Week 24
2’endpoints
Safety of each combination, describe rPFS, SSE-FS, OS
Follow up - 2 years active and 7 years LTFU
Ra-223 50 kBq/kgQ4wks x 6 cycles plus enzalutamide
Milestone Plan Actual
FPFV 17-Mar-14 7-Mar-14
FPFT 21-Mar-14 28-Mar-14
LPFT 12-Dec-15
LPLV 25-Jun-18
Principal Investigator: D. Petrylak, MD
Milestone Plan Actual
Primary completion 20-Jul -16
Primary completion DB lock
8-Sep-16
Stats report complete (full set of tables)
29-Oct-16
LPLV (end of study) 25-Jun-18
Up to date as of 20 Mar 15 TOTAL
# Countries 1
# Countries Open 1
# Sites selected 22 of 22
# Sites opened 13
# Patients Screened 33
# Patients in Screening 2
# Patients Randomised 19 (17
treated)
# Patients Discontinued 9

15396: Phase III study in combination with abiraterone in asymptomatic/mildly symptomatic CRPC
Chemo –naïve metastatic CRPC patients; Progressive disease after previous anti-
androgen therapy and withdrawal ; No known brain
metastasis or visceral metastasis; Asymptomatic or
mildly symptomatic
N=800
Ran
do
miz
ed, 1
:1
Radium 223 dichloride
50 KBq/Kg/4wks X 6 IV
+ Abiraterone + Prednisone/Prednisolone
Matching Placebo
+ Abiraterone + Prednisone/Prednisolone
Milestone Plan Actual
Primary completion
July 2017
Primary completion DB lock
Aug 2017
Stats report complete (full set of tables)
Sep 2017
LPLV (end of study)
Jul 2020 or when last pt transferred to LTFUP study
1’ endpoint: SSE-FS
2’ endpoints:
OS
Time to opiate use
Time to pain
Time to chemotherapy
rPFS
Follow up – 7 years LTFU
Principal Investigator: Dr Celestia Higano & Dr Matthew Smith
Milestone Plan Actual
FPFV Mar-14 30-Mar -14
FPFT Apr-14 24-Apr-14
LPFT Dec-15
LPLT Jun-16
Up to date as of 23 Mar 15 TOTAL USA
# Countries 19 -
# Countries Open 15 -
# Sites selected 162 29
# Sites opened 101 19
# Screened Patients 173 27
# Patients in Screening 12 7
# Patients Randomised 94 11
# Treated patients 85 11

16298: Phase II of Ra 223 dichloride vs placebo in metastatic HER2 negative hormone receptor positive metastatic breast cancer patients with bone metastases treated with hormonal
treatment
Patient population
N=227
Ran
do
miz
ed, 1
:1
BAY 88-8223 50 KBq/Kg/4wks X 6 IV
+ HT (except exemestane), BP/denosumab
Matching Placebo
+ HT (except exemestane), BP/denosumab
Primary endpoint:
SSE-FS
Secondary endpoint:
Safety, rPFS, OS, bone markers endpoints,
bone pain
Follow up
TBD
Principal Investigator: Robert Coleman, MD
Up to date as of 20 Mar 15 Total USA
# Countries 23 (EU & AP) 1
# Countries Open 1 1
# Sites selected 154 22
# Sites opened 3 5
# Sites CMC ready 63 12
# Treated patients 0 0
Milestone Plan Actual
FPFV 28FEB2015 17FEB2015
FPFT 20MAR2015
LPFT 30JUN16
LPLT 29NOV16
Milestone Plan Actual
Primary completion
17MAY17
Primary completion DB lock
17MAY17
Stats report complete (full set of tables)
05SEP17
LPLV (end of study)
17MAY17

17096: Phase II trial of Ra 223 vs placebo in metastatic HER2 negative hormone receptor positive breast cancer with bone metastases treated with exemestane and everolimus
Patient population
N=310
Ran
do
miz
ed, 1
:1
BAY 88-8223 50 KBq/Kg/4wks X 6 IV
+ Exemestane + everolimus, BP/denosumab
Matching Placebo
+ Exemestane + everolimus, BP/denosumab
Primary endpoint:
SSE-FS
Secondary endpoint:
Safety, rPFS, OS, bone markers endpoints,
bone pain
Follow up
TBD
Principal Investigator: Hope Rugo, MD
Up to date as of 20 Mar 2015 TOTAL USA
# Countries 2 -
# Countries Open 1 -
# Sites selected 146 25
# Sites opened 3 5
# Sites CMC ready 63 12
# Treated patients 0 0
Mile-stone
Plan Actual
FPFV May 2015
FPFT June 2015
LPFT Jan 2017
LPLT June 2017
Milestone Plan Actual
Primary completion
Primary completion DB lock
Sep 2017
Stats report complete (full set of tables)
Nov 2017
LPLV (end of study)
Jul 2017
Sites are open for 17096 but must wait for
Amendment 1 approval prior to enrolment

CONCLUSIONES
Se trata de un fármaco con actividad antitumoral
que es capaz de incrementar la supervivencia
global en enfermos afectados de un CPRC
Debido a su actividad y escaso perfil de toxicidad es
un fármaco a tener en cuenta tanto en pre como
en post-docetaxel.
Fármaco seguro con datos de seguimiento a largo
plazo.












