efectosde_la_movilizacion_en_pcte_postrado.

of 17
-
Upload
superkarencita -
Category
Documents
-
view
220 -
download
0
Transcript of efectosde_la_movilizacion_en_pcte_postrado.
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
1/17
Introduction 143
Conceptual framework for clinical decisionmaking 144
The oxygen transport pathway 144Factors contributing to cardiopulmonary
dysfunction 146
Therapeutic effects of positioning andmobilization 147
To improve oxygen transport in acutecardiopulmonary dysfunction 147
To improve oxygen transport in postacute andchronic cardiopulmonary dysfunction 154
To prevent the negative effects of restrictedmobility 156
Summary and conclusion 156
5
Effects of positioningand mobilization
Elizabeth Dean
CHAPTER CONTENTS
INTRODUCTION
The purpose of this chapter is to provide a
framework for clinical decision making in themanagement of patients with cardiopulmonarydysfunction with special emphasis on positioningand mobilization. Cardiopulmonary dysfunctionrefers to impairment of one or more steps in theoxygen transport pathway. First, the oxygen trans-port pathway and the factors that contribute toimpairment of oxygen transport are described.Second, three clinically significant effects of posi-tioning and mobilization are distinguished:
to improve oxygen transport in acute
cardiopulmonary dysfunction to improve oxygen transport in the post-acute
and chronic stages of cardiopulmonarydysfunction
to prevent the negative effects of restrictedmobility, particularly those that adverselyaffect oxygen transport.
In addition, the physiological and scientificrationale for use of positioning and mobilizationfor each of the above effects is described.Conceptualizing cardiopulmonary dysfunctionas impairment of the steps in the oxygen trans-port pathway and exploiting positioning andmobilization as primary interventions in remedi-ating this impairment will maximize physiother-apy efficacy. Emphasis is placed on impairmentof oxygen transport given that such impairmentin large part determines disability and handicap(Verbrugge & Lette 1993), as defined by theWorld Health Organization (1980), secondary tocardiopulmonary dysfunction.
143
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
2/17
The following terms (Ross & Dean 1989) havebeen adopted in this chapter.
1. Positioning refers to the application of bodypositioning to optimize oxygen transport,
primarily by manipulating the effect of gravityon cardiopulmonary and cardiovascularfunction.
2. Mobilization and exercise refer to the applicationof progressive exercise to elicit acute cardio-pulmonary and cardiovascular responses toenhance oxygen transport. In the context ofcardiopulmonary physiotherapy, mobiliz-ation refers to low-intensity exercise for typi-cally acutely ill patients or those with severelycompromised functional work capacity.
3. Optimizing oxygen transport is the goal of posi-tioning and mobilization. The adaptation ortraining-sensitive zone defines the upper andlower limits of the various indices of oxygentransport needed to elicit the optimal adap-tation of the steps in the oxygen transportpathway. This zone is based on an analysis ofthe factors that contribute to cardiopulmonarydysfunction and thus is specific for each patient.
CONCEPTUAL FRAMEWORK FORCLINICAL DECISION MAKING
The oxygen transport pathway
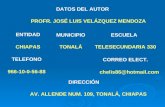
Optimal cardiopulmonary function and gasexchange reflect the optimal matching of oxygendemand and supply (Dantzker 1983, Weber et al1983). Oxygen delivery and oxygen consumptionbased on demand are essential components ofthe oxygen transport system. Figure 5.1 showsthe components of oxygen delivery (DO2),namely arterial oxygen content and cardiacoutput (CO) and the components of oxygenconsumption (VO2), namely the arteriovenousoxygen content difference and CO. In health,DO2 is approximately fourfold greater than VO2 atrest so there is considerable oxygen reserve thatis drawn upon during times of increased meta-bolic demand such as exercise, stress, illness andrepair. Because of the large reserve, VO2 isthought to be normally supply independent. Thisreserve capacity, however, becomes compro-
144 ASSESSMENT, INVESTIGATIONS, SKILLS, TECHNIQUES AND MANAGEMENT
mised secondary to acute and chronic pathologi-cal conditions. In critically ill patients in whomDO2 is severely compromised, VO2 may besupply dependent until DO2 reaches a criticalthreshold, i.e. the level at which metabolicdemands are met (Phang & Russell 1993). Belowthis critical threshold, patients are increasinglydependent on anaerobic metabolism reflectedby increased minute ventilation, respiratoryexchange ratio and serum lactate levels.
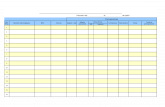
The efficiency with which oxygen is transportedfrom the atmosphere along the steps of the oxygentransport pathway to the tissues determines theefficiency of oxygen transport overall (Fig. 5.2).The steps in the oxygen transport pathway includeventilation of the alveoli, diffusion of oxygenacross the alveolar capillary membrane, perfusion
Oxygen delivery
DO2 = Arterial oxygen contentx Cardiac output
Oxyhaemoglobin + Dissolved oxygen
Oxyhaemoglobin + Dissolved oxygen
Hgb x 1.34 x SaO2 PaO2 x 0.003
Hgb x 1.34 x SVO2 PVO2 x 0.003
Oxygen consumption
VO2 = (Arterial oxygen content -Venous oxygen content) x Cardiac output
Oxygen extraction ratio
OER =Oxygen consumption
Oxygen delivery
VO2
DO2
Figure 5.1 The components of oxygen delivery (DO2) andoxygen consumption (VO2).
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
3/17
EFFECTS OF POSITIONING AND MOBILIZATION 145
Figure
5.2
Aschemeofthecomponentsofventilatorycardiovascularmetaboliccouplingunderlyingoxy
gentransportmodifiedfromWasserm
anetal(1987).
CNS,centralnervoussystem;AN
S,autonomicnervoussystem;DPG,diphosphoglycerate;RBC,redblood
cell;Hct,haematocrit;Hb,haemoglo
bin.
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
4/17
of the lungs, biochemical reaction of oxygen withthe blood, affinity of oxygen with haemoglobin,cardiac output, integrity of the peripheral circula-tion and oxygen extraction at the tissue level(Johnson 1973, Wassermann et al 1987). At rest,
the demand for oxygen reflects basal metabolicrequirements. Metabolic demand changes nor-mally in response to gravitational (positional),exercise and psychological stressors. When one ormore steps in the oxygen transport pathway isimpaired secondary to cardiopulmonary dys-function, oxygen demand at rest and in responseto stressors can be increased significantly.Impairment of one step in the pathway may becompensated by other steps, thereby maintainingnormal gas exchange and arterial oxygenation.With severe impairment involving several steps,arterial oxygenation may be reduced, the work ofthe heart and lungs increased, tissue oxygenationimpaired and, in the most extreme situation,multiorgan system failure may ensue.
While the oxygen transport pathway ensuresthat an adequate supply of oxygen meets thedemands of the working tissues, the carbondioxide pathway ensures that carbon dioxide, aprimary byproduct of metabolism, is eliminated.This pathway is basically the reverse of theoxygen transport pathway in that carbon dioxideis transported from the tissues via the circulationto the lungs for elimination. Carbon dioxide is ahighly diffusible gas and is readily eliminatedfrom the body. However, carbon dioxide reten-tion is a hallmark of diseases in which the venti-latory muscle pump is operating inefficiently orthe normal elastic recoil of the lung parenchymais lost.
Factors contributing tocardiopulmonary dysfunction
Cardiopulmonary dysfunction, in whichoxygen transport is threatened or impaired,results from four principal factors: the underly-ing disease pathophysiology, bedrest/recum-bency and restricted mobility, extrinsic factorsimposed by the patients medical care andintrinsic factors relating to the patient (Box 5.1)(Dean 1993a, Dean & Ross 1992a). An analysis of
146 ASSESSMENT, INVESTIGATIONS, SKILLS, TECHNIQUES AND MANAGEMENT
those factors that contribute to cardiopul-monary dysfunction provides the basis forassessment and prescribing the parameters ofpositioning and mobilization to enhance oxygentransport for a given patient. The treatment isdirected at the specific underlying contributingfactors. In some cases, e.g. low haemoglobin, theunderlying impairment of oxygen transportcannot be affected directly by physical interven-tion. However, mobilization and exercise can
Box 5.1 Factors contributing to cardiopulmonarydysfunction, i.e. factors that compromise or threatenoxygen transport (adapted from Dean 1993a, Dean &Ross 1992a and Ross & Dean 1992)
Cardiopulmonary pathophysiologyAcuteChronic primary
secondaryAcute and chronic
Bedrest/recumbency and restricted mobility
Extrinsic factorsReduced arousalSurgical proceduresIncisionsDressings and bindingsCasts/splinting devices/tractionInvasive lines/cathetersMonitoring equipmentMedicationsIntubationMechanical ventilationSuctioningPainAnxietyHospital admission
Intrinsic factorsAgeGenderEthnicityCongenital abnormalitiesSmoking historyOccupationAir qualityObesityNutritional deficitsDeformityFluid and electrolyte balanceConditioning levelImpaired immunityAnaemia/polycythaemiaThyroid abnormalitiesMultisystem complicationsPrevious medical and surgical history
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
5/17
improve aerobic capacity in patients withanaemia, a factor not directly modifiableby non-invasive physiotherapy interventions,by increasing the efficiency of other steps in theoxygen transport pathway (Williams 1995).
Further, even though some factors are notdirectly modifiable by non-invasive physiotherapy interventions, they influence treatmentoutcome and thus need to be considered whenplanning, modifying and progressing treatment.
Multisystem organ dysfunction and failure maylead to or result from cardiopulmonary dys-function; thus they are associated with significantmortality and morbidity. In these conditions,multiple factors impair multiple steps in theoxygen transport pathway so identifying whichsteps are affected and amenable to physiotherapyinterventions is central to optimal treatmentoutcome (Dean & Frownfelter 1996).
EFFECTS OF POSITIONING AND MOBILIZATION 147
THERAPEUTIC EFFECTS OFPOSITIONING AND MOBILIZATION
To improve oxygen transport in acutecardiopulmonary dysfunction
Positioning and mobilization have profound acuteeffects on cardiovascular and cardiopulmonaryfunction and hence on oxygen transport (Table5.1). These effects translate into improved gasexchange overall: reduction in the fraction ofinspired oxygen, pharmacological and ventilatorysupport (Burns & Jones 1975, Dean 1985, Svanberg1957). Such effects need to be exploited in themanagement of acute cardiopulmonary dysfunc-tion with the use of positioning and mobilizationas primary treatment interventions to enhanceoxygen transport and as between-treatment inter-ventions (Dean & Ross 1992b, Ross & Dean 1992).The physiotherapists role is to prescribe these
Table 5.1 Acute effects of upright positioning and mobilization on oxygen transport (adapted from Dean & Ross (1992a) andImle & Klemic (1989))
Systemic responseStimulus
Positioning (supine to upright) Mobilization
Cardiopulmonary Total lung capacity Alveolar ventilation Tidal volume Tidal volume Vital capacity Breathing frequency Functioning residual capacity AaO2 gradient Residual volume Pulmonary arteriovenous shunt Expiratory reserve volume VA/Q
matching Forced expiratory volumes Distension and recruitment of lung Forced expiratory flows units with low ventilation and low Lung compliance perfusion Airway resistance Mobilization of secretions Airway closure Pulmonary lymphatic drainage PaO2 Surfactant production and distribution AP diameter of chest
Lateral diameter of rib cage and abdomenAltered pulmonary blood flow distribution Work of breathing Diaphragmatic excursion Mobilization of secretions
Cardiovascular Total blood volume Cardiac output Central blood volume Stroke volume and heart rate Central venous pressure Oxygen binding in blood Pulmonary vascular congestion Oxygen dissociation and extraction Lymphatic drainage at the tissue level Work of the heart
AP, anteroposterior; , increases; , decreases.
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
6/17
interventions judiciously to optimize gas exchangeand oxygen transport overall. This role is distinctfrom routine positioning and mobilization oftenperformed jointly by the physiotherapy andnursing staff. The aim of routine positioning and
mobilization is primarily to reduce the adverseeffects of restricted mobility including pulmonarycomplications, bedsores and contractures.
To simulate the normal physiologic body posi-tion, the primary goal of physiotherapy is to getthe patient upright and moving. Mobilization andexercise are the most physiologic and potent inter-ventions to optimize oxygen transport and aerobiccapacity and so need to be exploited with everypatient. Body positioning, however, is discussedin this chapter first because a patient cannot be ina position uninfluenced by gravity. Furthermore, apatients oxygen transport status reflects the bodyposition assumed regardless of whether theposition is part of a treatment regimen, a routinepositioning regimen or assumed randomly bythe patient.
Positioning
Physiological and scientific rationale. The distrib-utions of ventilation (VA), perfusion (Q) and venti-lation and perfusion matching in the lungs areprimarily influenced by gravity and thereforebody position (Clauss et al 1968, West 1962, 1977).The intrapleural pressure becomes less negativedown the upright lung. Thus, the apices have agreater initial volume and reduced compliancethan do the bases. Because the bases are more com-pliant in this position, they exhibit greater volumechanges during ventilation. In addition to thesegravity-dependent interregional differences inlung volume, ventilation is influenced by intrare-gional differences which are dependent onregional mechanical differences in the complianceof the lung parenchyma and the resistance toairflow in the airways. Perfusion increases downthe upright lung such that the VA/Q ratio in theapices is disproportionately high compared withthat in the bases. Ventilation and perfusion match-ing is optimal in the mid-lung region.Manipulating body position, however, alters bothinterregional and intraregional determinants of
148 ASSESSMENT, INVESTIGATIONS, SKILLS, TECHNIQUES AND MANAGEMENT
ventilation and perfusion and their matching.When choosing specific positions to enhance arte-rial oxygenation for a given patient, one needs toconsider the underlying pathophysiology impair-ing cardiopulmonary function, the effects of bed
rest/recumbency and restricted mobility, extrinsicfactors related to the patients care and intrinsicfactors related to the patient.
Although the negative effects of the supineposition have been well documented for severaldecades (Dean & Ross 1992b, Dripps & Waters1941), supine or recumbent positions are fre-quently assumed by patients in hospital. Thesepositions are non-physiologic and are associatedwith significant reductions in lung volumes andflow rates and increased work of breathing(Craig et al 1971, Hsu & Hickey 1976). Thedecrease in functional residual capacity (FRC)contributes to closure of the dependent airwaysand reduced arterial oxygenation (Ray et al1974). This effect is accentuated in older persons(Leblanc et al 1970), patients with cardio-pulmonary disease (Fowler 1949), patients withabdominal pathology, smokers and obeseindividuals.
The haemodynamic consequences of thesupine position are also remarkable. The gravity-dependent increase in central blood volume mayprecipitate vascular congestion, reduced compli-ance and pulmonary oedema (Blomqvist & Stone1983, Sjostrand 1951). The commensurate increasein stroke volume increases the work of the heart(Levine & Lown 1952). Within 6 hours, a compen-satory diuresis can lead to a loss of circulatingblood volume and orthostatic intolerance, i.e.haemodynamic intolerance to the upright posi-tion. Bed rest reconditioning has been attributedto this reduction in blood volume and the impair-ment of the volume-regulating mechanismsrather than physical deconditioning per se(Hahn-Winslow 1985). Thus, the upright positionis essential to maximize lung volumes and flowrates and this position is the only means of opti-mizing fluid shifts such that the circulating bloodvolume and the volume-regulating mechanismsare maintained. The upright position coupledwith movement is necessary to promote normalfluid regulation and balance (Lamb et al 1964).
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
7/17
The upright position is a potent stimulus to thesympathetic nervous system. This is an import-ant effect clinically which offsets impaired bloodvolume and pressure-regulating mechanismssecondary to recumbency (Hahn-Winslow 1985).
Stimulation of the sympathetic nervous systemhas been reported to augment the effects ofpotent sympathomimetic pharmacological agentssuch that the dosages of these drugs can bereduced (Warren et al 1983). The reduction orelimination of sympathomimetic drugs is animportant outcome of non-invasive physio-therapy interventions.
Side-to-side positioning is frequently used inthe clinical setting. If applied in response toassessment rather than routinely (Chuley et al1982), the benefits derived from such positioningcan be enhanced. Adult patients with unilaterallung disease may derive greater benefit when theaffected lung is uppermost (Remolina et al 1981).Markedly improved gas exchange without dele-terious haemodynamic effects has been reportedfor patients with severe hypoxaemia secondary topneumonia (Dreyfuss et al 1992). Arterial oxygentension is increased secondary to improved venti-lation of the unaffected lung when this lung isdependent. Patients with uniformly distributedbilateral lung disease may derive greater benefitwhen the right lung is lowermost (Zack et al1974). In this case, arterial oxygen tension isincreased secondary to improved ventilation ofthe right lung, which may reflect the increasedsize of the right lung compared with the leftand that, in this position, the heart and adjacentlung tissue are subjected to less compression.Improved gas exchange through non-invasiveinterventions can reduce or eliminate the need forsupplemental oxygen which are primary treat-ment outcomes. Although various studies haveshown beneficial effects of side lying, positioningshould be based on multiple considerationsincluding the distribution of disease if optimalresults are to be obtained.
The prone position has long been known tohave considerable physiological justification inpatients with cardiopulmonary compromise(Douglas et al 1977), even those who are criticallyill with acute respiratory failure (Bittner et al 1996,
EFFECTS OF POSITIONING AND MOBILIZATION 149
Chatte et al 1997, Mure et al 1997) and patientswith trauma-induced adult respiratory distresssyndrome (Friedrich et al 1996). The beneficialeffects of the prone position on arterial oxygen-ation may reflect improved lung compliance sec-
ondary to stabilization of the anterior chest wall,tidal ventilation, diaphragmatic excursion, FRCand reduced airway closure (Dean 1985, Pelosi etal 1998). In a dog model of acute lung injury,however, improved PaO2 in prone has been attrib-uted to a reduced shunt fraction (Albert et al1987). A variant of the prone position, proneabdomen free, has shown additional benefits overprone abdomen restricted. In the prone abdomen-free position, the patient is positioned such thatthe movement of the abdomen is unencumberedby the bed. This can be achieved either by raisingthe patients body in relation to the bed so that theabdomen falls free or by using a bed with a holecut out at the level of the abdomen. Despite com-pelling evidence to support the prone position, itmay be poorly tolerated in some patients or maybe contraindicated in haemodynamically unstablepatients. In these situations, intermediate posi-tions approximating prone may produce many ofthe beneficial effects and minimize any potentialhazard.
Positioning for drainage of pulmonary secre-tions may be indicated in some patients (Kirilloffet al 1985). Historically, these positions have beenbased on the anatomical arrangement of thebronchopulmonary segments to facilitate drain-age of a particular segment. The bronchiole to thesegment of interest is positioned perpendicularto facilitate drainage with the use of gravity. Theefficacy of postural drainage compared withdeep breathing and coughing induced withmobilization/exercise and repositioning of thepatient has not been established. However, thefact that mobilization impacts on more steps inthe oxygen transport pathway including theairways, to effect secretion clearance, supportsthe exploitation of mobilization coupled withdeep breathing manoeuvres and coughing as aprimary treatment intervention.
Physiotherapists need to consider two aspectsof body positioning when the goal is to optimizeoxygen transport. One is to select and apply
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
8/17
specific body positions based on the patientspresentation, laboratory test results and radio-graphic imaging. The other is to elicit physio-logic stir-up (Dean 1996a, Dripps & Waters1941). The purpose is to effect the normal gravi-
tational stress on cardiopulmonary and cardio-vascular function that is experienced in health.This is best simulated if patients are changedfrom one extreme position to another, e.g.supine to prone or upright, rather than fromhalf to full side lying which is associated with alesser stir-up effect. Haemodynamically unsta-ble patients, however, require greater monitor-ing during extreme position changes and maynot tolerate some position changes well. Thus,based on assessment and patient response, fre-quent extreme position changes may be prefer-able to minimal shifts in body position in orderto optimize cardiovascular, pulmonary andhaemodynamic function.
Assessment and treatment planning. Body posi-tioning, i.e. the specific positions selected, theduration of time spent in each position and thefrequency with which the position is assumed, isbased on a consideration of the factors that con-tribute to cardiopulmonary dysfunction, andtreatment response. Understanding of the physi-
150 ASSESSMENT, INVESTIGATIONS, SKILLS, TECHNIQUES AND MANAGEMENT
ology of cardiopulmonary and cardiovascularfunction and the effects of disease highlightscertain positions that are theoretically ideal.However, these positions need to be modified ormay be contraindicated for a given patient, based
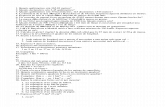
on other considerations (see Box 5.1). Forexample, if extreme positional changes are con-traindicated, small degrees of positional rotationperformed frequently can have significantbenefit on gas exchange and arterial oxygena-tion. A three-quarters prone position mayproduce favourable results when the full proneposition is contraindicated or is not feasible. Thismodification may simulate the prone abdomen-free position which has been shown to augmentthe effect of the traditional prone abdomen-restricted position (Douglas et al 1977).Furthermore, a three-quarters prone positionmay be particularly beneficial in patients withobese or swollen abdomens who may not tolerateother variations of the prone position. With atten-tion to the patients condition, invasive lines andleads and appropriate monitoring, a patient canbe aggressively positioned (Fig. 5.3).
The time which a patient spends in a positionand the frequency with which that position isassumed over a period of time are based on the
Figure 5.3 Positioning a criticallyill patient may require severalpeople and continual monitoring ofthe patients response. Eventhough a position (particularly anupright position) may only betolerated for a short period of time,the physiological benefits areconsiderable.
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
9/17
indications for the position and treatmentoutcome. Objective measures of the various stepsthat are compromised in the oxygen transportpathway as well as indices of oxygen transportoverall are used in making these decisions.Subjective evaluation based on clinical judge-ment also has a role. A specific position can bejustified, provided there is objective and subjec-tive evidence of improvement. Signs and symp-toms of deterioration need to be monitored sothat deleterious positions can be avoided anddeterioration secondary to excessive time in anyone position can be detected. Prolonged durationin any single position will inevitably lead to com-promise of the function of dependent lung zonesand impaired gas exchange.
The ratio of treatment to between-treatmenttime is low. Typically, between-treatment timeconsists of some combination of positioning andmobilization. Positioning and mobilizing patientsbetween treatments may be incorporated as anextension of treatment. Patients require monitor-ing and observation during these periods, as wellas treatments. Between-treatment time may incor-porate the use of maximally restful positions thatdo not compromise oxygen transport. Lastly,patients are positioned and mobilized betweentreatments to prevent the negative effects ofrestricted mobility and recumbency.
Special consideration (e.g. with respect tospecific positioning and the use of supports)needs to be given to positioning patients who arecomatose or paralysed because their joints andmuscles are relatively unprotected and prone totrauma. Positions need to be selected that avoidinjury to unprotected head, neck and limbs.
Progression. Progression of positioninginvolves new positions or modification of previ-ous positions and modification of the durationspent in each position and the frequency withwhich each position is assumed over a period oftime. These clinical decisions are based on thefactors that contribute to cardiopulmonary dys-function and objective and subjective indices ofchange in the patients cardiopulmonary status.With improvement in cardiopulmonary status, thepatient spends more time in erect positions and ismobilized more frequently and independently.
EFFECTS OF POSITIONING AND MOBILIZATION 151
Mobilization
Physiological and scientific rationale. Comparedwith long-term exercise, the mechanisms under-lying adaptation of the oxygen transport system to
acute exercise, i.e. from session to session and dayto day, are less well understood. However,although these mechanisms have yet to be eluci-dated, the responses to acute exercise are welldocumented. The acute response to mobilization/exercise reflects a commensurate increase inoxygen transport to provide oxygen to the work-ing muscles and other organs. The increase isdependent on the intensity of the mobilization/exercise stimulus. The demand for oxygen andoxygen consumption (VO2) increases as exercisecontinues, with commensurate increases inminute ventilation (VE), i.e. the amount of airinhaled per minute, cardiac output and oxygenextraction at the tissue level. Relatively low inten-sities of mobilization can have a direct and pro-found effect on oxygen transport in patients withacute cardiopulmonary dysfunction (Dean & Ross1992a, Dull & Dull 1983, Lewis 1980) and need tobe instituted early after the initial pathologicalinsult (Orlava 1959, Wenger 1982). The resultingexercise hyperpnoea, i.e. the increase in VE, iseffected by an increase in tidal volume and breath-ing frequency. In addition, ventilation and perfu-sion matching is augmented by the distension andrecruitment of lung zones with low ventilationand low perfusion. Spontaneous exercise-induceddeep breaths are associated with improved flowrates and mobilization of pulmonary secretions(Wolff et al 1977). In clinical populations, theseeffects elicit spontaneous coughing. When mobil-ization is performed in the upright position,the anteroposterior diameter of the chest wallassumes a normal configuration compared withthe recumbent position in which the anteroposter-ior diameter is reduced and the transverse dia-meter is increased. In addition, diaphragmaticexcursion is favoured, flow rates augmented andcoughing is mechanically facilitated. The work ofbreathing may be reduced with caudal displace-ment of the diaphragm and the work of the heartis minimized by the displacement of fluid awayfrom the central circulation to the legs. Thus,
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
10/17
despite increased metabolic demands of mobiliz-ation and exercise, the goal is to ensure that thisincreased demand is not wasteful and the demandcan be met by the supply.
With respect to cardiovascular effects, acute
mobilization/exercise increases CO by increas-ing stroke volume and heart rate. This is associ-ated with increased blood pressure and increasedcoronary and peripheral muscle perfusion.
Passive movement of the limbs may stimulatedeep breaths and heart function (West 1995).There is little scientific evidence, however, tosupport any additional benefit from various facil-itation techniques (Bethune 1975). Thus, timeallocated to the use of passive manoeuvres maycompete with time for positioning and mobiliza-tion, i.e. interventions with demonstrated clinicalefficacy. Although passive movements have arelatively small effect on cardiopulmonary func-tion, they have several important benefits forneuromuscular and musculoskeletal functionwhich support their use provided they do notreplace active movement.
Assessment and treatment planning. For practi-cal and ethical considerations, the mobilizationplan for the patient with acute cardiopulmonarydysfunction cannot be based on a standardizedexercise test, as is the case for patients withchronic conditions. However, response to amobilization/exercise stimulus can be assessedduring a mobilization challenge test, i.e. duringthe patients routine activities such as turning ormoving in bed, activities of daily living orresponding to routine nursing and medical pro-cedures (Dean 1996b). Comparable to prescribingexercise for the patient with chronic cardio-pulmonary dysfunction, the parameters arespecifically defined so that the stimulus is opti-mally therapeutic. The optimal stimulus is thatwhich stresses the oxygen transport capacity ofthe patient and effects the greatest adaptationwithout deterioration or distress.
To promote adaptation of the steps in theoxygen transport pathway to the stimulation ofacute mobilization, the stimulus is administeredin a comparable manner to that in an exercise pro-gramme prescribed for chronic cardiopulmonarydysfunction. The components include a pre-exer-
152 ASSESSMENT, INVESTIGATIONS, SKILLS, TECHNIQUES AND MANAGEMENT
cise period, a warm-up period, a steady-stateperiod, a cool-down period and a recovery period(Blair et al 1988). These components optimize theresponse to exercise by preparing the cardiopul-monary and cardiovascular systems for steady-
state exercise and by permitting these systems toreestablish resting conditions following exercise.The cool-down period, in conjunction with therecovery period, ensures that exercise does notstop abruptly and allows for biochemical degra-dation and removal of the byproducts of metabo-lism. Mobilization consists of discrete warm-up,steady-state and cool-down periods; the compo-nents need to be identified, even in the patientwith a very low functional capacity, i.e. a criticallyill patient who may be only able to sit up over theedge of the bed. In such cases, preparing to sit upconstitutes a warm-up period for the patient; thestimulus of sitting unsupported for severalminutes while being aroused and encouraged totalk or be interactive non-verbally, if mechanicallyventilated, constitutes a steady-state period;returning to bed constitutes the cool-downperiod. In the recovery period, observation of thepatient continues to ensure that mobilization istolerated well and that the indices of oxygentransport return to resting levels. This informa-tion is then used as the basis for mobilization inthe next treatment.
Valid and reliable monitoring practices providethe basis for defining the parameters of mobiliza-tion, assessing the need for progression anddefining the adaptation or training-sensitive zone.Monitoring is also essential given that subjectingpatients to mobilization/exercise stimulation isinherently risky, particularly for patients with car-diopulmonary dysfunction. Indices of overalloxygen transport in addition to indices of thefunction of the individual steps in the oxygentransport pathway provide a detailed profile ofthe patients cardiopulmonary status. In criticalcare settings, the physiotherapist has access to awide range of measures to assess the adequacy ofgas exchange. Minimally, in the general wardsetting, measures of breathing frequency, arterialblood gases, arterial saturation, heart rate, bloodpressure and clinical observation provide the basisfor ongoing assessment, mobilization/exercise
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
11/17
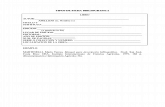
and progression. With appropriate attention to thepatients condition, invasive lines and leads andappropriate monitoring, a patient can be aggres-sively mobilized and ambulated (Fig. 5.4).
A fundamental requirement in defining the
parameters for mobilization is that the patientsoxygen transport system is capable of increasingthe oxygen supply to meet an increasing meta-bolic demand. If not, mobilization is absolutelycontraindicated and the treatment of choice tooptimize oxygen transport is body positioning.However, in the case of a patient being severelyhaemodynamically unstable, even the stress ofpositioning may be excessive. Thus, althoughcritically ill patients may be treated aggressively,every patient has to be considered individually,otherwise the patient may deteriorate or beseriously endangered.
Progression. Progression and modification ofthe mobilization stimulus occur more rapidly inthe management of the patient with acute cardio-pulmonary dysfunction compared with the pro-gression of the exercise stimulus for the patientwith chronic illness. The status of acutely ill
EFFECTS OF POSITIONING AND MOBILIZATION 153
patients can vary considerably within minutes orhours. Whether the mobilization stimulus isincreased or decreased in intensity depends on thepatients status and altered responses to mobiliza-tion. The mobilization stimulus is adjusted such
that it remains optimal despite the patientschanging metabolic needs. Capitalizing on narrowwindows of opportunity for therapeutic interven-tion must be exploited 24 hours a day with respectto the type of mobilization stimulus, its intensity,duration and frequency, particularly in the criti-cally ill patient.
The immovable patient. Given the well-documented negative effects of restricted mobil-ity, the immovable patient deserves specialconsideration. Although bed rest or activityrestriction is ordered for patients frequentlywithout reservation, the risks need to be weighedagainst the benefits. Restricted mobility coupledwith recumbency constitutes a death knell formany severely compromised patients. Thus, anorder for bed rest needs to be evaluated and chal-lenged to ensure that this order is physiologicallyjustified.
Figure 5.4 Example of mobilizing a patient to a self-supported upright sittingposition. Mobilizing a critically ill patient needs to be a priority wherever possible.Short frequent sessions to the erect position (sitting or standing if possible) withcontinual monitoring of the patients response should be the goal. As the patientprogresses, sessions increase in intensity and duration and reduce in frequency.
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
12/17
Kinetic beds and chairs. Advances in furnituretechnology to facilitate positioning and mobiliz-ing patients have lagged behind advances inclinical medicine, particularly in the critical carearea. Conventional hospital beds are designed to
be stationary and their widths and heights areoften non-adjustable, making it difficult for thepatient to get in and out of bed. Kinetic beds andchairs have become increasingly available overthe past decade but they are not widely used clin-ically. These devices were originally designed tofacilitate positioning and moving heavy andcomatose patients. Some beds are designed torotate on their long axis from side to side overseveral minutes. Other beds simulate a side-to-side movement with inflation and deflation ofthe two sides of an air-filled mattress. Althoughthese beds have potential cardiopulmonarybenefit (Glavis et al 1985, Kyle et al 1992), they donot replace active positioning and movement.
Mechanically adjustable bedside chairs consti-tute an important advance. These chairs adjust toa flat horizontal surface that can be matched tobed height and positioned beneath the patientlying on the bed. The device with the patient ontop is then wheeled parallel to the bed where itcan be adjusted back into a chair and thus thepatient assumes a seated position. The degree ofrecline can be altered to meet the patients needsand for comfort. This chair also facilitates return-ing the patient to bed. Comparable to these chairsare beds which can be converted into a chairwhile the patient is lying down. These avoid thenegative effects of using tilt tables where thefluid shifts caudally are extreme and more riskyby comparison.
The disadvantages of kinetic beds and chairsinclude the expense and the potential for overre-liance on them. Without these devices, a heavypatient may require several people and severalminutes to position in a chair which may be onlytolerated for a few minutes. However, the cardio-pulmonary benefits of the stimulation of pre-paring to be moved, the reflex attempts of thepatient to assist and adjust to changing position,as well as actually sitting upright in a chair arenot reproduced by bed positioning alone or by akinetic bed. Research is needed to determine the
154 ASSESSMENT, INVESTIGATIONS, SKILLS, TECHNIQUES AND MANAGEMENT
indications and potential benefits of kinetic bedsand chairs so that they can be used judiciously inthe clinical setting as an integral therapeuticintervention.
To improve oxygen transport inpost-acute and chroniccardiopulmonary dysfunction
In post-acute and chronic cardiopulmonary dys-function, a primary consequence of impairedoxygen transport is reduced functional workcapacity (Belman & Wasserman 1981, Wasserman& Whipp 1975). Work capacity can be improvedwith long-term exercise which improves theefficiency of the steps in the oxygen transportpathway and promotes compensation within thepathway as well as by other mechanisms. Tooptimize the patients response, exercise can becarried out in judicious body positions in whichoxygen transport is favoured.
Exercise is the treatment of choice for patientswhose impaired oxygen transport has resultedfrom chronic cardiopulmonary dysfunction.Body positioning, however, may have some rolein severe patients in optimizing oxygen transportat rest. Barach & Beck (1954), for example,reported that emphysematous patients were lessbreathless, had reduced accessory muscle activ-ity and had a significant reduction in ventilationwhen positioned in a 16 head-down position.Some patients exhibited greater symptomaticimprovement than in the upright position withsupplemental oxygen. Classic relaxation posi-tions, e.g. leaning forward with the forearms sup-ported, can also be supported physiologically.Coupling such physiologically justifiable posi-tions with mobilization/exercise will augmentthe benefits of exercise.
Physiological and scientific rationale. Althoughthe physiological responses to long-term exercisein patients with chronic cardiopulmonarydisease may differ from those in healthy persons,patients can significantly improve their func-tional work capacity (Table 5.2). In healthypersons, an improvement in aerobic capacityreflects improved efficiency of the steps in theoxygen transport pathway to adapt to increased
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
13/17
oxygen demands imposed by exercise stress.This adaptation is effected by both central(cardiopulmonary) and peripheral (at the tissuelevel) changes (Dean & Ross 1992a, Wasserman &Whipp 1975). Such aerobic conditioning is char-
acterized by a training-induced bradycardiasecondary to an increased stroke volume andincreased oxygen extraction capacity of theworking muscle. These adaptation or trainingresponses result in an increased maximal oxygenuptake and maximal voluntary ventilation andreduced submaximal VE, cardiac output, heartrate, blood pressure and perceived exertion.Patients with chronic lung disease, however, areoften unable to exercise at the intensity requiredto elicit an aerobic training response. Their func-tional work capacity is improved by other mech-anisms, e.g. desensitization to breathlessness,improved motivation, improved biomechanicalefficiency, increased ventilatory muscle strengthand endurance or some combination (Belman &Wasserman 1981, Loke et al 1984). Patients withchronic heart disease, such as those withinfarcted left ventricles, may be able to train aero-bically; however, training adaptation primarilyresults from peripheral rather than central factors
EFFECTS OF POSITIONING AND MOBILIZATION 155
(Bydgman & Wahren 1974, Hossack 1987, Wardet al 1987).
Planning an exercise programme. The exerciseprogramme is based on the principle that oxygendelivery and uptake are enhanced in response to
an exercise stimulus which is precisely definedfor an individual in terms of the type of exercise,its intensity, duration, frequency and the courseof the training programme. These parameters arebased on an exercise test in conjunction withassessment findings. Exercise tests are performedon a cycle ergometer or treadmill or with a walktest. The general procedures and protocols arestandardized to maximize the validity and relia-bility of the results (Dean et al 1989, Blair et al1988). The principles of and guidelines for exer-cise testing and training patients with chroniclung and heart disease have been well docu-mented (Dean 1993b). The training-sensitivezone is defined by objective and subjective meas-ures of oxygen transport determined from theexercise test. The components of each exercisetraining session include baseline, warm-up,steady-state portion, cool-down and recoveryperiod (Blair et al 1988, Dean 1993b). The cardio-pulmonary and cardiovascular systems aregradually primed for sustaining a given levelof exercise stress, whilst in addition the mus-culoskeletal system adapts correspondingly.Following the steady-state portion of the trainingsession, the cool-down period permits a return tothe resting physiological state. Cool-down andrecovery periods are essential for the biochemicaldegradation and elimination of the metabolicbyproducts of exercise.
Progression. Progression of the exercise pro-gramme is based on a repeated exercise test. Thisis indicated when the exercise prescription nolonger elicits the desired physiological responses specifically, when the steady-state work rateconsistently elicits responses at the low end orbelow the lower limit of the training-sensitivezone for the given indices of oxygen transport.This reflects that maximal adaptation of the stepsin the oxygen transport pathway to the givenexercise stimulus has occurred. The degree ofconditioning achieved is precisely matched to thedemands of the exercise stimulus imposed.
Table 5.2 Chronic effects of mobilization/exercise onoxygen transport
Systemic response Effect
Cardiopulmonary Capacity for gas exchange Cardiopulmonary efficiency Submaximal minute ventilation Work of breathing
Cardiovascular Exercise-induced bradycardia Maximum VO2 Submaximal heart rate, blood
pressure, myocardial oxygen
demand, stroke volume, cardiacoutput
Work of the heart Perceived exertion Plasma volumeCardiac hypertrophy Vascularity of the myocardium
Tissue level Vascularity of working muscle Myoglobin content and oxidative
enzymes in muscle Oxygen extraction capacity
, increases; , decreases.
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
14/17
To prevent the negative effects ofrestricted mobility
Although physiologically distinct, the effects ofimmobility are frequently confounded by the
effects of recumbency in the hospitalized patient.Restricted mobility and the concomitant reduc-tion in exercise stress affect virtually every organsystem in the body with profound effects on thecardiovascular and neuromuscular systems.Recumbency and the elimination of the verticalgravitational stress exert their effects primarilyon the cardiovascular and cardiopulmonarysystems (Blomqvist & Stone 1983, Dock 1944,Harrison 1944). The most serious consequencesof restricted mobility and recumbency are those
resulting from the effects on the cardiopul-monary and cardiovascular systems and henceon oxygen transport. Although other conse-quences of restricted mobility, e.g. increased riskof infection, skin breakdown and deformity, maynot constitute the same immediate threat tooxygen transport and tissue oxygenation, theycan have significant implications with respect tomorbidity and mortality (Rubin 1988). Thus,restricted mobility and recumbency need to be
156 ASSESSMENT, INVESTIGATIONS, SKILLS, TECHNIQUES AND MANAGEMENT
minimized and mobility and the upright positionmaximized to avert the negative consequences ofrestricted mobility, the risk of morbidity associ-ated with these effects and the direct and indirectcardiopulmonary and cardiovascular effects.
These negative consequences are preventablewith frequent repositioning and mobilizing ofthe patient (Table 5.3). The prevention of theseeffects is a primary goal of positioning and mobi-lizing patients between treatments.
SUMMARY AND CONCLUSION
Cardiopulmonary dysfunction refers to impair-ment of one or more steps in the oxygen transportpathway which can impair oxygen transportoverall. Thus, a conceptual framework for clinicalproblem solving in the management of patientswith cardiopulmonary dysfunction, based onoxygen transport, can facilitate the identificationof deficits and the directing of treatment to eachspecific deficit. Factors that can impair the trans-port of oxygen from the atmosphere to the tissuesinclude cardiopulmonary pathology, bedrest,recumbency and restricted mobility, extrinsicfactors related to the patients medical care,
Table 5.3 Effects of positioning and mobilization that prevent the negative effects of restricted mobility and recumbency*
Systemic response Effect
Cardiopulmonary Alveolar ventilation Airway closureAlters the distributions of ventilation, perfusion and ventilation and perfusion matchingAlters pulmonary blood volumeAlters distending forces on uppermost lung fields Secretion poolingSecretion mobilization and redistributionAlters chest wall configuration and pulmonary mechanicsVaries work of breathing
Cardiovascular Alters cardiac compression (positioning), wall tensions, filling pressuresAlters preload, afterload and myocardial contractionAlters lymphatic drainageVaries work of the heartPromotes fluid shiftsStimulates pressure- and volume-regulating mechanisms of the circulationStimulates vasomotor activityMaintains normal fluid balance and distribution
Tissue level Alters hydrostatic pressure and tissue perfusionMaintains oxygen extraction capacity (mobilization)
*Some of the preventive effects of body positioning and mobilization are comparable; however, the magnitude of these effectsin response to mobilization tends to be greater than with body positioning.
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
15/17
intrinsic factors related to the patient or a combin-ation of these. Positioning and mobilization aretwo interventions that have potent and directeffects on several of the steps in the oxygen trans-port pathway. These interventions have aprimary
role in improving oxygen transport in acute andchronic cardiopulmonary dysfunction and inaverting the negative effects of restricted mobilityand recumbency, particularly those related tocardiopulmonary and cardiovascular function.
The principal goal of physiotherapy in themanagement of cardiopulmonary dysfunction isto optimize oxygen transport. A systematicapproach to achieving this goal consists of:
1. Distinguishing the specific steps in the oxygen
transport pathway which are impaired orthreatened.
2. Establishing which factors contribute to thisimpairment
3. Distinguishing which factors are (a) amenableto positioning and mobilization and (b) notdirectly amenable to positioning and mobil-ization, as these factors will modify treatment
4. Specifying the parameters for positioning andmobilization so that they directly address thefactors responsible for the cardiopulmonary
EFFECTS OF POSITIONING AND MOBILIZATION 157
dysfunction wherever possible, i.e. to elicitthe acute effects of these interventions toenhance oxygen transport or to elicit the long-term effects on oxygen transport, i.e. trainingresponses and improved functional work
capacity5. Avoiding the multisystem consequences of
restricted mobility and recumbency, particu-larly those that impair or threaten oxygentransport
6. Recognizing when positioning or mobilizing apatient needs to be modified to avoid a delete-rious outcome.
Conceptualizing cardiopulmonary dysfunc-tion as deficits in the steps in the oxygen
transport pathway and identifying the factorsresponsible for each impaired step providesa systematic, evidence-based approach to clinicaldecision making in cardiopulmonary physiother-apy. Positioning and mobilization can then bespecifically directed at the mechanisms under-lying cardiopulmonary dysfunction whereverpossible. Such an approach will maximize theefficacy of positioning and mobilizing patientswith cardiopulmonary dysfunction and enhancethe outcome of medical management overall.
REFERENCES
Albert RK, Leasa D, Sanderson M, Robertson HT, HlastalaMP 1987 The prone position improves arterialoxygenation and reduced shunt in oleic-acid-inducedacute lung injury. American Review of RespiratoryDiseases 138: 828833
Barach AL, Beck GJ 1954 Ventilatory effect of head-downposition in pulmonary emphysema. American Journal ofMedicine 16: 5560
Belman MJ, Wasserman K 1981 Exercise training and testing
in patients with chronic obstructive pulmonary disease.Basics of Respiratory Disease 10: 16Bethune DD 1975 Neurophysiological facilitation of
respiration in the unconscious patient. PhysiotherapyCanada 27: 241245
Bittner E, Chendrasekhar A, Pillai S 1996 Changes inoxygenation and compliance as related to body positionin acute lung injury. American Journal of Surgery 62:10381041
Blair SN, Painter P, Pate RR et al 1988 Resource manual forguidelines for exercise testing and prescription. Lea andFebiger, Philadelphia
Blomqvist CG, Stone HL 1983 Cardiovascular adjustments togravitational stress. In: Shepherd JT, Abboud FM (eds)
Handbook of physiology. Section 2: circulation, vol 2.American Physiological Society, Bethesda, pp 10251063
Burns JR, Jones FL 1975 Early ambulation of patientsrequiring ventilatory assistance. Chest 68: 608
Bydgman S, Wahren J 1974 Influence of body position on theanginal threshold during leg exercise. European Journalof Clinical Investigation 4: 201206
Chatte G, Sab J-M, Dubois J-M 1997 Prone position inmechanically ventilated patients with severe acute
respiratory failure. American Journal of Critical CareMedicine 155: 473478Chuley M, Brown J, Summer W 1982 Effect of postoperative
immobilization after coronary artery bypass surgery.Critical Care Medicine 10: 176178
Clauss RH, Scalabrini BY, Ray RF, Reed GE 1968 Effects ofchanging body position upon improved ventilationperfusion relationships. Circulation 37(suppl 2): 214217
Craig DB, Wahba WM, Don HF 1971 Closing volume andits relationship to gas exchange in seated and supinepositions. Journal of Applied Physiology 31: 717721
Dantzker DR 1983 The influence of cardiovascularfunction on gas exchange. Clinics in Chest Medicine4: 149159
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
16/17
Dean E 1985 Effect of body position on pulmonary function.Physical Therapy 65: 613618
Dean E 1993a Bedrest and deconditioning. NeurologyReport 17: 69
Dean E 1993b Advances in rehabilitation for older personswith cardiopulmonary dysfunction. In: Katz PR, Kane RL,
Mezey MD (eds) Advances in long-term care. Springer-Verlag, New York, pp 171Dean E 1996a Body positioning. In: Frownfelter D, Dean E
(eds) Principles and practice of cardiopulmonary physicaltherapy, 3rd edn. Mosby, St Louis
Dean E 1996b Mobilization and exercise. In: Frownfelter D,Dean E (eds) Principles and practice of cardiopulmonaryphysical therapy, 3rd edn. Mosby, St Louis
Dean E, Frownfelter D 1996 Clinical case study guide toaccompany principles and practice of cardiopulmonaryphysical therapy, 3rd edn. Mosby, St Louis
Dean E, Ross J 1992a Mobilization and exercise conditioning.In: Zadai C (ed) Pulmonary management in physicaltherapy. Churchill Livingstone, New York
Dean E, Ross J 1992b Discordance between cardiopulmonary
physiology and physical therapy: toward a rational basisfor practice. Chest 101: 16941698
Dean E, Ross J, Bartz J, Purves S 1989 Improving the validityof exercise testing: the effect of practice on performance.Archives of Physical Medicine and Rehabilitation 70:599604
Dock W 1944 The evil sequelae of complete bed rest. Journalof the American Medical Association 125: 10831085
Douglas WW, Rehder K, Froukje BM 1977 Improvedoxygenation in patients with acute respiratory failure: theprone position. American Review of Respiratory Disease115: 559566
Dreyfuss D, Djedaini K, Lanore J-J, Mier L, Froidevaux R,Coste F 1992 A comparative study of the effects ofalmitrine bismesylate and lateral position duringunilateral bacterial pneumonia with severe hypoxemia.American Review of Respiratory Disease 148: 295299
Dripps RD, Waters RM 1941 Nursing care of surgical patients.I. The stir-up. American Journal of Nursing 41: 530534
Dull JL, Dull WL 1983 Are maximal inspiratory breathingexercises or incentive spirometry better than earlymobilization after cardiopulmonary bypass? PhysicalTherapy 63: 655659
Fowler WS 1949 Lung function studies. III. Unevenpulmonary ventilation in normal subjects and patientswith pulmonary disease. Journal of Applied Physiology2: 283299
Fredrich P, Krafft P, Hochleuthner H 1996 The effects oflong-term prone positioning in patients with trauma-
induced adult respiratory distress syndrome. Anesthesiaand Analgesia 83: 12061211Glavis C, Sparacino P, Holzemer W, Skov P 1985 Effect of a
rotating bed on mechanically ventilated critically illpatients. Paper presented at the Third Kinetic TherapySeminar, San Antonio
Hahn-Winslow E 1985 Cardiovascular consequences of bedrest. Heart and Lung 14: 236246
Harrison TR 1944 The abuse of rest as a therapeutic measurefor patients with cardiovascular disease. JAMA 125:10751078
Hossack KF 1987 Cardiovascular responses to dynamicexercise. In: Hanson P (ed) Exercise and the heart. WBSaunders, Philadelphia, pp 147156
158 ASSESSMENT, INVESTIGATIONS, SKILLS, TECHNIQUES AND MANAGEMENT
Hsu HO, Hickey RF 1976 Effect of posture on functionalresidual capacity postoperatively. Anesthesiology 44:520521
Imle PC, Klemic N 1989 Changes with immobility andmethods of mobilization. In: Mackenzie CF (ed) Chestphysiotherapy in the intensive care unit, 2nd edn.
Williams and Wilkins, Baltimore, pp 188214Johnson RL 1973 The lung as an organ of oxygen transport.Basics of Respiratory Disease 2: 16
Kirilloff LH, Owens HR, Rogers RM, Mazzocco MC1985 Does chest physical therapy work? Chest
88: 436444Kyle K, Jackiw A, Schroeder S et al 1992 Cardiopulmonary
effects of kinetic bed therapy in mechanically ventilatedpatients. Paper presented at the American ThoracicSociety Meeting, San Antonio
Lamb LE, Johnson RL, Stevens PM 1964 Cardiovasculardeconditioning during chair rest. Aerospace Medicine 23:646649
Leblanc P, Ruff F, Milic-Emili J 1970 Effects of age and bodyposition on airway closure in man. Journal of Applied
Physiology 28: 448451Levine SA, Lown B 1952 Armchair treatment of acute
coronary thrombosis. JAMA 148: 13651369Lewis FR 1980 Management of atelectasis and pneumonia.
Surgical Clinics of North America 60: 13911401Loke J, Mahler DA, Man SFP 1984 Exercise improvement in
chronic obstructive pulmonary disease. Clinics in ChestMedicine 5: 121143
Mure M, Martling C-R, Lindahl SGE 1997 Dramatic effect onoxygenation in patients with severe acute lunginsufficiency treated in the prone position. Critical CareMedicine 25: 15391544
Orlava OE 1959 Therapeutic physical culture in the complextreatment of pneumonia. Physical Therapy Review 39:153160
Pelosi P, Tubiolo D, Mascheroni D 1998 Effects of the proneposition on respiratory mechanics and gas exchangeduring acute lung injury. American Journal of CriticalCare Medicine 157: 387393
Phang PT, Russell JA 1993. When does VO2 depend on VO2?Respiratory Care 38: 618630
Ray JF, Yost L, Moallem S et al 1974 Immobility, hypoxemiaand pulmonary arteriovenous shunting. Archives ofSurgery 109: 537541
Remolina C, Khan AV, Santiago TV, Edelman NH 1981Positional hypoxemia in unilateral lung disease. NewEngland Journal of Medicine 304: 523525
Ross J, Dean E 1989 Integrating physiological principles intothe comprehensive management of cardiopulmonary
dysfunction. Physical Therapy 69: 255259Ross J, Dean E 1992 Body positioning. In: Zadai C (ed)Pulmonary management in physical therapy. ChurchillLivingstone, New York
Rubin M 1988 The physiology of bed rest. American Journalof Nursing 88: 5056
Sjostrand T 1951 Determination of changes in theintrathoracic blood volume in man. Acta PhysiologicaScandinavica 22: 116128
Svanberg L 1957 Influence of position on the lung volumes,ventilation and circulation in normals. ScandinavianJournal of Laboratory Investigation 25(suppl): 7175
Verbrugge LM, Jette AM 1993 The disablement process.Social Sciences and Medicine 38: 114
-
7/30/2019 efectosde_la_movilizacion_en_pcte_postrado.
17/17
Ward A, Malloy P, Rippe J 1987 Exercise prescriptionguidelines for normal and cardiac populations.Cardiology Clinics 5: 197210
Warren JB, Turner C, Dalton N, Thomson A, Cochrane GM,Clark TJH 1983 The effect of posture on thesympathoadrenal response to theophylline infusion.
British Journal of Clinical Pharmacology 16: 405411Wasserman K, Whipp BJ 1975 Exercise physiology in healthand disease. American Review of Respiratory Disease112: 219249
Wasserman K, Hansen JE, Sue DY, Whipp BJ 1987 Principlesof exercise testing and interpretation. Lea and Febiger,Philadelphia
Weber KT, Janicki JS, Shroff SG, Likoff MJ 1983 Thecardiopulmonary unit: the bodys gas transport system.Clinics in Chest Medicine 4: 101110
Wenger NK 1982 Early ambulation: the physiologic basisrevisited. Advances in Cardiology 31: 138141
EFFECTS OF POSITIONING AND MOBILIZATION 159
West JB 1962 Regional differences in gas exchange in the lungof erect man. Journal of Applied Physiology 17: 893898
West JB 1977 Ventilation and perfusion relationships.American Review of Respiratory Disease 116: 919943
West JB 1995 Respiratory physiology the essentials.Williams and Wilkins, Baltimore
Williams C 1995 Haemoglobin is more better? NephrologyDialysis and Transplant 2 (suppl): 4855Wolff RK, Dolovich MB, Obminski G, Newhouse MT 1977
Effects of exercise and eucapnic hyperventilation onbronchial clearance in man. Journal of AppliedPhysiology 43: 4650
World Health Organization 1980 International classificationof impairments, disabilities and handicaps. A manual forclassification relating to the consequences of disease.World Health Organization, Geneva
Zack MB, Pontoppidan H, Kazemi H 1974 The effect oflateral positions on gas exchange in pulmonary disease.American Review of Respiratory Disease 110: 4955
FURTHER READING
American College of Sports Medicine 1991 Guidelines forexercise testing and prescription, 4th edn. Lea andFebiger, Philadelphia
Bates DV 1989 Normal pulmonary function. Respiratoryfunction in disease, 3rd edn. WB Saunders, Toronto
Convertino VA 1987 Aerobic fitness, endurance training andorthostatic intolerance. Exercise and Sports SciencesReview 15: 223259
Dantzker DR 1991 Cardiopulmonary critical care, 2nd edn.WB Saunders, Philadelphia
McArdle WD, Katch FI, Katch VL 1996 Exercise physiology.Energy, nutrition and human performance, 4th edn. Leaand Febiger, Philadelphia
Pollack ML, Wilmore JH 1990 Exercise in health and disease,2nd edn. WB Saunders, Philadelphia
Reinhart K, Eyrich K (eds) 1989 Clinical aspects of oxygentransport and tissue oxygenation. Springer-Verlag, London
West JB 1990 Ventilation, blood flow and gas exchange, 5thedn. Blackwell Science, Oxford
West JB 1995 Respiratory physiology: the essentials, 5th edn.Williams and Wilkins, Baltimore