Impacto de múltiples lesiones placentarias en mortalidad ......placentaria única y resultados...
19
Impacto de múltiples lesiones placentarias en mortalidad neonatal, displasia broncopulmonar, y déficit de neurodesarrollo en infantes prematuros Imran N. Mir, Lina F. Chalak, L. Steven Brown, Sarah Johnson-Welch, Roy Heyne, Charles R. Rosenfeld and Vishal S. Kapadia FUNDAMENTO: Determinar la asociación de patología placentaria, incluyendo múltiples lesiones placentarias, con la presencia y severidad de DBP, muerte, y déficit del neurodesarrollo (ND) en infantes PT. MÉTODO: Estudio de cohorte retrospectivo de neonatos <29 semanas de EG nacidos en el Parkland Hospital desde 8/2009 hasta 8/2012. Los infantes se estratificaron como sigue: Grupo 1: sin patología de placenta significativa; Grupo 2: única lesión placentaria significativa; y Grupo 3: ≥2 lesiones placentarias (lesiones múltiples). El resultado primario fue muerte y/o DBP. Se comparó ND a los 2 años de seguimiento. RESULTADOS: En total, 42% (100/241) de los infantes tuvo una sola lesión placentaria, y 34% (82/241) ≥2 lesiones. Con el aumento del número de lesiones patológicas (no lesiones vs. 1 vs. ≥2), la ocurrencia de muerte o DBP aumentó (25%, 37%, y 52% respectivamente; P=0.004). Más aún, los infantes con múltiples lesiones patológicas estuvieron más propensos a tener déficit ND (29%, 29%, y 46%, respectivamente; P=0.03). Después de la regresión logística, los infantes con múltiples lesiones patológicas fueron más propensos a desarrollar DBP moderada-severa (P<0.01; OR 3.9 (1.5- 10.1) pero no ´déficit ND. CONCLUSIONES: Los neonatos <29 sem EG con múltiples lesiones placentarias tienen un riesgo aumentado de desarrollar DBP, sugiriendo una interacción entre inflamación placentaria y patología vascular y la patogénesis de DBP; sin embargo, el riesgo de déficit ND no está aumentado. INTRODUCCIÓN Pese a los progresos en el cuidado obstétrico y neonatal, los infantes prematuros <29 semanas EG continúan con alto riesgo de muerte y discapacidad (1). La DBP es la morbilidad respiratoria crónica más común en infantes prematuros sobrevivientes, con una incidencia reportada de ≈45% en infantes <29sem EG (2). Muchos factores de riesgo potenciales para DBP han sido identificados, incluyendo RCIU, falta de esteroides antenatales, corioamnionitis clínica, EG y PN, sexo del infante, requerimiento prolongado de ventilación mecánica y oxígeno suplementario, y sepsis (3). Los niños con DBP experimentan varios resultados adversos en salud, incluyendo déficits cardiopulmonares crónicos, fallo del crecimiento, déficits visual y auditivo, retraso del ND, y mortalidad postneonatal (3). Notablemente, 15% de los infantes prematuros <29 sem EG también
Transcript of Impacto de múltiples lesiones placentarias en mortalidad ......placentaria única y resultados...

Impacto de múltiples lesiones placentarias en mortalidad neonatal, displasia broncopulmonar, y déficit de neurodesarrollo en infantes prematuros
Imran N. Mir, Lina F. Chalak, L. Steven Brown, Sarah Johnson-Welch, Roy Heyne, Charles R. Rosenfeld and Vishal S. Kapadia
FUNDAMENTO: Determinar la asociación de patología placentaria, incluyendo múltiples lesiones placentarias, con la presencia y severidad de DBP, muerte, y déficit del neurodesarrollo (ND) en infantes PT.
MÉTODO: Estudio de cohorte retrospectivo de neonatos <29 semanas de EG nacidos en el Parkland Hospital desde 8/2009 hasta 8/2012. Los infantes se estratificaron como sigue: Grupo 1: sin patología de placenta significativa; Grupo 2: única lesión placentaria significativa; y Grupo 3: ≥2 lesiones placentarias (lesiones múltiples). El resultado primario fue muerte y/o DBP. Se comparó ND a los 2 años de seguimiento.
RESULTADOS: En total, 42% (100/241) de los infantes tuvo una sola lesión placentaria, y 34% (82/241) ≥2 lesiones. Con el aumento del número de lesiones patológicas (no lesiones vs. 1 vs. ≥2), la ocurrencia de muerte o DBP aumentó (25%, 37%, y 52% respectivamente; P=0.004). Más aún, los infantes con múltiples lesiones patológicas estuvieron más propensos a tener déficit ND (29%, 29%, y 46%, respectivamente; P=0.03). Después de la regresión logística, los infantes con múltiples lesiones patológicas fueron más propensos a desarrollar DBP moderada-severa (P<0.01; OR 3.9 (1.5- 10.1) pero no ´déficit ND.
CONCLUSIONES: Los neonatos <29 sem EG con múltiples lesiones placentarias tienen un riesgo aumentado de desarrollar DBP, sugiriendo una interacción entre inflamación placentaria y patología vascular y la patogénesis de DBP; sin embargo, el riesgo de déficit ND no está aumentado.
INTRODUCCIÓN
Pese a los progresos en el cuidado obstétrico y neonatal, los infantes prematuros <29 semanas EG continúan con alto riesgo de muerte y discapacidad (1). La DBP es la morbilidad respiratoria crónica más común en infantes prematuros sobrevivientes, con una incidencia reportada de ≈45% en infantes <29sem EG (2). Muchos factores de riesgo potenciales para DBP han sido identificados, incluyendo RCIU, falta de esteroides antenatales, corioamnionitis clínica, EG y PN, sexo del infante, requerimiento prolongado de ventilación mecánica y oxígeno suplementario, y sepsis (3). Los niños con DBP experimentan varios resultados adversos en salud, incluyendo déficits cardiopulmonares crónicos, fallo del crecimiento, déficits visual y auditivo, retraso del ND, y mortalidad postneonatal (3). Notablemente, 15% de los infantes prematuros <29 sem EG también

desarrollan PC y aproximadamente la mitad desarrollarán anormalidades en la cognición, desarrollo del lenguaje, y comportamiento (4).
La placenta juega un papel crucial en mantener el bienestar fetal, crecimiento, y desarrollo durante la gestación (5). La evidencia de insultos antenatales en la placenta se correlaciona con morbilidades y mortalidad en infantes prematuros, pero la evidencia es conflictiva acerca de la asociación entre diferentes patologías placentarias y los resultados neonatales (6, 7). Muchos estudios han estado limitados por una muestra pequeña, sesgo de selección, y uso de diferentes definiciones para varias patologías placentarias, resultando en una variedad de clasificaciones. Más aún, la mayoría de los estudios han descrito una asociación entre una lesión patológica placentaria única y resultados neonatales, ej. Corioamnionitis histológica aguda (CHA) y DBP, mala perfusión vascular materna (MVU) y DBP, etc (8-10). Recientemente, Chisholm et al. (11) publicaron una detallada revisión de patología placentaria y morbilidades neonatales asociadas en las cuales ellos notaron una asociación entre la patología placentaria con morbilidades neonatales, incluyendo DBP; sin embargo, no corrigieron para múltiples lesiones patológicas de la placenta y no examinaron déficit ND. Mestan et al. (12) emplearon la clasificación de Redline para lesiones patológicas placentarias y reportaron que los cambios patológicos en la placenta de la MPV están asociados con DBP y HPPN en infantes prematuros. No corrigieron para múltiples lesiones patológicas de la placenta, por ej. La presencia de ≥2 lesiones patológicas. Por tanto la presencia de múltiples lesiones placentarias y su asociación con los resultados en prematuros sigue sin conocerse. Nuestra hipótesis es que lesiones patológicas múltiples placentarias están asociadas con DBP y déficit ND (DND) en infantes prematuros < 29 sem EG. Los objetivos de este estudio fueron (1) determinar la asociación de la patología placentaria con muerte neonatal, DBP, y subsiguiente DND en infantes prematuros empleando una clasificación uniforme de histopatología placentaria, (2) describir la incidencia de múltiples lesiones placentarias, y (3) determinar si la presencia está asociada con la ocurrencia de muerte neonatal, DBP, y DND.
MATERIAL Y MÉTODOS
Diseño del estudio
Estudio retrospectivo de cohorte conducido en Parkland Hospital, Dallas, TX entre Agosto 2009 y Agosto 2012 en infantes prematuros <29 sem EG. El estudio fue aprobado por los Comités de Revisión del Hospital Parkland y el Southwestern Medical center de la Universidad de Texas. Todos los infantes prematuros nacidos entre 23 0/7 y 28 6/7 sem EG durante el período de estudio fueron identificados en el Registro de UCIN de Parkland. Los infantes que recibieron cuidado de confort planeado en la sala de partos y aquellos con anomalías congénitas o anormalidades cromosómicas fueron excluidos.
Patología de la placenta
Las placentas de todos los partos prematuros en el Hospital Parkland son enviadas rutinariamente para examen macro e histológico por un patólogo de placentas de acuerdo al protocolo vigente brevemente descripto (13). Se realizó el examen macroscópico inicial de cordón umbilical,

membranas, y disco placentario. Luego de remover el cordón umbilical, las membranas fetales, y coágulos de sangre no adherentes, se obtuvo el peso de la placenta. El disco placentario fue seccionado cada 1-2 cm y examinado para lesiones intraparenquimatosas. Secciones representativas del cordón umbilical, membranas fetales, parénquima placentario, y cualquier anormalidad observada en el examen macro fueron enviadas para examen histológico estándar. Durante el período que se recopilaban los casos del estudio, los patólogos de nuestra institución emplearon la clasificación Redline para describir los hallazgos mayores (14). La definición a priori de “patología placentaria significativa” fue determinada por un patólogo independiente ciego a la información sobre la salud del paciente, incluyendo los resultados clínicos. Esta definición está estandarizada en nuestra institución y excluye la patología placentaria menor en cada categoría mayor de patologías placentarias que tienen poca o ninguna consecuencia clínica y se considera que están presentes en la mayoría de los exámenes histopatológicos de los neonatos normales a término. La definición de “patología de placenta significativa” está basada en la clasificación Redline modificada que recientemente publicamos (15). Esto incluye las siguientes patologías placentarias: (1) CHA- respuesta inflamatoria materna: presencia de respuestas inflamatorias maternas (subcorionitis aguda o corioamnionitis aguda); CHA- respuesta inflamatoria fetal (vasculitis en los vasos umbilicales y/o en los vasos de la placa coriónica). (2) Villitis de Alto grado: villitis crónica en parches o difusa con o sin vasculopatía fetal obliterativa; se definió villitis crónica como la presencia de inflamación crónica de las vellosidades coriónicas. Lesiones de alto grado incluyeron focos inflamatorios comprometiendo >10 focos/vellosidades, ya sea en distribución limitada (parches) o más extensa (difusa). (3) MVU: MVU fue definida por hipoplasia vellositaria distal, vasculopatía severa de la decidua materna (necrosis fibrinoide y/o cambios agudos ateromatosos), y/o infartos comprometiendo >20% del volumen placentario. (4) Vasculopatía trombótica fetal (FTV): las dos variables de trombos de vasos grandes y daño de vellosidades por perfusión fetal reducida (vellosidad avascular o cariorrexis vascular del estroma de la vellosidad) fueron agrupados bajo la denominación de FTV. (5) Placentas PEG/ GEG: el peso placentario <percentilo 10 para la EG fue definido como placenta PEG y el percentilo >90 para EG fue definido como grande- GEG (16). La presencia de alguna de las 6 lesiones descriptas fue considerada como patología placentaria significativa. La presencia de más de una de las lesiones placentarias definidas fue clasificada como patología placentaria múltiple. Hemos reportado previamente 100% de concordancia entre el reporte de rutina de patología placentaria y la revisión independiente de la placenta por un patólogo infantil cegado (16). Todos los reportes de patología placentaria fueron revisados por un patólogo infantil y un neonatólogo (SJ.-W y I.N.M.), que estaban cegados para la historia clínica y resultados. Los pacientes del estudio estuvieron divididos en tres grupos basados en la patología placentaria: (1) Sin patología placentaria, (2) Una sola patología placentaria significativa, y (3) Múltiples lesiones patológicas placentarias (presencia de ≥2 lesiones significativas).
Recolección de datos
Se compararon las características basales maternas y del infante, morbilidades, y mortalidad. Además del examen del registro electrónico de datos, también se obtuvieron datos de la Base de

la UCIN del Hospital Parkland, que contiene datos recolectados prospectivamente de todos los RN ingresados a UCIN por >30 años y ha sido validada. Se definió ruptura prematura de membranas (RPM) a la producida ≥18 horas antes del nacimiento. Se empleó la definición del panel de expertos de NICHD para la definición clínica de corioamnionitis (17). RCIU se definió como índice ponderal en percentilo <10 para EG.
Resultados clínicos a corto plazo neonatal
Se recolectaron de la base de datos de UCIN durante la estadía en UCIN las morbilidades incluyendo SDR, DBP, sepsis, HIV severa, ECN, duración de la hospitalización, y muerte. Se definió DBP como requerimiento persistente de O2 por >28 días. DBP moderada-severa se definió por la necesidad de O2 suplementario a las 36 semanas de edad postmenstrual (2). Se registró sepsis si el hemocultivo era positivo para un organismo patógeno ≤72 hrs de nacido (sepsis precoz) y >72 hrs después de nacer (tardía). HIV severa fue definida como Grado III uni o bilateral o mayor en cualquier ecografía cerebral obtenida durante la internación (18). ECN fue definida como Estadio ≥2 según los criterios de Bell modificados (19).
Evaluación de ND
Los neonatos <29 sem EG pasan por evaluaciones neurológicas rutinarias estandarizadas sistemáticas y con Bayley III a los 22-26 meses de EC en nuestra clínica de seguimiento ambulatorio (4, 20). DND moderado-severo se definió como la presencia de alguno de los siguientes: PC con score GMFCS ≥2, score cognitivo o motor de Bayley <85, déficit visual o pérdida auditiva permanente que no permita al niño comprender las indicaciones del examinador y comunicarse con o sin amplificación. DND severo fue definido con alguno de los siguientes: PC severa con score GMFCS ≥4, score cognitivo y motor de Bayley <70, ceguera bilateral o déficit auditivo bilateral +/- amplificación (4).
Medidas de resultado
El resultado primario del estudio fue el compuesto muerte y/o DBP. Resultados secundarios pre-especificados incluyeron muerte, HIV severa, DBP, ECN, DND moderado-severo, DND severo, y componentes individuales de la evaluación del ND.
Estas medidas de resultado clínico fueron elegidas para el análisis dado que la patología placentaria ha sido previamente asociada con estas morbilidades (5).
Análisis estadístico
Se utilizó SPSS versión 19 (IBM) para realizar el análisis estadístico. Se calcularon estadísticas descriptivas para comparar los neonatos de los tres grupos de patología placentaria descriptos más arriba. Las variables categóricas fueron analizadas con Chi- cuadrado para tendencias. Las variables continuas fueron analizadas con ANOVA. Un nivel de significancia de 0.05 fue empleado para todos los análisis. En caso de un resultado significativo en ANOVA, se empleó posteriormente el procedimiento de comparación múltiple con corrección de Bonferroni para grupos separados.

Para los resultados DBP y DND, se hizo regresión logística para determinar confusores. Junto a aquellas variables pre-especificadas conocidas como asociadas con los resultados de interés, todas las variables con p<0.1 fueron incluidas en la regresión logística. Variables confundidoras para DBP incluyeron EG, PN, sexo, corticoides antenatales, y administración de surfactante. Para los resultados de ND, incluímos EG, sexo, corticoides antenatales, y administración de magnesio antenatal en la regresión logística.
RESULTADOS
Población del estudio
Durante el período de estudio, 251 neonatos nacieron a las 23-28.6 sem EG. Después de excluir a los RN que recibieron cuidados de confort o nacidos con anomalías congénitas o anormalidades cromosómicas, fueron incluidos 241 (Fig. 1). No se observaron diferencias en las características maternas entre los 3 grupos. 24% (59/241) de los infantes no presentaron patología placentaria (Grupo 1), 41% (100/241) tuvo una sola lesión placentaria patológica (Grupo 2), y 34% (82/241) lesiones múltiples (Grupo 3, Tabla 1). Los neonatos con patología placentaria tuvieron menor EG, PN más bajo, y score de Apgar al minuto (Tabla 1). Sólo 12% (28/241) de infantes se perdieron en el seguimiento a largo plazo (Fig.1).
Distribución de lesiones patológicas placentarias
La lesión patológica más común fue la corioamnionitis aguda, ocurriendo en 49% de neonatos, con vasculitis fetal en 32%. La segunda lesión placentaria más común fue MVU (20%). Un número importante de placentas fueron PEG (20%); sin embargo, 77% no mostró evidencia de MVU.

Dieciséis por ciento de las placentas fueron GEG, y 77% de ellos mostraron signos histológicos de corioamnionitis. En infantes con lesiones patológicas múltiples (34%), la combinación más común fue GEG+corioamnionitis [n=30, 12%], seguidos por PEG con corioamnionitis [n=15, 6%] y MVU+ corioamnionitis [n=11, 5%] (Fig.2).
La asociación de patologías placentarias múltiples con DBP y DND
Ninguna lesión placentaria individual estuvo significativamente asociada con muerte neonatal, DBP, o DND. Sin embargo, a medida que el número de lesiones patológicas placentarias aumentó (0 lesión vs. 1 lesión vs. ≥2 lesiones), la ocurrencia de DBP aumentó desde 35% a 49% y 65% respectivamente; (P= 0.002). Esto fue también verdad para la ocurrencia de DBP moderada/severa y muerte o DBP (P0 0.004) (Tabla 2). Notablemente, la incidencia de muerte o DBP fue también más alta en los infantes prematuros con lesiones múltiples (P= 0.004), y ellos pasaron más días en VM (P<0.01), oxígeno (P<0.001), y en el hospital (P= 0.009) (Tabla 2). Después de ajustar por EG, PN, género, uso de corticoides antenatales, y administración de surfactante, los infantes con múltiples lesiones patológicas fueron más propensos a desarrollar DBP moderada-severa (OR 3.9 [1.5-10.1], P<0.01). Cuando se examinó el seguimiento, los infantes con múltiples lesiones patológicas fueron dos veces más propensos a presentar DND en el análisis bivariado (P= 0.03) (Tablas 3 y 4). Sin embargo, después de ajustar por EG, género, uso de esteroides antenatales, y administración de magnesio antenatal, las lesiones placentarias patológicas múltiples no continuaron asociadas con DND (OR 1.6 [0.7-3.7], P= 0.28).
DISCUSIÓN
Evidencia creciente sugiere que la ocurrencia de eventos prenatales resultantes en alteración de la histología placentaria y presencia de lesiones patológicas placentarias puede estar relacionada o asociada con la ocurrencia de subsiguiente morbilidad neonatal y DND (5). En este estudio, empleando la clasificación uniforme Redline, 75% de los infantes prematuros tuvieron evidencia de al menos una patología placentaria y 34% tuvieron múltiples lesiones. Pese a que ninguna lesión placentaria individual estuvo asociada con la ocurrencia de DBP, la presencia de múltiples lesiones estuvo significativamente asociada con muerte o la ocurrencia de DBP. Más aún, los infantes prematuros con múltiples patologías placentarias estuvieron más propensos a desarrollar DND, pero esto no fue significativo después de ajustar por potenciales confundidores.
La asociación entre DBP y la presencia de varias patologías placentarias tales como MVU, FTV, vellositis crónica, edema de vellosidades, y corioamnionitis aguda ha sido inconsistente (5, 8, 9, 12, 21-24).

Por ejemplo, MVU es una lesión histopatológica asociada con pre-eclampsia y otros desórdenes hipertensivos de la gestación que llevan a insuficiencia útero-placentaria. Mientras que algunos han reportado relación inversa entre MVU y DBP (21), otros han reportado que MVU está asociada con la severidad de la DBP y PAH (12). Igualmente, el rol de CHA y DBP también ha sido controvertido; algunos estudios no han mostrado asociación con DBP (21-24), mientras que otros han reportado una asociación entre AHC y desarrollo de DBP (8, 9). Esto podría reflejar la falta de

documentación de las múltiples lesiones patológicas placentarias. A pesar de que no encontramos ninguna lesión individual significativamente asociada con la ocurrencia de DBP, la presencia de múltiples lesiones patológicas placentarias estuvo fuertemente asociada con la ocurrencia de DBP-
La combinación más común de lesiones en las placentas con lesiones múltiples fueron GEG+corioamnionitis, seguida de PEG+ corioamnionitis y MVU+ corioamnionitis. Una posible hipótesis vascular explicando esta asociación sugiere que la patología placentaria tal como MVU resulta en insuficiencia placentaria que a su vez puede llevar a: (1) disminución de factores angiogénicos tales como factores de crecimiento placentario y factor A de crecimiento endotelial vascular (VEGF-S) (25, 26), (2) exceso de factores anti-angiogénicos en líquido amniótico tales como el antagonista del receptor VEGF gms-símil tirokinasa-1 (27), y (3) subsiguiente hipoxia fetal crónica (28). Estos factores también pueden resultar en disrupción del crecimiento/desarrollo vascular pulmonar y alveolización (28). Notablemente, la presencia de hipoxia crónica fetal en ovejas que está asociada a MVU y el desarrollo de insuficiencia placentaria lleva a los hallazgos clásicos histológicos de DBP (29). La hipótesis alternativa de inflamación para la ocurrencia de DBP sugiere que la corioamnionitis resulta en una respuesta inflamatoria sistémica fetal causando

expresión pulmonar aumentada de citoquinas proinflamatorias, apoptosis, y remodelación de los pulmones fetales (30, 31). Notablemente, esta inflamación también puede estar asociada con respuestas atenuadas a tratamiento con surfactante exógeno y entonces la necesidad de ventilación mecánica prolongada (32). La colonización con Ureaplasma urealyticum o Ureaplasma pravum o riesgo aumentado de sepsis postnatal también pueden contribuir al desarrollo de DBP en infantes prematuros con corioamnionitis aguda histológica en el examen placentario (33). Especulamos que la asociación de DBP con múltiples lesiones placentarias, pero no con patología aislada, sugiere que hay efectos interactivos entre los procesos vasculares e inflamatorios que promueven el desarrollo de DBP. Esto es especialmente relevante dado que no todos los infantes prematuros expuestos a corioamnionitis o a MVU desarrollan DBP. Por lo tanto, es posible que insultos múltiples/severos tengan que ocurrir en el curso de la gestación, más que un evento aislado, para que aumente el riesgo de desarrollar DBP en neonatos <29 sem EG.
Este es el primer estudio que ha explorado la asociación de múltiples lesiones patológicas placentarias con los datos del ND empleando Bayley III. Similar a la DBP, los estudios han sido realizados para mostrar asociación entre DND y varias patologías placentarias, incluyendo corioamnionitis, MVU, FTV, y villitis crónica pero estas asociaciones han sido inconsistentes (10, 34-36). Por ejemplo, pese a que la asociación entre CHA y resultados adversos en el ND ha sido estudiada, la asociación es bastante variable, con algunos reportando que AHC es predictor significativo de PC (34) y DND (10), mientras que otros no reportan asociación entre CHA y resultado ND (35). Igualmente, hay pocos estudios que hayan examinado MVU y NDI (36). Se ha sugerido que MVU puede llevar a hipoxia fetal, que contribuye a la ruptura de la barrera hematoencefálica y dispara la excitoxicidad al glutamato. Los radicales libres en combinación con una falta del desarrollo de enzimas antioxidantes en los oligodendrocitos pueden explicar el impacto de la hipoxia en el cerebro prematuro (37). Mientras que ha sido reportada asociación significativa entre el infarto placentario (sugiriendo MVU) y DND (38), eso no ha sido observado por otros (39). Esta variabilidad en estudios previos puede, en parte, estar basada en una falta de poder estadístico, análisis retrospectivo, y diferencias en el momento de las evaluaciones del ND. Más aún, ninguno de estos estudios evaluó lesiones múltiples. En nuestro estudio, los infantes con múltiples lesiones patológicas de la placenta fueron más propensos a presentar DND moderado-severo; sin embargo, después de ajustar por potenciales confusores, esta asociación despareció. Como en DBP, es posible que exista un efecto interactivo entre las lesiones vascular e inflamatoria de la placenta en la ocurrencia de la injuria cerebral, pero es necesaria una cohorte mayor para explorar esta asociación.
Las fortalezas de nuestro estudio incluyen una cohorte amplia con muestreo consecutivo para disminuir el sesgo de selección, relativa homogeneidad de los sujetos de estudio nacidos y asistidos en un solo centro, alta tasa de seguimiento ≈90% con examen sistemático de resultados a largo plazo, y disponibilidad de histopatología de la placenta en todos los infantes prematuros nacidos en nuestra institución. También examinamos una gran variedad de lesiones placentarias, definidas su significancia a priori, empleamos un método uniforme de clasificación, y examinamos lesiones múltiples. Nuestro estudio tuvo algunas limitaciones tales como su enfoque retrospectivo.

Aunque la regresión logística fue hecha para valorar variables conocidas, es posible que confundidores desconocidos no estén considerados. No registramos datos acerca de neumonía asociada a respirador (NAR) y el score SNAPPE. , porque estos datos no son recolectados rutinariamente en nuestra institución. Es muy posible que las lesiones múltiples placentarias no sólo indiquen una interacción entre lesiones tipo vascular e inflamatoria pero también pueden

indicar severidad del insulto vascular o inflamatorio. Estudios futuros deberían explorar el rol de esas lesiones y la interacción en la patogénesis de morbilidades neonatales.
Hasta donde sabemos, este es el primer reporte demostrando una asociación entre la presencia de múltiples lesiones placentarias, DBP, y su severidad en neonatos <29 semanas EG, demostrando la importancia de la patología de rutina en placenta y el reporte de lesiones múltiples. Especulamos que puede haber una interacción entre la patogénesis de lesiones vasculares e inflamación placentaria que contribuya al desarrollo de DBP y su severidad. La asociación con patología placentaria debería ser incluida en futuros modelos predictivos de DBP, y debieran diseñarse extensos estudios clínicos prospectivos animales para determinar cómo varias patologías placentarias interactúan y su rol en el desarrollo de morbilidades neonatales.
REFERENCES
1. Glass, H. C. et al. Outcomes for extremely premature infants. Anesth. Analg. 120, 1337–1351 (2015). 2. Stoll, B. J. et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993-2012. JAMA 314, 1039–1051 (2015). 3. Jensen, E. A. & Schmidt, B. Epidemiology of bronchopulmonary dysplasia. Birth Defects Res. A Clin. Mol. Teratol. 100, 145–157 (2014). 4. Vohr, B. R. et al. Are outcomes of extremely preterm infants improving? Impact of Bayley assessment on outcomes. J. Pediatr. 161, 222.e3–228.e3 (2012). 5. Roescher, A. M., Timmer, A., Erwich, J. J. & Bos, A. F. Placental pathology, perinatal death, neonatal outcome, and neurological development: a systematic review. PLoS ONE 9, e89419 (2014). 6. Roescher, A. M. et al. Placental pathology and neurological morbidity in preterm infants during the first two weeks after birth. Early Hum. Dev. 90, 21–25 (2014). 7. Ogunyemi, D., Murillo, M., Jackson, U., Hunter, N. & Alperson, B. The relationship between placental histopathology findings and perinatal outcome in preterm infants. J. Matern. Fetal Neonatal Med. 13, 102–109 (2003). 8. Lee, H. J. et al. Chorioamnionitis, respiratory distress syndrome and bronchopulmonary dysplasia in extremely low birth weight infants. J. Perinatol. 31, 166–170 (2011). 9. Kunjunju, A. M., Gopagondanahalli, K. R., Chan, Y. & Sehgal, A. Bronchopulmonary dysplasia-associated pulmonary hypertension: clues from placental pathology. J. Perinatol. 37, 1310–1314 (2017). 10. Pappas, A. et al. Chorioamnionitis and early childhood outcomes among extremely low-gestational-age neonates. JAMA Pediatr. 168, 137–147 (2014). 11. Chisholm, K. M. et al. Correlation of preterm infant illness severity with placental histology. Placenta 39, 61–69 (2016). 12. Mestan, K. K. et al. Placental pathologic changes of maternal vascular underperfusion in bronchopulmonary dysplasia and pulmonary hypertension. Placenta 35, 570–574 (2014). 13. Greer, L. G. et al. An immunologic basis for placental insufficiency in fetal growth restriction. Am. J. Perinatol. 29, 533–538 (2012). 14. Redline, R. W., Heller, D., Keating, S. & Kingdom, J. Placental diagnostic criteria and clinical correlation-a workshop report. Placenta 26(Suppl A), S114–S117 (2005). 15. Mir, I. N. et al. Placental pathology is associated with severity of neonatal encephalopathy and adverse developmental outcomes following hypothermia. Am. J. Obstet. Gynecol. 213, 849.e1–849.e7 (2015). 16. Pinar, H., Sung, C. J., Oyer, C. E. & Singer, D. B. Reference values for singleton and twin placental weights. Pediatr. Pathol. Lab. Med. 16, 901–907 (1996). 17. Higgins, R. D. et al. Evaluation and management of women and newborns with a maternal diagnosis of chorioamnionitis: summary of a workshop. Obstet. Gynecol. 127, 426–436 (2016). 18. Papile, L.-A., Burstein, J., Burstein, R. & Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J. Pediatr. 92, 529–534 (1978). 19. Bell, M. J. et al. Neonatal necrotizing enterocolitis - therapeutic decisions based upon clinical staging. Ann. Surg. 187, 1–7 (1978). 20. Albers, C. A. & Grieve, A. J. Test Review: Bayley, N. (2006). Bayley Scales of Infant and Toddler Development–Third Edition. San Antonio, TX: Harcourt Assessment. J. Psychoeduc. Assess. 25, 180–198 (2007).

21. Redline, R. W., Wilson-Costello, D. & Hack, M. Placental and other perinatal risk factors for chronic lung disease in very low birth weight infants. Pediatr. Res. 52, 713–719 (2002). 22. Kent, A. & Dahlstrom, J. E. Chorioamnionitis/funisitis and the development of bronchopulmonary dysplasia. J. Paediatr. Child Health 40, 356–359 (2004). 23. Van Marter, L. J. et al. Chorioamnionitis, mechanical ventilation, and postnatal sepsis as modulators of chronic lung disease in preterm infants. J. Pediatr. 140, 171–176 (2002). 24. Hartling, L., Liang, Y. & Lacaze-Masmonteil, T. Chorioamnionitis as a risk factor for bronchopulmonary dysplasia: a systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 97, F8–F17 (2012). 25. Abman, S. H. Bronchopulmonary dysplasia: “a vascular hypothesis”. Am. J. Respir. Crit. Care Med. 164(Pt 1), 1755–1756 (2001). 26. Thebaud, B. & Abman, S. H. Bronchopulmonary dysplasia: where have all the vessels gone? Roles of angiogenic growth factors in chronic lung disease. Am. J. Respir. Crit. Care Med. 175, 978–985 (2007). 27. Tang, J. R., Karumanchi, S. A., Seedorf, G., Markham, N. & Abman, S. H. Excess soluble vascular endothelial growth factor receptor-1 in amniotic fluid impairs lung growth in rats: linking preeclampsia with bronchopulmonary dysplasia. Am. J. Physiol. Lung Cell. Mol. Physiol. 302, L36–L46 (2012). 28. Strouss, L., Goldstein, N. D., Locke, R. & Paul, D. A. Vascular placental pathology and the relationship between hypertensive disorders of pregnancy and neonatal outcomes in very low birth weight infants. J. Perinatol. 38, 324–331 (2018). 29. Rozance, P. J. et al. Intrauterine growth restriction decreases pulmonary alveolar and vessel growth and causes pulmonary artery endothelial cell dysfunction in vitro in fetal sheep. Am. J. Physiol. Lung Cell. Mol. Physiol. 301, L860–L871 (2011). 30. Ghezzi, F. et al. Elevated interleukin-8 concentrations in amniotic fluid of mothers whose neonates subsequently develop bronchopulmonary dysplasia. Eur. J. Obstet. Gynecol. Reprod. Biol. 78, 5–10 (1998). 31. Yoon, B. H. et al. Amniotic fluid cytokines (interleukin-6, tumor necrosis factoralpha, interleukin-1 beta, and interleukin-8) and the risk for the development of bronchopulmonary dysplasia. Am. J. Obstet. Gynecol. 177, 825–830 (1997). 32 Been, J. V. et al. Chorioamnionitis alters the response to surfactant in preterm infants. J. Pediatr. 156, 10.e1–15.e1 (2010). 33. Schelonka, R. L., Katz, B., Waites, K. B. & Benjamin, D. K. Jr Critical appraisal of the role of Ureaplasma in the development of bronchopulmonary dysplasia with metaanalytic techniques. Pediatr. Infect. Dis. J. 24, 1033–1039 (2005). 34. Wu, Y. W. & Colford, J. M. Jr Chorioamnionitis as a risk factor for cerebral palsy: a meta-analysis. JAMA 284, 1417–1424 (2000). 35. Andrews, W. W. et al. Early preterm birth: association between in utero exposure to acute inflammation and severe neurodevelopmental disability at 6 years of age. Am. J. Obstet. Gynecol. 198, 466.e1–466.e11 (2008). 36. Vinnars, M. T., Vollmer, B., Nasiell, J., Papadogiannakis, N. & Westgren, M. Association between cerebral palsy and microscopically verified placental infarction in extremely preterm infants. Acta Obstet. Gynecol. Scand. 94, 976–982 (2015). 37. Rezaie, P. & Dean, A. Periventricular leukomalacia, inflammation and white matter lesions within the developing nervous system. Neuropathology 22, 106–132 (2002). 38. Blair, E., de Groot, J. & Nelson, K. B. Placental infarction identified by macroscopic examination and risk of cerebral palsy in infants at 35 weeks of gestational age and over. Am. J. Obstet. Gynecol. 205, 124.e1–124.e7 (2011). 39. Leviton, A. et al. Microbiologic and histologic characteristics of the extremely preterm infant's placenta predict white matter damage and later cerebral palsy. the ELGAN study. Pediatr. Res. 67, 95–101 (2010).

CLINICAL RESEARCH ARTICLE
Impact of multiple placental pathologies on neonatal death,bronchopulmonary dysplasia, and neurodevelopmentalimpairment in preterm infantsImran N. Mir1, Lina F. Chalak1, L. Steven Brown2, Sarah Johnson-Welch3, Roy Heyne1, Charles R. Rosenfeld1 and Vishal S. Kapadia1
BACKGROUND: To determine the association of placental pathology, including multiple placental lesions, with the occurrence andseverity of bronchopulmonary dysplasia (BPD), death, and neurodevelopmental impairment (NDI) in preterm infants.METHOD: A retrospective cohort study of neonates <29 weeks gestational age (GA) born at Parkland Hospital from 08/2009 to 08/2012. Infants were stratified as follows: Group 1: no significant placental pathology; Group 2: single significant placental lesion; andGroup 3: ≥2 placental lesions (multiple lesions). Primary outcome was death and/or BPD. Two-year neurodevelopmental follow-upwas compared.RESULTS: In all, 42% (100/241) of infants had one placental lesion, and 34% (82/241) ≥2 lesions. As the number of the pathologiclesions increased (no lesions vs. 1 vs. ≥2), the occurrence of death or BPD increased (25%, 37%, and 52%, respectively; P= 0.004).Moreover, infants with multiple pathologic lesions were more likely to have NDI (29%, 29%, and 46%, respectively; P= 0.03). Afterlogistic regression, infants with multiple pathologic lesions were more likely to develop moderate-to-severe BPD [P < 0.01; OR 3.9(1.5–10.1)] but not NDI.CONCLUSION(S): Neonates <29 weeks GA with multiple placental pathologic lesions have an increased risk for developing BPD,suggesting an interaction between placental inflammation and vascular pathology and the pathogenesis of BPD; however, the riskof NDI is not increased.
Pediatric Research _#####################_ ; https://doi.org/10.1038/s41390-019-0715-y
INTRODUCTIONDespite improvements in obstetric and neonatal care, preterminfants <29 weeks gestational age (GA) remain at high risk fordeath and disability.1 Bronchopulmonary dysplasia (BPD) is themost common chronic respiratory morbidity in surviving preterminfants, with a reported incidence of ~45% in infants <29 weeksGA.2 Many potential risk factors for BPD have been identified,including intrauterine growth restriction, lack of antenatal steroids,clinical chorioamnionitis, GA and birth weight, sex of the infant,prolonged need for mechanical ventilation and supplementaloxygen, and sepsis.3 Children with BPD experience several adversehealth outcomes, including chronic cardiopulmonary impairments,growth failure, hearing and vision deficits, neurodevelopmentaldelay, and post-neonatal mortality.3 Notably, 15% of preterminfants <29 weeks GA also develop cerebral palsy and approxi-mately half will develop abnormalities in cognition, languagedevelopment, and behavior.4
The placenta plays a crucial role in maintaining fetal well-being,growth, and development during pregnancy.5 Placental evidenceof antenatal insults correlates with morbidities and mortalityin preterm infants, but there is conflicting evidence of anassociation between different placental pathologies and neonataloutcomes.6,7 Many studies have been limited by small sample size,selection bias, and use of different definitions for various placentalpathologies, resulting in a range of classifications. Moreover, most
of the studies have described an association between a singleplacental pathology lesion and neonatal outcomes, e.g., acutehistologic chorioamnionitis (AHC) and BPD, maternal vascularunderperfusion (MVU) and BPD, etc.8–10 Recently, Chisholm et al.11
have provided a detailed review of placental pathology andassociated neonatal morbidities in which they noted an associa-tion between placental pathology with neonatal morbidities,including BPD; however, they did not correct for multipleplacental pathologic lesions and did not examine neurodevelop-mental impairment (NDI). Mestan et al.12 used the Redlineclassification for placental pathologic lesions and reported thatplacental pathologic changes of MVU are associated with BPD andpulmonary arterial hypertension (PAH) in preterm infants. They didnot correct for multiple placental pathologic lesions, i.e., thepresence of ≥2 pathologic lesions. Thus the presence of multipleplacental lesions and its association with preterm outcomesremain unknown. We hypothesize that multiple placentalpathologic lesions are associated with BPD and NDI in preterminfants born <29 weeks GA. The objectives of this study were to (1)determine the association of placental pathology with neonataldeath, BPD, and subsequent NDI in preterm infants using auniform classification of placental histopathology, (2) describe theincidence of multiple placental lesions, and (3) determine whethertheir presence is associated with the occurrence of neonataldeath, BPD, and NDI.
Received: 10 June 2019 Revised: 13 November 2019 Accepted: 18 November 2019
1Division of Neonatal-Perinatal Medicine, Department of Pediatrics, UT Southwestern Medical School, Dallas, TX 75390, USA; 2Parkland Health and Hospital Systems, UTSouthwestern Medical School, Dallas, TX 75390, USA and 3Department of Pathology, UT Southwestern Medical School, Dallas, TX 75390, USACorrespondence: Imran N. Mir ([email protected])
www.nature.com/pr
© International Pediatric Research Foundation, Inc. 2019
1234567890();,:

MATERIALS AND METHODSStudy designA retrospective cohort study was conducted at Parkland Hospital,Dallas, TX between August 2009 and August 2012 in preterminfants <29 weeks GA. The study was approved by the Universityof Texas Southwestern Medical Center and Parkland Hospital andHealth Systems Institutional Review Boards. All preterm neonatesborn 23 0/7 to 28 6/7 weeks GA during the study period wereidentified in the Parkland Neonatal Intensive Care Unit (NICU)Registry. Infants receiving planned comfort care in the deliveryroom and those born with congenital anomalies or chromosomalabnormalities were excluded.
Placental pathologyPlacentas from all preterm births at Parkland Hospital are routinelysubmitted for gross and histologic examination by a placentalpathologist according to a standing protocol as described briefly.13
Initial gross examination of the umbilical cord, membranes, andplacental disc was performed. Placental weight was obtained afterremoval of the umbilical cord, fetal membranes, and non-adherentblood clots. The placental disk was sectioned at 1–2-cm intervalsand examined for intraparenchymal lesions. Representativesections of the umbilical cord, fetal membranes, placentalparenchyma, and any abnormalities seen on gross examinationwere submitted for standard histological examination. During thetime that study cases were accumulated, the pathologists at ourinstitution used the Redline classification to describe majorplacental findings.14 The a priori definition of “significant placentalpathology” was determined by an independent pathologistblinded to patient health information, including the clinicaloutcomes. This definition is standardized at our institution andexcludes minor placental pathology in each major category ofplacental pathologies that have little or no clinical consequenceand are considered to be present in most of the placentalhistologic examinations of normal term neonates. The definition of“significant placental pathology” is based on modified Redlineclassification that we recently published.15 This includes thefollowing placental pathologies: (1) AHC—maternal inflammatoryresponse: presence of maternal inflammatory responses (acutesubchorionitis or acute chorioamnionitis); AHC—fetal inflammatoryresponse (vasculitis in the umbilical vessels and/or chorionic platevessels). (2) High-grade villitis: patchy/diffuse chronic villitis with orwithout obliterative fetal vasculopathy; chronic villitis was definedas the presence of chronic inflammation of chorionic villi. High-grade lesions included inflammatory foci involving >10 villi/focus,either limited in distribution (patchy) or more extensive (diffuse).(3) MVU: MVU was defined by distal villous hypoplasia, severematernal decidual vasculopathy (fibrinoid necrosis and/or acuteatheromatous changes), and/or infarcts involving >20% of theplacental volume. (4) Fetal thrombotic vasculopathy (FTV): the twovariables of large vessel thrombi and villous damage from reducedfetal perfusion (avascular villi or villous stromal vascular karyor-rhexis) were grouped under the heading of FTV. (5) Small for GA(SGA)/large for GA (LGA) placentas: trimmed placental weight<10th percentile for GA was defined as SGA placenta and >90thpercentile for GA was defined as LGA placenta.16 Presence of anyone of the six lesions described was considered as significantplacental pathology. The presence of more than one of the definedplacental lesions was classified as multiple placental pathology. Wepreviously reported 100% concordance between the routineplacental pathology report and independent review of placentaby a blinded pediatric pathologist.15 All placental pathologyreports were reviewed by a pediatric pathologist and neonatologist(S.J.-W. and I.N.M.), who were blinded to the clinical history andoutcomes. Study patients were divided into three groups based onplacental pathology: (1) No placental pathology, (2) One significantplacental pathology, and (3) Multiple placental pathologic lesions(presence of ≥2 significant lesions).
Data collectionBaseline maternal and infant characteristics, morbidities, andmortality were compared. In addition to examination of theelectronic health record, data were also obtained from theParkland Hospital NICU Database, which contains prospectivelycollected data on all neonates admitted to the NICU for >30 yearsand has been validated. Prolonged rupture of membrane wasdefined as rupture of membranes ≥18 h before birth. The NationalInstitute of Child Health and Human Development expert paneldefinition for clinical chorioamnionitis was used.17 Intrauterinefetal growth restriction was defined by Ponderal Index <10thpercentile for GA.
Neonatal short-term clinical outcomesMorbidities including respiratory distress syndrome), BPD, sepsis,severe intraventricular hemorrhage (IVH), necrotizing enterocolitis(NEC), length of hospitalization, and death during NICU stay werecollected from the NICU database. BPD was defined as persistentoxygen requirement for >28 days. Moderate-to-severe BPD wasdefined as the need for supplemental oxygen at 36 weekspostmenstrual age.2 Sepsis was recorded if the blood culture waspositive for a pathogenic organism ≤72 h after birth (early onset)and >72 h after birth (late onset) sepsis evaluations. Severe IVHwas defined as unilateral or bilateral grade III or higher on anyhead ultrasounds obtained during hospitalization.18 NEC wasdefined as Stage ≥2 based on the modified Bell’s criteria.19
Neurodevelopmental assessmentNeonates <29 weeks GA routinely undergo systematic standar-dized neurologic assessments and the Bayley Scales of Infant andToddler Development—Third edition (Bayley III) at 22–26 monthscorrected age at our outpatient follow-up clinic.4,20 Moderate-to-severe NDI was defined as the presence of any one of thefollowing: cerebral palsy with a gross motor functional classifica-tion system (GMFCS) score ≥2, Bayley III cognitive or motor score<85, visual impairment or permanent hearing loss that does notpermit the child to understand directions from the examiner andcommunicate with or without amplification. Severe NDI wasdefined as any of the following: severe cerebral palsy with GMFCSscore ≥4, Bayley III cognitive and motor score <70, bilateralblindness or bilateral hearing impairment +/− amplification.4
Outcome measuresThe composite of death and/or BPD was the primary outcome ofthe study. Pre-specified secondary outcomes included death,severe IVH, BPD, NEC, moderate-to-severe NDI, severe NDI, andindividual components of the neurodevelopmental assessment.These clinical outcome measures were chosen for analysis sinceplacental pathology has previously been associated with thesemorbidities.5
Statistical analysisSPSS version 19 (IBM) was used to perform statistical analyses.Descriptive statistics were calculated to compare neonatesbetween three placental pathologic groups described above.Categorical variables were analyzed by Chi-square for trend.Continuous variables were analyzed by one-way analysis ofvariance (ANOVA). A two-sided 0.05 level of significance was usedfor all analyses. In the event of significant result from one-wayANOVA, post hoc multiple comparison procedure was employedwith Bonferroni correction to separate groups. For the outcomesof BPD and NDI, stepwise forward logistic regression wasperformed to account for confounders. In addition to those pre-specified variables known to be associated with the outcomes ofinterest, all variables with P values < 0.1 were included in thelogistic regression. Confounding variables for BPD included GA,birth weight, sex, antenatal corticosteroids, and surfactantadministration. For neurodevelopmental outcomes, we included
Impact of multiple placental pathologies on neonatal death,. . .IN Mir et al.
2
Pediatric Research _#####################_

GA, sex, antenatal corticosteroids, and antenatal magnesiumadministration in the logistic regression.
RESULTSStudy populationDuring the study period, 251 neonates were born at 23–28.6 weeksGA. After excluding neonates who received comfort care or wereborn with congenital anomalies or chromosomal abnormalities,241 were included (Fig. 1). There were no differences in maternalcharacteristics across the three groups. Twenty-four percent(59/241) of infants had no placental pathology (Group 1), 41%(100/241) had a single placental pathologic lesion (Group 2), and34% (82/241) multiple lesions (Group 3, Table 1). Neonates withplacental pathology had lower GA, lower birth weight, and 1minApgar score (Table 1). Only 12% (28/241) infants were lost to long-term follow-up (Fig. 1).
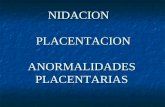
Distribution of placental pathologic lesionsAcute chorioamnionitis was the most common pathologic lesion,occurring in 49% neonates, with fetal vasculitis occurring in 32%.The second most common placental lesion was MVU (20%). Largenumbers of placentas were SGA (20%); however, 77% did notshow evidence of MVU. Sixteen percent of the placentas wereLGA, and 77% of them showed histological signs of chorioamnio-nitis. In infants with multiple placental pathologic lesions (34%),the most common combination was that of LGA+chorioamnio-nitis [n= 30, 12%], followed by SGA with chorioamnionitis [n= 15,6%] and MVU+chorioamnionitis [n= 11, 5%] (Fig. 2).
Association of multiple placental pathologies with BPD and NDINone of the individual placental pathologies were significantlyassociated with neonatal death, BPD, or NDI. However, as thenumber of the placental pathologic lesions increased (no lesionsvs. 1 lesion vs. ≥2 lesions), the occurrence of BPD increased from
35% to 49% and 65%; respectively; (P= 0.002). This was also truefor the occurrence of moderate/severe BPD and death or BPD(P= 0.004) (Table 2). Notably, the incidence of death or BPD wasalso highest in preterm infants with multiple lesions (P= 0.004),and they spent more days on mechanical ventilation (P < 0.01),oxygen (P < 0.001), and in the hospital (P= 0.009) (Table 2). Afteradjusting for GA, birth weight, gender, use of antenatal steroids,and surfactant administration, infants with multiple pathologiclesions were more likely to develop moderate-to-severe BPD [oddsratio (OR) 3.9 (1.5–10.1), P < 0.01]. When follow-up was examined,infants with multiple pathologic lesions were twice as likely tohave an NDI on bivariate analysis (P= 0.03) (Tables 3 and 4).However, after adjusting for GA, gender, use of antenatal steroids,and antenatal magnesium administration, multiple placentalpathologic lesions were no longer associated with NDI [OR 1.6(0.7–3.7), P= 0.28].
DISCUSSIONIncreasing evidence suggest that the occurrence of prenatalevents resulting in alterations in placental histology and thepresence of placental pathologic lesions may be related to orassociated with the occurrence of subsequent neonatal morbidityand NDI.5 In this study, using the uniform Redline classification,75% of preterm infants had evidence of at least one placentalpathology and 34% had multiple lesions. Although no individualplacental pathologic lesion was associated with the occurrence ofBPD, the presence of multiple lesions was significantly associatedwith subsequent death or the occurrence of BPD. Moreover,preterm infants with multiple placental pathologies were morelikely to develop NDI, but this was not significant after adjustingfor potential confounders.The association between BPD and the presence of various
placental pathologies such as MVU, FTV, chronic villitis, villousedema, and acute chorioamnionitis has been inconsistent.5,8,9,12,21–24
<29 weeks’ GA bornduring the study period
n = 251
ExcludedComfort care only
n = 10
Eligible Infantsn = 241
No placentalpathology
n = 59
Died n = 9;Lost to follow up
n = 10
Died n = 20;Lost to follow up
n = 10
Completed follow-upn = 40
Completed follow-upn = 70
Completed follow-upn = 58
Died, n = 16;Lost to follow up
n = 8
1 significant placentelpathologyn = 100
≥ 2 significantplacentel pathology
n = 82
Fig. 1 Flow diagram of the study population.
Impact of multiple placental pathologies on neonatal death,. . .IN Mir et al.
3
Pediatric Research _#####################_

For instance, MVU is a placental histopathological lesion associatedwith pre-eclampsia and other gestational hypertensive disordersleading to utero-placental insufficiency. While some have reportedinverse relationship between MVU and BPD,21 others have reported
that MVU is associated with severity of BPD and PAH.12 Similarly, therole of AHC in BPD has also been controversial; some studies haveshown no association with BPD,21–24 while others have reported anassociation between AHC and development of BPD.8,9 This could
Table 1. Relationship between placental pathology and maternal and infant characteristics.
No significant pathology(n= 59)
1 placental pathology(n= 100)
≥2 placental pathology(n= 82)
P value
Maternal
Age (years) 27 ± 6 27 ± 7 28 ± 6 NS
Antenatal steroids 25 (42%) 51 (51%) 48 (59%) NS
Diabetes 11 (19%) 16 (16%) 8 (10%) NS
Pregnancy-induced hypertension 21 (36%) 28 (28%) 18 (22%) NS
Antenatal magnesium therapy 26 (44%) 49 (49%) 39 (48%) NS
Prolonged rupture of membranes 10 (20%) 15 (15%) 21 (30%) NS
Clinical chorioamnionitis 1 (2%) 8 (8%) 11 (13%) NS
Delivered by cesarean section 40 (68%) 70 (70%) 53 (65%) NS
Infant
Female 28 (48%) 47 (47%) 39 (48%) NS
OB EGA, weeks 27 ± 1a 26 ± 2b 26 ± 1b 0.001
Birth weight, g 1044 ± 261a 945 ± 228a,b 910 ± 227b 0.006
IUGR 1 (2%) 4 (4%) 4 (6%) NS
Multiples 17 (33%) 22 (22%) 10 (15%) NS
Umbilical arterial pH 7.26 ± 0.07 7.27 ± 0.08 7.25 ± 0.12 NS
Umbilical arterial BD 6.3 ± 2.7 5.8 ± 3.1 6.2 ± 4.9 NS
Intubation in DR 30 (60%) 59 (59%) 58 (74%) NS
CPR 0 0 0 NS
Apgar scores, median (25th–75th centile)
1min 5 (3, 6)a 4 (2, 5)a 3 (1, 5)b 0.003
5min 7 (5, 8) 7 (6, 8) 7 (7, 8) NS
Data are the means ± SD. Numbers in parenthesis are percentages. Different superscripts of the letters (a or b) across rows designate significant differencesbetween groups by multiple comparison procedure with Bonferroni correctionNS not significant, OB EGA obstetric gestational age, IUGR intrauterine growth restriction, BD base deficit, DR delivery room, CPR cardiopulmonary resuscitation
FTV -18
MC - 119
FC - 78
VE - 3
LGA - 39
HGV - 8
MVU - 48
No pathology- 59
SGA - 48
Fig. 2 Venn diagrams showing complexity of placental lesions (overlapping lesions). MC chorioamnionitis without fetal vasculitis, FCchorioamnionitis with fetal vasculitis, MVU maternal vascular underperfusion, FTV fetal thrombotic vasculopathy, HGV high grade villitis, VEvillous edema, SGA small for gestational age placenta, LGA large for gestational age placenta. The most common pathological lesion in theplacentas in our patient population was histological acute chorioamnionitis (n= 119, 49%) and maternal vascular underperfusion (includingSGA placentas) (n= 96, 40%). The most common complex placental pathological lesions (multiple lesions) were a combination of histologicalacute chorioamnionitis with LGA placentas (n= 30, 12%), followed by histological acute chorioamnionitis with SGA placentas (n= 15, 6%) andacute chorioamnionitis with MVU (n= 11, 5%). Chronic villitis and villous edema was seen in very small percentage of placentas (<5%).
Impact of multiple placental pathologies on neonatal death,. . .IN Mir et al.
4
Pediatric Research _#####################_

reflect the lack of documentation of multiple placental pathologiclesions. Although we did not find any individual placental pathologysignificantly associated with the occurrence of BPD, the presence ofmultiple placental pathologic lesions was strongly associated withthe occurrence of BPD.The most common combination of lesions in placentas with
multiple lesions were LGA+chorioamnionitis, followed by SGA+chorioamnionitis and MVU+chorioamnionitis. A possible vascu-lar hypothesis explaining this association suggests that placentalpathology such as MVU results in placental insufficiency that inturn may lead to: (1) decreases in angiogenic factors such asplacental growth factors and vascular endothelial growth factor A(VEGF-A),25,26 (2) excess of amniotic fluid anti-angiogenic factorssuch as VEGF receptor antagonist gms-like tyrokinase-1,27 and (3)subsequent chronic fetal hypoxia.28 These factors may also resultin disruption of pulmonary vascular growth/development andalveolarization.28 Notably, the presence of chronic hypoxia in fetalsheep that is associated with MVU and the development ofplacental insufficiency leads to the classic histologic findings ofBPD.29 The alternative inflammatory hypothesis for the occurrenceof BPD suggests chorioamnionitis results in a systemic fetalinflammatory response causing increased pulmonary expression
of proinflammatory cytokines, apoptosis, and remodeling of thefetal lungs.30,31 Notably, this inflammation may also be associatedwith attenuated responses to exogenous surfactant therapy andthus the need for prolonged mechanical ventilation.32 Coloniza-tion with Ureaplasma urealyticum or Ureaplasma pravum orincreased risk of postnatal sepsis may also contribute to thedevelopment of BPD in preterm infants with histologic acutechorioamnionitis on placental examination.33 We speculate thatthe association of BPD with multiple placental lesions, but notwith isolated pathology, suggests that there are interactive effectsbetween vascular and inflammatory processes that promote thedevelopment of BPD. This is especially relevant since not allpreterm infants exposed to chorioamnionitis or to MVU developBPD. Therefore, it is possible that multiple/severe insults need tooccur over the course of pregnancy, rather than an isolated event,in order to increase the risk of developing of BPD in neonates<29 weeks GA.This is the first study that has looked at an association of
multiple placental pathologic lesions with neurodevelopmentaloutcome data using Bayley III. Similar to BPD, studies have beendone to show an association between NDI and various placentalpathologies, including chorioamnionitis, MVU, FTV, and chronic
Table 2. Relationship between the placental pathology and short-term neonatal outcomes and BPD.
No placental pathology (n= 59) 1 placental pathology (n= 100) ≥2 placental pathology (n= 82) P value
Respiratory distress syndrome 51 (90%) 90 (90%) 69 (86%) NS
Received surfactant 45 (79%) 71 (71%) 57 (71%) NS
BPD: O2 therapy >28 days 20 (35%)a 49 (49%)a 52 (65%)b 0.002
Moderate/severe BPD 7 (12%)a 21 (21%)a 29 (35%)b 0.004
Days received oxygen 36 ± 35a 45 ± 37a 70 ± 61b <0.001
Days required mechanical ventilation 8 ± 11a 13 ± 16a 20 ± 22b <0.01
Sepsis proven (not suspect) 1 (2%) 1 (1%) 2 (2%) NS
IVH grade III or IV 5 (9%) 16 (16%) 16 (20%) NS
Necrotizing enterocolitis 9 (15%) 12 (12%) 17 (21%) NS
Length of hospitalization (days) 79 ± 34a 92 ± 32a,b 104 ± 57b 0.009
Death 9 (15%) 20 (20%) 16 (20%) NS
Death or BPD 15 (25%)a 37 (37%)a 43 (52%)a 0.004
Data are the means ± SD. Numbers in parenthesis are percentages. Different superscripts of letters (a or b) across rows designate significant differencesbetween groups by multiple comparison procedure with Bonferroni correctionNS not significant, BPD bronchopulmonary dysplasia, IVH intraventricular hemorrhage
Table 3. Relationship between the placental pathology and neurodevelopmental outcomes.
No placental pathology (N= 59) 1 placental pathology (N= 100) ≥2 placental pathology (N= 82) P value
NDI 17 (29%)a 29 (29%)a 38 (46%)b 0.03
NDI or death 26 (44%)a 46 (46%)a 51 (62%)b 0.04
Severe NDI (NDI < 70) 2 (3%) 10 (10%) 12 (15%) NS
Severe NDI or death 11 (19%) 27 (27%) 25 (31%) NS
Cognitive impairment 87.0 ± 9.3 85.0 ± 13.3 81.6 ± 13.7 NS
Motor impairment 90.6 ± 11.6 88.2 ± 15.1 83.7 ± 14.6 NS
Normal neurologic exam 48 (81%) 73 (73%) 52 (63%) NS
Abnormal neurologic exam 8 (14%) 13 (13%) 15 (18%) NS
Non-CP definition abnormal 1 (2%) 6 (6%) 10 (12%) NS
Cerebral palsy 2 (3%) 8 (8%) 5 (6%) NS
Data are the means ± SD. Numbers in parenthesis are percentages within a column. Different superscripts of letters (a or b) across rows designate significantdifferences between groups by multiple comparison procedure with Bonferroni correction. Comparison groups with different subscripts (a or b) signifystatistical difference and similar subscripts are not statistically differentNS not significant, NDI neurodevelopmental impairment, Non-CP non-cerebral palsy
Impact of multiple placental pathologies on neonatal death,. . .IN Mir et al.
5
Pediatric Research _#####################_

villitis; but these associations have been inconsistent.10,34–36 Forinstance, although the association between AHC and adverseneurodevelopmental outcomes has been studied, the associationis quite variable, with some reporting that AHC is a significantpredictor of cerebral palsy34 and NDI,10 while others reporting noadverse association between AHC and neurodevelopmentaloutcome.35 Similarly, there are few studies that have examinedMVU and NDI.36 It has been suggested that MVU may lead to fetalhypoxia, which contributes to the breakdown of the blood–brainbarrier and triggers glutamate excitotoxicity. Free radicals incombination with a developmental lack of antioxidant enzymes inoligodendrocytes may explain the impact of hypoxia on thepremature brain.37 While significant association between placentalinfarction (suggesting MVU) and NDI has been reported,38 this wasnot seen by others.39 This variability in the previous studies may,in part, be accounted for by a lack of statistical power,retrospective analysis, and differences in time of neurodevelop-mental assessments. Moreover, none of these studies evaluatedmultiple lesions. In our study, infants with multiple placentalpathologic lesions were more likely to have moderate-to-severeNDI; however, after adjusting for potential confounders, thisassociation disappeared. As in BPD, it is possible that there isinteractive effect between placental vascular and inflammatorylesions on the occurrence of cerebral injury, but a larger cohort isneeded to examine this association.The strengths of our study include a large cohort with
consecutive sampling to decrease selection bias, relative homo-geneity of the study subjects delivered and cared for at a singlecenter, high rate of follow-up (~90%) with systematic assessmentof long-term outcomes, and availability of placental histopathol-ogy in all preterm infants delivered in our institution. We also
assessed a large variety of placental lesions, defined theirsignificance a priori, used a uniform method for classification,and assessed multiple lesions. Our study did have some limitationssuch as its retrospective nature. Even though logistic regressionwas done to account for known variables, it is possible thatunknown confounders are not accounted for. We did not collectthe data on ventilator associated pneumonia (VAP) and Score forneonatal acute physiology with perinatal extenstion (SNAP-PE), asthese data are not collected routinely at our institution. It is highlylikely that multiple placental lesions not only indicate aninteraction between vascular and inflammatory lesions but mayalso indicate severity of the vascular or inflammatory insult. Futurestudies should explore role of such lesions and the interaction inpathogenesis of neonatal morbidities.To the best of our knowledge, this is the first report
demonstrating an association between the presence of multipleplacental lesions, BPD, and its severity in neonates <29 weeks GA,demonstrating the importance of routine placental pathology andreporting multiple lesions. We speculate that there may aninteraction between the pathogenesis of placental vascular andinflammatory lesions that contribute to the development of BPDand its severity. The association between placental pathologyshould be included in future predictive models of BPD, and largeanimal and prospective clinical studies should be designed todetermine how various placental pathologies interact and theirrole in development of neonatal morbidities.
ACKNOWLEDGEMENTSThis work was supported by NICHD/NIH 1K23HD083511-01A1.
AUTHOR CONTRIBUTIONSAll authors contributed to drafting the article or revising it critically for importantintellectual content and final approval of the submitted version. Specifically, I.N.M.participated in concept, study design, sample and data acquisition and interpretation,performed the statistical analysis, drafted the first version of the manuscript, andfinalized the manuscript for submission after comments from the other authors. L.F.C.participated in concept, study design, data interpretation and review, revision of themanuscript, and reviewed the final version. S.J.-W. participated in concept, helpedwith pathology classification, data interpretation, revision of the manuscript, andreviewed the final version. L.S.B. performed the statistical analysis, participated indata interpretation and review, revision of the manuscript, and reviewed the finalversion. C.R.R. participated in concept, study design, data interpretation, revision ofthe manuscript, and participated in finalizing the manuscript after comments fromthe other authors. R.H. participated in concept, study design, provided the follow-updata of the infants, participated in data interpretation, and reviewed the finalmanuscript. V.K. participated in concept, study design, data interpretation andreview, revision of the manuscript, and participated in finalizing the manuscript aftercomments from the other authors.
ADDITIONAL INFORMATIONCompeting interests: The authors declare no competing interests.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claimsin published maps and institutional affiliations.
REFERENCES1. Glass, H. C. et al. Outcomes for extremely premature infants. Anesth. Analg. 120,
1337–1351 (2015).2. Stoll, B. J. et al. Trends in care practices, morbidity, and mortality of extremely
preterm neonates, 1993-2012. JAMA 314, 1039–1051 (2015).3. Jensen, E. A. & Schmidt, B. Epidemiology of bronchopulmonary dysplasia. Birth
Defects Res. A Clin. Mol. Teratol. 100, 145–157 (2014).4. Vohr, B. R. et al. Are outcomes of extremely preterm infants improving? Impact of
Bayley assessment on outcomes. J. Pediatr. 161, 222.e3–228.e3 (2012).5. Roescher, A. M., Timmer, A., Erwich, J. J. & Bos, A. F. Placental pathology, perinatal
death, neonatal outcome, and neurological development: a systematic review.PLoS ONE 9, e89419 (2014).
Table 4. Description of placental pathology in BPD vs. no BPDpatients.
Placental pathologies No BPD (n= 115) BPD (n= 121)
SGA 17 (15%) 31 (26%)
LGA 16 (14%) 22 (18%)
MC 52 (45%) 65 (54%)
FC 33 (29%) 42 (35%)
MVU 20 (17%) 27 (22%)
FTV 5 (4%) 12 (10%)
HGV 4 (4%) 4 (3%)
VE 2 (2%) 1 (1%)
SGA+MC 4 (4%) 11 (9%)
SGA+FC 2 (2%) 6 (5%)
SGA+MVU 2 (2%) 9 (7%)
SGA+FTV 2 (2%) 5 (4%)
LGA+MC 14 (12%) 16 (13%)
LGA+FC 12 (10%) 12 (10%)
LGA+MVU 5 (4%) 4 (3%)
LGA+FTV 2 (2%) 0 (0%)
MC+MVU 8 (7%) 11 (9%)
MC+FTV 1 (1%) 3 (3%)
FC+MVU 6 (5%) 8 (7%)
FC+FTV 1 (1%) 2 (2%)
Numbers in parenthesis are percentages within a columnSGA small for gestational age, LGA large for gestational age, MC maternalchorioamnionitis, FC chorioamnionitis with fetal vasculitis, MVU maternalvascular underperfusion, FTV fetal thrombotic vasculopathy, HGV high-grade villitis, VE villous edema
Impact of multiple placental pathologies on neonatal death,. . .IN Mir et al.
6
Pediatric Research _#####################_

6. Roescher, A. M. et al. Placental pathology and neurological morbidity in preterminfants during the first two weeks after birth. Early Hum. Dev. 90, 21–25 (2014).
7. Ogunyemi, D., Murillo, M., Jackson, U., Hunter, N. & Alperson, B. The relationshipbetween placental histopathology findings and perinatal outcome in preterminfants. J. Matern. Fetal Neonatal Med. 13, 102–109 (2003).
8. Lee, H. J. et al. Chorioamnionitis, respiratory distress syndrome and broncho-pulmonary dysplasia in extremely low birth weight infants. J. Perinatol. 31,166–170 (2011).
9. Kunjunju, A. M., Gopagondanahalli, K. R., Chan, Y. & Sehgal, A. Bronchopulmonarydysplasia-associated pulmonary hypertension: clues from placental pathology. J.Perinatol. 37, 1310–1314 (2017).
10. Pappas, A. et al. Chorioamnionitis and early childhood outcomes among extre-mely low-gestational-age neonates. JAMA Pediatr. 168, 137–147 (2014).
11. Chisholm, K. M. et al. Correlation of preterm infant illness severity with placentalhistology. Placenta 39, 61–69 (2016).
12. Mestan, K. K. et al. Placental pathologic changes of maternal vascular under-perfusion in bronchopulmonary dysplasia and pulmonary hypertension. Placenta35, 570–574 (2014).
13. Greer, L. G. et al. An immunologic basis for placental insufficiency in fetal growthrestriction. Am. J. Perinatol. 29, 533–538 (2012).
14. Redline, R. W., Heller, D., Keating, S. & Kingdom, J. Placental diagnostic criteria andclinical correlation-a workshop report. Placenta 26(Suppl A), S114–S117 (2005).
15. Mir, I. N. et al. Placental pathology is associated with severity of neonatal ence-phalopathy and adverse developmental outcomes following hypothermia. Am. J.Obstet. Gynecol. 213, 849.e1–849.e7 (2015).
16. Pinar, H., Sung, C. J., Oyer, C. E. & Singer, D. B. Reference values for singleton andtwin placental weights. Pediatr. Pathol. Lab. Med. 16, 901–907 (1996).
17. Higgins, R. D. et al. Evaluation and management of women and newborns with amaternal diagnosis of chorioamnionitis: summary of a workshop. Obstet. Gynecol.127, 426–436 (2016).
18. Papile, L.-A., Burstein, J., Burstein, R. & Koffler, H. Incidence and evolution ofsubependymal and intraventricular hemorrhage: a study of infants with birthweights less than 1,500 gm. J. Pediatr. 92, 529–534 (1978).
19. Bell, M. J. et al. Neonatal necrotizing enterocolitis - therapeutic decisions basedupon clinical staging. Ann. Surg. 187, 1–7 (1978).
20. Albers, C. A. & Grieve, A. J. Test Review: Bayley, N. (2006). Bayley Scales of Infantand Toddler Development–Third Edition. San Antonio, TX: Harcourt Assessment.J. Psychoeduc. Assess. 25, 180–198 (2007).
21. Redline, R. W., Wilson-Costello, D. & Hack, M. Placental and other perinatal riskfactors for chronic lung disease in very low birth weight infants. Pediatr. Res. 52,713–719 (2002).
22. Kent, A. & Dahlstrom, J. E. Chorioamnionitis/funisitis and the development ofbronchopulmonary dysplasia. J. Paediatr. Child Health 40, 356–359 (2004).
23. Van Marter, L. J. et al. Chorioamnionitis, mechanical ventilation, and postnatalsepsis as modulators of chronic lung disease in preterm infants. J. Pediatr. 140,171–176 (2002).
24. Hartling, L., Liang, Y. & Lacaze-Masmonteil, T. Chorioamnionitis as a risk factor forbronchopulmonary dysplasia: a systematic review and meta-analysis. Arch. Dis.Child. Fetal Neonatal Ed. 97, F8–F17 (2012).
25. Abman, S. H. Bronchopulmonary dysplasia: “a vascular hypothesis”. Am. J. Respir.Crit. Care Med. 164(Pt 1), 1755–1756 (2001).
26. Thebaud, B. & Abman, S. H. Bronchopulmonary dysplasia: where have all thevessels gone? Roles of angiogenic growth factors in chronic lung disease. Am. J.Respir. Crit. Care Med. 175, 978–985 (2007).
27. Tang, J. R., Karumanchi, S. A., Seedorf, G., Markham, N. & Abman, S. H. Excesssoluble vascular endothelial growth factor receptor-1 in amniotic fluid impairslung growth in rats: linking preeclampsia with bronchopulmonary dysplasia. Am.J. Physiol. Lung Cell. Mol. Physiol. 302, L36–L46 (2012).
28. Strouss, L., Goldstein, N. D., Locke, R. & Paul, D. A. Vascular placental pathologyand the relationship between hypertensive disorders of pregnancy and neonataloutcomes in very low birth weight infants. J. Perinatol. 38, 324–331 (2018).
29. Rozance, P. J. et al. Intrauterine growth restriction decreases pulmonary alveolar andvessel growth and causes pulmonary artery endothelial cell dysfunction in vitro infetal sheep. Am. J. Physiol. Lung Cell. Mol. Physiol. 301, L860–L871 (2011).
30. Ghezzi, F. et al. Elevated interleukin-8 concentrations in amniotic fluid of motherswhose neonates subsequently develop bronchopulmonary dysplasia. Eur. J.Obstet. Gynecol. Reprod. Biol. 78, 5–10 (1998).
31. Yoon, B. H. et al. Amniotic fluid cytokines (interleukin-6, tumor necrosis factor-alpha, interleukin-1 beta, and interleukin-8) and the risk for the development ofbronchopulmonary dysplasia. Am. J. Obstet. Gynecol. 177, 825–830 (1997).
32. Been, J. V. et al. Chorioamnionitis alters the response to surfactant in preterminfants. J. Pediatr. 156, 10.e1–15.e1 (2010).
33. Schelonka, R. L., Katz, B., Waites, K. B. & Benjamin, D. K. Jr Critical appraisal of therole of Ureaplasma in the development of bronchopulmonary dysplasia withmetaanalytic techniques. Pediatr. Infect. Dis. J. 24, 1033–1039 (2005).
34. Wu, Y. W. & Colford, J. M. Jr Chorioamnionitis as a risk factor for cerebral palsy: ameta-analysis. JAMA 284, 1417–1424 (2000).
35. Andrews, W. W. et al. Early preterm birth: association between in utero exposureto acute inflammation and severe neurodevelopmental disability at 6 years ofage. Am. J. Obstet. Gynecol. 198, 466.e1–466.e11 (2008).
36. Vinnars, M. T., Vollmer, B., Nasiell, J., Papadogiannakis, N. & Westgren, M. Asso-ciation between cerebral palsy and microscopically verified placental infarction inextremely preterm infants. Acta Obstet. Gynecol. Scand. 94, 976–982 (2015).
37. Rezaie, P. & Dean, A. Periventricular leukomalacia, inflammation and white matterlesions within the developing nervous system. Neuropathology 22, 106–132(2002).
38. Blair, E., de Groot, J. & Nelson, K. B. Placental infarction identified by macroscopicexamination and risk of cerebral palsy in infants at 35 weeks of gestational ageand over. Am. J. Obstet. Gynecol. 205, 124.e1–124.e7 (2011).
39. Leviton, A. et al. Microbiologic and histologic characteristics of the extremelypreterm infant's placenta predict white matter damage and later cerebral palsy.the ELGAN study. Pediatr. Res. 67, 95–101 (2010).
Impact of multiple placental pathologies on neonatal death,. . .IN Mir et al.
7
Pediatric Research _#####################_