Inmunización contra la hepatitis B para los recién … · con placebo/ninguna intervención, la...
81
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitis B Lee C, Gong Y, Brok J, Boxall EH, Gluud C Reproducción de una revisión Cochrane, traducida y publicada en La Biblioteca Cochrane Plus, 2008, Número 2 Producido por Si desea suscribirse a "La Biblioteca Cochrane Plus", contacte con: Update Software Ltd, Summertown Pavilion, Middle Way, Oxford OX2 7LG, UK Tel: +44 (0)1865 513902 Fax: +44 (0)1865 516918 E-mail: [email protected] Sitio web: http://www .update-softw are.com Usado con permiso de John Wiley & Sons, Ltd. © John Wiley & Sons, Ltd. Ningún apartado de esta revisión puede ser reproducido o publicado sin la autorización de Update Software Ltd. Ni la Colaboración Cochrane, ni los autores, ni John Wiley & Sons, Ltd. son responsables de los errores generados a partir de la traducción, ni de ninguna consecuencia derivada de la aplicación de la información de esta Revisión, ni dan grantía alguna, implícita o explícitamente, respecto al contenido de esta publicación. El copyright de las Revisiones Cochrane es de John Wiley & Sons, Ltd. El texto original de cada Revisión (en inglés) está disponible en www.thecochranelibrary.com.
-
Upload
nguyenphuc -
Category
Documents
-
view
217 -
download
0
Transcript of Inmunización contra la hepatitis B para los recién … · con placebo/ninguna intervención, la...

Inmunización contra la hepatitis B para los recién nacidos de madrescon pruebas positivas para el antígeno de superficie de la hepatitis
B
Lee C, Gong Y, Brok J, Boxall EH, Gluud C
Reproducción de una revisión Cochrane, traducida y publicada en La Biblioteca Cochrane Plus, 2008, Número 2
Producido por
Si desea suscribirse a "La Biblioteca Cochrane Plus", contacte con:
Update Software Ltd, Summertown Pavilion, Middle Way, Oxford OX2 7LG, UKTel: +44 (0)1865 513902 Fax: +44 (0)1865 516918E-mail: [email protected] web: http://www.update-software.com
Usado con permiso de John Wiley & Sons, Ltd. © John Wiley & Sons, Ltd.Ningún apartado de esta revisión puede ser reproducido o publicado sin la autorización de Update Software Ltd.Ni la Colaboración Cochrane, ni los autores, ni John Wiley & Sons, Ltd. son responsables de los errores generadosa partir de la traducción, ni de ninguna consecuencia derivada de la aplicación de la información de esta Revisión,ni dan grantía alguna, implícita o explícitamente, respecto al contenido de esta publicación.El copyright de las Revisiones Cochrane es de John Wiley & Sons, Ltd.El texto original de cada Revisión (en inglés) está disponible en www.thecochranelibrary.com.

ÍNDICE DE MATERIAS
RESUMEN...................................................................................................................................................................1
RESUMEN EN TÉRMINOS SENCILLOS....................................................................................................................2
ANTECEDENTES........................................................................................................................................................2
OBJETIVOS.................................................................................................................................................................2
CRITERIOS PARA LA VALORACIÓN DE LOS ESTUDIOS DE ESTA REVISIÓN......................................................2
ESTRATEGIA DE BÚSQUEDA PARA LA IDENTIFICACIÓN DE LOS ESTUDIOS....................................................3
MÉTODOS DE LA REVISIÓN.....................................................................................................................................3
DESCRIPCIÓN DE LOS ESTUDIOS..........................................................................................................................4
CALIDAD METODOLÓGICA.......................................................................................................................................6
RESULTADOS.............................................................................................................................................................6
DISCUSIÓN.................................................................................................................................................................7
CONCLUSIONES DE LOS AUTORES........................................................................................................................9
AGRADECIMIENTOS..................................................................................................................................................9
POTENCIAL CONFLICTO DE INTERÉS.....................................................................................................................9
NOTAS.........................................................................................................................................................................9
FUENTES DE FINANCIACIÓN....................................................................................................................................9
REFERENCIAS.........................................................................................................................................................10
TABLAS......................................................................................................................................................................17
Characteristics of included studies.....................................................................................................................17
Characteristics of excluded studies....................................................................................................................42
Table 01 Search strategies.................................................................................................................................44
Table 02 Intervention by group............................................................................................................................45
CARÁTULA................................................................................................................................................................48
RESUMEN DEL METANÁLISIS.................................................................................................................................49
GRÁFICOS Y OTRAS TABLAS..................................................................................................................................52
01 Vacuna versus placebo o ninguna intervención.............................................................................................52
01 Eventos de hepatitis B según el tipo de vacuna.....................................................................................52
02 Eventos de hepatitis B según la calidad metodológica...........................................................................53
03 Eventos de hepatitis B - Análisis de sensibilidad....................................................................................54
04 Eventos de hepatitis B según el estado de HBeAg de la madre............................................................55
05 Eventos de hepatitis B según la primera administración de la vacuna...................................................56
02 VR versus VDP..............................................................................................................................................57
01 Eventos de hepatitis B............................................................................................................................57
02 Eventos de hepatitis B según la calidad metodológica...........................................................................57
03 Eventos de hepatitis B - análisis de sensibilidad....................................................................................58
04 Eventos de hepatitis B según el estado de HBeAg de la madre............................................................59
05 Anti-HBs menor de 10 UI/L.....................................................................................................................59
03 Vacuna con dosis alta versus vacuna con dosis baja....................................................................................60
01 Eventos de hepatitis B............................................................................................................................60
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB i
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

02 Eventos de hepatitis B según la calidad metodológica...........................................................................61
03 Eventos de hepatitis B - análisis de sensibilidad....................................................................................62
04 Eventos de hepatitis B según el estado de HBeAg de la madre............................................................63
05 Anti-HBs menor de 10 UI/L.....................................................................................................................63
04 VDP en tres dosis más IGHB versus VDP en dos dosis más IGHB..............................................................64
01 Eventos de hepatitis B............................................................................................................................64
02 Anti-HBs menor de 10 UI/L.....................................................................................................................64
05 VDP al nacer versus VDP al mes...................................................................................................................64
01 Eventos de hepatitis B............................................................................................................................64
06 Un tipo de VDP versus otro tipo de VDP........................................................................................................65
01 Eventos de hepatitis B............................................................................................................................65
07 Cuatro vacunaciones de VR versus tres vacunaciones de VR......................................................................65
01 Eventos de hepatitis B............................................................................................................................65
02 Anti-HBs menor de 10 UI/L.....................................................................................................................65
08 Un tipo de VR versus otro tipo de VR con el mismo esquema de vacunación..............................................66
01 Eventos de hepatitis B............................................................................................................................66
02 Anti-HBs menor de 10 UI/L.....................................................................................................................66
09 IGHB versus placebo o ninguna intervención................................................................................................67
01 Eventos de hepatitis B............................................................................................................................67
02 Eventos de hepatitis B según la calidad metodológica de los ensayos..................................................68
03 Eventos de hepatitis B - análisis de sensibilidad....................................................................................69
04 Eventos de hepatitis B según el estado de HBeAg de la madre............................................................70
05 Eventos de hepatitis B según el tiempo de administración de la IGHB..................................................71
06 Eventos de hepatitis B según un esquema de vacunas estándar y rápido............................................72
07 Anti-HBs menor de 10 UI/L.....................................................................................................................73
08 Título de anti-HBs...................................................................................................................................73
09 Eventos adversos...................................................................................................................................73
10 IGHB múltiple más VDP versus IGHB simple más VDP................................................................................74
01 Eventos de hepatitis B............................................................................................................................74
11 VDP más IGHB versus placebo o ninguna intervención................................................................................74
01 Eventos de hepatitis B............................................................................................................................74
02 Eventos de hepatitis B según la calidad metodológica de los ensayos..................................................75
03 Eventos de hepatitis B - análisis de sensibilidad....................................................................................76
04 Eventos de hepatitis B según el estado de HBeAg de la madre............................................................77
05 Eventos de hepatitis B según el tiempo de administración de la IGHB..................................................78
06 Eventos adversos...................................................................................................................................78
ÍNDICE DE MATERIAS
ii Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de lahepatitis B
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

Inmunización contra la hepatitis B para los recién nacidos de madrescon pruebas positivas para el antígeno de superficie de la hepatitisB
Lee C, Gong Y, Brok J, Boxall EH, Gluud C
Esta revisión debería citarse como:Lee C, Gong Y, Brok J, Boxall EH, Gluud C. Inmunización contra la hepatitis B para los recién nacidos de madres con pruebaspositivas para el antígeno de superficie de la hepatitis B (Revisión Cochrane traducida). En: La Biblioteca Cochrane Plus, 2008Número 2. Oxford: Update Software Ltd. Disponible en: http://www.update-software.com. (Traducida de The Cochrane Library,2008 Issue 2. Chichester, UK: John Wiley & Sons, Ltd.).Fecha de la modificación más reciente: 22 de febrero de 2006Fecha de la modificación significativa más reciente: 22 de febrero de 2006
RESUMEN
AntecedentesSe considera la vacuna contra la hepatitis B y la inmunoglobulina de la hepatitis B para los recién nacidos de madres con pruebaspositivas para el HBsAg, para prevenir la infección por hepatitis B.
ObjetivosEvaluar los efectos beneficiosos y perjudiciales de las vacunas contra la hepatitis B y la inmunoglobulina de la hepatitis B enrecién nacidos de madres con pruebas positivas para el HBsAg.
Estrategia de búsquedaSe identificaron ensayos mediante búsquedas en el Registro Especializado de Ensayos Controlados del Grupo Cochrane deNeonatología (The Cochrane Neonatal Group Controlled Trials Register), el Registro Especializado de Ensayos Controladosdel Grupo Cochrane Hepatobiliar, (The Cochrane Hepato-Biliary Group Controlled Trials Register), el Registro CochraneCentral de Ensayos Controlados (Cochrane Central Register of Controlled Trials, CENTRAL) en The Cochrane Library,MEDLINE, y EMBASE (hasta febrero de 2004), y por contacto con autores de ensayos y compañías farmacéuticas.
Criterios de selecciónEnsayos clínicos aleatorios que comparen: la vacuna derivada de plasma (VDP) o la vacuna recombinante (VR) versus ningunaintervención, placebo u otras vacunas activas; la inmunoglobulina de la hepatitis B versus ninguna intervención, placebo u otrainmunoglobulina de control; así como la VDP o la VR más la inmunoglobulina de la hepatitis B versus ninguna intervención,placebo u otras vacunas de control o inmunoglobulina.
Recopilación y análisis de datosLas medidas de resultado se evaluaron en el período máximo de seguimiento. La medida de resultado primaria fue la apariciónde hepatitis B, basada en una muestra de sangre positiva para el HBsAg, el HBeAg o el anticuerpo anticore de la hepatitis B(anti-HBc). Se informan las medidas de resultado binarias como riesgos relativos (RR) con intervalos de confianza (IC) del 95%.Se realizaron análisis de subgrupos con respecto a la calidad metodológica del ensayo, el estado del HBe-Ag de la madre y eltiempo de inmunización después del nacimiento.
Resultados principalesSe identificaron 29 ensayos clínicos aleatorios, 5 de los cuales se consideraron de alta calidad. Sólo 3 ensayos informaron lainclusión de madres con pruebas negativas para el antígeno "e" de la hepatitis B. En comparación con placebo/ninguna intervención,la vacuna disminuyó la aparición de hepatitis B (RR 0,28; intervalo de confianza (IC) del 95%: 0,20 a 0,40; 4 ensayos). No seencontraron diferencias significativas de la aparición de hepatitis B al comparar la vacuna recombinante (VR) versus la vacunaderivada del plasma (VDP) (RR 1,00; IC del 95%: 0,71 a 1,42; 4 ensayos) y la vacuna con dosis altas versus la vacuna con dosisbajas (VDP: RR 0,97; IC del 95%: 0,55 a 1,68; 3 ensayos; VR: RR 0,78; IC del 95%: 0,31 a 1,94; 1 ensayo). En comparación
Página 1
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

con placebo/ninguna intervención, la inmunoglobulina de la hepatitis B o la combinación de la vacuna más la inmunoglobulinade la hepatitis B disminuyó la aparición de hepatitis B (inmunoglobulina de la hepatitis B: RR 0,50; IC del 95%: 0,41 a 0,60; 1ensayo; VDP más inmunoglobulina de la hepatitis B: RR 0,08; IC del 95%: 0,03 a 0,17; 3 ensayos). En comparación con lavacuna sola, la vacuna más la inmunoglobulina de la hepatitis B disminuyó la aparición de hepatitis B (RR 0,54; IC del 95%:0,41 a 0,73; 10 ensayos). La vacuna contra la hepatitis B y la inmunoglobulina de la hepatitis B parecen seguras, pero pocosensayos informaron los eventos adversos.
Conclusiones de los autoresLa vacuna, la inmunoglobulina de la hepatitis B y la vacuna más la inmunoglobulina de la hepatitis B previenen la aparición dehepatitis B en recién nacidos de madres con pruebas positivas para el HBsAg.
✦
RESUMEN EN TÉRMINOS SENCILLOS
La vacuna contra la hepatitis B, la inmunoglobulina de la hepatitis B y la combinación de la vacuna más la inmunoglobulinaprevienen la transmisión perinatal de la hepatitis B
La vacunación contra la hepatitis B y la inmunoglobulina de la hepatitis B se consideran medidas preventivas para los reciénnacidos de madres con pruebas positivas para el HBsAg. Cuando se combinaron todos los ensayos identificados, la vacuna contrala hepatitis B sola, la inmunoglobulina de la hepatitis B sola, y la vacuna más la inmunoglobulina de la hepatitis B disminuyeronla transmisión perinatal de la hepatitis B en comparación con placebo o ninguna intervención. La vacuna contra la hepatitis Bmás la inmunoglobulina de la hepatitis B fueron superiores a la vacunación contra la hepatitis B sola. Los eventos adversos fueronraros y la mayoría no graves.
✦
ANTECEDENTES
El virus de la hepatitis B es una enfermedad global transmisibleaguda y crónica que ocasiona enfermedad hepática grave, conaproximadamente 350 millones de personas infectadas (Beasley1984). La transmisión de madre a hijo ocurre con frecuencia,ya sea en el útero (cuando el feto todavía no nació), a través dela vía placentaria o mediante la exposición a la sangre o a loslíquidos contaminados con sangre en el momento del nacimientoo cerca del mismo. Se cree que dicha transmisión perinatalrepresenta del 35% al 50% de los portadores de hepatitis B (Yao1996). El riesgo de transmisión perinatal está asociado con elestado del HBeAg de la madre. Si la madre es positiva a HBsAgy HBeAg, del 70% al 90% de los niños se convierten encrónicamente infectados (Stevens 1975; Akhter 1992). Si lamadre es HBsAg positiva pero HBeAg negativa, el riesgodisminuye significativamente (Okada 1976; Beasley 1977;Beasley 1983b; Nayak 1987; Aggarwal 2004).
Se han autorizado dos tipos de vacunas. Un tipo se deriva delplasma humano (vacuna derivada de plasma [VDP]) y el otroes producto de la tecnología del ADN recombinante (vacunarecombinante [VR]) en células de levadura o de mamíferos(Assad 1999). Se requieren inyecciones repetidas durante mesespara alcanzar una respuesta efectiva de anticuerpos con lavacunación. La inmunoglobulina de la hepatitis B es unainmunoglobulina con un alto contenido de anticuerpos contrael antígeno de superficie de la hepatitis B (anti-HBs). Se
considera que la inmunoglobulina de la hepatitis B es efectivainmediatamente y parece que protege durante varios mesesdespués de los cuales esta protección disminuyeprogresivamente (Beasley 1983; Nair 1984).
No se pudieron identificar metanálisis o revisiones sistemáticassobre la inmunización contra la hepatitis B para los reciénnacidos de madres con pruebas positivas para el HBsAg. Se hapublicado una revisión narrativa sobre la eficacia de la vacunacontra la hepatitis B en recién nacidos (Andre 1994) y variasguías internacionales (CDC 1999; WHO 2002). Sin embargo,estas publicaciones no representan revisiones sistemáticas quecuentan con una evaluación de la calidad metodológica de losensayos y no presentan datos originales.
OBJETIVOS
Evaluar los efectos beneficiosos y perjudiciales de la vacunacontra la hepatitis B y la inmunoglobulina de la hepatitis B enrecién nacidos de madres con pruebas positivas para el HBsAg.
CRITERIOS PARA LA VALORACIÓN DE LOSESTUDIOS DE ESTA REVISIÓN
Tipos de estudios
Se incluyeron ensayos clínicos aleatorios, independientementedel cegamiento, el estado de publicación o el idioma.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 2
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

Tipos de participantes
Se incluyeron recién nacidos de cualquier sexo de madres conpruebas positivas para el HBsAg. La inmunización debecomenzar en el primer mes de vida.
Tipos de intervención
Se realizaron los siguientes análisis:• VDP o VR versus placebo o ninguna intervención.• Inmunoglobulina de la hepatitis B versus placebo o
ninguna intervención.• VDP o VR más inmunoglobulina de la hepatitis B versus
placebo, ninguna intervención, VDP o VR.
Tipos de medidas de resultado
Se evaluaron todas las medidas de resultado en el tiempo deseguimiento máximo.
Medida de resultado primaria(1) Aparición de la hepatitis B: muestra de sangre positiva parael HBsAg, el HBeAg, o el anticuerpo anticore de la hepatitis B(anti-HBc).
Medidas de resultado secundarias(2) Número de recién nacidos con anti-HBs menor de 10 UI/L,lo que se considera insuficiente para prevenir la infección porel virus de la hepatitis B (Szmuness 1981; Hadler 1986).(3) Anti-HBs expresado como media geométrica del título(MGT) o media del título.(4) Eventos adversos sistémicos: eventos adversos comomalestar general, náuseas, fiebre, artralgia y erupción cutáneadespués de cada inyección de la vacuna.(5) Eventos adversos locales: eventos adversos como dolor,enrojecimiento, tumefacción y/o mialgia en la zona, despuésde cada inyección de la vacuna.(6) Cualquier evento adverso: eventos adversos que incluyeneventos adversos locales y/o eventos adversos sistémicos. Loseventos adversos se dividen en graves y no graves. Un eventoadverso grave, según el International Committee onHarmonisation Guidelines (ICH 1997), es cualquier evento queaumenta la mortalidad; es potencialmente mortal; requierehospitalización; origina una discapacidad persistente osignificativa; o cualquier evento médico importante que puedeamenazar al paciente o requiere una intervención preventiva.El resto de los eventos adversos se consideran no graves.(7) Efectividad en relación a los costes.
ESTRATEGIA DE BÚSQUEDA PARA LAIDENTIFICACIÓN DE LOS ESTUDIOS
Se realizaron búsquedas en el Registro Especializado deEnsayos Controlados del Grupo Cochrane de Neonatología(Cochrane Neonatal Group Controlled Trials Register), en elRegistro Especializado de Ensayos Controlados del GrupoCochrane Hepatobiliar (Cochrane Hepato-Biliary GroupControlled Trials Register), El Registro Cochrane Central deEnsayos Controlados (Cochrane Central Register of Controlled
Trial)(CENTRAL) en The Cochrane Library,MEDLINE/PubMed, y en EMBASE. Las estrategias y laduración de las búsquedas se especifican en Tabla 01. Seconsultó con The Cochrane Vaccines Field (Área Cochrane deVacunas) para identificar ensayos adicionales, pero no serecibieron respuestas. Se leyeron las bibliografías de losartículos recuperados para identificar ensayos adicionales. Severificaron las listas de referencias de los artículos pertinentespara identificar ensayos nuevos. Se escribió a los autoresprincipales de los ensayos identificados y a las compañíasfarmacéuticas (SmithKline Beecham and Merck, Sharp &Dohme; GreenCross Vaccine; GlaxoSmithKline; Pasteur; yAbbott) involucradas en la producción de vacunas contra lahepatitis B, para obtener información faltante y ensayosadicionales publicados o no publicados.
MÉTODOS DE LA REVISIÓN
Selección de los ensayos para su inclusiónCL tomó las decisiones sobre la inclusión de los ensayos y laselección fue validada por YG, JB, y CG. No se realizócegamiento de los nombres de los autores, los investigadores,las instituciones y los resultados. Los ensayos excluidos seidentificaron y listaron junto con las razones de exclusión.
Extracción de los datosCL, YG, y JB extrajeron independientemente los datos de losensayos aleatorios incluidos. Se escribió a los autores de losensayos si los datos faltaban en el informe.
Se extrajo: autor principal; número de participantes; criteriosde inclusión y exclusión; estado de HBeAg de la madre; calidadmetodológica (ver abajo); dosificación y tipos de vacunas; sitiode la inyección; programas de vacunación; duración delseguimiento; medidas de resultado; y número y tipo de eventosadversos en el grupo de intervención y el grupo control.
Calidad MetodológicaSe definió la calidad metodológica como la confianza de queel diseño y el informe restringen el sesgo en la comparación dela intervención (Moher 1998; Kjaergard 2001). Debido al riesgode sobrestimación de los efectos de la intervención en losensayos aleatorios con calidad metodológica inadecuada(Schultz 1995; Moher 1998; Kjaergard 2001), la calidadmetodológica se evaluó mediante los siguientes criterios:
Generación de la secuencia de asignación• Adecuada, si la secuencia de asignación fue generada por
ordenador o una tabla de números aleatorios. Seconsideraron adecuados procedimientos tales como elsorteo, moneda al aire, barajada de cartas y el lanzamientode dados, si la persona que realizó el procedimiento noparticipó en el reclutamiento de los participantes.
• Incierto, si el ensayo fue descrito como aleatorio, pero nose describió el método que se utilizó para la generaciónde la secuencia de la asignación.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 3
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
• Inadecuado, si se utilizó para la asignación de los pacientesun sistema que incluía fechas, nombres o números deingresos. Se excluyeron tales estudios cuasialeatorios.
Ocultamiento de la asignación• Adecuado, si la asignación de los pacientes incluyó una
unidad central independiente, un sistema informatizadoin situ sin acceso, botellas o recipientes de fármacos deapariencia idéntica, numerados y preparados por unfarmacéutico o investigador independiente, o sobrescerrados.
• Incierto, si el ensayo fue descrito como aleatorio, pero nose describió el método utilizado para ocultar la asignación.
• Inadecuado, si los investigadores que asignaron a losparticipantes conocían la secuencia de asignación.
Cegamiento (o enmascaramiento)• Adecuado, si se describió el ensayo como doble ciego y
el método de cegamiento incluyó un placebo idéntico ofármacos activos.
• Incierto, si se describió el ensayo como doble ciego, perono se describió el método de cegamiento.
• No realizado, si el ensayo no fue doble ciego.
Seguimiento• Adecuado, si se describió el número y los motivos de los
abandonos y retiros en todos los grupos de intervención,o si se especificó que no hubo abandonos ni retiros.
• Incierto, si el informe dio la impresión de que no huboabandonos ni retiros, pero no se especificó estainformación.
• Inadecuado, si el número o las razones de los abandonosy retiros no fueron descritos.
Los ensayos se definieron post hoc de alta calidad cuando almenos dos de los tres componentes de calidad fueron adecuados:la generación de la secuencia de asignación, el ocultamiento dela asignación y el cegamiento. Esto se debió al hecho de queen sólo un ensayo los tres componentes tenían alta calidad.
Métodos estadísticosSe utilizó Review Manager 4.2. para realizar los metanálisis.Los datos se analizaron con el uso de un modelo de efectosaleatorios (DerSimonian 1986) y un modelo de efectos fijos(DeMets 1987). Cuando los resultados de ambos análisisarrojaron el mismo resultado global en lo que respecta a lasignificación, sólo se informaron los resultados del análisis conel uso del modelo de efectos fijos.
Se expresaron las medidas de resultado binario como riesgosrelativos (RR) con intervalos de confianza (IC) del 95%, y lasmedidas de resultado continuo como diferencia de mediasponderada (DMP) con IC del 95%. Se exploró la presencia deheterogeneidad con el uso de la prueba de ji cuadrado con unasignificación establecida al valor de p < 0,10 y el grado de
heterogeneidad se estimó con el uso de I2 (Higgins 2002).
Se realizó análisis de metarregresión sobre la aparición de
hepatitis B con STATA(r) cuando se incluyeron más de 10
ensayos. El análisis de metarregresión examinó el efecto de laintervención con relación a la calidad metodológica de losensayos, la dosificación de la inmunoglobulina y la vacuna dela hepatitis B, y el tiempo de la inmunización.
Se realizaron análisis de subgrupos para comparar los efectosde las vacunas en madres con HBsAg (+)/HBeAg (+) encomparación con HBsAg (+)/HBeAg (-), la dosis (alta versusbaja), así como la calidad metodológica de los ensayos (altaversus baja). Se estimó la diferencia entre las estimaciones dedos subgrupos según Altman 2003.
En relación con la aparición de la hepatitis B se incluyeronrecién nacidos con datos incompletos o ausentes en los análisisde sensibilidad, los que fueron imputados en los siguientesanálisis (los últimos cuatro fueron análisis del tipo intenciónde tratar [intention-to-treat analyses]):
• Análisis con datos disponibles: sólo datos de los pacientescuyos resultados son conocidos que utilizan comodenominador al número total de pacientes que completaronel ensayo;
• Suposición de un resultado deficiente: los abandonos enel grupo experimental y el grupo control tenían la medidade resultado primaria;
• Suposición de un buen resultado: ninguno de losabandonos en el grupo experimental y en el grupo controltenía la medida de resultado primaria;
• Caso extremo que favorece la intervención experimental:ninguno de los abandonos en el grupo experimental, perotodos en el grupo control tenían la medida de resultadoprimaria;
• Caso extremo que favorece la intervención de control:todos los abandonos en el grupo experimental, peroninguno en el grupo control tenía la medida de resultadoprimaria.
Se utilizó el gráfico en embudo (funnel plot) para obtener unaevaluación visual sobre si las estimaciones del tratamientoestaban asociadas al tamaño del estudio. Se exploró el sesgode publicación y otro sesgo según los métodos de Begg y Egger(Begg 1994; Egger 1997).
DESCRIPCIÓN DE LOS ESTUDIOS
Se identificaron 226 referencias, pero 186 eran referenciasclaramente irrelevantes. Se incluyeron las 40 referenciasrestantes que describían 29 ensayos aleatorios. Estabanpublicados 28 ensayos como artículos completos y un ensayocomo un resumen. No se pudieron extraer datos pertinentes deacuerdo con las medidas de resultado de 3 ensayos (Yeoh 1986;Zhu 1987; Grosheide 1993). Los estudios excluidos aparecenlistados en "Características de los estudios excluidos" con larazón de la exclusión. Las dosis y los esquemas de inmunizaciónen los ensayos incluidos variaron de manera significativa, comose describe más adelante. Las letras mayúsculas de lasreferencias se refieren a los brazos de intervención del ensayo,como se describe en la "Tabla de los estudios incluidos".
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 4
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

Vacuna versus placebo o ninguna intervenciónLa dosis de la vacuna utilizada fue de 3 microgramos (Ip 1989CD), 16 microgramos (Xu 1995 AD), ó 20 microgramos (Liu1987 AB; Xu 1995 BD). Los esquemas de vacunación fueron0-1-6 meses (Liu 1987 AB; Xu 1995 AD/Xu 1995 BD), 0-1-2-6meses (Ip 1989 CD), o 0-1-2-14 meses (Khukhlovich 1996).
VR versus VDPLa dosis de las vacunas fue de 5 microgramos (Lee 1995AB/Lee 1995 CB), 10 microgramos (Pongpipat 1989), ó 20microgramos (Halliday 1992 AB; Zhu 1994). Los esquemas devacunación fueron 0-1-6 meses (Pongpipat 1989; Halliday 1992AB; Zhu 1994) o 0-1-2-12 meses (Lee 1995 AB/Lee 1995 CB).
Vacuna en dosis alta versus vacuna en dosis bajaLas dosis de VDP fueron 10 microgramos, 5 microgramos y 2microgramos (Oon 1986 AB, Oon 1986 CD, Pongpipat 1988;Theppisai 1990). Las dosis de VR fueron 20 microgramos y 10microgramos (Halliday 1992 DC). Los programas de vacunaciónfueron 0-1-6 meses (Halliday 1992 DC), 0-1-2 meses (Oon1986 AB/Oon 1986 CD), o 0-1-2-12 meses (Pongpipat 1988).
VDP en tres dosis más inmunoglobulina de la hepatitis Bversus VDP en dos dosis más inmunoglobulina de la hepatitisBUn ensayo evaluó la VDP en tres dosis más la inmunoglobulinade la hepatitis B versus la VDP en dos dosis más lainmunoglobulina de la hepatitis B (Piazza 1985). Ambos gruposrecibieron 50 UI de inmunoglobulina de la hepatitis B al nacer,luego 5 microgramos de VDP en un período de 5 días y a los2 meses. El grupo experimental recibió una dosis adicional deVDP al mes.
VDP al nacer versus VDP al mesUn ensayo evaluó 20 microgramos de VDP a 0-1-6 meses versus20 microgramos de VDP a 1-2-7 meses (Beasley 1983b). Ambosgrupos recibieron 145 UI de inmunoglobulina de la hepatitis Bal nacer.
Un tipo de VDP versus otro tipo de VDPUn ensayo evaluó diferentes tipos de VDP (VDP1 (NIAID)versus VDP2 (BIVS) (Xu 1995 AB). La dosis fue 16microgramos de VDP1 y 20 microgramos de VDP2. Losesquemas fueron de 0-1-6 meses.
Cuatro vacunaciones con VR versus tres vacunaciones conVRUn ensayo evaluó 4 vacunaciones con VR (0-1-2-12 meses)versus 3 vacunaciones con VR (0-1-6 meses) (Lolekha 2002).La dosis de cada VR fue 5 microgramos.
Una VR versus otra VR con el mismo programa devacunaciónDos ensayos evaluaron diferentes tipos de VR (VR1 (Beijing,China) versus VR2 (Instituto de Medicina Preventiva, China)(Kang 1995) y un ensayo evaluó la vacuna cubana versusEngerix-B (Galban 1992). Dos ensayos evaluaron diferentestipos de VR más la inmunoglobulina de la hepatitis B(Hepavax-Gene versus Engerix-B) (Hieu 2002) y HB-VAX II
versus Engerix-B (Lee 1995 CA/Lee 1995 DE). Las dosis deVR fueron 5 versus 10 microgramos (Lee 1995 CA/Lee 1995DE), 10 versus 10 microgramos (Hieu 2002), o 20 versus 20microgramos (Kang 1995). Los programas de vacunación fueron0-1-6 meses (Kang 1995; Hieu 2002) o 0-1-2-12 meses (Lee1995 CA/Lee 1995 DE).
Inmunoglobulina de la hepatitis B versus placebo o ningunaintervenciónLa dosis de la inmunoglobulina de la hepatitis B varió de 90 a260 UI. Se administró la inmunoglobulina de la hepatitis B enlas primeras 12 horas de vida en 7 ensayos (Beasley 1983aAB/Beasley 1983a CB; Lo 1985 AB/Lo 1985 CB; Theppisai1987; Ip 1989 AC/ Ip 1989 BC; Halliday 1992 CA; Xu 1995CB; Poovorawan 1997), dentro de las primeras 24 horas en 3ensayos (Farmer 1987; Sehgal 1992; Assateerawatt 1993), odentro de las primeras 48 horas en un ensayo (Liu 1987 CA).Los programas de vacunación fueron 0-3-6 meses (Beasley1983a AB/Beasley 1983a CB), 0-6 semanas -6 meses (Farmer1987), 0-1-6 meses (Ip 1989 AC/Ip 1989 BC; Theppisai 1987;Xu 1995 CB), 0-1-2-6 meses ( Liu 1987 CA), 0-2-6-10 semanas(Lo 1985 AB/Lo 1985 CB), y 0-4-8 semanas (Sehgal 1992).
Inmunoglobulina de la hepatitis B múltiple versusinmunoglobulina de la hepatitis B simpleUn ensayo comparó 5 microgramos de VDP a 2-6-10 semanasmás 50 UI de inmunoglobulina de la hepatitis B al nacer con osin inmunoglobulina de la hepatitis B adicional al mes (Lo 1985CA). Un ensayo comparó 3 microgramos de VDP a 1-2-6 mesesmás 200 UI de inmunoglobulina de la hepatitis B al nacer cono sin inmunoglobulina de la hepatitis B adicional a 1-2-3-4-5-6meses (Ip 1989 AB)
VDP más inmunoglobulina de la hepatitis B versus placeboo ninguna intervenciónUn ensayo comparó 200 UI de inmunoglobulina de la hepatitisB a 0-1-2-3-4-5-6 meses más 3 microgramos de VDP a 0-1-2-6meses versus 200 UI de inmunoglobulina de la hepatitis B alnacer más 3 microgramos de VDP a 0-1-2-6 meses versusplacebo (Ip 1989 AD/Ip 1989 BD). Un ensayo comparó 20microgramos de VDP a 0-1-2-6 meses más inmunoglobulinade la hepatitis B al nacer con placebo (Liu 1987 CB). Un ensayocomparó 20 microgramos de VDP a 0-1-6 meses más 250 UIde inmunoglobulina de la hepatitis B al nacer versus placebo(Xu 1995 CD). Se administró la inmunoglobulina de la hepatitisB dentro de las primeras 12 horas (Ip 1989 AD/Ip 1989 BD),o dentro de las primeras 24 horas (Xu 1995 CD), y dentro delas primeras 48 horas (Liu 1987 CB).
Algunos ensayos tenían varios brazos de intervención. Paraobtener detalles de los ensayos incluidos se proporcionó Tabla02 mediante un registro de las comparaciones pertinentes y delos ensayos que evaluaron esta comparación. Las letrasmayúsculas que se encuentran después del año de publicaciónen las referencias se refieren a los brazos de comparación delensayo individual.
Estado del HBeAg de la madre
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 5
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

Dieciocho ensayos incluyeron sólo madres con pruebas positivaspara el HBeAg. Tres ensayos incluyeron madres con pruebaspositivas o negativas para el HBeAg (Lee 1995 AB; Oon 1986AB; Xu 1995 AB), y en 8 ensayos no se informó el estado delHBeAg de la madre.
Peso al nacer de los recién nacidosDiez ensayos informaron la exclusión de los recién nacidos conbajo peso al nacer. Los límites para la exclusión variaron de 1600 a 3 000 g. Los 19 ensayos restantes no informaron criteriosde exclusión relacionados con el peso al nacer. La duraciónpromedio del seguimiento fue 19 meses (rango de 6 a 60 meses).
CALIDAD METODOLÓGICA
La generación de la secuencia de asignación fue adecuada en6 ensayos (Piazza 1985; Oon 1986 AB/Oon 1986 CD; Farmer1987; Halliday 1992 AB/Halliday 1992 CA/Halliday 1992 DC;Assateerawatt 1993; Hieu 2002).La asignación al tratamiento estaba adecuadamente oculta en6 ensayos (Ip 1989 AD/Ip 1989 BD/Ip 1989 CD; Piazza 1985;Liu 1987 AB/Liu 1987 CA/Liu 1987 CB; Halliday 1992AB/Halliday 1992 CA/Halliday 1992 DC; Grosheide 1993;Hieu 2002).En 3 ensayos se informó un método adecuado de doblecegamiento (Ip 1989 AD/Ip 1989 BD/Ip 1989 CD; Liu 1987AB/Liu 1987 CA/Liu 1987 CB; Halliday 1992 AB/Halliday1992 CA/Halliday 1992 DC).De acuerdo con los criterios, se clasificaron 5 ensayos comoensayos de alta calidad (Ip 1989 AD/Ip 1989 BD/Ip 1989 CD;Piazza 1985; Liu 1987 AB/Liu 1987 CB; Halliday 1992AB/Halliday 1992 CA/Halliday 1992 DC; Hieu 2002).El número y los motivos de los abandonos y retiros fueroninformados de manera adecuada en 6 ensayos (Beasley 1983aAB/Beasley 1983a CB/Beasley 1983b; Piazza 1985; Theppisai1987; Halliday 1992 AB/Halliday 1992 CA/Halliday 1992 DC;Grosheide 1993).
RESULTADOS
Vacunas contra la hepatitis B versus placebo o ningunaintervención (Comparación 01-01 a 01-05)En la comparación con placebo/ninguna intervención, lavacunación contra la hepatitis B disminuyó significativamenteel riesgo de aparición de hepatitis B (RR 0,28; IC del 95%: 0,20a 0,40; 4 ensayos). El análisis mostró heterogeneidad (P = 0,07;
I2 = 54,2%). Los resultados de los análisis de sensibilidad conrespecto a los abandonos fueron consistentes. Los análisis deVDP y VR individualmente mostraron que ambas vacunasdisminuyeron significativamente el riesgo de aparición dehepatitis B.
Los análisis de subgrupos no encontraron una diferenciasignificativa entre los ensayos de alta y baja calidad, el estadode HBeAg de la madre o el momento de administración de la
vacuna (pruebas de interacción; P = 0,25; 0,07 y 0,11respectivamente). El análisis de subgrupos post hoc de acuerdocon los programas de vacunación (0-1-6 meses versus 0-1-2-6o 12 meses) no mostró diferencias significativas (prueba deinteracción, P = 0,75). No se informaron datos sobre eventosadversos.
VR versus VDP (Comparación 02-01 a 02-05)No se encontraron diferencias significativas entre la VR y laVDP en la aparición de hepatitis B (RR 1,00; IC del 95%: 0,70
a 1,42; 4 ensayos). La heterogeneidad fue moderada (I2 =29,4%). Los resultados de los análisis de sensibilidad conrespecto a los abandonos confirmaron el resultado. Los análisisde subgrupos no encontraron una diferencia significativa conrespecto a la calidad metodológica o al estado de HBeAg de lamadre (ambas pruebas de interacción, P = 0,21).
Significativamente menos recién nacidos con VR encomparación con VDP tuvieron anti-HBs menores de 10 UI/L(RR 0,51; IC del 95%: 0,36 a 0,72; 3 ensayos).
Vacuna con dosis alta versus vacuna con dosis baja(Comparación 03-01 a 03-05)No se encontraron diferencias estadísticas en la aparición dehepatitis B al comparar la vacuna con dosis alta versus la vacunacon dosis baja (VDP: RR 0,97; IC del 95%: 0,55 a 1,68; 3ensayos; VR: RR 0,78; IC del 95%: 0,31 a 1,94; 1 ensayo). Nohubo diferencias significativas entre la vacuna con dosis altaversus la vacuna con dosis baja en el título de anti-HBs menorde 10 UI/L (RR 1,02; IC del 95%: 0,82; 1,27; 2 ensayos).
VDP en 3 dosis versus VDP en 2 dosis (Comparación 04-01a 04-02)La VDP en 3 dosis más la inmunoglobulina de la hepatitis Bno previno significativamente la aparición de hepatitis B encomparación con la VDP en 2 dosis más la inmunoglobulinade la hepatitis B (RR 0,50; IC del 95%: 0,05 a 5,28; 1 ensayo).Sin embargo, la VDP de tres dosis más la inmunoglobulina dela hepatitis B resultaron en un número significativamenteinferior de recién nacidos con anti-HBs menor de 10 UI/L encomparación con la VDP en dos dosis más la inmunoglobulinade la hepatitis B (RR 0,05; IC del 95%: 0,00 a 0,78; 1 ensayo).
VDP al nacer versus VDP al mes (Comparación 05-01)La VDP administrada por primera vez al nacer no difiriósignificativamente de la VDP administrada por primera vez almes de vida, con respecto al número de recién nacidos que tuvohepatitis B (RR 0,70; IC del 95%: 0,18 a 2,77; 1 ensayo).
Un tipo de VDP versus otro tipo de VDP (Comparación06-01)Un ensayo comparó dos tipos diferentes de VDP y no seencontraron diferencias significativas en la aparición de hepatitisB (Xu 1995 AB).
Vacunación con VR en 4 dosis versus vacunación con VRen 3 dosis (Comparación 07-01 a 07-02)Un ensayo (Lolekha 2002) comparó un tipo de VR con 4vacunaciones (0-1-2-12 meses) versus la misma VR con 3
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 6
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
vacunaciones (0-1-6 meses). No se encontraron diferenciassignificativas en la aparición de hepatitis B (RR 1,49; IC del95%: 0,51 a 4,37) o el título de anti-HBs menor de 10 UI/L(RR 0,53; IC del 95%: 0,10 a 2,77).
Un tipo de VR versus otro tipo de VR con el mismoprograma de vacunación (Comparación 08-01 a 08-02)Se evaluaron VR de distintos fabricantes y no se encontrarondiferencias significativas en la aparición de hepatitis B o elanti-HBs menor de 10 UI/L.
Inmunoglobulina de la hepatitis B versus placebo o ningunaintervención (Comparación 09-01 a 09-08)En términos generales, la inmunoglobulina de la hepatitis Bdisminuyó significativamente el riesgo de aparición de hepatitisB en los recién nacidos (RR 0,52; IC del 95%: 0,44 a 0,63; 11ensayos). En comparación con placebo/ninguna intervención,la inmunoglobulina de la hepatitis B sola disminuyósignificativamente la aparición de hepatitis B (RR 0,50; IC del95%: 0,41 a 0,60; 1 ensayo). En comparación con la vacunación,la vacunación más la administración de inmunoglobulina de lahepatitis B fue igualmente superior (RR 0,54; IC del 95%: 0,41a 0,73; 10 ensayos). Los análisis de sensibilidad con respectoa los abandonos fueron consistentes, lo que indicó la solidezde los resultados. En los análisis de metarregresión, ningunade las características del ensayo (calidad metodológica,dosificación de la inmunoglobulina de la hepatitis B o tiempode la inyección de inmunoglobulina de la hepatitis B) se asocióde manera significativa con el efecto de la inmunoglobulina dela hepatitis B (P = 0,92; 0,67 y 0,79; respectivamente). Losanálisis de subgrupos no encontraron una diferencia significativaentre los ensayos de calidad alta y calidad baja, el estado deHBeAg de la madre o el tiempo de la inyección deinmunoglobulina de la hepatitis B (pruebas de interacción; P =0,70; 0,62 y 0,63 respectivamente).
La inmunoglobulina de la hepatitis B no tuvo efectossignificativos sobre el número de recién nacidos con un títulode anti-HBs menor de 10 UI/L (RR 1,55; IC del 95%: 0,89 a2,73; 4 ensayos).
Algunos ensayos informaron eventos adversos. Cuando losautores informaron los datos de los eventos adversos noespecificaron en qué grupo de intervención ocurrieron. Porconsiguiente, no se pudo realizar un metanálisis con los eventosadversos. En un ensayo (Beasley 1983a AB/Beasley 1983aCB), murió un recién nacido que recibió la inmunoglobulinade la hepatitis B. La muerte no pareció estar relacionada con lainmunoglobulina de la hepatitis B.
Los gráficos de Egger y de Begg y sus correspondientes pruebassobre la aparición de la hepatitis B no proporcionaron pruebasde asimetría (prueba de Egger, P = 0,31; prueba de Begg, P =0,23).
Administración de la inmunoglobulina de la hepatitis Bmúltiple versus de la inmunoglobulina de la hepatitis Bsimple (Comparación 10-01)
La inmunoglobulina de la hepatitis B múltiple más VDP versusla inmunoglobulina de la hepatitis B simple más VDP nodisminuyó significativamente el riesgo de aparición de hepatitisB (RR 0,87; IC del 95%: 0,30 a 2,47; 2 ensayos) sin
heterogeneidad (I2 = 0%).
VDP más inmunoglobulina de la hepatitis B versus placeboo ninguna intervención (Comparación 11-01 a 11-06)En comparación con placebo/ninguna intervención la VDP másinmunoglobulina de la hepatitis B disminuyeronsignificativamente la aparición de hepatitis B (RR 0,08; IC del95%: 0,03 a 0,17; 3 ensayos). Los análisis de sensibilidadconfirmaron la solidez del resultado. Los análisis de subgruposno encontraron una diferencia significativa entre los ensayosde calidad alta y calidad baja, el estado de HBeAg de la madreo el tiempo de la inyección de inmunoglobulina de la hepatitisB (pruebas de interacción; P = 0,13; 0,28 y 0,22respectivamente).
Un ensayo informó el número de eventos adversos: 3 de los 71recién nacidos que recibieron vacunación versus 5 de los 34del grupo control (Ip 1989 AD/Ip 1989 BD). Los resultados nomostraron una diferencia significativa (0,29; 0,07 a 1,13)
DISCUSIÓN
Esta revisión sistemática demuestra que la vacuna contra lahepatitis B, la inmunoglobulina de la hepatitis B o lacombinación de la vacuna más la inmunoglobulina de lahepatitis B administradas a los recién nacidos de madres conpruebas positivas para el HBsAg previenen la aparición dehepatitis B. Además, la combinación de la vacuna más lainmunoglobulina de la hepatitis B fue superior a la vacuna sola.Estos beneficios no estuvieron asociados significativamentecon la calidad metodológica de los ensayos, el estado de HBeAgde la madre, el tiempo de la inmunización o el número de reciénnacidos que abandonaron.
Esta revisión presenta varias limitaciones potenciales. Primero,algunos análisis incluyen pocos ensayos y un pequeño númerode recién nacidos. Segundo, la mayoría de los ensayos eran decalidad metodológica baja. Sin embargo, no se encontró unaasociación fuerte entre la calidad metodológica y los resultadosdel ensayo. Estos hallazgos apoyan la solidez de los resultadosde la presente revisión, pero no excluyen la posibilidad de sesgo(Schultz 1995; Moher 1998; Kjaergard 2001; Als-Nielsen 2004).Tercero, aunque no se encontraron asimetrías en los gráficosen embudo (funnel plots), no se puede excluir el sesgo depublicación. Cuarto, sólo pocos investigadores respondieron ala solicitud de información adicional y a menudo la respuestafue que se habían perdido los detalles de los datos. Quinto, lamayoría de los ensayos sólo informó medidas de resultadoalternativas (estado de HBsAg o título de anti-HBs) y nomedidas de resultado clínicas a largo plazo. Vale la penamencionar el hecho de que un ensayo con seguimiento a largoplazo encontró más pacientes con hepatitis crónica en el grupo
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 7
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

de VDP más inmunoglobulina de la hepatitis B en comparacióncon el grupo de VDP (Ip 1989 AC). Tal aumento de la hepatitiscrónica puede deberse a la contaminación de la inmunoglobulinade la hepatitis B con el virus de la hepatitis C.
Los resultados de esta revisión demuestran convincentementeque la vacunación contra la hepatitis B disminuye la infecciónpor hepatitis B en los recién nacidos de madres con pruebaspositivas al antígeno de superficie de la hepatitis B. No seencontraron diferencias significativas entre la VR y la VDP enlas infecciones por hepatitis B (RR 1,00; IC del 95%: 0,70 a1,42). Sin embargo, fue mayor el número de recién nacidos conVDP que no logró un título de anti-HBs mayor de 10 UI/L (RR1,96; IC del 95%: 1,39 a 2,78). La ventaja de la VR quizá sedeba a la diferencia en las características químicas y físicas delos antígenos que componen las vacunas (Heijtink 2002). LaVR es la vacuna que se utiliza en los países de altos ingresosdebido al temor a la infección por el virus de lainmunodeficiencia humana y otras infecciones, incluidas lasencefalopatías espongiformes transmisibles (MacGregor 2004).El resultado de esta revisión parece apoyar la introducción delas VR en la práctica clínica.
El régimen de prevención recomendado para la profilaxisinmune difiere entre los países (David 1996; CDC 1999). Deigual manera, en los ensayos incluidos las dosis y los esquemasinformados variaron de manera significativa (Tabla 02). Engeneral, no se pudo demostrar diferencias significativas entrelas diversas dosis, programas, formas de VDP y VR sobre laaparición de hepatitis B. Además, los análisis de subgrupos nomostraron asociaciones fuertes entre el tiempo de la inyección(en 12, 24 o 48 horas) y la magnitud de los efectos. El númerode recién nacidos evaluado en estas comparaciones fue pequeño.Por consiguiente, los ensayos futuros deben ser mucho másgrandes para que pueda establecerse que existe equivalencia ono inferioridad.
Los metanálisis demostraron que la inmunoglobulina de lahepatitis B, sola o cuando se administra junto con la vacunacontra la hepatitis B, disminuyó significativamente el riesgo deinfección por hepatitis B (RR 0,52; IC del 95%: 0,44 a 0,63).Un reciente estudio no aleatorio no informó beneficios deincorporar inmunoglobulina de la hepatitis B a la vacuna enmadres con pruebas negativas para el HBeAg (Yang 2003).Solamente un ensayo pequeño de los 11 ensayos revisadosincluyó recién nacidos de madres con pruebas negativas parael HBeAg (Xu 1995 AB). Como era de esperar, el análisis desubgrupos no encontró diferencias estadísticamentesignificativas entre los recién nacidos de madres con pruebasnegativas y madres con pruebas positivas para el HBeAg. Enconsecuencia, parece justificado realizar más ensayos aleatoriosque agreguen la inmunoglobulina de la hepatitis B a la vacunapara los recién nacidos de madres con pruebas negativas parael HBeAg. Se debe tener en cuenta que la inmunoglobulina dela hepatitis B, así como la VDP, tiene el potencial de transmitirinfecciones hematógenas (CDC 1991).
Pocos ensayos informaron los eventos adversos. De acuerdocon lo que se ha informado, la vacuna contra la hepatitis B y lainmunoglobulina de la hepatitis B parecen seguras. Estosresultados están en conformidad con dos revisiones Cochranerecientes sobre la vacunación contra la hepatitis B para pacientesen diálisis y profesionales de la salud (Niu 1996; Chen 2005).Además, varios estudios de cohortes encontraron que lavacunación contra la hepatitis B se tolera bien y que los eventosadversos graves son raros (ICH 1997; Niu 1999; DuVernoy2000; Kojouharova 2001; Lewis 2001; Bohlke 2003; Deeks2003). Sin embargo, un estudio de cohortes halló que la vacunaaumentó el riesgo de artritis crónica y de infecciones agudasdel oído (Fisher 2001). No se puede determinar si este resultadoes fiable debido a la debilidad metodológica de los estudios decohortes (CDC 1999). Por otro lado, los ensayos clínicosaleatorios pueden pasar por alto los eventos adversos, debidoal número relativamente escaso de participantes y/o a lanotificación deficiente de los eventos adversos (Hayashi 1996;Ioannidis 2001; Etminan 2004). Los ensayos adicionales debencentrarse en estos eventos adversos según las guías de laICH-GCP (ICH 1997).
El riesgo de transmisión perinatal por madres con pruebasnegativas para el HBeAg se considera mucho menor que pormadres con pruebas positivas para el HBeAg (Okada 1976). Sise infectan, los recién nacidos de madres con pruebas negativaspara el HBeAg a menudo presentan una infección asintomática(Dusheiko 1998). Los resultados de esta revisión se basanprincipalmente en la profilaxis inmune de los recién nacidosde madres con pruebas positivas para el HBsAg y el HBeAg.Las pruebas provenientes de ensayos clínicos aleatorios soninsuficientes para apoyar o refutar la profilaxis inmune de losrecién nacidos de madres con pruebas negativas al antígeno ede la hepatitis B. Por consiguiente, la aplicabilidad de losresultados es limitada en las madres con pruebas negativas parael HBeAg, que se encuentran en proporciones altas p.ej., enEstados Unidos y Europa del norte (Funk 2002).
Los estudios de coste-efectividad indican que la vacunacióncontra la hepatitis B para los recién nacidos de madres conpruebas positivas para el HBsAg es efectiva en función de loscostes en los países con prevalencia baja (Bloom 1993; Tormans1993; Da Villa 1999; Harris 2001), intermedia y alta de hepatitisB (Hall 1993; Liu 1995; Margolis 1995; Sriprakash 1997). Nose identificaron estudios de coste-efectividad que evaluaran losefectos de agregar inmunoglobulina de la hepatitis B a lavacuna. Como la inmunoglobulina de la hepatitis B parece capazde disminuir el riesgo de infección por hepatitis B, parecejustificada la necesidad de realizar estudios de coste-efectividadbasados en ensayos aleatorios.
No se incluyeron 2 ensayos que examinaron una nueva manerade prevenir la transmisión vertical de la hepatitis B, por no estarde acuerdo con los criterios de inclusión de esta revisión (Lee2004). Los dos ensayos asignaron al azar a mujeres embarazadascon pruebas positivas para el antígeno de superficie de lahepatitis B a recibir la inmunoglobulina de la hepatitis B versus
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 8
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

ninguna intervención antes del parto (Zhu 1997; Li 2003). Enel grupo que recibió inmunoglobulina hubo menos reciénnacidos con pruebas positivas al antígeno de superficie de lahepatitis B durante el seguimiento. La calidad metodológica delos dos ensayos fue baja. Además, las madres están en riesgode desarrollar una enfermedad por complejos inmunes debidoa que la inmunoglobulina de la hepatitis B reacciona con suspropios antígenos de superficie de la hepatitis B circulantes.Por consiguiente, se necesitan más ensayos antes de que sepueda adoptar esta intervención.
CONCLUSIONES DE LOS AUTORES
Implicaciones para la práctica
Madres con pruebas positivas para el HBsAg y el HBeAgLas pruebas indican que la vacuna contra la hepatitis B, lainmunoglobulina de la hepatitis B y la combinación de la vacunacontra la hepatitis B y la inmunoglobulina de la hepatitis Bdisminuyen el riesgo de transmisión perinatal de la hepatitis Ben los recién nacidos de madres con pruebas positivas para elHBsAg que también tienen pruebas positivas para el HBeAg.Sin embargo, el régimen de tratamiento óptimo continúaincierto.
Madres con pruebas positivas para el HBsAg y con pruebasnegativas para el HBeAgNo hay pruebas suficientes para apoyar o refutar el uso de lavacuna contra la hepatitis B, la inmunoglobulina de la hepatitisB y la combinación de la vacuna contra la hepatitis B y lainmunoglobulina en recién nacidos de madres con pruebaspositivas para el HBsAg y con pruebas negativas para elHBeAg. El número necesario a tratar para prevenir un eventode hepatitis B es probablemente mucho más grande que en lasmadres con pruebas positivas para el HBsAg y el HBeAg.
Implicaciones para la investigación
Se deben estudiar con mayor profundidad los potencialeseventos adversos relacionados con la profilaxis de la hepatitisB, especialmente el riesgo de infección del oído y de artritiscrónica. Se debe examinar en ensayos clínicos aleatorios dealta calidad la nueva forma de prevenir la hepatitis B en reciénnacidos, la administración de la inmunoglobulina de la hepatitisB a la madre embarazada. Se debe evaluar con mayorprofundidad el coste-efectividad de la vacunación contra lahepatitis B y la inmunoglobulina de la hepatitis B en base a losresultados de ensayos clínicos aleatorios. Los ensayosadicionales deben examinar los efectos de la vacuna contra lahepatitis B y la inmunoglobulina de la hepatitis B en reciénnacidos de madres con pruebas positivas para el HBsAg quetienen pruebas negativas para el HBsAg. Los ensayosadicionales deben examinar los efectos de la vacuna contra lahepatitis B y la inmunoglobulina de la hepatitis B en reciénnacidos prematuros y de bajo peso al nacer de madres conpruebas positivas para el HBsAg. Los ensayos futuros debenexaminar si la vacuna contra la hepatitis B más múltiples dosis
de inmunoglobulina de la hepatitis B es superior a la vacunacontra la hepatitis B más una sola dosis de inmunoglobulina dela hepatitis B.
AGRADECIMIENTOS
Se agradece a Jefferson, M Pratt, J Buttery y N El-Shukri, queparticiparon en la elaboración del primer protocolo Cochranesobre este tema. Se agradece al Dr. Nikolova, del GrupoCochrane Hepatobiliar (Cochrane Hepato-Biliary Group), porla traducción de un ensayo en idioma ruso y la recuperación deartículos. Damos las gracias a D Haughton, Grupo Cochranede Neonatología, por la recuperación de artículos. Damos lasgracias a Y Poovorawan y a M Piazza por aclarar informaciónsobre sus ensayos. Se agradece a A Dutta, MM Hassan y SDLee por proporcionar ayuda para identificar los autores de losensayos, y a JU Olsen, GlaxoSmithKline, Dinamarca, porproporcionar información sobre ensayos clínicos aleatorios.
POTENCIAL CONFLICTO DE INTERÉS
Ninguno conocido.
NOTAS
1. Un protocolo de una revisión sistemática sobre este tema sepublicó por primera vez en el Número 2 de 1998 de TheCochrane Library y continuó su publicación hasta el Número1 de 2004 con el título "Vacunas para la prevención de lahepatitis B en recién nacidos de alto riesgo". Los autores,Jefferson TO, Pratt M, Buttery J, y El-Shukri N, hanabandonado la revisión sistemática. Esta revisión requirió unaactualización del protocolo y fue realizada por un nuevo equipode revisores, ahora integrado por Lee C, Gong Y, Brok J, BoxallEH y Gluud C.2. Se modificó la definición de aparición de hepatitis B comose muestra en la presente revisión.3. En este protocolo se exigió que cada ensayo debía evaluarla medida de resultado serológica en dos y más muestrasconsecutivas de sangre. Se comprendió que en la mayoría delos ensayos este requisito no se podía alcanzar. Por consiguientese decidió ignorar este requisito.
FUENTES DE FINANCIACIÓN
Recursos externos
• S.C. Van Foundation DENMARK
Recursos internos
• Public Health Laboratory Service UK
• Tri-Service General Hospital TAIWAN
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 9
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

• Copenhagen Trial Unit, Centre for Clinical Intervention Research, H:S Rigshospitalet DENMARK
✦
REFERENCIAS
Referencias de los estudios incluidos en esta revisión
Assateerawatt 1993 {published data only}Assateerawatt A, Tanphaichitr VS, Suvatte V, Yodthong S. Immunogenicityand efficacy of a recombinant DNA hepatitis B vaccine, GenHevac BPasteur in high risk neonates, school children and healthy adults. AsianPacific Journal of Allergy Immunology 1993;11(1):85-91.
Beasley 1983a AB {published data only}*Beasley RP, Hwang LY, Stevens CE, Lin CC, Hsieh FJ, Wang KY, et al.Efficacy of hepatitis B immune globulin for prevention of perinataltransmission of the hepatitis B virus carrier state: final report of arandomized double-blind, placebo-controlled trial. Hepatology1983;3(2):135-41.
Beasley RP, Hwang LY, Szmuness W, Stevens CE, Lin CC, Hsieh FJ, etal. HBIG prophylaxis for perinatal HBV infections - final report of theTaiwan trial. Developmental Biology Standard 1983;54:363-75.
Beasley 1983a CB {published data only}*Beasley RP, Hwang LY, Stevens CE, Lin CC, Hsieh FJ, Wang KY, et al.Efficacy of hepatitis B immune globulin for prevention of perinataltransmission of the hepatitis B virus carrier state: final report of arandomized double-blind, placebo-controlled trial. Hepatology1983;3(2):135-41.
Beasley RP, Hwang LY, Szmuness W, Stevens CE, Lin CC, Hsieh FJ, etal. HBIG prophylaxis for perinatal HBV infections - final report of theTaiwan trial. Developmental Biology Standard 1983;54:363-75.
Beasley 1983b {published data only}Beasley RP, Hwang LY, Lee GC, Lan CC, Roan CH, Huang FY, et al.Prevention of perinatally transmitted hepatitis B virus infections withhepatitis B virus infections with hepatitis B immune globulin and hepatitisB vaccine. Lancet 1983;2(8359):1099-102.
Farmer 1987 {published data only}Farmer K, Gunn T, Woodfield DG. A combination of hepatitis B vaccineand immunoglobulin does not protect all infants born to hepatitis B e antigenpositive mothers. New Zealand Medical Journal 1987;100(827):412-4.
Garcia 1992 {published data only}Garcia EG, Gonzalez JRB, Guillot CC, Curbelo GT, Griego AG, GonzalezMGD. [Field trial of the Cuban recombinant vaccine against hepatitis B(Heberbiovac HB). Study in newborn infants born to AgsHB+ mothers].Revista Cubana de Medicina Tropical 1992;44(2):149-57.
Grosheide 1993 {published data only}*Grosheide PM, del Canho R, Heijtink RA, Nuijten AS, Zwijnenberg J,Banffer JR, et al. Passive-active immunization in infants of hepatitis Beantigen-positive mothers. Comparison of the efficacy of early and delayedactive immunization. American Journal of Diseases of Children1993;147(12):1316-20.
Mazel JA, Schalm SW, de Gast BC, Nuijten AS, Heijtink RA, Botman MJ,et al. Passive-active immunisation of neonates of HBsAg positive carriermothers: preliminary observations. British Medical Journal (ClinicalResearch Ed.) 1984;288(6416):513-5.
Halliday 1992 AB {published data only}Halliday ML, Kang LY, Rankin JG, Coates RA, Corey PN, Hu ZH, et al.An efficacy trial of a mammalian cell-derived recombinant DNA hepatitisB vaccine in infants born to mothers positive for HBsAg, in Shanghai,China. International Journal of Epidemiology 1992;21(3):564-73.
Halliday 1992 CA {published data only}Halliday ML, Kang LY, Rankin JG, Coates RA, Corey PN, Hu ZH, et al.An efficacy trial of a mammalian cell-derived recombinant DNA hepatitisB vaccine in infants born to mothers positive for HBsAg, in Shanghai,China. International Journal of Epidemiology 1992;21(3):564-73.
Halliday 1992 DC {published data only}Halliday ML, Kang LY, Rankin JG, Coates RA, Corey PN, Hu ZH, et al.An efficacy trial of a mammalian cell-derived recombinant DNA hepatitisB vaccine in infants born to mothers positive for HBsAg, in Shanghai,China. International Journal of Epidemiology 1992;21(3):564-73.
Hieu 2002 {published data only}Hieu NT, Kim KH, Janowicz Z, Timmermans I. Comparative efficacy,safety and immunogenicity of Hepavax-Gene and Engerix-B, recombinanthepatitis B vaccines, in infants born to HBsAg and HBeAg positive mothersin Vietnam: an assessment at 2 years. Vaccine 2002;20(13-14):1803-8.
Ip 1989 AB {published data only}*Ip HM, Lelie PN, Wong VC, Kuhns MC, Reesink HW. Prevention ofhepatitis B virus carrier state in infants according to maternal serum levelsof HBV DNA. Lancet 1989;1(8635):406-10.
Ip HM, Wong VC, Lelie PN, Reesink HW, Schaasberg W, Yeung CY, etal. Hepatitis B infection in infants after neonatal immunization. ActaPaediatric Japanese 1989;31(6):654-8.
Ip 1989 AC {published data only}*Ip HM, Lelie PN, Wong VC, Kuhns MC, Reesink HW. Prevention ofhepatitis B virus carrier state in infants according to maternal serum levelsof HBV DNA. Lancet 1989;1(8635):406-10.
Ip HM, Wong VC, Lelie PN, Reesink HW, Schaasberg W, Yeung CY, etal. Hepatitis B infection in infants after neonatal immunization. ActaPaediatric Japanese 1989;31(6):654-8.
Ip 1989 AD {published data only}Ip HM, Lelie PN, Wong VC, Kuhns MC, Reesink HW. Prevention ofhepatitis B virus carrier state in infants according to maternal serum levelsof HBV DNA. Lancet 1989;1(8635):406-10.
Ip HM, Wong VC, Lelie PN, Reesink HW, Schaasberg W, Yeung CY, etal. Hepatitis B infection in infants after neonatal immunization. ActaPaediatric Japanese 1989;31(6):654-8.
*Wong VC, Ip HM, Reesink HW, Lelie PN, Reerink-Brongers EE, YeungCY, et al. Prevention of the HBsAg carrier state in newborn infants ofmothers who are chronic carriers of HBsAg and HBeAg by administrationof hepatitis-B vaccine and hepatitis-B immunoglobulin. Double-blindrandomised placebo-controlled study. Lancet 1984;1(8383):921-6.
Ip 1989 BC {published data only}*Ip HM, Lelie PN, Wong VC, Kuhns MC, Reesink HW. Prevention ofhepatitis B virus carrier state in infants according to maternal serum levelsof HBV DNA. Lancet 1989;1(8635):406-10.
Ip HM, Wong VC, Lelie PN, Reesink HW, Schaasberg W, Yeung CY, etal. Hepatitis B infection in infants after neonatal immunization. ActaPaediatric Japanese 1989;31(6):654-8.
Ip 1989 BD {published data only}Ip HM, Lelie PN, Wong VC, Kuhns MC, Reesink HW. Prevention ofhepatitis B virus carrier state in infants according to maternal serum levelsof HBV DNA. Lancet 1989;1(8635):406-10.
Ip HM, Wong VC, Lelie PN, Reesink HW, Schaasberg W, Yeung CY, etal. Hepatitis B infection in infants after neonatal immunization. ActaPaediatric Japanese 1989;31(6):654-8.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 10
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

*Wong VC, Ip HM, Reesink HW, Lelie PN, Reerink-Brongers EE, YeungCY, et al. Prevention of the HBsAg carrier state in newborn infants ofmothers who are chronic carriers of HBsAg and HBeAg by administrationof hepatitis-B vaccine and hepatitis-B immunoglobulin. Double-blindrandomised placebo-controlled study. Lancet 1984;1(8383):921-6.
Ip 1989 CD {published data only}Ip HM, Lelie PN, Wong VC, Kuhns MC, Reesink HW. Prevention ofhepatitis B virus carrier state in infants according to maternal serum levelsof HBV DNA. Lancet 1989;1(8635):406-10.
Ip HM, Wong VC, Lelie PN, Reesink HW, Schaasberg W, Yeung CY, etal. Hepatitis B infection in infants after neonatal immunization. ActaPaediatric Japanese 1989;31(6):654-8.
*Wong VC, Ip HM, Reesink HW, Lelie PN, Reerink-Brongers EE, YeungCY, et al. Prevention of the HBsAg carrier state in newborn infants ofmothers who are chronic carriers of HBsAg and HBeAg by administrationof hepatitis-B vaccine and hepatitis-B immunoglobulin. Double-blindrandomised placebo-controlled study. Lancet 1984;1(8383):921-6.
Kang 1995 {published data only}*Kang P, Shen XM, Yu HM. [Study on the efficacy of geneticallyengineered vaccines against hepatitis B for interruption of perinataltransmission]. Zhonghua Hu Li Za Zhi 1995;30(7):390-2.
Khukhlovich 1996 {published data only}Khukhlovich PA, Shakhgil'dian IV, Narkevich MI, Anan'ev VA, KuzinSN, Sergeeva NA, et al. [The vaccinal prophylaxis of hepatitis B amongchildren born to mothers with persistent HBs-antigenemia]. ZhurnalMikrobiologii, Epidemiologii, i Immunobiologii 1996;2:55-9.
Kuru 1995 AB {published data only}Kuru U, Turan O, Kuru N, Saglam Z, Alver A. Results of vaccinated infantsborn to HBsAg-positive mothers with different hepatitis B vaccines anddoses. The Turkish Journal of Pediatrics 1995;37(2):93-102.
Kuru 1995 AC {published data only}Kuru U, Turan O, Kuru N, Saglam Z, Alver A. Results of vaccinated infantsborn to HBsAg-positive mothers with different hepatitis B vaccines anddoses. The Turkish Journal of Pediatrics 1995;37(2):93-102.
Kuru 1995 BC {published data only}Kuru U, Turan O, Kuru N, Saglam Z, Alver A. Results of vaccinated infantsborn to HBsAg-positive mothers with different hepatitis B vaccines anddoses. The Turkish Journal of Pediatrics 1995;37(2):93-102.
Lee 1995 AB {published data only}Lee CY, Huang LM, Chang MH, Hsu CY, Wu SJ, Sung JL, et al. Theprotective efficacy of recombinant hepatitis B vaccine in newborn infantsof hepatitis B e antigen-positive-hepatitis B surface antigen carrier mothers.The Pediatric infectious Disease Journal 1991;10(4):299-303.
Lee PI, Lee CY, Huang LM, Chang MH. Long-term efficacy of recombinanthepatitis B vaccine and risk of natural infection in infants born to motherswith hepatitis B e antigen. The Journal of Pediatrics 1995;126(5 Pt1):716-21.
*Lee PI, Lee CY, Huang LM, Chen JM, Chang MH. A follow-up study ofcombined vaccination with plasma-derived and recombinant hepatitis Bvaccines in infants. Vaccine 1995;13(17):1685-9.
Lee 1995 CA {published data only}Lee CY, Huang LM, Chang MH, Hsu CY, Wu SJ, Sung JL, et al. Theprotective efficacy of recombinant hepatitis B vaccine in newborn infantsof hepatitis B e antigen-positive-hepatitis B surface antigen carrier mothers.The Pediatric infectious Disease Journal 1991;10(4):299-303.
Lee PI, Lee CY, Huang LM, Chang MH. Long-term efficacy of recombinanthepatitis B vaccine and risk of natural infection in infants born to motherswith hepatitis B e antigen. The Journal of Pediatrics 1995;126(5 Pt1):716-21.
*Lee PI, Lee CY, Huang LM, Chen JM, Chang MH. A follow-up study ofcombined vaccination with plasma-derived and recombinant hepatitis Bvaccines in infants. Vaccine 1995;13(17):1685-9.
Lee 1995 CB {published data only}Lee CY, Huang LM, Chang MH, Hsu CY, Wu SJ, Sung JL, et al. Theprotective efficacy of recombinant hepatitis B vaccine in newborn infantsof hepatitis B e antigen-positive-hepatitis B surface antigen carrier mothers.The Pediatric infectious Disease Journal 1991;10(4):299-303.
Lee PI, Lee CY, Huang LM, Chang MH. Long-term efficacy of recombinanthepatitis B vaccine and risk of natural infection in infants born to motherswith hepatitis B e antigen. The Journal of Pediatrics 1995;126(5 Pt1):716-21.
*Lee PI, Lee CY, Huang LM, Chen JM, Chang MH. A follow-up study ofcombined vaccination with plasma-derived and recombinant hepatitis Bvaccines in infants. Vaccine 1995;13(17):1685-9.
Lee 1995 DE {published data only}Lee CY, Huang LM, Chang MH, Hsu CY, Wu SJ, Sung JL, et al. Theprotective efficacy of recombinant hepatitis B vaccine in newborn infantsof hepatitis B e antigen-positive-hepatitis B surface antigen carrier mothers.The Pediatric infectious Disease Journal 1991;10(4):299-303.
Lee PI, Lee CY, Huang LM, Chang MH. Long-term efficacy of recombinanthepatitis B vaccine and risk of natural infection in infants born to motherswith hepatitis B e antigen. The Journal of Pediatrics 1995;126(5 Pt1):716-21.
*Lee PI, Lee CY, Huang LM, Chen JM, Chang MH. A follow-up study ofcombined vaccination with plasma-derived and recombinant hepatitis Bvaccines in infants. Vaccine 1995;13(17):1685-9.
Liu 1987 AB {published data only}Liu LH. [Comparative study of the efficacy of hepatitis B virus (HBV)vaccine combined with hepatitis B immunoglobulin(HBIG) versus vaccinealone in the interruption of the perinatal transmission of HBV carrier state].Zhonghua Liu Xing Bing Xue Za Zhi 1987;8(6):325-8.
Liu 1987 CA {published data only}Liu LH. [Comparative study of the efficacy of hepatitis B virus (HBV)vaccine combined with hepatitis B immunoglobulin(HBIG) versus vaccinealone in the interruption of the perinatal transmission of HBV carrier state].Zhonghua Liu Xing Bing Xue Za Zhi 1987;8(6):325-8.
Liu 1987 CB {published data only}Liu LH. [Comparative study of the efficacy of hepatitis B virus (HBV)vaccine combined with hepatitis B immunoglobulin(HBIG) versus vaccinealone in the interruption of the perinatal transmission of HBV carrier state].Zhonghua Liu Xing Bing Xue Za Zhi 1987;8(6):325-8.
Lo 1985 AB {published data only}Goudeau A, Lo KJ, Coursaget P, Tong MJ, Yeh CL, Tsai YT, et al.Prevention of hepatitis B virus infection in children born to HBsAgpositive/HBeAg positive mothers. Preliminary results of active andpassive-active immunization. Developmental Biology Standard1983;54:399-404.
*Lo KJ, Tsai YT, Lee SD, Yeh CL, Wang JY, Chiang BN, et al. Combinedpassive and active immunization for interruption of perinatal transmissionof hepatitis B virus in Taiwan. Hepatogastroenterology 1985;32(2):65-8.
Lo 1985 CA {published data only}Goudeau A, Lo KJ, Coursaget P, Tong MJ, Yeh CL, Tsai YT, et al.Prevention of hepatitis B virus infection in children born to HBsAgpositive/HBeAg positive mothers. Preliminary results of active andpassive-active immunization. Developmental Biology Standard1983;54:399-404.
*Lo KJ, Tsai YT, Lee SD, Yeh CL, Wang JY, Chiang BN, et al. Combinedpassive and active immunization for interruption of perinatal transmissionof hepatitis B virus in Taiwan. Hepatogastroenterology 1985;32(2):65-8.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 11
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

Lo 1985 CB {published data only}Goudeau A, Lo KJ, Coursaget P, Tong MJ, Yeh CL, Tsai YT, et al.Prevention of hepatitis B virus infection in children born to HBsAgpositive/HBeAg positive mothers. Preliminary results of active andpassive-active immunization. Developmental Biology Standard1983;54:399-404.
*Lo KJ, Tsai YT, Lee SD, Yeh CL, Wang JY, Chiang BN, et al. Combinedpassive and active immunization for interruption of perinatal transmissionof hepatitis B virus in Taiwan. Hepatogastroenterology 1985;32(2):65-8.
Lolekha 2002 {published data only}Lolekha S, Warachit B, Hirunyachote A, Bowonkiratikachorn P, West DJ,Poerschke G. Protective efficacy of hepatitis B vaccine without HBIG ininfants of HBeAg-positive carrier mothers in Thailand. Vaccine2002;20(31-32):3739-43.
Oon 1986 AB {published data only}Oon CJ, Tan KL, Goh KT, Wong-Yong L, Viegas O, McCarthy T, et al.Evaluation of a low dose of hepatitis B vaccine given within a childhoodimmunisation programme in Singapore. The Journal of Infection1986;13(3):255-67.
Oon 1986 CD {published data only}Oon CJ, Tan KL, Goh KT, Wong-Yong L, Viegas O, McCarthy T, et al.Evaluation of a low dose of hepatitis B vaccine given within a childhoodimmunisation programme in Singapore. The Journal of Infection1986;13(3):255-67.
Piazza 1985 {published data only}Piazza M, Picciotto L, Villari R, Guadagnino V, Orlando R, Isabella L, etal. Hepatitis B immunisation with a reduced number of doses in newbornbabies and children. Lancet 1985;1(8435):949-51.
Pongpipat 1986 {published data only}Pongpipat D, Suvatte V, Assateerawatts A. Efficacy of hepatitis-Bimmunoglobulin and hepatitis-B vaccine in prevention of the HBsAg carrierstate in newborn infants of mothers who are chronic carriers of HBsAg andHBeAg. Asian Pacific Journal of Allergy Immunology 1986;4(1):33-6.
Pongpipat 1988 {published data only}Pongpipat D, Suvatte V, Assateerawatts A. Hepatitis B immunization inhigh risk neonates born from HBsAg and HBeAg positive mothers:comparison of standard and low dose regimens. Asian Pacific Journal ofAllergy Immunology 1988;6(2):107-10.
Pongpipat 1989 {published data only}Pongpipat D, Suvatte V, Assateerawatts A. Hepatitis B immunization inhigh risk neonates born from HBsAg positive mothers: comparison betweenplasma derived and recombinant DNA vaccine. Asian Pacific Journal ofAllergy Immunology 1989;7(1):37-40.
Poovorawan 1997 {published data only}*Poovorawan Y, Sanpavat S, Chumdermpadetsuk S, Safary A. Long-termhepatitis B vaccine in infants born to hepatitis B e antigen positive mothers.Archives of Disease in Childhood. Fetal and Neonatal Edition1997;77(1):F47-F51.
Poovorawan Y, Sanpavat S, Pongpunglert W, Chumdermpadetsuk S,Sentrakul P, Vandepapeliere P, et al. Long term efficacy of hepatitis Bvaccine in infants born to hepatitis B e antigen-positive mothers. ThePediatric Infectious Disease Journal 1992;11(10):816-21.
Sehgal 1992 {published data only}Sehgal A, Gupta I, Sehgal R, Ganguly NK. Hepatitis B vaccine alone or incombination with anti-HBs immunoglobulin in the perinatal prophylaxisof babies born to HBsAg carrier mothers. Acta Virologica1992;36(4):359-66.
*Sehgal A, Sehgal R, Gupta I, Bhakoo ON, Ganguly NK. Use of hepatitisB vaccine alone or in combination with hepatitis B immunoglobulin forimmunoprophylaxis of perinatal hepatitis B infection. Journal of TropicalPediatrics 1992;38(5):247-51.
Theppisai 1987 {published data only}Theppisai U, Thanuntaseth C, Chiewsilp P, Siripoonya P. A comparisonbetween the efficacy of passive-active and active immunization forprevention of perinatal transmission of hepatitis B virus. Journal of MedicalAssociation, Thailand 1987;70(8):459-62.
Theppisai 1990 {published data only}Theppisai U, Thanuntaseth C, Chiewsilp P, Siripoonya P. Prevention ofhepatitis B infection in infants born to hepatitis B carrier mothers: lowdosage vaccination. International Journal of Gynaecology and Obstetrics1990;32(4):353-7.
Xu 1995 AB {published data only}*Xu ZY, Duan SC, Margolis HS, Purcell RH, Ou-Yang PY, Coleman PJ,et al. Long-term efficacy of active postexposure immunization of infantsfor prevention of hepatitis B virus infection. United States-People's Republicof China Study Group on Hepatitis B. The Journal of Infectious Diseases1995;171(1):54-60.
Xu ZY, Francis DP, Liu CB, Purcell RH, Duan SC, Chen RJ, et al.Prevention of hepatitis B virus carriage of infants using HBV vaccine inShanghai. Preliminary report of a randomized double-blindplacebo-controlled trial. Chinese Medical Journal 1985;98(9):623-6.
Xu ZY, Liu CB, Francis DP, Purcell RH, Gun ZL, Duan SC, et al.Prevention of perinatal acquisition of hepatitis B virus carriage usingvaccine: preliminary report of a randomized, double-blindplacebo-controlled and comparative trial. Pediatrics 1985;76(5):713-8.
Xu 1995 AD {published data only}*Xu ZY, Duan SC, Margolis HS, Purcell RH, Ou-Yang PY, Coleman PJ,et al. Long-term efficacy of active postexposure immunization of infantsfor prevention of hepatitis B virus infection. United States-People's Republicof China Study Group on Hepatitis B. The Journal of Infectious Diseases1995;171(1):54-60.
Xu ZY, Francis DP, Liu CB, Purcell RH, Duan SC, Chen RJ, et al.Prevention of hepatitis B virus carriage of infants using HBV vaccine inShanghai. Preliminary report of a randomized double-blindplacebo-controlled trial. Chinese Medical Journal 1985;98(9):623-6.
Xu ZY, Liu CB, Francis DP, Purcell RH, Gun ZL, Duan SC, et al.Prevention of perinatal acquisition of hepatitis B virus carriage usingvaccine: preliminary report of a randomized, double-blindplacebo-controlled and comparative trial. Pediatrics 1985;76(5):713-8.
Xu 1995 BD {published data only}*Xu ZY, Duan SC, Margolis HS, Purcell RH, Ou-Yang PY, Coleman PJ,et al. Long-term efficacy of active postexposure immunization of infantsfor prevention of hepatitis B virus infection. United States-People's Republicof China Study Group on Hepatitis B. The Journal of Infectious Diseases1995;171(1):54-60.
Xu ZY, Francis DP, Liu CB, Purcell RH, Duan SC, Chen RJ, et al.Prevention of hepatitis B virus carriage of infants using HBV vaccine inShanghai. Preliminary report of a randomized double-blindplacebo-controlled trial. Chinese Medical Journal 1985;98(9):623-6.
Xu ZY, Liu CB, Francis DP, Purcell RH, Gun ZL, Duan SC, et al.Prevention of perinatal acquisition of hepatitis B virus carriage usingvaccine: preliminary report of a randomized, double-blindplacebo-controlled and comparative trial. Pediatrics 1985;76(5):713-8.
Xu 1995 CB {published data only}*Xu ZY, Duan SC, Margolis HS, Purcell RH, Ou-Yang PY, Coleman PJ,et al. Long-term efficacy of active postexposure immunization of infantsfor prevention of hepatitis B virus infection. United States-People's Republicof China Study Group on Hepatitis B. The Journal of Infectious Diseases1995;171(1):54-60.
Xu ZY, Francis DP, Liu CB, Purcell RH, Duan SC, Chen RJ, et al.Prevention of hepatitis B virus carriage of infants using HBV vaccine inShanghai. Preliminary report of a randomized double-blindplacebo-controlled trial. Chinese Medical Journal 1985;98(9):623-6.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 12
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

Xu ZY, Liu CB, Francis DP, Purcell RH, Gun ZL, Duan SC, et al.Prevention of perinatal acquisition of hepatitis B virus carriage usingvaccine: preliminary report of a randomized, double-blindplacebo-controlled and comparative trial. Pediatrics 1985;76(5):713-8.
Xu 1995 CD {published data only}*Xu ZY, Duan SC, Margolis HS, Purcell RH, Ou-Yang PY, Coleman PJ,et al. Long-term efficacy of active postexposure immunization of infantsfor prevention of hepatitis B virus infection. United States-People's Republicof China Study Group on Hepatitis B. The Journal of Infectious Diseases1995;171(1):54-60.
Xu ZY, Francis DP, Liu CB, Purcell RH, Duan SC, et al. Prevention ofhepatitis B virus carriage of infants using HBV vaccine in Shanghai.Preliminary report of a randomized double-blind placebo-controlled trial.Chinese Medical Journal 1985;98(9):623-6.
Xu ZY, Liu CB, Francis DP, Purcell RH, Gun ZL, Duan SC, et al.Prevention of perinatal acquisition of hepatitis B virus carriage usingvaccine: preliminary report of a randomized, double-blindplacebo-controlled and comparative trial. Pediatrics 1985;76(5):713-8.
Yeoh 1986 {published data only}Yeoh EK, Chang WK, Ip P, Chan KH, Chan E, Fung C. Efficacy and safetyof recombinant hepatitis B vaccine in infants born to HBsAg-positivemothers. The Journal of Infection 1986;13 Suppl A:15-8.
Zhu 1987 {published data only}Zhu Q-Y, Radvan GH. A randomized controlled trial of hepatitis B vaccinein high risk newborn infants in China. Australian & New Zealand Journalof Medicine 1987;17:498.
Zhu 1994 {published data only}Zhu QR, Gu XH, Duan SC, Xu HF. Long-term immunogenicity and efficacyof recombinant yeast derived hepatitis B vaccine for interruption ofmother-infant transmission of hepatitis B virus. Chinese Medical Journal1994;107(12):915-8.
Referencias de los estudios excluidos de esta revisión
Chung 1988Chung WK. Persistence and boosting response of antibody to HBsAginduced by vaccine treatment. Tropical Gastroenterology 1988;9(1):26-30.
Chung 1988 BChung WK, Choi KY, Shim KS, Chung JW, Sun HS, Chung KW, et al.Safety, immunogenicity, and efficacy of a new heat-inactivated hepatitisB vaccine in the newborn. Viral Hepatitis and Liver Disease 1988:1014-6.
Coursaget 1984Coursaget P, Deciron F, Tortey E, Barin F, Chiron JP, Yvonnet B, et al.Immune response to hepatitis B vaccine in infants and newborns: controltrial in an endemic area (Senegal). International Agency for Research onCancer 1984;63:319-35.
Da 1995Da Villa G, Picciottoc L, Elia S, Peluso F, Montanaro F, Maisto T. HepatitisB vaccination: universal vaccination of newborn babies and children at 12years of age versus high risk groups. A comparison in the field. Vaccine1995;13(13):1240-3.
Delage 1993Delage G, Remy-Prince S, Montplaisir S. Combined active-passiveimmunization against the hepatitis B virus: five-year follow-up of childrenborn to hepatitis B surface antigen-positive mothers. The Pediatric InfectiousDisease Journal 1993;12(2):126-30.
Esteban 1986Esteban JI, Genesca J, Esteban R, Hernandez JM, Seijo G, Buti M, et al.Immunoprophylaxis of perinatal transmission of the hepatitis B virus:efficacy of hepatitis B immune globulin and hepatitis B vaccine in alow-prevalence area. Journal of Medical Virology 1986;18(4):381-91.
Goh 1992Goh KT, Tan KL, Kong KH, Oon CJ, Chan SH. Comparison of the immuneresponse of four different dosages of a yeast-recombinant hepatitis B vaccinein Singapore children: a four-year follow-up study. Bulletin of the WorldHealth Organization 1992;70(2):233-9.
Kang 1986Kang Y. Efficacy of domestic hepatitis B viral vaccines in preventingtransmission of e antigen from mothers to newborn infants. Zhonghua LiuXing Bing Xue Za Zhi 1986;7(2):81-3.
Lai 1986Lai CL, Yeoh EK, Chang WK, Lo VW, Ng LN. Use of the hepatitis Brecombinant DNA yeast vaccine (H-B-VAX II) in children: two doses vs.three doses of 5 micrograms regime; an interim report. The Journal ofInfection 1986;13 Suppl A:19-25.
Lai 1993Lai CL, Wong BC, Yeoh EK, Lim WL, Chang WK, Lin HJ. Five-yearfollow-up of a prospective randomized trial of hepatitis B recombinantDNA yeast vaccine vs. plasma-derived vaccine in children: immunogenicityand anamnestic responses. Hepatology 1993;18(4):763-7.
Laille 1988Laille M, Brethes B, Moreau JP, Pillot J. [Trial of hepatitis B prophylaxisin children born to mothers carrying HBs antigen in New Caledonia].Bulletin de la Societe de Pathologie Exotique et de ses Filiales1988;81(4):673-8.
Lin 1987Lin KH, Twu SJ, Chen DS, Su S, Lee CJ. Efficacy of the national hepatitisB vaccination program in the Republic of China: preliminary observationsfrom Taoyuan area. Taiwan Yi Xue Hui Za Zhi 1987;86(8):869-72.
Linder 2000Linder N, Handsher R, German B, Sirota L, Bachman M, Zinger S, et al.Controlled trial of immune response of preterm infants to recombinanthepatitis B and inactivated poliovirus vaccines administered simultaneouslyshortly after birth. Archives of Disease in Childhood. Fetal and neonataledition 2000;83(1):F24-F27.
Milne 1989Milne A, Heydon JL, Hindle RC, Pearce NE. Prevalence of hepatitis B inchildren in a high risk New Zealand community, and control usingrecombinant DNA vaccine. New Zealand Medical Journal1989;102(866):182-4.
Mittal 1994Mittal SK, Rao S, Kumari S, Aggarwal V, Prakash C, Thirupuram S.Simultaneous administration of hepatitis B vaccine with other E.P.I.vaccines. Indian Journal of Pediatrics 1994;61(2):183-8.
Moulia-Pelat 1994Moulia-Pelat JP, Spiegel A, Martin PM, Cardines R, Boutin JP, Roux JF,et al. A 5-year immunization field trial against hepatitis B using a Chinesehamster ovary cell recombinant vaccine in French Polynesian newborns:results at 3 years. Vaccine 1994;12(6):499-502.
Nair 1984Nair PV, Weissman JY, Tong MJ, Thursby MW, Paul RH, Henneman CE.Efficacy of hepatitis B immune globulin in prevention of perinataltransmission of the hepatitis B virus. Gastroenterology 1984;87(2):293-8.
Okoth 1994Okoth FA, Kobayashi M, Takayanagi N, Kapttich DC, Kaiguri PM, TukeiPM. Efficacy of hepatitis B vaccine in a rural community in Muranga,Kenya. East African Medical Journal 1994;71(4):250-2.
Perrin 1986Perrin J, Coursaget P, Ntareme F, Chiron JP. Hepatitis B immunization ofnewborns according to a two dose protocol. Vaccine 1986;4(4):241-4.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 13
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

Pongpipat 1984Pongpipat D, Suvatte V, Assateerawatts A. Vaccination against hepatitisB virus infection in neonates. Helvetica Paediatrica Acta 1984;39(3):231-6.
Poovorawan 1989Poovorawan Y, Sanpavat S, Pongpunlert W, Chumdermpadetsuk S,Sentrakul P, Safary A. Protective efficacy of a recombinant DNA hepatitisB vaccine in neonates of HBe antigen-positive mothers. The Journal of theAmerican Medical Association 1989;261(22):3278-81.
Poovorawan 1990Poovorawan Y, Sanpavat S, Pongpunlert W, Chumdermpadetsuk S,Sentrakul P, Chitinand S, et al. Comparison of a recombinant DNA hepatitisB vaccine alone or in combination with hepatitis B immune globulin forthe prevention of perinatal acquisition of hepatitis B carriage. Vaccine1990;8 Suppl:S56-S59; discussion S60-S62.
Shikata 1984Shikata T, Yano M, Shiraki K, Oda T. Efficacy trial of HBIG and hepatitisB vaccine for the prevention of perinatal HBV transmission. Viral Hepatitisand Liver Disease 1984:596-7.
Stevens 1987Stevens CE, Taylor PE, Tong MJ, Toy PT, Vyas GN, Nair PV, et al.Yeast-recombinant hepatitis B vaccine. Efficacy with hepatitis B immuneglobulin in prevention of perinatal hepatitis B virus transmission. TheJournal of the American Medical Association 1987;257(19):2612-6.
Stevens 1988Stevens CE, Taylor PE, Tong MJ, Toy PT, Vyas GN, Zang EA, et al.Prevention of perinatal hepatitis B virus infection with hepatitis B immuneglobulin and hepatitis B vaccine. Viral Hepatitis and Liver Disease1988:982-8.
Stevens 1990Stevens CE, Taylor PE, Tong MJ, Toy PT. Hepatitis B immune globulinand yeast-recombinant hepatitis B vaccine in prevention of perinatal HBVinfection in the USA. Viral Hepatits and Hepatocellular Carcinoma1990:377-84.
Stevens 1992Stevens CE, Toy PT, Taylor PE, Lee T, Yip HY. Prospects for control ofhepatitis B virus infection: implications of childhood vaccination andlong-term protection. Pediatrics 1992;90(1 Pt 2):170-3.
Surya 1996Surya IGP, Kishimoto S, Sudaryat S, Tsuda F, Hamid A, Takahashi K, etal. Prevention of mother-to-infant transmission of hepatitis B virus withuse of a preS2-containing vaccine in Bali, Indonesia. Vaccine Research1996;5(4):203-12.
Suwignyo 1994Suwignyo S, Surya IGP, Mulyanto, Montessori, Domoto K, Tsuda F, et al.The use of a PreS2-containing recombinant vaccine for the prevention ofmaternal transmission of hepatitis B virus in Indonesian neonates. ViralHepatitis and Liver Disease 1994:536-9.
Theppisai 1988Theppisai U, Thanuntaseh C, Chiewsilp P, Siripoonya P. Two-year studyof passive-active immunization for prevention of hepatitis B infection innewborns. Journal of the Medical Association of Thailand 1988;71(8):413-6.
Theppisai 1989Theppisai U, Thanuntaseth C, Chiewsilp P, Siripoonya P. Long-termimmunoprophylaxis of hepatitis B surface antigen carrier in infants bornto hepatitis B surface antigen positive mothers using plasma derived vaccine.Asia Oceania Journal of Obstetrics and Gynaecology 1989;15(2):111-5.
Wheeley 1991Wheeley SM, Jackson PT, Boxall EH, Tarlow MJ, Gatrad AR, AndersonJ, et al. Prevention of perinatal transmission of hepatitis B virus (HBV): acomparison of two prophylactic schedules. Journal of Medical Virology1991;35(3):212-5.
Young 2003Young BW, Lee SS, Lim WL, Yeoh EK. The long-term efficacy ofplasma-derived hepatitis B vaccine in babies born to carrier mothers. Journalof Viral Hepatitis 2003;10(1):23-30.
Yuen 1999Yuen MF, Lim WL, Cheng CC, Lam SK, Lai CL. Twelve-year follow-upof a prospective randomized trial of hepatitis B recombinant DNA yeastvaccine versus plasma-derived vaccine without booster doses in children.Hepatology 1999;29(3):924-7.
Zanetti 1986Zanetti AR, Dentico P, Del Vecchio Blanco C, Sagnelli E, Villa E, FerroniP, et al. Multicenter trial on the efficacy of HBIG and vaccine in preventingperinatal hepatitis B. Final report. Journal of Medical Virology1986;18(4):327-34.
Zhu 2003Zhu Q, Yu G, Yu H, Lu Q, Gu X, Dong Z, et al. A randomized control trialon interruption of HBV transmission in uterus. Chinese Medical Journal2003;116(5):685-7.
Referencias adicionales
Aggarwal 2004Aggarwal R, Ranjan P. Preventing and treating hepatitis B infection. BMJ(Clinical Research Ed.) 2004;329(7474):1080-6.
Akhter 1992Akhter S, Talukder MQ, Bhuiyan N, Chowdhury TA, Islam MN, BegumS. Hepatitis B virus infection in pregnant mothers and its transmission toinfants. Indian Journal of Pediatrics 1992;59(4):411-5.
Als-Nielsen 2004Als-Nielsen B, Gluud LL, Gluud C. Methodological quality and treatmenteffects in randomised trials - a review of six empirical studies (abstract).Cochrane Colloquium 2004, Ottawa, Canada. 2004.
Altman 2003Altman DG, Bland JM. Interaction revisited: the difference between twoestimates. BMJ (Clinical Research Ed.) 2003;326:219.
Andre 1994Andre FE, Zuckerman AJ. Review: protective efficacy of hepatitis Bvaccines in neonates. Journal of Medical Virology 1994;44(2):144-51.
Assad 1999Assad S, Francis A. Over a decade of experience with a yeast recombinanthepatitis B vaccine. Vaccine 1999;18(1-2):57-67.
Beasley 1977Beasley RP, Trepo C, Stevens CE, Szmuness W. The e antigen and verticaltransmission of hepatitis B surface antigen. American Journal ofEpidemiology 1977;105(2):94-8.
Beasley 1983Beasley RP, Hwang LY. Postnatal infectivity of hepatitis B surfaceantigen-carrier mothers. Journal of Infectious Diseases 1983;147(2):185-90.
Beasley 1984Beasley RP, Hwang LY. Hepatocellular carcinoma and hepatitis B virus.Seminars in Liver Disease 1984;4(2):113-21.
Begg 1994Begg CB, Mazumdar M. Operating characteristics of a rank correlation testfor publication bias. Biometrics 1994;50(4):1088-101.
Bloom 1993Bloom BS, Hillman AL, Fendrick AM, Schwartz JS. A reappraisal ofhepatitis B virus vaccination strategies using cost-effectiveness analysis.Annals of Internal Medicine 1993;118(4):298-306.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 14
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

Bohlke 2003Bohlke K, Davis RL, Marcy SM, Braun MM, DeStefano F, Black SB, etal. Risk of anaphylaxis after vaccination of children and adolescents.Pediatrics 2003;112(4):815-20.
CDC 1991Centers for Disease Control and Prevention. Hepatitis B virus: acomprehensive strategy for eliminating transmission in the United Statesthrough universal childhood vaccination: recommendations of theImmunization Practices Advisory Committee (ACIP). Morbidity andMortality Weekly Report. Recommendations and Reports/Centers forDisease Control 1991;40:1-19.
CDC 1999Centers for Disease Control and Prevention. Notice to readers update:recommendations to prevent hepatitis B virus transmission - UnitedStates-updated. Morbidity and Mortality Weekly Report 1999;48(2):33-4.
Chen 2005Chen W, Gluud C. Vaccines for preventing hepatitis B in health-careworkers. The Cochrane Database of Systematic Reviews 2005, Issue 4. Art.No.: CD000100. DOI: 10.1002/14651858.CD000100.pub3
Da Villa 1999Da Villa G, Sepe A. Immunization programme against hepatitis B virusinfection in Italy: Cost-effectiveness. Vaccine 1999;17(13-14):1734-8.
David 1996David MS, Norman TB. Immunisation against Infectious Disease. London:HMSO, 1996.
Deeks 2003Deeks JJ, Dinnes J, D'Amico R, Sowden AJ, Sakarovitch C, Song F, et al.Evaluating non-randomised intervention studies. Health TechnologyAssessment 2003;7(27):1-173.
DeMets 1987DeMets DL. Methods for combining randomized clinical trials: strengthsand limitations. Statistics in Medicine 1987;6(3):341-50. 3616287.
DerSimonian 1986DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled ClinicalTrials 1986;7(3):177-88. 3802833.
Dusheiko 1998Dusheiko G. Hepatitis B. In: Bircher J, Benhamou JP, McIntyre N, RizzettoM, Rodés J, editor(s). Oxford Textbook of Clinical Hepatology. Oxford,UK: Oxford Medical Publications, 1998:876-96.
DuVernoy 2000DuVernoy TS, Braun MM. Hypotonic-hyporesponsive episodes reportedto the Vaccine Adverse Event Reporting System (VAERS), 1996-1998.Pediatrics 2000;106(4):E52.
Egger 1997Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysisdetected by a simple graphical test. BMJ (Clinical Research Ed.)1997;315(7109):629-34. 9310563.
Etminan 2004Etminan M, Carleton B, Rochon PA. Quantifying adverse drug events: Aresystematic reviews the answer?. Drug Safety 2004;27(11):757-61.
Fisher 2001Fisher MA, Eklund SA, James SA, Lin X. Adverse events associated withhepatitis B vaccine in U.S. children less than six years of age, 1993 and1994. Annals of Epidemiology 2001;11(1):13-21.
Funk 2002Funk ML, Rosenberg DM, Lok AS. World-wide epidemiology ofHBeAg-negative chronic hepatitis B and associated precore and corepromoter variants. Journal of Viral Hepatitis 2002;9:52-61.
Hadler 1986Hadler SC, Francis DP, Maynard JE, Thompson SE, Judson FN, EchenbergDF, et al. Long-term immunogenicity and efficacy of hepatitis B vaccinein homosexual men. The New England Journal of Medicine1986;315(4):209-14. 2941687.
Hall 1993Hall AJ, Robertson RL, Crivelli PE, Lowe Y, Inskip H, Snow SK, et al.Cost-effectiveness of hepatitis B vaccine in the Gambia. Transactions ofthe Royal Society of Tropical Medicine and Hygiene 1993;87(3):333-6.
Harris 2001Harris A, Yong K, Kermode M. An economic evaluation of universal infantvaccination against hepatitis B virus using a combination vaccine(Hib-HepB): a decision analytic approach to cost effectiveness. Australianand New Zealand Journal of Public Health 2001;25(3):222-9.
Hayashi 1996Hayashi K, Walker AM. Japanese and American reports of randomizedtrials: Differences in the reporting of adverse effects. Controlled ClinicalTrials 1996;17(2):99-110.
Heijtink 2002Heijtink RA, Kruining J, van Bergen P, de Rave S, van Hattum J, SchuttenM, et al. Characterization of a human monoclonal antibody obtained afterimmunization with plasma vaccine and a booster with recombinant-DNAhepatitis B vaccine. Journal of Medical Virology 2002;66(3):304-11.11793381.
Higgins 2002Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis.Statistics in Medicine 2002;21:1539-58.
ICH 1997International Conference on Harmonisation Expert Working Group. Codeof Federal Regulations & International Conference on HarmonizationGuidelines. Media: Parexel Barnett, 1997.
Ioannidis 2001Ioannidis JP, Lau J. Completeness of safety reporting in randomized trials:an evaluation of 7 medical areas. JAMA 2001;285(4):437-43.
Kjaergard 2001Kjaergard LL, Villumsen J, Gluud C. Reported methodological quality anddiscrepancies between large and small randomized trials in meta-analyses.Annals of Internal Medicine 2001;135(11):982-9. 11730399.
Kojouharova 2001Kojouharova M, Teoharov P, Bahtchevanova T, Maeva I, Eginlian A,Deneva M. Safety and immunogenicity of a yeast-derived recombinanthepatitis B vaccine in Bulgarian newborns. Infection 2001;29(6):342-4.
Lee 2004Lee C, Gong Y, Brok J, Boxall EH, Gluud C. Hepatitis B prophylaxis fornewborns of hepatitis B surface antigen-positive mothers. (Protocol) TheCochrane Database of Systematic Reviews 2004, Issue 2. Art. No.:CD004790. DOI: 10.1002/14651858.CD004790
Lewis 2001Lewis E, Shinefield HR, Woodruff BA, Black SB, Destefano F, Chen RT,et al. Safety of neonatal hepatitis B vaccine administration. The PediatricInfectious Disease Journal 2001;20(11):1049-54.
Li 2003Li XM, Yang YB, Hou HY, Shi ZJ, Shen HM, Teng BQ, et al. Interruptionof HBV intrauterine transmission: a clinical study. World Journal ofGastroenterology 2003;9:1501-3.
Liu 1995Liu ZG, Zhao SL, Zhang YX. Cost-benefit analysis on immunization ofnewborns with hepatitis B vaccine in Jinan City (Chinese). Zhonghua LiuXing Bing Xue Za Zhi 1995;16(2):81-4.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 15
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

MacGregor 2004MacGregor IR. Screening assays for transmissible spongiformencephalopathies (TSEs). Vox Sanguinis 2004;87 Suppl 2:3-6.
Margolis 1995Margolis H, Coleman P, Brown R, Mast E, Sheingold S, Arevalo J.Prevention of hepatitis B virus transmission by immunization. An economicanalysis of current recommendations. JAMA 1995;274(15):1201-8.
Moher 1998Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al. Doesquality of reports of randomised trials affect estimates of interventionefficacy reported in meta-analyses. Lancet 1998;352(9128):609-13.9746022.
Nayak 1987Nayak NC, Panda SK, Zuckerman AJ, Bhan MK, Guha DK. Dynamics andimpact of perinatal transmission of hepatitis B virus in north India. Journalof Medical Virology 1987;21(2):137-45.
Niu 1996Niu MT, Davis DM, Ellenberg S. Recombinant hepatitis B vaccination ofneonates and infants: emerging safety data from the Vaccine Adverse EventReporting System. The Pediatric Infectious Disease Journal1996;15(9):771-6.
Niu 1999Niu MT, Salive ME, Ellenberg SS. Neonatal deaths after hepatitis B vaccine:the vaccine adverse event reporting system, 1991-1998. Archives ofPediatrics & Adolescent Medicine 1999;153(12):1279-82.
Okada 1976Okada K, Kamiyama I, Inomata M, Imai M, Miyakawa Y. E antigen andanti-e in the serum of asymptomatic carrier mothers as indicators of positiveand negative transmission of hepatitis B virus to their infants. New EnglandJournal of Medicine 1976;294(14):746-9.
Schultz 1995Schultz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence ofmethodological quality associated with estimates of treatment effects incontrolled trials. The Journal of the American Medical Association1995;273:408-12.
Sriprakash 1997Sriprakash I, Anil T. Routine prenatal screening of Indian women forHBsAg: benefits derived versus cost. Tropical Doctor 1997;27(3):176-7.
Stevens 1975Stevens CE, Beasley RP, Tsui J, Lee WC. Vertical transmission of hepatitisB antigen in Taiwan. The New England Journal of Medicine1975;292(15):771-4.
Szmuness 1981Szmuness W, Stevens CE, Zang EA, Harley EJ, Kellner AA. A controlledclinical trial of the efficacy of the hepatitis B vaccine: a final report.Hepatology 1981;1(5):377-85. 7030902.
Tormans 1993Tormans G, Van Damme P, Carrin G, Clara R, Eylenbosch W.Cost-effectiveness analysis of prenatal screening and vaccination againsthepatitis B virus - the case of Belgium. Social Society of Medicine1993;37(2):173-81.
WHO 2002World Health Organization Department of Communicable DiseaseSurveillance and Response. Hepatitis B.http://www.who.int/csr/disease/hepatitis/HepatitisB_whocdscsrlyo2002_2.pdf(Accessed 7 February 2006).
Yang 2003Yang Y, Liu C, Chen T, Lee M, Chen S, Shi H, et al. Role of hepatitis Bimmunoglobulin in infants born to hepatitis B e antigen-negative carriermothers in Taiwan. Pediatrics Infection Disease Journal 2003;22(7):584-8.
Yao 1996Yao JL. Perinatal transmission of hepatitis B virus infection and vaccinationin China. Gut 1996;38 Suppl 2:S37-S38.
Zhu 1997Zhu Q, Lu Q, Gu X, Xu H, Duan S. A preliminary study on interruption ofHBV transmission in uterus. Chinese Medical Journal 1997;110(2):145-7.
* El asterisco señala los documentos más importantes para este estudio
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Página 16
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.

TABLAS
Characteristics of included studies
Assateerawatt 1993Study
Generation of allocation sequence: adequate - random permutation table.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - only number of dropouts reported in each group, the reasonsnot described.
Methods
Country: Thailand.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.
Participants
Group A: HBIG 100 IU at birth and GenHevac (RV) 20 microgram at birth, 1, 2 and 12months.Group B: GenHevac (RV) 20 microgram at birth, 1, 2 and 12 months.
Interventions
HBsAgAnti-HBsAnti-HBc
Outcomes
Follow-up time: 14, 18 or 30 months.Adverse events: there were no serious reactions to the vaccine, and the adverse effectsobserved were mild and transient. Local swelling and erythema were observed in 3.3%of neonates.
Notes
BAllocation concealment
Beasley 1983a ABStudy
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: unclear - described as double blind, but method of blinding not described.Follow-up: adequate - number and reasons reported.
Methods
Página 17
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Country: Taiwan.Publication language: English.Inclusion criteria:HBsAg- and HBeAg-positive mothers.Infant birth weight over 2500 gm with Apgar scores > 8 at 1 minute.Exclusion criteria:HBeAg negative mother.Participants:(1) Group A (control group)received no prophylaxis against HBV. 23 were infants born in the same hospital and61 were those randomised blind to receive placebo in another HBIG prophylaxis trial.Birth weight: (3239+-407) gramOlder siblings (mean number): 0.5+-0.6Cord blood positive (%): 29.5%Age 1st treatment (minutes): 36.0+-76.8Age 2nd treatment (minutes): 98.4+-9.0Age 3rd treatment (minutes): 190.1+-8.8Mother's mean age: 24.8+-3.1HBsAg titer: 12.1+-1.7Drop-out: 12(2) Group BBirth weight: (3209+-308) gramOlder siblings (mean number): 0.7+-0.6Cord blood positive (%): 23.9%Age 1st treatment (minutes): 20.5+-20.4Age 2nd treatment (minutes): 97.1+-7.9Age 3rd treatment (minutes): 186.8+-10.3Mother's mean age: 26.3+-3.7HBsAg titer: 11.9+-1.8Drop-out: 9(3) Group CBirth weight: (3232+-372) gramOlder siblings (mean number): 0.6+-0.7Cord blood positive (%): 22.8%Age 1st treatment (minutes): 35.8+-135.1Age 2nd treatment (minutes): 98.0+-8.0Age 3rd treatment (minutes): 189.0+-9.5Mother's mean age: 25.5+-3.3HBsAg titer: 12.0+-1.9Drop-out: 6
Participants
Group A: HBIG 1.0 mL (180 mIU, Abbott) at birth and saline at 3 and 6 months.Group B: saline at birth, 3 and 6 months.Group C: given HBIG 0.5 mL (90 mIU, Abbott) diluted in 0.5 mL of immune serumglobulin at birth, 3 and 6 months.The mean administration time of HBIG was within 36 minutes of birth: 95% were treatedwithin an hour; all were treated within 30 hours.
Interventions
Hepatitis events at 15 months follow-up. HBsAg, Anti-HBs, Anti-HBc, and HBeAg.Outcomes
Follow-up time: 15 months.Adverse events: One infant died, but the death appeared unrelated to HBIG.12 dropouts in Group A, including 10 refuse and 2 lost; 9 in Group B, including 7 refuseand 2 lost; 6 dropouts in Group C, all because of refusal.
Notes
BAllocation concealment
Página 18
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Beasley 1983a CBStudy
This trial is the same as Beasley 1983a BA, but has been entered with its own identifierdue to technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Beasley 1983bStudy
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: unclear - described as double blind but the method of blinding was notdescribed.Follow-up: adequate - no dropouts.
Methods
Country: Taiwan.Publication language: English.Inclusion criteria:HBsAg- and HBeAg-positive mothers.infant birth weight over 3000 gm and one-minute Apgar scores >= 9.Participants:(1) Control groupreceived no prophylaxis against HBV. 23 were infants born in the same hospital and61 were those randomised blind to receive placebo in another HBIG prophylaxis trial.Birth weight (mean +- SD): (3185+-438 gram)Sex ratio (% male): 50.7Apgar score: 9.9+-0.1Age initial HBIG (min): not reported.Mother's age: 25.1+-3.3(2) Group ABirth weight (mean +- SD): (3392+-399 gram)Sex ratio (% male): 60.8Apgar score: 9.9+-0.4Age initial HBIG (min): 65+-186Mother's age: 26.1+-4.1(3) Group BBirth weight (mean +- SD): (3288+-264 gram)Sex ratio (% male): 56Apgar score: 9.9+-0.3Age initial HBIG (min): 171+-328Mother's age: 25.4+-2.6(4) Group CBirth weight (mean +- SD): (3192+-367 gram)Sex ratio (% male): 53.4Apgar score: 9.7+-0.8Age initial HBIG (min): 145+-312Mother's age: 26.3+-3.4
Participants
Página 19
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Control group: saline at birth (mean and SD = 2.1+-4.8 h), 3 and 6 months (from previousstudy).Group A: HBIG 0.5 mL (145 IU, Abbott) at birth, a second dose at 3 months of age, atwhich time vaccination (20 microgram, Merck Sharp and Dohme) is initiated (88.6+-14.5days). Followed by boosters a month and 6 month later.Group B: HBIG 0.5 mL at birth only and vaccination was initiated when they were 4 to7 days old (6.3+-1.5). Followed by boosters a month and 6 month later.Group C: HBIG 0.5 mL only and vaccination was initiated when they were approximately1 month old (30.2+-4.3 days). Followed by boosters a month and 6 month later.
Interventions
Hepatitis events at maximum HBsAg, anti-HBs.Outcomes
Follow-up time: 9 months.Adverse events:The data in control group (84 infants) were obtained from another trial (Beasley, 1983)
Notes
BAllocation concealment
Farmer 1987Study
Generation of allocation sequence: adequate - random number list.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - not specified in the each groups.
Methods
Country: New Zealand.Publication language: English.Inclusion criteria:Both HBsAg and HBeAg positive mothers.infant birth weight over 2500 gm with Apgar scores > 8 at 1 minute.Exclusion criteria:not reported.Participants:(1) Group A(3) Group B
Participants
Group A: 0.25 mL (5 microgram) Hepavax (PDV, Merck Sharp and Dohme) I.M. atbirth, 6 weeks and 6 months.Group B: 0.25 mL (5 microgram) Hepavax (PDV, Merck Sharp and Dohme) I.M. plusHBIG 0.25 mL (25 IU/kg) at birth then Hepavax + HBIG 0.25 mL (25 IU/kg) at 6 weeks.Finally, another Hepavax vaccine in 6 months.
Interventions
Hepatitis events at maximum follow-up.HBsAg. HBeAg and anti-HBs.
Outcomes
Follow-up time: 12 months.Adverse events: not reported.Four infants were lost to follow-up.
Notes
BAllocation concealment
Garcia 1992Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: unclear - described as double blind but the method of blinding was notdescribed.Follow-up: inadequate - not described.
Methods
Página 20
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Country: Cuba.Publication language: Spanish.Inclusion criteria:HBsAg positive mothers.
Participants
Group A (Cuban): RV 10 microgram at birth, 1 and 2 months.Group B (SK): RV 10 microgram at birth, 1, and 2 months.
Interventions
Anti-HBs, HBsAg, Anti-HBc.Outcomes
Follow up time: 6 months.Adverse events: not reported.
Notes
BAllocation concealment
Grosheide 1993Study
Generation of allocation sequence: unclear - described as randomised, but the methodnot described.Allocation concealment: adequate - sealed envelops.Blinding: not performed.Follow-up: adequate - number and reasons for dropouts described.
Methods
Country: NetherlandsPublication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.Exclusion criteria:Participants:Group A:Mother median age: 23 (19;33)Country of birth, No. (%)The Netherlands +other: 3 (8.6)Mediterranean: 15 (42.9)Surinam: 5 (14.3)Asia: 12 (34.3)Group B:Mother median age: 24 (17;38)Country of birth, No. (%)The Netherlands +other: 2 (5.4)Mediterranean: 16 (43.2)Surinam: 7 (18.9)Asia: 12 (32.4)Eight infants (schedule A, three infants; schedule B, five infants) were excluded fromfurther analysis.
Participants
Group A: HBIG (0.5 mL/kg body weight) given within 2 hours of birth and PDV 10microgram 2 days after birth, 1, 2, and 11 months.Group B: HBIG (0.5 mL/kg body weight) and PDV 10 microgram at 3, 4, 5 and 11months (with diphtheria, pertussis, tetanus, poliomyelitis concomitantly. HBIG (0.5mL/kg body weight) was given at the age of 3 months.
Interventions
Number of HBsAg positive children in each group.Anti-HBs level.
Outcomes
Página 21
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Follow-up time: 12 months.Adverse events: no side-effect were observed after neither passive or activeimmunisation (data from Mazel et al, 1984, a duplication publication). The data in thistrial were not usable because the PDV vaccination schedule were different.
Notes
AAllocation concealment
Halliday 1992 ABStudy
Generation of allocation sequence: adequate - random code.Allocation concealment: adequate - by independent unit.Blinding: adequate - injection was administered by a doctor who was not part of theresearch team. No one on the research team, or in the laboratory that performed theHBV marker tests, knew which vaccine was administered or whether the infant receivedHBIG.Follow-up: adequate - number and reasons described in each groups.
Methods
Country: China.Publication language: English.Inclusion criteria:HBsAg positive mothers.infant weight equal to or greater than 2500 gm and a 5-minute Apgar score equal toor greater than 7or infant weights less than 2500 gm but greater than 1600 gm and a 5-minute Apgarscore of at least 9.Exclusion criteria:not reported.Participants:(1) Group A(2) Group B(3) Group C(4) Group D
Participants
Group A: Betagen (20 microgram, RV) at birth, and 1 and 6 months.Group B: Lanzhou (20 microgram, PDV) at birth, and 1 and 6 months.Group C: HBIG (260 IU) at birth and RV (10 microgram) at birth, and 1 and 6 months.Group D: HBIG (260 IU) at birth and RV (20 microgram) at birth, and 1 and 6 months.
Interventions
Percentage of infants with HBsAg at maxim (12 months) follow-up.Percentage of infants with HBsAg, by mother's HBsAg/HBeAg status.Geometric mean titre of anti-HBs in each group.Percentage of infants in each group with anti-HBsAg level higher than 10 mIU/mL.
Outcomes
Follow-up time: 12 months.Reasons not to entering the trial:living too far to travel for follow-up visitstoo many blood testsdid not want the baby to be hurtdid not think vaccination was necessarywould be going away.
Notes
AAllocation concealment
Halliday 1992 CAStudy
This trial is the same as Halliday 1992 BA, but has been entered with its own identifierdue to technical limits of RevMan in order to make data comparison.
Methods
Participants
Página 22
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Interventions
Outcomes
Notes
AAllocation concealment
Halliday 1992 DCStudy
This trial is the same as Halliday 1992 BA, but has been entered with its own identifierdue to technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
AAllocation concealment
Hieu 2002Study
Generation of allocation sequence: adequate - sequence generated by a computerprogram.Allocation concealment: adequate - sealed envelopes.Blinding: not performed.Follow-up: inadequate - not described.
Methods
Country: Vietnam.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.birth weight more than 2500 gm.Apgar score at least 8 at 1 minute.gestational age >= 37 completed weeks.In good general health as determined by birth history and physical examination.Exclusion criteria:Fever or significant malnutrition.confirmed HIV positive individuals.Evidence of significant haematological, cardiovascular or neoplastic disease.Participants:(1) Hepavax-Gene Group (n = 53)Mother's mean age: 26.8(2) Engerix-B Group (n = 51)Mother's mean age: 27.9
Participants
Hepavax-Gene Group : HBIG 100 microgram+ Hepavax 10 microgram I.M. at birth,then Hepavax at 30 days and 180 days of age.Engerix-B Group: HBIG 100 microgram+ Engerix-B 10 microgram I.M. at birth, thenEngerix-B at 30 days and 180 days of age.
Interventions
Number of infants with HBsAg during the follow-up period.Anti-HBsAnti-HBs titerGMT of Anti-HBsNumber of anti-HBc positive infants.
Outcomes
Página 23
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Characteristics of included studies
Follow-up times: 30-60-180-210-360 days and 2 years.Adverse events:The majority of AEs were mild fever of less than 38 C degree.One infant had mild hyperexcitability (excessive crying).
Notes
AAllocation concealment
Ip 1989 ABStudy
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: unclear - described as double blind, but method of blinding not described.Follow-up: inadequate - not described in each group.
Methods
Country: HongKong, China.Publication language: English.Inclusion criteria:HBeAg positive mothers.Participants:(1) Group A:(2) Group B:(3) Group C:(4) Group D: (control)
Participants
Group A: received four 3 microgram of PDV at birth and at the age of 1, 2, and 6 months,respectively. Also, received HBIG 200 IU at birth, and 100 IU at monthly intervals duringthe first 6 months after birth.Group B: received four 3 microgram of PDV at birth and at the age of 1, 2, and 6 months.Also, received HBIG 200 IU at birth.Group C: received four 3 microgram of PDV at birth and at the age of 1, 2, and 6 months.Group D: control group (not randomised).
Interventions
HBsAgHBeAg, HBV DNA
Outcomes
Follow-up time: 36 months.Adverse events: not reported.The code was broken in Oct, 1983. After that no new babies entered the placebo groupand eligible babies were only randomly allocated to one of the first three interventiongroups. Part of the infants of the Ip 1989 trial originated from the Wong 1984 trial.
Notes
BAllocation concealment
Ip 1989 ACStudy
This trial is the same as Ip 1989 AB, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Página 24
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Characteristics of included studies
Ip 1989 ADStudy
Generation of allocation sequence: unclear - not described.Allocation concealment: adequate.Blinding: adequate.Follow-up: inadequate - reasons for dropouts described only, number was not reported.
Methods
Página 25
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Country: China.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.Exclusion criteria:Infants birthweight less than 2500 gm, gestational age less than 37 weeks, Apgar scoreless than 7, or in whom there were gross congenital abnormalities.Participants:Group A (n = 36):Mothers:age (yr): 26.0+-4.3number of pregnancies: 1.7+-1.1parity: 0.6+-0.1duration of labour (minutes): 371+-268mode of delivery:normal: 64%forceps: 8%lower section caesarean section: 8%induction of labour: 28%Infants:males: 47%birthweight (gm): 3112+-307maturity (weeks): 40+-1breastfed: 18%Group B (n = 35):Mothers:age (yr): 24.20+-3.6number of pregnancies: 1.4+-0.8parity: 0.5+-1.0duration of labour (minutes): 452+-252mode of delivery:normal: 51%forceps: 23%lower section caesarean section: 26%induction of labour: 21%Infants:males: 60%birthweight (gm): 3204+-341maturity(weeks): 40+-1breastfed: 18%Group C (n = 35):Mothers:age (yr): 25.6+-4.1number of pregnancies: 1.5+-1.0parity: 0.5+-0.8duration of labour (minutes): 396+-243mode of delivery:normal: 60%forceps: 23%lower section caesarean section: 17%induction of labour: 20%Infants:males: 57%birthweight (gm): 3107+-393
Participants
Página 26
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
maturity(weeks): 40+-2breastfed: 21%Group D (n = 34):Mothers:age (yr): 24.6+-3.8number of pregnancies: 1.4+-0.6parity: 0.3+-0.6duration of labour (minutes): 430+-231mode of delivery:normal: 56%forceps: 12%lower section caesarean section: 32%induction of labour: 24%Infants:males: 47%birthweight (gm): 3231+-362maturity(weeks): 40+-2breastfed: 21%.
Group A: HBIG 200 IU and PDV 3 microgram were given at birth. Then HBIG 100 IUwas given at 1, 2, 3, 4, 5, and 6 months. PDV 3 microgram were given at 1, 2, and 6months.Group B: HBIG 200 IU was given at birth. Placebo B was given at 1, 2, 3, 4, 5 and 6months. PDV 3 microgram was given at birth, 1, 2 and 6 months.Group C: PDV 3 microgram was given at birth, 1, 2 and 6 months. Placebo B was givenat birth, 1, 2, 3, 4, 5 and 6 months.Group D: placebo B was given at birth, 1, 2, 3, 4, 5, and 6 months. Placebo A wasgiven at birth, 1, 2, and 6 months.
Interventions
HBsAg HBeAg Anti-HBs Anti-HBe IgM-anti-HBcOutcomes
Follow-up time: 12 months.Adverse events:No serious side-effects from the injections were noticed. Six mothers observed a smallswelling at the site of injection for 1 day; 6 babies had low-grade fever for 1 day; and2 babies had low-grade fever for 1 day.Definition of persistent HBsAg antigenemia: all babies having been HBsAg-positive forover 6 months. The Wong 1984 trial constituted part of the infants in the Ip 1989 trial.
Notes
AAllocation concealment
Ip 1989 BCStudy
This trial is the same as Ip 1989 AB, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Ip 1989 BDStudy
This trial is the same as Ip 1989 AD, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Página 27
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Participants
Interventions
Outcomes
Notes
AAllocation concealment
Ip 1989 CDStudy
This trial is the same as Ip 1989 AD, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
AAllocation concealment
Kang 1995Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - not described.
Methods
Country: China.Publication language: Chinese.Inclusion criteria:HBsAg+ HBeAg positive mothers.Participants:(1) Group A:(2) Group B:(3) Group C:
Participants
Group A: received 20 microgram of RV at birth and at the age of 1 and 6 months,respectively.Group B: received 20 microgram of genetic engineering vaccine at birth and at the ageof 1 and 6 months.Group C: received 10 microgram of genetic engineering vaccine and HBIG 200 IU atbirth and 10 microgram doses of genetic engineering vaccine at the age of 1 and 6months.
Interventions
HBsAg, Anti-HBsAnti-HBc
Outcomes
Follow-up time: 7 months1% soap solution was applied to avoid contamination by mothers' faeces.No adverse events was reported. Data was comparable for Group A and Group B.
Notes
BAllocation concealment
Página 28
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Khukhlovich 1996Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: unclear - described as double blind, but method of blinding not described.Follow-up: inadequate - not described.
Methods
Country: Uzbekistan and Moldova (former Soviet Union).Publication language: Russian.Inclusion criteria:HBsAg positive carrier mothers.The children were healthy without any contraindications.
Participants
Treatment Group: Engerix B 1 mL was given at birth, 1, 2, and 14 months.Control Group: no vaccines.
Interventions
Anti-HBs, HBsAg.Outcomes
Follow-up time:2 years.Adverse events: skin reactions, weak pain, little swollen of the injection site (transientreactions, disappeared within 1-3 days). Rare adverse events: without good sleep, overexcited, dyspepsia, subfebrile temperature. After the vaccination, no other adverseevent was observed.
Notes
BAllocation concealment
Kuru 1995 ABStudy
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: unclear.
Methods
Country: Turkey.Publication language: English.Inclusion criteria:HBsAg positive mothers.Participants:(1) Group A (Hevac B 0.5 mL)(2) Group B (Hevac B 1 mL)(3) Group C (Engerix B).
Participants
Group A (Hevac B 0.5 mL): received 2.5 microgram of vaccine and HBIG 200 IU atbirth and vaccine at the age of 1, 2, and 12 months, respectively.Group B (Hevac B 1 mL): received 5 microgram of vaccine and HBIG 200 IU at birthand vaccine at the age of 1, 2, and 12 months respectively.Group C (Engerix B 0.5 mL): received 10 microgram of vaccine and HBIG 200 IU atbirth and vaccine at the age of 1, 2, and 12 months, respectively.
Interventions
HBsAg,Anti-HBs (geometric mean titer, GMT),HBeAg, Anti-HBe.
Outcomes
Follow-up time:13 monthswithout the primary outcome defined in the protocol, which is Hepatitis B events atmaximum follow-up.Adverse events: no side effects in the infants after the vaccination.
Notes
BAllocation concealment
Página 29
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Kuru 1995 ACStudy
This trial is the same as Kuru 1995 AB, but has been entered with its own identifierdue to technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Kuru 1995 BCStudy
This trial is the same as Kuru 1995 AB, but has been entered with its own identifierdue to technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Lee 1995 ABStudy
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: Not performed.Follow-up: inadequate - number of dropouts reported, but reasons not described.
Methods
Country: Taiwan. Publication language: English. Inclusion criteria: HBsAg and HBeAgpositive/negative mothers.
Participants
Group A (HBeAg+ mother): HBIG 145 IU (0)+ PDV 5 microgram (0)+ Engerix-B 10microgram (1)+ Engerix-B 10 microgram (2)+ Engerix-B 10 microgram (12)Group B (HBeAg+ mother): HBIG 145 IU (0)+ PDV 5 microgram (0)+ PDV 5 microgram(1)+ PDV 5 microgram (2)+ PDV 5 microgram (12)Group C (HBeAg+ mother): HBIG 145 IU (0)+ PDV 5 microgram (0)+ H-B-VAX II 5microgram (1)+ H-B-VAX II 5 microgram (2)+ H-B-VAX II 5 microgram (12)Group D (HBeAg+ mother): HBIG 145 IU (0)+ PDV 5 microgram (0)+ PDV 5 microgram(1)+ H-B-VAX II 5 microgram (2)+ H-B-VAX II 5 microgram (12)Group E (HBeAg+ mother): HBIG 145 IU (0)+ PDV 5 microgram (0)+ PDV 5 microgram(1)+ Engerix-B 10 microgram (2)+ Engerix 10 microgram (12)Group F (HBeAg- mother): HBIG 145 IU (0)+ PDV 5 microgram (0)+ Engerix-B 10microgram (2)+ Engerix-B 10 microgram (6)Group G (HBeAg- mother): HBIG 145 IU (0)+ PDV 5 microgram (0)+ H-B-VAX II 5microgram(2)+ H-B-VAX II 5 microgram(6)
Interventions
HBsAg, HBeAg,Anti-HBs by radioimmunoassay.
Outcomes
Follow-up time: 6, 14, and 30 months (high risk infants).Adverse events: there was no significant adverse reaction in any of the children duringthe study period.
Notes
BAllocation concealment
Página 30
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Lee 1995 CAStudy
This trial is the same as Lee 1995 A1C, but has been entered with its own identifierdue to technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Lee 1995 CBStudy
This trial is the same as Lee 1995 A1C, but has been entered with its own identifierdue to technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Lee 1995 DEStudy
This trial is the same as Lee 1995 A1C, but has been entered with its own identifierdue to technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Liu 1987 ABStudy
Generation of allocation sequence: unclear - not described.Allocation concealment: adequate - sealed envelopes.Blinding: adequate - with placebo.Follow-up: inadequate - not described.
Methods
Country: China.Publication language: Chinese.Inclusion criteria:HBsAg+ HBeAg positive mothers or HBsAg titre >= 1:512.
Participants
Group A: received 20 microgram of vaccine at birth and at the age of 1, 2, and 6 months,respectively.Group B: placebo (normal saline) at birth and at the age of 1, 2, and 6 months,respectively.Group C: received 20 microgram of vaccine and HBIG 1: 1600,000 to 1: 3200,000(RIA) at birth and vaccine at the age of 1, 2, and 6 months respectively.
Interventions
Página 31
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
Characteristics of included studies
Overall number of HBsAg newborns in each tests.Anti-HBs, Anti-HBc (RIA)
Outcomes
Follow-up time: 6-9-12 months.The numbers of HBsAg newborns were the sum of number of HBsAg positive newbornsdetected in 6, 9 and 12 months, not only in 12 months follow-up.Adverse events: no systemic reaction and serious local events. Some infants had localswollen and red, but all disappeared in 1 to 2 days.
Notes
AAllocation concealment
Liu 1987 CAStudy
This trial is the same as Liu 1987 AC, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
AAllocation concealment
Liu 1987 CBStudy
This trial is the same as Liu 1987 AC, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
AAllocation concealment
Lo 1985 ABStudy
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: unclear.
Methods
Country: Taiwan.Publication language: English.Inclusion criteria:HBsAg+ HBeAg positive mothers.Mother age: 20 to 36 years, mean 27 years old.
Participants
Group A: received HBIG 50 IU at birth, then Hevac-B 5 microgram at 2 weeks, 6 weeks,and 10 weeks.Group B: received Hevac-B 5 microgram at 2 weeks, 6 weeks, and 10 weeks.Group C: received Hevac-B 5 microgram at 2 weeks, 6 weeks, and 10 weeks. PlusHBIG 50 IU at birth and one month of age.Group D: control group (refused vaccination).
Interventions
Página 32
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
The status of HBsAg and HBeAg in infantsNumber of infants with HBsAg positive in 6 weeks, 10 weeks and 6 months of age.The incidence of persistent HBsAg carrier state.A summary of adverse events of HBV vaccination.
Outcomes
Follow-up time: 6 weeks- 10 weeks- 6 months (all with number of infants HBsAg (+)).Adverse events:Fever: 2.8%Diarrhoea: 0.5%Swelling erythema: 6.6%Restlessness: 22.2%Two infants in Group 3 had an ALT rise. One was considered to be related to the useof traditional herbal drug. The other could not be accounted for. Both children returnedto normal ALT within the follow-up period.
Notes
BAllocation concealment
Lo 1985 CAStudy
This trial is the same as Lo 1985 BA, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Lo 1985 CBStudy
This trial is the same as Lo 1985 BA, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Lolekha 2002Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - not described.
Methods
Página 33
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Country: Thailand.Publication language: English.Inclusion criteria:HBsAg- and HBeAg-positive mothers.Infant birth weight >= 2000 gram, Apgar score >= 7 at 5 minutesParticipants:(1) Group AMale (%): 52Female (%): 48Birth weight (kg)Range: 2.15-4.26Mean: 3.1Median: 3.05(2) Group BMale (%): 51Female (%): 49Birth weight (kg)Range: 2.34-4.25Mean: 3.04Median: 3.02
Participants
Group A: received 5 microgram of vaccine at birth (0 to 3 days) and at the age of 1 and6 months, respectively.Group B: received 5 microgram of vaccine at birth (0 to 3 days) and at the age of 1, 2,and 12 months, respectively.
Interventions
HBsAgHBeAgAnti-HBcAnti-HBs
Outcomes
Follow-up time: 13 months.Adverse events: None of the vaccines had a serious adverse experience and nonewithdrew from the study because of a vaccine related adverse experience.
Notes
BAllocation concealment
Oon 1986 ABStudy
Generation of allocation sequence: adequate - by lottery or the use of coded numbers.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - not described.
Methods
Country: SingaporePublication language: English.Inclusion criteria:HBsAg positive and negative mothers.Participants:Group A: HBsAg (-) mothers (n = 28)Group B: HBeAg (-)/HBsAg (+) mothers (n = 188)Group C: HBeAg (+)/HBsAg (+) mothers (n = 99)Group D: HBsAg (-) mothers (n = 39)Group E: HBeAg (-)/HBsAg (+) mothers (n = 205)Group F: HBeAg (+)/HBsAg (+) mothers (n = 103)
Participants
Página 34
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Group A: 10 microgram PDV at birth, 1 and 2 months.Group B: 5 microgram PDV at birth, 1 and 2 months.Group C: HBIG 100 IU and 10 microgram PDV at birth and 10 microgram PDV at 1and 2 months.Group D: HBIG 0.5 mL (100 IU) and 5 microgram PDV at birth and 5 microgram PDVat 1 and 2 months.Group E: 5 microgram PDV at birth, 1 and 2 months.Group F: 10 microgram PDV at birth, 1 and 2 months.
Interventions
HBsAgHBeAgAnti-HBs
Outcomes
Follow-up time: 12 months.Adverse effects: none was observed during the surveillance period.
Notes
BAllocation concealment
Oon 1986 CDStudy
This trial is the same as Oon 1986 EB, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Piazza 1985Study
Generation of allocation sequence: adequate - random number.Allocation concealment: adequate - sealed envelopes.Blinding: unclear.Follow-up: adequate - reasons and numbers described.
Methods
Country: Italy.Publication language: English.Inclusion criteria:HBsAg-positive mothers. Mothers with HBsAg, anti-HBs, anti-HBc negative were alsoincluded in this study with different comparison groups.Participants: (partly included, some children were not infants)Group A: 2 withdrawn by their parents.Group B: 1 withdrawn by their parents.Group C: 5 withdrawn by their parents.Group D: 5 withdrawn by their parents.
Participants
Group A: HBIG 50 IU at birth, PDV 5 microgram within 5 days after birth and at 2months.Group B: HBIG 50 IU at birth, PDV 5 microgram within 5 days after birth and at 1 and2 months.Group C: PDV 5 microgram within 5 days after birth and at 2 months.Group D: PDV 5 microgram within 5 days after birth and at 1 and 2 months.
Interventions
HBsAgAnti-HBc
Outcomes
Página 35
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Follow-up time: 6 months.Adverse events: 2 children reported a sore arm after the 2nd dose of vaccine, and inboth the complaint resolved a few hours later. There were no other adverse reactions.
Notes
AAllocation concealment
Pongpipat 1986Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - reasons not described.
Methods
Country: Thailand.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.
Participants
Group A: HBIG (Gamma-protect) 200 IU (at birth) + Havac B 5 microgram (birth-1-2months).Group B: HBIG (Hepatect) 100 IU (0)+ HB vax (PDV) 10 microgram (birth-1-6 months).
Interventions
HBsAgAnti-HBc
Outcomes
Follow-up time: 12 months.Adverse events: neither local nor systemic reactions were observed after immunisation.
Notes
BAllocation concealment
Pongpipat 1988Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - number reported only.
Methods
Country: Thailand.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.Participants:Group A:Group B:
Participants
Group A (HBIG+ Hevac B): received 5 microgram of vaccine and HBIG 100 IU at birthand vaccine at the age of 1, 2, and 12 months, respectively.Group B (HBIG+ Hevac B): received 2 microgram of vaccine and HBIG 100 IU at birthand vaccine at the age of 1, 2, and 12 months respectively.
Interventions
GMT (anti-HBs)seroconversion rateHBsAgAnti-PreS2Anti-HBc
Outcomes
Follow-up time: 4, 6, 12, and 13 months.Adverse events: neither local nor systemic reactions were observed after immunizationwith HBIG and hepatitis B vaccine.
Notes
BAllocation concealment
Página 36
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Pongpipat 1989Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - number for dropouts described only.
Methods
Country: Thailand.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.Participants:Group A:Group B:
Participants
Group A (HBIG+ HBVax): received 10 microgram of PDV and HBIG 100 IU (0.5mL) atbirth and vaccine at the age of 1, 2, and 12 months, respectively.Group B (HBIG+ HBVax II): received 5 microgram of RV and HBIG 100 IU (0.5mL) atbirth and vaccine at the age of 1, 2, and 12 months respectively.
Interventions
GMT (anti-HBs)seroconversion rate (definition: higher than 5 mIU/mL after vaccination) HBsAg.
Outcomes
Follow-up time: 12 months.Adverse events: neither local nor systemic reactions were observed after immunizationwith HBIG and both kinds of hepatitis B vaccine.
Notes
BAllocation concealment
Poovorawan 1997Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - reasons for dropouts described only, number was not reported.
Methods
Country: Thailand.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.Weight of 2 kg or more at birth and with a 5 minute Apgar score of 7 or higher.
Participants
Open design without randomisationGroup A: were vaccinated with Engerix-B (RV) 10 microgram at birth and subsequentlyat 1, 2, and 12 months of age.Group B: were vaccinated with Engerix-B (RV) 10 microgram and HBIG 100 IU at birthand Engerix-B (RV) 10 microgram and Engerix-B 10 microgram subsequently at 1, 2,and 12 months of age.Randomised groups:Group C: were vaccinated with Engerix-B (RV) 10 microgram at birth and subsequentlyat 1 and 6 months of age.Group D: were vaccinated with Engerix-B (RV) 10 microgram and HBIG 100 IU at birthand Engerix-B 10 microgram subsequently at 1 and 6 months of age. A booster wasadministered at 60 months for Group C and Group D.
Interventions
HBsAgGMT (Anti-HBs)Anti-HBc
Outcomes
Página 37
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
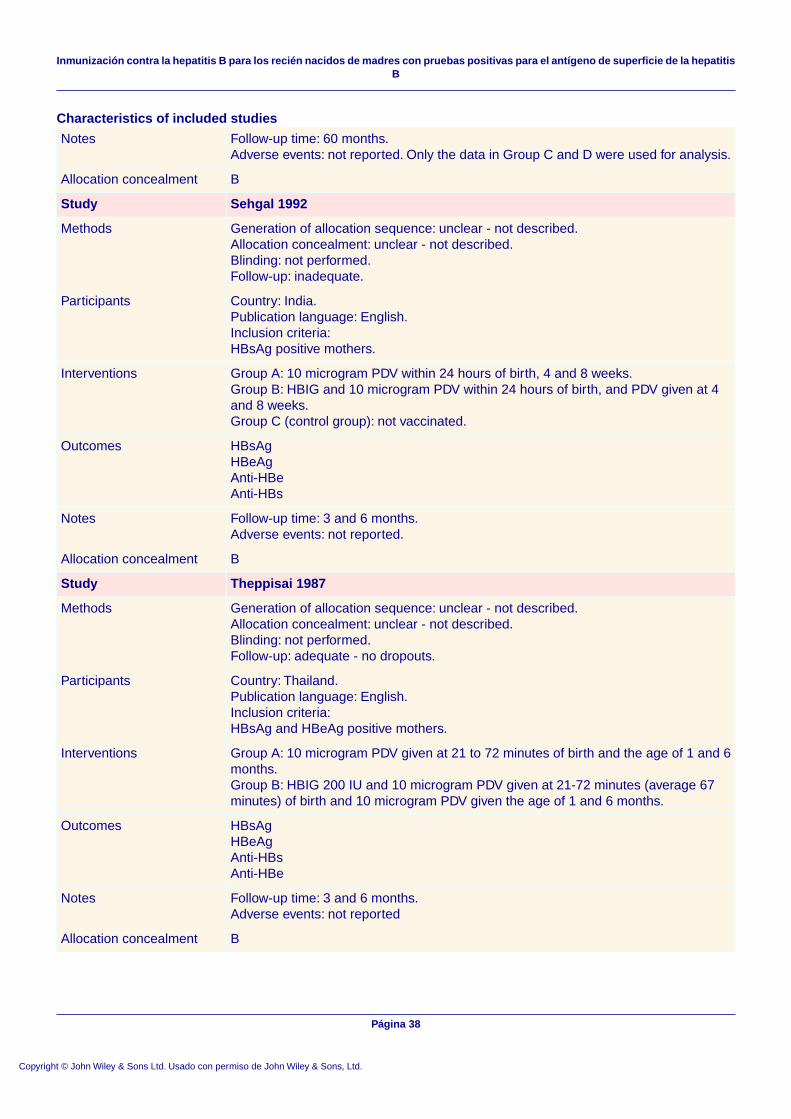
Characteristics of included studies
Follow-up time: 60 months.Adverse events: not reported. Only the data in Group C and D were used for analysis.
Notes
BAllocation concealment
Sehgal 1992Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate.
Methods
Country: India.Publication language: English.Inclusion criteria:HBsAg positive mothers.
Participants
Group A: 10 microgram PDV within 24 hours of birth, 4 and 8 weeks.Group B: HBIG and 10 microgram PDV within 24 hours of birth, and PDV given at 4and 8 weeks.Group C (control group): not vaccinated.
Interventions
HBsAgHBeAgAnti-HBeAnti-HBs
Outcomes
Follow-up time: 3 and 6 months.Adverse events: not reported.
Notes
BAllocation concealment
Theppisai 1987Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: adequate - no dropouts.
Methods
Country: Thailand.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.
Participants
Group A: 10 microgram PDV given at 21 to 72 minutes of birth and the age of 1 and 6months.Group B: HBIG 200 IU and 10 microgram PDV given at 21-72 minutes (average 67minutes) of birth and 10 microgram PDV given the age of 1 and 6 months.
Interventions
HBsAgHBeAgAnti-HBsAnti-HBe
Outcomes
Follow-up time: 3 and 6 months.Adverse events: not reported
Notes
BAllocation concealment
Página 38
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
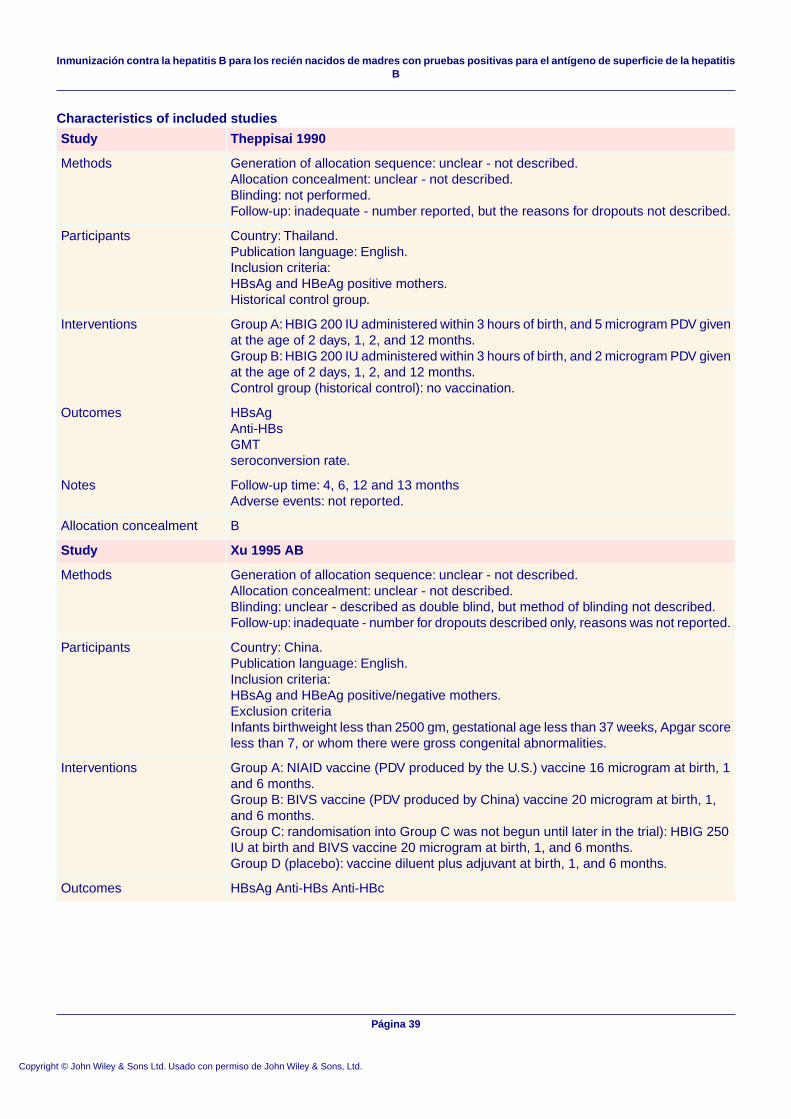
Characteristics of included studies
Theppisai 1990Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - number reported, but the reasons for dropouts not described.
Methods
Country: Thailand.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.Historical control group.
Participants
Group A: HBIG 200 IU administered within 3 hours of birth, and 5 microgram PDV givenat the age of 2 days, 1, 2, and 12 months.Group B: HBIG 200 IU administered within 3 hours of birth, and 2 microgram PDV givenat the age of 2 days, 1, 2, and 12 months.Control group (historical control): no vaccination.
Interventions
HBsAgAnti-HBsGMTseroconversion rate.
Outcomes
Follow-up time: 4, 6, 12 and 13 monthsAdverse events: not reported.
Notes
BAllocation concealment
Xu 1995 ABStudy
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: unclear - described as double blind, but method of blinding not described.Follow-up: inadequate - number for dropouts described only, reasons was not reported.
Methods
Country: China.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive/negative mothers.Exclusion criteriaInfants birthweight less than 2500 gm, gestational age less than 37 weeks, Apgar scoreless than 7, or whom there were gross congenital abnormalities.
Participants
Group A: NIAID vaccine (PDV produced by the U.S.) vaccine 16 microgram at birth, 1and 6 months.Group B: BIVS vaccine (PDV produced by China) vaccine 20 microgram at birth, 1,and 6 months.Group C: randomisation into Group C was not begun until later in the trial): HBIG 250IU at birth and BIVS vaccine 20 microgram at birth, 1, and 6 months.Group D (placebo): vaccine diluent plus adjuvant at birth, 1, and 6 months.
Interventions
HBsAg Anti-HBs Anti-HBcOutcomes
Página 39
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Follow-up time: 60 months, but due to the poor reporting, data on 6th month wereextracted.Adverse events: not reportedHBsAg event was defined as HBsAg positive at any time >= 1 month of age.Chronic HBsAg was defined as HBsAg positive for >= 6 months.
Notes
BAllocation concealment
Xu 1995 ADStudy
This trial is the same as Xu 1995 AB, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Xu 1995 BDStudy
This trial is the same as Xu 1995 AB, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Xu 1995 CBStudy
This trial is the same as Xu 1995 AB, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Xu 1995 CDStudy
This trial is the same as Xu 1995 AB, but has been entered with its own identifier dueto technical limits of RevMan in order to make data comparison.
Methods
Participants
Interventions
Outcomes
Notes
BAllocation concealment
Página 40
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
Yeoh 1986Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate.
Methods
Country: China.Publication language: English.Inclusion criteria:HBsAg-positive mothers.Infants birthweight over 2000 gm. Apgar score >= 7 at 5 minutes.
Participants
HBsAg(+)/ HBeAg(+) mothers (150 infants):Group A: HBIG 0.5 mL at birth and PDV 10 microgram were administered at birth, 1,and 6 months.Group B: HBIG 0.5 mL at birth and RV 5 microgram were administered at birth, 1, and6 months.HBsAg(+)/ HBeAg(-) mothers (150 infants).Group C: HBIG 0.5 mL at birth and PDV 10 microgram were administered at birth, 1,and 6 months.Group D: HBIG 0.5 mL at birth and RV 5 microgram were administered at birth, 1, and6 months.
Interventions
HBsAgHBeAgAnti-HBsAnti-HBcAnti-HBe
Outcomes
This trial was published as an abstract. We were not able to extract any relevant datafrom this abstract. Follow-up time: 6 and 9 months.Adverse events were few and minor, and no serious side-effects were attributable toeither vaccine.
Notes
BAllocation concealment
Zhu 1987Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: unclear - described as double blind, but method of blinding not described.Follow-up: inadequate.
Methods
Country: ChinaPublication language: English.Inclusion criteria:HBsAg positive mothers.
Participants
Treatment group: 16 microgram vaccine (PDV or RV ?) was given at birth, 1, and 6months.Control group (n = 57): buffer of HBV at the same interval.
Interventions
Transaminase abnormalities and hepatitis markers.Outcomes
Página 41
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of included studies
This trial was published as an abstract. We were not able to extract relevant data fromthis abstract.Follow-up time: 24 months.Adverse events: not reported.
Notes
BAllocation concealment
Zhu 1994Study
Generation of allocation sequence: unclear - not described.Allocation concealment: unclear - not described.Blinding: not performed.Follow-up: inadequate - number for dropouts described only, reasons was not reported.
Methods
Country: China.Publication language: English.Inclusion criteria:HBsAg and HBeAg positive mothers.Participants:Group 1 (RV):Birth weight: (mean+-SD): 3290+- 312Apgar score: 9.3No of male infants (%): 28 (52%)No of caesarean births (%): 9 (17%)Group 2 (PDV):Birth weight: (mean+-SD): 3301+- 347Apgar score: 9.1No of male infants (%): 26 (50%)No of caesarean births (%): 7 (14%)
Participants
Group A: RV 20 microgram was administered at birth, 1 and 6 months.Group B: PDV 20 microgram was administered at birth, 1, and 6 months.
Interventions
HBsAgAnti-HBs
Outcomes
Follow-up time: 6, 12, 24, 36, 48 and 60 months.Adverse events: These recipients of RV have no side effects and the vaccine is safe.Regarding Table 2 and 3. We considered '' negative'' patients as having no anti-HBsdespite it is unclear in the report.
Notes
BAllocation concealment
Characteristics of excluded studies
Reason for exclusionStudy
Non-randomised clinical study.Chung 1988
Not newborns of HBsAg-positive mothers.Chung 1988 B
Non-randomised clinical study.Coursaget 1984
Non-randomised clinical study.Da 1995
Non-randomised clinical study.Delage 1993
Non-randomised clinical study.Esteban 1986
The study population were not newborns but 1-12 year-old children.Goh 1992
Página 42
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Characteristics of excluded studies
Non-randomised clinical study.Kang 1986
The study population were not newborns but 3 months to 11 year-old children and the motherswere negative for all hepatitis B viral markers.
Lai 1986
The study population were not newborns but 3 months to 11 year-old children.Lai 1993
Non-randomised clinical study.Laille 1988
Non-randomised clinical study.Lin 1987
The study population were not high-risk newborns.Linder 2000
The study population were healthy newborns, not high-risk newborns of HBsAg-positivemothers.
Milne 1989
Non-randomised clinical study.Mittal 1994
The study population were healthy newborns, not high-risk newborns of HBsAg-positivemothers.
Moulia-Pelat 1994
Non-randomised clinical study.Nair 1984
The study population was not newborns of HBsAg-positive mothers.Okoth 1994
The study population in this study was not newborns of HBsAg-positive mothers.Perrin 1986
Non-randomised clinical study.Pongpipat 1984
Non-randomised clinical study.Poovorawan 1989
Non-randomised clinical study.Poovorawan 1990
Non-randomised clinical study.Shikata 1984
Non-randomised clinical study.Stevens 1987
Non-randomised clinical study.Stevens 1988
Non-randomised clinical study.Stevens 1990
Non-randomised clinical study.Stevens 1992
Non-randomised clinical study.Surya 1996
Non-randomised clinical study.Suwignyo 1994
Non-randomised clinical study.Theppisai 1988
Non-randomised clinical study.Theppisai 1989
Non-randomised clinical study.Wheeley 1991
Non-randomised clinical study.Young 2003
The study population was not newborns of HBsAg-positive mothers.Yuen 1999
Non-randomised clinical study.Zanetti 1986
The study population was not exclusively newborns of HBsAg-positive mothers.Zhu 2003
Página 43
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

TABLAS ADICIONALES
Table 01 Search strategies
Search strategyPeriodDatabase
vaccin* AND 'hepatitis B' AND (newborn* OR infant* OR child* ORbaby OR babies) AND 'high risk'
Until February2004
The CochraneHepato-Biliary GroupControlled Trials Register
A request for search on the Neonatal Group Controlled Trials Registerwas made (20 Feb, 2004)
20 February 2004The Cochrane NeonatalGroup Controlled TrialsRegister
A request for search on the Vaccine Field Controlled Trials Registerwas made (20 Feb, 2004). But no reply were obtained.
Not obtainedThe Cochrane VaccinesField Controlled TrialsRegister
vaccin* AND 'hepatitis B' AND (newborn* OR infant* OR child* ORbaby OR babies) AND 'high risk'
Until February2004
The Cochrane CentralRegister of ControlledTrials (CENTRAL/CCTR)in The Cochrane Library
#1 explode "Vaccination"/ all subheadings#2 explode "Hepatitis-B-Vaccines"/ all subheadings#3 explode "Vaccines"/ all subheadings#4 vaccin*#5 PDV#6 YDV#7 #1 or #2 or #3 or #4 or #5 or #6#8 explode "Hepatitis-B"/ all subheadings#9 hepatitis B#10 #8 or #9#11 explode "Infant-Newborn"/ all subheadings#12 newborn* or infant* or child* or baby or babies#13 #11 or #12#14 #13 and high risk#15 #7 and #10 and #14#16 random* or blind* or placebo* or meta-analysis#17 #15 and #16#18 (DTP-HB or Hib-HB or Comvax or Pediarix)
Until February2004
PubMed
Página 44
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Table 01 Search strategies
#1 explode "Vaccination"/ all subheadings#2 explode "Hepatitis-B-Vaccines"/ all subheadings#3 explode "Vaccines"/ all subheadings#4 vaccin*#5 PDV#6 YDV#7 #1 or #2 or #3 or #4 or #5 or #6#8 explode "Hepatitis-B"/ all subheadings#9 hepatitis B#10 #8 or #9#11 explode "Infant-Newborn"/ all subheadings#12 newborn* or infant* or child* or baby or babies#13 #11 or #12#14 #13 and high risk#15 #7 and #10 and #14#16 random* or blind* or placebo* or meta-analysis#17 #15 and #16#18 (DTP-HB or Hib-HB or Comvax or Pediarix)
January 1966 toFebruary 2004
MEDLINE
#1 explode "vaccination"/ all subheadings#2 explode "hepatitis-B-vaccine"/ all subheadings#3 explode "hepatitis-vaccine"/ all subheadings#4 explode "vaccine"/ all subheadings#5 vaccin*#6 PDV#7 YDV#8 #1 or #2 or #3 or #4 or #5 or #6 or #7#9 explode "hepatitis-B"/ all subheadings#10 hepatitis B#11 #9 or #10#12 explode "infant"/ all subheadings#13 explode "newborn"/ all subheadings#14 explode "newborn-hepatitis"/ all subheadings#15 explode "baby"/ all subheadings#16 #12 or #13 or #14 or #15#17 newborn* or infant* or child* or baby or babies#18 #16 or #17#19 #18 and high risk#20 #8 and #11 and #19#21 random* or blind* or placebo* or meta-analysis#22 #20 and #21#23 (DTP-HB or Hib-HB or Comvax or Pediarix)
January 1980 toFebruary 2004
EMBASE
Table 02 Intervention by group
Control groupIntervention groupTrial
B: RV 20 microgram at birth and at 1, 2, and12 months.
A*: HBIG 100 IU at birth and RV 20 microgram atbirth and at 1, 2, and 12 months.
Assateerawatt1993
B: saline at birth and 3 and 6 months.A: HBIG 1.0 ml (180 IU) at birth and saline at 3 and6 months. C: HBIG 0.5 ml (90 IU) diluted in 0.5 mlof immune serum globulin at birth and 3 and 6months.
Beasley 1983a
Página 45
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Table 02 Intervention by group
B: HBIG 0.5 ml (145 IU) and PDV 20microgram at 1 month. Followed by boosters1 and 6 months later.
A: HBIG 0.5 ml (145 IU) at birth and PDV 20microgram at 4-7 days. Followed by boosters 1 and6 months later.
Beasley 1983b
B: PDV 0.25 ml (5 microgram) at birth andat 6 weeks and 6 months.
A: PDV 0.25 ml (5 microgram) + HBIG 0.25 ml (25IU/kg) at birth then PDV + HBIG 0.25 ml (25 IU/kg)at 6 weeks and PDV at 6 months.
Farmer 1987
B: 10 microgram RV-2 at birth and at 1 and2 months.
A: 10 microgram RV-1 at birth and at 1 and 2months.
Garcia 1992
B: HBIG 0.5 ml/kg body weight and PDV 10microgram at 3, 4, 5, and 11 months (withdiphtheria, pertussis, tetanus, poliomyelitisconcomitantly). HBIG 0.5 ml/kg body weightat 3 months.
A: HBIG 0.5 ml/kg body weight at birth and PDV10 microgram at 2 days and at 1, 2, and 11 months.
Grosheide 1993
B: PDV 20 microgram at birth and at 1 and6 months. D: HBIG 260 IU at birth and RV10 microgram at birth and at 1 and 6 months.
A: RV 20 microgram at birth and at 1 and 6 months.C: HBIG 260 IU at birth and RV 20 microgram atbirth and at 1 and 6 months.
Halliday 1992
B: HBIG 100 microgram + 10 microgramRV-2 at birth and Engerix-B at 30 and 180days.
A: HBIG 100 microgram + 10 microgram RV-1 atbirth and Hepavax at 30 and 180 days.
Hieu 2002
B: PDV 3 microgram at birth and at 1, 2, and6 months + HBIG 200 IU at birth. D: placebo.
A: PDV 3 microgram at birth and at 1, 2, and 6months. Also, HBIG 200 IU at birth, and HBIG 100IU at monthly intervals during the first 6 monthsafter birth. C: PDV 3 microgram at birth and at 1,2, and 6 months.
Ip 1989
B: 20 microgram RV-2 at birth and at 1 and6 months.
A: 20 microgram RV-1 at birth and at 1 and 6months.
Kang 1995
B: No vaccines.A: RV 1 ml at birth and at 1, 2, and 14 months.Khukhlovich 1996
B: PDV 1 ml (5 microgram) and HBIG 200IU at birth and PDV at 1, 2, and 12 months.
A: PDV 0.5 ml (2.5 microgram) and HBIG 200 IUat birth and PDV at 1, 2, and 12 months. C: RV 0.5ml (10 microgram) and HBIG 200 IU at birth andRV at 1, 2, and 12 months.
Kuru 1995
B: HBIG 145 IU at birth + PDV 5 microgramat birth + PDV 5 microgram at 1, 2, and 12months.D: HBIG 145 IU at birth + PDV 5 microgramat birth and 1 month + 5 microgram RV-2 at2 and 12 months.F: HBIG 145 IU at birth + PDV 5 microgramat birth and RV-1 at 2 and 6 months.
A: HBIG 145 IU at birth + PDV 5 microgram at birth+ 10 microgram RV-1 at 1, 2, and 12 months.C: HBIG 145 IU at birth + PDV 5 microgram at birth+ 5 microgram RV-2 at 1, 2, and 12 months.E: HBIG 145 IU at birth + PDV 5 microgram at birthand 1 month + 10 microgram RV-1 at 2 and 12months.G: HBIG 145 IU at birth + PDV 5 microgram at birthand RV-2 at 2 and 6 months.
Lee 1995 *
B: placebo (normal saline) at birth and at 1,2, and 6 months.
A: PDV 20 microgram at birth and at 1, 2, and 6months. C: PDV 20 microgram at birth and at 1, 2,and 6 months and HBIG at birth.
Liu 1987
B: PDV 5 microgram at 2, 6, and 10 weeks.A: HBIG 50 IU at birth, then PDV 5 microgram at2, 6, and 10 weeks. C: PDV 5 microgram at 2, 6,and 10 weeks + HBIG 50 IU at birth and 1 month.
Lo 1985
Página 46
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Table 02 Intervention by group
B: RV 5 microgram at birth and at 1, 2, and12 months.
A: RV 5 microgram at birth and at 1 and 6 months.Lolekha 2002
B: PDV 5 microgram at birth and at 1 and 2months. D: HBIG 100 IU and PDV 5microgram at birth and PDV 5 microgram at1 and 2 months.
A: PDV 10 microgram at birth and at 1 and 2months. C: HBIG 100 IU and PDV 10 microgramat birth and PDV 10 microgram at 1 and 2 months.
Oon 1986
B:PDV 5 microgram and HBIG 50 IU at birthand PDV at 2 months.
A: PDV 5 microgram and HBIG 50 IU at birth andPDV at 1 and 2 months.
Piazza 1985
B: 100 IU HBIG-2 at birth + 10 microgramPDV2 at birth and at 1 and 6 months.
A: 200 IU HBIG-1 at birth + 5 microgram PDV1 atbirth and at 1 and 6 months.
Pongpipat 1986
B:PDV 2 microgram and HBIG 100 IU at birth+ PDV at 1, 2, and 12 months.
A: PDV 5 microgram and HBIG 100 IU at birth +PDV at 1, 2, and 12 months.
Pongpipat 1988
B: PDV 10 microgram and HBIG 100 IU atbirth and PDV at 1, 2, and 12 months.
A: RV 5 microgram and HBIG 100 IU at birth andRV at 1, 2, and 12 months.
Pongpipat 1989
B: RV 10 microgram at birth and at 1 and 6months. A booster was administered at 60months.
A: RV 10 microgram and HBIG 100 IU at birth andRV 10 microgram at 1 and 6 months. A boosterwas administered at 60 months.
Poovorawan 1997
B: PDV 10 microgram at birth and at 4 and8 weeks.
A: HBIG 0.5 ml and PDV 10 microgram at birth,and PDV at 4 and 8 weeks.
Sehgal 1992
B: PDV 10 microgram at birth and at 1 and6 months.
A: HBIG 200 IU and PDV 10 microgram at birth andPDV 10 microgram at 1 and 6 months.
Theppisai 1987
B: HBIG 200 IU at birth and PDV 2microgram at the age of 2 days, 1, 2, and 12months.
A: HBIG 200 IU at birth and PDV 5 microgram atthe age of 2 days, 1, 2, and 12 months.
Theppisai 1990
B: 20 microgram PDV-2 at birth and at 1 and6 months. D: vaccine diluent plus adjuvantat birth and at 1 and 6 months.
A: 16 microgram PDV-1 at birth and at 1 and 6months. C: HBIG 250 IU at birth and 20 microgramPDV2 at birth and at 1 and 6 months.
Xu 1995
B: HBsAg(+)/ HBeAg(+) mothers (150infants): HBIG 0.5 ml at birth and RV 5microgram at birth and at 1 and 6 months.D: HBsAg(+)/ HBeAg(-) mothers (150infants). HBIG 0.5 ml at birth and RV 5microgram at birth and at 1 and 6 months.
A: HBsAg(+)/ HBeAg(+) mothers (150 infants):HBIG 0.5 ml at birth and PDV 10 microgram at birthand at 1 and 6 months. C: HBsAg(+)/ HBeAg(-)mothers (150 infants). HBIG 0.5 ml at birth andPDV 10 microgram at birth and at 1 and 6 months.
Yeoh 1986
B: buffer of HBV given at birth, 1 and 6months
A: 16 microgram vaccine given at birth, 1 and 6months.
Zhu 1987
B: PDV 20 microgram at birth and at 1 and6 months.
A: RV 20 microgram at birth and at 1 and 6 months.Zhu 1994
* HBeAg-positivemothers in A to Egroups.HBeAg-negativemothers in F andG group.
Página 47
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

CARÁTULA
Inmunización contra la hepatitis B para los recién nacidos de madres conpruebas positivas para el antígeno de superficie de la hepatitis B
Titulo
Lee C, Gong Y, Brok J, Boxall EH, Gluud CAutor(es)
CL desarrollaron la estrategia de búsqueda, identificaron los ensayos, extrajeronlos datos, realizaron los análisis estadísticos y redactaron partes de la revisión.YG extrajo los datos, realizó los análisis estadísticos, redactó partes de larevisión y la revisó.YG es el garante.JB validó la evaluación de la calidad metodológica de los ensayos incluidos,validó los datos de 6 ensayos seleccionados al azar, redactó partes de la revisióny la revisó.EHB tiene experiencia de investigación en este tema. Proporcionó ensayospara esta revisión, validó la extracción de datos y examinó la revisión.CG coordinó la revisión, actuó como árbitro en los casos de desacuerdo, redactópartes de la revisión y la revisó.
Contribución de los autores
2004/2Número de protocolo publicadoinicialmente
2006/2Número de revisión publicadainicialmente
22 febrero 2006Fecha de la modificación másreciente"
22 febrero 2006"Fecha de la modificaciónSIGNIFICATIVA más reciente
El autor no facilitó la informaciónCambios más recientes
El autor no facilitó la informaciónFecha de búsqueda de nuevosestudios no localizados
El autor no facilitó la informaciónFecha de localización de nuevosestudios aún noincluidos/excluidos
01 febrero 2004Fecha de localización de nuevosestudios incluidos/excluidos
El autor no facilitó la informaciónFecha de modificación de lasección conclusiones de losautores
Página 48
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Dr Yan GongCopenhagen Trial UnitCentre for Clinical Intervention Research, Copenhagen University HospitalDept. 7102, Blegdamsvej 9H:S RigshospitaletCopenhagenDK-2100DENMARKTélefono: +45 3545 7161E-mail: [email protected]: +45 3545 7101
Dirección de contacto
CD004790Número de la Cochrane Library
Cochrane Hepato-Biliary GroupGrupo editorial
HM-LIVERCódigo del grupo editorial
RESUMEN DEL METANÁLISIS
01 Vacuna versus placebo o ninguna intervención
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
0.28 [0.20, 0.40]Riesgo Relativo (efectosfijos) IC del 95%
403501 Eventos de hepatitis B segúnel tipo de vacuna
0.28 [0.20, 0.40]Riesgo Relativo (efectosfijos) IC del 95%
403502 Eventos de hepatitis B segúnla calidad metodológica
Subtotalesúnicamente
Riesgo Relativo (efectosfijos) IC del 95%
03 Eventos de hepatitis B -Análisis de sensibilidad
0.29 [0.20, 0.41]Riesgo Relativo (efectosfijos) IC del 95%
403704 Eventos de hepatitis B segúnel estado de HBeAg de la madre
0.28 [0.20, 0.40]Riesgo Relativo (efectosfijos) IC del 95%
403505 Eventos de hepatitis B segúnla primera administración de lavacuna
02 VR versus VDP
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
1.00 [0.70, 1.42]Riesgo Relativo (efectosfijos) IC del 95%
382501 Eventos de hepatitis B
1.00 [0.70, 1.42]Riesgo Relativo (efectosfijos) IC del 95%
382502 Eventos de hepatitis B segúnla calidad metodológica
Subtotalesúnicamente
Riesgo Relativo (efectosfijos) IC del 95%
03 Eventos de hepatitis B -análisis de sensibilidad
1.00 [0.70, 1.42]Riesgo Relativo (efectosfijos) IC del 95%
382504 Eventos de hepatitis B segúnel estado de HBeAg de la madre
Página 49
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
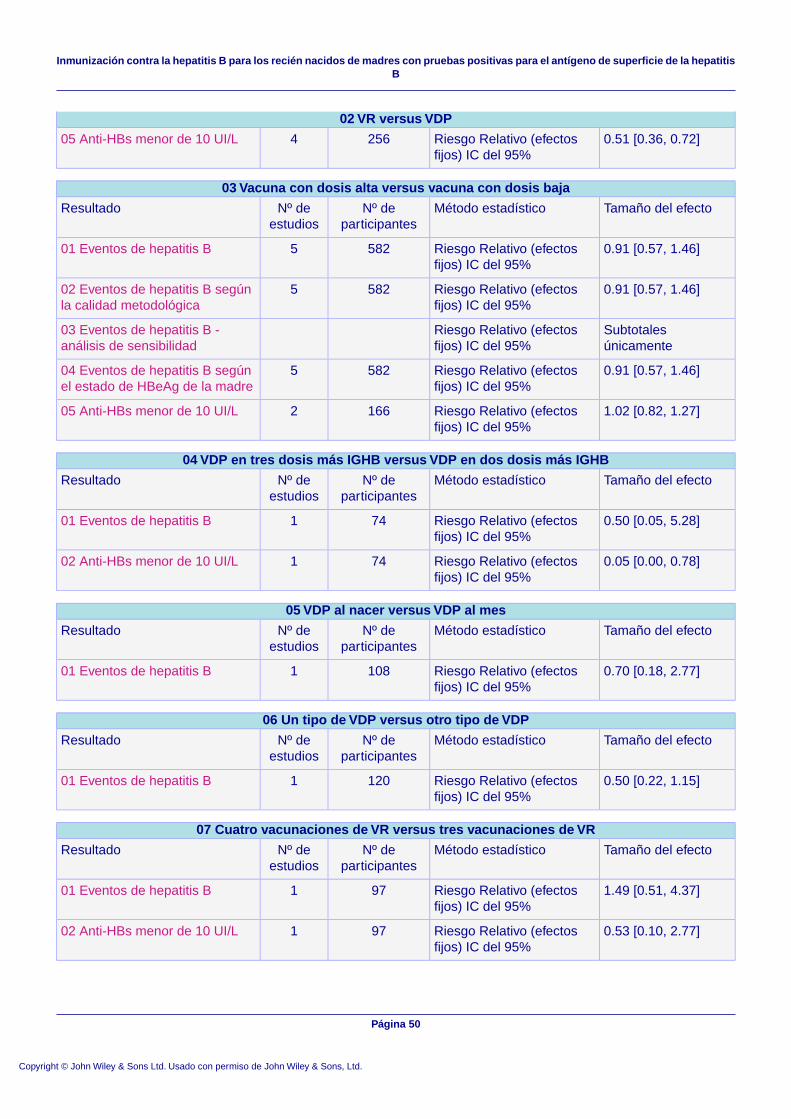
02 VR versus VDP
0.51 [0.36, 0.72]Riesgo Relativo (efectosfijos) IC del 95%
256405 Anti-HBs menor de 10 UI/L
03 Vacuna con dosis alta versus vacuna con dosis baja
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
0.91 [0.57, 1.46]Riesgo Relativo (efectosfijos) IC del 95%
582501 Eventos de hepatitis B
0.91 [0.57, 1.46]Riesgo Relativo (efectosfijos) IC del 95%
582502 Eventos de hepatitis B segúnla calidad metodológica
Subtotalesúnicamente
Riesgo Relativo (efectosfijos) IC del 95%
03 Eventos de hepatitis B -análisis de sensibilidad
0.91 [0.57, 1.46]Riesgo Relativo (efectosfijos) IC del 95%
582504 Eventos de hepatitis B segúnel estado de HBeAg de la madre
1.02 [0.82, 1.27]Riesgo Relativo (efectosfijos) IC del 95%
166205 Anti-HBs menor de 10 UI/L
04 VDP en tres dosis más IGHB versus VDP en dos dosis más IGHB
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
0.50 [0.05, 5.28]Riesgo Relativo (efectosfijos) IC del 95%
74101 Eventos de hepatitis B
0.05 [0.00, 0.78]Riesgo Relativo (efectosfijos) IC del 95%
74102 Anti-HBs menor de 10 UI/L
05 VDP al nacer versus VDP al mes
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
0.70 [0.18, 2.77]Riesgo Relativo (efectosfijos) IC del 95%
108101 Eventos de hepatitis B
06 Un tipo de VDP versus otro tipo de VDP
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
0.50 [0.22, 1.15]Riesgo Relativo (efectosfijos) IC del 95%
120101 Eventos de hepatitis B
07 Cuatro vacunaciones de VR versus tres vacunaciones de VR
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
1.49 [0.51, 4.37]Riesgo Relativo (efectosfijos) IC del 95%
97101 Eventos de hepatitis B
0.53 [0.10, 2.77]Riesgo Relativo (efectosfijos) IC del 95%
97102 Anti-HBs menor de 10 UI/L
Página 50
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

08 Un tipo de VR versus otro tipo de VR con el mismo esquema de vacunación
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
Subtotalesúnicamente
Riesgo Relativo (efectosfijos) IC del 95%
01 Eventos de hepatitis B
Subtotalesúnicamente
Riesgo Relativo (efectosfijos) IC del 95%
02 Anti-HBs menor de 10 UI/L
09 IGHB versus placebo o ninguna intervención
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
0.52 [0.44, 0.63]Riesgo Relativo (efectosfijos) IC del 95%
10861401 Eventos de hepatitis B
0.52 [0.44, 0.63]Riesgo Relativo (efectosfijos) IC del 95%
10861402 Eventos de hepatitis B segúnla calidad metodológica de losensayos
Subtotalesúnicamente
Riesgo Relativo (efectosfijos) IC del 95%
03 Eventos de hepatitis B -análisis de sensibilidad
0.52 [0.44, 0.63]Riesgo Relativo (efectosfijos) IC del 95%
10861504 Eventos de hepatitis B segúnel estado de HBeAg de la madre
0.52 [0.44, 0.63]Riesgo Relativo (efectosfijos) IC del 95%
10861405 Eventos de hepatitis B segúnel tiempo de administración de laIGHB
0.53 [0.39, 0.74]Riesgo Relativo (efectosfijos) IC del 95%
711906 Eventos de hepatitis B segúnun esquema de vacunas estándary rápido
1.55 [0.89, 2.73]Riesgo Relativo (efectosfijos) IC del 95%
348407 Anti-HBs menor de 10 UI/L
Subtotalesúnicamente
Diferencia de mediasponderada (efectos fijos) ICdel 95%
08 Título de anti-HBs
3.47 [0.14, 83.67]Riesgo Relativo (efectosfijos) IC del 95%
136109 Eventos adversos
10 IGHB múltiple más VDP versus IGHB simple más VDP
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
0.87 [0.30, 2.47]Riesgo Relativo (efectosfijos) IC del 95%
198201 Eventos de hepatitis B
11 VDP más IGHB versus placebo o ninguna intervención
Tamaño del efectoMétodo estadísticoNº departicipantes
Nº deestudios
Resultado
0.08 [0.03, 0.17]Riesgo Relativo (efectosfijos) IC del 95%
246401 Eventos de hepatitis B
Página 51
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

11 VDP más IGHB versus placebo o ninguna intervención
0.08 [0.03, 0.17]Riesgo Relativo (efectosfijos) IC del 95%
246402 Eventos de hepatitis B segúnla calidad metodológica de losensayos
Subtotalesúnicamente
Riesgo Relativo (efectosfijos) IC del 95%
03 Eventos de hepatitis B -análisis de sensibilidad
0.08 [0.04, 0.18]Riesgo Relativo (efectosfijos) IC del 95%
246504 Eventos de hepatitis B segúnel estado de HBeAg de la madre
0.08 [0.03, 0.17]Riesgo Relativo (efectosfijos) IC del 95%
246405 Eventos de hepatitis B segúnel tiempo de administración de laIGHB
0.29 [0.07, 1.13]Riesgo Relativo (efectosfijos) IC del 95%
105206 Eventos adversos
GRÁFICOS Y OTRAS TABLAS
Fig. 01 Vacuna versus placebo o ninguna intervención
01.01 Eventos de hepatitis B según el tipo de vacuna
Página 52
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

01.02 Eventos de hepatitis B según la calidad metodológica
Página 53
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

01.03 Eventos de hepatitis B - Análisis de sensibilidad
Página 54
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
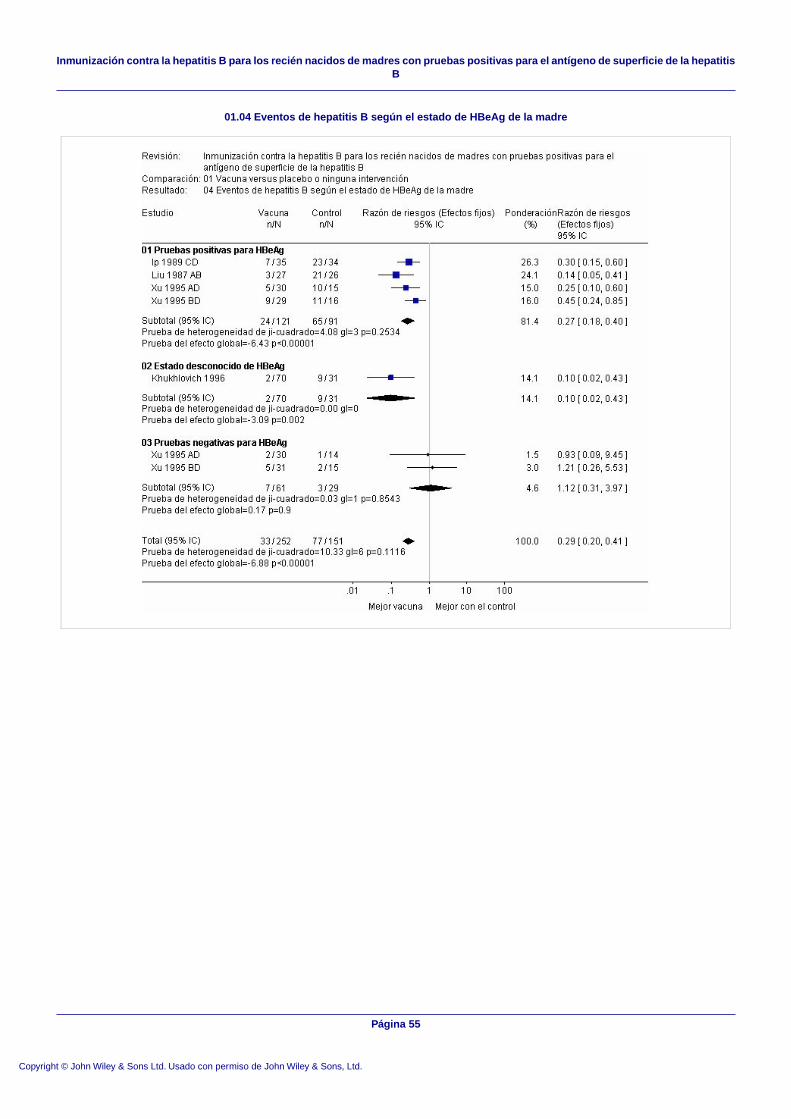
01.04 Eventos de hepatitis B según el estado de HBeAg de la madre
Página 55
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

01.05 Eventos de hepatitis B según la primera administración de la vacuna
Página 56
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Fig. 02 VR versus VDP
02.01 Eventos de hepatitis B
02.02 Eventos de hepatitis B según la calidad metodológica
Página 57
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

02.03 Eventos de hepatitis B - análisis de sensibilidad
Página 58
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

02.04 Eventos de hepatitis B según el estado de HBeAg de la madre
02.05 Anti-HBs menor de 10 UI/L
Página 59
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Fig. 03 Vacuna con dosis alta versus vacuna con dosis baja
03.01 Eventos de hepatitis B
Página 60
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

03.02 Eventos de hepatitis B según la calidad metodológica
Página 61
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

03.03 Eventos de hepatitis B - análisis de sensibilidad
Página 62
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

03.04 Eventos de hepatitis B según el estado de HBeAg de la madre
03.05 Anti-HBs menor de 10 UI/L
Página 63
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Fig. 04 VDP en tres dosis más IGHB versus VDP en dos dosis más IGHB
04.01 Eventos de hepatitis B
04.02 Anti-HBs menor de 10 UI/L
Fig. 05 VDP al nacer versus VDP al mes
05.01 Eventos de hepatitis B
Página 64
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Fig. 06 Un tipo de VDP versus otro tipo de VDP
06.01 Eventos de hepatitis B
Fig. 07 Cuatro vacunaciones de VR versus tres vacunaciones de VR
07.01 Eventos de hepatitis B
07.02 Anti-HBs menor de 10 UI/L
Página 65
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Fig. 08 Un tipo de VR versus otro tipo de VR con el mismo esquema de vacunación
08.01 Eventos de hepatitis B
08.02 Anti-HBs menor de 10 UI/L
Página 66
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Fig. 09 IGHB versus placebo o ninguna intervención
09.01 Eventos de hepatitis B
Página 67
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

09.02 Eventos de hepatitis B según la calidad metodológica de los ensayos
Página 68
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

09.03 Eventos de hepatitis B - análisis de sensibilidad
Página 69
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
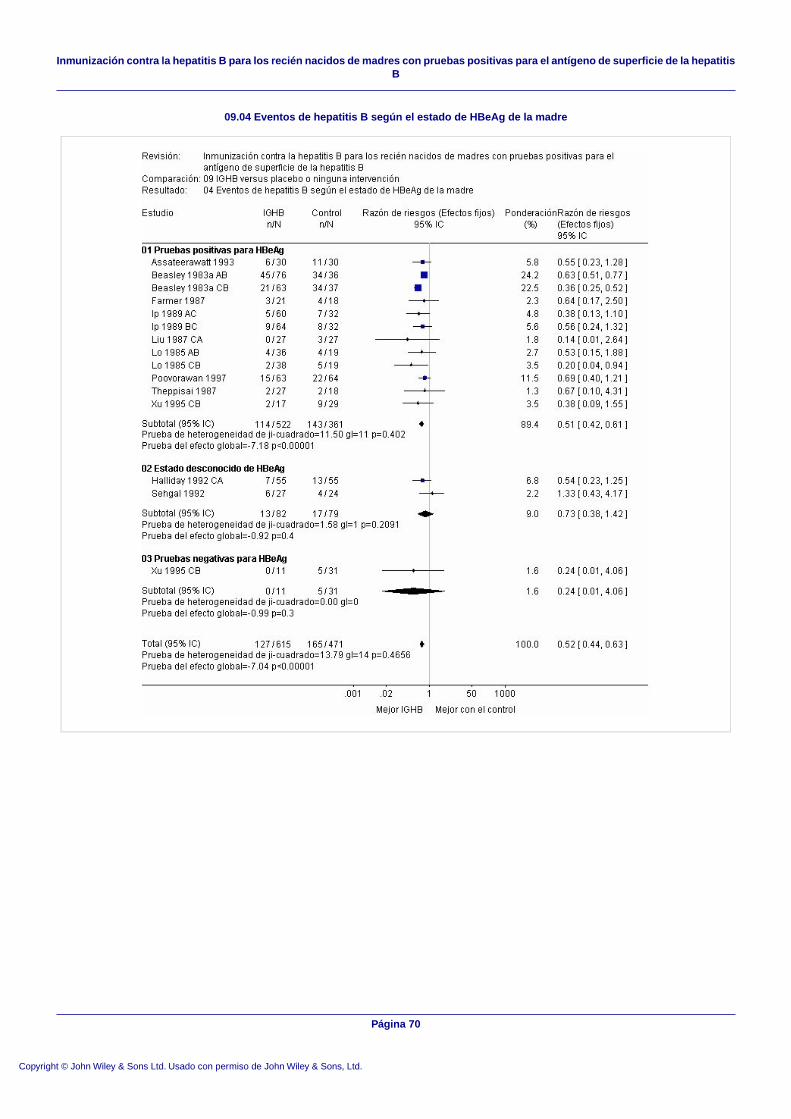
09.04 Eventos de hepatitis B según el estado de HBeAg de la madre
Página 70
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

09.05 Eventos de hepatitis B según el tiempo de administración de la IGHB
Página 71
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

09.06 Eventos de hepatitis B según un esquema de vacunas estándar y rápido
Página 72
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

09.07 Anti-HBs menor de 10 UI/L
09.08 Título de anti-HBs
09.09 Eventos adversos
Página 73
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

Fig. 10 IGHB múltiple más VDP versus IGHB simple más VDP
10.01 Eventos de hepatitis B
Fig. 11 VDP más IGHB versus placebo o ninguna intervención
11.01 Eventos de hepatitis B
Página 74
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

11.02 Eventos de hepatitis B según la calidad metodológica de los ensayos
Página 75
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB

11.03 Eventos de hepatitis B - análisis de sensibilidad
Página 76
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
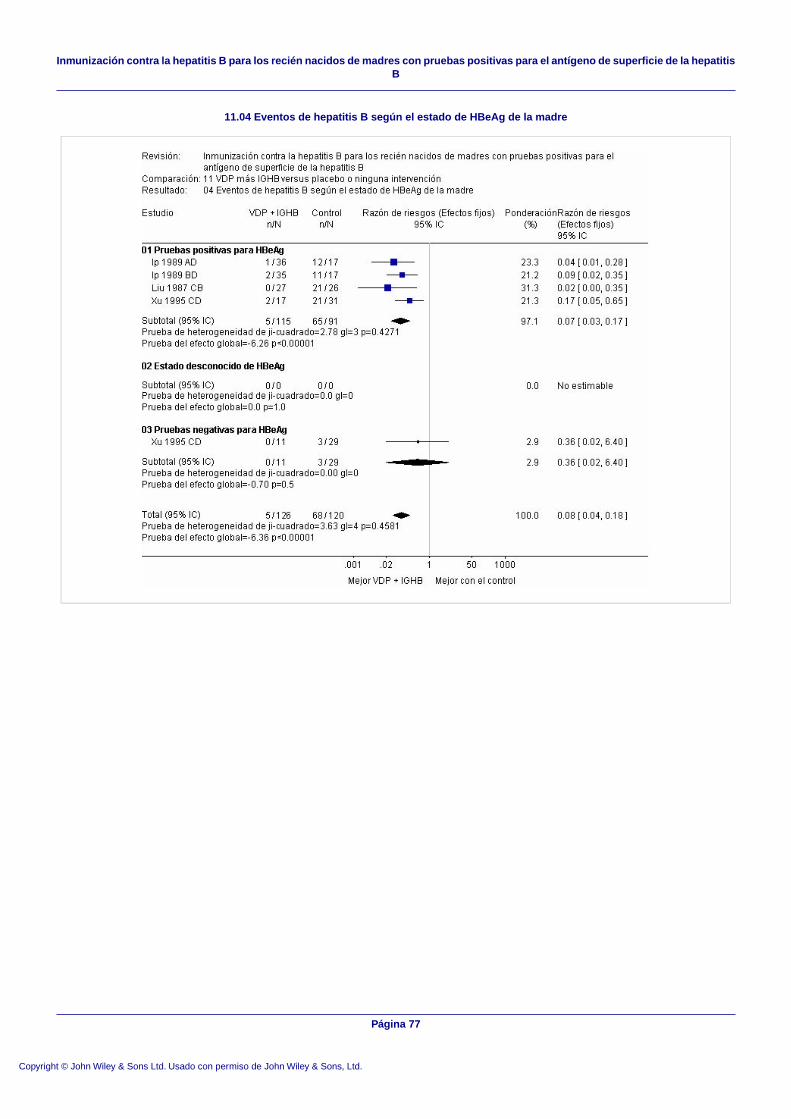
11.04 Eventos de hepatitis B según el estado de HBeAg de la madre
Página 77
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB
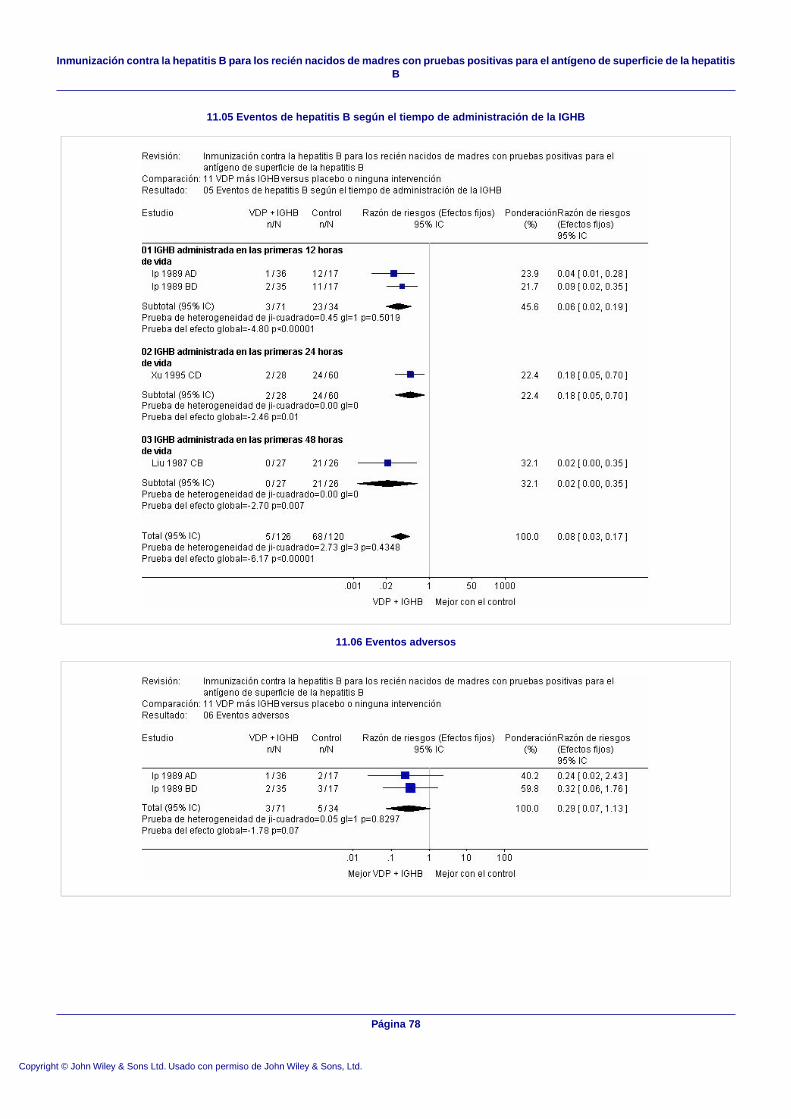
11.05 Eventos de hepatitis B según el tiempo de administración de la IGHB
11.06 Eventos adversos
Página 78
Copyright © John Wiley & Sons Ltd. Usado con permiso de John Wiley & Sons, Ltd.
Inmunización contra la hepatitis B para los recién nacidos de madres con pruebas positivas para el antígeno de superficie de la hepatitisB