Presentation Lapsus Kardiologi
24
Case Report : ST Elevation Myocardial Infarction Presented by Dzulfadhil Syamsir Supervisor Dr. Abdul Hakim Alkatiri, Sp.JP, FIHA Department Of Cardiology And Vascular Medicine Medical Faculty Of Hasanuddin University Makassar 2016
-
Upload
fadhil-syamsir -
Category
Documents
-
view
230 -
download
0
description
Laporan Kasus Passion STEMI
Transcript of Presentation Lapsus Kardiologi
Case Report :ST Elevation Myocardial Infarction
Presented byDzulfadhil Syamsir
SupervisorDr. Abdul Hakim Alkatiri, Sp.JP, FIHA
Department Of Cardiology And Vascular MedicineMedical Faculty Of Hasanuddin UniversityMakassar2016

Patient IdentityName : Mr. BT
Date of Birth / Age: 11-09-1958 / 57 y.o
ID : 450384
Occupation : Civil Worker
Marriage Status : Marriage
Addres : Pangkep
Date Of Admission : 09/02/2016

HistoryChief Complaint : BreathlessAnamnesis : Suffered since 1 weak ago, worsened one day ago. DOE (+),
Ortophneu (-), PND (-). Patient sleep with two pillows. There are chest pain and epigastric pain but not spesific. Cough since one week ago without sputum. There is history of nausea
but no vomiting, there is no history of fever. Defecation and urination are good.

HistoryPast History :• History of chest pain about 5 years ago with result of coronary
angiography is narrowing of 3 artery of the heart• Hipertension since 5 years ago, with sistolic pressure about 160 but
not regulary take medication.• History of smoking• History of diabetes mellitus, not regulary take medication.• No history of alcohol consumption• No history of heart disease in family

Physical Examination• General Condition Moderate Illness/Well Nourished / Compos Mentis (GCS 15)• Vital Sign
• Blood pressure : 150/100 mmHg
• Heart rate : 110 bpm
• Respiratory rate : 33 rpm
• Temperature : 36,5 oC

Physical Examination• Cor :
• Inspection : ictus cordis not visible• Palpation : ictus cordis not palpable, thrill (-)• Percussion :
Upper border 2nd ICS sinistraRight border 4th ICS linea parasternalis dextraLeft border 5th ICS linea axillaris anterior sinistra
• Auscultation : heart sound I/II pure, regular, murmur (-)
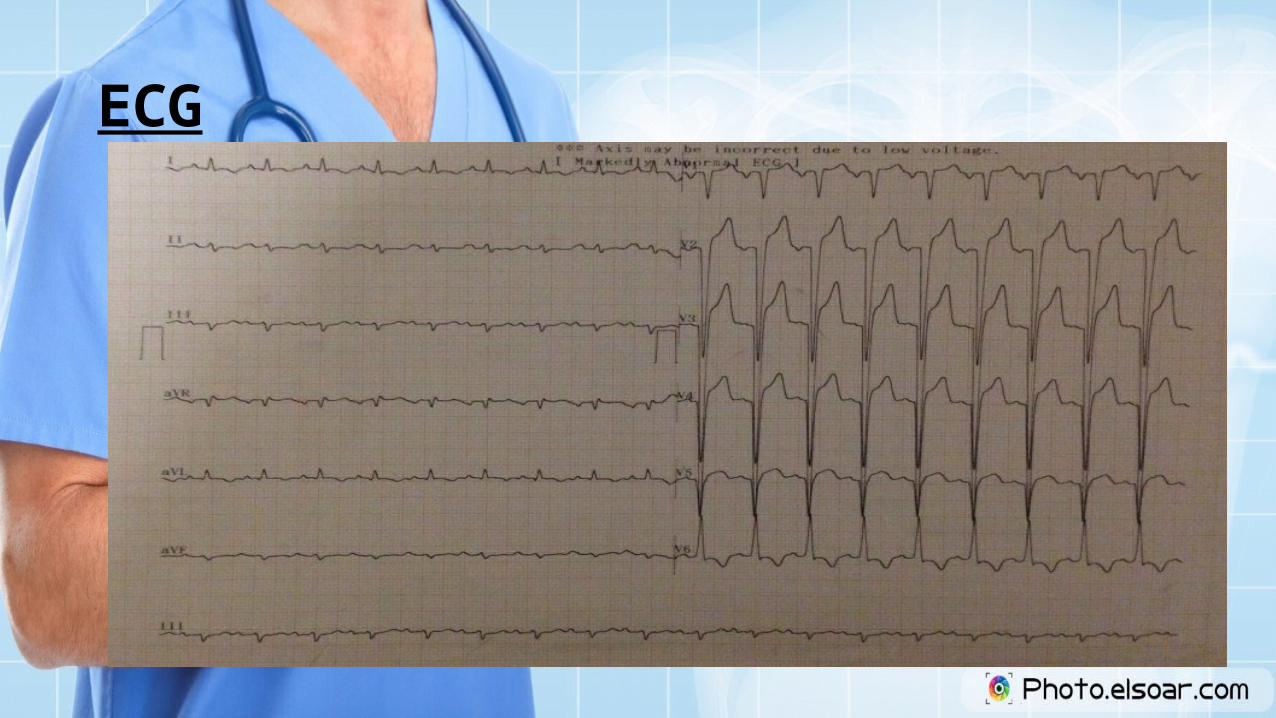
ECG

Laboratory ExaminationTEST RESULT NORMAL VALUE
WBC 11000 x 103/uL 4.0 – 10.0 x 103
RBC 4.71 4.0 – 6.0 x 106
HGB 14,9 12 – 16
HCT 44,4 37 – 48
PLT 188x 103/uL 150 – 400 x 103
PT 11,7 10 - 14
APTT 27,9 22,0 - 30,0
INR 1.13
GDS 347mg/dl 140
GD2PP - <200
SGOT 36 u/L <38
SGPT 45 u/L <41
TEST RESULT NORMAL VALUE
Tot.Choles 212mg/dl 200
HDL 51 mg/dl >59
LDL 121 mg/dl 130
Trigliserida 134 mg/dl 200
Ureum 36 10-50
Kreatinin 1,09 0,5-1,2
Troponin I 0,13 <0,01
CK 204 <190
CKMB 59,7 <25
Natrium 134 136 - 145
Kalium 4,9 3,5 - 5,1
Klorida 106 97 - 111
Asam Urat - 3,4-7,0

X-Ray Imaging

Resume• Male, 52 y.o, admitted to the hospital with chief complaint breatless
since one week ago and worsened one day ago. DOE (+), chest pain (+) epigastric pain (+), cough (+) w.o sputum.
• History of chest pain 5 years ago with result of coronary angiography is narrowing of 3 artery in the heart but patient refused PCI.
• History of smoking, History of hipertension and DM since 5 years ago but not taking medication regulary.

Resume• ECG shown sinus tachycardia, regular, HR 115 bpm, normoaxis,
anteroseptal wall myocardial infarction and LVH• Laboratory result WBC : 11.100, GDS : 347, CK 204, CKMB 59,7,
Troponin I 0,13.• Chest X-Ray Cardiomegaly with signs of pulmonary edema and
Dilatatatio elongation et atherosclerosis aortae

Diagnosis• STEMI onset >12 hours, KILLIP II• Hipertensi Heart Disease• DM Tipe II Non Obesed

Treatment• Oksigen 2-4 lpm via nasal kanul• IVFD NaCl 0,9% 500 cc/24 hours/IV• Aspilet 160mg 80mg/24 hours/oral• Clopidogrel 300mg 75 mg/24 hours/oral• Isosorbid 10 mg/8 hours/oral• Arixtra 2,5mg/24 hours /SC• Furosemide 40mg/12 hours/IV• Captopril 12.5mg/8 hours /oral• Atorvastatin 20 mg/24 hours/oral• Alprazolam 0,5mg/24 hours/oral• Laxadyne syr 10ml/24 hours/oral• Levemir 0-0-10 mcg/SC• Novorapid 6-6-6 mcg/SC

Discussion…..

Anatomy & Physiology

Definition of ACSAcute coronary syndrome (ACS) refers to a spectrum of clinical presentations ranging from those for ST-segment elevation myocardial infarction (STEMI) to presentations found in non–ST-segment elevation myocardial infarction (NSTEMI) or in unstable angina. It is almost always associated with rupture of an atherosclerotic plaque and partial or complete thrombosis of the infarct-related artery.

Pathopyhsiology

Pathopyhsiology

Diagnosis

Diagnosis
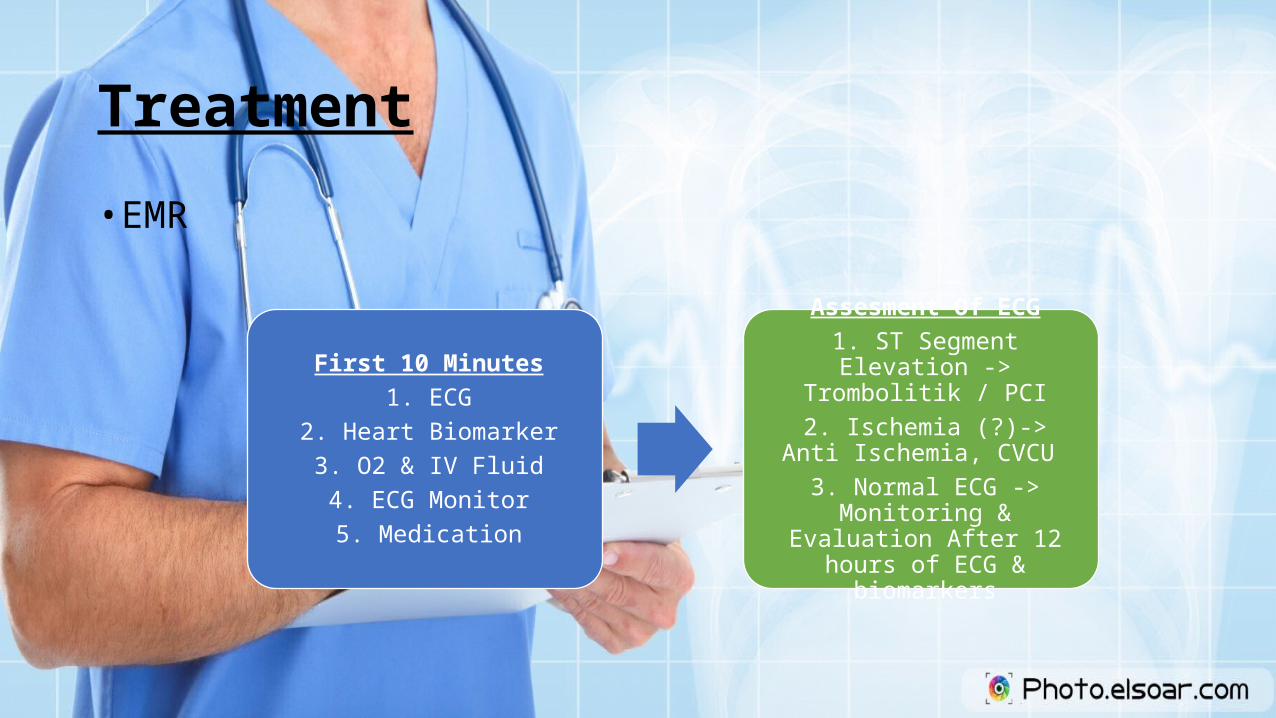
Treatment• EMR
First 10 Minutes1. ECG
2. Heart Biomarker3. O2 & IV Fluid4. ECG Monitor5. Medication
Assesment Of ECG1. ST Segment Elevation ->
Trombolitik / PCI2. Ischemia (?)-> Anti Ischemia,
CVCU 3. Normal ECG -> Monitoring &
Evaluation After 12 hours of ECG & biomarkers

Treatment

Treatment

Thank You….