
RECURRENCE MALIGNANT TRITON TUMOR OF THE MAXILLA: IS RADICAL
6
35 SAVAŞ SEREL, ATİLLA ERSOY, ZEYNEP ŞEN, ZEKİ CAN, MURAT EMİROĞLU, ERDEM YORMUK Savaş Serel* ✥ Atilla Ersoy* ✥ Zeynep Şen* ✥ Zeki Can** Murat Emiroğlu*** ✥ Erdem Yormuk*** 35 Y. Adı, Y. Adı RECURRENCE MALIGNANT TRITON TUMOR OF THE MAXILLA: IS RADICAL SURGERY REALLY NECESSARY? ––––––––––––––––––––––––– * Resident, Ankara University, Medical Faculty, Department of Plastic and Reconstrutive Surgery ** Associated Professor, Ankara Universitiy, Medical Faculty Department of Plastic and Reconstructive Surgery, *** Professor, Ankara Universitiy, Medical Faculty Department of Plastic and Reconstructive Surgery –––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––– Received: Oct. 27, 2003 Accepted: Feb 23, 2004 JOURNAL OF ANKARA MEDICAL SCHOOL V ol 26, No 1, 2004 35-40 SUMMARY Malignant triton tumor (MTT) is a soft tissue sarcoma consisting of a malignant schwannoma with rhabdomyoblastic differentiation (1). MTT is a very rare clinipathological entity, with about 90 cases so far reported. It develops at a relatively young age; (average of 35 years) (2). The biological behaviour of this tumor is more aggressive than the usual malignant schwannoma (3). It shows rapid growth, early metastasis and poor prognosis (4). We have reported a 30–year-old woman who presented to our department with a complaint of a progressively enlarging intraoral mass with malignant triton tumor of the maxilla in 1998. The woman was treated by total maxillectomy and radiotherapy (60 Gy in 6 weeks) after surgery. There was no sign of recurrence after 2 years of follow-up (5). The recurrence was seen in the same region after 37 months postsurgery. The patient succumbed to recurrent local and metastatic disease. In this article we discussed the radical surgery of the malignant triton tumor. Key Words: Malignant Triton Tumor, Recurrence, surgical Treatment. ÖZET Maksilla Malign Triton Tümörü’nün Nüksü: Radikal Cerrahi Gerçekten Gerekli mi? Malign triton tümörü (MTT) rabdomiyoblastik diferansiyasyon gösteren malign schwannomayı içeren bir yumuşak doku sarkomudur (1). MTT bugüne kadar yaklaşık 90 vakanın bildirildiği son derece nadir klinikopatolojik bir durumdur. Daha çok genç yaşlarda ortalama olarak 35 yaşında gelişir (2). Bu tümörün biyolojik davranışı malign schwannomanın genel davranışına göre çok daha agresiftir (3). Hızlı büyüme, erken metastaz ve kötü prognoz gösterir (4). Daha önce ağız içinde gittikçe büyüyen kitle şikayeti ile başvuran 30 yaşındaki maksillasında MTT’lü kadın hastayı 1998 yılında yayınlamıştık. Hasta total maksillektomiyi takiben haftada 60 Gy olacak şekilde radyoterapi ile tedavi edilmişti. İki yıllık takiplerde herhangi bir nüks bulgusuna rastlanmamıştı (5). Operasyondan 37 ay sonra aynı bölgede nükse rastlandı. Hasta lokal nükse ve metastatik hastalığa yenik düştü. Anahtar Kelimeler: Malign Triton Tümörü, Nüks, Cerrahi Tedavi. Malignant Triton tumor is malignant schwannoma with rhabdomyoblastic differentiation. In comparison with classic malignant schwannomas, it carries a more ominous prognosis and therefore should be regarded as a distinct clinical entity (2). Case Report A 30-year-old woman had presented to our department with a complaint of a progressively enlarging intraoral mass (Fig 1). Three years earlier the patient had undergone extraction of the upper third molar in the right maxilla and had experienced postoperative swelling in the same region. Parenteral antibiotic therapy had resulted in only a small reduction of the mass. Several biopsies had revealed “chronic inflammatory process”.
Transcript of RECURRENCE MALIGNANT TRITON TUMOR OF THE MAXILLA: IS RADICAL
35SAVAŞ SEREL, ATİLLA ERSOY, ZEYNEP ŞEN, ZEKİ CAN, MURAT EMİROĞLU, ERDEM YORMUK
SSaavvaaşş SSeerreell** ✥ AAttiillllaa EErrssooyy** ✥ ZZeeyynneepp ŞŞeenn** ✥ ZZeekkii CCaann****MMuurraatt EEmmiirrooğğlluu****** ✥ EErrddeemm YYoorrmmuukk******
35Y. Adı, Y. Adı
RREECCUURRRREENNCCEE MMAALLIIGGNNAANNTT TTRRIITTOONN TTUUMMOORR OOFF TTHHEEMMAAXXIILLLLAA:: IISS RRAADDIICCAALL SSUURRGGEERRYY RREEAALLLLYY NNEECCEESSSSAARRYY??
–––––––––––––––––––––––––* Resident, Ankara University, Medical Faculty, Department of Plastic and Reconstrutive Surgery** Associated Professor, Ankara Universitiy, Medical Faculty Department of Plastic and Reconstructive Surgery,*** Professor, Ankara Universitiy, Medical Faculty Department of Plastic and Reconstructive Surgery––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Received: Oct. 27, 2003 Accepted: Feb 23, 2004
JOURNAL OF ANKARA MEDICAL SCHOOL Vol 26, No 1, 2004 35-40
SSUUMMMMAARRYY
Malignant triton tumor (MTT) is a soft tissue sarcomaconsisting of a malignant schwannoma withrhabdomyoblastic differentiation (1). MTT is a very rareclinipathological entity, with about 90 cases so farreported. It develops at a relatively young age; (averageof 35 years) (2). The biological behaviour of this tumor ismore aggressive than the usual malignant schwannoma(3). It shows rapid growth, early metastasis and poorprognosis (4).
We have reported a 30–year-old woman who presentedto our department with a complaint of a progressivelyenlarging intraoral mass with malignant triton tumor ofthe maxilla in 1998. The woman was treated by totalmaxillectomy and radiotherapy (60 Gy in 6 weeks) aftersurgery. There was no sign of recurrence after 2 years offollow-up (5). The recurrence was seen in the sameregion after 37 months postsurgery. The patientsuccumbed to recurrent local and metastatic disease. Inthis article we discussed the radical surgery of themalignant triton tumor.
KKeeyy WWoorrddss:: Malignant Triton Tumor, Recurrence,surgical Treatment.
ÖÖZZEETT
MMaakkssiillllaa MMaalliiggnn TTrriittoonn TTüümmöörrüü’’nnüünn NNüükkssüü:: RRaaddiikkaallCCeerrrraahhii GGeerrççeekktteenn GGeerreekkllii mmii??
Malign triton tümörü (MTT) rabdomiyoblastikdiferansiyasyon gösteren malign schwannomayı içerenbir yumuşak doku sarkomudur (1). MTT bugüne kadaryaklaşık 90 vakanın bildirildiği son derece nadirklinikopatolojik bir durumdur. Daha çok genç yaşlardaortalama olarak 35 yaşında gelişir (2). Bu tümörünbiyolojik davranışı malign schwannomanın geneldavranışına göre çok daha agresiftir (3). Hızlı büyüme,erken metastaz ve kötü prognoz gösterir (4).
Daha önce ağız içinde gittikçe büyüyen kitle şikayeti ilebaşvuran 30 yaşındaki maksillasında MTT’lü kadınhastayı 1998 yılında yayınlamıştık. Hasta totalmaksillektomiyi takiben haftada 60 Gy olacak şekilderadyoterapi ile tedavi edilmişti. İki yıllık takiplerdeherhangi bir nüks bulgusuna rastlanmamıştı (5).Operasyondan 37 ay sonra aynı bölgede nükse rastlandı.Hasta lokal nükse ve metastatik hastalığa yenik düştü.
AAnnaahhttaarr KKeelliimmeelleerr:: Malign Triton Tümörü, Nüks, CerrahiTedavi.
Malignant Triton tumor is malignantschwannoma with rhabdomyoblasticdifferentiation. In comparison with classicmalignant schwannomas, it carries a moreominous prognosis and therefore should beregarded as a distinct clinical entity (2).
CCaassee RReeppoorrtt
A 30-year-old woman had presented to our
department with a complaint of a progressivelyenlarging intraoral mass (Fig 1). Three yearsearlier the patient had undergone extraction ofthe upper third molar in the right maxilla and hadexperienced postoperative swelling in the sameregion. Parenteral antibiotic therapy had resultedin only a small reduction of the mass. Severalbiopsies had revealed “chronic inflammatoryprocess”.
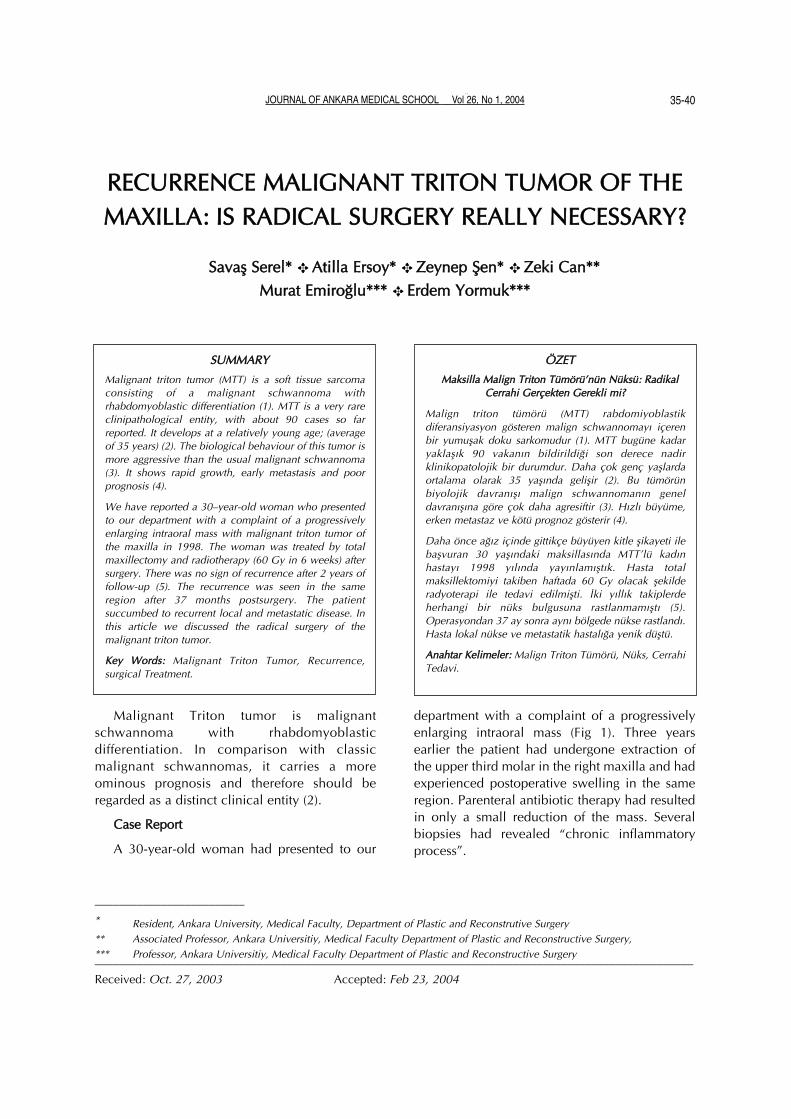
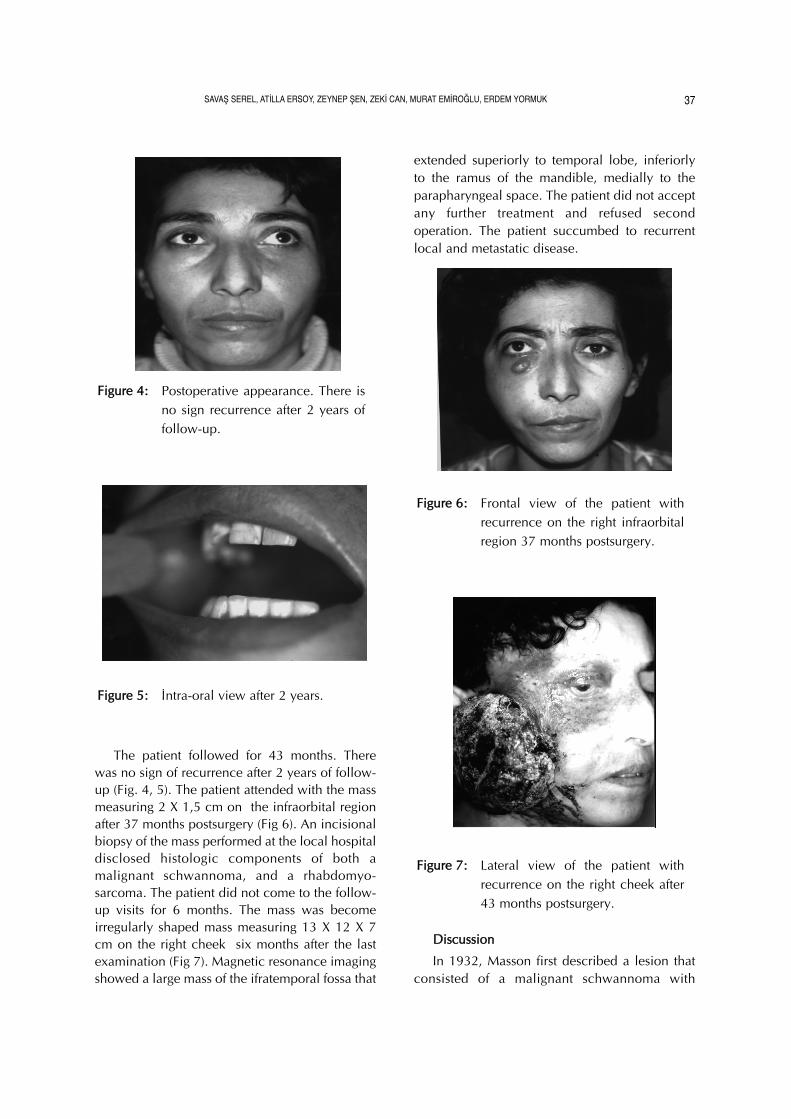
On admission, physical examination hadconfirmed an ulcerated and irregularly shapedmass measuring 8 X 8 X 5 cm on the rightgingivobuccal sulcus (Fig 2). There had been nolimitation of jaw movement and regionallymphadenopathy. The patient had showed noclinical evidence of Von Recklinghausen’sdisease. Computed tomography (CT) hadrevealed a soft-tissue mass lying between thelateral pterygoid, atlas, ramus mandible, andlateral wall of the nasopharynx. The mass hadalso eroded the anterior, posterior and lateralwalls of the maxillary sinus. Chest radiography,carotid angiography, cranial tomography, andbone scintigraphy had been normal. Incisionalbiopsy had showed a spindle cell sarcoma.Following biopsy and diagnosis of maxillarysarcoma, treatment had been planned. Totalmaxillectomy had been performed with Weber –Ferguson – Longmire incision (Fig 3). Tumor –free margins had been obtained at the time ofsurgical resection macroscopically. Immediatereconstruction had not been planned because ofthe high malignant potential of the tumor. Theentire cavity had been allowed to heal withsecondary intention. Three weeks after surgery afinal prosthesis with teeth had been fabricated bythe prosthodontist (5).
The histopathological diagnosis had beenmalignant schwannoma with rhabdomyosar-comatous components-namely, MTT. We hadperformed an immunohistochemical evaluation
to verify the diagnosis of MTT. The tumor hadbeen found to be positive for S-100, desmin, andmyoglobin. Three weeks after surgery,radiotherapy (60 Gy in 6 wees) had beencommenced for the right maxilla and cheek. Thepostoperative period had been uneventful (5).
FFiigguurree 33:: Intra-operative view
FFiigguurree 22:: Clinical photograph of the intraoralpresentation of the tumor.
FFiigguurree 11:: Frontal view of the patient withmalignant Triton tumor.
36 RECURRENCE MALIGNANT TRİTON TUMOR OF THE MAXILLA: IS RADICAL SURGERY REALLY NECESSARY?
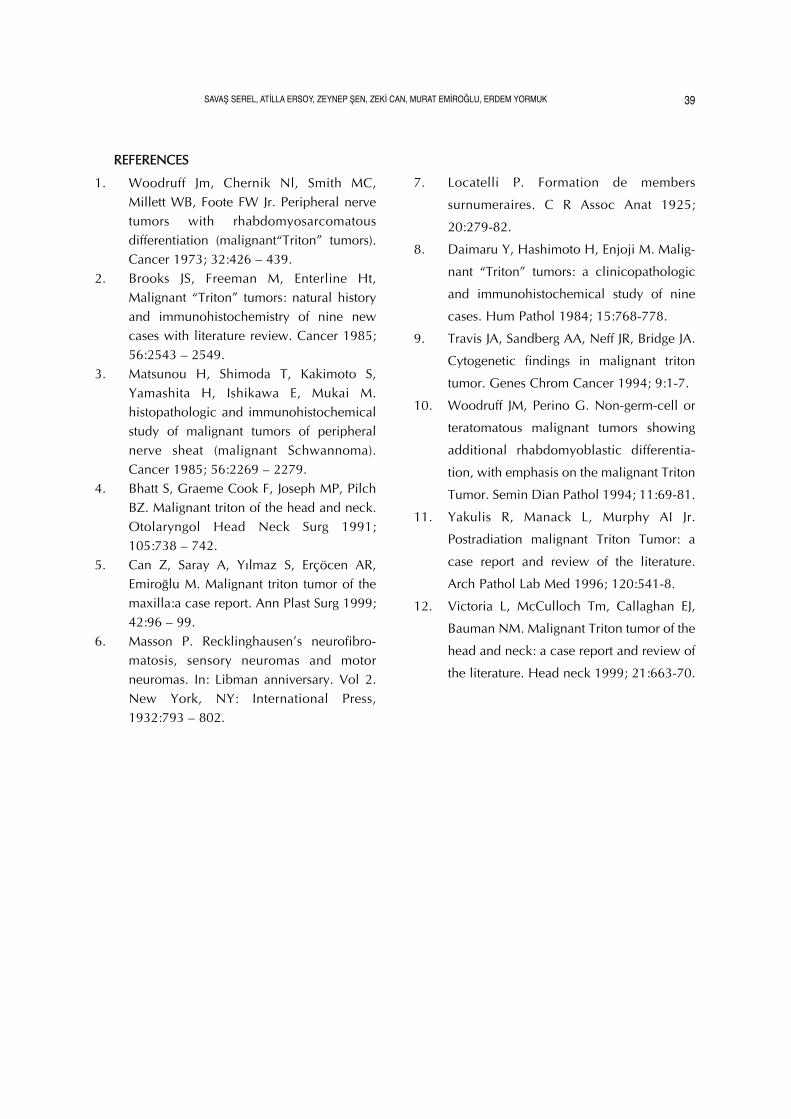
The patient followed for 43 months. Therewas no sign of recurrence after 2 years of follow-up (Fig. 4, 5). The patient attended with the massmeasuring 2 X 1,5 cm on the infraorbital regionafter 37 months postsurgery (Fig 6). An incisionalbiopsy of the mass performed at the local hospitaldisclosed histologic components of both amalignant schwannoma, and a rhabdomyo-sarcoma. The patient did not come to the follow-up visits for 6 months. The mass was becomeirregularly shaped mass measuring 13 X 12 X 7cm on the right cheek six months after the lastexamination (Fig 7). Magnetic resonance imagingshowed a large mass of the ifratemporal fossa that
extended superiorly to temporal lobe, inferiorlyto the ramus of the mandible, medially to theparapharyngeal space. The patient did not acceptany further treatment and refused secondoperation. The patient succumbed to recurrentlocal and metastatic disease.
DDiissccuussssiioonn
In 1932, Masson first described a lesion thatconsisted of a malignant schwannoma with
FFiigguurree 77:: Lateral view of the patient withrecurrence on the right cheek after43 months postsurgery.
FFiigguurree 66:: Frontal view of the patient withrecurrence on the right infraorbitalregion 37 months postsurgery.
FFiigguurree 55:: İntra-oral view after 2 years.
FFiigguurree 44:: Postoperative appearance. There isno sign recurrence after 2 years offollow-up.
37SAVAŞ SEREL, ATİLLA ERSOY, ZEYNEP ŞEN, ZEKİ CAN, MURAT EMİROĞLU, ERDEM YORMUK

rhabdomyoblastic differentiation (6). Subsequ-ently, Woodruff et al coined the term “MalignantTriton Tumor” (MTT) to indicate such a neoplasm(1). The name refers to Locatelli’s experiment inwhich a sciatic nerve implanted onto the back ofa supernumerary limb made up of neural andmuscular tissue (7). The previously reported casesof MTT occurred predominantly in the head,neck, and trunk regions (2). Daimaru et al’s reportof nine cases of MTT showed a predilection forthe thigh and buttock (8). There are two types oftumors in the category of MTT. Those with vonReckling-hausens neurofibromatosis constituteover 70% in a review of 36 cases and displayeda marked male predominance, young age, andcommon presentation in the head and neck. Bycontrast, those without von Recklinghausensneurofibromatosis are of an older age, femalepredominance and frequently located on thetrunk (2).
Twenty percent of cases of triton tumor arisein the head and neck, 32% in the trunk, and 24%in the extremities (4, 9). The prognosis of MTThas been analyzed by several authors, who foundthat the tumor is more aggressive than malignantperipheral nerve sheath tumors, with 5-yearcrude and specific survival rates of 11% and26%, respectively (14, 11). Yakulis et al alsolooked at the impact on the survival rate of
different variables such as location of the tumor,age, sex, and association with NF-1 by means ofa Cox regression analysis (11). The prognosisbetter for head and neck, upper extremity, andlower extremity sites and worse for buttock,trunk, and retro peritoneum.
The natural history of MTT is much moreaggressive than sporadic malignant schwannoma(3, 4). It is always difficult to speculate ontreatment guidelines when dealing with a raredisease. However, as with any other sarcoma,resection of the tumor with a wide marginfollowed by radiotherapy is generally recom-mended, and the role of chemotherapy has notyet been clearly defined (12). It is recommendedthat the therapeutic plan in MTT of the head andneck must be highly individualized, taking intoaccount patient’s age, health, location of theprimary site, and the presence of neurofibro-matosis (4).
Unfortunately, despite proper treatmentprotocols, the local recurrence and distantmetastasis rates approximate 25 and 48 per cent,respectively. Survival of patients with head andneck MTT ranges between four months and 22years (2). Therefore we conclude that radicalsurgery for the malignant triton tumor may notnecessary.
38 RECURRENCE MALIGNANT TRİTON TUMOR OF THE MAXILLA: IS RADICAL SURGERY REALLY NECESSARY?
RREEFFEERREENNCCEESS
1. Woodruff Jm, Chernik Nl, Smith MC,Millett WB, Foote FW Jr. Peripheral nervetumors with rhabdomyosarcomatousdifferentiation (malignant“Triton” tumors).Cancer 1973; 32:426 – 439.
2. Brooks JS, Freeman M, Enterline Ht,Malignant “Triton” tumors: natural historyand immunohistochemistry of nine newcases with literature review. Cancer 1985;56:2543 – 2549.
3. Matsunou H, Shimoda T, Kakimoto S,Yamashita H, Ishikawa E, Mukai M.histopathologic and immunohistochemicalstudy of malignant tumors of peripheralnerve sheat (malignant Schwannoma).Cancer 1985; 56:2269 – 2279.
4. Bhatt S, Graeme Cook F, Joseph MP, PilchBZ. Malignant triton of the head and neck.Otolaryngol Head Neck Surg 1991;105:738 – 742.
5. Can Z, Saray A, Yılmaz S, Erçöcen AR,Emiroğlu M. Malignant triton tumor of themaxilla:a case report. Ann Plast Surg 1999;42:96 – 99.
6. Masson P. Recklinghausen’s neurofibro-matosis, sensory neuromas and motorneuromas. In: Libman anniversary. Vol 2.New York, NY: International Press,1932:793 – 802.
7. Locatelli P. Formation de members
surnumeraires. C R Assoc Anat 1925;
20:279-82.
8. Daimaru Y, Hashimoto H, Enjoji M. Malig-
nant “Triton” tumors: a clinicopathologic
and immunohistochemical study of nine
cases. Hum Pathol 1984; 15:768-778.
9. Travis JA, Sandberg AA, Neff JR, Bridge JA.
Cytogenetic findings in malignant triton
tumor. Genes Chrom Cancer 1994; 9:1-7.
10. Woodruff JM, Perino G. Non-germ-cell or
teratomatous malignant tumors showing
additional rhabdomyoblastic differentia-
tion, with emphasis on the malignant Triton
Tumor. Semin Dian Pathol 1994; 11:69-81.
11. Yakulis R, Manack L, Murphy AI Jr.
Postradiation malignant Triton Tumor: a
case report and review of the literature.
Arch Pathol Lab Med 1996; 120:541-8.
12. Victoria L, McCulloch Tm, Callaghan EJ,
Bauman NM. Malignant Triton tumor of the
head and neck: a case report and review of
the literature. Head neck 1999; 21:663-70.
39SAVAŞ SEREL, ATİLLA ERSOY, ZEYNEP ŞEN, ZEKİ CAN, MURAT EMİROĞLU, ERDEM YORMUK

40 RECURRENCE MALIGNANT TRİTON TUMOR OF THE MAXILLA: IS RADICAL SURGERY REALLY NECESSARY?


















