
REUNIÓN DE LAS ASOCIACIONES TERRITORIALES DE LA … · DIAGNOSTIC INMUNOHISTOCHEMISTRY . DAVID...
38
CIV REUNIÓN DE LAS ASOCIACIONES TERRITORIALES DEL NOROESTE DE LA PENÍSULA IBÉRICA Isabel Viqueira Rodríguez Complejo Asistencial de Burgos 30 noviembre 2012
-
Upload
dinhnguyet -
Category
Documents
-
view
214 -
download
0
Transcript of REUNIÓN DE LAS ASOCIACIONES TERRITORIALES DE LA … · DIAGNOSTIC INMUNOHISTOCHEMISTRY . DAVID...

CIV REUNIÓN DE LAS ASOCIACIONES TERRITORIALES DEL NOROESTE DE LA PENÍSULA
IBÉRICA
Isabel Viqueira Rodríguez Complejo Asistencial de Burgos
30 noviembre 2012
CASO CLÍNICO: Varón de 43 años de edad.
AP: gastritis crónica atrófica antral. erradicación de H.P Actualmente: Niveles de ferritina elevados
desde 2007 con sangrías cada 3 meses. RMN: sobrecarga férrica hepática. Lesión
subdiafragmática en lob. Izq. de 15 mm isointensa en T1 con importante captación arterial.
TC: captación nodular en el segmento IV del lóbulo Izquierdo de15mm. isointensa en fase venoso-portal y parenquimatosa.
DESCRIPCIÓN MACROSCÓPICA: DATO CLÍNICO:
Hepatocarcinoma en segmento IV sin biopsia previa.
MACROSCÓPICO:
Tejido de morfología ovalada de 5,7x4,5x2cm Superficie lisa pardo-violacea. Lesión subcapsular nodular amarillenta de 1,6x1,4x1,2 cm En vecindad a una estructura vascular de gran calibre.
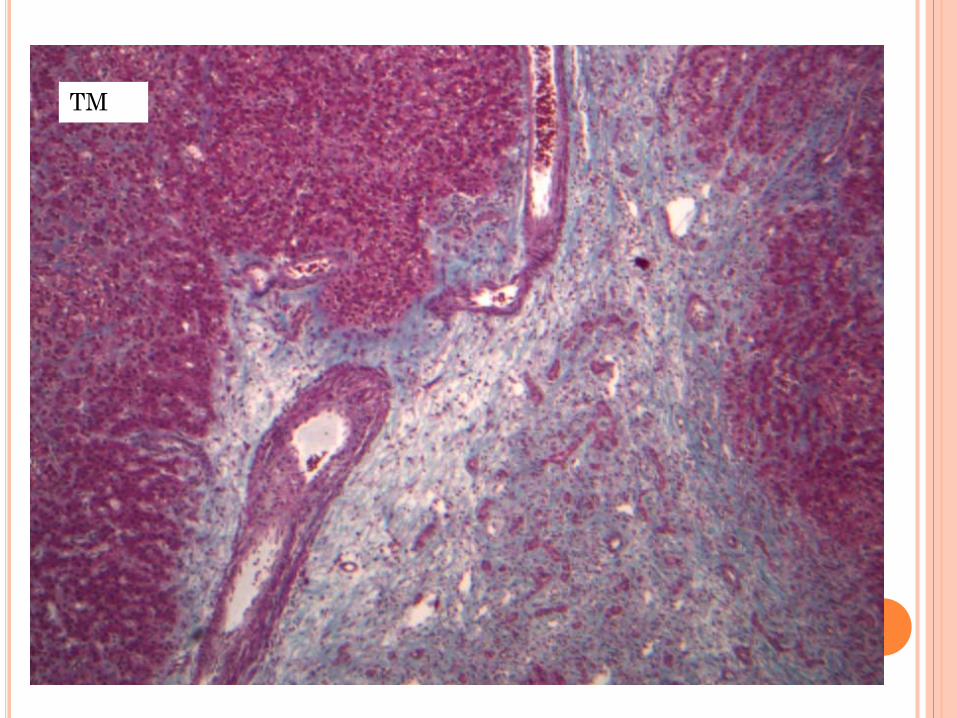
TM
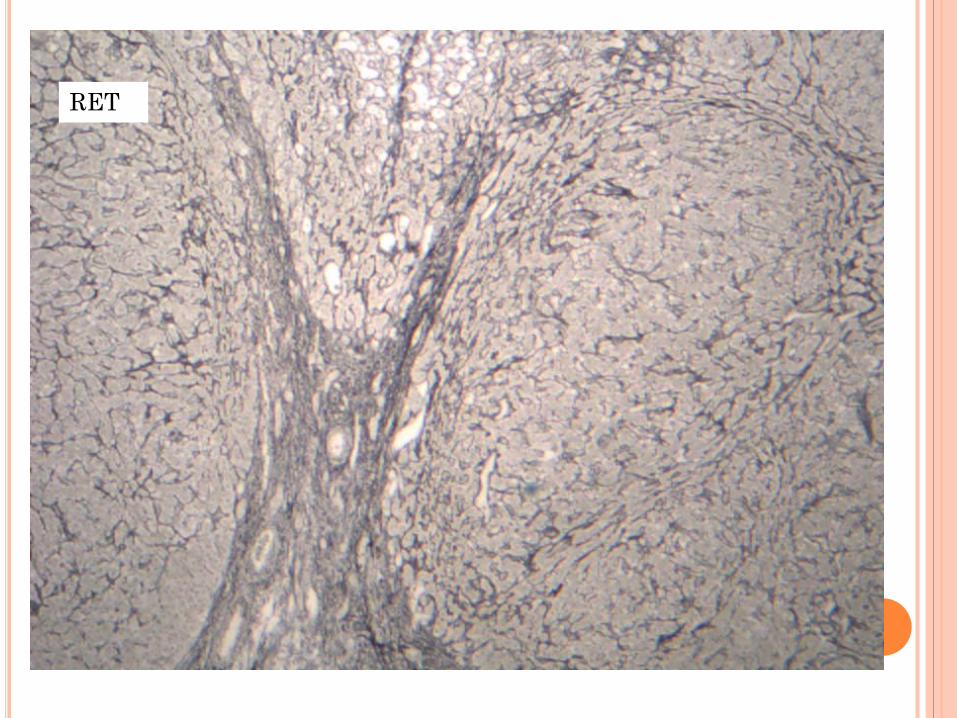
RET
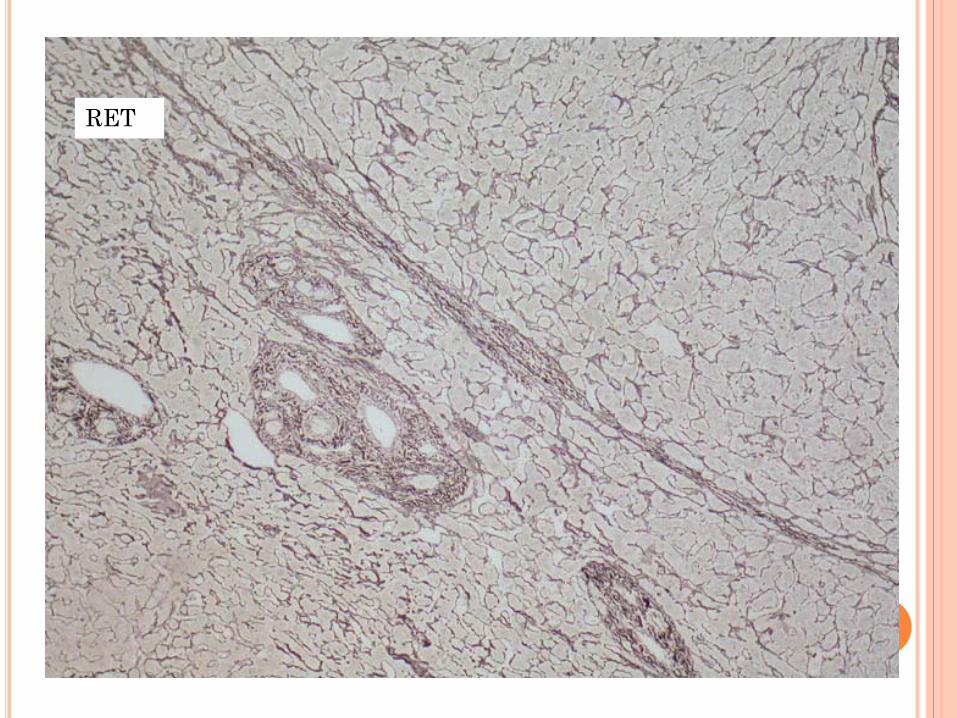
RET RET
CD10
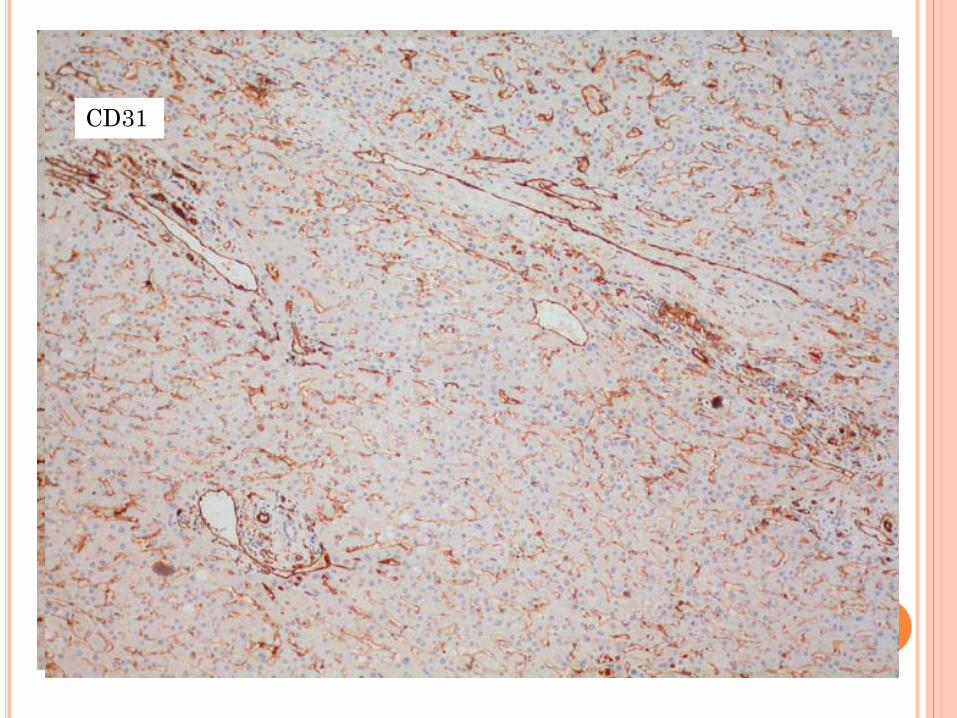
CD10 CD31

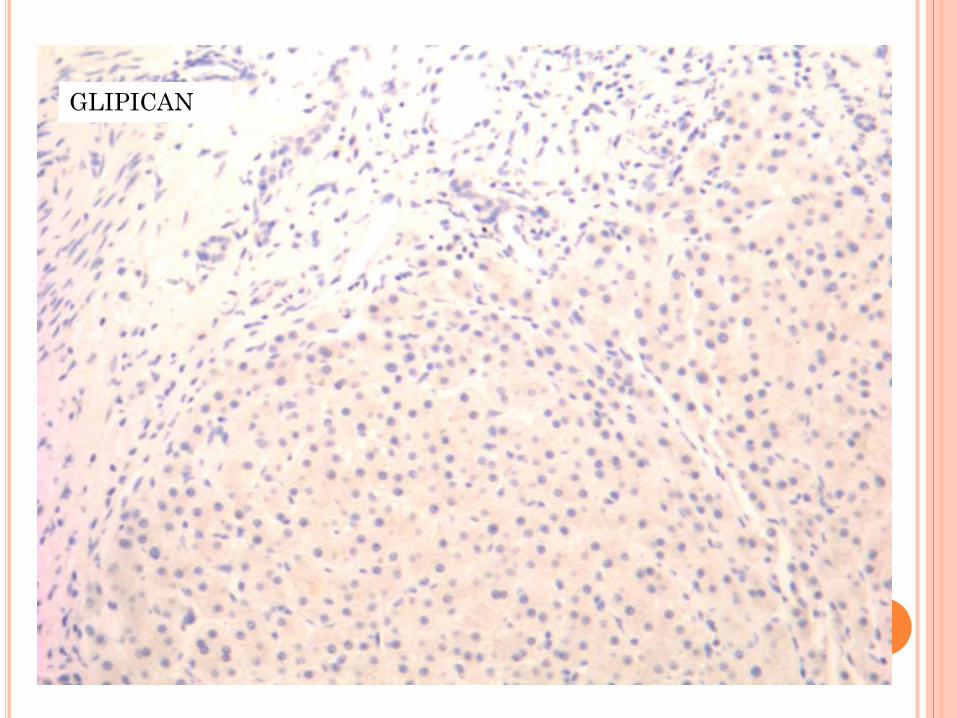
GLIPICAN
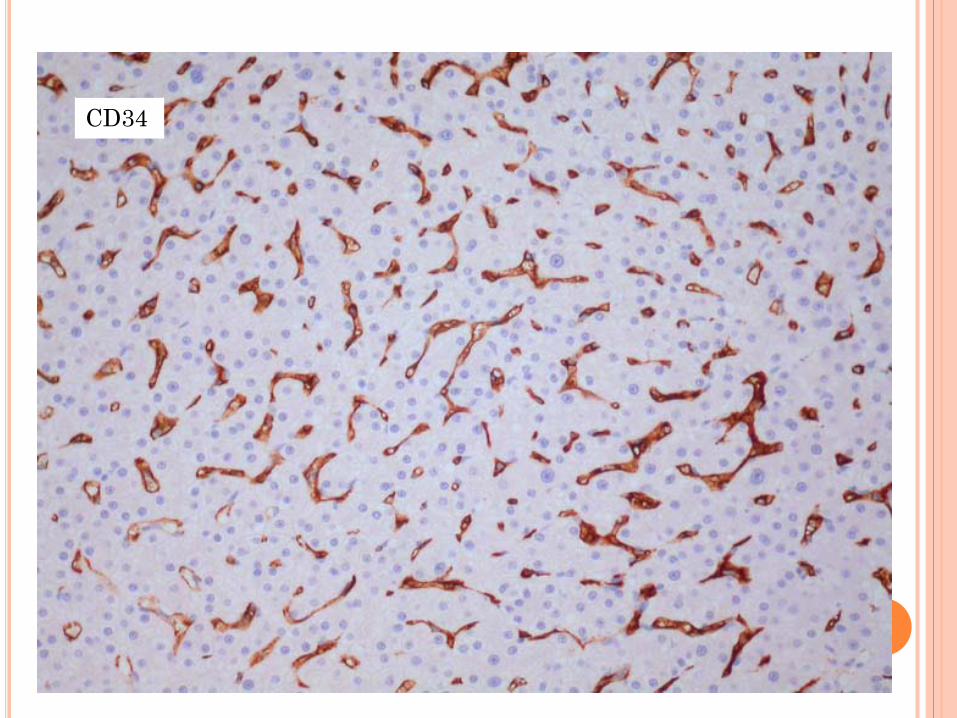
CD34


DIAGNÓSTICO:
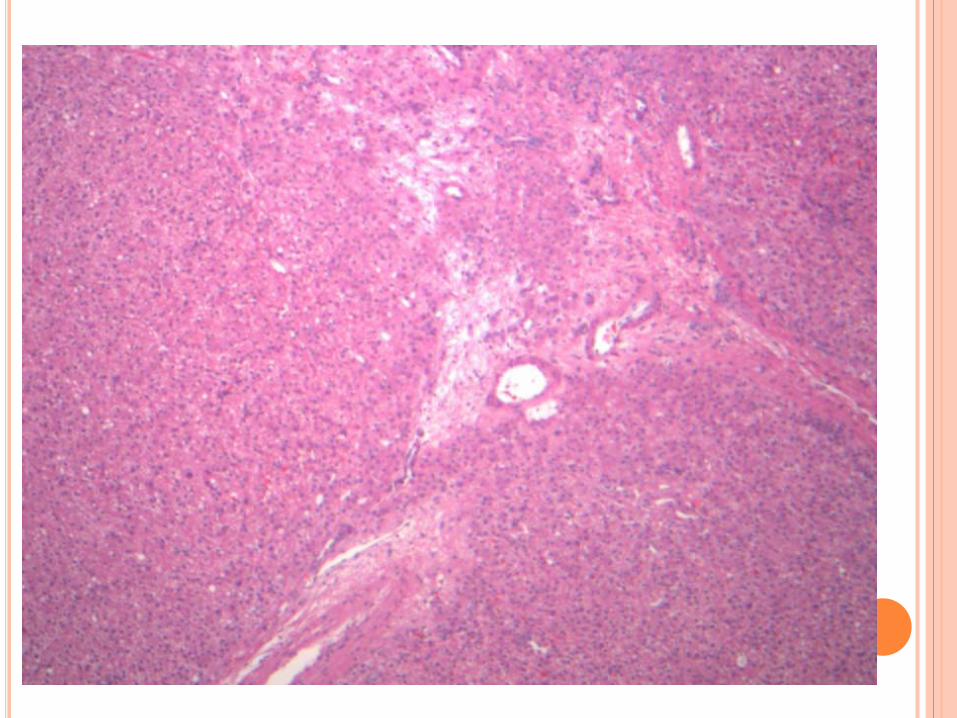
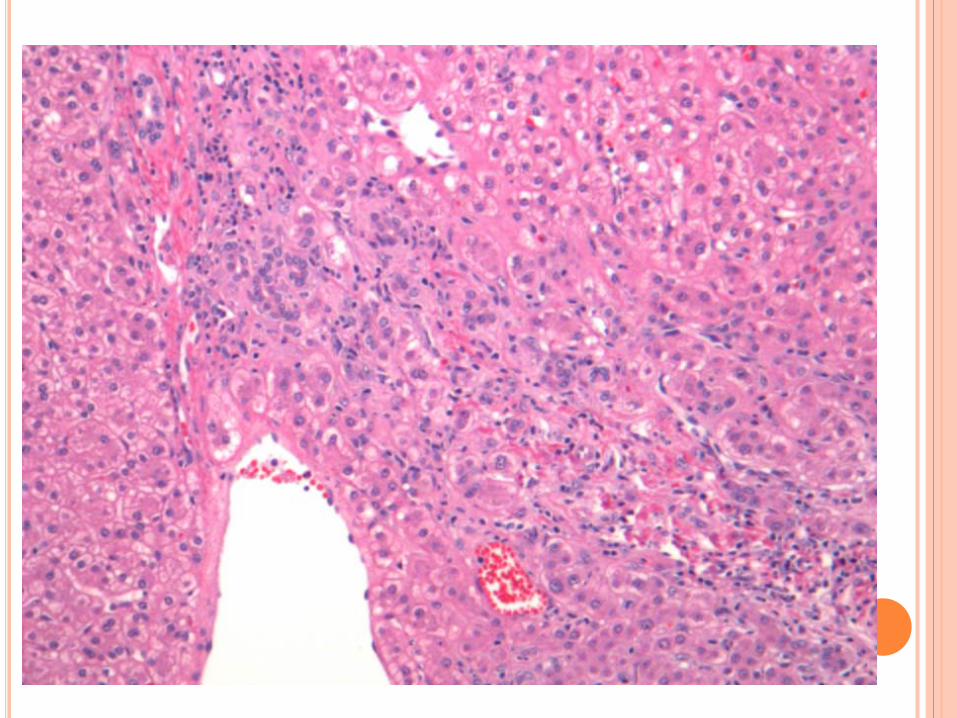
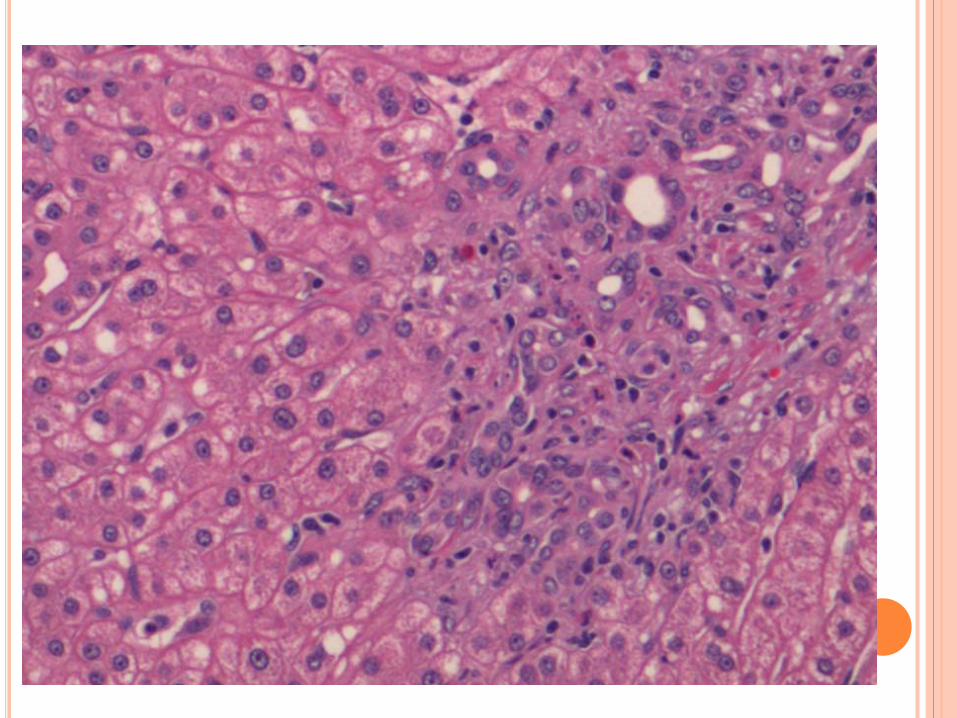
HIPERPLASIA NODULAR FOCAL.
POR QUÉ HEMOS ELEGIDO ESTE CASO????
HIPERPLASIA NODULAR FOCAL Cualquier edad (más 30-40 aa). Más en mujeres (2:1). No relacionado con la toma de ACO. Hallazgo incidental durante un test Rx.
Clínica: asintomática puede: dolor raro: hemorragia. Función hepática: normal. puede: glutariltranspep.
Lesión solitaria: 20-30 % multifocal. Multifocales: asociados a:
Hemangiomas, defectos estructurales arteriales, aneurisma cerebral, meningioma, astrocitoma….
Hipótesis: Crecimiento alterado de los vasos que rodean una
lesión arterial preexistente. Expresión de genes angiopoyéticos aberrante.
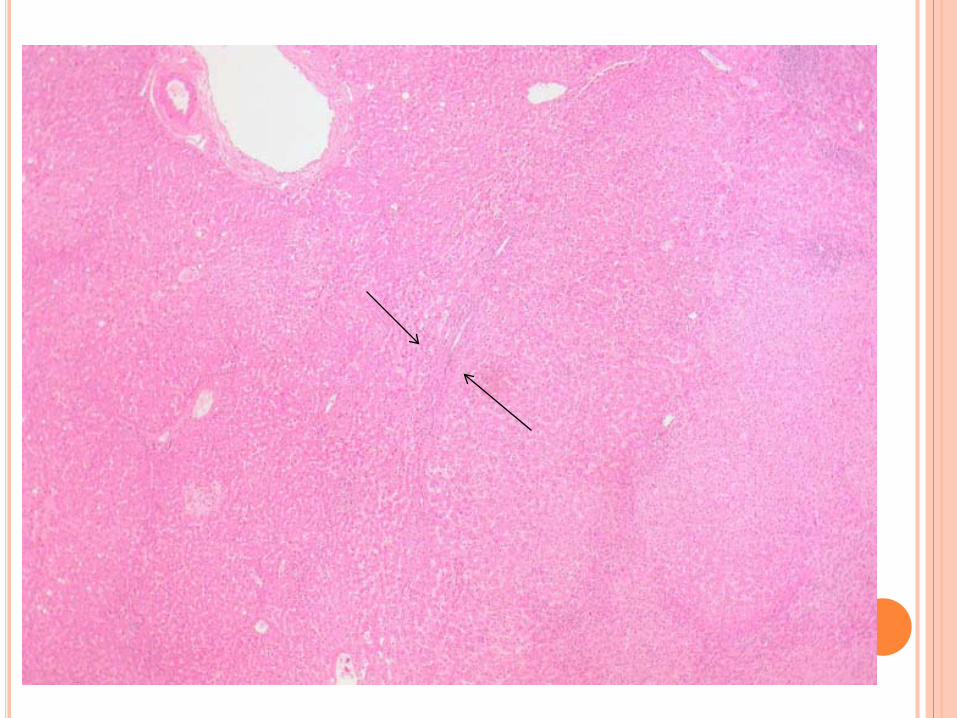
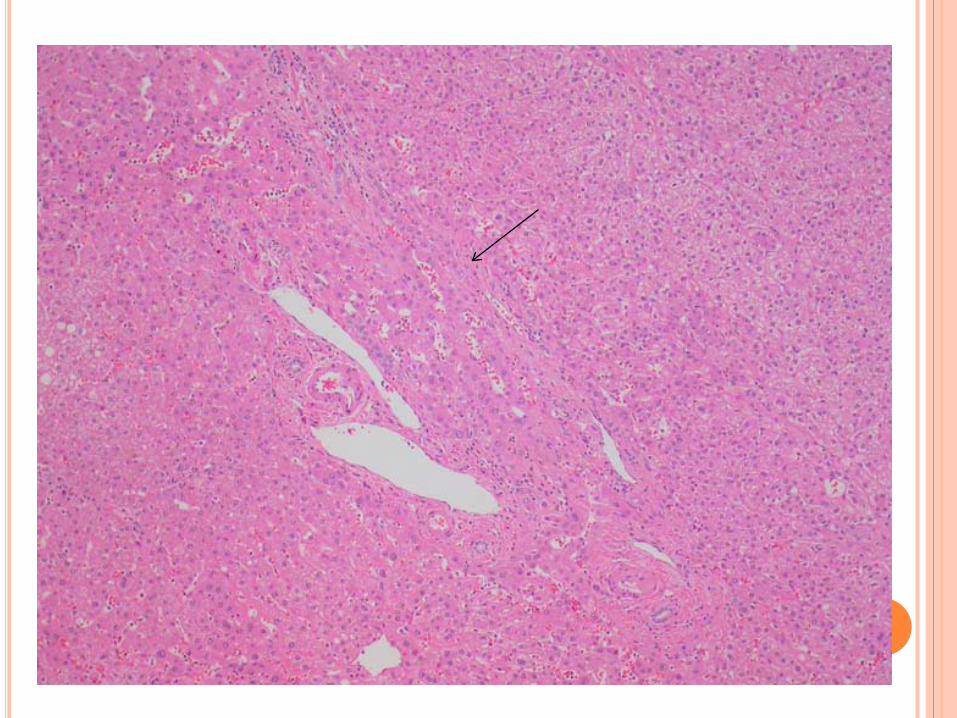
Macroscopía: Lesión nodular. Subcapsular (formas pediculadas). Bien demarcados, no capsulados. < 5cm. Cicatriz central fibrovascular (no si <1cm)
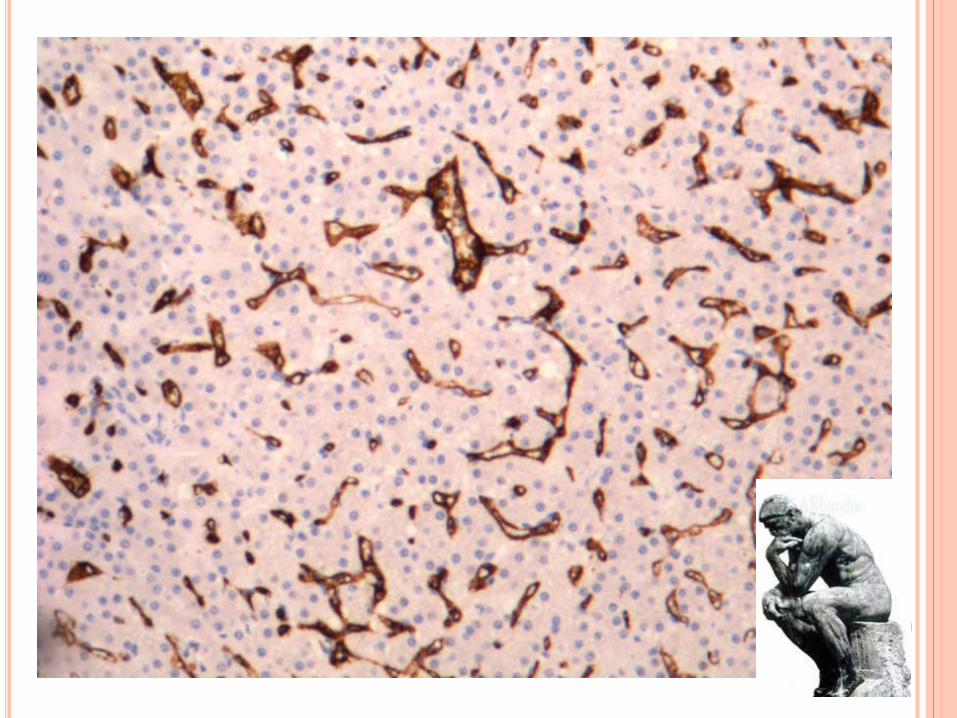
Imagen: homogénea con cicatriz central. DX: H-E RET ARQUITECTURA IHQ: AFP CD34 LITERATURA: clásicamente el CD34 ha sido
considerado como un marcador útil en el diagnóstico den HCC. Pero se esta observando que también aparece frecuentemente en la HNF y adenoma hepático .
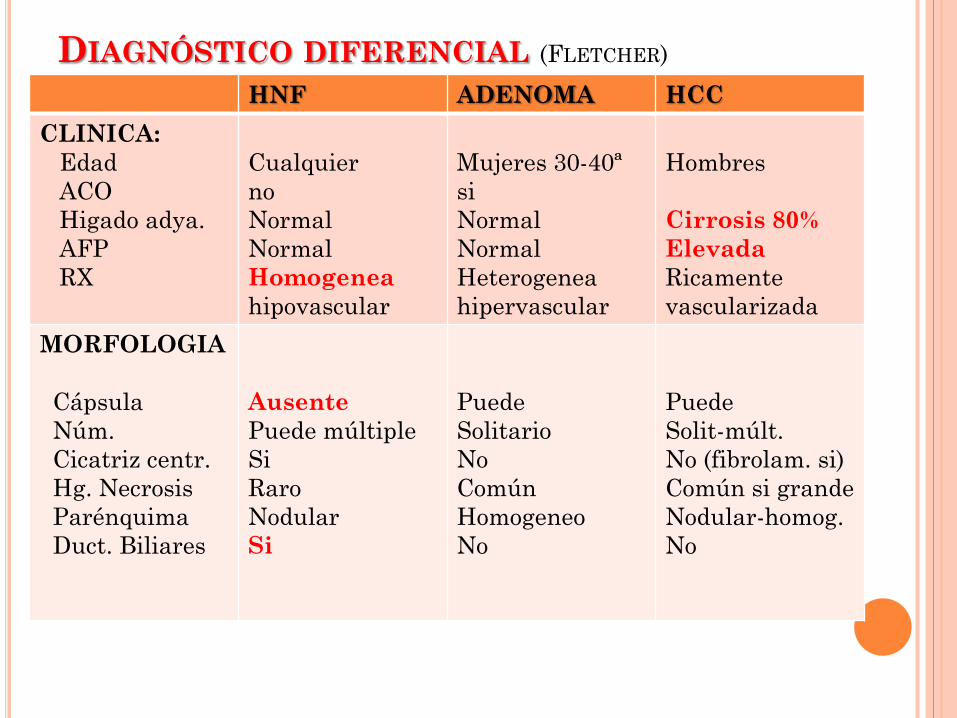
DIAGNÓSTICO DIFERENCIAL (FLETCHER) HNF ADENOMA HCC
CLINICA: Edad ACO Higado adya. AFP RX
Cualquier no Normal Normal Homogenea hipovascular
Mujeres 30-40ª si Normal Normal Heterogenea hipervascular
Hombres Cirrosis 80% Elevada Ricamente vascularizada
MORFOLOGIA Cápsula Núm. Cicatriz centr. Hg. Necrosis Parénquima Duct. Biliares
Ausente Puede múltiple Si Raro Nodular Si
Puede Solitario No Común Homogeneo No
Puede Solit-múlt. No (fibrolam. si) Común si grande Nodular-homog. No
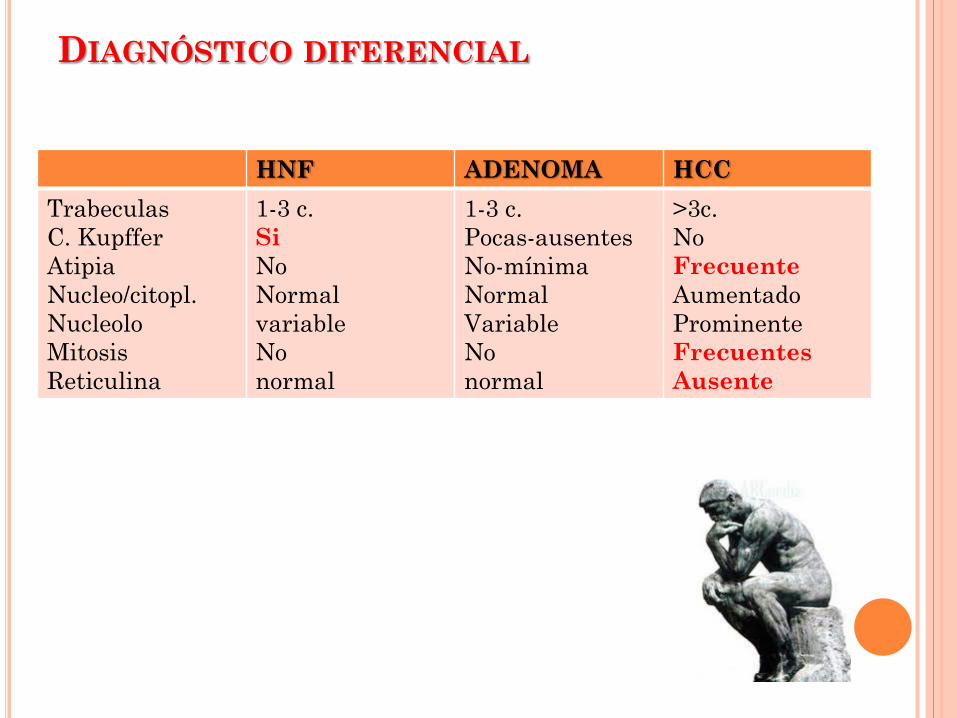
DIAGNÓSTICO DIFERENCIAL
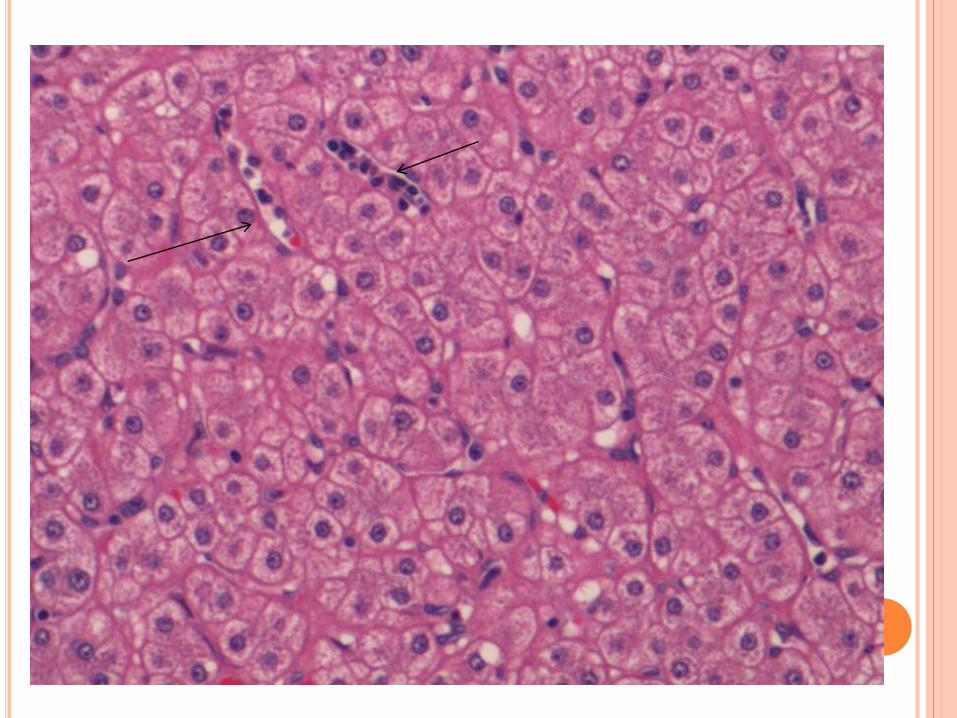
HNF ADENOMA HCC Trabeculas C. Kupffer Atipia Nucleo/citopl. Nucleolo Mitosis Reticulina
1-3 c. Si No Normal variable No normal
1-3 c. Pocas-ausentes No-mínima Normal Variable No normal
>3c. No Frecuente Aumentado Prominente Frecuentes Ausente
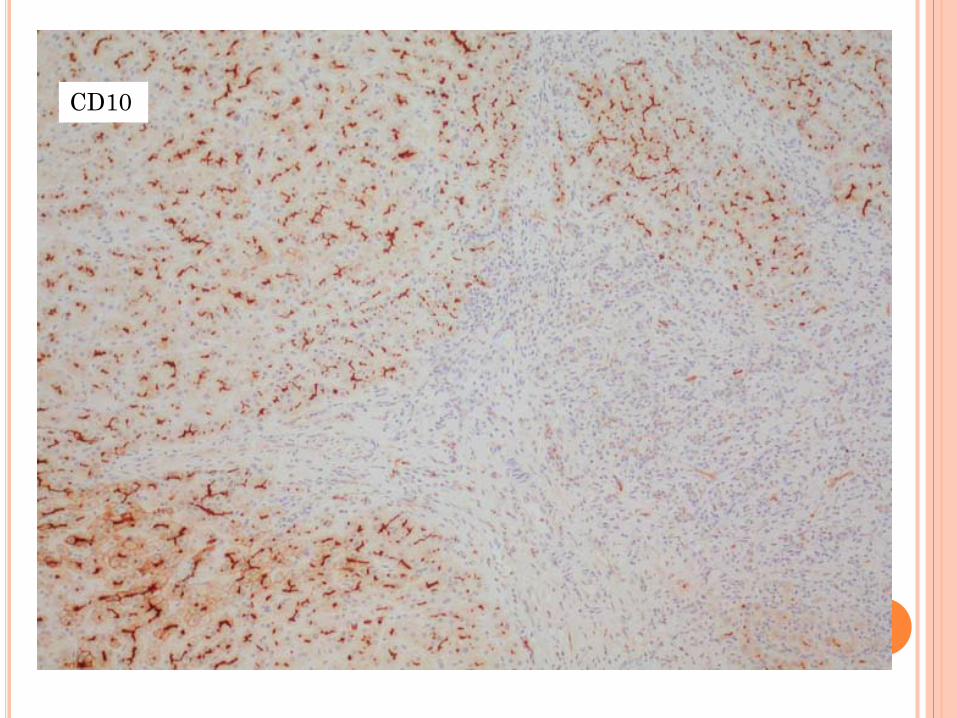
DIAGNOSTIC INMUNOHISTOCHEMISTRY DAVID DABBS CD34-CD31:
Althougt hepatocytes (benign or malignant) do not stain with these antibodies, they can be used as ancillary antibodies in the identification of HCC and assist in the distinction of HCC from hepatocellular adenoma, focal nodular hiperplasia, and rgenerative cirrhotic nodule. HCC cords, trabecula and acini are invested with an encircling endothelial cell layer that is CD34 or CD31 positive, even in the absence of well defined sinusoids. The sinusoidal endothelial lining around benign hepatic lesions do not stain with these antibodies.
CD34 en nuestro caso
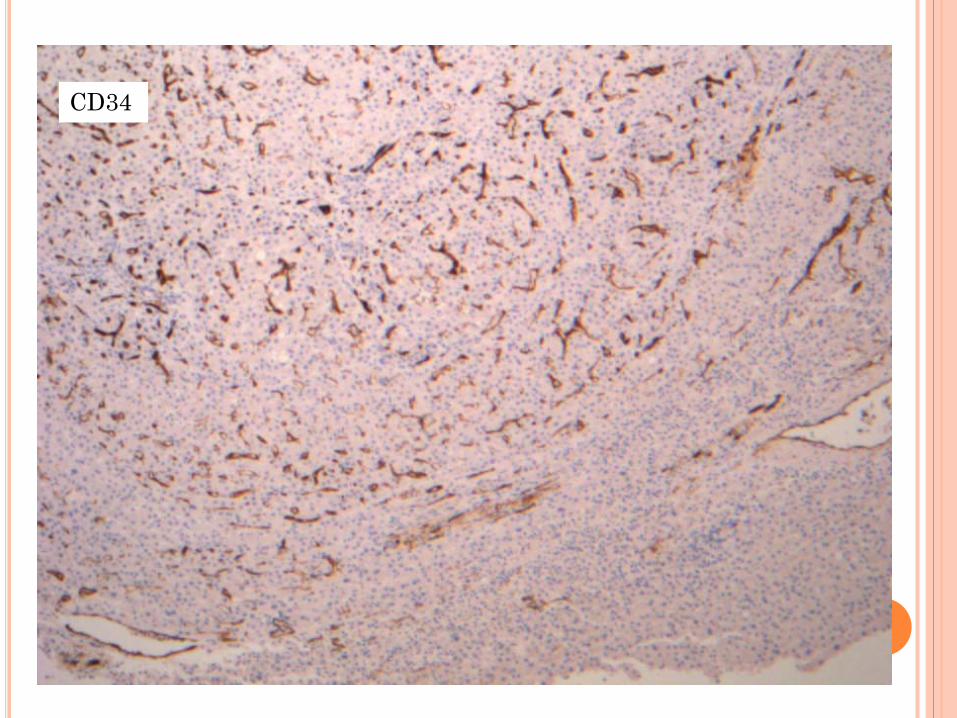
CD34

CD 34 UTIL PARA DIAGNÓSTICO DIFERENCIAL DE HCC-HNF???
Cuidado en la interpretación de CD34 positivo en las biopsias de pequeño tamaño donde no se puede valorar la arquitectura de la lesión.

CASO 2: AÑO 2012. Mujer de 36 años. LOE hepática de 11 cm en el lóbulo izquierdo. IMAGEN: nódulo isoecogénico ,e hipogénico a
nivel central. MACRO: cilindro pardo amarillento de 17x1mm.

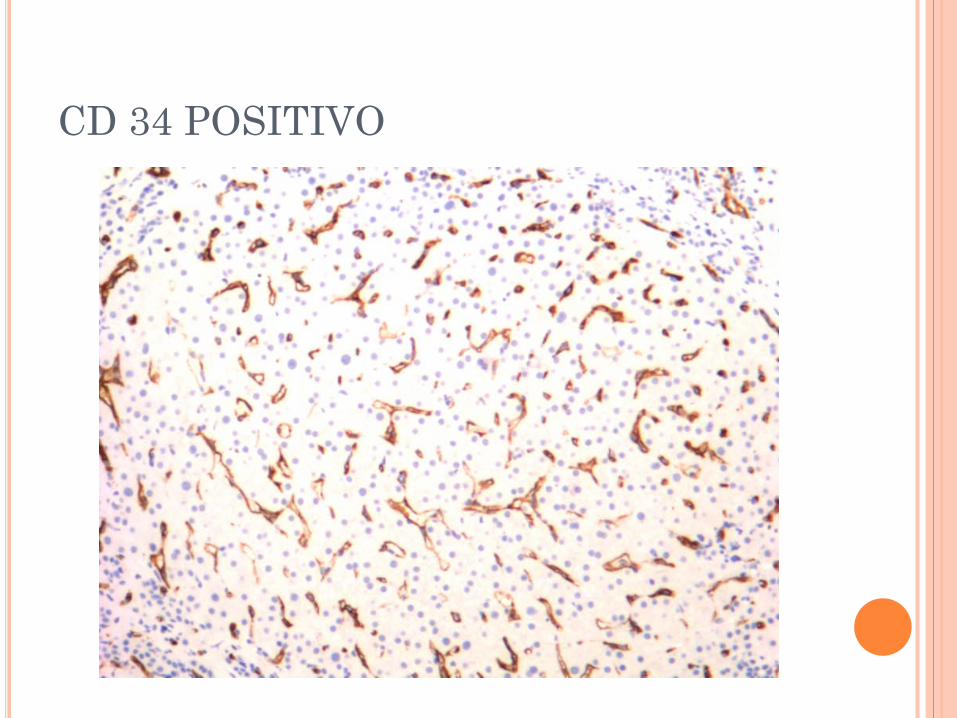
CD 34 POSITIVO

BIBLIOGRAFÍA: Peter Tatrai and Cols. Agrin and CD34 inmunohistichemistry for
the discrimination of benign versus malignant hepatocellular lesions. Surg pathology 2009; vol33.
Francisco Colina and Cols. Protocolo y guía para el diagnóstico histopatológico de hepatocarcinoma. Revista Española de patología 2007;vol 40.
Sthephen A. and Cols. Application of inmunohistochemistry to liver and gastrointestinal neoplasms. Arch. Pathol. Lab. Med. 2008 vol: 132.
linda Ferrell. Liver pathology: Cirrhosis, hepatitis, and primari Liver tumours, Update and diagnostic problems. United States and Canadian Academy of pathology. 2000.Vol: 13.
David Dabbs, diagnosti inmunohistochemistry Fletcher. Diagnostic histopathology of tumors. Rosai and Ackerman´s. Surgical Pathology. Tend edition



















