TYUITe

of 7
-
Upload
yuritrujillo33 -
Category
Documents
-
view
224 -
download
0
Transcript of TYUITe
-
7/30/2019 TYUITe
1/7
Clinical correlates, natural history and outcomeof neonatal apnoea
Terry M. Baird)
Case Western Reserve University, 11100 Euclid Ave., Cleveland, OH 44106, USA
Summary Apnoea is common in the newborn period and especially in pretermnewborns. Bradycardia and desaturation of oxyhaemoglobin typically occur with ap-noea. These abnormalities reflect an immature cardiorespiratory system and resolu-tion of this immaturity can be expected within a predictable time frame. Infantswho have apnoea in the newborn period are thought not to be at higher risk for sud-den infant death syndrome (SIDS). Whether apnoea episodes are associated witha higher incidence of long-term handicap for these infants is not yet clear. 2003 Elsevier Ltd. All rights reserved.
KEYWORDSApnoea;Bradycardia;Sudden infant death
syndrome (SIDS)
Episodes of apnoea resulting from immaturity of re-spiratory control decrease with advancing age andeventually the breathing abnormalities exhibitedby premature infants become indistinguishablefrom their counterparts born at full term.1,2 Thereare two areas of concern regarding neonatal ap-noea: first, whether these episodes are precursorsto, or predictors of, any other cardiorespiratoryproblems and second whether apnoea episodesand the resultant hypoxia compromise a newbornslong-term outcome. Immature cardiorespiratorycontrol has been traditionally described in terms
of the effect on heart rate and breathing pattern.Recently interest had been directed towardoxyhaemoglobin saturation as detected by pulseoximetry. Abnormalities in breathing are thereforeseen as apnoea, bradycardia and desaturations and
the development of cardiorespiratory control canbe described and followed clinically in all three.
Clinical aspects of apnoea,bradycardia and their resolution
Pauses in breathing are a relatively common phe-nomenon in newborns and these pauses are in-creasingly frequent and longer in duration withdecreasing gestational age.3,4 These episodes arepresent beginning on the first day of life for somepremature infants and often include bradycardiaand oxyhaemoglobin desaturation as measured bypulse oximetry.3,5,6 Apnoea can be classified ac-cording to various physiological mechanisms (cen-tral, obstructive and mixed).7 Central apnoeaoccurs in the absence of respiratory effort. Ob-structive apnoea occurs when there is collapse ofthe airway and no airflow takes place despite con-tinued breathing effort. When airway collapse oc-curs in association with a central pause, mixedapnoea results. Because these subtypes differ in
) Tel.: D1-216-844-5140; fax: D1-216-844-3380.E-mail address: [email protected].
Seminars in Neonatology (2004) 9, 205e211
www.elsevierhealth.com/journals/siny
1084-2756/$ - see front matter 2003 Elsevier Ltd. All rights reserved.doi:10.1016/j.siny.2003.11.007
mailto:[email protected]://www.elsevierhealth.com/journals/sinyhttp://www.elsevierhealth.com/journals/sinymailto:[email protected] -
7/30/2019 TYUITe
2/7
certain physiological features, the detection of ap-noea is dependent on the methodology employedto observe it. Most neonatal intensive care units(NICUs) and home monitors utilize impedance tech-nology. Impedance pneumography detects respira-tion by translating changes in electrical propertiesof the thorax into a waveform that represents
breathing. Movement of the chest wall contributesthe signal of greatest magnitude, although bloodflow through the heart and great vessels alsoaffects this signal. Both false-positive and false-negative detection of apnoea can occur. Preterminfants typically exhibit mixed apnoea,8 whichcan go undetected by transthoracic impedance.Therefore the extent of abnormal breathing willnot be appreciated. Respiratory inductance pleth-ysmography may give a more accurate picture ofan infants cardiorespiratory development, howeverthis technique is not in widespread clinical use.9
Additional features of immature cardiorespiratory
control are similarly dependent on technologicalconsiderations, such as whether pulse oximetry ismonitored and how these data are displayed andrecorded.
Clinical findings associated with apnoea may in-clude cyanosis, pallor and hypotonia. While apnoeamay occur as an isolated event, it commonly isassociated with bradycardia and desaturation ofperipheral oxyhaemoglobin. These associationsare consistently seen in both hospitalized infantsand those on home monitoring. While clinical carehas focused on prolonged apnoea, that is, pauses
greater than 20 s, alterations of heart rate and oxy-haemoglobin saturation may be seen with shorterepisodes. Additionally, apnoea events exceeding30 s are occasionally seen in both healthy termand preterm infants.1 This suggests that apnoea du-ration per se may not be the critical feature of al-tered breathing and its relation to circulatoryconsequences.
Apnoea episodes lasting longer than 30 s weredescribed by Daily (1969) in 25% of hospitalizedpreterm infants.10 Later reports would focus onapnoea that continued after discharge from thehospital, with the apnoea duration interval ofinterest shortened to 15e20 s. While no data havebeen offered to arrive at an optimal definition ofapnoea, the conventional definition is absence ofbreathing for more than 20 s, or a shorter pause as-sociated with clinical signs, such as bradycardia orcyanosis.
Numerous conditions in the newborn may haveapnoea as a presenting sign. Before concludingthat apnoea is due to immature respiratory control,other potential causes should be considered. Cen-tral nervous system problems, particularly intra-
cranial bleed can produce apnoea. Infections(sepsis, meningitis) and anaemia may also presentwith an abnormal breathing pattern. Other condi-tions that sometimes precipitate apnoea includemetabolic disorders, especially hypoglycaemia,temperature instability and drugs administered tothe mother such as opiates and magnesium.
The possibility of gastro-oesophageal reflux(GOR) as a cause for apnoea should be consideredcautiously. Although both apnoea and GOR are of-ten seen in premature infants, investigations intothe timing of reflux suggest the relationship is oftencoincidental rather than causal. This may explainthe finding that treatment of reflux in prematureinfants has little effect on apnoea episodes.11
Episodes of bradycardia are common in preterminfants and often occur along with apnoea. Brady-cardia may be a result of chemoreceptor inducedinhibition of heart rate,12 or possibly hypoxia asso-ciated with apnoea (Fig. 1). Episodes of bradycar-
dia that include intervals of as long as 3 s withouta QRS complex are sometimes seen in preterm in-fants, typically with no clear evidence of a distur-bance in cardiac rhythm.
With the increasing availability and accuracy ofpulse oximetry, attention has turned to desatura-tion events.13 Episodes of oxyhaemoglobin desatu-ration are familiar in preterm infants and can alsobe demonstrated in healthy term infants. Whenhome monitoring data were sampled for epochsof non-event data in a control (healthy term) co-hort of infants, occasional episodes of desaturation
were not uncommon. Desaturation to at least 10%below baseline was found in 59% of the infants.These episodes occurred in 0.51% of the sampledtime intervals.14
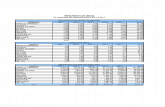
The likelihood of oxyhaemoglobin desaturationand the depth of this desaturation are generallyrelated to the duration of apnoea and to any asso-ciated heart rate change. When 21 647 events of
APNOEA,HYPOVENTILATION
BRADYCARDIA DESATURATION
inhibitoryreflexes
decreasedoxygendelivery
carotid body
Decreased Respiratory Drive
Figure 1 Possible mechanisms relating apnoea, brady-cardia and oxyhaemoglobin desaturation (reprinted withpermission from Ref.13).
206 T.M. Baird
-
7/30/2019 TYUITe
3/7
apnoea were analyzed for decrease in oxyhaemo-globin saturation (SpO2), median desaturation in-creased (SpO2 was lower) with increasing lengthof apnoea duration. Furthermore, by categorizingbradycardia according to severity, this desaturationwas seen to worsen with increasing severity of bra -dycardia, except the most extreme events (Fig. 2).1
Treatment of apnoea
The methylxanthines are the pharmacologicalagents most commonly used for the treatment ofapnoea. Theophylline (1,3-dimethylxanthine) wasfirst reported for use in apnoea of prematurity inthe 1970s.15 It has been used extensively since thattime. Initial reports emphasized increased respira-tory centre output16 and enhanced diaphragmaticcontractility17 as a mechanism of action.
Caffeine (1,3,7-trimethylxanthine) has also beenshown to decrease apnoea in preterm infants andmay be the preferable agent for a number of rea-sons. Its therapeutic index is higher, making toxicityless of a concern. Also, because of its longer half-life, once a day dosing is possible.18 A Cochranereview of the use of methylxanthines concludedthat there is evidence that they reduce apnoeaepisodes and decrease the use of intermittentpositive pressure ventilation (IPPV) in preterminfants.19 Although the precise site of action andmechanism(s) whereby apnoea is decreased havenot been determined, evidence suggests methyl-xanthines stimulate central neural output to therespiratory muscles, probably via antagonism ofadenosine receptors.
Side effects of theophylline include hyperactiv-ity, tachycardia, cardiac dysrhythmias, feeding in-tolerance and seizures. Mild diuresis is seen with allmethylxanthines. Possible drugedrug interactionsinclude medications that affect liver function andmedications where clearance is dependent on cyto-chrome P-450. Due to the limited therapeutic ben-efit and ongoing questions regarding long-term sideeffects,20 clinical trials continue in the use ofmethylxanthines for apnoea of prematurity.
Doxapram is a respiratory stimulant that is typi-
cally used in addition to a methylxanthine.21,22
Intwo head-to-head trials (both involving small num-bers of infants) it was shown to be effective but nobetter for the reduction of apnoea in preterm in-fants and may have some additive effect when usedin refractory cases.23,24 Side effects include poortolerance of the oral preparation and a report ofsecond-degree heart block in a small number ofpreterm infants.25
Non-pharmacological approaches have beenused in the treatment of apnoea. Continuous posi-tive airway pressure (CPAP) is a relatively safe andeffective treatment. CPAP is thought to decreasethe frequency of apnoea by splinting the upper air-way with positive pressure. Because apnoea fre-quently involves an obstructive component, CPAPis effective in infants whose episodes are precipi-tated or prolonged by pharyngeal obstruction.High-flow nasal cannula has been suggested as anequivalent treatment modality.26 For refractorycases, endotracheal intubation and artificial venti-lation may be needed. Minimal ventilator settingsshould be used to allow for spontaneous ventilatoryefforts and to minimize the risk of barotrauma.
0
5
10
15
20
25
30
Mediande
crease%SpO2
None Mild Moderate Severe
Bradycardia
< 16 s
1619.9 s
2029.9 s
> 30 s
Apnoea
duration
Figure 2 Decrease in percentage of oxygen saturation (SpO2) in infants experiencing apnoea or bradycardia. Thebaseline saturation for all events was 98e99% (reproduced with permission from Ref.1).
Clinical correlates, natural history and outcome of neonatal apnoea 207
-
7/30/2019 TYUITe
4/7
Resolution of apnoea
Frequency and severity of events
In the largest study to date of post-dischargecardiorespiratory events, the Collaborative HomeInfant Monitoring Evaluation (CHIME study) des-
cribed 6993 events exceeding conventional monitorthresholds in 445 infants. These subjects were froma total enrollment of 1097 infants that included sixepidemiological groups thought to possibly be atrisk for SIDS, and normal control infants. Therewas a total of 718 358 h of monitor use; inductanceplethysmography was utilized. Events occurred in41% of all infants, including the healthy term (con-trol) infants. The majority of events were apnoeawithout bradycardia: 75% of all events.1 This is incontrast to reports of events when transthoracicimpedance is utilized, which have suggested that
bradycardia is the predominant event.27
This dis-crepancy is most likely due to methodology as ex-plained above. Indeed, 70% of all apnoeic eventsincluded at least three obstructed breaths in theCHIME study event data. When apnoea of shorterduration is considered, the frequency of eventsrises dramatically.1,4 Di Fiore et al. describedevents in a group of infants referred for clinicalbedside studies; she found that the incidence of20 s apnoea episodes was relatively low and didnot distinguish clinically abnormal infants frommatched controls. There were numerous eventsof shorter duration and these were often associated
with bradycardia and desaturations.28 In a cohortof 35 infants monitored overnight, there were865 events of either apnoea, bradycardia or desa-turation. When considering the question of long-term morbidity associated with apnoea, shortevents will therefore account for the majorityof instances of oxyhaemoglobin desaturation, al-though the magnitude of desaturation increasesas apnoea duration lengthens. If recurrent episodesof hypoxia are found to compromise an infantslong-term outcome, measuring and quantifyingevents will be a central question in describing ab-
normal breathing.
Resolution of apnoea
Both full term and preterm infants show a progres-sive decrease in apnoea episodes over time. How-ever, a large variation of apnoea frequency isfound between infants and in the same infant onrepeat apnoea recordings. Both periodic breathingdensity and apnoea density decrease with advanc-ing age. In a relatively small study describing these
abnormalities in normal infants, apnoea exceeding15 s was only found in the first month of life, al-though the duration of shorter apnoeas did notchange as development proceeded.29
Apnoea of prematurity can be expected to re-solve by about 37 weeks post-conceptual age(PCA), with some notable exceptions. CHIME Study
data showed that cardiorespiratory events in pre-term infants return to the baseline normal levelat about 43e44 weeks PCA. In other words, beyond43e44 weeks post-PCA the incidence of cardiore-spiratory events in preterm infants does not signif-icantly exceed that in term babies.1 In an earlierreport of term and preterm infants, 249 infantswith apnoea were drawn from a pool of O25000births. Apnoea episodes were shown to disappearby 37 weeks PCA in 92% of these infants and by 40weeks PCA 98% were apnoea-free.30 This samplemay not have included sufficient numbers of ex-tremely small infants to reflect their special prob-
lems. More recently, it has been shown that inthe most premature infants (24e28 weeks gesta-tion) apnoea frequently persists beyond 36 weekspost-PCA and may persist beyond 40 weeks post-PCA.31
Discharge from hospital
Most preterm infants no longer have significant ep-isodes of apnoea by the time they are ready for hos-pital discharge. This generally occurs at about thesame time as maturation of temperature controland feeding pattern. An apnoea-free observationperiod, usually ranging from 3e7 days is often uti-lized as a criterion for determining discharge. Inthe only study that has attempted to address thisissue, an apnoea-free interval of 8 days was sug-gested.32 In a subset of infants, however, dischargemay be delayed by persistence of cardiorespiratoryevents. In these infants, home cardiorespiratorymonitoring until 43e44 weeks PCA may offer an al-ternative to a prolonged hospital stay.
Home monitoring
When home cardiorespiratory monitoring is pre-scribed, documented (event recording) monitoringcan help the clinician follow the ongoing resolutionof events. The question of whether or not monitor-ing otherwise benefits these infants is still unre-solved. One of the ways in which the homeapnoea monitor may function is as a therapeuticdevice. It has been suggested that the alarm maynot only alert the caregivers, but the auditory stim-ulus may arouse the infant sufficiently to terminate
208 T.M. Baird
-
7/30/2019 TYUITe
5/7
an event. This hypothesis has never been rigorouslytested. Alternatively, the monitor may serve as analarm mechanism. According to this model, themonitor alarm alerts a caregiver to a potentiallydangerous condition and intervention can be madein a timely fashion. However, there is no good evi-dence to suggest that monitors as they are cur-
rently configured and used provide a warningthat is related to an impending dangerous event.It is similarly not known whether such an eventcould be terminated while in progress. It has beensuggested that infants with frequent events shouldbe rehospitalized and have further studies and thatadditional diagnoses might come to medical atten-tion in this manner.27 Whether these infants wouldeventually declare themselves otherwise is un-certain. Epidemiological studies have not shownan effect of home monitors when used in Sudden In-fant Death Syndrome (SIDS) prevention.33
Rosen et al. have recently observed that sleep
disordered breathing in 8e11 year old children ismore prevalent in those with a history of prematu-rity.34 This raises the questions as to whether a priorhistory of apnoea of prematurity and accompany-ing physiological phenomena might predispose tolonger lasting disordered respiratory regulationand might be worthy of a prospective study.
Consequences of apnoea of prematurity
Developmental outcome
There are few conclusive reports describing the re-lationship between apnoea in premature infantsand neurodevelopmental outcome. The reportsthat do exist are all confronted with the problemof separating the consequences of premature birthfrom the effects of apnoea. Infants born prema-turely have a higher rate of central nervous systeminjury, especially periventricular leukomalacia andintraventricular haemorrhage. These conditions bythemselves contribute to poor neurodevelopmen-tal outcome and also cause apnoea. No study haslooked at baseline neurological status and retestedthis finding after the occurrence of events. Finally,studies that assess improvement in long-term out-come as a result of treating apnoea of prematurityare few and are confounded by these same issues.
Nevertheless, a few follow-up studies of at-riskinfants have attempted to address this problem.In one cohort of preterm infants, factors that pre-dicted poor neurodevelopmental outcomes at earlyschool age included apnoea of prematurity.35 Out-comes measured in this group included cognitive
function, neuropsychological abilities, academicachievement and parent and teacher ratings ofchild behaviour and school performance. Anotherseries of very low birth weight (VLBW) infants fol-lowed to 24 months of age showed a correlation be-tween predischarge apnoea and lower mental andmotor neurodevelopmental scores.36 Other series
of case comparisons have reported no differencein outcome of infants with apnoea.37,38 It is possi-ble that recurrent hypoxia, not apnoea per se isthe detrimental feature of the breathing abnormal-ities exhibited by some preterm infants. However,even if an association between recurrent hypoxiaand poor neurodevelopment can be established,this does not prove a cause and effect relationship.
Relationship to SIDS
Evidence indicates that apnoea is not predictive of,or a precursor to, SIDS. An initial case report fromthe early 1970s linked apnoea and SIDS in multipleinfants in a family.39 This report generated the hy-potheses that apnoea might be a precursor to SIDSand also that abnormal breathing might predictwhich infants might later die of SIDS. When this ini-tial case report was revealed (years later) to bemultiple cases of infanticide, reconsideration ofthe role of apnoea was warranted. Numerous ab-normalities in breathing, heart rate and sleep havebeen identified in selected populations thought to
represent infants who might die of SIDS. Suspectedabnormalities have included periodic breathing,40
abnormalities in short-term descriptors of heartrate and breathing41,42 and apnoea characteris-tics.43 Many of the described abnormalities wereseen in infants with a so-called near-miss event,or who came to attention as subsequent siblingsof SIDS infants. These groups may be a heteroge-neous mixture with various problems and findingshave been inconsistent. A prospective approachhas been to describe breathing abnormalities in in-fants who had physiological studies (for variousreasons) and who would later die of SIDS. Whereasone of these population-based studies identifiedsubtle breathing and heart rate abnormalities,44
generally this approach has failed to show any con-clusive predictors.45 Similarly, epidemiologicallybased data on the use of home apnoea monitorsare limited, but have failed to show any conclusiveeffect of home monitoring on SIDS rates.32,46 Whenage at SIDS death is compared to the disappearanceof pathological apnoea, it is seen that apnoea ofprematurity resolves prior to the peak incidenceof SIDS. This finding lends further support to the
Clinical correlates, natural history and outcome of neonatal apnoea 209
-
7/30/2019 TYUITe
6/7
notion that apnoea of prematurity is unrelated toSIDS (Fig. 3).
References
1. Ramanathan R, Corwin M, Hunt C, Lister G, Tinsley LR, BairdT, et al. Cardiorespiratory events recorded on home
monitors: comparison of healthy infants with those atincreased risk for SIDS. J Am Med Assoc 2001;285:2199e207.
2. Parmelee AH, Stern E, Harris MA. Maturation of respiration inprematures and young infants. Neuropadiatrie 1972;3:294e304.
3. Henderson-Smart DJ. The effect of gestational age on theincidence and duration of recurrent apnoea in newbornbabies. Aust Pediatr J 1981;17:273e6.
4. Hodgeman JE, Gonzalez F, Hoppenbrouwers T, Cabal LA.
Apnea, transient episodes of bradycardia, and periodicbreathing in preterm infants.Am J Dis Child1990;144:54e7.
5. Barrington K, Finer N. The natural history of the appearanceof apnea of prematurity. Pediatr Res 1991;29:372e5.
6. Carlo WA, Martin RJ, Versteegh FGA, Goldman MD, RobertsonSS, Fanaroff AA. The effect of respiratory distress syndromeon chest wall movements and respiratory pauses in preterminfants. Am Rev Respir Dis 1982;26:103e7.
7. Miller MJ, Martin RJ. Pathophysiology of apnea of pre-maturity. In: Polin RA, Fox WW, editors. Fetal and neonatal
physiology. 2nd ed. London: W.B. Saunders Company; 1998.p. 1129e41.
8. Thach BT, Stark AR. Spontaneous neck flexion and airwayobstructionduring apneic spells in preterm infants.J Pediatr1979;94:275.
9. Brouillette RT, Morrow AS, Weese-Mayer DE, Hunt CE.Comparison of respiratory inductive plethysmography andthoracic impedance for apnea monitoring. J Pediatr 1987;111:377e83.
10. Daily WJR, Klaus M, Meyer HBP. Apnea in premature in-fants: monitoring, incidence, heart rate changes, and aneffect of environmental temperature. Pediatrics 1969;43:510e8.
11. Kimball AL, Carlton DP. Gastroesophageal reflux medicationsin the treatment of apnea in premature infants. J Pediatr2001;138:355e60.
12. Henderson-Smart DJ, Butcher-Puech MC, Edwards DA. In-cidence and mechanism of bradycardia during apnoea inpreterm infants. Arch Dis Child 1986;61:227e32.
13. Martin RJ, Fanaroff AA. Neonatal apnea, bradycardia or
desaturation: does it matter? J Pediatr 1998;132:758e9.14. Hunt CE, Corwin MJ, Lister G, Weese-Mayer DE, Neuman MR,
Tinsley L, et al. Longitudinal assessment of hemoglobinoxygen saturation in healthy infants during the first 6 monthsof age. J Pediatr 1999;134:580e6.
15. Aranda JV, Gorman W, Bergsteinsson H, Gunn T. Efficacy ofcaffeine in treatment of apnea in the low-birthweightinfant. J Pediatr 1977;90:467e72.
16. Gerhardt T, McCarthey J, Bancalari E. Effect of aminophyl-line on respiratory center activity and metabolic rate inpremature infants with idiopathic apnea. Pediatrics 1979;63:537e42.
17. Aubier M, DeTroyer A, Sampson M, Macklem PT, Roussos C.Aminophylline improves diaphragmatic contractility. N Engl
J Med 1981;305:249e52.18. Aranda JV, Cook CE, Gorman W, Collinge JM, Laughnan PM,
Outerbridge EW, et al. Pharmacokinetic profile of caffeine inthe premature newborn infant with apnea. J Pediatr1979;94:664e8.
19. Steer PA, Henderson-Smart DJ. Caffeine versus theophyllinefor apnea in preterm infants. Cochrane Database Syst Rev2000;2:CD000273.
20. Schmidt B. Methylxanthine therapy in premature infants:sound practice, disaster, or fruitless byway? J Pediatr1999;135:526e8.
21. Bairam A, Faulon M, Monin P, Vert P. Doxapram for the initialtreatment of idiopathic apnea of prematurity. Biol Neonate1992;61:209e13.
Term 3 months 6 months
Relativeincidence
} SIDS (m SD)24 weeks GA
40 weeks GA
Apnoea of prematurity
Age
Pre-term
Figure 3 Relationship between the timing of peak inci-dence of SIDS (sudden infant death syndrome) to the(relative) incidence of apnoea in infants with apnoea ofprematurity. GA, gestational age; m, mean; SD, standarddeviation (reproduced with permission from Ref.47).
Practice points
A thorough consideration of the possiblecauses is necessary for each infant whopresents with apnoea.
The time course for the resolution ofapnoea of prematurity is predictable onthe basis of post-conceptual age.
The most premature infants can beexpected to take longer to resolve theirapnoea of prematurity.
Methylxanthines may decrease the needfor more invasive respiratory support,however, further investigation regardingtheir long-term side effects is warranted.
Research directions
Research is needed for the following:
Understanding of the relationship of apnoeicepisodes to oxygenation of vital organs,particularly the brain.
Determining the long-term consequences of
treating apnoea with methylxanthines. Defining a method for quantifying apnoea in
the newborn. Determining whether apnoea has any long-
term outcome consequences independent ofpreterm birth.
210 T.M. Baird
-
7/30/2019 TYUITe
7/7
22. Poets CF, Darraj S, Bohnhorst B. Effect of doxapram onepisodes of apnoea, bradycardia and hypoxaemia in preterminfants. Biol Neonate 1999;76:207e13.
23. Eyal F, Alpan G, Sagi E, Glick B, Peleg O, Dgani Y, et al.Aminophylline versus doxapram in idiopathic apnea ofprematurity: a double-blind controlled study. Pediatrics1985;75:709e19.
24. Peliowski A, Finer N. A blinded, randomized, placebo-controlled trial to compare theophylline and doxapram for
the treatment of apnea of prematurity. J Pediatr 1990;116:648e53.
25. De Villers GS, Walele A, Van Der Merwe P-L, Kalis NN.Second-degree atrioventricular heart block after doxapramadministration. J Pediatr 1998;133:149e50.
26. Sreenan C, Lemke RP, Hudson-Mason A, Osiovich H. High-flow nasal cannulae in the management of apnea ofprematurity: a comparison with conventional nasal contin-uous positive airway pressure. Pediatrics 2001;107:1081e3.
27. Cote A, Hum C, Brouilette RT, Themens M. Frequency andtiming of recurrent events in infants using home cardiore-spiratory monitors. J Pediatr 1998;312:783e9.
28. Di Fiore JM, Arko MK, Miller MJ, Krauss A, Betkerur A, ZadellA, et al. Cardiorespiratory events in preterm infants referredfor apnea monitoring studies. Pediatrics 2001;108:1304e8.
29. Hoppenbrouwers T, Hodgeman JE, Harper RM, Hofman E,Sterman MB, McGinty DJ. Polygraphic studies of normalinfants during the first six months of life: III. Incidence ofapnea and periodic breathing. Pediatrics 1977;60:418e25.
30. Henderson-Smart DJ. The effect of gestational age on theincidence and duration of recurrent apnoea in newbornbabies. Aust Paediatr J 1981;17:273e6.
31. Eichenwald EC, Aina A, Stark AR. Apnea frequently persistsbeyondterm gestation in infants deliveredat 24 to 28 weeks.Pediatrics 1997;100:354e9.
32. Darnall RA, Kattwinkel J, Nattie C, Robinson M. Margin ofsafety for discharge after apnea in preterm infants.Pediatrics 1977;100:795e801.
33. Ward SL, Keens TG, Chan LS, Chipps BE, Carson SH, DemingDD, et al. Suddeninfant death syndrome in infants evaluated
by apnea programs in California. Pediatrics 1986;77:451e5.34. Rosen CL, Larkin EK, Kirchner L, Emancipator JL, Bivins SF,
Surovec SA, et al. Prevalence and risk factors for sleep-disordered breathing in 8- to 11-year-old children: associa-tion with race and prematurity. J Pediatr 2003;142:383e9.
35. Taylor HG, Klein N, Schatschneider C, Hack M. Predictors ofearly school age outcomes in very low birth weight infants.
J Dev Behav Pediatr1998;19:235e43.36. Cheung P, Barrington KJ, Finer NN, Robertson CMT. Early
childhoodneurodevelopmentin very low birth weight infantswith predischarge apnea. Pediatr Pulmonol 1999;27:14e20.
37. Koons AH, Mojica N, Jadeja N, Ostfeld B, Hiatt M, Hegyi T.Neurodevelopmental outcome of infants with apnea ofinfancy. Am J Perinatol 1993;10:208e11.
38. Levitt GA, Mushin A, Bellman S, Harvey DR. Outcome ofpreterm infants who suffered neonatal apnoeic attacks.Early Hum Dev 1998;16:235e43.
39. Steinschneider A. Prolonged apnea and the sudden infantdeath syndrome: clinical and laboratory observations.Pediatrics 1972;50:646e54.
40. Kelly DH, Shannon DC. Periodic breathing in infants withnear-miss sudden infant death syndrome. Pediatrics 1979;63:355e69.
41. Leistner HL, Haddad GG, Epstein RA, Lai TL, Epstein MA,Mellins RB. Heart rate and heart rate variability during sleepin aborted sudden infant death syndrome. J Pediatr 1980;97:51e5.
42. Gordon D, Cohen RJ, Kelly D, Akselrod S, Shannon DC.Sudden infant death syndrome: abnormalities in short term
fluctuations in heart rate and respiratory activity. PediatrRes 1984;18:921e6.
43. Kahn A, Blum D, Rebuffat E, Sottiaux M, Levitt J, Bochner A,et al. Polysomnographic studies of infants who subsequentlydied of sudden infant death syndrome. Pediatrics 1988;82:721e7.
44. Schectman VL, Harper RM, Wilson AJ, Southall DP. Sleepapnea in infants who succumb to the sudden infant deathsyndrome. Pediatrics 1991;7:841e6.
45. HoffmanHJ, Damus K, Hillman L, Krongrad E. Risk factors forSIDS. Results of the National Institute of Child Health andHuman Development SIDS Cooperative EpidemiologicalStudy. Ann N Y Acad Sci 1988;533:13e30.
46. MacKay M, Abreu e Silva FA, MacFadyen UM, Williams A,Simpson H. Home monitoring for central apnea. Arch DisChild1984;59:136e42.
47. Miller MT, Fanaroff AA, Martin RJ. Respiratory disorders inpreterm and term infants. In: Fanaroff AA, Martin RJ,editors. Neonataleperinatal medicine. 7th ed. Philadelphia:Harcourt; 2002. p. 1025e49.
Clinical correlates, natural history and outcome of neonatal apnoea 211