
UNIVERSIDAD DE GUAYAQUIL FACULTAD DE …repositorio.ug.edu.ec/bitstream/redug/18194/1/BCIEQ-MBC-134...
51
UNIVERSIDAD DE GUAYAQUIL FACULTAD DE CIENCIAS QUÍMICAS MAESTRÍA EN BIOQUÍMICA CLÍNICA TRABAJO DE TITULACIÓN EXAMEN COMPLEXIVO PARA LA OBTENCIÓN DEL GRADO DE MAGISTER EN BIOQUÍMICA CLÍNICA “DETECCION DE LINFOMA DE HODGKIN ASOCIADO A ANORMALIDADES EN EL TRACTO GASTROINTESTINAL MEDIANTE ANÁLISIS CLÍNICO” AUTOR: Q.F. KARINA ALEXANDRA CORDERO LOPEZ TUTOR: Q.F. AÍDA CASTRO POSLIGUA MSc. GUAYAQUIL – ECUADOR SEPTIEMBRE 2016
Transcript of UNIVERSIDAD DE GUAYAQUIL FACULTAD DE …repositorio.ug.edu.ec/bitstream/redug/18194/1/BCIEQ-MBC-134...
UNIVERSIDAD DE GUAYAQUIL
FACULTAD DE CIENCIAS QUÍMICAS
MAESTRÍA EN BIOQUÍMICA CLÍNICA
TRABAJO DE TITULACIÓN EXAMEN COMPLEXIVO
PARA LA OBTENCIÓN DEL GRADO DE MAGISTER EN
BIOQUÍMICA CLÍNICA
“DETECCION DE LINFOMA DE HODGKIN ASOCIADO A
ANORMALIDADES EN EL TRACTO GASTROINTESTINAL
MEDIANTE ANÁLISIS CLÍNICO”
AUTOR: Q.F. KARINA ALEXANDRA CORDERO LOPEZ
TUTOR: Q.F. AÍDA CASTRO POSLIGUA MSc.
GUAYAQUIL – ECUADOR
SEPTIEMBRE 2016
REPOSITORIO NACIONAL EN CIENCIAS Y TECNOLOGÍA FICHA DE REGISTRO ESTUDIO DE CASO EXAMEN COMPLEXIVO TÍTULO: DETECCION DE LINFOMA DE HODGKIN ASOCIADO A ANORMALIDADES EN EL TRACTO GASTROINTESTINAL MEDIANTE ANÁLISIS CLÍNICO. AUTOR: Q.F. KARINA A. CORDERO LÓPEZ REVISORES:
INSTITUCIÓN: UNIVERSIDAD DE GUAYAQUIL FACULTAD: CIENCIAS QUÍMICAS
PROGRAMA: MAESTRÍA EN BIOQUÍMICA CLÍNICA
FECHA DE PULICACIÓN: 17-08-2016 NO. DE PÁGS: 25 ÁREA TEMÁTICA: CIENCIAS DE LA VIDA PALABRAS CLAVES: Linfoma de Hodgking, Linfoma No Hodgkin, Virus de Epstein Barr, Pediatría. RESUMEN: El cáncer, en cualquiera de sus formas, tiene mayor incidencia en el mundo y afecta a todas las edades, y aunque se realizan investigaciones para detectar su presencia, en muchos de los casos se descubren demasiado tarde. El linfoma es una forma de cáncer que presenta manifestaciones clínicas que pueden estar enmascaradas bajo una infección leve, haciendo que el tratante desvíe su diagnóstico, sobre todo cuando los signos y síntomas tanto del Linfoma de Hodgkin y No Hodgkin presentan cuadros similares, razón por la cual no es posible detectarlo con la información de un examen físico, ni existe una regla para incluir biomarcadores específicos que sirvan para determinar la existencia o no de la enfermedad, lo ideal es proponer pruebas cuyos resultados determinen su estado actual como punto de partida y basándose en ellos estar orientados a pruebas más específicas. La investigación en éste caso, no sólo está basada en el análisis clínico que demuestra la situación inicial del paciente y sirve como medio de orientación para la toma de decisiones, sino que está complementada con la utilización de imágenes y otros medios exploratorios cuyos resultados en la fase de discusión sirven para establecer las razones por las que se excluyen otras patologías y permiten discernir por un diagnóstico final.
N° DE REGISTRO(en base de datos): N° DE CLASIFICACIÓN: Nº
DIRECCIÓN URL (estudio de caso en la web) www.nejm.org
ADJUNTO URL (estudio de caso en la web): www.nejm.org
ADJUNTO PDF: SI: X NO
CONTACTO CON AUTOR: Teléfono: 2888930
E-mail: [email protected]
CONTACTO EN LA INSTITUCION: Nombre:
Teléfono:
ii
CERTIFICACIÓN DEL TUTOR
En mi calidad de tutor del estudiante Q.F. KARINAALEXANDRA CORDERO
LÓPEZ, del Programa de Maestría/Especialidad BIOQUÍMICA CLÍNICA, nombrado
por el Decano de la Facultad de CIENCIAS QUÍMICAS. CERTIFICO: que el estudio
de caso del Examen Complexivo titulado: DETECCION DE LINFOMA DE
HODGKIN ASOCIADO A ANORMALIDADES EN EL TRACTO
GASTROINTESTINAL MEDIANTE ANÁLISIS CLÍNICO, en opción al grado
académico de Magíster (Especialista) en BIOQUÍMICA CLÍNICA, cumple con los
requisitos académicos, científicos y formales que establece el Reglamento aprobado
para tal efecto.
Atentamente
Q.F. AÍDA CASTRO POSLIGUA MSc.
Guayaquil, 17 de Agosto de 2016
iii
DEDICATORIA
A mi mami
A mi Esposo e Hijos
A mi papá y a mis hermanos
iv

AGRADECIMIENTO
Al Dr. Vicente Illingworth Ashton, DCP.
v

DECLARACIÓN EXPRESA
“La responsabilidad del contenido de esta Tesis de Grado, me corresponden
exclusivamente; y el patrimonio intelectual de la misma a la UNIVERSIDAD DE
GUAYAQUIL”
Q.F. KARINA ALEXANDRA CORDERO LÓPEZ
vi

ABREVIATURAS
AFP: Alfafetoproteína
CMV: Citomegalovirus
GPT: Transaminasa glutámico pirúvica
HIV: Virus de Inmunodeficiencia Humana
HTLV-1: Virus linfotrópico de células T humano Tipo I
LH: Linfoma de Hodgkin
LNH: Linfoma No Hodgkin
PCR: Proteína C Reactiva
PET-TC: Tomografía Computarizada por emisión de positrones
TC: Tomografía Computarizada
VEB: Virus de Epstein Barr
VSG: Velocidad de Sedimentación Globular
vii

TABLA DE CONTENIDOS
CERTIFICACIÓN DEL TUTOR…………………….…..………………………… iii
DEDICATORIA ………………………......…………………...…...…….....….. iv
AGRADECIMIENTO.……………………...…………….…………...…………... v
DECLARACIÓN EXPRESA ……………………………………..….………...…. vi
ABREVIATURAS…………………………………...………………...……….…. vii
TABLA DE CONTENIDOS……………………......………………...……….…. viii
INDICE DE TABLAS………………………………….....…………….….………. ix
RESUMEN ………………………………………………...….………..…………. x
ABSTRACT……………………………………………...………………………. xii
INTRODUCCIÓN …………………………………………...……...….……….….. 1
DESARROLLO ……………………………………………...…...…...………..…. 5
1. Marco Teórico …………………………………………………....…….….. 5
2. Marco Metodológico………………………………………….…………….. 8
2.1 Metodología …………………………………………...………......…..... 8
2.2 Descripción del Método ……………...……………………...….……… 8
2.2.1 Análisis de Laboratorio Clínico …..…...……………….….……. 8
2.2.2 Imagenología ………………………….....……………………… 9
2.2.3 Patología ……...……………………………..………………….. 9
2.2.4 Exploración Endoscópica ……………………………………… 10
2.3 Premisa …………………………………..…………………………….. 10
2.4 Descripción de las unidades de análisis ………...…………..…………. 12
viii
2.4.1 Análisis Químico Clínico ………….………………….……….. 12
2.4.2 Imágenes ……………………...………………………….……. 13
2.4.3 Muestras para patología ………………...……………….…….. 14
2.4.4 Endoscopía …………………….…...…………………….......... 14
2.5 Gestión de Datos …………………………….………..………...…...... 14
2.6 Criterios éticos de la Investigación ………...….…………………...…. 14
3. Resultados …………………….………………...……………………….... 15
3.1 Antecedentes de la Unidad de Análisis …………………..……...…...... 15
3.2 Presentación de resultados …………………….……...……...…....….. 15
3.2.1 Resultados basados en el laboratorio clínico ……...…..…......... 15
3.2.2 Resultados basados en imágenes …………………...………..... 18
3.2.3 Resultados basados en el estudio patológico ……...…..…......... 18
3.2.4 Resultados de la exploración endoscópica ……...……………... 19
4. Discusión ………………...…………………………………………..…..… 20
4.1 Contrastación Empírica ……………...………………………………… 20
4.2 Limitaciones ……………...…………………………………..…..……. 22
4.3 Líneas de Investigación …………………………..…….…..…..……… 22
4.4 Aspectos novedosos del estudio del caso ……………..…………..…… 23
5. Propuesta ….……………………………………………………………….. 24
Conclusiones y recomendaciones …………...……………………..……… 25
Referencias Bibliográficas …………...……..…………………………….. 26
ix
ÍNDICE DE TABLAS
Tabla1. Datos de Laboratorio…………………………………………………….. 16
x

RESUMEN
Cada día el cáncer, en cualquiera de sus formas, tiene mayor incidencia
en el mundo y afecta a todas las edades, y aunque se realizan investigaciones para
detectar su presencia, en muchos de los casos se descubren demasiado tarde. El
linfoma es una forma de cáncer que presenta manifestaciones clínicas que pueden estar
enmascaradas bajo una infección leve, haciendo que el tratante desvíe su diagnóstico,
sobre todo cuando los signos y síntomas de los Linfomas de Hodgkin y No Hodgkin
presentan cuadros similares, por lo que no es posible detectarlo con la información de
un examen físico, ni existe una regla para incluir biomarcadores específicos que sirvan
para determinar la existencia o no de la enfermedad, sin embargo, se pueden incluir
como punto de partida, pruebas de laboratorio que permitan establecer el estado de la
enfermedad y basándose en ellas, orientar y seleccionar pruebas más específicas. La
investigación en éste caso, no sólo está basada en el análisis clínico que demuestra la
situación inicial del paciente y sirve como medio de orientación para la toma de
decisiones, sino que está complementada con la utilización de imágenes y otros medios
exploratorios cuyos resultados en la fase de discusión sirven para establecer las razones
por las que se excluyen otras patologías y permiten discernir por un diagnóstico final.
Palabras claves:
Linfoma de Hodgking, Linfoma No Hodking, Virus de Epstein Barr, Tracto
Gastrointestinal.
xi
ABSTRACT
Every day cancer, in any form, has more prevalence in the world and
affects all ages, and although investigations are conducted to detect its presence, in
many cases it is discovered too late. Lymphoma is a form of cancer that has clinical
manifestations that may be masked by a mild infection, causing a divert in the
diagnosis, especially when the signs and symptoms of Hodgkin's and Non-Hodgkin
are similar, so it is not possible to detect with the information of a physical
examination, nor is there a rule to include specific biomarkers to determine the
existence or not of the disease, however, laboratory test can be included as a starting
point, for establishing the status of the disease and based on them, guide and select
more specific tests. The investigation in this case, is not only based on clinical analysis
that shows the initial condition of the patient and serves as a means of orientation for
decision-making, but is complemented by the use of images and other exploration
resources which results in the discussion phase serve to establish the reasons to exclude
other pathologies and allow discern a final diagnosis.
Keywords:
Hodgkin's lymphoma, No Hodgkin's lymphoma, Epstein Barr virus, Gastrointestinal
Tract.
xii
INTRODUCCIÓN
La medicina de laboratorio amplía cada día más su ámbito de acción porque
gracias a los resultados obtenidos se llega a un diagnóstico clínico eficiente y preciso
que asegura la salud del paciente. El desarrollo de pruebas y la tecnología a utilizar
permiten que los valores de los biomarcadores encaminen al profesional médico a
establecer estrategias para llegar a un diagnóstico efectivo y precoz de enfermedades,
por lo tanto, las pruebas de laboratorio juegan un papel fundamental a la hora de tomar
decisiones en la terapéutica a utilizar.
En el análisis clínico, hay pruebas que con un solo resultado pueden establecer
el curso de una enfermedad y su tratamiento, también es necesario aclarar que las
pruebas de laboratorio no son definitivas, pero son el camino a seguir para orientar al
tratante cuando se desconoce la patología y sólo se tiene información de un examen
físico, por lo tanto, los niveles sanguíneos proporcionan la información necesaria a la
hora de la toma de decisiones. En muchos de los casos, éstos niveles revelan
resultados que no estaban considerados en la propuesta médica, el analista clínico
puede sugerir pruebas que refuercen los marcadores en investigación.
En el presente caso, se pretende detectar la presencia de un Linfoma,
inicialmente mediante exploración física considerando signos y síntomas clínicos, y
luego reforzar la información con los datos obtenidos en el laboratorio clínico, pero el
linfoma no responde a biomarcadores conocidos ni la bibliografía médica es definitiva
para dar un diagnóstico. La literatura acerca de los linfomas en general ha adolecido
de una falta de uniformidad en los diagnósticos y clasificaciones. En el caso de los
1
Linfomas Intestinales, esto no ha sido diferente, a lo largo de la historia, se han
aplicado a éstos las sucesivas clasificaciones que la comunidad médica ha generado.
(López San Román, A. Villarrubia Espinoza, J. 2011)
Los estudios han determinado que de acuerdo al tipo de Linfoma, los cuadros
clínicos presentan comportamiento diferentes de acuerdo a la edad, sin embargo no se
puede establecer desde el inicio hacia donde puede llevar la información de una
sintomatología. Existen dos clases de linfomas, el de Hodgkin y el de no Hodgkin y
su diferencia radica principalmente en las características de las células malignas, cómo
se comportan, se propagan y cómo responden al tratamiento, de modo que es
importante diferenciarlos a través de pruebas específicas de laboratorio como
una biopsia y evaluación microscópica de las células cancerígenas. (Natgeo, 2015),
cabe destacar que el uso de métodos de serológicos en corto tiempo orientan hacia el
diagnóstico evitando que se pierda tiempo valioso, tal es el caso de la prueba
serológica para detectar virus de Epstein Barr que por su relación con los linfomas
(Lynphoma Research Fundation, 2011) es importante su ensayo, sobre todo en
situaciones de emergencia, sirviendo de guía para excluir enfermedades o comenzar
un tratamiento.
Este caso cobra interés, puesto que en su evaluación, se observan
manifestaciones típicas con relación al Linfoma No Hodgkin, sin embargo las pruebas
clínicas a lo largo de su estudio indican la presencia de Linfoma de Hodgkin. La
Etiología revela que generalmente, la primera señal del linfoma de Hodgkin es una
inflamación de los ganglios linfáticos que aparece sin una causa conocida. La
enfermedad puede diseminarse a los ganglios linfáticos cercanos y más tarde al bazo,
hígado, médula ósea u otros órganos. (Gersten, 2016) Mientras que las
2
manifestaciones clínicas del LNH dependen de su presentación extranodal que es más
frecuente, e involucra a otros órganos y sistemas como cabeza y cuello, tórax,
abdomen, gónadas y hueso. (Sistema Nacional de Salud, 2011)
El caso en que se presenta ésta ambigüedad de resultados, pertenece al
Departamento de Pediatría, Radiología y Patología del Hospital general de
Massachusetts y al Departamento de Pediatría, Radiología y Patología de la Escuela
de Medicina de Harvard en Boston. Está enfocado en un menor de 12 años que acude
al hospital por presentar síntomas de malestar, fiebre, dolor abdominal y palidez, que
son el punto de partida para la investigación a continuación y que sirven para el
análisis, evaluación y diagnóstico de la enfermedad.
3
OBJETIVO GENERAL
Destacar la importancia del uso de métodos de Laboratorio Clínico que orienten
a comprobar o descartar la presencia de Linfoma de Hodgkin a corto tiempo.
OBJETIVOS ESPECÍFICOS
• Exponer la importancia de los resultados de un análisis clínico como punto
de partida en la toma de decisiones.
• Aconsejar, si es posible, algún método alternativo que contribuya a
minimizar el tiempo de espera para la detección precoz de Linfoma de
Hodgkin antes de llegar a los métodos invasivos.
• Mostrar los cuestionamientos que se presentan a la hora de interpretar los
resultados durante la evaluación del caso
• Indicar la importancia de los biomacardores para la exclusión de posibles
enfermedades con sintomatología similar.
4

1. MARCO TEÓRICO
El área investigativa de la medicina avanza a pasos acelerados para descubrir
y/o establecer métodos que permitan mitigar la acción degenerativa de las
enfermedades. Es un desafío constante al que se somete el investigador para encontrar
el origen de las anormalidades y establecer tratamiento eficaz que conlleve a la salud
del paciente. Estas investigaciones no son aisladas y van de la mano con una serie de
parámetros sean éstos físicos, bioquímicos, histológicos, genéticos, etc., sin embargo, a
pesar del arduo trabajo, cada día hay un giro en la evolución de las enfermedades que
no permiten establecer a simple vista su presencia. Detectar una enfermedad es muy
difícil, la misma anormalidad puede presentar diferente sintomatología y por lo tanto
desviar la atención del tratante. Tal es el caso del linfoma o cáncer de las células
linfáticas, cuyas manifestaciones clínicas son diferentes dependiendo de su origen y
localización.
Linfoma es el nombre de un grupo de tipos de cáncer de la sangre que
comienzan en el sistema linfático, es la segunda causa de cáncer infantil en América
Latina. (Rangel Vega, Villano Castillejos, López facio, Covarrubias Espinoza, &
Rendón García, 2013) Los dos tipos principales de linfoma son el Linfoma de Hodgkin
y el linfoma No Hodgkin. Alrededor del 90 por ciento de las personas con un
diagnóstico de linfoma, tienen linfoma No Hodgkin (NHL, por sus siglas en inglés); el
resto tiene linfoma de Hodgkin. (Leukemia & Lymphoma Society, 2014) El Linfoma
de Hodgkin (LH) comprende el 6% de los cánceres pediátricos, se caracteriza por la
5
presencia en ganglios linfáticos de células atípicas multinucleadas denominadas células
de Reed-Sternberg, las cuales representan el componente maligno del tumor. El nombre
de la enfermedad fue dado en honor al Dr. Thomas Hodgkin, ya que fue el primero en
identificarla en 1832. Solo fue hasta 1865 cuando el Dr. Wilks realiza una extensa
revisión de pacientes, donde se consideran los hallazgos del Dr. Hodgkin como una
nueva enfermedad y se propone el nombre de “Enfermedad de Hodgkin”. El origen del
LH parece ser unifocal y hasta en 90% de los casos presenta una diseminación linfática
por contigüidad. (Ministerio de Salud y Protección Social - Colciencias, 2013)
Los LH y LNH, tienen origen desconocido, no se sabe con certeza su origen,
pero se ha podido establecer factores de riesgo, es decir, aquello que aumenta las
probabilidades de que una persona pueda padecer la enfermedad, que deben ser
tomados en cuenta al momento de una decisión médica.
• Edad: En los casos de LH se presenta en personas de 15 – 40 años y en mayores
de 55 años, mientras que el LNH, el envejecimiento es un factor de riego
pudiendo presentarse en personas entre 60 y 69 años. Aunque en ambos casos,
dependiendo del tipo, pueden presentarse a cualquier edad.
• Sexo: Hay mayor prevalencia en hombres que en mujeres.
• Geografía y Grupos étnicos: Se observa mayor número de casos en
Norteamérica y Europa, siendo menos común en los países asiáticos, asimismo
se ha podido comprobar más casos en personas de raza blanca que en personas
de raza negra o de origen asiático.
• Deficiencia en el sistema inmunológico: el riesgo aumenta en personas que
padecen HIV, así como en personas que se encuentran inmunodeprimidas como
resultado de trasplantes o cualquier otro tratamiento médico.
6

• Infección por virus de Epstein-Barr: Las personas que han tenido
mononucleosis infecciosa que es una infección causada por el virus de Epstein-
Barr (EBV), tienen un riesgo aumentado de enfermedad de Hodgkin, donde las
células B han sufrido una mutación destructiva en el gen que activa la apoptosis,
debido a la presencia de EBV. La infección por EBV se produce en 10 a 70%
de los pacientes con linfoma clásico de Hodgkin, dependiendo del subtipo; un
porcentaje muy alto de estos pacientes tienen el subtipo de celularidad mixta de
linfoma de Hodgkin y son niños o adultos mayores (tercera edad).
• Otros: aunque se encuentran en menor número, no hay que descartar la
exposición a cierto químicos (como el benceno o pesticidas) o la exposición a
radiaciones.
7
2. MARCO METODOLÓGICO
2.1 METODOLOGÍA
Se presenta el caso de un niño de 12 años que acude al hospital con malestar
general, palidez en el rostro, fiebre y dolor abdominal. Un mes antes de la aparición de
los síntomas, el niño presentaba buena salud. Poco tiempo después, aparecen los
síntomas de forma intermitente. Inicialmente se le diagnostica una enfermedad viral,
pero debido a la persistencia de los síntomas, es ingresado a un hospital donde se le
realizan pruebas rutinarias, posteriormente, el paciente es trasladado a otro hospital
donde una vez realizado el examen físico y revisada la sintomatología, se enmarca el
estudio por etapas de investigación, iniciando con el análisis de laboratorio, luego la
investigación por imágenes, estudios patológicos y exploración endoscópica.
2.2 DESCRIPCIÓN DEL MÉTODO
2.2.1. Análisis de Laboratorio Clínico
Biometría Hemática: Recuento de Glóbulos Rojos, glóbulos blancos, Hemoglobina,
hematocrito y Fórmula leucocitaria.
Marcadores Infecciosos: A las muestras del paciente se le realizan las pruebas para
descartar virus para HIV y CMV, como marcadores infecciosos.
Marcadores Reumatológicos: Se evalúa en el laboratorio el complejo de anticuerpos
ANA, anti-Ro, anti-DNA, anti-La, anti-SM, anti-RNP, como marcadores
reumatológicos, para descartar procesos inflamatorios de carácter autoinmune.
8
Marcadores Gastrointestinales: Se realiza la prueba de sangre oculta, no se realiza la
prueba de Helicobacter pylori porque ésta patología no suele producir fiebre. También
se realizan pruebas de Ac. Antigliadina IgA, Ac. Antigliadina IgG, Ac.
Antitransglutaminasa IgA, Ac. Antitransglutaminasa IgG, Ac. Endomisio IgA.
Marcadores Tumorales: Se revisan las células sanguíneas mediante frotis periférico y
se realizan pruebas complementarias de AFP y Gonadotrofina coriónica.
Otros: Examen de Orina, Cultivo de Sangre y Heces, Malaria.
2.2.2. Imagenología
Ecografía de abdomen: Se inicia un amplio estudio diagnóstico que inicialmente
incluye un examen de ultrasonido del abdomen.
Tomografía computarizada (TC): de tórax, abdomen y pelvis.
Resonancia Magnética: en pecho, abdomen y pelvis
2.2.3. Patología
Se realiza biopsia de muestras de: Ganglio linfático retroperitoneal, médula
ósea de ambas crestas iliacas, mucosa de esófago, estómago, duodeno, íleon y colon.
Tinciones de Inmunohistoquímica.
Hibridación de ARN de VEB
2.2.4 Exploración Endoscópica
Se realiza una endoscopía digestiva alta, una colonoscopía y una cápsula
endoscópica.
9
2.3 PREMISA
El paciente es ingresado al hospital e informa dolor de cabeza, náuseas, dolor
en la parte superior derecha del abdomen y en la pierna izquierda. Su temperatura es de
37.3°C y la piel se ve pálida. Además informa náuseas y diarrea ocasional. El paciente
es trasladado a otro hospital.
• Información brindada por el paciente: Náuseas, diarrea ocasional y dolor
abdominal.
• Exploración inicial: se recogen los siguientes datos:
Temperatura: 37,8°C, Estatura: 132 cm (1 ° percentil para su edad)
Peso: 26,8 kg (Percentil 1, el peso había disminuido en 1 kg <1 mes)
Masa corporal índice: 15,9 (el peso en kilogramos dividido por el cuadrado de la
estatura en metros).
Piel: pálida, tibia y seca
Abdomen: blando, sin dolor, y no hay hepatoesplenomegalia
Latidos Cardiacos: 123 latidos/seg
El resto del examen se presenta normal.
• Niveles sanguíneos de glucosa, calcio, GPT, fosfatasa alcalina y bilirrubinas total
y directa mantienen niveles normales, al igual que los resultados de las pruebas de
función renal.
• Evaluación del Servicio de Urgencias:
Tos leve, mialgias, fatiga en aumento desde hace 1 mes, mareos ocasionales durante
las 2 últimas semanas, constante dolor periumbilical.
Heces diarias de consistencia pastosa de coloración verdosa, de vez en cuando
mezclado con algo de sangre.
10
Ha sido saludable y sus vacunas están al día, con la excepción de una vacuna contra
la influenza.
No toma ningún medicamento, ni reporta alguna alergia conocida.
Es originario del Caribe, ha llegado a los Estados Unidos 4 años antes de la
manifestación de los síntomas, es estudiante, y vive con sus padres y hermanos.
Ha visitado la República Dominicana, incluyendo un pueblo rural, 3 meses antes
del ingreso.
No hay antecedentes familiares de enfermedad de células falciformes, anemia
hereditaria, enfermedad inflamatoria intestinal, o enfermedades autoinmunes.
• Examen físico:
El paciente está delgado y se ve más joven para su edad.
Signos vitales y saturación de oxígeno: normales.
La conjuntiva y la mucosa oral están pálidas.
No hay linfadenopatía periférica palpable.
El abdomen está distendido, con leve dolor a la palpación en los cuadrantes superior
derecho e inferior izquierdo.
Revisando el estado al ingreso del paciente, no se puede determinar cuál es la
causa probable de la enfermedad puesto que los síntomas que presenta, sugieren el
diagnóstico de una enfermedad leve. Por tal motivo, se necesita la información
complementaria para establecer las posibles causas de la enfermedad que inicialmente
podrían ser de origen infeccioso, reumatológico, gastrointestinal u oncológico.
11
2.4 DESCRIPCIÓN DE LAS UNIDADES DE ANÁLISIS
2.4.1 Análisis Químico Clínico
Los análisis de sangre sirven para determinar el estado fisiológico del paciente
midiendo las cantidades de ciertos tipos de células y químicos en la sangre y aunque
no se usan para diagnosticar linfoma, son de mucha ayuda a la hora de determinar el
grado de avance del mismo. Un recuento completo de células sanguíneas, es de mucha
importancia porque se puede determinar las diferentes células en la sangre, tales como
glóbulos rojos, los glóbulos blancos y las plaquetas. En pacientes que se sabe tienen
linfoma, los bajos recuentos de células sanguíneas pueden indicar que el linfoma está
creciendo en la médula ósea y está afectando la formación de nuevas células sanguíneas.
Además, de verificar la función renal y hepática, es importante medir los niveles de
DHL, un nivel elevado de L-lactato deshidrogenasa (LDH) predice esta complicación.
Para algunos tipos de linfoma, es recomendable realizar pruebas que
determinen si el paciente ha sido infectado con algún virus, el VIH, virus de Hepatitis
ya sean HAV, Hepatitis B o Hepatitis (HCV), porque su presencia podría afectar el
tratamiento. El virus de Epstein-Barr está implicado entre las causas del linfoma de
Hodgkin. Una gran proporción de pacientes de linfoma de Hodgkin presentan valores
altos de VEB; ello indica que un aumento en la activación del VEB puede preceder a la
presentación del linfoma de Hodgkin en algunos pacientes. Los pacientes con
antecedentes de mononucleosis infecciosa comprobada mediante serología tienen
cuatro veces más riesgo de presentar linfoma de Hodgkin positivo para VEB. (Instituto
Nacional del Cáncer , 2016)
12
Los marcadores inflamatorios PCR y Eritrosedimentación, suben y bajan de
manera diferente con la inflamación. La Proteína C Reactiva que sigue de cerca el
proceso inflamatorio subyacente, se eleva de forma aguda cuando el problema comienza
y se normaliza rápidamente cuando el problema está resuelto. La Eritrosedimentación
se eleva lentamente y se normaliza pocas semanas después de que se resuelve la
inflamación, ésta prueba es utilizada para monitorear el curso de enfermedades
inflamatorias.
A pesar de que sólo el 6% de todos los casos presentan fiebre de origen
desconocido, se debe descartar el cáncer, por lo tanto se realizan las pruebas de AFP y
Gonadotrofina coriónica
Se evalúa en el laboratorio el complejo de anticuerpos ANA, anti-Ro, anti-
DNA, anti-La, anti-SM, anti-RNP, como marcadores reumatológicos, para descartar
procesos inflamatorios de carácter autoinmune.
Las pruebas: Ac. Antigliadina IgA, Ac. Antigliadina IgG, Ac.
Antitransglutaminasa IgA, Ac. Antitransglutaminasa IgG, Ac. Endomisio IgA,se realizan
cuando hay sospecha de enfermedad celiaca. (López García, Osuna Molina, & Osuna
Molina, 2013) La prueba de sangre oculta se realiza en las heces para confirmar la
presencia de hematoquecia.
2.4.2 Imágenes
Ecografía de abdomen: La intención de esta prueba es investigar con prontitud
agrandamiento de órganos, un absceso o una masa oculta, y ganglios linfáticos
abdominales agrandados.
13
Tomografía computarizada (TC): Se realiza para comprobar la presencia de
linfadenopatías
Resonancia Magnética: Es un método para observar los grados de linfoma en
niños. Es una herramienta que ha demostrado ser muy útil para la evaluación temprana
de la enfermedad frente a un tratamiento.
2.4.3 Muestras para Patología
Se realiza la toma de muestras de tejidos para descubrir la presencia de células atípicas
y la Inmunohistoquímica para determinar la clase de Linfoma.
2.4.4 Endoscopía
Se realiza ésta exploración para determinar las causas de dolor abdominal y sangrado,
dependiendo del caso.
2.5 GESTIÓN DE DATOS
Corresponde al médico tratante, recopilar los datos, interpretarlos y establecer
el diagnóstico de la enfermedad.
2.6 CRITERIOS ÉTICOS DE LA INVESTIGACIÓN
El paciente de éste caso es un menor de edad, por lo tanto corresponde a sus
padres o tutores dar la aprobación para la publicación del mismo. No está implícita
dicha aprobación en el documento, aunque cabe destacar que no se violan los derechos
de confidencialidad y privacidad del paciente porque durante la exposición del caso no
se da el nombre ni otra característica que revele su identidad o la de sus familiares.
14
3. RESULTADOS
3.1 ANTECEDENTES DE LA UNIDAD DE ANÁLISIS
Se presenta el caso de un niño de 12 años que acude al hospital con malestar
general, fiebre, dolor abdominal, y palidez; una vez atendido, es sometido a varias
pruebas de laboratorio, de imágenes, patológicas y exploratorias, con la finalidad de
llegar a un diagnóstico definitivo.
3.2 PRESENTACIÓN DE RESULTADOS
Realizadas todas las pruebas de Laboratorio, Imágenes, Patológicas y
endoscópicas en el paciente se obtienen los siguientes resultados:
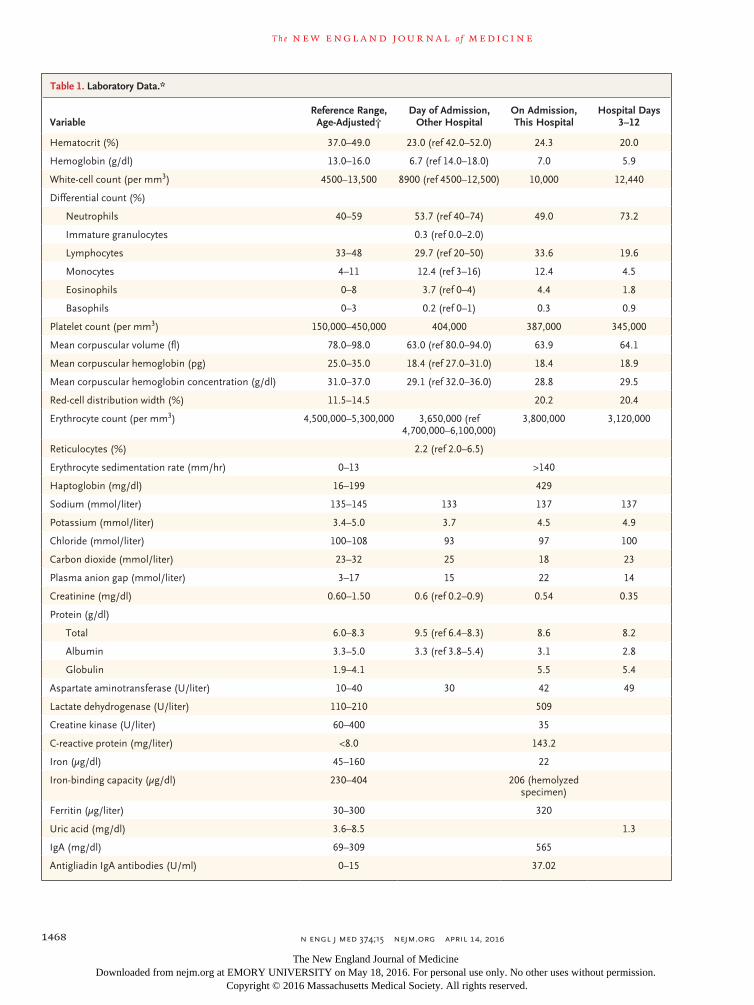
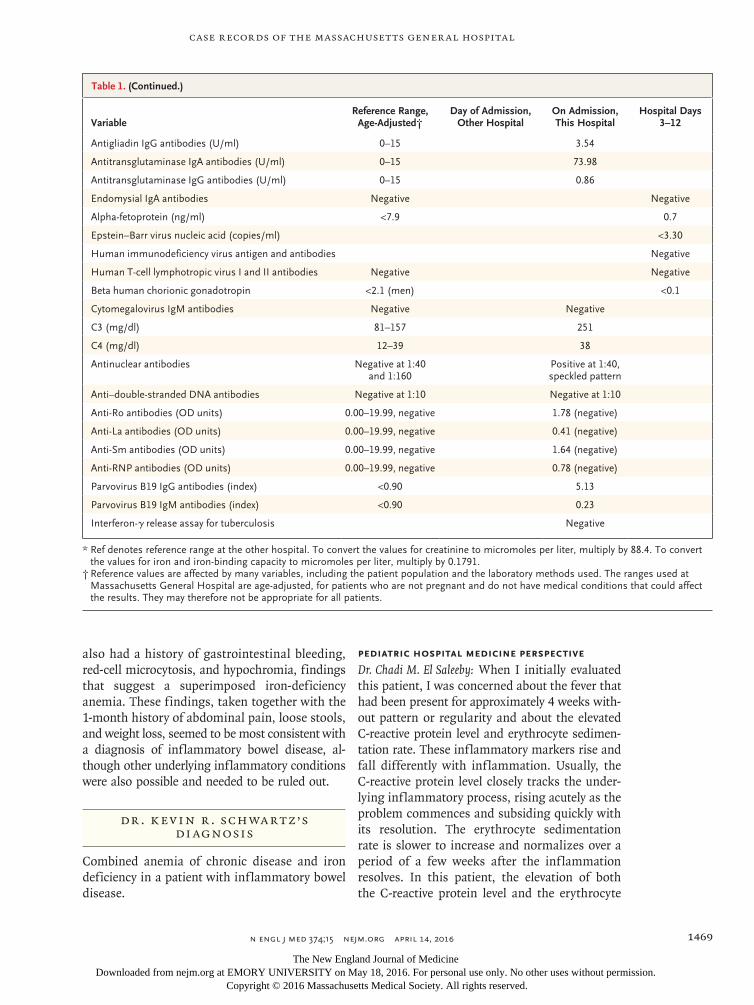
3.2.1 Resultados basados en el Laboratorio Clínico (Tabla 1)
Hemograma: En los resultados de las muestras tomadas antes, durante y en
días posteriores al ingreso es evidente la anemia, presentando niveles de Glóbulos rojos,
Hemoglobina y hematocrito bajos. La fórmula leucocitaria y el recuento de glóbulos
blancos inician con normalidad, pero en los días posteriores al ingreso muestran
resultados compatibles con una infección. Al observar las células sanguíneas no se
detecta la presencia de blastos.
Electrolitos: Niveles normales
PCR y Eritrosedimentación: ambos elevados lo que indica un proceso
subagudo en el momento.
HIV y CMV: Negativos.
Ac. ANA: Positivo 1:40 (patrón moteado)
Anti-Ro, anti-DNA, anti-La, anti-SM, anti-RNP: Negativos
15

TABLA 1. Datos de Laboratorio
VARIABLE UNIDADES RANGOS DE REFERENCIA AJUSTADOS A LA EDAD
ADMISIÓN 1ER HOSPITAL
ADMISIÓN HOSPITAL
DÍAS DE HOSPITALIZACÓN
(3 – 12)
Hematocrito % 37-49 23.0 24.3 20.0
Hemoglobina g/dl 13,0 -16,0 6,7 7 5,9
Leucocitos por mm3 4500 – 13,000 8,9 10 12,44
Formula Leucocitaria
Neutrófilos % 40 - 59 53,7 49 73,2
Linfocitos % 33 - 48 29,7 33,6 19,6
Monocitos % 04-nov 12,4 12,4 4,5
Eosinófilos % 0 – 8 3,7 4,4 1,8
Basófilos % 0 – 3 0,2 0,3 0,9
Plaquetas Por mm3 150,000 – 450,000 404 387 345
VCM ft 78,0 – 98,0 63 63,9 64,1
HCM pg 25,0 – 35,0 18,4 18,4 18,9
CHCM g/dl 31,0 – 37,0 29,1 28,8 29,5
Ancho de distrib. GR % 11,5 – 14,5 20,2 20,4
Glóbulos Rojos Por mm3 4,500,000 – 5,300,000 3,650,000 3,800,000 3,120,000
Reticulocitos % 2,0 – 6,5 2,2
Eritrosedimentación mm/h 0 -13 >140
Haptoglobina mg/dl 16 – 99 429
Sodio mmol/L 135 – 145 133 137 137
Potasio mmol/L 3,40 – 5,00 3,7 4,5 4,9
Cloro mmol/L 100 – 108 93 97 100
Reserva Alcalina mmol/L 23 – 32 25 18 23
Plasma Anion Gap mmol/L 3 – 17 15 22 14
Creatinina mg/dl 0,60 – 1,50 0,6 0,54 0,35
Proteínas g/dl
Total 6,0 – 8,3 9,5 8,6 8,2
Albúmina 3,3 – 5,0 3,3 3,1 2,8
Globulinas 1,9 – 4,1 5,5 5,4
GOT U/L 10 – 40 30 42 49
DHL U/L 110 – 210 509
CK U/L 60 – 400 35
Proteína C Reactiva mg/L <8,0 143,2
Hierro ug/dl 45 – 160 22
Capac. Fijación Hierro ug/dl 230 – 404 206 *
Ferritina L 30 – 300 320
Ácido úrico mg/dl 3,6 – 8,5 1,3
IgA mg/dl 69 – 309 565
16

Ac. antigliadina IgA U/ml 0 – 15 37,02
Ac. antigliadina IgG U/ml 0 – 15 3,54
Ac. Antitransglutaminasa IgA U/ml 0 – 15 73,98
Ac. Antitransglutaminasa IgG U/ml 0 – 15 0,86
Ac. Endomisio IgA Negativo Negativo
Alfafetoproteína ng/ml <7,9 0,7
Virus de Epstein – Barr copias/ml <3,30
HIV Negativo Negativo
Virus linfotrópico de células T
Gonadotrofina coriónica <2,1 <0,1
Ac. CMV IgM Negativo Negativo
C3 mg/dl 81 – 157 251
C4 mg/dl dic-39 38
Ac. Antinucleares Pos 1:40
Ac anti-DNA Neg 1:10
Ac. Anti-Ro OD 0,00 - 19,99 1,78
Ac. Anti-La OD 0,00 - 19,100 0,41
Ac. Anti-Sm OD 0,00 - 19,101 1,64
Ac. Anti-RNP OD 0,00 - 19,102 0,78
Ac. Parvovirus B19 IgM <0,90 5,13
Ac. Parvovirus B19 IgG <0,91 0,23
Ac. Parvovirus B19 IgG Negativo
Prueba de Sangre Oculta en Heces: Negativo, no confirman la hematoquecia
reportada.
Ac. Antigliadina IgA, Ac. Antigliadina IgG, Ac. Antitransglutaminasa IgA,
Ac. Antitransglutaminasa IgG, Ac. Endomisio IgA: Resultado positivo en la
primera toma de muestra.
AFP y Gonadotrofina coriónica: Negativos.
17

3.2.2 Resultados basados en las Imágenes
Ecografía de abdomen: revela agrandamiento de múltiples ganglios
retroperitoneales y mesentéricos y las paredes de las asas del intestino delgado
engrosadas en la parte media del abdomen.
Tomografía computarizada (TC): de tórax, abdomen y pelvis se comprueban las
linfadenopatías paratraqueal, subcarinal, en el hilio, paravertebral, retroperitoneal
mesentérica así como una lesión hipodensa en el hígado y el engrosamiento en la
pared de las asas del intestino delgado.
Resonancia Magnética: revela extensa linfadenopatía en el pecho, el abdomen y la
pelvis. Intensa fijación de la sustancia en las paredes engrosadas del intestino, al
igual que una intensa captación en el lado derecho del hígado. No hay captación
anormal en el bazo.
3.2.3 Resultados basados en el Estudio Patológico
Biopsia de muestras de:
Ganglio linfático retroperitoneal: presenta
Células atípicas: Las células atípicas tienen las características de las células de
Hodgkin y células de Reed-Sternberg.
Tinciones de inmunohistoquímica: las células dieron resultados fuertemente
positivos para CD30 y débilmente para CD15
Resultado: Linfoma de Hodgkin clásico, consistente con celularidad mixta.
Médula ósea de ambas crestas ilíacas: Presenta hematopoyesis normal, no hay
evidencia de linfoma.
Mucosa del esófago, estómago, duodeno, íleon y colon: negativas para linfoma.
18
Estómago: muestra evidencia de gastritis crónica con agregados linfoides y muy
pocas bacterias de H. pylori.
Hibridación de ARN de VEB: Positivo
3.2.4 Resultados de la Exploración Endoscópica
Endoscopia digestiva alta, una colonoscopia y una cápsula endoscópica: No
muestra evidencia de hemorragia gastrointestinal reciente. La cápsula endoscópica
no muestra hallazgos consistentes con la enfermedad celíaca.
19

4. DISCUSIÓN
4.1 CONTRASTACIÓN EMPÍRICA
El paciente del caso en estudio se ha sometido a varias pruebas para detectar la
enfermedad que le provoca los síntomas, el primer hallazgo en la Biometría Hemática
es una anemia microcítica clínicamente significativa; como causa de ésta alteración
debe considerarse: la deficiencia de hierro, anemia por enfermedad crónica, talasemia o
envenenamiento por plomo. De acuerdo a los datos, el paciente no tiene antecedentes
de envenenamiento por plomo, su antecedente étnico y bajo recuento de glóbulos rojos,
no respaldan un diagnóstico de talasemia; por lo tanto, las causas se reducen a la
deficiencia de hierro, una anemia por enfermedad crónica, o ambos.
La deficiencia de hierro es la causa más común de anemia. Los pacientes
afectados clásicamente se presentan con un bajo volumen corpuscular medio, bajo nivel
de hemoglobina corpuscular media, alta amplitud de distribución de glóbulos rojos, e
hipocromía; todos estos hallazgos de laboratorio se observaron en este paciente. El nivel
de ferritina en suero es un indicador sensible y específico de deficiencia de hierro,
puesto que constituye el principal depósito de hierro en los tejidos orgánicos; aunque,
en un paciente con inflamación aguda, este nivel suele elevarse, como es el caso de éste
paciente en que está marcadamente elevado, al igual que los marcadores inflamatorios,
como el nivel de proteína C reactiva y la eritrosedimentación; de acuerdo con esto es
probable que el paciente presente anemia por enfermedad crónica.
20

La anemia por enfermedad crónica (Medicina Interna Basada en la
evidencia, 2015) puede ser el resultado de cualquier condición que se asocia con una
respuesta inflamatoria; sin embargo, un volumen corpuscular medio de menos de 70 fl
e hipocromía clínicamente significativa, rara vez se asocian con la anemia de
enfermedad crónica, pueden existir otras causas. Los marcadores inflamatorios
Proteína C Reactiva y la Eritrosedimentación se muestran elevados lo que indica un
proceso subagudo en el momento. (Arthritis Foundation, 2014)
De todas las entidades que causan la fiebre de origen desconocido, la infección
representa aproximadamente el 50% de casos, por lo tanto no se puede descartar las
infecciones de periodos de incubación largos como amebiasis, hepatitis y malaria, pero
de acuerdo a los niveles bajos de las enzimas del paciente y el resultado negativo para
malaria, se descartan ambas patologías. Tampoco se puede descartar antecedentes de
otros tipos de infección como el HIV en el que se ha podido establecer una estrecha
relación con la aparición de linfoma gastrointestinal. Los virus juegan un papel
importante en la patogénesis de los linfomas asociados al HIV, así como en alteraciones
asociadas a la infección por el VEB, los pacientes con infección por HIV y LNH se
presentan habitualmente con enfermedad avanzada y/o extraganglionar al momento del
diagnóstico en aproximadamente 80% de los casos, en general, los linfomas asociados
con la infección por HIV tienen un comportamiento biológico agresivo y rápidamente
fatal sin embargo, el diagnóstico temprano y el tratamiento adecuado para ambas
condiciones han mejorado significativamente el pronóstico de estos pacientes. (Avilés
Salas, Herrera Goepfert, Aguilar León, Candelaria Hernánde, & Martínez Cordero,
2011)
21
Las pruebas relacionadas con la enfermedad Celiaca como son: Ac.
Antigliadina IgA, Ac. Antigliadina IgG, Ac. Antitransglutaminasa IgA, Ac.
Antitransglutaminasa IgG, Ac. Endomisio IgA, dan un resultado positivo, pero éstos
resultados no son considerados concluyentes debido a que la enfermedad celiaca no se
manifiesta con fiebre. (Vivas Alegre & Santolaria Piedrafita, 2011)
A pesar de que sólo el 6% de todos los casos presentan fiebre de origen
desconocido, se debe descartar el cáncer. La leucemia es poco probable, porque en la
fórmula leucocitaria no se observan blastos, y la anemia parece ser un fenómeno
secundario.
Las imágenes muestran linfadenopatía que asociada con engrosamiento de la
pared intestinal presentan características compatibles con linfoma, el compromiso
extranodal (que se ve en este caso) por lo general se asocia con el linfoma no Hodgkin,
la afectación ganglionar y el bazo se asocian con un diagnóstico de linfoma de Hodgkin.
Además, en pacientes con linfoma de Hodgkin, la participación de intestino es poco
común y enfermedades hepáticas casi siempre se asocian con enfermedad esplénica.
Una confluencia de linfáticos agrandados que encierran vasos mesentéricos, que se
observa en este caso, es una característica común en el linfoma abdominal. (Ghimire,
Wu, & Zhu, 2011)
4.2 LIMITACIONES
El estudio no muestra limitaciones durante la evaluación, los analistas y
tratantes del caso mantienen comunicación constante sobre los resultados del paciente,
presentando sus puntos de vista desde diferentes áreas y haciendo uso de los recursos
disponibles para llegar a la resolución del caso.
22

4.3 LÍNEAS DE INVESTIGACIÓN
La etiología en la mayoría de los linfomas es desconocida, pero hoy se conoce
su origen viral. Se citan diferentes tipos de agentes virales en su etiología, como el virus
de Epstein-Barr, el virus del Sida, y el virus HTLV-1, entre otros. El linfoma gástrico
está, a menudo, ocasionado por la bacteria Helicobacter pylori. También, dentro de los
factores etiológicos, están las inmunodeficiencias, el uso de inmunosupresores que se
emplean en el trasplante de órganos (enfermedad linfoproliferativa postrasplante) y la
afectación por ciertos productos químicos como pesticidas, alimentos, disolventes o
fertilizantes. (Verdecia Cañizares, Santos Labarcena, & Lam Díaz, 2015)
Se reconoce que no existen métodos efectivos disponibles para reconocer a los
pacientes con riesgo de Linfoma. Actualmente los pacientes se identifican cuando
desarrollan linfadenopatías o síntomas extranodales asociados a la enfermedad.
(Sistema Nacional de Salud, 2011)
4.4 ASPECTOS NOVEDOSOS DEL ESTUDIO DE CASO
El caso presentado demuestra que la literatura médica no es definitiva, al
momento de la exploración médica, una de las características es la presencia de
linfadenopatías, sin embargo el paciente de éste caso no las presenta, con los resultados
de imágenes se puede establecer la presencia de linfoma por los engrosamientos
presentes en el intestino, aun así, no se puede establecer la tipología del linfoma puesto
que la ubicación extranodal del mismo lo categorizan en el tipo No Hodgkin, finalmente
es el resultado inmunohistoquímico el que revela el diagnóstico definitivo de Linfoma
de Hodgkin clásico, subtipo celularidad mixta, por lo tanto la ambigüedad presente en
el caso constituye un evento para resaltar.
23

5. PROPUESTA
En la mayoría de los casos en que el paciente presenta fiebre, el diagnóstico
apunta hacia una infección, en casos en que la etiología de una enfermedad se
desconoce, es necesario descartar las causas probables de la fiebre y proponer un
tratamiento rápido. Durante el desarrollo del caso, se consideró en el paciente la
probabilidad de que haya sido infectado por el virus de Epstein-Barr, sin embargo la
decisión de realizar una prueba que determine la existencia de la misma fue durante la
biopsia, es decir, una toma de muestra de tipo invasiva y por el método de “Hibridación
in situ” que alarga el tiempo de espera, si bien es cierto que por su alta sensibilidad ésta
técnica es más recomendada para el diagnóstico histológico, no se deben descartar los
métodos serológicos que aportan con resultados confiables y en corto tiempo.
24
CONCLUSIONES
De los resultados obtenidos en el presente caso de estudio de un paciente con
12 años de edad con malestar general, fiebre, dolor abdominal, y palidez, se concluye
que:
Salvo marcadas excepciones, es necesario realizar varias pruebas en el
laboratorio para delimitar las posibles causas de una patología.
Un solo análisis no es concluyente a la hora de tomar decisiones, se necesitan
otras técnicas que respalden el diagnóstico final.
El linfoma es una patología que de acuerdo a varios estudios está asociada a un
antecedente de infección por virus de Epstein Barr.
De acuerdo al caso presentado, los hallazgos en los estudios de imagen y la
evaluación patológica, determinan que el paciente presenta linfoma de Hodgkin
en estadio IV.
Aunque el hígado, el bazo y los ganglios linfáticos intraabdominales a menudo
están involucrados en el linfoma de Hodgkin etapa avanzada, cierto compromiso
del tracto gastrointestinal es bastante raro.
RECOMENDACIONES
Utilizar métodos serológicos para virus de Epstein Barr, con menor tiempo de
espera y resultados efectivos.
Comparar la eficacia de los resultados obtenidos con pruebas serológicas vs los
resultados obtenidos por hibridación in situ.
Establecer relación tiempo de espera vs eficacia de resultados.
25
REFERENCIAS BIBLIOGRÁFICAS
American Cancer Society. (29 de Febrero de 2016). Factores de Riesgo de
Linfoma de Hodgkin. Obtenido de www.cancer. org
Arthritis Foundation. (26 de Septiembre de 2014). Análisis de Sangre.
Obtenido de PCR y VSG: http://espanol.arthritis.org
Avilés Salas, A., Herrera Goepfert, R., Aguilar León, D., Candelaria Hernánde,
M., & Martínez Cordero, E. C. (22 de Diciembre de 2011). Linfomas plasmoblásticos
del tracto gastrointestinal en pacientes con sida. Obtenido de Scielo: www.scielo.org.ar
Gersten, T. (1 de 2 de 2016). Medline Plus. Obtenido de Medline Plus:
https://medlineplus.gov
Ghimire, P., Wu, G.-Y., & Zhu, L. (14 de Febrero de 2011). World Journal
Gastroenterology. Obtenido de Primary gastrointestinal lymphoma:
http://www.ncbi.nlm.nih.gov
IBL Internacional. (20 de Enero de 2012). Instrucciones de Uso. Epstein Barr
Virus EBNA-1 IgM Elisa. Obtenido de http://www.ibl-international.com
Instituto Nacional del Cáncer . (27 de Abril de 2016). Instituto Nacional del
Cáncer. Obtenido de Linfoma de Hodgkin infantil: Tratamiento : www.cancer.gov
Instituto Nacional del Cáncer. (27 de Abril de 2016). Linfoma de Hodgkin
Infantil. Obtenido de www.cancer.gov
Leukemia & Lymphoma Society. (01 de 01 de 2014). La Guía sobre el
Linfoma. Obtenido de www.lls.org
López García, M. J., Osuna Molina, A., & Osuna Molina, R. (2013).
Enfermedades Gastrointestinales. En M. J. López García, A. Osuna Molina, & R. Osuna
26
Molina, Manual de laboratorio en las Enfermedades Autoinmunes Digestivas (págs.
19-20). Andalucía: OmniaScience (Omnia Publisher SL).
Lynphoma Research Fundation. (15 de Junio de 2011). Obteniendo los Datos.
Obtenido de Linfoma de Hodgkin: www.lymphoma.org
Medicina Interna Basada en la evidencia. (18 de Junio de 2015). Medicina
Interna Basada en la Evidencia. Obtenido de Anemia en enfermedades crónicas:
http://empendium.com
Ministerio de Salud y Protección Social - Colciencias. (30 de Abril de 2013).
Guía de Práctica Clínica para la detección oportuna, diagnóstico, tratamiento y
seguimiento de Linfoma de Hodgkin y Linfoma No Hodgkin en niños y adolescentes.
Obtenido de Guía de Práctica Clínica: http://gpc.minsalud.gov.co
Natgeo, R. (23 de 09 de 2015). National Geographic en español. Obtenido de
National Geographic en Español: www.ngenespanol.com
Pavlosky, A. (2014). Tratamiento del Linfoma de Hodgkin adaptado al
resultado del PET. Evidencias actuales y perspectivas futuras. Hematología Vol 18, 234-
238.
Pinheiro, P. (30 de Noviembre de 2015). MD. SAUDE . Obtenido de Linfoma
de Hodgkin y Linfoma No Hodgkin: www.saude.com
Rangel Vega, A., Villano Castillejos, J. C., López facio, E. E., Covarrubias
Espinoza, G., & Rendón García, H. (2013). Linfomas en Pediatría. Abordaje Clínico.
Experiencia en el Hospital Infantil del Estado de Sonora. HES, 42-47.
Roche Diagnostics. (09 de Enero de 2012). VENTANA. Obtenido de INFORM
EBER (Epstein-Barr Virus Early RNA) Probe : www.ventana.com
Rueda, A. (16 de Marzo de 2015). SEOM. Obtenido de Linfoma de Hodgkin:
www.seom.org
27
Sistema Nacional de Salud. (20 de 07 de 2011). Guía de Prácticas Clínicas.
Detección oportuna y Diagnóstico del Linfoma No Hodking en edad Pediátrica.
México, DF., México, México: Centro Nacional de Excelencia Tecnológica en Salud.
Verdecia Cañizares, C., Santos Labarcena, M. E., & Lam Díaz, R. M. (1 de
Diciembre de 2015). Comportamiento del linfoma no Hodgkin en la edad pediátrica.
Obtenido de Scielo: http://scielo.sld.cu
Vivas Alegre, S., & Santolaria Piedrafita, S. (2011). Sección III. Capítulo 23.
Enfermedad Celiaca. En A. e. Gastroenterología, Manual de Tratamiento de las
Enfermedades Gastroenterológicas (págs. 265-278). Madrid: Asociación Española de
Gastroenterología.
28

n engl j med 374;15 nejm.org April 14, 20161466
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
Pr esen tation of C a se
Dr. Katherine L. Tuttle (Pediatrics): A 12-year-old boy was admitted to this hospital because of malaise, fevers, abdominal pain, and worsening pallor.
The patient had been well until 1 month before admission, when headache and abdominal pain developed. Examination by a school nurse revealed a temperature of 38.6°C and pale skin. A diagnosis of a viral illness was made, and follow-up with his pediatrician was recommended. When the patient was reexamined by the nurse 4 days later, the temperature was normal. The skin was pale, the pharynx was slightly erythematous, and the abdomen was tender. At follow-up visits with the school nurse 10 and 6 days before admission, the patient reported persistent upper abdominal pain; the temperature was 38.6°C at both visits.
On the day of admission, the patient reported headache, nausea, and pain in the right upper abdomen and left leg. The temperature was 37.3°C, and the skin ap-peared to be more pale. He was taken by ambulance to the emergency department of another hospital, where he reported nausea, occasional diarrhea, and abdomi-nal pain. On examination, he appeared mildly ill. The temperature was 37.8°C, the blood pressure 92/58 mm Hg, the pulse 123 beats per minute, the respiratory rate 18 breaths per minute, and the oxygen saturation 98% while he was breathing ambient air. The height was 132 cm (1st percentile for his age), the weight 26.8 kg (1st percentile; the weight had decreased 1 kg in <1 month), and the body-mass index (the weight in kilograms divided by the square of the height in meters) 15.4 (9th percentile). The skin was pale, warm, and dry. The abdomen was soft and non-tender, and there was no hepatosplenomegaly; the remainder of the examination was normal. Blood levels of glucose, calcium, alanine aminotransferase, alkaline phosphatase, and total and direct bilirubin were normal, as were results of renal-function tests; other test results are shown in Table 1. Normal saline, acetamino-phen, and oxygen (through a nasal cannula at a rate of 2 liters per minute) were administered; the tachycardia resolved. The patient was transferred by ambulance to this hospital.
On evaluation in the emergency department, the patient reported a mild cough,
From the Departments of Pediatrics (K.R.S., C.M.E.S., A.M.F., A.M.), Radiolo‑gy (K.N.), and Pathology (L.R.Z.), Massa‑chusetts General Hospital, and the De‑partments of Pediatrics (K.R.S., C.M.E.S., A.M.F., A.M.), Radiology (K.N.), and Pa‑thology (L.R.Z.), Harvard Medical School — both in Boston.
N Engl J Med 2016;374:1466-76.DOI: 10.1056/NEJMcpc1512458Copyright © 2016 Massachusetts Medical Society.
Founded by Richard C. Cabot Eric S. Rosenberg, M.D., Editor Nancy Lee Harris, M.D., Editor Jo‑Anne O. Shepard, M.D., Associate Editor Alice M. Cort, M.D., Associate Editor Sally H. Ebeling, Assistant Editor Emily K. McDonald, Assistant Editor
Case 11-2016: A 12-Year-Old Boy with Malaise, Fevers, Abdominal Pain, and Pallor
Kevin R. Schwartz, M.D., Chadi M. El Saleeby, M.D., Katherine Nimkin, M.D., Alison M. Friedmann, M.D., Aeri Moon, M.D., and Lawrence R. Zukerberg, M.D.
Case Records of the Massachusetts General Hospital
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

n engl j med 374;15 nejm.org April 14, 2016 1467
Case Records of the Massachusetts Gener al Hospital
myalgias, fatigue that had been worsening for 1 month, and occasional dizziness during the pre-vious 2 weeks. He also reported nearly constant periumbilical pain that occasionally radiated to the left lower quadrant; he described the pain as “squeezing” and rated it at up to 7 on a scale of 0 to 10 (with 10 indicating the most severe pain). He had daily loose stools that were green, with occasional blood mixed in and on the toilet pa-per, but he had no increased bruising or bleeding when he brushed his teeth. He had been previ-ously healthy and his immunizations were re-portedly current, with the exception of a sea-sonal influenza vaccine. He took no medications and had no known allergies. He had been born in the Caribbean, had come to the United States 4 years earlier, was a student, and lived with his parents and two siblings. He had visited the Dominican Republic, including a rural village, 3 months before admission; he had not taken malaria prophylaxis. He had pet fish and no expo-sures to animals or sick contacts. There was no family history of sickle cell disease, other heredi-tary anemia, inflammatory bowel disease, or autoimmune diseases.
On examination, the patient was thin and ap-peared younger than his age. The vital signs and oxygen saturation (while he was breathing ambi-ent air) were normal. The conjunctiva and oral mucosa were pale. There was no palpable periph-eral lymphadenopathy. The abdomen was distend-ed, with mild tenderness on palpation in the right upper and left lower quadrants; there were ecchymoses on the shins, and the remainder of the examination was normal. A stool specimen showed no occult blood. Blood levels of glucose, phosphorus, magnesium, calcium, alkaline phos-phatase, alanine aminotransferase, and total and direct bilirubin were normal, as were results of renal-function tests. Other test results are shown in Table 1.
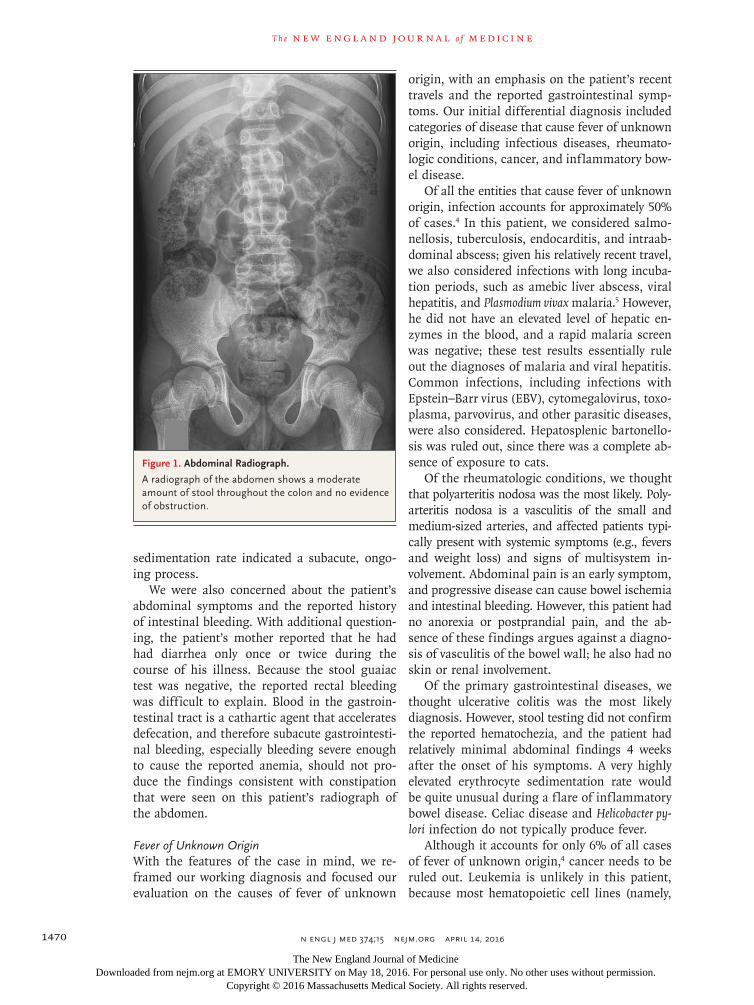
Dr. Katherine Nimkin: A radiograph of the abdo-men (Fig. 1) showed a moderate amount of fecal matter in the colon and no dilated bowel loops, free air, or skeletal abnormality.
Dr. Tuttle: Urinalysis revealed 1+ urobilinogen. Blood and stool specimens were sent for culture. Screening of blood specimens for malaria–specific antigens was negative and for cold agglutinins was nonreactive at a dilution of 1:16. The patient was admitted to the hospital, and additional di-agnostic tests were performed.
Differ en ti a l Di agnosis
Emergency Department Perspective
Dr. Kevin R. Schwartz: All the discussants were in-volved in the care of this child and are aware of the diagnosis. This 12-year-old boy presented with a 1-month history of intermittent and poorly localized abdominal pain, loose stools with oc-casional hematochezia, intermittent fevers, weight loss of 1 kg, and anemia. My initial differential diagnosis included infectious, rheumatologic, gas-trointestinal, and oncologic causes, but when the patient was in the emergency department, I fo-cused my workup on the finding of profound anemia.
AnemiaThe patient had clinically significant microcytic anemia. Causes of microcytic anemia include iron deficiency, anemia of chronic disease, thalassemia, and lead poisoning.1 The patient had no history of lead poisoning, and his ethnic background, high red-cell distribution width, and low red-cell count did not support a diagnosis of thalassemia. Thus, we narrowed our differential diagnosis to include iron deficiency, anemia of chronic disease, or both.
Iron deficiency is the most common cause of anemia. Affected patients classically present with a low mean corpuscular volume, low mean cor-puscular hemoglobin level, high red-cell distribu-tion width, and hypochromia; all these labora-tory findings were noted in this patient. The serum ferritin level is the most sensitive and specific in-dicator of iron deficiency.2 However, in a patient with acute inflammation, interpretation of the ferritin level can be challenging, since it is an acute-phase reactant. This patient’s ferritin level was markedly elevated, as were other inflamma-tory markers, including the C-reactive protein level and erythrocyte sedimentation rate; these findings suggest that anemia of chronic disease is most likely contributing to his anemia.
Anemia of chronic disease can result from any condition that is associated with an inflam-matory response; however, a mean corpuscular volume of less than 70 fl and clinically signifi-cant hypochromia are rarely associated with iso-lated anemia of chronic disease,3 and these find-ings prompted us to consider other underlying causes to explain this patient’s illness. Although he had evidence of anemia of chronic disease, he
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
n engl j med 374;15 nejm.org April 14, 20161468
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
VariableReference Range,
Age-Adjusted†Day of Admission,
Other HospitalOn Admission, This Hospital
Hospital Days 3–12
Hematocrit (%) 37.0–49.0 23.0 (ref 42.0–52.0) 24.3 20.0
Hemoglobin (g/dl) 13.0–16.0 6.7 (ref 14.0–18.0) 7.0 5.9
White‑cell count (per mm3) 4500–13,500 8900 (ref 4500–12,500) 10,000 12,440
Differential count (%)
Neutrophils 40–59 53.7 (ref 40–74) 49.0 73.2
Immature granulocytes 0.3 (ref 0.0–2.0)
Lymphocytes 33–48 29.7 (ref 20–50) 33.6 19.6
Monocytes 4–11 12.4 (ref 3–16) 12.4 4.5
Eosinophils 0–8 3.7 (ref 0–4) 4.4 1.8
Basophils 0–3 0.2 (ref 0–1) 0.3 0.9
Platelet count (per mm3) 150,000–450,000 404,000 387,000 345,000
Mean corpuscular volume (fl) 78.0–98.0 63.0 (ref 80.0–94.0) 63.9 64.1
Mean corpuscular hemoglobin (pg) 25.0–35.0 18.4 (ref 27.0–31.0) 18.4 18.9
Mean corpuscular hemoglobin concentration (g/dl) 31.0–37.0 29.1 (ref 32.0–36.0) 28.8 29.5
Red‑cell distribution width (%) 11.5–14.5 20.2 20.4
Erythrocyte count (per mm3) 4,500,000–5,300,000 3,650,000 (ref 4,700,000–6,100,000)
3,800,000 3,120,000
Reticulocytes (%) 2.2 (ref 2.0–6.5)
Erythrocyte sedimentation rate (mm/hr) 0–13 >140
Haptoglobin (mg/dl) 16–199 429
Sodium (mmol/liter) 135–145 133 137 137
Potassium (mmol/liter) 3.4–5.0 3.7 4.5 4.9
Chloride (mmol/liter) 100–108 93 97 100
Carbon dioxide (mmol/liter) 23–32 25 18 23
Plasma anion gap (mmol/liter) 3–17 15 22 14
Creatinine (mg/dl) 0.60–1.50 0.6 (ref 0.2–0.9) 0.54 0.35
Protein (g/dl)
Total 6.0–8.3 9.5 (ref 6.4–8.3) 8.6 8.2
Albumin 3.3–5.0 3.3 (ref 3.8–5.4) 3.1 2.8
Globulin 1.9–4.1 5.5 5.4
Aspartate aminotransferase (U/liter) 10–40 30 42 49
Lactate dehydrogenase (U/liter) 110–210 509
Creatine kinase (U/liter) 60–400 35
C‑reactive protein (mg/liter) <8.0 143.2
Iron (μg/dl) 45–160 22
Iron‑binding capacity (μg/dl) 230–404 206 (hemolyzed specimen)
Ferritin (μg/liter) 30–300 320
Uric acid (mg/dl) 3.6–8.5 1.3
IgA (mg/dl) 69–309 565
Antigliadin IgA antibodies (U/ml) 0–15 37.02
Table 1. Laboratory Data.*
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
n engl j med 374;15 nejm.org April 14, 2016 1469
Case Records of the Massachusetts Gener al Hospital
also had a history of gastrointestinal bleeding, red-cell microcytosis, and hypochromia, findings that suggest a superimposed iron-deficiency anemia. These findings, taken together with the 1-month history of abdominal pain, loose stools, and weight loss, seemed to be most consistent with a diagnosis of inflammatory bowel disease, al-though other underlying inflammatory conditions were also possible and needed to be ruled out.
Dr . K e v in R . Sch wa rt z’s Di agnosis
Combined anemia of chronic disease and iron deficiency in a patient with inflammatory bowel disease.
Pediatric Hospital Medicine PerspectiveDr. Chadi M. El Saleeby: When I initially evaluated this patient, I was concerned about the fever that had been present for approximately 4 weeks with-out pattern or regularity and about the elevated C-reactive protein level and erythrocyte sedimen-tation rate. These inflammatory markers rise and fall differently with inflammation. Usually, the C-reactive protein level closely tracks the under-lying inflammatory process, rising acutely as the problem commences and subsiding quickly with its resolution. The erythrocyte sedimentation rate is slower to increase and normalizes over a period of a few weeks after the inflammation resolves. In this patient, the elevation of both the C-reactive protein level and the erythrocyte
VariableReference Range,
Age-Adjusted†Day of Admission,
Other HospitalOn Admission, This Hospital
Hospital Days 3–12
Antigliadin IgG antibodies (U/ml) 0–15 3.54
Antitransglutaminase IgA antibodies (U/ml) 0–15 73.98
Antitransglutaminase IgG antibodies (U/ml) 0–15 0.86
Endomysial IgA antibodies Negative Negative
Alpha‑fetoprotein (ng/ml) <7.9 0.7
Epstein–Barr virus nucleic acid (copies/ml) <3.30
Human immunodeficiency virus antigen and antibodies Negative
Human T‑cell lymphotropic virus I and II antibodies Negative Negative
Beta human chorionic gonadotropin <2.1 (men) <0.1
Cytomegalovirus IgM antibodies Negative Negative
C3 (mg/dl) 81–157 251
C4 (mg/dl) 12–39 38
Antinuclear antibodies Negative at 1:40 and 1:160
Positive at 1:40, speckled pattern
Anti–double‑stranded DNA antibodies Negative at 1:10 Negative at 1:10
Anti‑Ro antibodies (OD units) 0.00–19.99, negative 1.78 (negative)
Anti‑La antibodies (OD units) 0.00–19.99, negative 0.41 (negative)
Anti‑Sm antibodies (OD units) 0.00–19.99, negative 1.64 (negative)
Anti‑RNP antibodies (OD units) 0.00–19.99, negative 0.78 (negative)
Parvovirus B19 IgG antibodies (index) <0.90 5.13
Parvovirus B19 IgM antibodies (index) <0.90 0.23
Interferon‑γ release assay for tuberculosis Negative
* Ref denotes reference range at the other hospital. To convert the values for creatinine to micromoles per liter, multiply by 88.4. To convert the values for iron and iron‑binding capacity to micromoles per liter, multiply by 0.1791.
† Reference values are affected by many variables, including the patient population and the laboratory methods used. The ranges used at Massachusetts General Hospital are age‑adjusted, for patients who are not pregnant and do not have medical conditions that could affect the results. They may therefore not be appropriate for all patients.
Table 1. (Continued.)
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
n engl j med 374;15 nejm.org April 14, 20161470
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
sedimentation rate indicated a subacute, ongo-ing process.
We were also concerned about the patient’s abdominal symptoms and the reported history of intestinal bleeding. With additional question-ing, the patient’s mother reported that he had had diarrhea only once or twice during the course of his illness. Because the stool guaiac test was negative, the reported rectal bleeding was difficult to explain. Blood in the gastroin-testinal tract is a cathartic agent that accelerates defecation, and therefore subacute gastrointesti-nal bleeding, especially bleeding severe enough to cause the reported anemia, should not pro-duce the findings consistent with constipation that were seen on this patient’s radiograph of the abdomen.
Fever of Unknown OriginWith the features of the case in mind, we re-framed our working diagnosis and focused our evaluation on the causes of fever of unknown
origin, with an emphasis on the patient’s recent travels and the reported gastrointestinal symp-toms. Our initial differential diagnosis included categories of disease that cause fever of unknown origin, including infectious diseases, rheumato-logic conditions, cancer, and inflammatory bow-el disease.
Of all the entities that cause fever of unknown origin, infection accounts for approximately 50% of cases.4 In this patient, we considered salmo-nellosis, tuberculosis, endocarditis, and intraab-dominal abscess; given his relatively recent travel, we also considered infections with long incuba-tion periods, such as amebic liver abscess, viral hepatitis, and Plasmodium vivax malaria.5 However, he did not have an elevated level of hepatic en-zymes in the blood, and a rapid malaria screen was negative; these test results essentially rule out the diagnoses of malaria and viral hepatitis. Common infections, including infections with Epstein–Barr virus (EBV), cytomegalovirus, toxo-plasma, parvovirus, and other parasitic diseases, were also considered. Hepatosplenic bartonello-sis was ruled out, since there was a complete ab-sence of exposure to cats.
Of the rheumatologic conditions, we thought that polyarteritis nodosa was the most likely. Poly-arteritis nodosa is a vasculitis of the small and medium-sized arteries, and affected patients typi-cally present with systemic symptoms (e.g., fevers and weight loss) and signs of multisystem in-volvement. Abdominal pain is an early symptom, and progressive disease can cause bowel ischemia and intestinal bleeding. However, this patient had no anorexia or postprandial pain, and the ab-sence of these findings argues against a diagno-sis of vasculitis of the bowel wall; he also had no skin or renal involvement.
Of the primary gastrointestinal diseases, we thought ulcerative colitis was the most likely diagnosis. However, stool testing did not confirm the reported hematochezia, and the patient had relatively minimal abdominal findings 4 weeks after the onset of his symptoms. A very highly elevated erythrocyte sedimentation rate would be quite unusual during a flare of inflammatory bowel disease. Celiac disease and Helicobacter py-lori infection do not typically produce fever.
Although it accounts for only 6% of all cases of fever of unknown origin,4 cancer needs to be ruled out. Leukemia is unlikely in this patient, because most hematopoietic cell lines (namely,
Figure 1. Abdominal Radiograph.
A radiograph of the abdomen shows a moderate amount of stool throughout the colon and no evidence of obstruction.
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

n engl j med 374;15 nejm.org April 14, 2016 1471
Case Records of the Massachusetts Gener al Hospital
white cells and platelets) were preserved, no blasts were noted on a peripheral-blood smear, and the anemia seemed to be a secondary phe-nomenon. Other possibilities include lymphoma or solid tumors (e.g., neuroblastoma), but the clinical examination did not reveal intraabdomi-nal masses or enlarged lymph nodes.
After my first evaluation of this patient, I did not have a firm sense of direction. Salmonello-sis, endocarditis, extrapulmonary tuberculosis, an intraabdominal abscess, and polyarteritis nodosa were at the top of my differential diagnosis. We therefore began a broad workup that initially in-cluded an ultrasound examination of the abdomen. The intention of this testing was to promptly in-vestigate for organ enlargement, an occult ab-scess or a mass, and enlarged abdominal lymph nodes.
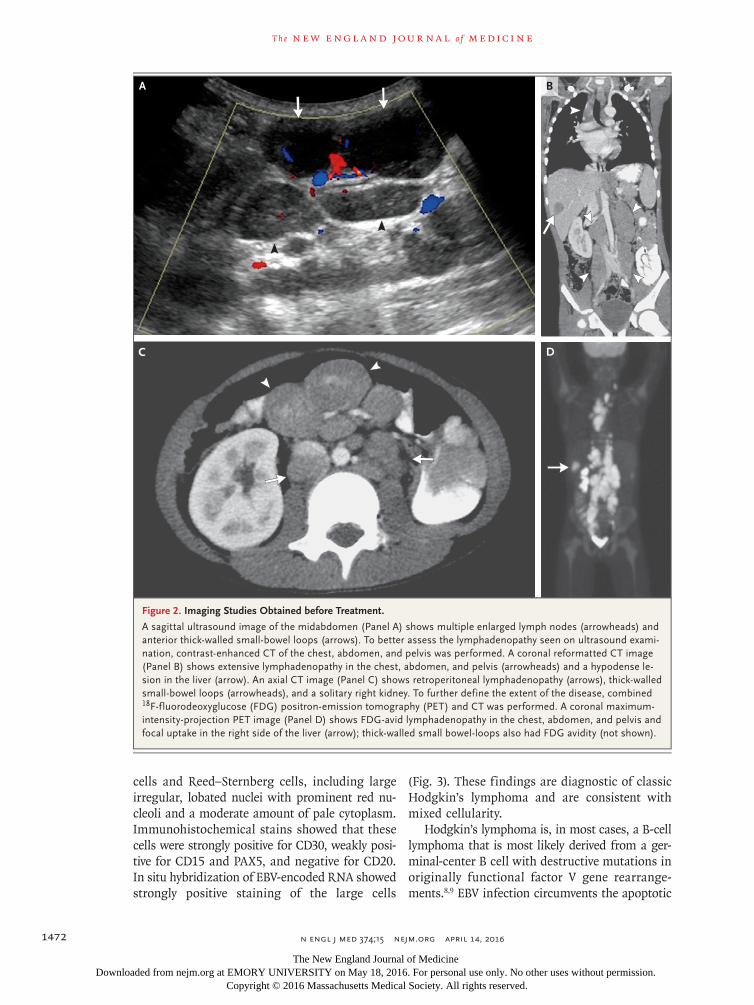
Dr. Nimkin: The abdominal ultrasound exami-nation (Fig. 2A) revealed multiple enlarged ret-roperitoneal and mesenteric lymph nodes and thick-walled small-bowel loops in the anterior midabdomen. A 2-cm hypoechoic lesion was pres-ent in the liver, and the solitary right kidney had mild hydronephrosis.
Subsequent computed tomography (CT) of the chest, abdomen, and pelvis (Fig. 2B and 2C), performed after the administration of intravenous and oral contrast material, revealed paratracheal, subcarinal, right hilar, and paravertebral lymph-adenopathy, as well as a hypodense lesion in the liver and extensive retrocrural, retroperitoneal, and mesenteric lymphadenopathy. Thick-walled small-bowel loops were also present.
The differential diagnosis of lymphadenopa-thy associated with bowel-wall thickening includes lymphoma, particularly non-Hodgkin’s lymphoma. Other gastrointestinal cancers in children are very rare. Infection, particularly tuberculosis, is also a consideration; however, in patients with tuber-culosis, lymph nodes are usually hypodense and have peripheral enhancement. Patients with in-flammatory bowel disease can also have these findings on CT; however, the lymphadenopathy is rarely as extensive as it was in this case. On rare occasions, patients with connective-tissue disor-ders or sarcoidosis may have extensive abdominal lymphadenopathy, but these disorders are uncom-mon in this patient’s age group. Patients with Henoch–Schönlein purpura or celiac disease typi-cally have fewer and smaller lymph nodes than those seen in this patient. Benign lymphoprolif-
erative diseases, such as Rosai–Dorfman disease, Kikuchi–Fujimoto disease, and Castleman’s dis-ease, are rare but are also considerations in this patient.
Given the broad differential diagnosis, we next performed combined 18F-fluorodeoxyglucose (FDG) positron-emission tomography and CT (PET-CT), which revealed extensive FDG-avid lymphadenopa-thy in the chest, abdomen, and pelvis (Fig. 2D). Intense uptake associated with the thick-walled small-bowel loops was present, as was a focus of intense uptake on the right side of the liver. No abnormal uptake was present in the spleen. These findings are consistent with stage IV lymphoma.
PET-CT is the primary method for the staging of lymphoma in children.6 Nodal and splenic in-volvement is associated with a diagnosis of Hodg-kin’s lymphoma, whereas extranodal involve-ment (which was seen in this case) is usually associated with non-Hodgkin’s lymphoma. Fur-thermore, in patients with Hodgkin’s lymphoma, bowel involvement is rare and hepatic disease is almost always associated with splenic disease. A confluence of enlarged nodes encasing mesen-teric vessels, which was seen in this case, is a common feature in abdominal lymphoma and has been described as the “sandwich sign.”7
Dr. El Saleeby: After I reviewed the findings on the imaging studies, lymphoma appeared to be the most likely diagnosis. I also thought tubercu-losis needed to be ruled out, although this diag-nosis was much less likely. In order to establish the diagnosis in this case, we asked the interven-tional radiology service to perform a CT-guided retroperitoneal lymph-node biopsy.
Dr . Ch a di M. El S a leeby ’s Di agnosis
Probable lymphoma involving the small bowel, abdominal lymph nodes, and liver, with associated anemia of chronic disease and iron deficiency; less likely intraabdominal tuberculosis.
Pathol o gic a l Discussion
Dr. Lawrence R. Zukerberg (Pathology): Examination of a core-needle biopsy specimen of a retroperito-neal lymph node showed replacement of the tissue by a mixed infiltrate composed of small lympho-cytes, histiocytes, eosinophils, and large atypical cells. The atypical cells had features of Hodgkin’s
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.
n engl j med 374;15 nejm.org April 14, 20161472
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
cells and Reed–Sternberg cells, including large irregular, lobated nuclei with prominent red nu-cleoli and a moderate amount of pale cytoplasm. Immunohistochemical stains showed that these cells were strongly positive for CD30, weakly posi-tive for CD15 and PAX5, and negative for CD20. In situ hybridization of EBV-encoded RNA showed strongly positive staining of the large cells
(Fig. 3). These findings are diagnostic of classic Hodgkin’s lymphoma and are consistent with mixed cellularity.
Hodgkin’s lymphoma is, in most cases, a B-cell lymphoma that is most likely derived from a ger-minal-center B cell with destructive mutations in originally functional factor V gene rearrange-ments.8,9 EBV infection circumvents the apoptotic
Figure 2. Imaging Studies Obtained before Treatment.
A sagittal ultrasound image of the midabdomen (Panel A) shows multiple enlarged lymph nodes (arrowheads) and anterior thick‑walled small‑bowel loops (arrows). To better assess the lymphadenopathy seen on ultrasound exami‑nation, contrast‑enhanced CT of the chest, abdomen, and pelvis was performed. A coronal reformatted CT image (Panel B) shows extensive lymphadenopathy in the chest, abdomen, and pelvis (arrowheads) and a hypodense le‑sion in the liver (arrow). An axial CT image (Panel C) shows retroperitoneal lymphadenopathy (arrows), thick‑walled small‑bowel loops (arrowheads), and a solitary right kidney. To further define the extent of the disease, combined 18F‑fluorodeoxyglucose (FDG) positron‑emission tomography (PET) and CT was performed. A coronal maximum‑intensity‑projection PET image (Panel D) shows FDG‑avid lymphadenopathy in the chest, abdomen, and pelvis and focal uptake in the right side of the liver (arrow); thick‑walled small bowel‑loops also had FDG avidity (not shown).
A B
DC
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

n engl j med 374;15 nejm.org April 14, 2016 1473
Case Records of the Massachusetts Gener al Hospital
pathway, which should otherwise be activated in B cells that lack a functional immunoglobulin gene. EBV infection occurs in 10 to 70% of patients with classic Hodgkin’s lymphoma, depending on sub-type; a very high percentage of these patients have
the mixed-cellularity subtype of Hodgkin’s lym-phoma and are children (such as this patient) or elderly, have immunosuppression, or are from resource-poor settings.
In this patient, examination of bone marrow–
Figure 3. Retroperitoneal Lymph Node–Biopsy Specimen.
Hematoxylin and eosin staining of the lymph node–biopsy specimen (Panels A and B) shows that the tissue is replaced by a mixed cellular infiltrate containing eosinophils, lymphocytes, histiocytes, and scattered large cells (Panel A), which are seen better at higher magnification (Panel B, arrows). Immunohistochemical staining of the large cells shows strong staining for CD30 (Panel C), weak granular staining for CD15 (Panel D), and faint nuclear staining for PAX5 (Panel E); in situ hybridization with the use of Epstein–Barr virus–encoded RNA shows strong nuclear staining (Panel F). Admixed granulocytes show strong staining for CD15 (Panel D), and B lymphocytes show strong staining for PAX5 (Panel E).
A B
DC
FE
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

n engl j med 374;15 nejm.org April 14, 20161474
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
biopsy specimens from both iliac crests showed normal hematopoiesis and no evidence of lym-phoma. Because the findings on imaging studies suggested intestinal-wall involvement, mucosal biopsies of the esophagus, stomach, duodenum, ileum, and colon were performed; the specimens were negative for lymphoma. The duodenum showed normal villous architecture but also showed a fo-cally increased number of intraepithelial lympho-cytes, a finding that is not specific and can be seen with gluten sensitivity, infection, Crohn’s disease, H. pylori gastritis, and a variety of other causes. Examination of the stomach-biopsy speci-men showed evidence of chronic gastritis with lymphoid aggregates and very few H. pylori bac-teria, features that most likely account for the findings seen in the duodenum.
Discussion of M a nagemen t
Oncology Perspective
Dr. Alison M. Friedmann: On the basis of the find-ings on imaging studies and the pathological evaluation, we determined that this patient had stage IV Hodgkin’s lymphoma with extensive su-pradiaphragmatic and infradiaphragmatic lymph-adenopathy and liver involvement. It was not clear whether the Hodgkin’s lymphoma involved the gastrointestinal tract, but the abnormalities in the abdomen on imaging studies were quite striking.
Although the liver, spleen, and intraabdomi-nal lymph nodes are often involved in advanced-stage Hodgkin’s lymphoma, true involvement of the gastrointestinal tract is quite rare. Only iso-lated cases are reported in the medical litera-ture10,11; these reports indicate that the stomach is the most common site, followed by the small and large intestines and finally the esophagus. Given the rarity of involvement of the gastroin-testinal tract, this patient’s possible history of gastrointestinal bleeding, and the markedly ab-normal findings on PET-CT, we consulted with the gastroenterology service to evaluate the gas-trointestinal tract before initiating treatment for Hodgkin’s lymphoma, since it would be impor-tant to identify other serious gastrointestinal conditions that might influence the child’s treat-ment course.
Gastroenterology Perspective
Dr. Aeri Moon: The pediatric gastroenterology ser-vice was asked to see this patient, who presented
with abdominal pain, nausea, poor growth, inter-mittent rectal bleeding, and iron-deficiency ane-mia. We performed an upper endoscopy, a colo-noscopy, and a capsule endoscopy; these studies showed no evidence of recent gastrointestinal bleeding. However, since the patient’s last re-ported episode of rectal bleeding was approxi-mately 2 weeks before the admission, the timing of the capsule endoscopy may not have been optimal to identify a source of bleeding; the di-agnostic yield is much higher when the endos-copy is performed closer to the time of overt obscure gastrointestinal bleeding.12
Although initial serologic testing for celiac disease was positive, findings on examination of the duodenal-biopsy specimen were nonspecific, including normal villous architecture with in-creased intraepithelial lymphocytes, a finding seen in approximately 10 to 20% of patients with celiac disease.13 Capsule endoscopy showed no findings supportive of celiac disease. Therefore, it is not clear whether this patient has celiac disease.
It is interesting to note that the risk of non-Hodgkin’s lymphoma among patients with celi-ac disease is 2 to 3 times as high as the risk among those without celiac disease,14 and the risk is higher among patients who receive a diag-nosis of celiac disease when they are older than 50 years of age. In view of the young age of this patient and the diagnosis of Hodgkin’s lympho-ma, I believe the positive serologic testing for celiac disease is unrelated to his current presen-tation. We repeated the testing 8 months later, and it was negative. Although the negative result could be attributable to immunosuppression af-ter chemotherapy, the total level of IgA antibod-ies at the time was normal. The next step would be to repeat the serologic testing for celiac disease, and if that is positive, to perform genetic testing for celiac disease.
Finally, examination of the gastric-biopsy speci-men showed evidence of H. pylori gastritis, which may be associated with extranodal marginal-zone lymphoma in adults, but I believe it is not related to this patient’s diagnosis of Hodgkin’s lymphoma. The infection was treated with antibiotic agents and omeprazole.
Oncology Perspective
Dr. Friedmann: We invited the patient to partici-pate in a St. Jude Children’s Research Hospital clinical trial for pediatric Hodgkin’s lymphoma
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

n engl j med 374;15 nejm.org April 14, 2016 1475
Case Records of the Massachusetts Gener al Hospital
(ClinicalTrials.gov number, NCT01920932) that is examining the substitution of brentuximab vedotin for vincristine in the regimen of OEPA (vincristine, etoposide, prednisone, and doxoru-bicin) followed by COPDac (cyclophosphamide, vincristine, prednisone, and dacarbazine) that was developed by the German Society of Pediatric On-cology and Hematology (GPOH).15 Brentuximab vedotin is a monoclonal antibody that is linked to a toxin directed against CD30 and has substan-tial activity in Hodgkin’s lymphoma.16 The family chose not to participate, and we therefore chose to administer the standard OEPA–COPDac regi-men.15 After two cycles of OEPA, a PET scan showed that the patient had had a complete re-sponse (Fig. 4). He then received four cycles of COPDac. We did not administer radiation therapy, given the results of a Children’s Oncology Group Study that investigated the role of radiation ther-apy in patients with intermediate-risk Hodgkin’s lymphoma.17 In this trial, patients with stage IB to IVA disease and a rapid early response to treatment were randomly assigned to either receive or not receive radiation therapy. There was no difference between the two groups in treatment outcome.
The patient completed his treatment 9 months ago (15 months after he received his diagnosis). He is currently doing well and is in complete remission. His gastrointestinal bleeding did not recur after treatment started, and his anemia re-solved over the course of his treatment.
Dr. Nancy L. Harris (Pathology): It is uncommon to have liver disease without splenic involvement in classic Hodgkin’s lymphoma (according to the study on laparotomy by Kadin et al.18). Is it possible that the normal-sized spleen nonetheless had mi-croscopic involvement?
Dr. Nimkin: Microscopic involvement of the spleen should have been detected on the PET scan, which did not show increased FDG avidity in the spleen.
Dr. Friedmann: I agree that this finding is un-usual, but it is just one of many unusual features of this case.
Dr. Harris: Dr. Moon, could the initial positive serologic testing for celiac disease have been part of an autoimmune component of this patient’s Hodgkin’s lymphoma? Patients with Hodgkin’s lymphoma can have autoimmune cytopenias, but I have never heard of associated positive serologic testing for celiac disease.
Dr. Moon: The presence of antitransglutamin-
ase IgA antibodies is not specific for celiac disease but rather is a general phenomenon related to mucosal lesions. Both the expression of trans-glutaminase and the production of antitransglu-taminase IgA antibodies may be related to apop-tosis that results from mucosal damage and scarring in celiac disease but also in other intes-tinal disorders, such as inflammatory bowel disease.19 I think it is unlikely that this patient has celiac disease, although repeat testing would be reasonable.
A nat omic a l Di agnosis
Mixed-cellularity subtype of classic Hodgkin’s lym-phoma and Epstein–Barr virus infection.
This case was presented at Pediatric Grand Rounds.No potential conflict of interest relevant to this article was
reported.
Figure 4. FDG-PET Scan Obtained after Treatment.
A coronal maximum‑intensity‑projection PET image shows that the patient had a complete response; a sol‑itary right kidney is visible (arrow).
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.

n engl j med 374;15 nejm.org April 14, 20161476
Case Records of the Massachusetts Gener al Hospital
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
We thank Dr. Stephanie Ruest (Pediatrics) and the Pediatric Grand Rounds Committee for assistance with organizing the conference.
References1. Lanzkowsky L. Manual of pediatric hematology and oncology. 5th ed. Lon-don: Academic Press, 2011.2. Camaschella C. Iron-deficiency ane-mia. N Engl J Med 2015; 372: 1832-43.3. Weiss G, Goodnough LT. Anemia of chronic disease. N Engl J Med 2005; 352: 1011-23.4. Chow A, Robinson JL. Fever of un-known origin in children: a systematic review. World J Pediatr 2011; 7: 5-10.5. Wilson ME. Fever in returned travel-ers. Atlanta: Centers for Disease Control and Prevention, 2015 (http://wwwnc .cdc .gov/ travel/ yellowbook/ 2016/ post-travel -evaluation/ fever-in-returned-travelers).6. Kluge R, Kurch L, Montravers F, Mauz-Körholz C. FDG PET/CT in children and adolescents with lymphoma. Pediatr Radiol 2013; 43: 406-17.7. Toma P, Granata C, Rossi A, Gara-venta A. Multimodality imaging of Hodg-kin disease and non-Hodgkin lymphomas in children. Radiographics 2007; 27: 1335-54.8. Kanzler H, Küppers R, Hansmann ML, Rajewsky K. Hodgkin and Reed-Sternberg cells in Hodgkin’s disease rep-resent the outgrowth of a dominant tumor clone derived from (crippled) germinal
center B cells. J Exp Med 1996; 184: 1495-505.9. Massini G, Siemer D, Hohaus S. EBV in Hodgkin lymphoma. Mediterr J Hema-tol Infect Dis 2009; 1(2): e2009013.10. Gandhi JS, Mehta A, Sharma A, Kam-boj M. Primary Hodgkin lymphoma of the ileum. J Cancer Res Ther 2010; 6: 342-3.11. Jones K, Pacella J, Wasty F. Hodgkin’s disease of the oesophagus: a literature re-view. Australas Radiol 2007; 51: 489-91.12. Singh A, Marshall C, Chaudhuri B, et al. Timing of video capsule endoscopy relative to overt obscure GI bleeding: im-plications from a retrospective study. Gastrointest Endosc 2013; 77: 761-6.13. Kakar S, Nehra V, Murray JA, Day-harsh GA, Burgart LJ. Significance of in-traepithelial lymphocytosis in small bow-el biopsy samples with normal mucosal architecture. Am J Gastroenterol 2003; 98: 2027-33.14. Elfström P, Granath F, Ekström Smedby K, et al. Risk of lymphoprolifera-tive malignancy in relation to small intes-tinal histopathology among patients with celiac disease. J Natl Cancer Inst 2011; 103: 436-44.15. Mauz-Körholz C, Hasenclever D, Dörffel W, et al. Procarbazine-free OEPA-
COPDAC chemotherapy in boys and stan-dard OPPA-COPP in girls have comparable effectiveness in pediatric Hodgkin’s lym-phoma: the GPOH-HD-2002 study. J Clin Oncol 2010; 28: 3680-6.16. Younes A, Gopal AK, Smith SE, et al. Results of a pivotal phase II study of bren-tuximab vedotin for patients with re-lapsed or refractory Hodgkin’s lympho-ma. J Clin Oncol 2012; 30: 2183-9.17. Friedman DL, Chen L, Wolden S, et al. Dose-intensive response-based chemo-therapy and radiation therapy for children and adolescents with newly diagnosed intermediate-risk Hodgkin lymphoma: a report from the Children’s Oncology Group Study AHOD0031. J Clin Oncol 2014; 32: 3651-8.18. Kadin ME, Glatstein E, Dorfman RF. Clinicopathologic studies of 117 untreat-ed patients subjected to laparotomy for the staging of Hodgkin’s disease. Cancer 1971; 27: 1277-94.19. Farrace MG, Picarelli A, Di Tola M, et al. Presence of anti-“tissue” transgluta-minase antibodies in inflammatory intes-tinal diseases: an apoptosis-associated event? Cell Death Differ 2001; 8: 767-70.Copyright © 2016 Massachusetts Medical Society.
LANTERN SLIDES UPDATED: COMPLETE POWERPOINT SLIDE SETS FROM THE CLINICOPATHOLOGICAL CONFERENCES
Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a teaching exercise or reference material is now eligible to receive a complete set of PowerPoint slides, including digital images, with identifying legends, shown at the live Clinicopathological Conference (CPC) that is the basis of the Case Record. This slide set contains all of the images from the CPC, not only those published in the Journal. Radiographic, neurologic, and cardiac studies, gross specimens, and photomicrographs, as well as unpublished text slides, tables, and diagrams, are included. Every year 40 sets are produced, averaging 50-60 slides per set. Each set is supplied on a compact disc and is mailed to coincide with the publication of the Case Record.
The cost of an annual subscription is $600, or individual sets may be purchased for $50 each. Application forms for the current subscription year, which began in January, may be obtained from the Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974) or e-mail [email protected].
The New England Journal of Medicine Downloaded from nejm.org at EMORY UNIVERSITY on May 18, 2016. For personal use only. No other uses without permission.
Copyright © 2016 Massachusetts Medical Society. All rights reserved.


















