
Àcid úric i progressió de la malaltia renal - socane.cat · Efectos de hiperuricemia sobre el...
66
Àcid úric i progressió de la malaltia renal José Luño Hospital General Universitario Gregorio Marañon
Transcript of Àcid úric i progressió de la malaltia renal - socane.cat · Efectos de hiperuricemia sobre el...

Àcid úric i progressió de la malaltia renal
José Luño Hospital General Universitario
Gregorio Marañon

Homeostasis del ácido úrico
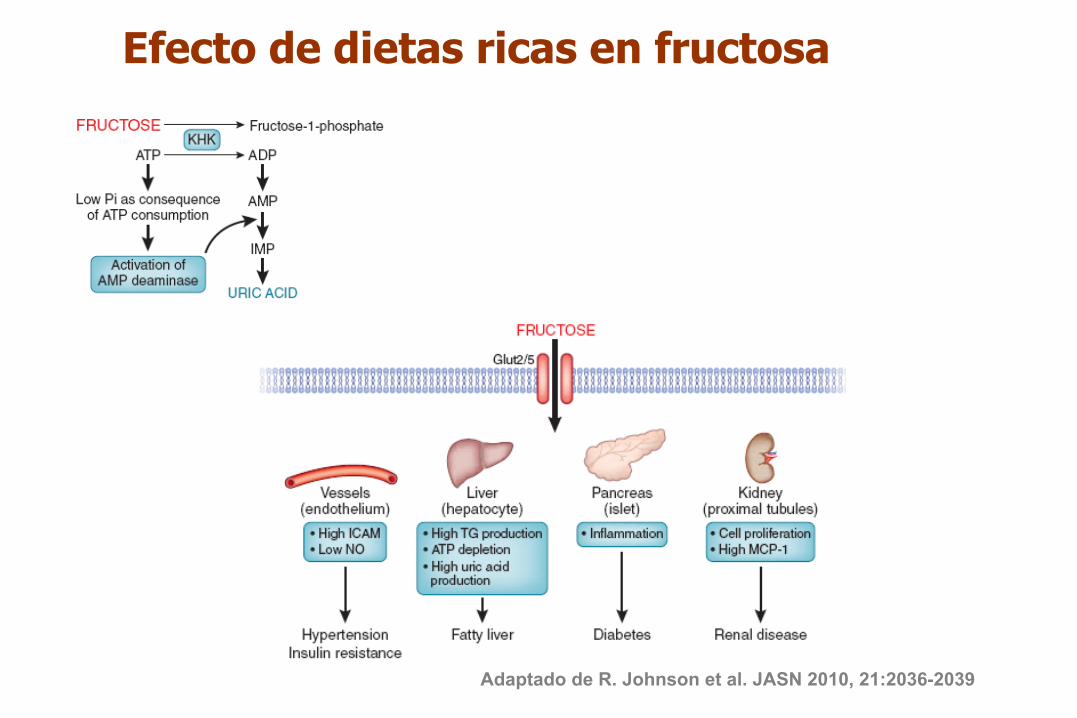
Efecto de dietas ricas en fructosa
Adaptado de R. Johnson et al. JASN 2010, 21:2036-2039

Arterial Hypertension Metabolic Syndrome Obstructive sleep apnea Syndrome Vascular Disease (coronary and carotid) Cerebrovascular disease and vascular dementia Preeclampsia Inflammatory biomarkers (hs- CRP, PAI-1, ..) Endothelial Dysfunction Oxydative Stress Renal Disease Progression
Uric Acid and Cardiovascular Risk Daniel I. Feig, Duk-Hee Kang, and Richard J. Johnson, M.D. NEJM 2008
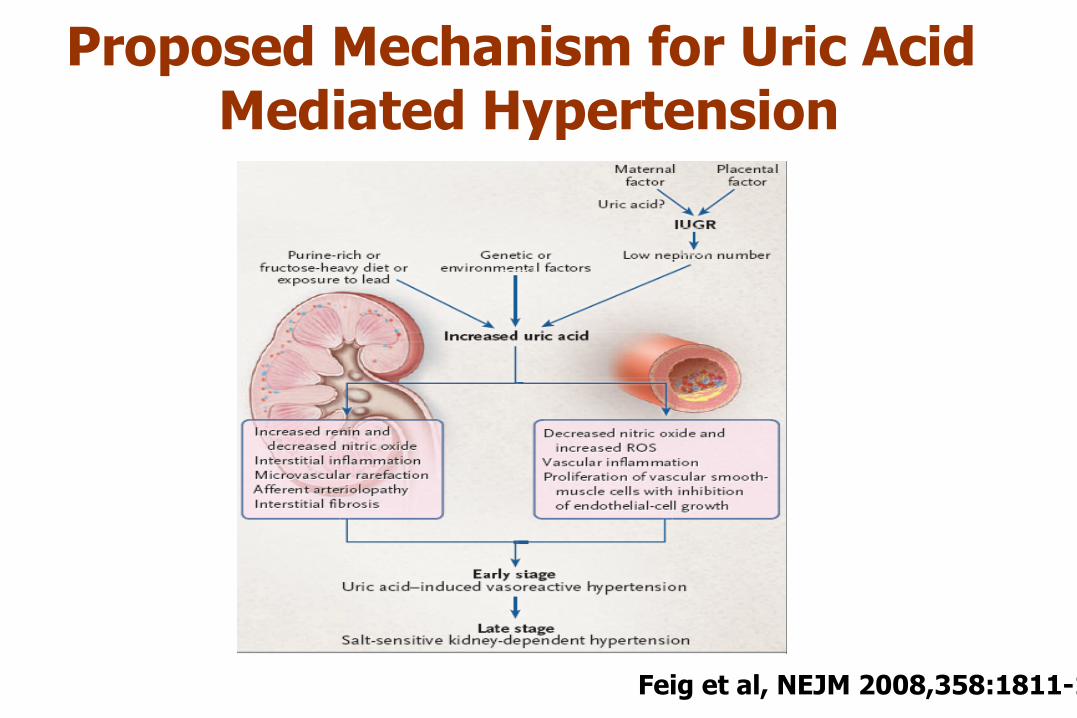
Proposed Mechanism for Uric Acid Mediated Hypertension
Feig et al, NEJM 2008,358:1811-1821

Ugtwo "Wtke"Cekf "Rtgf kevu"J { r gtvgpukqpStudy Population RelativeRisk
IsraeliHeartStudy(Khan,1972) 10,000males 2‐ foldriskat5YRS
KaiserPermanente(Selby,1990) 2,062subjects 2‐foldriskat6YRS
UnivofUtah(Hunt,1991) 1482adults 2‐foldriskat7YRS
OlivettiHeartStudy(Jossa,1994) 619males 2‐foldriskat12YRS
CARDIAstudy(Dyer,1999) 5115adults 2‐foldriskat10YRS
OsakaHealthSurvey(Taniguchi,2001) 6,356males 2‐foldriskat10YRS
Hawaii‐LosAngeles‐HiroshimaStudy(Imazu,2001) 140males 3.5‐foldriskat15YR
OsakaFactoryStudy(Masuo,2003) 433males 1.0mg/dlUApredicts_27mmHgat5YR
OsakaHealthSurvey(Nakanishi,2003) 2310males 1.6‐ foldriskat6YRS
Okinawa(Nagahama,2004) 4489adults 1.7‐foldriskat13YRSBogalusaHeart(Alper,2005) 679children Increasedriskat11yearsFramingham(Sündstrom,2005) 3329adults 1.6‐foldat4yesrsNormativeAgingStudy(Perlstein,2006) 2062males 1.5‐foldat21YRS
MRFIT(Krishnan,2007) 3073men 1.8‐foldat6YRS
ARIC(Mellen,2006) 9,104adults 1.5‐foldat9YRS
NurseHealthStudy(Forman,2009) 1500women 1.89foldat5years
HealthProfessionalFollowup(Forman,2007) 750men 1.08‐foldat8YRS*(Notsignificant)
The overall risk for incident hypertension increased 13% per 1 mg/dl increase in serum uric acid level

Uric Acid Level and Elevated Blood Pressure in US Adolescents (NHANES, 1999–2006)
Lauren F. Loeffler. Hypertension. 2012; 59:811-817.

Serum Uric Acid in Adolescents with Hypertension
• 125 consecutive referrals involved with
hypertension • After hypertension work-up the diagnosis
were; • Primary hypertension: 50% (n=63) • Secondary hypertension: 32% (n=40) • White-coat hypertension: 18% (n=22)
Feig and Johnson. Hypertension (2003) Feig and Johnson, Hypertension 42:247-252, 2003

1
9
8
7
6
5
4
3
2 Seru
m U
ric A
cid
(mg/
dl)
Primary Hypertension
N=63 Mean = 6.7mg/dl
Secondary Hypertension
N=39 Mean = 4.3 mg/dl
White Coat Hypertension
N=22 Mean = 3.5 mg/dl
Controls
N=41 Mean = 3.6mg/dl
Serum Uric Acid in Adolescents with Hypertension
Feig and Johnson, Hypertension 42:247-252, 2003
6.7
4.3 3.5 3.6

Age 15.1±2.1 yrs % Male 60% Weight 97±23 kg BMI 33±6.5 kg/m2
Race White 46% Hispanic 23% African American 31%
Uric Acid 6.9±1.2mg/dL Feig et al, JAMA 2008 Aug 27;300(8):924-32
Effect of allopurinol vs placebo in newly diagnosed hypertension in adolescents.
A Randomized, double-blind, placebo-controlled, crossover trial

Lowering Uric Acid Reduces SBP in Adolescents with Hypertension
In Subjects whose Uric acid was reduced to < 5 mg/dl, 86% (19/22) became normotensive versus 3% (1/30) controls

Risk of cardiovascular events for hyperuricemia
Gagliardi AC et al, Atherosclerosis 2009; 202:11-17
Letho et al
Hoieggen et al(LIFE)
Hozawa et al (ARIC)
Bos et al (Rotterdam)
1.93 (1.30-2.86)
0.91 (0.83-0.99)
1.22 (1.11-1.35)
1.17 (1.06-1.28) 1.00 (0.99-1.01) 1.49 (1.00-2.23) (stroke,no diuréticos)
1.68 (1.24-2.23) 1.11 (1.08-1.115)
RR (IC 95%)
Krishan et al
Fang et al (NHANES I) Alderman et al Culleton et al
3 1 0.1 Risk Ratio
Strasak et al (Austriaco) 1.51 (1.03-2.22)
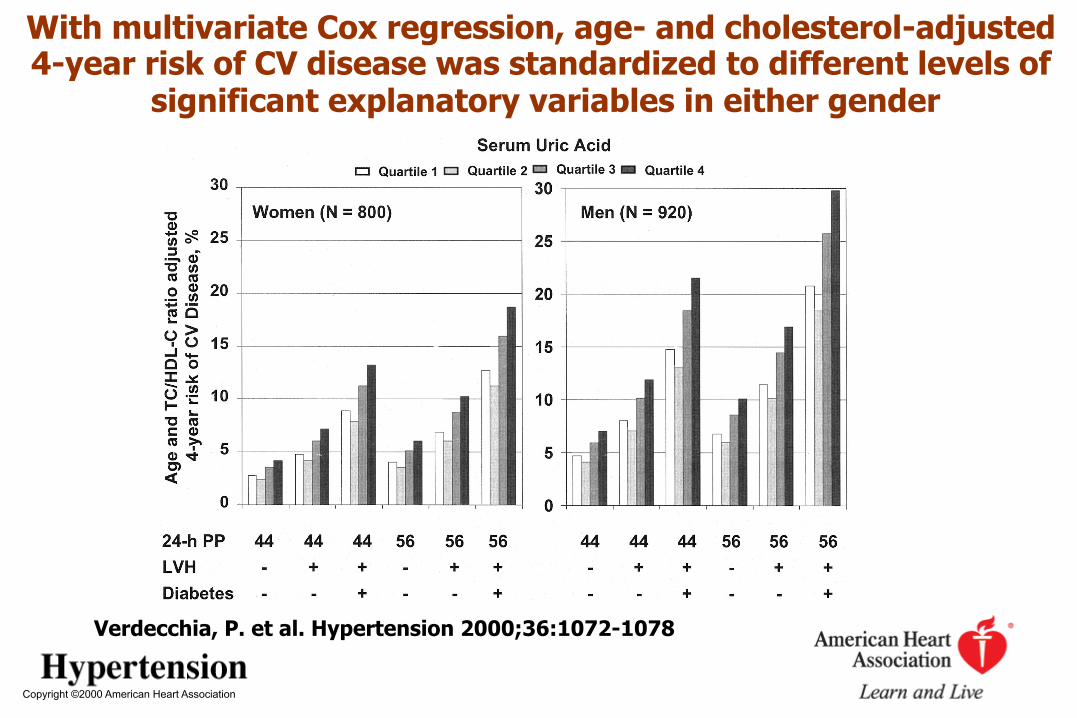
Copyright ©2000 American Heart Association
Verdecchia, P. et al. Hypertension 2000;36:1072-1078
With multivariate Cox regression, age- and cholesterol-adjusted 4-year risk of CV disease was standardized to different levels of
significant explanatory variables in either gender

Is High Serum UA a Risk Marker or a Target for Treatment? Independent Effect in a Large Cohort With Low CV Risk 484,568 adults (mean age: 41 years) participating in a medical screening program in Taiwan since 1994 were followed up for a median of 8.5 years
Chi Pang Wen, AJKD, 56, 2, 273-288, 2010
Uric Acid and Renal Disease

Efectos de hiperuricemia sobre el riñón Modelos experimentales
Vasoconstricción cortical Arteriolopatía aferente Hipertensión glomerular Infiltración macrófagos y linfocitos T Fibrosis intersticial
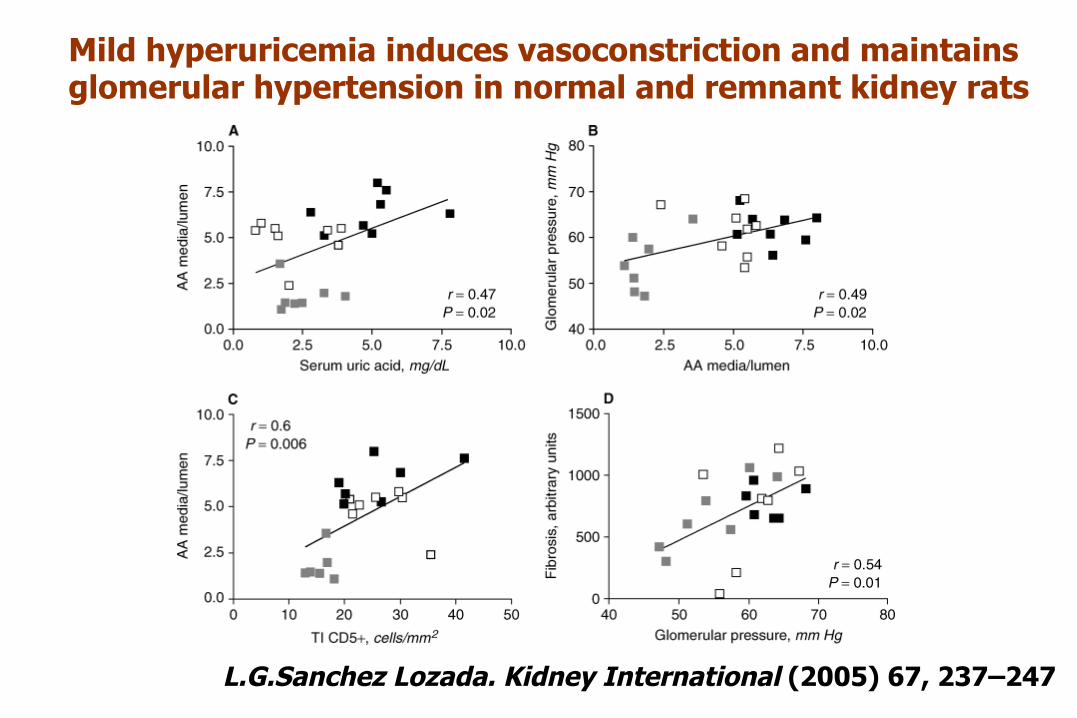
Mild hyperuricemia induces vasoconstriction and maintains glomerular hypertension in normal and remnant kidney rats
L.G.Sanchez Lozada. Kidney International (2005) 67, 237–247

Sanchez-Lozada et al, Kidney Int 2005, 67:237-247
Hiperuricemia y arteriolopatía aferente Ácido oxónico Alopurinol
5/6 nefrectomizadas

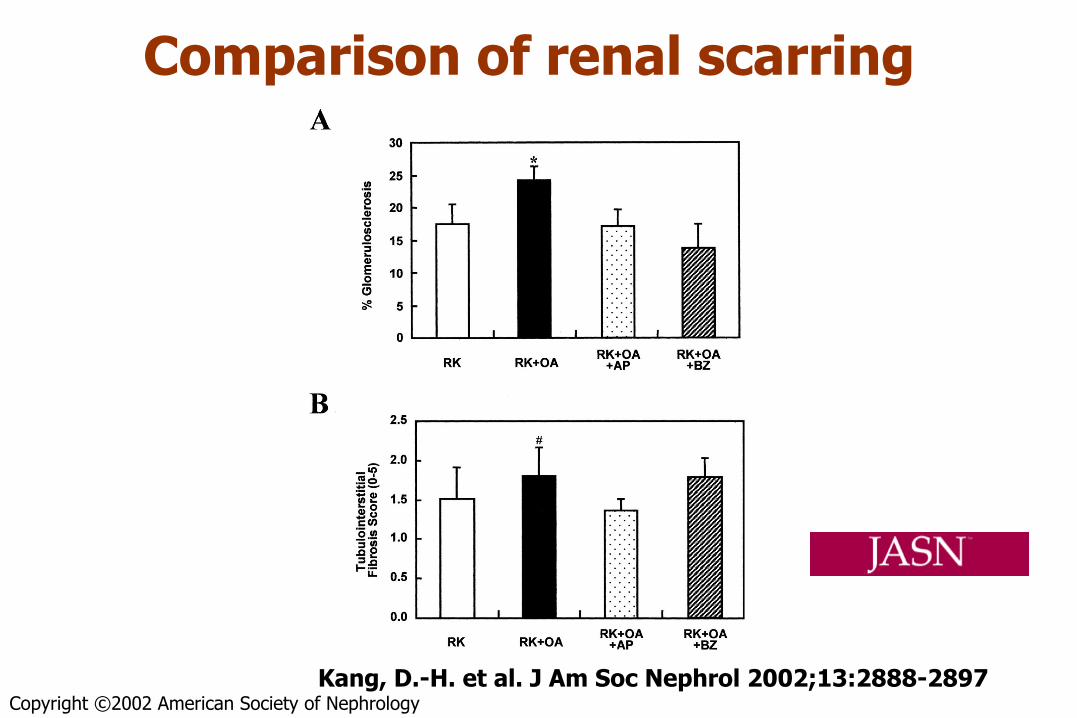
Copyright ©2002 American Society of Nephrology Kang, D.-H. et al. J Am Soc Nephrol 2002;13:2888-2897
Changes in serum uric acid and BP in the remnant kidney (RK), remnant kidney + oxonic acid (RK+OA; ), remnant kidney + oxonic acid + allopurinol (RK+OA+AP);
and remnant kidney + oxonic acid + benziodarone (RK+OA+BZ; rats
Copyright ©2002 American Society of Nephrology
Kang, D.-H. et al. J Am Soc Nephrol 2002;13:2888-2897
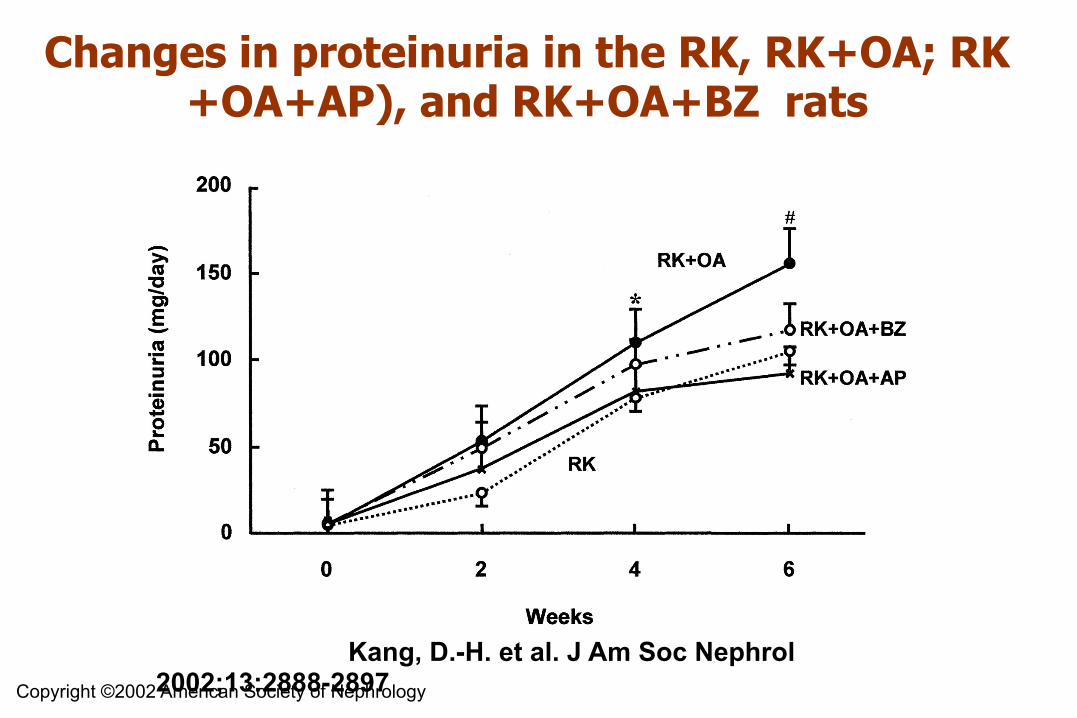
Changes in proteinuria in the RK, RK+OA; RK+OA+AP), and RK+OA+BZ rats

Copyright ©2002 American Society of Nephrology
Kang, D.-H. et al. J Am Soc Nephrol 2002;13:2888-2897
Correlation of serum uric acid with renin expression in renal cortex
Copyright ©2002 American Society of Nephrology Kang, D.-H. et al. J Am Soc Nephrol 2002;13:2888-2897
Comparison of renal scarring

An association between uric acid levels and renal arteriolopathy in CKD: a biopsy-based study
OR IC (95%) P Hyalinosis grade 3.13 1.23-7.94 0.02 Thickening wall grade 2.66 1.11-6.38 0.03
Hyperuricemia (UA > 7 mg/dl)
167 CKD patients
Kohagura K et al, Hypertens Res 2012, sep 6 (on line)
Adjusted for age, sex, hypertension , diabetes mellitus, eGFR

Association of Uric Acid with Change in Kidney Function in 900 Healthy Normotensive Individuals
Bellomo G. AJKD, Vol 56, 2 : 264-272, 2010

Richard J. Johnson. NDT Advance Access published March 29, 2013

Uric Acid and Risk of CKD
Feig et al, Curr Opin Nephrol Hypertens 18: 526-530,2009
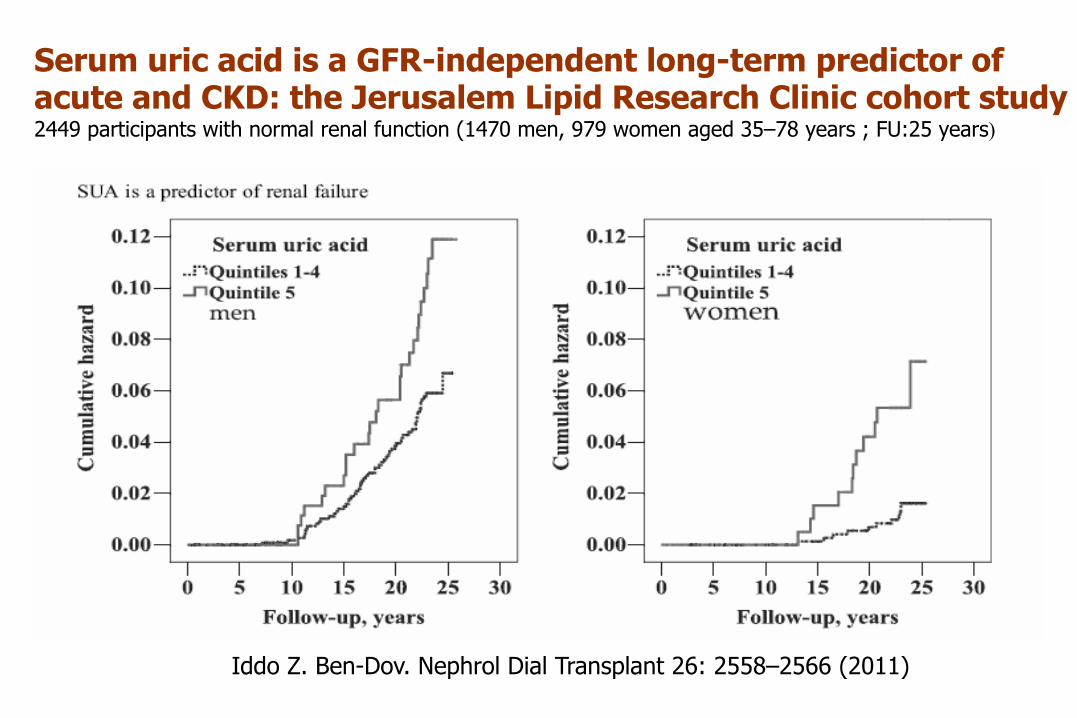
Serum uric acid is a GFR-independent long-term predictor of acute and CKD: the Jerusalem Lipid Research Clinic cohort study 2449 participants with normal renal function (1470 men, 979 women aged 35–78 years ; FU:25 years)
Iddo Z. Ben-Dov. Nephrol Dial Transplant 26: 2558–2566 (2011)
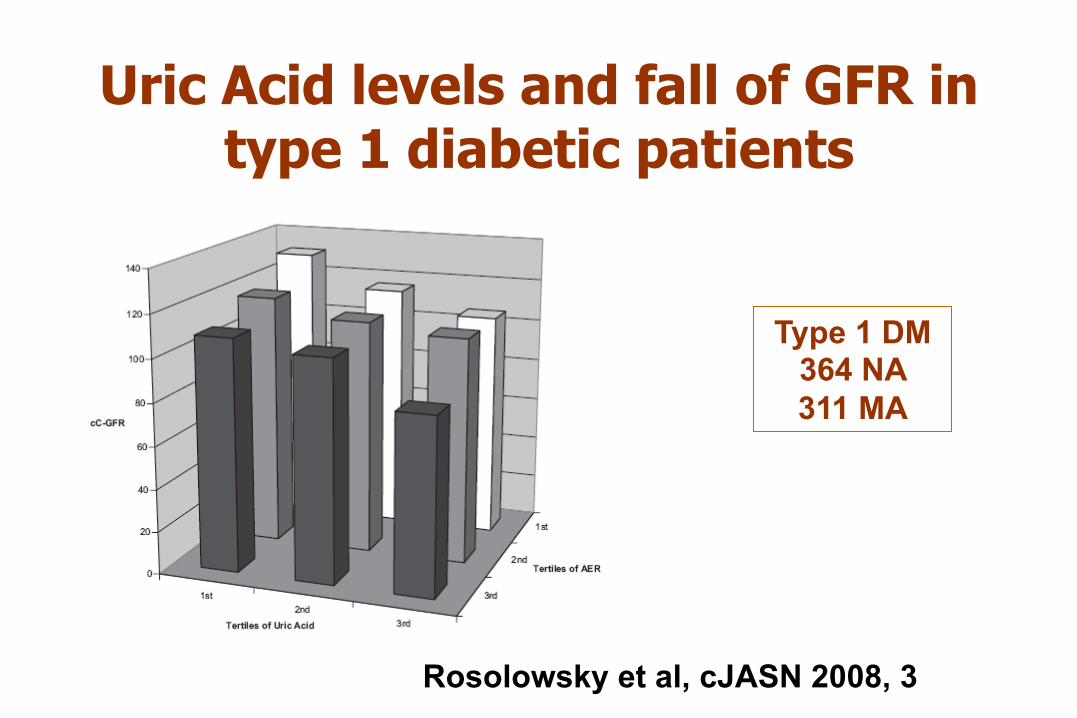
Uric Acid levels and fall of GFR in type 1 diabetic patients
Rosolowsky et al, cJASN 2008, 3:706-713
Type 1 DM 364 NA 311 MA
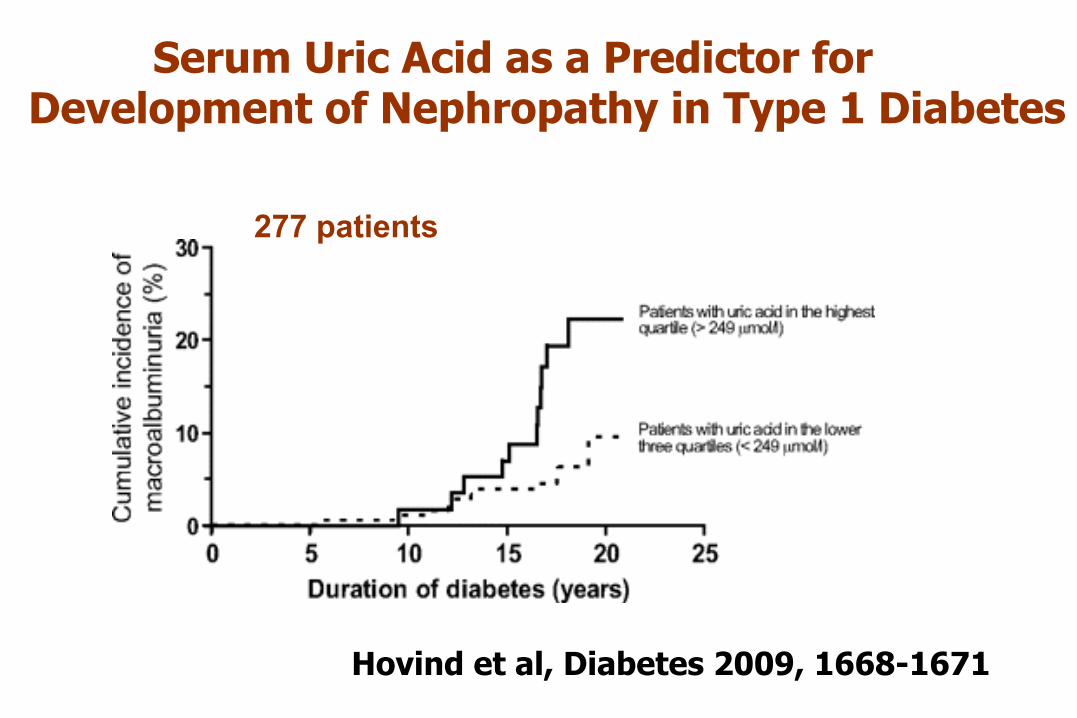
Serum Uric Acid as a Predictor for Development of Nephropathy in Type 1 Diabetes
Hovind et al, Diabetes 2009, 1668-1671
277 patients

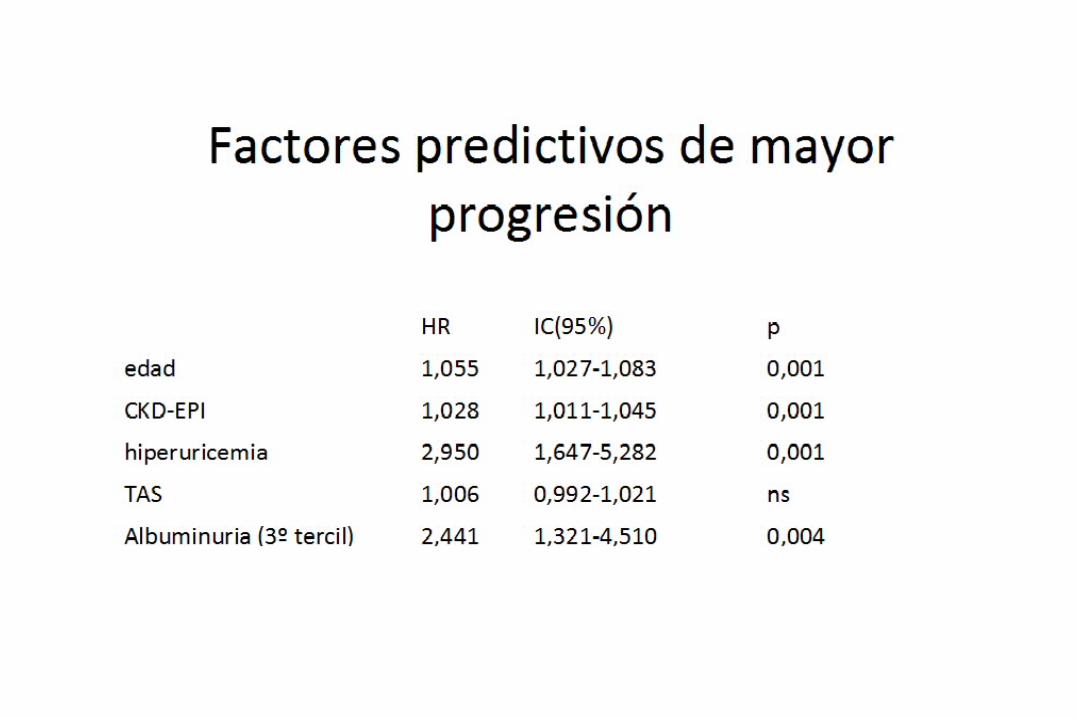
LA HIPERURICEMIA PREDICE LA PROGRESIÓN DE ERC EN PACIENTES CON DISMINUCIÓN DE LA MASA RENAL FUNCIONANTE. MONORRENOS N=337; Edad 59±17 años; Seguimiento : 60 ( 36-98 meses)

Adjusted HRs for all-cause mortality per 1 mg/dl greater uric acid level in all subjects stratified by presence or absence of DM, CVD, HTN, and gout n=(3303 stages 3–5 CKD patients . FU: 2.8 years)
Wan-Chun Liu. Clin J Am Soc Nephrol 7: 541–548, 2012
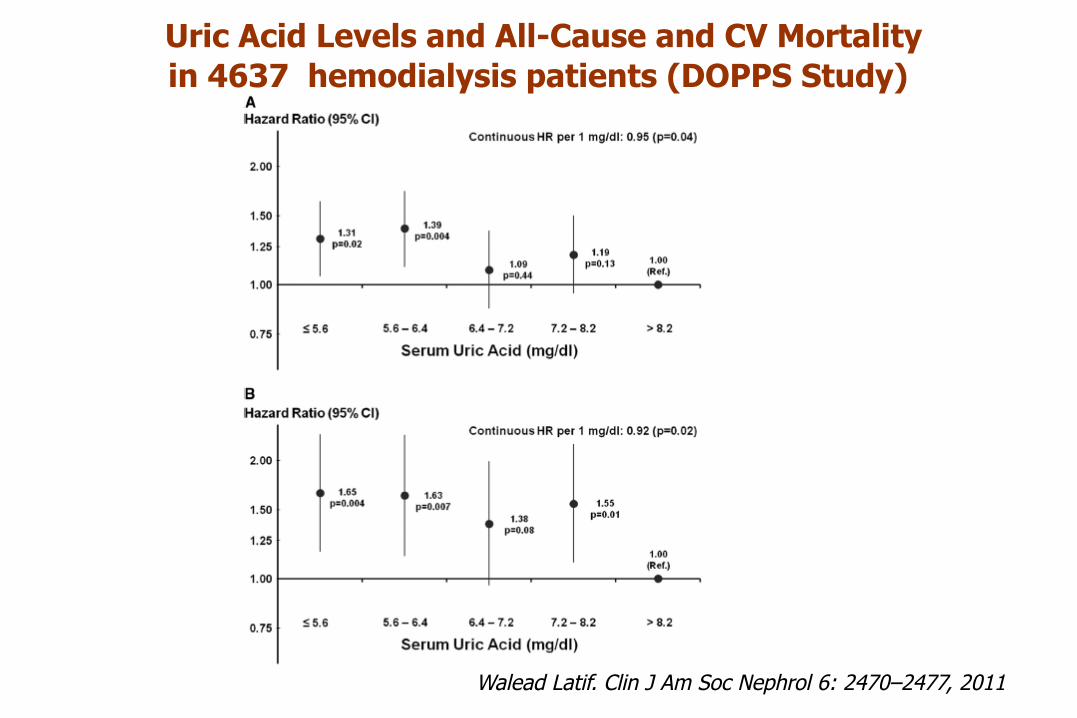
Uric Acid Levels and All-Cause and CV Mortality in 4637 hemodialysis patients (DOPPS Study)
Walead Latif. Clin J Am Soc Nephrol 6: 2470–2477, 2011

Uric Acid Levels during the first six months post RT and renal graft survival
212 patients Living Renal Transplants
FU:68±27 months
Haririan et al, Transplantation 2010, 89 (5) 573
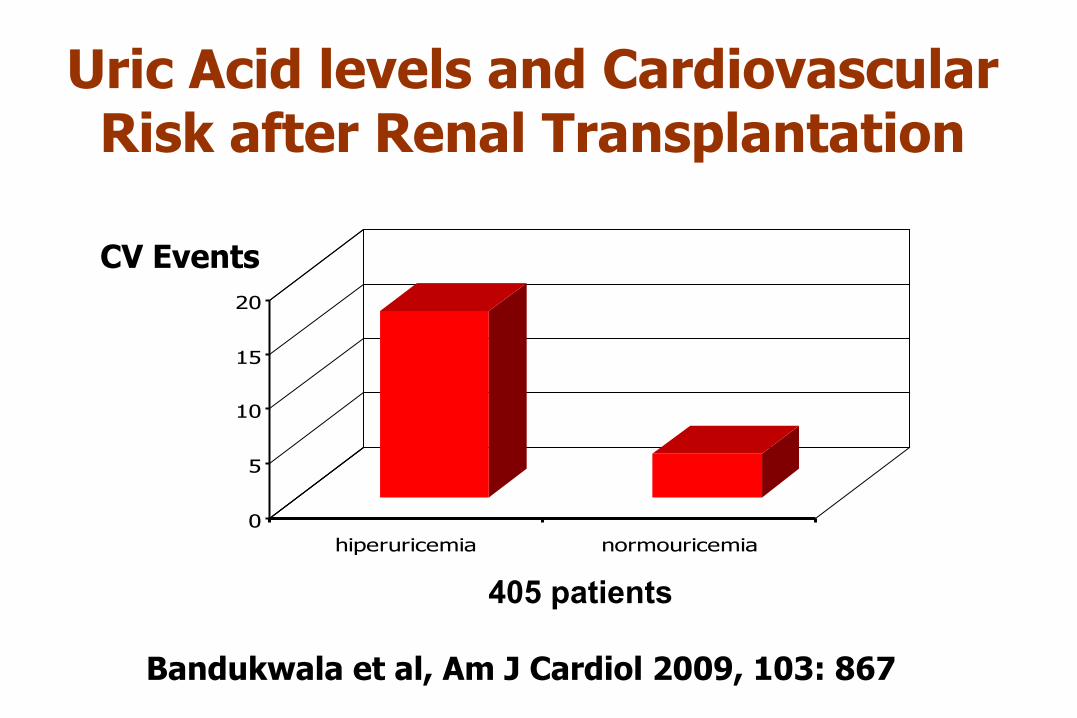
Uric Acid levels and Cardiovascular Risk after Renal Transplantation
0
5
10
15
20
hiperuricemia normouricemia
CV Events
Bandukwala et al, Am J Cardiol 2009, 103: 867-871
405 patients

36
P=0,007
Niveles de ácido úrico en pacientes con ERC
Hombres (n=228) Mujeres (n=172)
Goicoechea M, Garcia de Vinuesa S, Arroyo D, Luño J. Nefrología 2012, supl , 3:12-15
45 % de los hombres tienen hiperuricemia y un 11% de ellos están tratados con alopurinol
51 % de las mujeres tienen hiperuricemia y un 9% de ellas están tratados con alopurinol

A pesar del tratamiento con alopurinol,
un gran porcentaje de pacientes con ERC
presentan hiperuricemia.
ADENURIC® (Febuxostat): una nueva opción terapéutica
para la hiperuricemia en el tratamiento de la gota

Clinical interventional studies

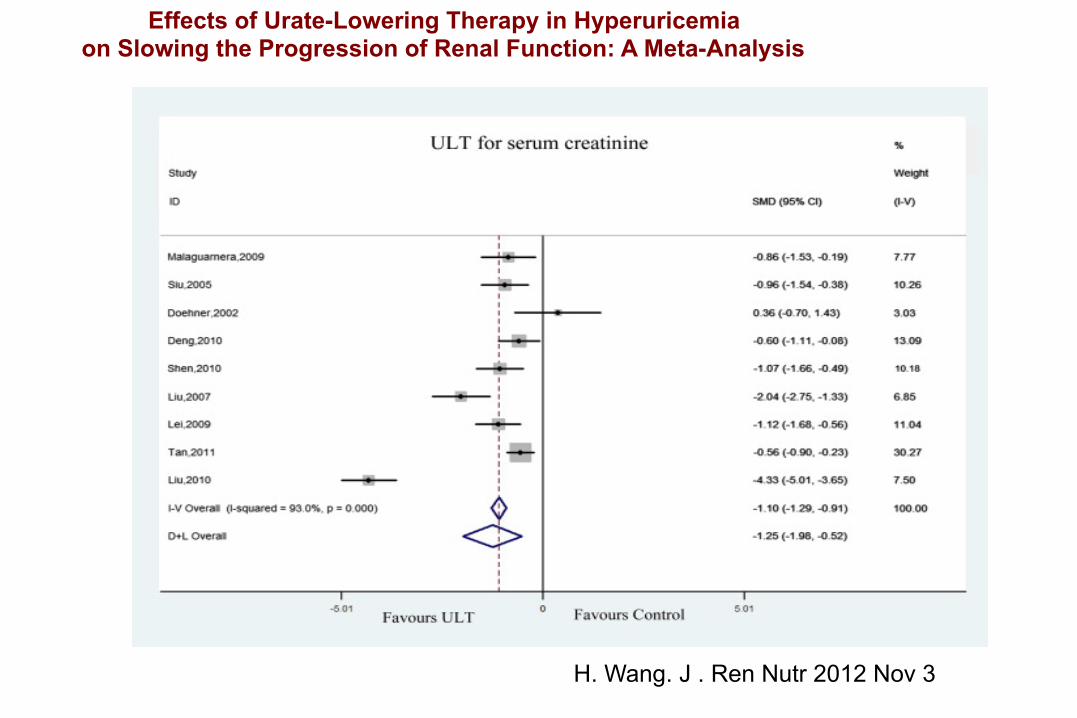
Effects of Urate-Lowering Therapy in Hyperuricemia on Slowing the Progression of Renal Function: A Meta-Analysis
H. Wang. J . Ren Nutr 2012 Nov 3.

Effects of Urate-Lowering Therapy in Hyperuricemia on Slowing the Progression of Renal Function: A Meta-Analysis
H. Wang. J . Ren Nutr 2012 Nov 3
H. Wang. J . Ren Nutr 2012 Nov 3
Effects of Urate-Lowering Therapy in Hyperuricemia on Slowing the Progression of Renal Function: A Meta-Analysis

Effects of Urate-Lowering Therapy in Hyperuricemia on Slowing the Progression of Renal Function: A Meta-Analysis
H. Wang. J . Ren Nutr 2012 Nov 3.
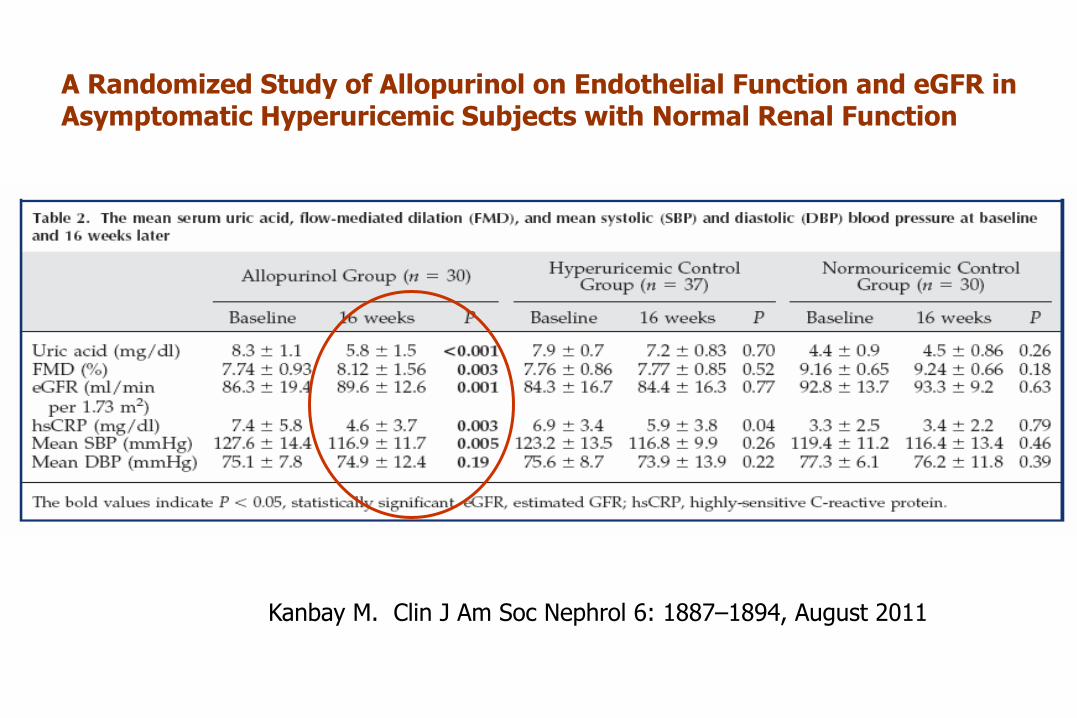
A Randomized Study of Allopurinol on Endothelial Function and eGFR in Asymptomatic Hyperuricemic Subjects with Normal Renal Function
Kanbay M. Clin J Am Soc Nephrol 6: 1887–1894, August 2011

Reduction in SUA on Renal Outcomes During Losartan Treatment . Post Hoc Analysis of RENAAL Study
Risk reduction per 0.5 mg/dL SUA decrement: 6% (95%CI:13-10)
Month 6 change uric acid (mg/dL)
Yan Miao. Hypertension. July 2011;58:2-7

M.Goicoechea, S. García de Vinuesa, U. Verdalles, C. Ruiz-Caro, J. Ampuero, A.Rincón, MA. Dominguez1, D.
Arroyo, J. Luño.
Effect of allopurinol in chronic kidney disease (CKD) progression and cardiovascular risk.
Clin J Am Soc Nephrol 5: 1388-1393, 2010

Allopurinol and progression of CKD and CV risk
• Inclusion criteria: eGFR < 60 ml/min., stable clinical condition & renal function, baseline serum uric acid 7.6 mg/dl
• Randomised to – Allopurinol 100 mg/d (N= 57) or – Placebo (N= 56)

Effect of Allopurinol in UA levels, albuminuria and inflammatory parameters
Control Group
Uric Acid mg/dl (p=0.016
HsCRP mg/L (p=0.018)
Fibrinogen mg/dl
Albuminuria mg/day
Baseline 7.3±1.6 3.4 (5.2) 384±104 32(383)
6 months 7.0±1.6 3.0 (7.6) 373±112 43(417)
12 months 7.4±2.0 3.2 (10.8) 402±98 51(296)
24 months 7.5±1.7
Allopurinol Group
Uric Acid mg/dl
HsCRP mg/L
Fibrinogen mg/dl
Albuminuria mg/day
Baseline 7.8± 2.1 4.4 (4.5) 381±78 36(388)
6 months 6.2±1.5* 3.0 (4.0)* 367±58 15(103)
12 months 6.0±1.8* 3.0 (2.5)* 369±49 16(166)
24 months 6.0±1.2*
-4
-3
-2
-1
0
1
2
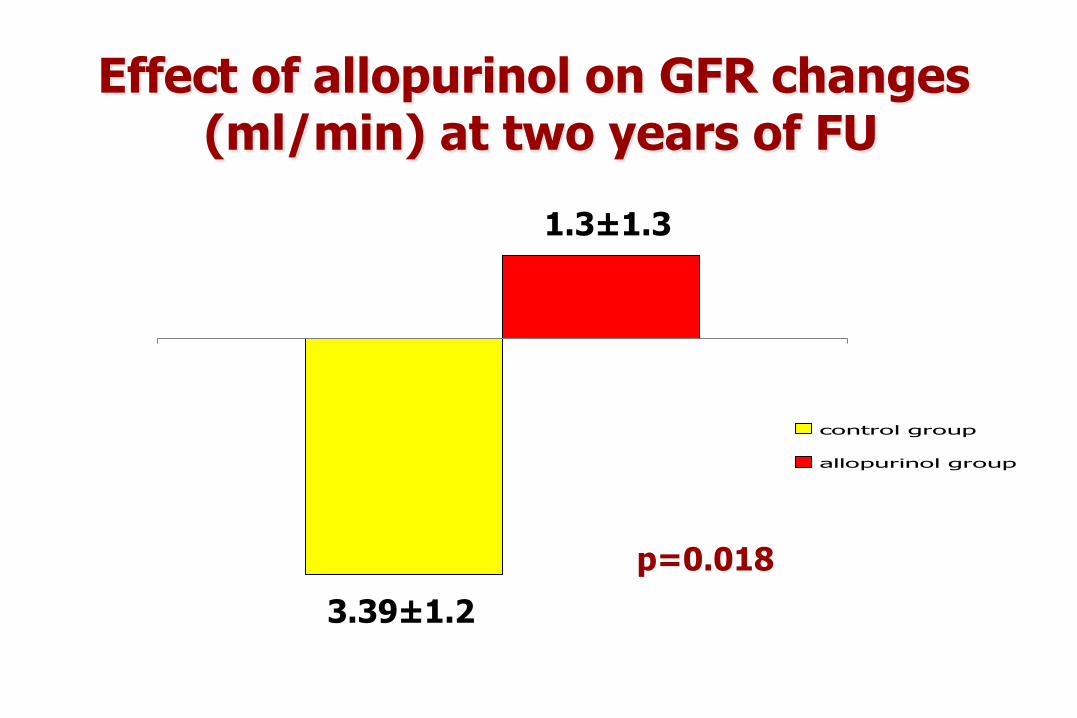
control group
allopurinol group
Effect of allopurinol on GFR changes (ml/min) at two years of FU
p=0.018
3.39±1.2
1.3±1.3
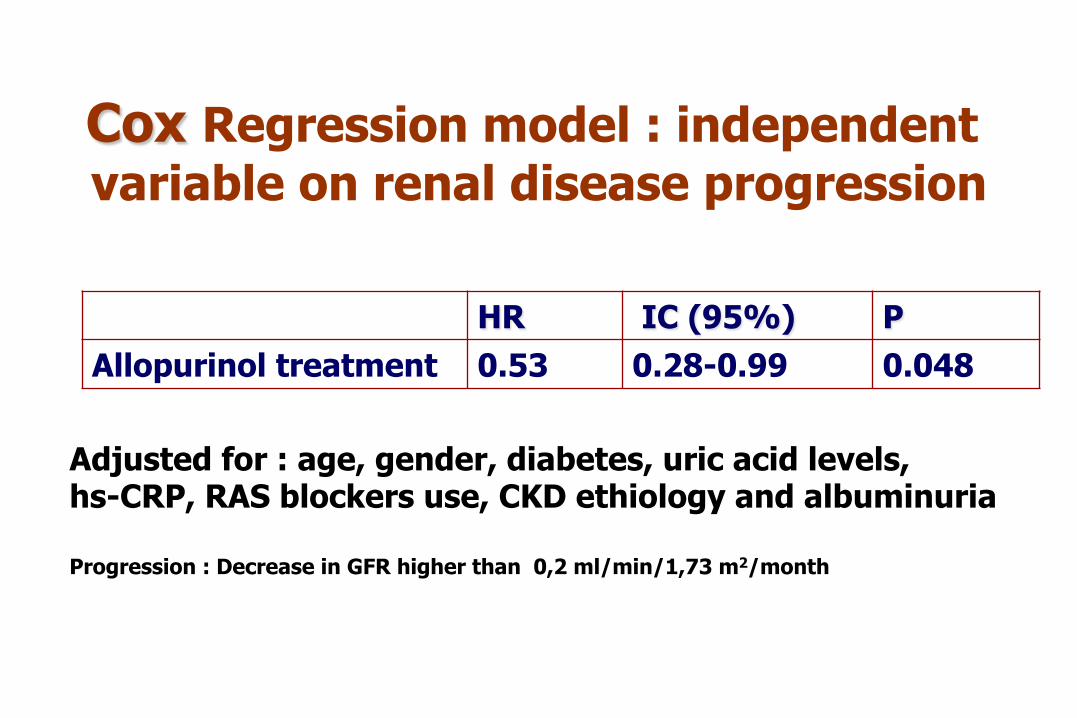
Cox Regression model : independent variable on renal disease progression
Adjusted for : age, gender, diabetes, uric acid levels, hs-CRP, RAS blockers use, CKD ethiology and albuminuria Progression : Decrease in GFR higher than 0,2 ml/min/1,73 m2/month
HR IC (95%) P Allopurinol treatment 0.53 0.28-0.99 0.048

Log rank=4.255 p=0.039
Effect of Allopurinol on CV events
22 CV events (15 patients on control group and 7 on the allopurinol group : 8 Heart failure; 7 CHD; 5 CVD; 1 PAD;1 Arrythmia.
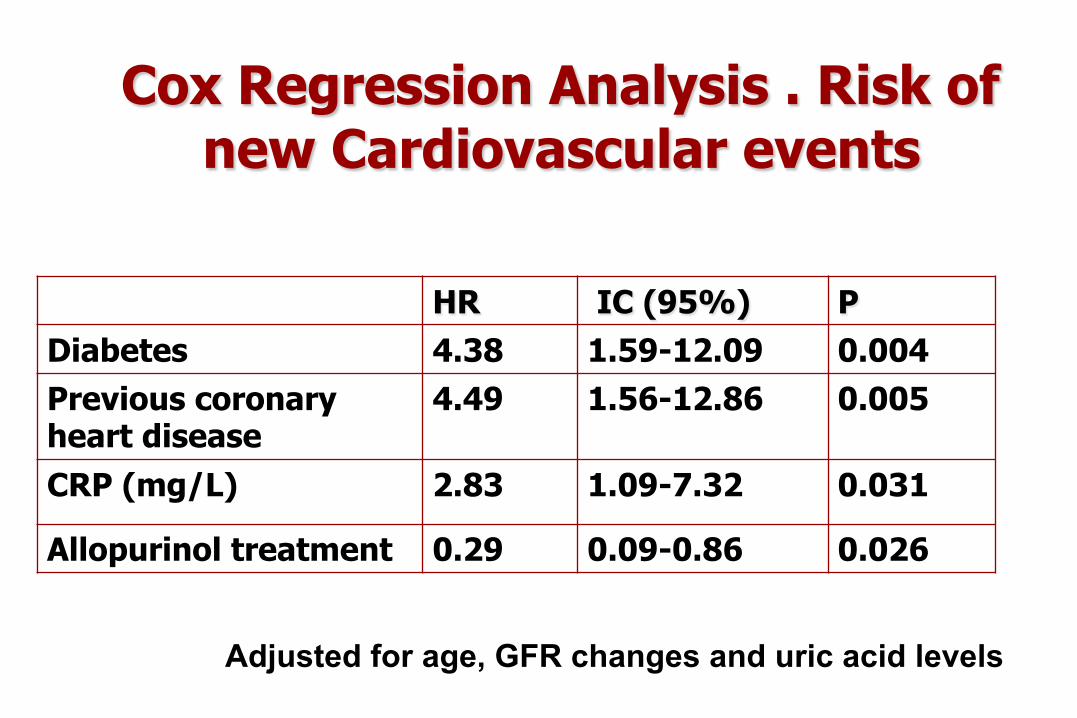
Cox Regression Analysis . Risk of new Cardiovascular events
HR IC (95%) P Diabetes 4.38 1.59-12.09 0.004 Previous coronary heart disease
4.49 1.56-12.86 0.005
CRP (mg/L) 2.83 1.09-7.32 0.031
Allopurinol treatment 0.29 0.09-0.86 0.026
Adjusted for age, GFR changes and uric acid levels
ADVERSE EVENTS ALLOPURINOL WAS WITHDRAWN IN TWO PATIENTS FOR
GASTROINTESTINAL SYMPTOMS. NO ABNORMALITIES IN LIVER FUNCTION TEST WERE ATTRIBUTED TO ALLOPURINOL TREATMENT. NO HEMATOLOGIC ALTERATIONS OR SERIOUS ADVERSE EVENTS IN RELATION TO ALLOPURINOL TREATMENT APPEARED IN THE FOLLOW-UP STUDY. SIX PATIENTS IN THE CONTROL GROUP AND THREE IN THE ALLOPURINOL GROUP WERE LOST DURING THE STUDY PERIOD .

CONCLUSIONS
We conclude that allopurinol treatment decreases inflammation and slows down the progression of renal disease in patients with moderate CKD.
In addition, allopurinol reduces cardiovascular and hospitalization risk.
These results have to be confirmed in larger prospective trials and are the basis for a hypothesis that still needs to be tested.
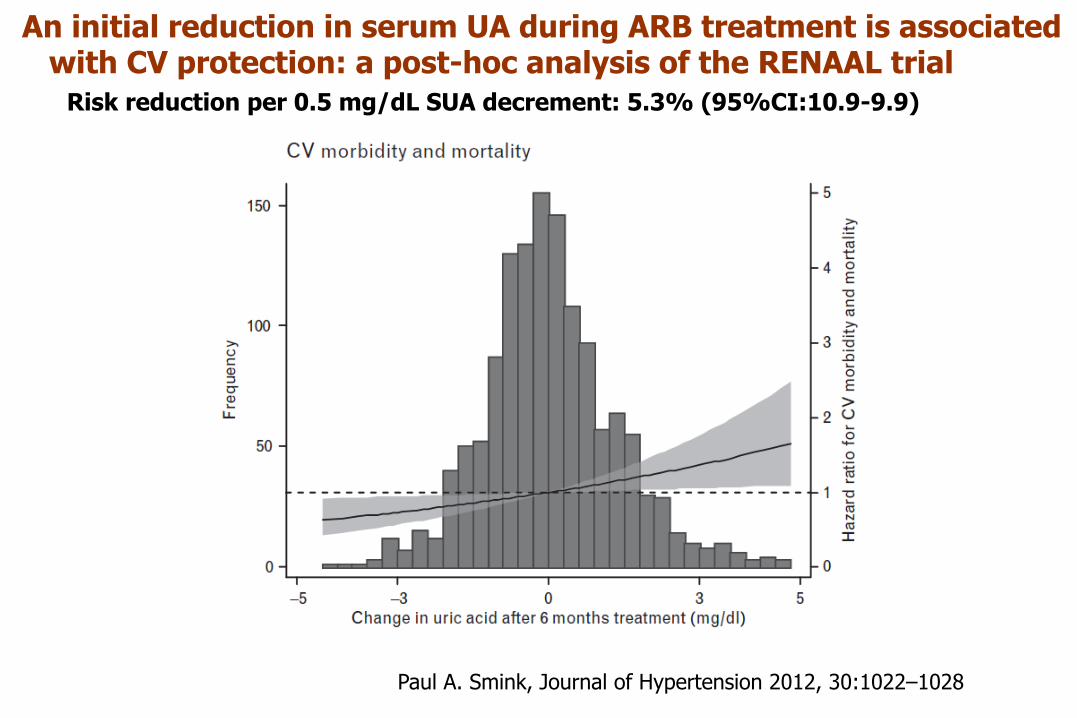
An initial reduction in serum UA during ARB treatment is associated with CV protection: a post-hoc analysis of the RENAAL trial Risk reduction per 0.5 mg/dL SUA decrement: 5.3% (95%CI:10.9-9.9)
Paul A. Smink, Journal of Hypertension 2012, 30:1022–1028
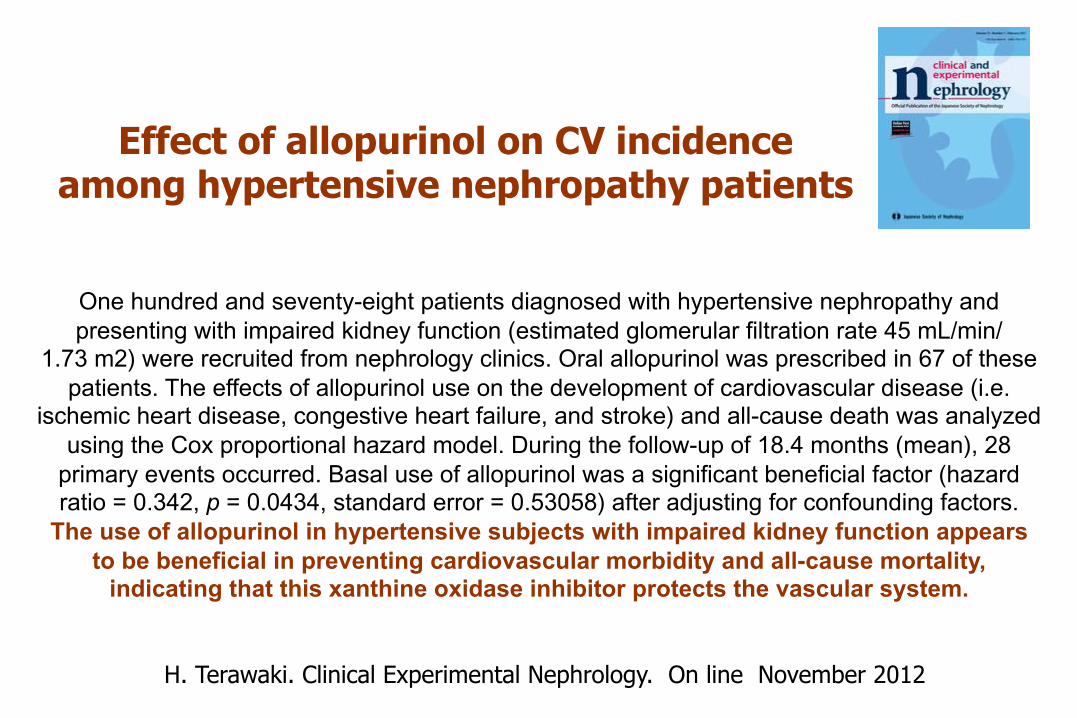
Effect of allopurinol on CV incidence among hypertensive nephropathy patients
H. Terawaki. Clinical Experimental Nephrology. On line November 2012
One hundred and seventy-eight patients diagnosed with hypertensive nephropathy and presenting with impaired kidney function (estimated glomerular filtration rate 45 mL/min/
1.73 m2) were recruited from nephrology clinics. Oral allopurinol was prescribed in 67 of these patients. The effects of allopurinol use on the development of cardiovascular disease (i.e.
ischemic heart disease, congestive heart failure, and stroke) and all-cause death was analyzed using the Cox proportional hazard model. During the follow-up of 18.4 months (mean), 28
primary events occurred. Basal use of allopurinol was a significant beneficial factor (hazard ratio = 0.342, p = 0.0434, standard error = 0.53058) after adjusting for confounding factors.
The use of allopurinol in hypertensive subjects with impaired kidney function appears to be beneficial in preventing cardiovascular morbidity and all-cause mortality,
indicating that this xanthine oxidase inhibitor protects the vascular system.

Is necessary to treat all patients with CKD And asymptomatic Hyperuricemia ?
Challenges of conducting a trial of uric-acid-lowering therapy in CKD Sunil V. Badve, Fiona Brown, Carmel M. Hawley, David W. Johnson, John Kanellis, Gopala K. Rangan and Vlado Perkovic. Nat. Rev. Nephrol. advance online publication 15 February 2011
An adequately powered randomized controlled trial is required to determine whether uric-acid-lowering therapy slows the progression of CKD. International collaboration is required to plan and conduct a large-scale multicenter trial in order to better inform clinical practice and public health policy about the optimal management of asymptomatic hyperuricemia in patients with CKD
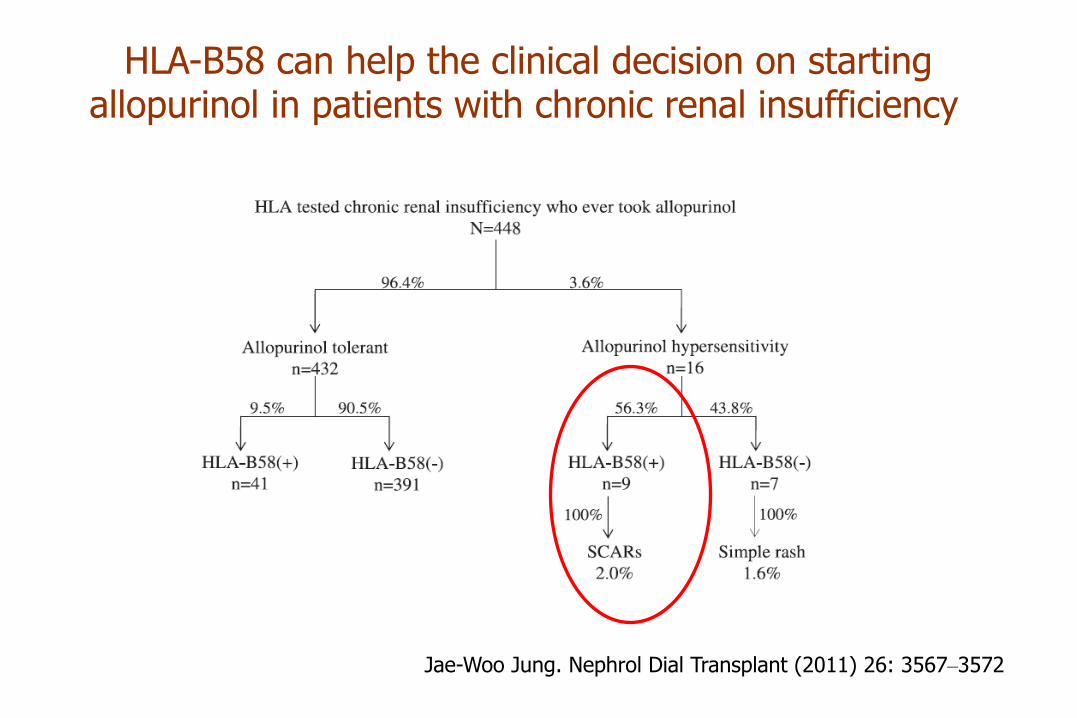
HLA-B58 can help the clinical decision on starting allopurinol in patients with chronic renal insufficiency
Jae-Woo Jung. Nephrol Dial Transplant (2011) 26: 3567–3572

Allopurinol association of severe coutaneous adverse reactions
Jae-Woo Jung. Nephrol Dial Transplant (2011) 26: 3567–3572

No se pude mostrar la imagen vinculada. Puede que se haya movido, cambiado de nombre o eliminado el archivo. Compruebe que el vínculo señala al archivo y ubicaciones correctos.
Rapid screening for the detection of HLA-B57 and HLA-B58 in prevention of drug hypersensitivity
L. Kostenko Tissue Antigens: 78: 1; 11–20, July 2011
HLA-B57 and HLA-B58 are major histocompatibility class (MHC)-I allotypes that are potentially predictive of important clinical immune phenotypes. HLA-B*5701 is strongly associated with hypersensitivity to the HIV drug abacavir, liver toxicity from the antibiotic flucloxacillin and is a marker for slow progression of HIV AIDS. HLA-B*5801 is associated with hypersensitivity to allopurinol used to treat hyperuricaemia and recurrent gout. Here we describe a monoclonal antibody (mAb) specific for HLA-B57 and HLA-B58 that provides an inexpensive and sensitive screen for these MHC-I allotypes. The usefulness of HLA-B57 screening for prediction of abacavir hypersensitivity was shown in three independent laboratories, including confirmation of the mAb sensitivity and specificity in a cohort of patients enrolled in the PREDICT-1 trial. Our data show that patients who test negative by mAb screening comprise 90%–95% of all individuals in most human populations and require no further human leukocyte antigen (HLA) typing. Patients who test positive by mAb screening should proceed to high-resolution typing to ascertain the presence of HLA-B*5701 or HLA-B*5801. Hence, mAb screening provides a low-cost alternative to high-resolution typing of all patients and lends itself to point-of-care diagnostics and rapid ascertainment of low-risk patients who can begin immediate therapy with abacavir, flucloxacillin or allopurinol.
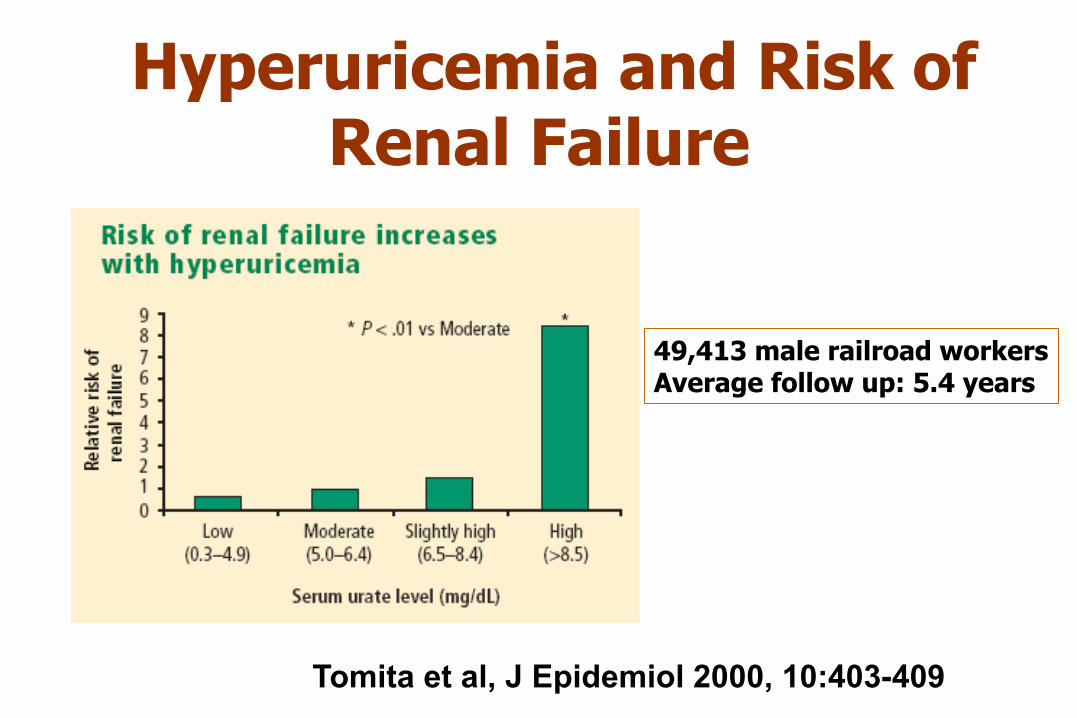
Hyperuricemia and Risk of Renal Failure
Tomita et al, J Epidemiol 2000, 10:403-409
49,413 male railroad workers Average follow up: 5.4 years
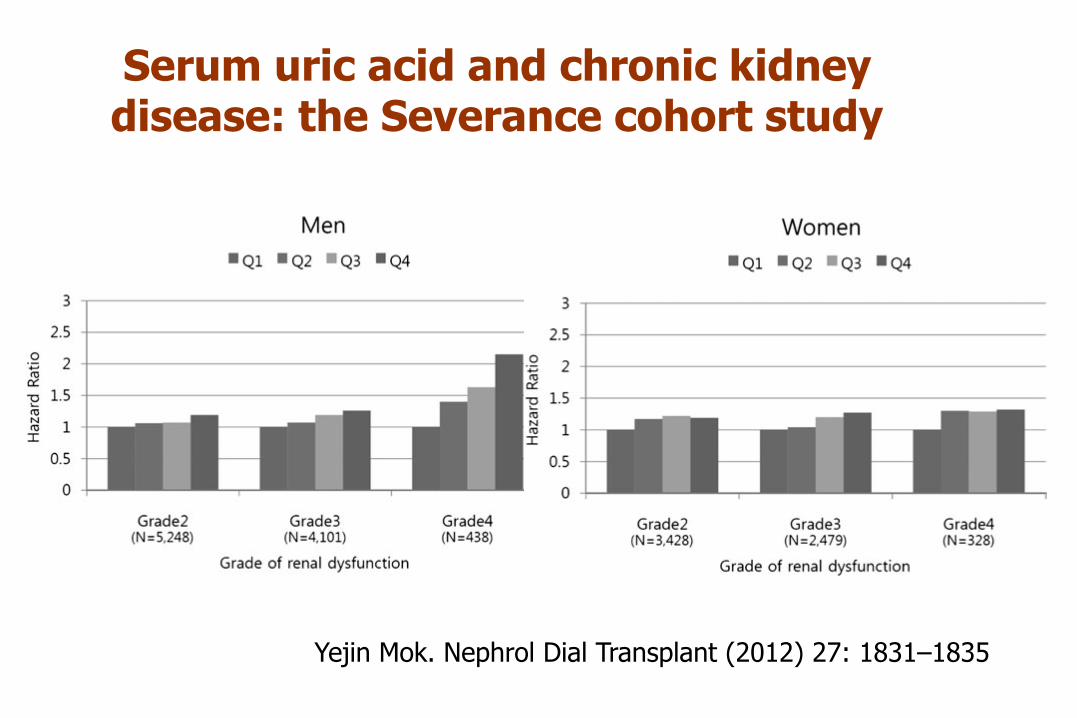
Serum uric acid and chronic kidney disease: the Severance cohort study
Yejin Mok. Nephrol Dial Transplant (2012) 27: 1831–1835
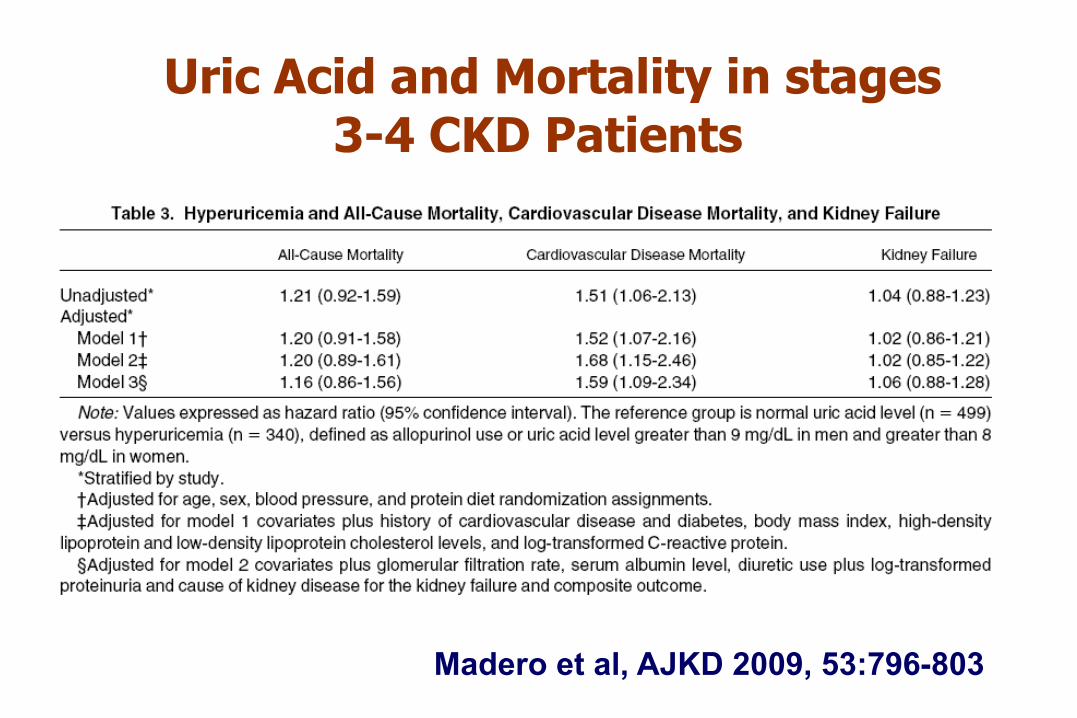
Uric Acid and Mortality in stages 3-4 CKD Patients
Madero et al, AJKD 2009, 53:796-803

20 of the 30 participants achieved normal BP during
the allopurinol phase, whereas only 1 of 30 achieved
normal BP during the placebo phase
Of the 10 participants who remained hypertensive
while taking allopurinol, 7 had a uric acid level of 5.0
mg/dl or higher at the end of the allopurinol phase
Lowering Uric Acid Reduces SBP in Adolescents with Hypertension

Use of Allopurinol in Slowing the Progression of Renal Disease Siu YP. American Journal of Kidney Diseases. 47:1, 51-59 , 2006
54 CKD patients with mean uric acid 9.75 mg/dl were randomized to treatment with allopurinol 100–300 mg/day o usual care during 12 moths. Treated patients had a tendency to slower progression. There was no statistically significant difference in serum Cr as a continuous variable, but the study was not powered to detect this endpoint
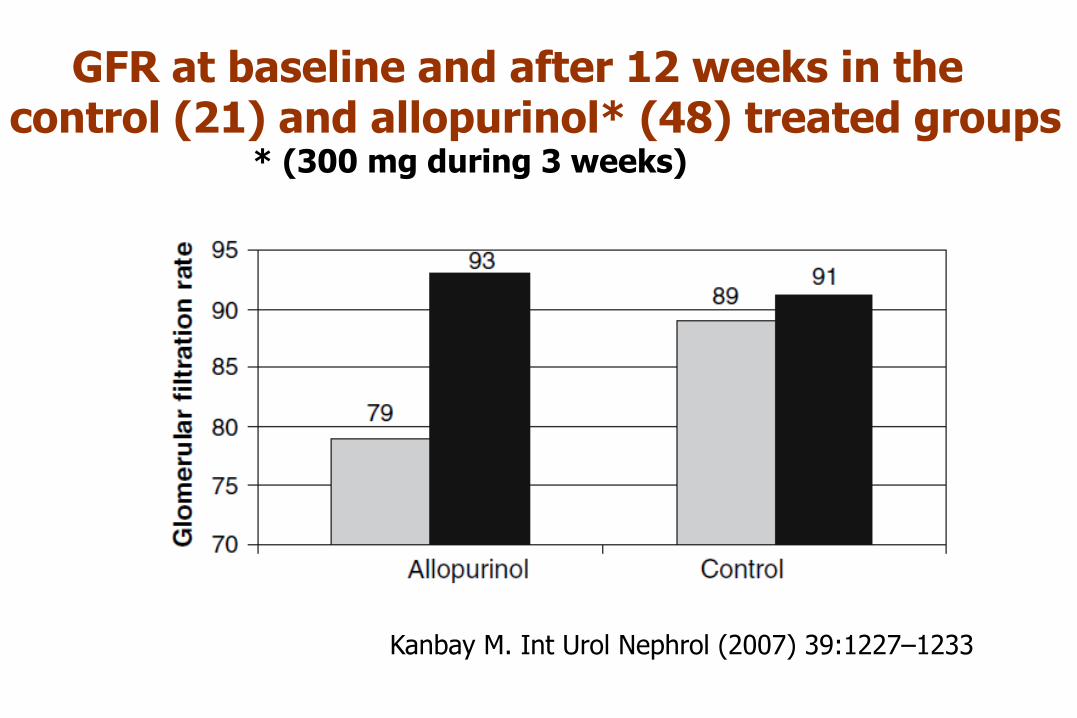
GFR at baseline and after 12 weeks in the control (21) and allopurinol* (48) treated groups * (300 mg during 3 weeks)
Kanbay M. Int Urol Nephrol (2007) 39:1227–1233








![LIC SOL FERRENTINO [Modo de compatibilidad] y... · Cuidados Independientes Plan de cuidados Valoración cte. Monitoreo continuo. Shock Cardiogénico Taquicardia Oliguria Vasoconstricción](https://static.fdocuments.es/doc/165x107/5a8175b27f8b9ada388d19d9/lic-sol-ferrentino-modo-de-compatibilidad-ycuidados-independientes-plan-de.jpg)








