Generalidades en el diagnóstico de epilepsia en pediatríakindermed.info/ · ! 10,5 millones de...
51
Generalidades en el diagnóstico de epilepsia en pediatría Dr. Alvaro Retamales M. Neurólogo Infantil - Miércoles, 13 de agosto de 2014 -
Transcript of Generalidades en el diagnóstico de epilepsia en pediatríakindermed.info/ · ! 10,5 millones de...
Generalidades en el diagnóstico de
epilepsia en pediatría
Dr. Alvaro Retamales M.
Neurólogo Infantil
- Miércoles, 13 de agosto de 2014 -
Temario
¤ 1. Definiciones y clasificación
¤ 2. Semiología
¤ 3. Exámenes complementarios
¤ 4. Diagnósticos diferenciales
Epilepsia y crisis epilépticas
¤ Epilepsia:
¤ Trastorno cerebral caracterizado por:
¤ Predisposición a generar crisis epilépticas
¤ Las consecuencias neurobiológicas,
cognitivas, psicológicas y sociales derivadas
de ella.
¤ Requiere al menos 1 crisis epiléptica
Epileptic seizures and epilepsy Definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy. Epilepsia (2005)
¤ 10,5 millones de niños <15
años tienen epilepsia.
¤ 80%de pacientes con
epilepsia son menores de 15
años.
¤ Aproximadamente un 60% de
los niños con epilepsia en la
niñez dejarán de padecerla
en la adultez.
Epilepsia y crisis epilépticas
¤ 6 a 7% de los niños
menores de 15 años
presentarán una crisis a lo
largo de su vida
(provocada o no)
¤ Aumenta a 7 – 12% en
países con bajo ingreso.
Epilepsia y crisis epilépticas
Epilepsia y crisis epilépticas
Epilepsia y crisis epilépticas
¤ Crisis epiléptica:
¤ Episodio causado por una
descarga anormal, excesiva y
sincrónica de un grupo de
neuronas que produce una
alteración en la función del
paciente.
Epileptic seizures and epilepsy Definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy. Epilepsia (2005)

Epilepsia y crisis epilépticas
¤ Otros conceptos:
¤ Epilepsia es una ENFERMEDAD.
¤ Evidencia clara de un síndrome epiléptico, se requiere 1 sola
crisis, aún cuando el riesgo de recurrencia sea bajo.
¤ 2 crisis se consideran independientes si tienen >24 hrs
¤ No hay límite de tiempo para una 2da crisis
¤ Epilepsia “resuelta”
¤ Información “imperfecta”: concepto de epilepsia “probable”
Otras definiciones
¤ Síndrome:
¤ Conjunto de síntomas y signos relacionados entre sí, que permiten
realizar una unidad diagnóstica.
¤ Síndrome epiléptico:
¤ Asociaciones particulares de manifestaciones clínicas y
electroencefalográficas frecuentemente edad dependiente, que
permiten:
¤ Orientar estudio etiológico
¤ Definir conducta terapéutica
¤ Definir pronóstico.

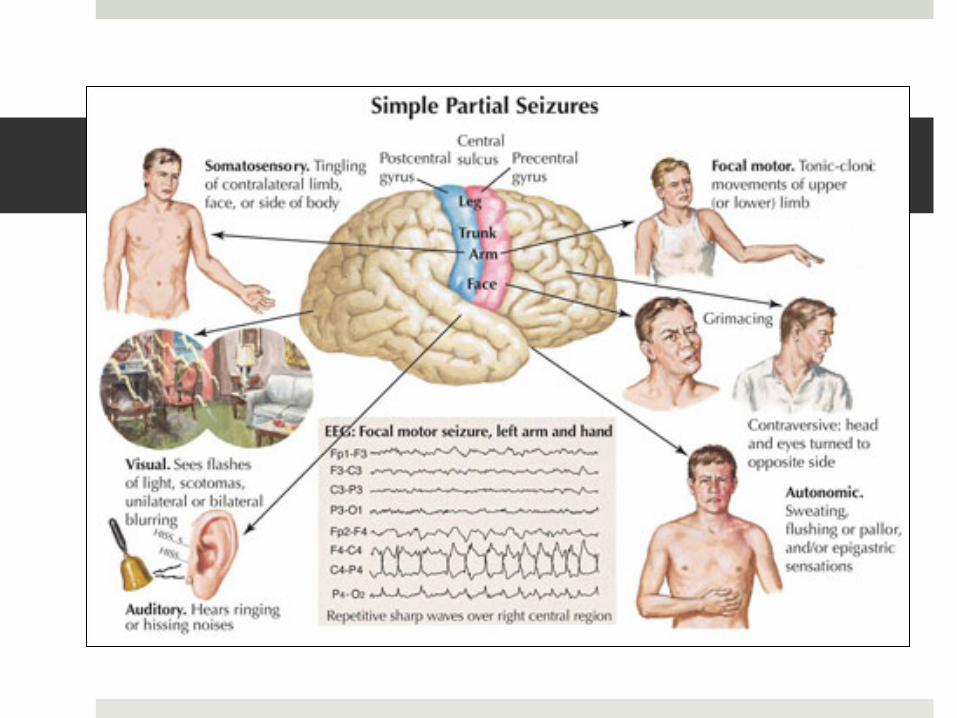
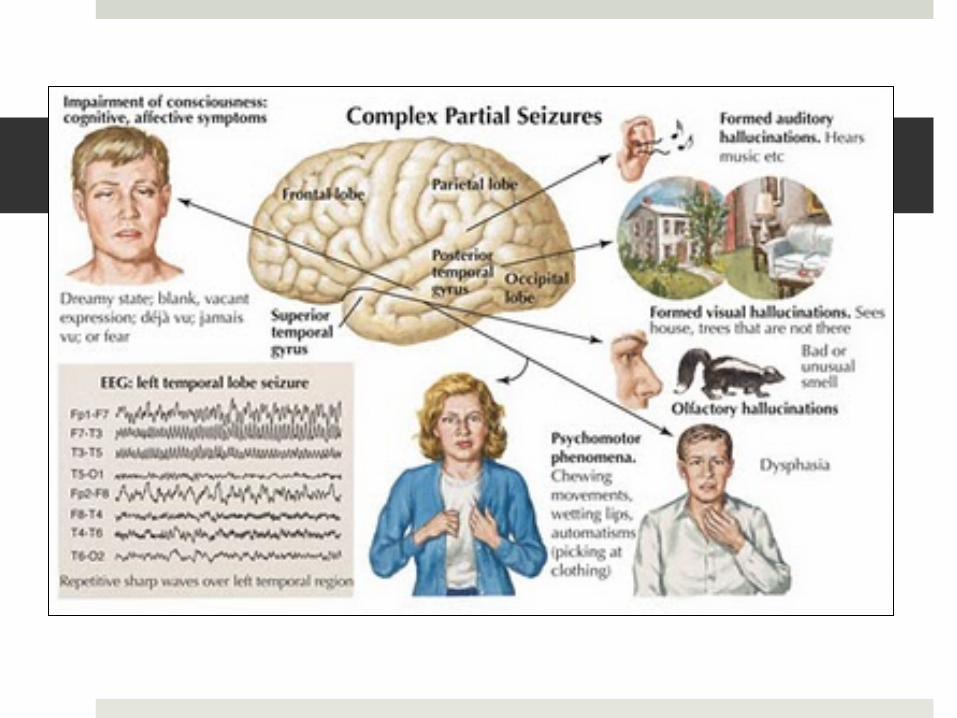
Clasificación internacional de crisis epilépticas (ILAE 1981) I. Crisis focales
A. Crisis parciales simples 1. Con signos motores 2. Con síntomas somatosensoriales 3. Con signos y síntomas autonómicos 4. Con síntomas psíquicos
B. Crisis parciales complejas 1. Inicio parcial simple 2. Parcial compleja desde el inicio
C. Crisis parciales secundariamente generalizadas 1. Parciales simples con GS. 2. Parciales complejas con GS. 3. Parcial simple, luego parcial compleja y GS
Clasificación internacional de crisis epilépticas (ILAE 1981) II. Crisis generalizadas
A. Ausencias
B. Mioclónicas
C. Clónicas
D. Tónicas
E. Tónico-clónicas
F. Atónicas
III. Crisis no clasificables.
¤ Etiología
¤ Idiopáticas
¤ Sintomáticas
¤ Criptogénicas
¤ Localización:
¤ Síndromes epilépticos
relacionados con la localización
¤ Síndromes epilépticos
generalizados
¤ Síndromes epilépticos de
localización indeterminada
¤ Síndromes especiales
Clasificación de 1989
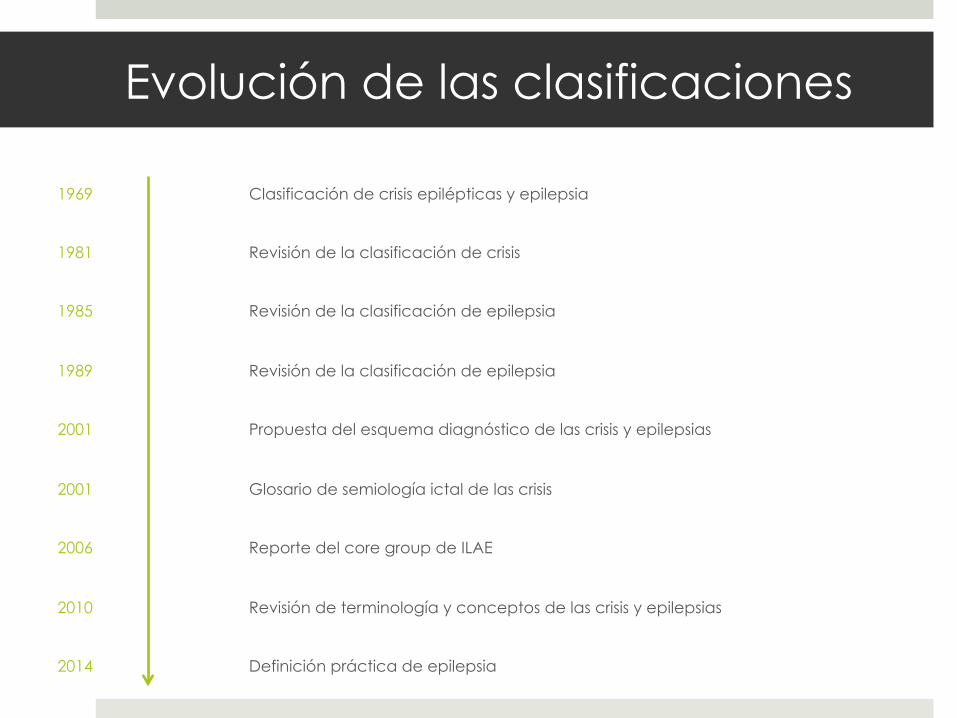
Evolución de las clasificaciones
1969 Clasificación de crisis epilépticas y epilepsia
1981 Revisión de la clasificación de crisis
1985 Revisión de la clasificación de epilepsia
1989 Revisión de la clasificación de epilepsia
2001 Propuesta del esquema diagnóstico de las crisis y epilepsias
2001 Glosario de semiología ictal de las crisis
2006 Reporte del core group de ILAE
2010 Revisión de terminología y conceptos de las crisis y epilepsias
2014 Definición práctica de epilepsia
Crisis epilépticas Semiología de las crisis
¤ Cuándo sospecharlas:
¤ Inicio abrupto
¤ Patrón estereotipado
¤ Eventos involuntarios e incontrolables, breves
¤ Fin abrupto y generalmente reconocible
¤ Conductas ictales no propositivas
¤ Compromiso post ictal: amnesia, sueño, alteraciones
neurológicas transitorias.
Crisis epilépticas
Epilepsia y crisis epilépticas
¤ Crisis Tónico clónico generalizadas:
¤ Involucran el tronco y probablemente el córtex prefrontal y
ganglios basales.
¤ Inicialmente existen mecanismos desinhibitorios (fase tónica)
con posterior instalación periódica de mecanismos
inhibitorios (fase clónica).
¤ En algunos casos, pueden precederse por mioclonías (crisis
clónico-tónico-clónicas)
Engel J. Report of the ILAE Classification Core Group. Epilepsia, 47(9):1558–1568, 2006
Epilepsia y crisis epilépticas
¤ Crisis mioclónicas:
¤ Contracción muscular súbita, breve (<350 ms).
¤ Pueden ser generalizadas, en la cara o en 1 o más
extremidades.
¤ Más breves que las clonías y no son rítmicas.
¤ Ocasionalmente ocasionan caídas (crisis astáticas)
¤ Compromiso de conciencia?
¤ Correlato EEG con actividad espiga o poliespiga onda
generalizada.
Engel J. Report of the ILAE Classification Core Group. Epilepsia, 47(9):1558–1568, 2006
Epilepsia y crisis epilépticas
¤ Espasmos epilépticos:
¤ Habitualmente en lactantes menores.
¤ Contracción muscular de predominio axial.
¤ 2 fases: rápida de contracción y lenta de relajación
¤ Pueden ser en flexión, extensión o mixtos.
¤ Característicamente en salvas con diferencias de <1 minuto.
¤ Predominio al despertar.
¤ Característicos del síndrome de West.
Engel J. Report of the ILAE Classification Core Group. Epilepsia, 47(9):1558–1568, 2006

Epilepsia y crisis epilépticas
¤ Atónicas:
¤ Pérdida súbita del tono muscular
¤ Pueden provocar caídas
¤ Compromiso de conciencia breve
¤ Pueden asociarse a mioclonías (crisis mioclónico astáticas)
¤ Correlato EEG con actividad espiga onda lenta a 1 o más
Hz o bien con una onda lenta generalizada seguida de
depresión de voltaje.
Engel J. Report of the ILAE Classification Core Group. Epilepsia, 47(9):1558–1568, 2006
Epilepsia y crisis epilépticas
¤ Ausencias:
¤ Cese brusco y breve de las actividades.
¤ Mirada fija (“perdida”).
¤ Frecuentes automatismos motores (parpadeo, “chupeteo”)
¤ Difícil distinción con crisis parciales complejas (Frontales)
¤ A veces en contexto de síndromes específicos.
¤ Correlato EEG: actividad espiga onda lenta a 3 cps.
Engel J. Report of the ILAE Classification Core Group. Epilepsia, 47(9):1558–1568, 2006

Exámenes complementarios
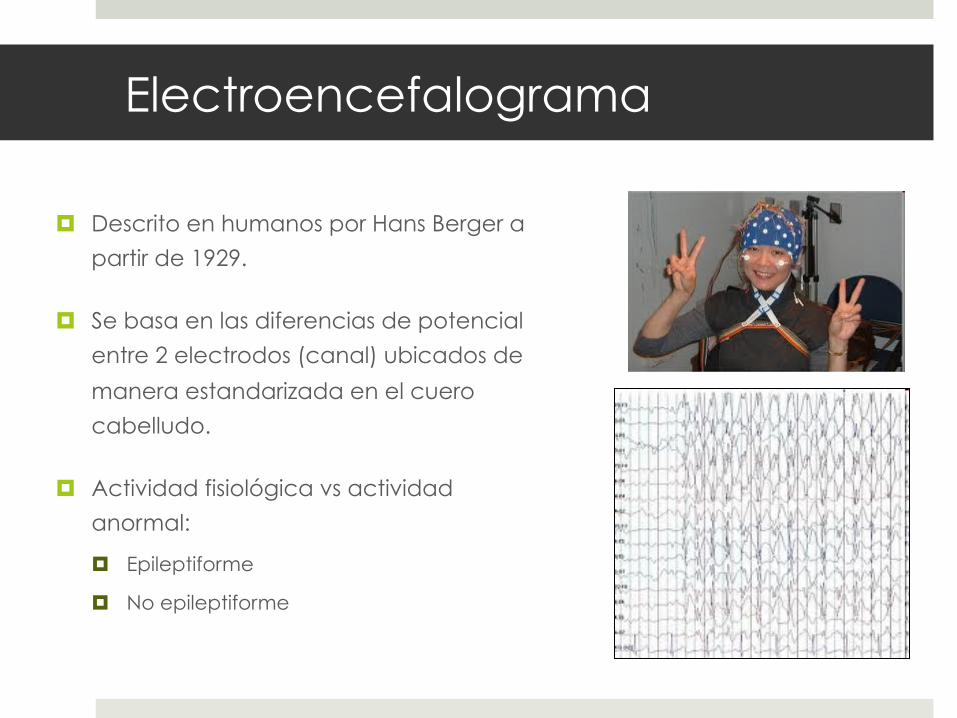
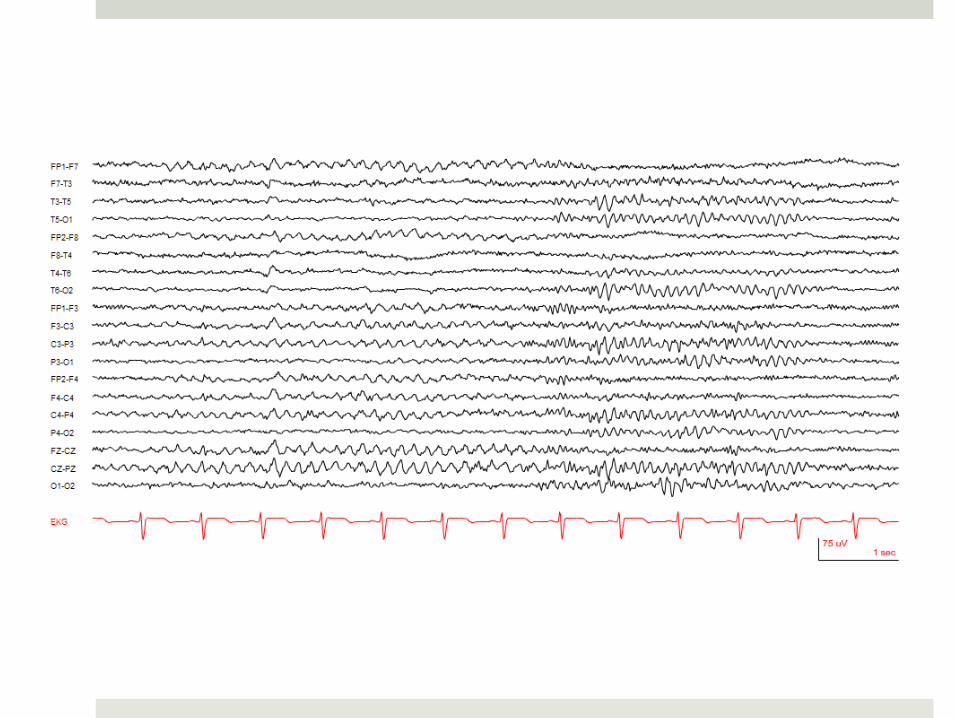
¤ Descrito en humanos por Hans Berger a
partir de 1929.
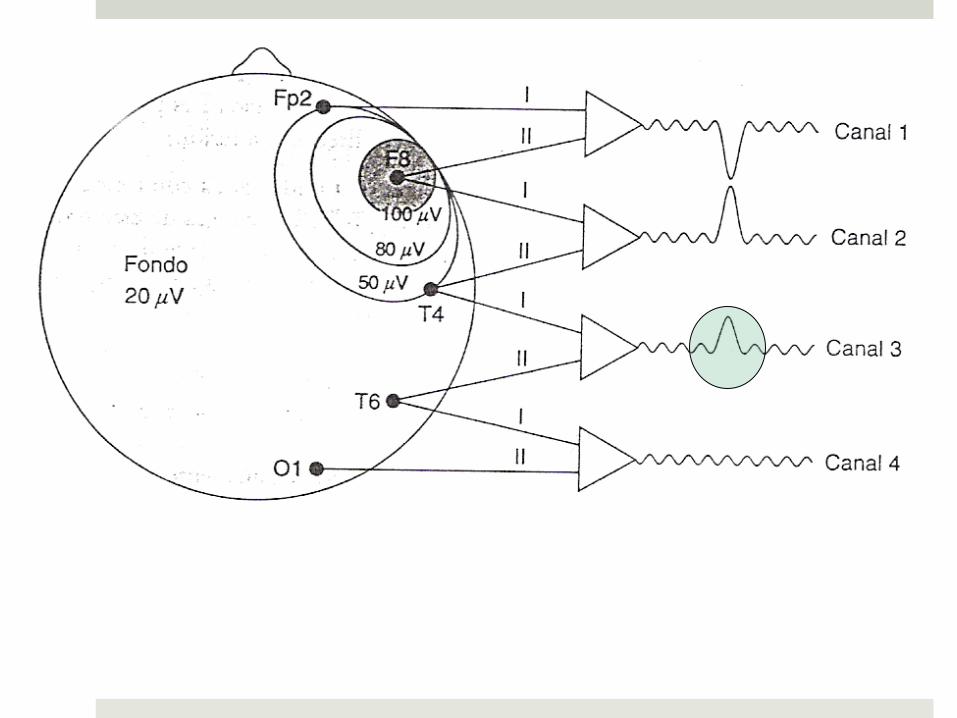
¤ Se basa en las diferencias de potencial
entre 2 electrodos (canal) ubicados de
manera estandarizada en el cuero
cabelludo.
¤ Actividad fisiológica vs actividad
anormal:
¤ Epileptiforme
¤ No epileptiforme
Electroencefalograma
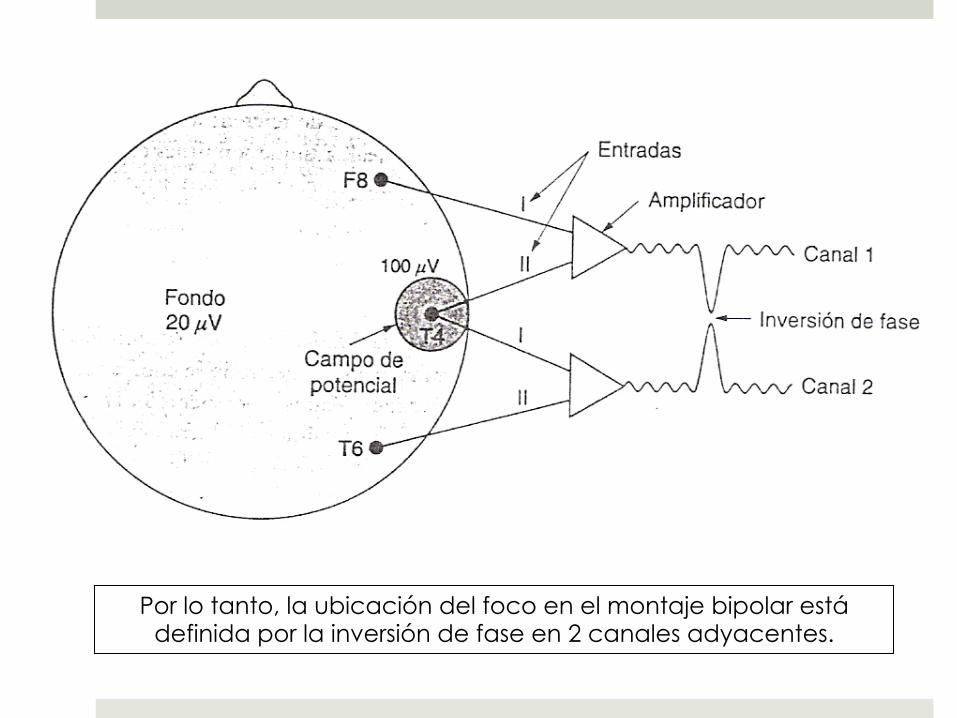
Por lo tanto, la ubicación del foco en el montaje bipolar está definida por la inversión de fase en 2 canales adyacentes.
Electroencefalograma
¤ No “hace” el diagnóstico de epilepsia.
¤ Primer EEG standard en crisis focales: sensibilidad 50%.
¤ La sensibilidad es de 84% con el 3er EEG y 92% con el 4to.
¤ Otros factores: edad temprana, EEG de sueño, epilepsia generalizada y
registro post crisis.
¤ Espigas focales en regiones inferiores o mesiales pueden no verse en EEG
de superficie.
¤ EEG continuamente normales levantan la sospecha de un TPNE.
¤ Procedimientos de activación aumentan la
sensibilidad:
¤ EFI y HV: aumentan probabilidad de encontrar descargas
generalizadas.
¤ Privación de sueño: aumenta la probabilidad de encontrar
anomalías focales.
La privación de sueño por sí misma es activadora.
Electroencefalograma
¤ Incidencia de 2 a 4% de alteraciones epileptiformes en
pacientes sin epilepsia.
¤ Esto puede aumentar hasta un 25% en pacientes estudiados
por TDAH.
¤ La mayoría presentan actividad epileptiforme de tipo
benigna (alto % centrotemporales).
Frequency of Epileptiform Discharges in the Sleep-Deprived Electroencephalogram in Children Evaluated for Attention-Deficit Disorders. Journal of Child Neurology 26(1) 6-11. 2011.
Electroencefalograma
Seminars in Neurology, Volume 23, Number 1, 2003
Special Article
CME Practice parameter: Evaluating afirst nonfebrile seizure in children
Report of the Quality Standards Subcommittee of theAmerican Academy of Neurology, the Child Neurology
Society, and the American Epilepsy SocietyD. Hirtz, MD; S. Ashwal, MD; A. Berg, PhD; D. Bettis, MD; C. Camfield, MD; P. Camfield, MD;
P. Crumrine, MD; R. Elterman, MD; S. Schneider, MD; and S. Shinnar, MD, PhD
Article abstract—Objective: The Quality Standards Subcommittee of the American Academy of Neurology developspractice parameters as strategies for patient management based on analysis of evidence. For this practice parameter, theauthors reviewed available evidence on evaluation of the first nonfebrile seizure in children in order to make practicerecommendations based on this available evidence. Methods: Multiple searches revealed relevant literature and eacharticle was reviewed, abstracted, and classified. Recommendations were based on a three-tiered scheme of classification ofthe evidence. Results: Routine EEG as part of the diagnostic evaluation was recommended; other studies such aslaboratory evaluations and neuroimaging studies were recommended as based on specific clinical circumstances. Conclu-sions: Further studies are needed using large, well-characterized samples and standardized data collection instruments.Collection of data regarding appropriate timing of evaluations would be important.NEUROLOGY 2000;55:616–623
The Quality Standards Subcommittee (QSS) of theAmerican Academy of Neurology (AAN) seeks to de-velop scientifically sound, clinically relevant practiceparameters for physicians for diagnostic procedures,treatment modalities, and clinical disorders. Practiceparameters are strategies for patient managementthat might include diagnosis, symptom, treatment,or procedure evaluation. They consist of one or morespecific recommendations based on the analysis ofevidence.
Every year, an estimated 25,000 to 40,000 USchildren experience their first nonfebrile seizure, adramatic and frightening event.1-4 This practice pa-rameter reviews available evidence concerning thevalue of diagnostic testing after a first nonfebrileseizure in a child, and provides recommendationsbased on this evidence. It addresses the evaluation ofchildren age 1 month to 21 years who have experi-enced a first nonfebrile seizure that cannot be ex-
plained by an immediate, obvious provoking causesuch as head trauma or intracranial infection. Re-ports concerning serum laboratory studies, CSF ex-amination, EEG, CT, and MRI are reviewed. Thisparameter concerns diagnostic evaluation; a subse-quent parameter will focus on treatment of the firstnonfebrile seizure.
The seizure types covered by this parameter in-clude partial (simple or complex partial, or partialwith secondary generalization), generalized tonic-clonic, or tonic seizures. We are specifically not in-cluding children diagnosed with epilepsy, defined astwo or more seizures without acute provocation. Forthis reason, myoclonic and atonic seizures are ex-cluded because they typically are not recognized un-til there have been multiple occurrences. We definedthe first seizure using the International LeagueAgainst Epilepsy (ILAE) criteria to include multipleseizures within 24 hours with recovery of conscious-
From the National Institute of Neurological Disorders and Stroke (Dr. Hirtz), National Institutes of Health, Bethesda, MD; Department of Pediatrics (Dr.Ashwal), Loma Linda University School of Medicine, Loma Linda, CA; Department of Biological Sciences (Dr. Berg), Northern Illinois University, Dekalb; Dr.David Bettis, Boise, ID; Department of Pediatric Neurology (Drs. C. Camfield and P. Camfield), IW Killam Hospital for Children, Halifax, Nova Scotia;Department of Neurology (Dr. Crumrine), Children’s Hospital of Pittsburgh, PA; Dr. Roy Elterman, Dallas, TX; Dr. Sanford Schneider, Riverside, CA; andthe Departments of Neurology and Pediatrics (Dr. Shinnar), Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY.Approved by the Quality Standards Subcommittee April 1, 2000. Approved by the Practice Committee May 3, 2000. Approved by the AAN Board of DirectorsJune 9, 2000.Received September 27, 1999. Accepted in final form June 13, 2000.Address correspondence and reprint requests to QSS, American Academy of Neurology, 1080 Montreal Avenue, St. Paul, MN 55116; phone: 800-879-1960
616 Copyright © 2000 by AAN Enterprises, Inc.
zure patients.40,41 In these studies, interpretationwas difficult in the presence of diffuse postictal slow-ing,42 and an EEG done at that time was not helpfulin determining which patients should be admitted tothe hospital.40
A recent analysis of selected findings from severalof the Class I studies referred to above25-27,30,31 con-cluded that an EEG should not be routinely per-formed after a first seizure because it does not yieldsufficient information to alter treatment decisions.43
To reach this conclusion, the authors did not con-sider evidence that the EEG result does in fact altertreatment decisions. They assumed a treatmentthreshold to be at an 80% risk of recurrence, andused a univariate analysis. However, where the EEGis used as one of several variables, it can identifychildren with very high and very low recurrencerisks.25,26,32,35 The EEG is not used solely to determinerecurrence, but also helps differentiate a seizurefrom other events, is essential to the diagnosis of asyndrome, and provides information on long-termprognosis; it influences the decision to perform sub-sequent neuroimaging studies44 and may influencecounseling about management of the child.
Conclusions. The majority of evidence from ClassI and Class II studies confirms that an EEG helps indetermination of seizure type, epilepsy syndrome,and risk for recurrence, and therefore may affectfurther management decisions. Experts commonlyrecommend that an EEG be performed after all firstnonfebrile seizures.39,45-47 It is not clear what the op-timal timing should be for obtaining an EEG. Al-though an EEG done within 24 hours of the seizureis most likely to show abnormalities,34 physiciansshould be aware that some abnormalities such aspostictal slowing that can be seen on EEG donewithin 24 to 48 hours of a seizure may be transientand must be interpreted with caution.
There is no evidence that the EEG must be donebefore discharge from the emergency department;the study may be arranged on an outpatient basis.Epileptiform EEG abnormalities may be useful inconfirming that the event was a seizure; however, anEEG abnormality by itself is not sufficient to make adiagnosis that an epileptic seizure occurred, nor canits absence rule out a seizure.46,47 The EEG is neces-sary to determine the epilepsy syndrome and thediagnosis of an epilepsy syndrome may be helpful indetermining the need for imaging studies.34 The EEGis also useful in predicting the prognosis forrecurrences.20,39,45-47
It is not clear what the optimal timing should befor obtaining an EEG. Although an EEG done within24 hours of the seizure is most likely to show abnor-malities, physicians should be aware that some ab-normalities such as postictal slowing that can beseen on EEG done within 24 to 48 hours of a seizuremay be transient and must be interpreted withcaution.
Recommendations.
• The EEG is recommended as part of the neurodi-agnostic evaluation of the child with an apparentfirst unprovoked seizure. (Standard)
Neuroimaging studies. Evidence—CT scans.There were five Class I studies regarding imaging byCT scan after a first seizure; the data pertained tochildren32 and adults24,42,48 with first seizures, and toadults and children over age 6 with both new onsetand established seizures.14 In the single Class Istudy of first seizures in children, the abnormalities(mostly atrophy) found in 12 children were “withouttherapeutic consequences” (95% CI 0, 3%).32 In one ofthe adult studies, 1.3% of the patients who had CTscans were diagnosed with tumors,24 and in another,of 62 patients there were three tumors seen on CT,all in patients with abnormal neurologic examina-tions.42 Of 119 adults who had CT scans after a firstgeneralized seizure, 20 had abnormalities that war-ranted therapeutic intervention.48 In the Class Istudy in which 19 CT scans were done in selectivecases (first seizures if greater than age 6 years, headtrauma, or focal seizure), there was one significantabnormality (age of the patient was not given), asubdural hematoma, not predicted by history andphysical examination.14
Of the 14 Class II studies, nine involved childrenonly (n ! 2559),17,19,49-56 four were of adults only (n !666),24,42,57,58 and one involved children and adults(n ! 109).59 Only a small percentage of children inthese studies (0 to 7%) had lesions on CT that al-tered or influenced management. These were mostcommonly brain tumors, communicating or obstruc-tive hydrocephalus, one subarachnoid and one poren-cephalic cyst, and three children with cysticercosis.The yield of abnormality on CT when the neurologicexamination and EEG were normal was 5 to 10%.50,54
In a Class II study in which seven children (14% ofchildren with nonfebrile seizures) had CT scans thatinfluenced management, five had focal or complexpartial seizures. Abnormalities on neuroimagingwere associated with a higher recurrence risk.54 Inone study of febrile and nonfebrile children, CTscans were always normal in the absence of de-fined risk factors such as known neurologic diagno-sis, age "5 months, or focal deficit.57 Focal lesions onCT scans tended to be more commonly found inadults (18 to 34%)40,48,57,58 than in children (0 to12%),17,32,49,52,54-56 particularly when ordered for spe-cific clinical indications. At least three studies pro-vided evidence that MRI scanning was preferable toCT51,54,60 in children following nonfebrile seizures.
Evidence—MRI. There was one Class I report re-garding MRI in children presenting with a first sei-zure54 and another Class I report of newly diagnosedepilepsy in children.60 Of 411 children who presentedwith a first seizure, 218 had neuroimaging studies.Four had lesions seen on MRI or CT (two brain tu-mors, two neurocysticercosis) that potentially altered
September (1 of 2) 2000 NEUROLOGY 55 619
Special Article
CME Practice parameter: Evaluating afirst nonfebrile seizure in children
Report of the Quality Standards Subcommittee of theAmerican Academy of Neurology, the Child Neurology
Society, and the American Epilepsy SocietyD. Hirtz, MD; S. Ashwal, MD; A. Berg, PhD; D. Bettis, MD; C. Camfield, MD; P. Camfield, MD;
P. Crumrine, MD; R. Elterman, MD; S. Schneider, MD; and S. Shinnar, MD, PhD
Article abstract—Objective: The Quality Standards Subcommittee of the American Academy of Neurology developspractice parameters as strategies for patient management based on analysis of evidence. For this practice parameter, theauthors reviewed available evidence on evaluation of the first nonfebrile seizure in children in order to make practicerecommendations based on this available evidence. Methods: Multiple searches revealed relevant literature and eacharticle was reviewed, abstracted, and classified. Recommendations were based on a three-tiered scheme of classification ofthe evidence. Results: Routine EEG as part of the diagnostic evaluation was recommended; other studies such aslaboratory evaluations and neuroimaging studies were recommended as based on specific clinical circumstances. Conclu-sions: Further studies are needed using large, well-characterized samples and standardized data collection instruments.Collection of data regarding appropriate timing of evaluations would be important.NEUROLOGY 2000;55:616–623
The Quality Standards Subcommittee (QSS) of theAmerican Academy of Neurology (AAN) seeks to de-velop scientifically sound, clinically relevant practiceparameters for physicians for diagnostic procedures,treatment modalities, and clinical disorders. Practiceparameters are strategies for patient managementthat might include diagnosis, symptom, treatment,or procedure evaluation. They consist of one or morespecific recommendations based on the analysis ofevidence.
Every year, an estimated 25,000 to 40,000 USchildren experience their first nonfebrile seizure, adramatic and frightening event.1-4 This practice pa-rameter reviews available evidence concerning thevalue of diagnostic testing after a first nonfebrileseizure in a child, and provides recommendationsbased on this evidence. It addresses the evaluation ofchildren age 1 month to 21 years who have experi-enced a first nonfebrile seizure that cannot be ex-
plained by an immediate, obvious provoking causesuch as head trauma or intracranial infection. Re-ports concerning serum laboratory studies, CSF ex-amination, EEG, CT, and MRI are reviewed. Thisparameter concerns diagnostic evaluation; a subse-quent parameter will focus on treatment of the firstnonfebrile seizure.
The seizure types covered by this parameter in-clude partial (simple or complex partial, or partialwith secondary generalization), generalized tonic-clonic, or tonic seizures. We are specifically not in-cluding children diagnosed with epilepsy, defined astwo or more seizures without acute provocation. Forthis reason, myoclonic and atonic seizures are ex-cluded because they typically are not recognized un-til there have been multiple occurrences. We definedthe first seizure using the International LeagueAgainst Epilepsy (ILAE) criteria to include multipleseizures within 24 hours with recovery of conscious-
From the National Institute of Neurological Disorders and Stroke (Dr. Hirtz), National Institutes of Health, Bethesda, MD; Department of Pediatrics (Dr.Ashwal), Loma Linda University School of Medicine, Loma Linda, CA; Department of Biological Sciences (Dr. Berg), Northern Illinois University, Dekalb; Dr.David Bettis, Boise, ID; Department of Pediatric Neurology (Drs. C. Camfield and P. Camfield), IW Killam Hospital for Children, Halifax, Nova Scotia;Department of Neurology (Dr. Crumrine), Children’s Hospital of Pittsburgh, PA; Dr. Roy Elterman, Dallas, TX; Dr. Sanford Schneider, Riverside, CA; andthe Departments of Neurology and Pediatrics (Dr. Shinnar), Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY.Approved by the Quality Standards Subcommittee April 1, 2000. Approved by the Practice Committee May 3, 2000. Approved by the AAN Board of DirectorsJune 9, 2000.Received September 27, 1999. Accepted in final form June 13, 2000.Address correspondence and reprint requests to QSS, American Academy of Neurology, 1080 Montreal Avenue, St. Paul, MN 55116; phone: 800-879-1960
616 Copyright © 2000 by AAN Enterprises, Inc.
zure patients.40,41 In these studies, interpretationwas difficult in the presence of diffuse postictal slow-ing,42 and an EEG done at that time was not helpfulin determining which patients should be admitted tothe hospital.40
A recent analysis of selected findings from severalof the Class I studies referred to above25-27,30,31 con-cluded that an EEG should not be routinely per-formed after a first seizure because it does not yieldsufficient information to alter treatment decisions.43
To reach this conclusion, the authors did not con-sider evidence that the EEG result does in fact altertreatment decisions. They assumed a treatmentthreshold to be at an 80% risk of recurrence, andused a univariate analysis. However, where the EEGis used as one of several variables, it can identifychildren with very high and very low recurrencerisks.25,26,32,35 The EEG is not used solely to determinerecurrence, but also helps differentiate a seizurefrom other events, is essential to the diagnosis of asyndrome, and provides information on long-termprognosis; it influences the decision to perform sub-sequent neuroimaging studies44 and may influencecounseling about management of the child.
Conclusions. The majority of evidence from ClassI and Class II studies confirms that an EEG helps indetermination of seizure type, epilepsy syndrome,and risk for recurrence, and therefore may affectfurther management decisions. Experts commonlyrecommend that an EEG be performed after all firstnonfebrile seizures.39,45-47 It is not clear what the op-timal timing should be for obtaining an EEG. Al-though an EEG done within 24 hours of the seizureis most likely to show abnormalities,34 physiciansshould be aware that some abnormalities such aspostictal slowing that can be seen on EEG donewithin 24 to 48 hours of a seizure may be transientand must be interpreted with caution.
There is no evidence that the EEG must be donebefore discharge from the emergency department;the study may be arranged on an outpatient basis.Epileptiform EEG abnormalities may be useful inconfirming that the event was a seizure; however, anEEG abnormality by itself is not sufficient to make adiagnosis that an epileptic seizure occurred, nor canits absence rule out a seizure.46,47 The EEG is neces-sary to determine the epilepsy syndrome and thediagnosis of an epilepsy syndrome may be helpful indetermining the need for imaging studies.34 The EEGis also useful in predicting the prognosis forrecurrences.20,39,45-47
It is not clear what the optimal timing should befor obtaining an EEG. Although an EEG done within24 hours of the seizure is most likely to show abnor-malities, physicians should be aware that some ab-normalities such as postictal slowing that can beseen on EEG done within 24 to 48 hours of a seizuremay be transient and must be interpreted withcaution.
Recommendations.
• The EEG is recommended as part of the neurodi-agnostic evaluation of the child with an apparentfirst unprovoked seizure. (Standard)
Neuroimaging studies. Evidence—CT scans.There were five Class I studies regarding imaging byCT scan after a first seizure; the data pertained tochildren32 and adults24,42,48 with first seizures, and toadults and children over age 6 with both new onsetand established seizures.14 In the single Class Istudy of first seizures in children, the abnormalities(mostly atrophy) found in 12 children were “withouttherapeutic consequences” (95% CI 0, 3%).32 In one ofthe adult studies, 1.3% of the patients who had CTscans were diagnosed with tumors,24 and in another,of 62 patients there were three tumors seen on CT,all in patients with abnormal neurologic examina-tions.42 Of 119 adults who had CT scans after a firstgeneralized seizure, 20 had abnormalities that war-ranted therapeutic intervention.48 In the Class Istudy in which 19 CT scans were done in selectivecases (first seizures if greater than age 6 years, headtrauma, or focal seizure), there was one significantabnormality (age of the patient was not given), asubdural hematoma, not predicted by history andphysical examination.14
Of the 14 Class II studies, nine involved childrenonly (n ! 2559),17,19,49-56 four were of adults only (n !666),24,42,57,58 and one involved children and adults(n ! 109).59 Only a small percentage of children inthese studies (0 to 7%) had lesions on CT that al-tered or influenced management. These were mostcommonly brain tumors, communicating or obstruc-tive hydrocephalus, one subarachnoid and one poren-cephalic cyst, and three children with cysticercosis.The yield of abnormality on CT when the neurologicexamination and EEG were normal was 5 to 10%.50,54
In a Class II study in which seven children (14% ofchildren with nonfebrile seizures) had CT scans thatinfluenced management, five had focal or complexpartial seizures. Abnormalities on neuroimagingwere associated with a higher recurrence risk.54 Inone study of febrile and nonfebrile children, CTscans were always normal in the absence of de-fined risk factors such as known neurologic diagno-sis, age "5 months, or focal deficit.57 Focal lesions onCT scans tended to be more commonly found inadults (18 to 34%)40,48,57,58 than in children (0 to12%),17,32,49,52,54-56 particularly when ordered for spe-cific clinical indications. At least three studies pro-vided evidence that MRI scanning was preferable toCT51,54,60 in children following nonfebrile seizures.
Evidence—MRI. There was one Class I report re-garding MRI in children presenting with a first sei-zure54 and another Class I report of newly diagnosedepilepsy in children.60 Of 411 children who presentedwith a first seizure, 218 had neuroimaging studies.Four had lesions seen on MRI or CT (two brain tu-mors, two neurocysticercosis) that potentially altered
September (1 of 2) 2000 NEUROLOGY 55 619

¤ Indicadas ante sospecha de epilepsias focales.
¤ Examen neurológico alterado
¤ Epilepsias de muy dificil manejo
¤ Cambios en el patrón habitual de crisis.
¤ Existe:
¤ Resonancia magnética
¤ Tomografía axial computada (TAC)
¤ Otras técnicas
Neuroimágenes
Special Article
CME Practice parameter: Evaluating afirst nonfebrile seizure in children
Report of the Quality Standards Subcommittee of theAmerican Academy of Neurology, the Child Neurology
Society, and the American Epilepsy SocietyD. Hirtz, MD; S. Ashwal, MD; A. Berg, PhD; D. Bettis, MD; C. Camfield, MD; P. Camfield, MD;
P. Crumrine, MD; R. Elterman, MD; S. Schneider, MD; and S. Shinnar, MD, PhD
Article abstract—Objective: The Quality Standards Subcommittee of the American Academy of Neurology developspractice parameters as strategies for patient management based on analysis of evidence. For this practice parameter, theauthors reviewed available evidence on evaluation of the first nonfebrile seizure in children in order to make practicerecommendations based on this available evidence. Methods: Multiple searches revealed relevant literature and eacharticle was reviewed, abstracted, and classified. Recommendations were based on a three-tiered scheme of classification ofthe evidence. Results: Routine EEG as part of the diagnostic evaluation was recommended; other studies such aslaboratory evaluations and neuroimaging studies were recommended as based on specific clinical circumstances. Conclu-sions: Further studies are needed using large, well-characterized samples and standardized data collection instruments.Collection of data regarding appropriate timing of evaluations would be important.NEUROLOGY 2000;55:616–623
The Quality Standards Subcommittee (QSS) of theAmerican Academy of Neurology (AAN) seeks to de-velop scientifically sound, clinically relevant practiceparameters for physicians for diagnostic procedures,treatment modalities, and clinical disorders. Practiceparameters are strategies for patient managementthat might include diagnosis, symptom, treatment,or procedure evaluation. They consist of one or morespecific recommendations based on the analysis ofevidence.
Every year, an estimated 25,000 to 40,000 USchildren experience their first nonfebrile seizure, adramatic and frightening event.1-4 This practice pa-rameter reviews available evidence concerning thevalue of diagnostic testing after a first nonfebrileseizure in a child, and provides recommendationsbased on this evidence. It addresses the evaluation ofchildren age 1 month to 21 years who have experi-enced a first nonfebrile seizure that cannot be ex-
plained by an immediate, obvious provoking causesuch as head trauma or intracranial infection. Re-ports concerning serum laboratory studies, CSF ex-amination, EEG, CT, and MRI are reviewed. Thisparameter concerns diagnostic evaluation; a subse-quent parameter will focus on treatment of the firstnonfebrile seizure.
The seizure types covered by this parameter in-clude partial (simple or complex partial, or partialwith secondary generalization), generalized tonic-clonic, or tonic seizures. We are specifically not in-cluding children diagnosed with epilepsy, defined astwo or more seizures without acute provocation. Forthis reason, myoclonic and atonic seizures are ex-cluded because they typically are not recognized un-til there have been multiple occurrences. We definedthe first seizure using the International LeagueAgainst Epilepsy (ILAE) criteria to include multipleseizures within 24 hours with recovery of conscious-
From the National Institute of Neurological Disorders and Stroke (Dr. Hirtz), National Institutes of Health, Bethesda, MD; Department of Pediatrics (Dr.Ashwal), Loma Linda University School of Medicine, Loma Linda, CA; Department of Biological Sciences (Dr. Berg), Northern Illinois University, Dekalb; Dr.David Bettis, Boise, ID; Department of Pediatric Neurology (Drs. C. Camfield and P. Camfield), IW Killam Hospital for Children, Halifax, Nova Scotia;Department of Neurology (Dr. Crumrine), Children’s Hospital of Pittsburgh, PA; Dr. Roy Elterman, Dallas, TX; Dr. Sanford Schneider, Riverside, CA; andthe Departments of Neurology and Pediatrics (Dr. Shinnar), Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY.Approved by the Quality Standards Subcommittee April 1, 2000. Approved by the Practice Committee May 3, 2000. Approved by the AAN Board of DirectorsJune 9, 2000.Received September 27, 1999. Accepted in final form June 13, 2000.Address correspondence and reprint requests to QSS, American Academy of Neurology, 1080 Montreal Avenue, St. Paul, MN 55116; phone: 800-879-1960
616 Copyright © 2000 by AAN Enterprises, Inc.
on long-term treatment and management.20,22 Fac-tors to be considered include the age of the child, theneed for sedation to perform the study, the EEGresults, a history of head trauma, and other clinicalcircumstances such as a family history of epilepsy.
Recommendations.
• If a neuroimaging study is obtained, MRI is thepreferred modality.50,51,54,60,62,63,65 (Guideline)
Emergent neuroimaging should be performed in achild of any age who exhibits a postictal focal deficit(Todd’s paresis) not quickly resolving, or who has notreturned to baseline within several hours after theseizure.46,66 (Option)
• Nonurgent imaging studies with MRI should beseriously considered in any child with a significantcognitive or motor impairment of unknown etiol-ogy, unexplained abnormalities on neurologic ex-amination, a seizure of partial (focal) onset with orwithout secondary generalization, an EEG thatdoes not represent a benign partial epilepsy ofchildhood or primary generalized epilepsy, or inchildren under 1 year of age.20,34 (Option)
Summary. In the child with a first nonfebrile sei-zure, diagnostic evaluations influence therapeuticdecisions, how families are counseled, and the needfor hospital admission and/or specific follow-upplans. This practice parameter has reviewed thepublished literature concerning the usefulness ofstudies following a first nonfebrile seizure in chil-dren, and has classified the strength of the availableevidence. There is sufficient Class I evidence, whichinvolves a well executed prospective study, to pro-vide a recommendation with the highest degree ofclinical certainty—i.e., a Standard—that an EEG beobtained in all children in whom a nonfebrile seizurehas been diagnosed, to predict the risk of recurrenceand to classify the seizure type and epilepsy syn-drome. The decision to perform other studies, includ-ing LP, laboratory tests, and neuroimaging, for thepurpose of determining the cause of the seizure anddetecting potentially treatable abnormalities, willdepend on the age of the patient and the specificclinical circumstances. Children of different agesmay require different management strategies.20,22
Future research. For most of the questions ad-dressed by this parameter, evidence was insufficientfor making a strong recommendation for a standardor guideline, particularly for laboratory studies. Inorder to generate definitive evidence regarding thevalue of routine (or selective) laboratory testing andthe use of routine neuroimaging studies, sufficientlylarge samples allowing for adequate statistical powerto provide precise estimates (i.e., with narrow confi-dence intervals) are needed. Neuroimaging studiesare needed to understand the significance of neuro-nal migration defects in the context of a first seizure,and are important because of the improved technical
ability of current MRI. In addition, prospective col-lection of data using standardized treatment proto-cols and standardized data collection instruments isessential. Results of studies will only be helpful ifthe patient sample and factors that resulted in inclu-sion into or exclusion from the sample are well de-scribed and documented. Ideally, large consecutiveseries of well-characterized patients are needed forthe results to be accurate and generalizable. Finally,future studies should present separate data fromchildren and adults, and it would be optimal for re-sults in children to be presented by age groupings.
Appropriate timing as well as the choice of evalu-ative studies have not been adequately studied. Chil-dren may present as actively having a seizure whenbrought to the emergency department, as postictal,or as alert with a history of a possible seizure epi-sode having occurred hours, days, or weeks previ-ously. Data regarding the appropriate timing oflaboratory testing, neuroimaging, or EEG studies re-quire adequate prospective studies of these specificquestions, with clearly defined entry criteria and acommon protocol for type and timing of evaluations.
Research studies with adequate sample sizes andappropriate protocols that provide answers to thesequestions may serve to reduce the expense and dis-comfort of unnecessary testing in children with firstseizures, and, more importantly, by identifying ap-propriate candidates, may improve the care andmanagement that these children receive.
Disclaimer. This statement is provided as an edu-cational service of the American Academy of Neurol-ogy. It is based on an assessment of current scientificand clinical information. It is not intended to includeall possible proper methods of care for a particularneurologic problem or all legitimate criteria forchoosing to use a specific procedure. Neither is itintended to exclude any reasonable alternativemethodologies. The AAN recognizes that specific pa-tient care decisions are the prerogative of the patientand the physician caring for the patient, based on allof the circumstances involved.
AcknowledgmentThe authors thank the members of the Quality Standards Sub-committee of the AAN, and Wendy Edlund, the AAN ClinicalPolicy Administrator, for their time, expertise, and efforts in de-veloping this document.
Appendix 1Classification of evidence
Class I. Must have all of a–d:a. Prospective study of a well defined cohort which includes a
description of the nature of the population, the inclusion/exclusioncriteria, demographic characteristics such as age and sex, andseizure type.
b. The sample size must be adequate with enough statisticalpower to justify a conclusion or for identification of subgroups forwhom testing does or does not yield significant information.
c. The interpretation of evaluations performed must be doneblinded to outcome.
d. There must be a satisfactory description of the technologyused for evaluations (e.g., EEG, MRI).
September (1 of 2) 2000 NEUROLOGY 55 621
Special Article
CME Practice parameter: Evaluating afirst nonfebrile seizure in children
Report of the Quality Standards Subcommittee of theAmerican Academy of Neurology, the Child Neurology
Society, and the American Epilepsy SocietyD. Hirtz, MD; S. Ashwal, MD; A. Berg, PhD; D. Bettis, MD; C. Camfield, MD; P. Camfield, MD;
P. Crumrine, MD; R. Elterman, MD; S. Schneider, MD; and S. Shinnar, MD, PhD
Article abstract—Objective: The Quality Standards Subcommittee of the American Academy of Neurology developspractice parameters as strategies for patient management based on analysis of evidence. For this practice parameter, theauthors reviewed available evidence on evaluation of the first nonfebrile seizure in children in order to make practicerecommendations based on this available evidence. Methods: Multiple searches revealed relevant literature and eacharticle was reviewed, abstracted, and classified. Recommendations were based on a three-tiered scheme of classification ofthe evidence. Results: Routine EEG as part of the diagnostic evaluation was recommended; other studies such aslaboratory evaluations and neuroimaging studies were recommended as based on specific clinical circumstances. Conclu-sions: Further studies are needed using large, well-characterized samples and standardized data collection instruments.Collection of data regarding appropriate timing of evaluations would be important.NEUROLOGY 2000;55:616–623
The Quality Standards Subcommittee (QSS) of theAmerican Academy of Neurology (AAN) seeks to de-velop scientifically sound, clinically relevant practiceparameters for physicians for diagnostic procedures,treatment modalities, and clinical disorders. Practiceparameters are strategies for patient managementthat might include diagnosis, symptom, treatment,or procedure evaluation. They consist of one or morespecific recommendations based on the analysis ofevidence.
Every year, an estimated 25,000 to 40,000 USchildren experience their first nonfebrile seizure, adramatic and frightening event.1-4 This practice pa-rameter reviews available evidence concerning thevalue of diagnostic testing after a first nonfebrileseizure in a child, and provides recommendationsbased on this evidence. It addresses the evaluation ofchildren age 1 month to 21 years who have experi-enced a first nonfebrile seizure that cannot be ex-
plained by an immediate, obvious provoking causesuch as head trauma or intracranial infection. Re-ports concerning serum laboratory studies, CSF ex-amination, EEG, CT, and MRI are reviewed. Thisparameter concerns diagnostic evaluation; a subse-quent parameter will focus on treatment of the firstnonfebrile seizure.
The seizure types covered by this parameter in-clude partial (simple or complex partial, or partialwith secondary generalization), generalized tonic-clonic, or tonic seizures. We are specifically not in-cluding children diagnosed with epilepsy, defined astwo or more seizures without acute provocation. Forthis reason, myoclonic and atonic seizures are ex-cluded because they typically are not recognized un-til there have been multiple occurrences. We definedthe first seizure using the International LeagueAgainst Epilepsy (ILAE) criteria to include multipleseizures within 24 hours with recovery of conscious-
From the National Institute of Neurological Disorders and Stroke (Dr. Hirtz), National Institutes of Health, Bethesda, MD; Department of Pediatrics (Dr.Ashwal), Loma Linda University School of Medicine, Loma Linda, CA; Department of Biological Sciences (Dr. Berg), Northern Illinois University, Dekalb; Dr.David Bettis, Boise, ID; Department of Pediatric Neurology (Drs. C. Camfield and P. Camfield), IW Killam Hospital for Children, Halifax, Nova Scotia;Department of Neurology (Dr. Crumrine), Children’s Hospital of Pittsburgh, PA; Dr. Roy Elterman, Dallas, TX; Dr. Sanford Schneider, Riverside, CA; andthe Departments of Neurology and Pediatrics (Dr. Shinnar), Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY.Approved by the Quality Standards Subcommittee April 1, 2000. Approved by the Practice Committee May 3, 2000. Approved by the AAN Board of DirectorsJune 9, 2000.Received September 27, 1999. Accepted in final form June 13, 2000.Address correspondence and reprint requests to QSS, American Academy of Neurology, 1080 Montreal Avenue, St. Paul, MN 55116; phone: 800-879-1960
616 Copyright © 2000 by AAN Enterprises, Inc.
on long-term treatment and management.20,22 Fac-tors to be considered include the age of the child, theneed for sedation to perform the study, the EEGresults, a history of head trauma, and other clinicalcircumstances such as a family history of epilepsy.
Recommendations.
• If a neuroimaging study is obtained, MRI is thepreferred modality.50,51,54,60,62,63,65 (Guideline)
Emergent neuroimaging should be performed in achild of any age who exhibits a postictal focal deficit(Todd’s paresis) not quickly resolving, or who has notreturned to baseline within several hours after theseizure.46,66 (Option)
• Nonurgent imaging studies with MRI should beseriously considered in any child with a significantcognitive or motor impairment of unknown etiol-ogy, unexplained abnormalities on neurologic ex-amination, a seizure of partial (focal) onset with orwithout secondary generalization, an EEG thatdoes not represent a benign partial epilepsy ofchildhood or primary generalized epilepsy, or inchildren under 1 year of age.20,34 (Option)
Summary. In the child with a first nonfebrile sei-zure, diagnostic evaluations influence therapeuticdecisions, how families are counseled, and the needfor hospital admission and/or specific follow-upplans. This practice parameter has reviewed thepublished literature concerning the usefulness ofstudies following a first nonfebrile seizure in chil-dren, and has classified the strength of the availableevidence. There is sufficient Class I evidence, whichinvolves a well executed prospective study, to pro-vide a recommendation with the highest degree ofclinical certainty—i.e., a Standard—that an EEG beobtained in all children in whom a nonfebrile seizurehas been diagnosed, to predict the risk of recurrenceand to classify the seizure type and epilepsy syn-drome. The decision to perform other studies, includ-ing LP, laboratory tests, and neuroimaging, for thepurpose of determining the cause of the seizure anddetecting potentially treatable abnormalities, willdepend on the age of the patient and the specificclinical circumstances. Children of different agesmay require different management strategies.20,22
Future research. For most of the questions ad-dressed by this parameter, evidence was insufficientfor making a strong recommendation for a standardor guideline, particularly for laboratory studies. Inorder to generate definitive evidence regarding thevalue of routine (or selective) laboratory testing andthe use of routine neuroimaging studies, sufficientlylarge samples allowing for adequate statistical powerto provide precise estimates (i.e., with narrow confi-dence intervals) are needed. Neuroimaging studiesare needed to understand the significance of neuro-nal migration defects in the context of a first seizure,and are important because of the improved technical
ability of current MRI. In addition, prospective col-lection of data using standardized treatment proto-cols and standardized data collection instruments isessential. Results of studies will only be helpful ifthe patient sample and factors that resulted in inclu-sion into or exclusion from the sample are well de-scribed and documented. Ideally, large consecutiveseries of well-characterized patients are needed forthe results to be accurate and generalizable. Finally,future studies should present separate data fromchildren and adults, and it would be optimal for re-sults in children to be presented by age groupings.
Appropriate timing as well as the choice of evalu-ative studies have not been adequately studied. Chil-dren may present as actively having a seizure whenbrought to the emergency department, as postictal,or as alert with a history of a possible seizure epi-sode having occurred hours, days, or weeks previ-ously. Data regarding the appropriate timing oflaboratory testing, neuroimaging, or EEG studies re-quire adequate prospective studies of these specificquestions, with clearly defined entry criteria and acommon protocol for type and timing of evaluations.
Research studies with adequate sample sizes andappropriate protocols that provide answers to thesequestions may serve to reduce the expense and dis-comfort of unnecessary testing in children with firstseizures, and, more importantly, by identifying ap-propriate candidates, may improve the care andmanagement that these children receive.
Disclaimer. This statement is provided as an edu-cational service of the American Academy of Neurol-ogy. It is based on an assessment of current scientificand clinical information. It is not intended to includeall possible proper methods of care for a particularneurologic problem or all legitimate criteria forchoosing to use a specific procedure. Neither is itintended to exclude any reasonable alternativemethodologies. The AAN recognizes that specific pa-tient care decisions are the prerogative of the patientand the physician caring for the patient, based on allof the circumstances involved.
AcknowledgmentThe authors thank the members of the Quality Standards Sub-committee of the AAN, and Wendy Edlund, the AAN ClinicalPolicy Administrator, for their time, expertise, and efforts in de-veloping this document.
Appendix 1Classification of evidence
Class I. Must have all of a–d:a. Prospective study of a well defined cohort which includes a
description of the nature of the population, the inclusion/exclusioncriteria, demographic characteristics such as age and sex, andseizure type.
b. The sample size must be adequate with enough statisticalpower to justify a conclusion or for identification of subgroups forwhom testing does or does not yield significant information.
c. The interpretation of evaluations performed must be doneblinded to outcome.
d. There must be a satisfactory description of the technologyused for evaluations (e.g., EEG, MRI).
September (1 of 2) 2000 NEUROLOGY 55 621

Diagnósticos diferenciales
¤ Causa de error diagnóstico
frecuente
¤ Tanto crisis como TPNE se presentan
de manera similar:
¤ Caídas
¤ Compromiso de conciencia
¤ Movimientos y posturas anormales
¤ Clave en éxito diagnóstico reside en:
¤ Conciencia de la existencia de TPNE
¤ Buena historia clínica
Diagnósticos diferenciales
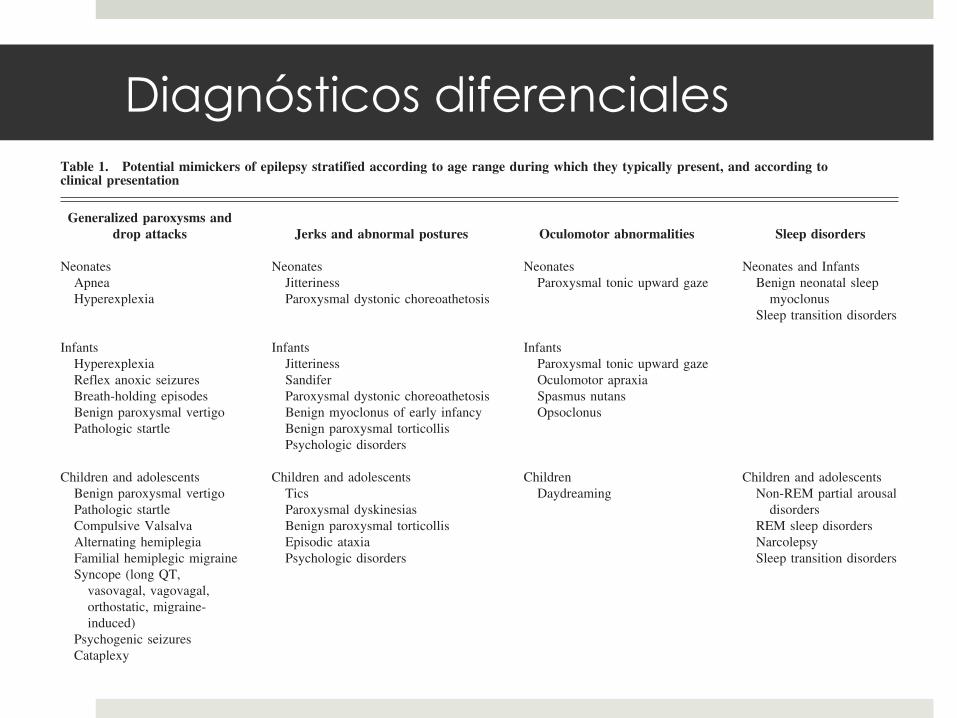
Diagnósticos diferenciales Table 1. Potential mimickers of epilepsy stratified according to age range during which they typically present, and according toclinical presentation
Generalized paroxysms anddrop attacks Jerks and abnormal postures Oculomotor abnormalities Sleep disorders
NeonatesApneaHyperexplexia
NeonatesJitterinessParoxysmal dystonic choreoathetosis
NeonatesParoxysmal tonic upward gaze
Neonates and InfantsBenign neonatal sleep
myoclonusSleep transition disorders
InfantsHyperexplexiaReflex anoxic seizuresBreath-holding episodesBenign paroxysmal vertigoPathologic startle
InfantsJitterinessSandiferParoxysmal dystonic choreoathetosisBenign myoclonus of early infancyBenign paroxysmal torticollisPsychologic disorders
InfantsParoxysmal tonic upward gazeOculomotor apraxiaSpasmus nutansOpsoclonus
Children and adolescentsBenign paroxysmal vertigoPathologic startleCompulsive ValsalvaAlternating hemiplegiaFamilial hemiplegic migraineSyncope (long QT,
vasovagal, vagovagal,orthostatic, migraine-induced)
Psychogenic seizuresCataplexy
Children and adolescentsTicsParoxysmal dyskinesiasBenign paroxysmal torticollisEpisodic ataxiaPsychologic disorders
ChildrenDaydreaming
Children and adolescentsNon-REM partial arousal
disordersREM sleep disordersNarcolepsySleep transition disorders
Abbreviation:REM ! Rapid eye movement
Table 2. Differences between generalized seizures and some generalized paroxysms that present with drop attacks or mimic generalizedtonic-clonic seizures
Precipitators Prodrome Ictal event Postictal period
Generalized seizures Sleep deprivation None Loss of consciousness: 2-3 minutesConsciousness might be preserved
if atonicSynchronous bilateral movementsTongue-biting
Delayed recovery withpostictal depression
Syncope with or withoutanoxic seizures
NeuralVasovagal Fatigue, emotional stress,
dehydrationBlurring of vision,
tinnitus,dizziness
Crying in breath-holdingepisodes
Loss of consciousness: secondsWhite discoloration in reflex
anoxic seizures
Rapid recovery with nopostictal depression
Reflex anoxicseizures
Minor bump to the head
Vagovagal Vomiting, swallowingOrthostatic Standing upHyperexplexia Bathing, awakening, auditory
and tactile stimuliRespiratory Injury, anger Loss of consciousness: seconds
Blue discolorationCardiac Exercise Loss of consciousness: seconds
White discolorationPsychogenic seizures Suggestion
Psychologic stressNone Loss of consciousness: "2-3
minutesGradual onsetAsynchronous, flailing limb
movementsVariable features between attacksNo injury
No postictal depression
310 PEDIATRIC NEUROLOGY Vol. 37 No. 5
¤ Síncope:
¤ Definido como pérdida de conciencia con
“colapso” o caída.
¤ Se presenta con “drop attacks”, que pueden
generar convulsiones (crisis anóxicas).
¤ Orgien:
¤ Neural
¤ Cardíaco
¤ Respiratorio
Diagnósticos diferenciales
¤ Claves diagnósticas:
¤ Habitualmente gatillados por estímulos.
¤ Pródromos son habituales
¤ Cambios de coloración en la piel
¤ Caídas pueden ser con hipo o hipertonía
¤ Las crisis pueden ser parecer clonías, pero son arrítmicas
¤ Incontinencia urinaria puede verse en aprox. 10%.
¤ Puede haber confusión post ictal
¤ Duración es menos de 1 minuto en la mayoría de los
casos.
Diagnósticos diferenciales
¤ Apneas emotivas:
¤ 2 tipos: pálidas y cianóticas
¤ Entre los 6 y 18 meses.
¤ Gatillados por lesiones, rabia
y frustración.
¤ Habitualmente asociados a
pérdida de conciencia y
postura tónica.
Diagnósticos diferenciales
¤ Vértigo paroxístico benigno de la infancia:
¤ Breves episodios de inestabilidad
¤ Aspecto “asustado”, se afirma de las cosas o se tira al suelo.
¤ Frecuente: palidez, diaforesis, nistagmo, nauseas y vómitos.
¤ Remiten en forma espontánea a los 5 años
Diagnósticos diferenciales
¤ Episodios de auto gratificación:
¤ Entre los 3 meses y 3 años
¤ Estereotipados
¤ Duración variable
¤ Vocalizaciones
¤ Enrojecimiento facial con diaforesis
¤ Postura y movimientos de predominio
en EEII
¤ Sin alteración de conciencia
¤ Examen neurológico y exámenes
normales.
Diagnósticos diferenciales
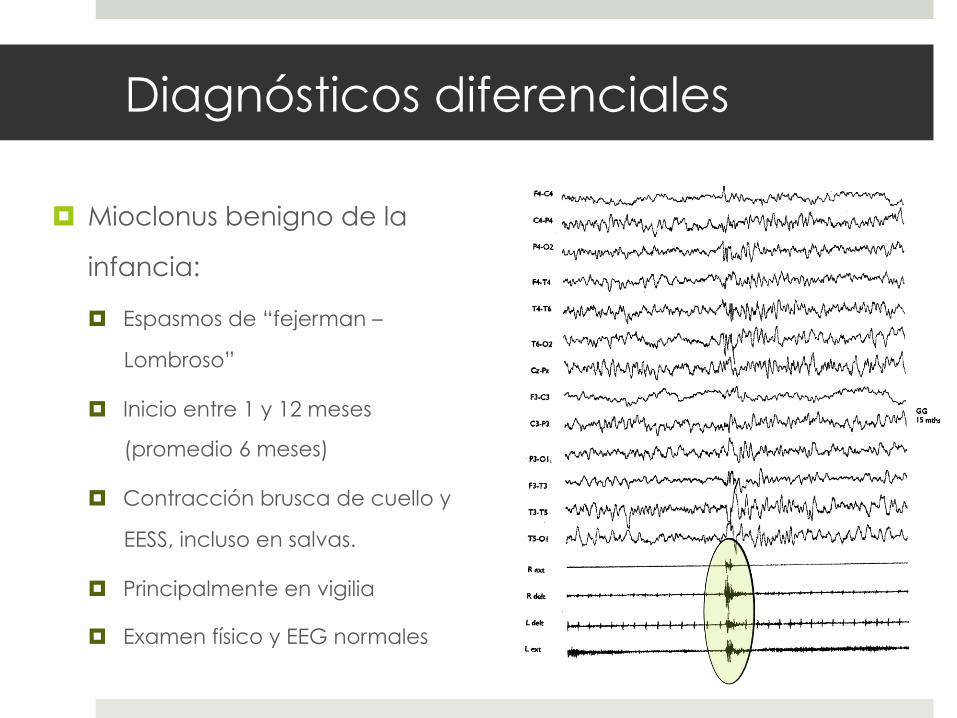
¤ Mioclonus benigno de la
infancia:
¤ Espasmos de “fejerman –
Lombroso”
¤ Inicio entre 1 y 12 meses
(promedio 6 meses)
¤ Contracción brusca de cuello y
EESS, incluso en salvas.
¤ Principalmente en vigilia
¤ Examen físico y EEG normales
Diagnósticos diferenciales
Diagnostic work-upBy definition of the inclusion criteria, neurologic exam-
ination, interictal, and ictal EEG were normal in all chil-dren. Brain imaging studies and neurometabolic screeningwere also normal.
Evolution and prognosisThe episodes disappeared at 6–30 months of age, in
most of the cases during the second year of life.As to incidence of epilepsy in this group, two cases pre-
sented clinical and EEG features of benign focal epilepsyin childhood.
Language and cognitive development were normal inall cases, and 15 (16.6%) of the children showed hyperki-netic behavior without specific learning disorders.
The personal series of 18 patients presented by Fejer-man in 1984 is now aged between 28 and 40 years. We arenot aware of any individual with developmental impair-ment or social disabilities among them, although details ofa number of them are lacking. We know that the first threecases of the original series that came to consultationalready treated with adrenocorticotropic hormone
(ACTH) because of a diagnosis of West syndrome arenow successful professionals and have normal children.
DiscussionWe are attempting to redefine the spectrum of clinical
manifestations of this condition on the basis of new neuro-physiologic evidence. It is clear that the differentiationbetween true myoclonus, brief tonic contractions, andatonic events is not easy only based on clinical events.Therefore, we are reclassifying the types of motor phe-nomena in this large series of patients as: myoclonic jerks;spasms (which by definition will be nonepileptic infantilespasms) and brief tonic contractions (referred to as con-tractions lasting for more than 200 or 300 ms); shudder-ing; and atonia or negative myoclonus.
Shuddering is not clearly distinguished from shivering,since the terms were used as synonyms (Vanasse et al.,1976; Kanazawa, 2000). Incidentally, in some patientswith severe encephalopathies, seizures with a brief toniccomponent followed by a kind of ‘‘vibratory’’ movementin the upper limbs may be observed. Since the initial
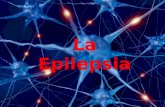
Figure 2.This is a 15-month-boy whostarted at 6 months of age withmultiple per day episodes ofsudden and brief contractionscharacterized by abduction ofupper limbs. The electromyo-graphy (EMG) trace shows arhomboid aspect that lasted foralmost 1 s, typical of spasms.The electroencephalography(EEG) trace does not show anyictal modification of cerebralactivity. A brief artifactualmodification occurred after themuscular manifestation. R ext,right digitorum extensor; Rdelt, right deltoid; L delt, leftdeltoid; L ext, left digitorumextensor.Epilepsia ILAE
1179
The Spectrum of BMEI
Epilepsia, 50(5):1176–1183, 2009doi: 10.1111/j.1528-1167.2008.01994.x
¤ Shuddering attacks:
¤ Similares al anterior
¤ Temblor rápido de la cabeza,
hombros y tronco de segundos
de duración.
¤ Habitualmente asociado a la
alimentación.
¤ Recurren varias veces al día.
¤ Frecuente antecedente de
temblor escencial en padres.
Diagnósticos diferenciales
¤ Tics:
¤ Movimientos involuntarios, no rítmcos de un grupo
muscular.
¤ Simples o complejos.
¤ Reprimibles (parcialmente) por la voluntad.
¤ Predominio hacia la tarde y exacerbados por el
stress.
¤ Antecedentes de trastornos psiquiátricos en la
familia.
Diagnósticos diferenciales

Conclusiones
¤ Epilepsia es frecuente en la población general
¤ Mayor incidencia es en la edad pediátrica.
¤ Diagnóstico es clínico.
¤ Dificil diferenciar de algunos trastornos
paroxísticos.
¤ Vital una buena historia clínica y examen físico.
Conclusiones
GRACIAS