LES pediátrico HIAEP Sor María Ludovica La Plata La Plata 2011 2011.
description

HOSPITAL DE NIÑOS SOR LUDOVICA DE LA PLATADr. Carlos Antelo.
ECMO

ECMO
EXTRACORPOREAL MEMBRANE OXIGENATION

ECMO: Hechos Históricos
1960 – 1968Lande AJ, et al: Development of membrane oxygenator
1972Hill et al.1st Successful use of prolonged ECLS
1973Soeter et al1st Reported use of ECMO in a child with POP TOF.
1976Bartlett RH et al.1st successful clinical application for neonatal respiratory failure
1986, ECMO as standard of care for neonatal respiratory failure


ECMO El soporte extra corpóreo consiste en el
drenaje de sangre venosa, la remoción de CO2 y adición de O2 mediante un pulmón artificial y el retorno de la sangre a la circulación, a través de un circuito veno - venoso o arterio - venoso.

ECMO Técnica de by pass cardiopulmonar. Parcial.
De larga duración.
Enfermedad grave reversible.

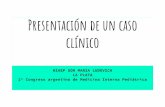
ECMO: tipos de by pass
VENO – ARTERIAL.
VENO – VENOSO.

FLUÍDOS HEPARINA
CÁNULA VENOSA
CÁNULA ARTERIALPUENTE
OXIGENADOR
CALENTADOR
SERVO CONTROL BOMBA


CANULACIÓN VENA Y ARTERIA FEMORAL
ARTERIA
VENA

Cánula arterialCánula venosa



vejiga
oxígenador
calentadorCánula venosa
Cánula arterial
bomba

Bomba centrífuga
oxigenador

Diferencias CEC / ECMO Quirófano. Soporte total. Corta duración. Canulación central. Cardioplejía. Hipotermia. Heparina TCA ≥400 Hematocrito 30%. Siempre veno-arterial.
Terapia intensiva Soporte parcial Larga duración Canulación periférica -central. Nunca cardioplejía Normo termia Heparina TCA 200-180 Hematocrito ≥30%

Indicaciones
ECMO Preop
Intraop
Postop

Indicaciones Síndrome de distres respiratorio agudo. Aspiración de líquido amniótico meconial. Hipertensión arterial pulmonar. Sepsis, neumonía y otras lesiones pulmonares
reversibles. Pre-Post operatorio de cirugía cardiovascular. Hernia diafragmática. Puente hacia el transplante cardiaco y/o
pulmonar.

ECMO contraindicaciones Injuria neurológica de rápida evolución.
Enfermedad pulmonar irreversible.
Coagulopatía severa.
RCP mayor de 1 hora previo a su ingreso a ECMO .

Criterios generales para ingreso a ECMO (Aprobados por la ELSO)
Extracorporeal Life Support Organization

Criterios generales para ingreso a ECMO (Aprobados por la ELSO)
INDICE DE OXIGENACIÓN ( MAP ).(FIO2 )
PaO2
Un índice de oxigenación igual o mayor de 40 por un tiempo de 5 a 6 horas identifica un
riesgo de mortalidad por lo menos del 80%. ECMO

Criterios generales para ingreso a ECMO (Aprobados por la ELSO)
DIFERENCIA ALVEOLO ARTERIAL DE OXÍGENO
AaDO2 = 760 mmHg. – (PaO2+ PaCO2+ 47 mmHg)
Una AaDO2 menor a 600- 620 mmHg. durante 4 a 12 horas ECMO

OTROS CRITERIOS ACEPTADOS
PH menor a 7,20 durante 2 horas, con hipotensión.
PaO2 menor 30 -40 mmHg.
Acido láctico en aumento.

Manejo del paciente en ECMO
Sitio de canulación:
Periférico (cuello o femoral).
Torácico(AD-Ao).
Chequear posición con RX.

Manejo del paciente en ECMO Manejo cardiovascular:
Disminuir inotrópicos y luego suspender, solo vasodilatadores (milrinona).
Manejar el volumen de asistencia para producir flujo pulsátil y diuresis espontanea. Inicial 120-160 ml/kg/min.
Al disminuir la presión pico y espiratoria aumenta el llenado ventricular.
Al ingresar en ECMO manejar niveles de calcio para evitar distensión del miocardio.
Evitar distensión de AI.

Manejo del paciente en ECMO
Temperatura:
36-37 C° pacientes sin paro cardio respiratorio (PCR).
34-36 C° luego de PCR por 24 hs.

Manejo del paciente en ECMO
Líquidos y Electrolitos:
100 a 130 ml. /k/ día . Balance estricto.
Tener en cuenta tercer espacio que se produce en los primeros días.
Hemodiafiltración .
Electrolitos dentro de límites normales.

Manejo del paciente en ECMO
Manejo respiratorio:
Pulmón en reposo. “ECMO setting en reposo”
PEEP: 8-10 cmH20 FiO2: 0.3 VT : 4-5 ml/KgPIP: ≤ 25 cm H2O FR: 10-14
Permeabilidad del tubo endotraqueal.

Manejo del paciente en ECMO
Manejo renal:
Frecuente oliguria transitoria, con recuperación en 48 horas aproximadamente.
Diuréticos.
Hemofiltración lenta e intermitente.
Hemodiafiltración

Manejo del paciente en ECMO
Manejo sedoanalgesia y SNC:
Sedantes y analgésicos que brinden confort y permita valoración clínica neurológica .
No relajantes salvo crisis de HTP.
Ecografía cerebral transfontanelar.
NIRS
Electroencefalograma .
Tomografía cerebral, eventual.

Manejo el paciente en ECMO
Profilaxis antibiótica :
Vancomicina a dosis habituales , y según corresponda adaptados a caída de filtrado glomerular o clearence de los sistemas empleados para reemplazo renal.
Cultivos sistemáticos.

Manejo del paciente en ECMO
Horario.EABElectrolitos
4 – 6 hHbPlaquetas Acido láctico
12 horas Creatinina
Diario RX TX HemocultivosEcografías
EEG inicial
Laboratorio:

Manejo del paciente en ECMO
Manejo hematológico:
Niveles adecuados de hemoglobina para optimizar transporte de oxígeno.
Recuento de plaquetas: arriba de 100.000/mm3.
Fibrinógeno: más de 150 mg%
Anticoagulación con heparina para lograr valores de TCA de 170-200 segundos .
Pruebas de coagulación cada 6-8 horas.

Régimen de anticoagulación
Objetivos hematológicos
Heparina Dosis inicial
○ 30-50 U/kg○ 3- 5 minutos pre-
canulación
Flujo continuo○ Circuito venoso.○ Comienza12 – 18 h
luego canulacion.
TCA :170 – 200 seg KPTT: 70 – 100 seg Anti- Xa: 0.35 – 0.65
u/ml RIN > 2 Fibrinogeno > 150. Hematocrito > 30 Plaquetas >
100,000/cm3
Manejo del paciente en ECMOManejo hematológico

Horario TCAKPTT sangre
entera. 4 horas
KPTT plasmaPlaquetas RINFibrinógeno
12-24 hNivel Antitrombina III Anti Xa.TEG.
o con o sin heparina
Anticoagulación:
Manejo del paciente en ECMO

ECMO: What could possibly go wrong? Oxygenator failure Raceway rupture Other tubing rupture Pump malfunction Heat exchanger malfunction Clots: oxygenator Clots: bridge Clots: bladder Clots: hemofilter Clots: other Air in circuit Cracks in pigtail connectors Cannula problems Hemorrhagic: GI hemorrhage Hemorrhagic: Cannulation site bleeding Hemorrhagic: Surgical site bleeding Hemorrhagic: Hemolysis (hgb > 50 mg/dl) Hemorrhagic: Disseminated intravascular coagulation
(DIC) Neurologic: Brain death clinically determined Neurologic: Seizures: clinically determined Neurologic: Seizures: EEG determined Neurologic: CNS infarction by US/CT Neurologic: CNS hemorrhage by US/CT
Renal: Creatinine 1.5 - 3.0 Renal: Creatinine > 3.0 Renal: Dialysis required Renal: Hemofiltration required Renal: CAVHD required Cardiovascular: Inotropes on ECLS Cardiovascular: CPR required Cardiovascular: Myocardial stun by echo Cardiovascular: Cardiac arrhythmia Cardiovascular: Hypertension requiring vasodilators Cardiovascular: PDA: R->L Cardiovascular: PDA: L->R Cardiovascular: PDA: bidirectional Cardiovascular: PDA: unknown Cardiovascular: Tamponade: blood Cardiovascular: Tamponade: serous Cardiovascular: Tamponade: air Pulmonary: Pneumothorax requiring treatment Pulmonary: Pulmonary hemorrhage Infectious: Culture proven infection (see Infections) Infectious: WBC < 1,500 Metabolic: Glucose < 40 Metabolic: Glucose > 240 Metabolic: pH < 7.20 Metabolic: pH > 7.60 Metabolic: Hyperbilirubinemia (> 2 direct or > 15 total)

ECMO complicaciones: definición a grandes rasgos
Complicaciones mecánicas: requieren un cambio en un componente (oxigenador tubuladura) u otra intervención específica.
Complicaciones respiratorias o cardíacas: surgen durante ECMO y requieren intervención médica adicional.

Complicaciones Mecánicas
Clotting complications are among the most common mechanical complications Clotting complications are higher in neonates
Circuit sizes Flow Rates Immature/difficult coagulation cascade
Survival is moderately high (>50%) for most mechanical complications except in cardiac patients Interruptions in support may be more dire in this population Cardiac patients fare worse in general compared to respiratory
Hemofilter complications also fare worse because patients requiring hemofilters fare worse than patients who do not
Neonatal Respiratory Pediatric Respiratory Infant Cardiac Neonatal Cardiac Pediatric CardiacIncidence Survive Incidence Survive Incidence Survive Incidence Survive Incidence Survive
Oxygenator failure 6% 53% 13% 43% 9% 29% 8% 23% 10% 43%Raceway rupture 0% 58% 1% 49% 1% 50% 0% 21% 1% 47%Other tubing rupture 1% 72% 2% 47% 1% 19% 1% 27% 1% 35%Pump malfunction 2% 66% 3% 47% 2% 36% 2% 28% 2% 48%Heat exchanger malfunction 1% 66% 0% 50% 0% 42% 1% 53% 0% 55%Clots: oxygenator 17% 65% 10% 50% 8% 42% 11% 27% 8% 50%Clots: bridge 10% 67% 5% 54% 4% 36% 5% 30% 3% 49%Clots: bladder 15% 68% 6% 54% 5% 40% 7% 25% 2% 48%Clots: hemofilter 3% 44% 5% 44% 4% 31% 4% 25% 2% 28%Clots: other 7% 57% 11% 51% 9% 44% 13% 31% 9% 53%Air in circuit 5% 70% 4% 49% 3% 51% 3% 28% 3% 38%Cracks in pigtail connectors 3% 70% 1% 51% 1% 34% 1% 48% 1% 38%Cannula problems 12% 67% 16% 51% 6% 40% 6% 34% 7% 42%

Complicaciones Medicas
Medical complications may be related more to patient management or patient underlying condition than ECMO system itself
Hemorrhagic complications are among the most fatal complications Most likely from inadequate anticoagulation monitoring Surgical site bleeding is higher in cardiac ECMO because of
post-op or chest cannulation
Neonatal Respiratory Pediatric Respiratory Infant Cardiac Neonatal Cardiac Pediatric CardiacIncidence Survive Incidence Survive Incidence Survive Incidence Survive Incidence Survive
Hemorrhagic: GI hemorrhage 2% 45% 4% 25% 2% 15% 1% 11% 3% 28%Hemorrhagic: Cannulation site bleeding 7% 64% 16% 51% 12% 40% 11% 29% 17% 52%Hemorrhagic: Surgical site bleeding 6% 44% 14% 46% 34% 39% 32% 30% 30% 47%Hemorrhagic: Hemolysis (hgb > 50 mg/dl) 11% 65% 10% 43% 10% 33% 11% 28% 9% 43%Hemorrhagic: Disseminated intravascular coagulation (DIC) 3% 39% 5% 26% 3% 23% 4% 17% 4% 37%Neurologic: Brain death clinically determined 1% 0% 5% 0% 4% 0% 1% 0% 7% 0%Neurologic: Seizures: clinically determined 10% 61% 6% 34% 10% 26% 8% 29% 5% 21%Neurologic: Seizures: EEG determined 1% 48% 2% 34% 3% 31% 3% 25% 1% 21%Neurologic: CNS infarction by US/CT 8% 54% 4% 35% 4% 32% 4% 25% 4% 39%Neurologic: CNS hemorrhage by US/CT 7% 44% 6% 22% 6% 30% 11% 22% 4% 23%Renal: Creatinine 1.5 - 3.0 7% 52% 10% 30% 10% 22% 13% 22% 15% 33%Renal: Creatinine > 3.0 1% 36% 5% 29% 2% 25% 2% 23% 8% 32%Renal: Dialysis required 3% 40% 14% 31% 12% 21% 10% 20% 12% 29%Renal: Hemofiltration required 15% 53% 22% 44% 22% 35% 26% 26% 19% 44%Renal: CAVHD required 2% 46% 7% 40% 5% 28% 6% 15% 7% 42%

“Weaning” ECMO Reducción de flujo ECMO .
Ventilación con parámetros adecuados al weaning.
Indicador fundamental : mejoría de función pulmonar y cardiaca .
Adrenalina 0.05gamas/k/x milrinona 0.5 g/k/x
Se clampean las cánulas , con decanulación diferida (1 hora entre decanulación arterial y venosa)
Con estabilidad clínica, ácido láctico dentro de límites normales se decanula y retira de ECMO.
Persiste heparina hasta momentos previos a la decanulación
arterial. Protamina luego de decanulación venosa.

Controles post ECMO Cardiacos:
Control ecocardiográfico:o Función ventricular.○ Descartar
Distensión de VI y AIInsuficiencia valvular.Derrame pericárdicoResiduo quirúrgico
Pulmonar:Distensibilidad

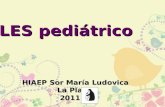
Experiencia HNLPMaterial y Métodos:
Se incluyeron a todos los pacientes que requirieron asistencia circulatoria extracorpórea .
Desde Octubre 1993 a Octubre de 2013. En éste lapso se realizaron 5.250 cirugías
cardiovasculares.

98%
2%
Periodo 20 años octubre 1993-octubre 2013Cirugias ECMO
Experiencia HNLP

ECMO
Tiempo promedio de permanencia en asistencia circulatoria fue de 3 días.
Entre 18 horas a 8 días .
La decanulación exitosa se logró en 43 de 117 pacientes , corresponde al 36% de los pacientes ingresados a ECMO.

92%
4% 2% 2%
ECMO IndicaciónECMO post op ECMO pre opECMO pre Tx ECMO no CC
Experiencia HNLP

Experiencia HNLP 117pacientes requirieron ECMO. 5 pacientes: preoperatorio CCV. 108 pacientes: post operatorios CCV. (corresponde al 1,80 % del total de ccv realizadas) 2 pacientes: miocardiopatías. 1 paciente : hernia diafragmática. 1 paciente: asma severo. Varones 61% - mujeres 39%. Edad promedio : 24 meses. (entre 24 horas a 14 años de vida) Peso promedio : 8. 280 g. (entre 1.800 Kg. y 71 Kg.)

Complicaciones durante el procedimiento
Medicas:
Coagulopatía : 21 pacientes. Insuficiencia renal: 17 pacientes. Sepsis: 11 pacientes. Fallo multiorgánico: 11 pacientes. Convulsiones: 4 pacientes.
Mecánicas:
Complicaciones mecánicas: 6 pacientes.

Decanulación exitosa43 pacientes
10 pacientes Muerte alejada
Sin lograr Externación
23%
11 pacientes con alta hospitalaria
presentaron Muerte súbita
(Entre los 3 y 24 meses
del alta)25,6%
23 pacientes sobreviven
en la actualidad
53.4%

ECMOCONCLUSIONES
Indicaciones de ECMO 2013:Preoperatorio C.C.VPost op C.C.V. imposibilidad de
desconexion CEC. Índices de oxigenación y volumen
minuto en descenso.Dosis de inotrópicos en ascenso. Neumopatía grave reversible.ECMO en preoperatorio de CCV mayor
sobrevida.

Circulation. 2010;122:S241-S248