Ingreso mensual total
14
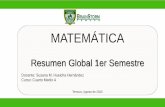
Página 1 de 2 Solo para uso oficial Priority Points A.C.C. Agency: PACE Intake Initials: Intake Date: Eligibiltiy Cert Date Nombre Inicial del segundo nombre Apellido Fecha de nacimiento MM/DD/YY DOMICILIO DE SERVICIO – Domicilio de residencia (no casilla de correo) Domicilio De Servicio Número de unidad Ciudad Condado LOS ANGELES Estado CA Código postal ¿Ha vivido en este domicilio durante los últimos 12 meses corridos? …………………………………………………………………….. ☐ Sí ☐ No ¿Su domicilio de servicio es el mismo que su domicilio de residencia?......................................................................... ☐ Sí ☐ No Domicilio postal Número de unidad Ciudad Condado LOS ANGELES Estado CA Código postal Número de seguridad social (SSN): Número telefónico ( ) Correo Electronico: Department of Community Services and Development Energy Intake Form CSD 43 (10/2017) PERSONAS QUE VIVEN EN EL HOGAR Ingrese la cantidad total de personas que viven en el hogar incluido usted INGRESOS Ingrese la cantidad total de personas que reciben ingresos Datos demográficos: Ingrese la cantidad de personas en el hogar que son: Indique e el ingreso mensual bruto total de todas las personas que viven en el hogar: Edades 0 – 2 años TANF / CalWorks $ Edades 3 - 5 años SSI / SSP $ Edades 6 - 18 años SSA / SSDI $ Edades 19 - 59 Cheque(s) de pago $ Edades mayor de 60 años Intereses $ Discapacitado Pensión $ Nativo Americano Otro $ Trabajador agrícola estacional o migrante Ingreso mensual total $ INTEGRANTES DEL HOGAR INGRESE LA INFORMACIÓN DE TODOS LOS INTEGRANTES DEL HOGAR Si en su hogar viven más de 7 personas, incluya su información en una hoja adicional. Nombre Apellido Relación con el solicitante Edad Fecha de nacimiento MM/DD/YY Monto del ingreso bruto total (Antes de impuestos y deducciones) Fuente de ingresos Usted Monto del ingreso bruto mensual total del hogar $
Transcript of Ingreso mensual total
Página 1 de 2
Solo para uso oficial Priority Points
A.C.C.
Agency: PACE Intake Initials: Intake Date: Eligibiltiy Cert Date
Nombre Inicial del segundo nombre
Apellido Fecha de nacimiento
MM/DD/YY
DOMICILIO DE SERVICIO – Domicilio de residencia (no casilla de correo) Domicilio De Servicio Número de unidad
Ciudad Condado LOS ANGELES
Estado CA
Código postal
¿Ha vivido en este domicilio durante los últimos 12 meses corridos? …………………………………………………………………….. ☐ Sí ☐ No
¿Su domicilio de servicio es el mismo que su domicilio de residencia?......................................................................... ☐ Sí ☐ No
Domicilio postal Número de unidad
Ciudad Condado LOS ANGELES
Estado CA
Código postal
Número de seguridad social (SSN):
Número telefónico ( )
Correo Electronico:
Department of Community Services and Development Energy Intake Form
CSD 43 (10/2017)
PERSONAS QUE VIVEN EN EL HOGAR Ingrese la cantidad total de personas que viven en el hogar incluido usted
INGRESOS Ingrese la cantidad total de personas que reciben ingresos
Datos demográficos: Ingrese la cantidad de personas en el hogar que son:
Indique e el ingreso mensual bruto total de todas las personas que viven en el hogar:
Edades 0 – 2 años TANF / CalWorks $
Edades 3 - 5 años SSI / SSP $
Edades 6 - 18 años SSA / SSDI $
Edades 19 - 59 Cheque(s) de pago $
Edades mayor de 60 años Intereses $
Discapacitado Pensión $
Nativo Americano Otro $
Trabajador agrícola estacional o migrante
Ingreso mensual total $
INTEGRANTES DEL HOGAR INGRESE LA INFORMACIÓN DE TODOS LOS INTEGRANTES DEL HOGAR Si en su hogar viven más de 7 personas, incluya su información en una hoja adicional.
Nombre Apellido Relación con el solicitante Edad
Fecha de nacimiento MM/DD/YY
Monto del ingreso bruto total (Antes de
impuestos y deducciones)
Fuente de ingresos
Usted
Monto del ingreso bruto mensual total del hogar $
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight

Página 2 de 2
¿Usted o alguien de su familia recibe ACTUALMENTE CalFresh (Cupones para alimentos)? ☐ Sí ☐ No
FACTURA DE PAGO ¿A qué factura de energía (ELIJA SÓLO UNA) desea que se aplique el beneficio LIHEAP?
☐ Gas Natural ☐ Electricidad ☐ Madera ☐ Propano ☐ Aceite combustible ☐ Kerosene ☐ Otro combustible
Ingrese la empresa de energía y el número de cuenta:
Nombre de la empresa: No. de cuenta:
¿Su servicio público está interrumpido? ☐ Sí ☐ No
¿Recibió una notificación por atraso? ☐ Sí ☐ No
¿Sus servicios públicos están incluidos en la renta? ☐ Sí ☐ No
¿Sus servicios públicos son todos eléctricos? ☐ Sí ☐ No
¿Su empresa de gas natural es la misma que su empresa eléctrica? ☐ Sí ☐ No
SERVICIO DE MADERA, PROPANO o ACEITE COMBUSTIBLE (WPO) ¿Actualmente no tiene combustible? (madera, propano, aceite, kerosene, otros combustibles) ☐ Sí ☐ No ☐ N/A
Indique la cantidad aproximada de días que quedan antes de que se quede sin combustible
(madera, propano, aceite, kerosene, otros combustibles). Cantidad de días: ☐ N/A
Debe incluirse una copia de una factura eléctrica aun cuando no use electricidad para calentar su hogar.¿Cuál es el combustible que más utiliza para CALENTAR su hogar? DEBE marcar una fuente principal. SELECCIONE UNO BIL SOLAMENTE
☐ Gas Natural ☐ Electricidad ☐ Madera ☐ Propano ☐ Aceite combustible ☐ Kerosene ☐ Otro combustibleAdemás de su fuente de calefacción principal, ¿usa alguno de los siguientes para calefaccionar su hogar? (puede elegir más de uno):
☐ Gas Natural ☐ Electricidad ☐ Madera ☐ Propano ☐ Aceite combustible ☐ Kerosene ☐ Otro combustible ☐ N/A
¿Usted es el titular de: La factura de Electricidad ☐ Yes ☐ No La factura de Gas Natural ☐ Yes ☐ No
La información de la presente solicitud se utilizará para determinar y verificar mi eligibilidad para recibir asistencia. Al firmar a continuación, presto mi consentimiento (permiso) al CSD, sus contratistas, consultores y otras oficinas federales o estatales (socios del CSD) y a mi empresa de servicios públicos y a sus contratistas para entregar información acerca de mi cuenta de servicios públicos doméstica, consumo de energía u otra información necesaria para prestarme los servicios y beneficios descriptos al final del presente formulario. Mi consentimiento tendrá vigencia por un plazo de 24 meses anteriores a la fecha de firma que se consigna a continuación y hasta 36 meses después. Entiendo que si mi solicitud para los beneficios o servicios LIHEAP/DOE es denegada, o si recibo una respuesta fuera de término o una prestación no satisfactoria, podré presentar una apelación escrita ante el proveedor del servicio local, y esta apelación será evaluada no más de 15 días después de su recepción. De no estar conforme con la decisión del proveedor del servicio, podré apelar ante el Departamento de Servicios Comunitarios y Desarrollo conforme al Artículo 100805, Título 22 del Código de Normas de California. De resultar aplicable, autorizo la instalación de medidas de climatización en mi residencia sin costos a mi cargo. Declaro, bajo pena por falso testimonio, que la información incluida en la presente solicitud es verdadera, correcta, y que los fondos recibidos se utilizarán exclusivamente a los Pagos de mis costos de energía.
X * * * FIRMA DEL SOLICITANTE * * * Fecha
NOMBRE DE LA OFICINA: Servicios Comunitarios y Desarrollo (CSD). UNIDAD RESPONSABLE DEL MANTENIMIENTO: Programa de Asistencia en Energía Doméstica (HEAP). AUTORIDAD: El Artículo 16367.6 del Código de Gobierno (a) nombre a CSD como oficina responsable del manejo del HEAP. OBJETO: La información que usted proporciona será utilizada para decidir si resulta apto para el pago de LIHEAP o los servicios de climatización. ENTREGA DE INFORMACIÓN: Este programa es voluntario. Si decide solicitar asistencia, debe entregar toda la información solicitada. OTRA INFORMACIÓN: CSD emplea definiciones estadísticas de la actualización anual de las Pautas sobre Pobreza, Ingresos Federales e Ingresos Medios del Estado del Departamento de Servicios Médicos y Humanos para determinar la aptitud al programa. Durante el procesamiento de la solicitud, el subcontratista designado de CSD podría necesitar más información para decidir respecto de su aptitud para uno o ambos programas. ACCESO: El subcontratista designado de CSD conservará su solicitud completa y toda otra información, de ser utilizada, para determinar su aptitud. Tiene derecho a acceder a todos los registros que contengan información sobre usted. CSD no discrimina al momento de prestar sus servicios como consecuencia de la raza, religión, color, nacionalidad, ancestros, discapacidad física, discapacidad mental, enfermedad, estado civil, sexo, edad ni orientación sexual.
SOLICITANTE: NO COMPLETE LA SIGUIENTE INFORMACIÓN. ESTA SECCIÓN ES SOLO PARA USO OFICIAL.
Utility Assistance being provided under which program ☐ HEAP ☐ Fast Track ☐ HEAP WPO ☐ ECIP WPOBase Benefit $ Supplement $ Total Benefit $
Total Energy Cost $ Energy Burden
Energy Services Restored after disconnection: ☐ Sí ☐ No Disconnection of Energy Services Prevented: ☐ Sí ☐ No
Home Referred for WX: ☐ Home Already Weatherized: ☐
INFORMACIÓN SOBRE ENERGÍALas siguientes preguntas son OBLIGATORIAS. Marque todas las fuentes de energía utilizadas para calentar su hogar. Debe presentar una copia de todas las facturas de energía recientes por todos los costos de energía doméstica. NOTA: debe incluirse una copia de una factura eléctrica aun cuando no use electricidad para calentar su hogar.
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight

Formulario de la Encuesta Demográfica
De acuerdo con los requisitos del programa fondo federal, por favor proporcione la siguiente información de
la encuesta demográfica. Por favor, marque lo que corresponda.
Procedimientos del Programa de Asistencia en Energía del Hogar (HEAP)
Favor de leer y reconocer lo siguiente con su firma:
1. El Programa de HEAP es una asistencia que puede ser utilizada solo una vez al año.
2. El Programa de HEAP no es un programa de derecho.
3. Todos pueden aplicar, no todos podrán calificar.
4. Si usted califica, un crédito será puesto en su cuenta de utilidad.
5. Si usted no califica, se le notificará por correo.
6. PACE no llamara a la compañía de servicios públicos de su parte por ninguna razón.
7. PACE no hace ningún pago.
8. Todos los pagos o créditos hechos hacia su cuenta de utilidad son por cuenta del Departamento de Servicios
Comunitarios y Desarrollo del estado de California.
9. Ninguna cuenta de utilidad será pagada de inmediato. Puede tomar hasta 5 meses. Usted tendrá que hacer sus propios
arreglos directamente con las compañías de utilidad para evitar la desconexión de su servicio.
Yo, ___________________________________, he leído y comprendido los procedimientos del Programa de HEAP.
(Nombre)
Firma: ________________________________________ Fecha: ______________________________
PROGRAMA DE CLIMATIZACIÓN GRATIS
Usted puede ser elegible para recibir $3055 - sin ningún costo a usted - las medidas de ahorro de
energía y trabajo de climatización para su hogar. Requisitos de elegibilidad incluyen bajos ingresos y
otros requisitos de evaluación pueden aplicar. Este programa está financiado por el Departamento de
Salud y Servicios Humanos, administrada por el Departamento de Servicios Comunitarios y
Desarrollo del estado de California.
34. ____Deseo recibir la aplicación para estos beneficios.
Ingresos y / o cualquier otra ayuda:
1. ____AFDC/TANF/CalWorks
2. ____SSI/SSP
3. ____SSA/Seguridad Social
4. ____Pensión /Retiro/Annuity
5. ____Empleo, IHSS, Crystal Stairs
6. ____Ingresos Autónomos
7. ____CAPI
8. ____EDD/SDI (Pagos de discapacidad)
9. ____Compensación de trabajadores
10. ____GR
11. ____Adopción/Cuidado tutelar
12. ____Inversiones/Interés
13. ____Beneficios de VA
14. ____Manutención de los hijos/del cónyuge
15. ____Apoyo de familia
16. ____Ingresos de alquiler
17. ____Ahorros
18. ____Cupones de alimentos
19. ____Otro (indique aquí)
____________________________________
____________________________________
Yo me considero
20. ____Afroamericano
21. ____Armenio
22. ____Caucásico
23. ____Chino
24. ____Coreano
25. ____Filipino
26. ____Latino
27. ____Nativo Indígena de América
28. ____Vietnamita
29. ____Otro: ____________________________________
Vivienda:
30. ____Yo tengo SECCIÓN 8 o HUD
Mi porción mensual es: $__________
31. ____ALQUILO un apartamento.
Mi renta mensual es: $__________
¿Aproximadamente cuántas unidades se encuentran en
su edificio? __________
32. ____ALQUILO una casa.
Mi renta mensual es: $__________
33. ____Yo soy DUEÑO(A) de casa.
Mi pago mensual es: $__________


Fecha Tiempo Fecha Tiempo Fecha Tiempo
Fecha
Opción de Certificación
Si la información fue entregada pero una firma no fue obtenible, usted puede marcar la caja apropiada abajo.
Yo cerifico que intente entregar la información siguiente a la dirección de arriba.
State of California
DEPARTMENT OF COMMUNITY SERVICES AND DEVELOPMENT
CSD 321 (Rev. 11/10/08)
CONFIRMACIÓN DE LA EDUCACIÓN DEL CLIENTE
Confirmación de Recibimiento
Fechas y tiempos que se trató de entregar la información.
Educación de Plomo Educación de la Energía Educación del Molde y Humedad Asesoramiento de su Presupuesto
Denegación de Firma — Yo cerifico que he hecho un esfuerzo en buena fe para entregar la informción a la
dirección de arriba en la fecha y la hora indicada y que el inquilino rechazó firmar la confirmación de recibimiento.
Además cetifico que he dejado una copia de la información en la unidad con el inquilino.
No se Encontró para Firmar — Yo certifico que he hecho un esfuerzo en buena fe para entregar la información a la
dirección de arriba y que el inquilino no se encontró para firmar la confirmación de recibimiento. Además certifico que he
dejado una copia de la información en la unidad deslizándola de bajo de la puerta.
Firma (Representativo de la Agencia)
Firma (Representativo de la Agencia) Nombre
Educación de Plomo Educación de la Energía Educación del Molde y Humedad Asesoramiento de su Presupuesto
Opción de Envío de la Certificación:
Yo cetifico que he enviado la siguiente información a la dirección de arriba (fije una copia del Certificado de
Correo para la Educación de Plomo solamente):
Nombre
Educación de la Energía – Información con respecto a cambios que puedo realizar para reducir la hogar
consumición de energía de mi hogar.
Asesoramiento de su Presupuesto - Información con respecto al manejamiento de sus financias personales.
He recibido la información siguiente:
FechaFirma del recipiente
Educación del Molde y Humedad - Una copia del folleto, Una Guía Breve de Monlde y Humedad en su Hogar ,
informándome como limpiar problemas residenciales del molde y como prevenir crecimiento de molde.
Educación de Plomo – Una copia del folleto, Remodelar correctamente: Información importante sobre los riesgos
causados por el plomo para familias, proveedores de cuidado infatil y escuelas (efectivo 12/22/08) información del riesgo
potencial de la exposición de plomo por la actividad de la climatización o renovación que se realizara en mi vivienda.
Nombre del Inquilino Edad de la Vivienda
Dirección de la vivienda
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight

90001 90002 90003 90006 90007 90008 90009 90011 90012 90013 90014 90015 90017 90020 90021 90024 90025 90027 90028 90029 90030 90036 90037 90038 90039 90043 90044 90045 90046 90047 90048 90049 90050 90051 90052 90053 90054 90055 90057 90059 90060 90061 90062 90064 90066 90067 90068 90069 90071 90077 90079 90094 90210 90211 90212 90220 90221 90222 90223 90224 90231 90245 90247 90248 90249 90250 90251 90254 90260 90261 90266 90267 90272 90277 90278 90291 90292 90294 90295 90296 90301 90302 90303 90304 90305 90306 90307 90308 90309 90310 90311 90312 90401 90402 90403 90404 90405 90406 90407 90408 90409 90410 90411 90501 90502 90503 90504 90505 90506 90507 90508 90509 90510 90723 90745 90746 90747 90749 91201 91202 91203 91204 91205 91206 91207 91208 91209 91210 91502 91503 91505 91506 91521 91522 91523 91603 91608
Pacific Asian Consortium in Employment (PACE) y el Programa de Asistencia en Energía
del Hogar (HEAP) ayuda a pagar parte de su cuenta de gas o electricidad
El PACE Programa de Asistencia en Energía del Hogar (HEAP) es un proyecto financiado por la Comisión Federal de Bajos Ingresos y Programa de Asistencia de Energía a través del Departamento de Servicios Comunitarios y Desarrollo del estado de California. Nuestra misión es ayudar a las familias elegibles y calificados de bajos ingresos compensen sus costos de calefacción y enfriamiento, proporcionando una vez al año el pago a cualquiera de su factura de gas o eléctrico.
El programa PACE HEAP sirve a los siguientes códigos postales:
****HEAP NO PROPORCIONA ESTACIONAMIENTO NI VALIDACIÓN****
Para obtener más información y para comprobar el estado de su solicitud: 213-989-3236 Inglés/Español 213-989-3173 Inglés/Español 213-989-3294 Inglés/Español 213-989-3177 Inglés/Español 213-989-3152 Inglés/Español 213-353-1228 Línea de información grabada disponible 24 horas al día (No deje un mensaje) Horario de oficina: lunes a viernes - 8:00 am a 3:00 pm
PACE Servicios de Energía y Medio Ambiente HEAP 1055 Wilshire Blvd. Suite 900E Los Ángeles, CA 90017 web: www.pacela.org
Uselo Sabiamente
Energía es Dinero
Para determinar la elegibilidad de su hogar, debe presentar copias de: Su ID de California con foto Su tarjeta de Seguro Social Su cuenta actual de electricidad y del gas Completa con todas las páginas que
cubren al menos 22 días de servicio con las marcas del medidor. Los dos biles se requieren. Incluya cualquier aviso final reciente o aviso de
corto de servicios de gas o electricidad. Entregue prueba de ingreso mensual actual. Incluya todos los miembros del
hogar que reciben ingresos. Esto debe mostrar ingresos antes de deducciones, y debe de mostrar los ingresos de los últimos 30 días. o TANF (AFDC), GR, manutención de los hijos, Kin-Gap y otros. Debe ser
para el mes actual. o SSI, SSA, VA debe ser para el año actual. o Salario, EDD, SDI, Pensión /Retiro por Discapacidad. Todos los talones
deben cubrir los últimos 30 días. Si el pago es en efectivo o por contribuciones, debe demonstrar la fecha, nombre, y dirección de la persona que presta dinero en efectivo.
Una copia de contrato de Sección 8/HUD, recibo de renta o pago de hipoteca Para determinar la elegibilidad también debe completar y firmar estas (3) formas: Energy Intake Form CSD 43 Forma de información demográfica Formulario de Confirmación de Educación de Cliente CSD 321 (ver el reverso)
IMPORTANTE 1. Envíe solo copias. No originales. 2. Usted será notificado por correo si usted no califica para recibir ayuda. 3. Debido a la popularidad de este programa, las solicitudes pueden tardar hasta 5 meses de proceso. 4. No hay garantía de que recibirán asistencia hasta que se apruebe su solicitud. 5. Es su responsabilidad ponerse en contacto con la compañía de utilidad para evitar la desconexión de servicios. Mientras se procesa su elegibilidad, continue haciendo los pagos a la compañía de utilidad 6. Si usted califica, un pago se enviará directamente a la compañía de utilidad seleccionada y un crédito será publicado hacia su cuenta de servicios públicos. 7. Se da prioridad a ancianos, discapacitados, familias con niños pequeños, y hogares que solicitan por primera vez esta asistencia, los hogares con bajos ingresos y cuentas más altos.
Las solicitudes no se procesarán si falta algún documento, o si algún documento no está completo o firmado.

Page 1 of 1
Department of Community Services and Development Account Holder Authorization and Consent Form CSD Form 081 (Rev. 12/17)
ACCOUNT HOLDER NAME(S) AND MAILING ADDRESS Account Holder’s Full Name
Account Holder’s mailing address (Street) Unit Number (if any)
(City) State Zip Code
Is the utility service address the same as the account holder’s mailing address? Yes No
Full Name of Applicant for Benefits (from Form 43)
Utility Service Address (Street) Unit Number (if any)
(City) State CA
Zip Code
UTILITY INFORMATION Please enter your utility company name and service account number below (you can find the account number on your bill). If different companies provide your electricity and gas services, please enter the name and account number for both utilities.
Name of Utility Company Service Account Number
Name of Utility Company (if you have a second Utility Company) Service Account Number
AUTHORIZATION AND CONSENT
By signing this form, you (Account Holder) give your authorization and consent (permission) to CSD, its contractors, consultants, other federal or state agencies (CSD Partners) and to your utility company and its contractors, to share information about your property’s utility account, meter usage and energy consumption data, and other information as needed for the period beginning 24 months prior to, and continuing for 36 months after, the date signed below. The information you authorize us to obtain and share will be used for the purposes of evaluating home energy usage of program beneficiaries so that CSD can: a) measure the effectiveness of the services we provide by determining how much your utility bills are reduced and how much our services reduce carbon emissions (air pollution), and b) report these results to federal and state authorities that fund and oversee energy assistance programs in California. CSD, its contractors, consultants, other federal or state agencies and affiliated programs (CSD Partners), working cooperatively with your utility company and its contractors, use this information to provide services that assist low-income families, such the applicant, to pay their home energy bills and mange those energy needs for the purposes stated in this Authorization.
REVOCATION OF AUTHORIZATION AND CONSENT You agree that your consent shall remain in effect for 36 months from the date you sign this Authorization, unless otherwise revoked by written notice mailed to: CSD Energy & Environmental Services Division, 2389 Gateway Oaks Drive, Suite 100, Sacramento, CA 95833. Revocation will be effective upon receipt, but will not apply to any information shared while this Authorization was valid.
APPLICABLE PROGRAMS
Some of the programs CSD oversees or partners with include:
- CSD Federal Low-Income Home Energy Assistance Program (LIHEAP)- CSD Federal Department of Energy Weatherization Assistance Program (DOE WAP)- State Low-Income Weatherization Program (LIWP)- Department of Housing and Urban Development (HUD) Lead Hazard Control and Healthy Homes Program- Utility Company Energy Savings Assistance (ESA) Program- Utility Company California Alternate Rates for Energy (CARE) Program
Signature of Account Holder Date Name of CSD Contractor/Partner Organization
PACE - Pacific Asian Consortium in Employment
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight


1
STATE OF CALIFORINADEPARTMENT OF COMMUNITY SERVICES AND DEVELOPMENTCSD 515A (Rev. 2/12/16)
1.2.
3.
4.
5.
6.
7.
8.
9.
10.
Owner-Occupant or Tenant InformationOwner-Occupant or Tenant (Print or type name) Address
ENERGY SERVICE AGREEMENT FOR OCCUPANTDwelling Information
Select the Dwelling Type I am the
Single-Family Mobile Home Multi-Unit Owner-Occupant Tenant
Apt./Unit No. City ZIP Code Telephone Number
Owner-Occupant or Tenant Email Address Owner-Occupant or Tenant FAX Number
Mobile home units only: I acknowledge that I may not receive services that require a permit if the registration on the mobile unit is not up-to-date.
Owner-Occupant or Tenant Acceptance of Terms for CSD Weatherization Services(to be completed by the Owner-Occupant or Tenant)
I agree to accept the following TERMS required for my primary residence to receive services from the Department of Community Services and Development (CSD) weatherization programs(s):
I acknowledge that the Rental Property Owner must grant the Contractor/Agency the same permissions by signing CSD 515B Energy Service Agreement for Rental Property Owner before any services are rendered.
I certify that the above-listed property is my primary residence.I (the Owner-Occupant or Tenant), grant the Contractor/Agency permission to enter my dwelling to perform assessments, conduct diagnostics, take photos only of weatherization work to be performed or deferred (as it relates to individual or whole house services), install feasible weatherization services and perform inspections in accordance with CSD weatherization program policies and standards to the above-listed dwelling.
I acknowledge that an assessment of my dwelling is necessary to determine the work that can be performed and that the work that is available may be limited due to the needs and condition of my residence. Identified work may not be provided if it does not meet all program requirements and specifications and may lead to full or partial deferral of work. My refusal of certain work may prevent the installation of other identified work in accordance to program requirements.
I hereby release and pledge to hold harmless the Contractor/Agency listed below, and its staff, from any liability in connection with the work identified on a summarized list, except as a consequence of gross negligence or willful and wanton misconduct.I authorize the Contractor/Agency to access my utility company records to obtain only energy usage data for a period of one year before and two years after weatherization measures are installed.
I grant the Contractor/Agency, local, State and/or Federal inspectors permission to enter the dwelling after reasonable notice to perform inspections to verify the existence and quality of work performed by the Contractor/Agency and compliance with local, State, and/or Federal building codes and programmatic guidelines and acknowledge that a permit may be required for specific weatherization work. I understand that I may be held financially responsible for the weatherization work if I refuse to allow access for inspection and permitting purposes.
I shall not remove any permanently installed energy conservation measures unless they are damaged or no longer functional in the residence from where they were installed.
I acknowledge and agree that this property is not for sale at the time of qualifying for the program and will not be offered for sale or otherwise distributed for at least sixty days following the completion of weatherization services.
Additional Certifications For Owner-Occupants ONLY:
Additional Certifications For Tenants ONLY:
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight

2
STATE OF CALIFORINADEPARTMENT OF COMMUNITY SERVICES AND DEVELOPMENTCSD 515A (Rev. 2/12/16)
ENERGY SERVICE AGREEMENT FOR OCCUPANT
11.
12.
13.
1.
2.3.4.
5.6.
Owner-Occupant or Tenant’s Signature Date
I understand that the Property Owner cannot raise the rent of the unit for a period of two years from the date of weatherization because of the increased value of the unit due solely to weatherization measures provided by the Contractor/Agency (allowable factors for rent increase include an actual increase in property taxes, actual cost of amortizing other improvements to the property accomplished after the date of work completed by the Contractor/Agency, or actual increases in expenses of maintaining and operating this property).
I acknowledge that I have been provided a copy of this Agreement explaining its terms effective for a two year period after weatherization services have been completed. Complaint Process: In the event the provisions of this Agreement related to increased rent or the landlord’s failure to decrease utility costs for master metered units are not met, tenants may contact the Contractor/Agency to submit a verbal or written complaint, which will be investigated by the Department of Community Services and Development. Contractor/Agency contact information is located on this Agreement under the section entitled, “Contractor/Agency Assurance.”
Contractor/Agency AssuranceContractor/Agency (Print name) Address
I may retain the replacement energy conservation measure installed by the CSD weatherization program(s) if the replaced appliance was my personal property .
I CERTIFY THAT I am the Owner-Occupant or Tenant residing in the dwelling listed above that serves as my primary residence and that all given statements are true and correct to the best of my knowledge. I have read and understand these TERMS and RELEASE, and agree to be bound by all of its terms and conditions in order to receive weatherization services under the CSD weatherization program(s).
CSLB Number (if applicable) City ZIP Code Contractor/Agency Telephone Number
Contractor/Agency Email Address Contractor/Agency FAX Number
The Contractor/Agency agrees to the following:Shall be responsible for the feasible cost of weatherization measures performed other than cash contribution from the Owner or Owner Agent, if applicable, and any subsequent non-compliance.Shall ensure that the Contractor/Agency is properly insured.Shall ensure that work is conducted in a professional manner and meets program and building code standards.Shall not make any significant structural changes to the dwelling without requesting written permission specifically describing the change from the dwelling owner.Shall provide in writing a list of all weatherization measures installed in the unit. Shall assure that the owner, or owner's agent, and tenant data shall be maintained in a confidential manner to assure compliance with the Information Practices Act of 1977, as amended, and the Federal Privacy Act of 1974, as amended.
Agency Program Manager’s Signature Agency Program Manager's Name (Print name) Date
Rachelle Arizmendi
Pacific Asian Consortium in Employment (PACE) 1055 Wilshire Blvd.,Suite 900E
Los Angeles 90017 (213) 989-3255
(213) [email protected]
mlee
Highlight
Page 1 of 3
STATE OF CALIFORINADEPARTMENT OF COMMUNITY SERVICES AND DEVELOPMENTCSD 515B (Rev. 2/12/16)
Single Mobile
City ZIP Code
City ZIP Code
City ZIP Code
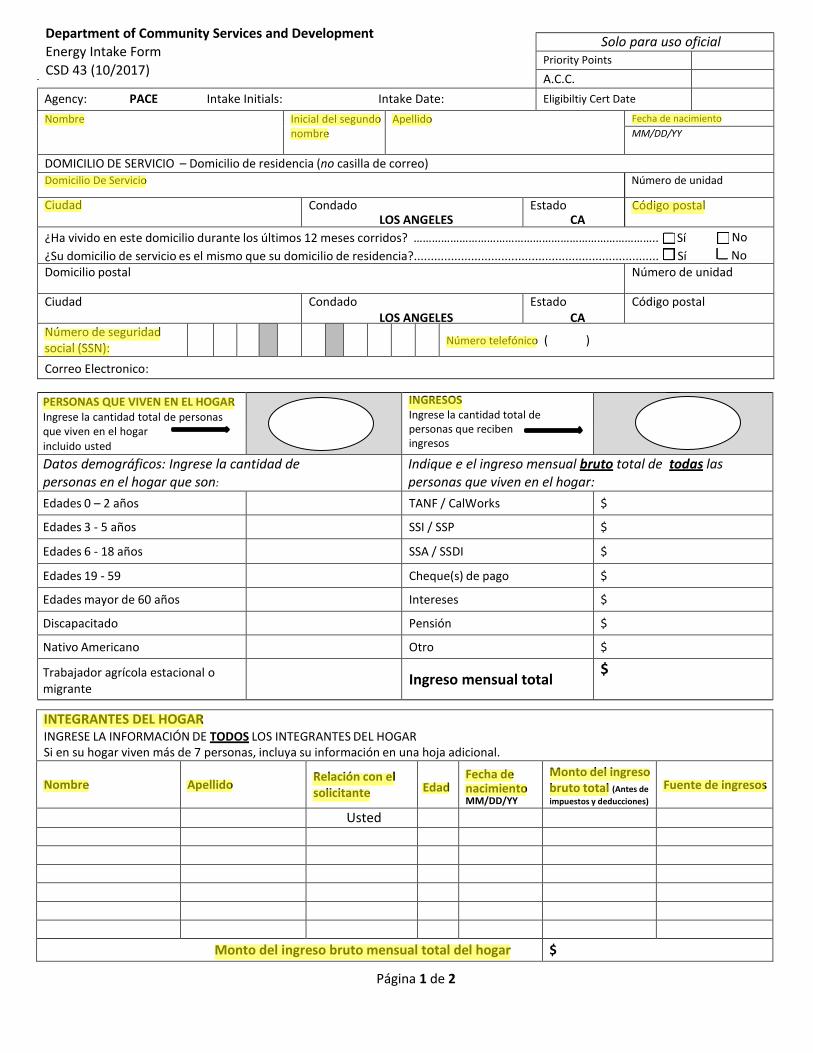
Agent Email Address Agent FAX Number
Apt./Unit No. City ZIP Code Agent Telephone Number
Owner Email Address Owner FAX Number
Apt./Unit No. City ZIP Code Owner Telephone Number
If the Owner uses an agent for the above-referenced property, complete both Owner and Agent information.Agent (Print or type name) Address
List Qualified Units List Vacant and Unqualified Units
Owner and Owner's Agent InformationOwner (Print or type name) Address
# of Units in Building # of Units to be Weatherized # of Vacant & Unqualified Units
List Qualified Units List Vacant and Unqualified Units
Building #3Complex/Building Name (if applicable) Building Address
# of Units in Building # of Units to be Weatherized # of Vacant & Unqualified Units
Building #2Complex/Building Name (if applicable) Building Address
# of Vacant & Unqualified Units
Number of Eligible Buildings in Complex: Use additional pages, if necessary.
Building #1Building AddressComplex/Building Name (if applicable)
List Qualified Units List Vacant and Unqualified Units
# of Units to be Weatherized# of Units in Building
City Zip Code Type
Multi-Family Dwelling/Complex Information
ENERGY SERVICE AGREEMENT FOR RENTAL PROPERTY OWNERSingle-Family/Mobile Home Dwelling Information
Tenant Name Dwelling Address
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight
mlee
Highlight

Page 2 of 3
STATE OF CALIFORINADEPARTMENT OF COMMUNITY SERVICES AND DEVELOPMENTCSD 515B (Rev. 2/12/16)
ENERGY SERVICE AGREEMENT FOR RENTAL PROPERTY OWNER
1.2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.14.
15.
I certify that I am the Owner (or Owner's Agent) of the above-listed rental property.I grant the Contractor/Agency permission to enter my property to perform assessments, conduct diagnostics, take photos only of weatherization work to be performed or deferred (as it relates to individual or whole house services), install feasible weatherization measures and perform inspections in accordance with CSD weatherization program policies and standards to the above-listed rental property.
I acknowledge that an assessment of my property is necessary to determine the work that can be performed and that the work that is available may be limited due to the needs and condition of my property. Identified work may not be provided if it does not meet all program requirements and specifications and may lead to full or partial deferral of work. My refusal of certain work may prevent the installation of other identified work in accordance to program requirements.
I shall not remove any energy conservation measures unless they are damaged or no longer functional in the rental property from where they were installed. If the replaced item (i.e. refrigerator or other appliance) was the personal property of my tenant, the tenant shall retain the replacement energy conservation measure installed by the CSD weatherization program(s).
Mobile home units only: I acknowledge that my property may not receive services that require a permit if the registration is not up-to-date.
I hereby release and pledge to hold harmless the Contractor/Agency listed below, and its staff, from any liability in connection with any work identified on a summarized list except as a consequence of gross negligence or willful and wanton misconduct.
Additional Certification for Unoccupied Multi-Unit Dwellings ONLY:
I certify that I, as the Owner or Owner's Agent, shall ensure that gas or electric service, or both, that is provided by a master-meter to tenants shall be charged at the utilities' costs in accordance with California Public Utilities Commission Code Section 739.5 or other applicable government regulations.
I certify that I, as the Owner or Owner's Agent, shall not raise the rent of any weatherized unit for a period of two years from the date of weatherization because of the increased value of the unit due solely to weatherization measures provided (allowable factors for rent increase include an actual increase in property taxes, actual cost of amortizing other improvements to the property accomplished after the date of work completed by the Contractor/Agency, or actual increases in expenses of maintaining and operating this property).
I acknowledge and agree that this property is not for sale at the time of qualifying for the program and will not be offered for sale or otherwise distributed for at least sixty days following the completion of weatherization services.
Owner or Owner's Agent Acceptance of Terms for CSD Weatherization Services(to be completed by the Owner or Owner's Agent)
I agree that "rent" is defined as the tenant's monthly payment to the Owner (non-subsidized housing) or the contract rent (subsidized housing).I shall submit to the Contractor/Agency a schedule of rents prior to commencement of work.
Federal, State or Local Government Rehabilitation Projects only: I certify that if a vacant unit is counted as being an eligible household for purposes of meeting the minimum threshold for whole building weatherization (66% rule), then the unit will become occupied by an eligible family within 180 days after the completion of weatherization (CFR 440.22(b)(2)(ii)).
I agree to accept all of the following TERMS required for my rental property to receive services from the Department of Community Services and Development (CSD) weatherization program(s):
I certify that I shall provide a copy of this Agreement explaining its terms to all tenants and subsequent tenants residing in the unit within the two year period. Complaint Process: In the event the provisions of this Agreement related to increased rent or the landlord’s failure to decrease utility costs for master metered units are not met, tenants may contact the Contractor/Agency to submit a verbal or written complaint, which will be investigated. Contractor/Agency contact information is located on this Agreement under the section entitled, “Contractor/Agency Assurance.”
I authorize the Contractor/Agency to access my complex's utility company master-metered records to obtain only energy usage data for a period of one year before and two years after weatherization measures are installed.
I grant the Contractor/Agency, local, State and/or Federal inspectors permission to enter the dwelling after reasonable notice to perform inspections to verify the existence and quality of work performed by the Contractor/Agency and compliance with local, State, and/or Federal building codes and programmatic guidelines and acknowledge that a permit may be required for specific weatherization work. I understand that I may be held financially responsible for the weatherization work if I refuse to allow access for inspection and permitting purposes.

Page 3 of 3
STATE OF CALIFORINADEPARTMENT OF COMMUNITY SERVICES AND DEVELOPMENTCSD 515B (Rev. 2/12/16)
ENERGY SERVICE AGREEMENT FOR RENTAL PROPERTY OWNER
1.
2.3.4.
5.6.
Y N Y N
Required Documentation:
Rent schedule received from Property Owner, if applicable? If applicable, CSD 75 completed?
Shall assure that the owner, or owner's agent, and tenant data shall be maintained in a confidential manner to assure compliance with the Information Practices Act of 1977, as amended, and the Federal Privacy Act of 1974, as amended.
Contractor/Agency Program Manager’s Signature Contractor/Agency Program Manager's Name (Print name) Date
Shall ensure that the Contractor/Agency is properly insured.Shall ensure that work is conducted in a professional manner and meets program and building code standards.Shall not make any significant structural changes to the dwelling without requesting written permission specifically describing the change from the dwelling owner.Shall provide in writing a list of all weatherization measures installed in the rental unit.
Contractor/Agency Email Address Contractor/Agency FAX Number
The Contractor/Agency agrees to the following:Shall be responsible for the feasible cost of weatherization measures performed other than cash contribution from the Owner or Owner Agent, if applicable, and any subsequent non-compliance.
CSLB Number (if applicable) City ZIP Code Contractor/Agency Telephone Number
Contractor/Agency AssuranceContractor/Agency (Print or type name) Address
I CERTIFY THAT I am the Owner or Owner's Agent of the Dwelling or Complex listed above, and that all given statements are true and correct to the best of my knowledge. I have read and understand these TERMS and RELEASE, and agree to be bound by all of its terms and conditions in order for my property to receive weatherization services under the CSD weatherization program(s).
Owner’s (or Owner's Agent’s) Signature Date
Rachelle Arizmendi
Pacific Asian Consortium in Employment (PACE) 1055 Wilshire Blvd., Suite 900E
Los Angeles 90017 (213) 989-3255
(213) [email protected]
mlee
Highlight