Nuevas estrategias en el tratamiento del cáncer de …2013/06/05 · BIG 2-06 / GSK EGF106708 A...
44
Nuevas estrategias en el tratamiento del cáncer de mama HER2 positivo Antonio González Martín Servicio Oncología Médica
Transcript of Nuevas estrategias en el tratamiento del cáncer de …2013/06/05 · BIG 2-06 / GSK EGF106708 A...

Nuevas estrategias en el tratamiento del cáncer de mama HER2 positivo
Antonio González Martín
Servicio Oncología Médica

Hudis C. N Engl J Med 2007;357:39-51
HER FAMILY

Trastuzumab es tratamiento esencial en cáncer de mama HER2+
CM Metastásico
• Tratuzumab + quimioterapia aumenta la RR, TTP, OS 1,2
CM Precoz
• Trastuzumab aumenta DFS y OS en adyuvancia3,4,5.
• Trastuzumab aumenta pCR en neo-adyuvancia 6,7
1. Slamon et al. N Eng J Med 2001. 2. Marty et al. J Clin Oncol 2005. 3. Perez et al. J Clin Oncol 2011 4. Gianni et al. Lancet Oncol 2011. 5. Slamon et al. N Eng J Med 2011. 6. Buzdar et al. J Clin Oncol 2005. 7. Gianni L et al. Lancet 2010.
Dawood et al. J Clin Oncol 2010.

Se debe mantener terapia anti-HER2 tras progresión a trastuzumab
Lapatinib-capecitabina es superior a capecitabina
Trastuzumab-capecitabina es superior a capecitabina
Von Minckwitz et al. J Clin Oncol 2009 Geyer et al. N Eng J Med 2006

Bloqueo dual traztuzumab (MoAb) + lapatinib (TKI) es superior a lapatinib monoterapia en pacientes
pretratadas con trastuzumab
Blackwell et al. J Clin Oncol 2012

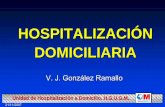
Neo-ALTTO trial (BIG 01-06)
Stratification: • T≤5 cm vs. T>5 cm •ER or PgR + vs. ER & PgR – • N 0-1 vs. N ≥ 2 •BCS or not
Invasive operable HER2+ BC T > 2 cm (IBC excluded) LVEF 50% N=450
34 weeks
52 weeks of anti-HER2 therapy
lapatinib
trastuzumab
lapatinib
trastuzumab
FEC X 3
S U R G E R Y
R A N D O M I Z E
lapatinib
trastuzumab
lapatinib
trastuzumab
paclitaxel
paclitaxel
paclitaxel
+ 12 wks 6 wks
Baselga J et al. SABCS 2010

Efficacy – pCR and tpCR
L: lapatinib; T: trastuzumab; L+T: lapatinib plus trastuzumab pCR pathologic complete response

Valachis. Breast Cancer Res Treat (2012) 135:655–662
Trastuzumab > lapatinib
Trastuzumab + lapatinib > trastuzumab

ALTTO
(Adjuvant Lapatinib and/or Trastuzumab Treatment Optimisation) study. BIG 2-06 / GSK EGF106708 A randomised, multicentre, open-label, phase III study of adyuvant lapatinib, trastuzumab, their sequence and their combination in patients with HER2/ErbB2 positive primary breast cancer. NCT00490139
Design 1: All (neo)adjuvant chemotherapy is completed prior to study treatments Design 2: A taxane is given concurrently with study treatments Design 2B: Nonanthracycline regimen containing docetaxel and carboplatin given concurrently with study treatments (Design 2B available in North America only for new patient enrollment)

Potential Molecular Mechanisms of Trastuzumab Resistance
Upregulation of HER2 downstream signaling pathways
MAPK PI3K
Obstacles for trastuzumab binding to HER2
Her2
Signaling through alternate pathways
IGFR / HER3
Intracellular signalling pathways
SRC

HER2:HER3 dimers may provide an escape mechanism from trastuzumab
+ + + +
+ + + + + + +
Signalling activity
+ + + +
Homodimers Heterodimers
HER1:HER1 HER2:HER2
HER3:HER3 HER4:HER4 HER1:HER2 HER1:HER3 HER1:HER4 HER2:HER3
HER2:HER4 HER3:HER4
Tzahar et al. Mol Cell Biol 1996 Sergina et al. Nature 2007

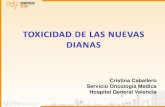
HER2
Dominio de dimerización
Cho et al. Nature 2003;421:756–760; Fendly et al. Cancer Res 1990;50:1550–1558; Franklin et al. Cancer Cell 2004;5:317–328; Nahta et al. Cancer Res 2004;64:2343–2346; Scheuer et al. Cancer Res 2009;69:9330–9336
Pertuzumab
HER3
Trastuzumab
Subdominio IV
• Trastuzumab
• Inhibe la pérdida del dominio extracelular de HER2 y por tanto inhibe la formación de p95
• Pertuzumab
• Previene la dimerización del receptor
• Inhibe la señalización mediadas
por HER2/HER2 y HER2/HER3
• Activan la citotoxicidad celular dependiendo de anticuerpo
Pertuzumab, el primer inhibidor de la dimerización de HER2

Ensayo fase II de Trastuzumab más Pertuzumab en pacientes
con cáncer de mama metastásico que progresan durante el
tratamiento con Trastuzumab
Cohorte 1 y 2: Trastuzumab + Pertuzumab Cohorte 3: Pertuzumab (tras PE) Trastuzumab + Pertuzumab
Respuesta, n (%) TRZ +PRT (n = 66)
PTZ (n = 29a)
PRT+TRZ (n = 16b)
Respuesta completa 4 (6,1)c 0 (0,0) 0 (0,0)
Respuesta parcial 12 (18,2)c 1 (3,4) 3 (21,4)
Tasa de respuesta objetiva 16 (24,2) 1 (3,4) 3 (21,4)
Enfermedad estable durante 8 ciclos (6 meses) 17 (25,8) 2 (6,9) 3 (21,4)
Tasa de beneficio clínico 33 (50,0) 3 (10,3) 6 (42,8)
Progresión de la enfermedad 33 (50,0) 24 (82,8) 8 (57,1)
Nuevas Estrategias en el Tratamiento del Cáncer de Mama HER2+. SEOM, Madrid 2010

Gianni SABCS 2010

NeoSphere: RCp en la mama. Población ITT
Gianni L et al. Lancet Oncol 2012

Cáncer de Mama Metastásico HER2 + (lab central) Primera linea n=808
Docetaxel 75mg/m2
Trastuzumab 8mg/kg seguido 6mg/kg
Docetaxel 75mg/m2
Trastuzumab 8 mg/kg seguido 6 mg/kg Pertuzumab 840 mg seguido de 420 mg
1:1
CLEOPATRA Trial
Baselga et al, NEJM 2011 Swain et al, Lancet Oncol 2013



Swain et al, Lancet Oncol 2013
Baselga et al, NEJM 2011
HR 0·66, 95% CI 0·52−0·84; p=0·0008; Survival median 36 m vs NR
HR 0.64 95% CI, 0.47 to 0.88; P = 0.005

CLEOPATRA Trial Toxicidad

International randomised study (approx. 120 sites worldwide) HER2-positive MBC progressing after first-line trastuzumab-based therapy
PHEREXA: A Phase II trial of trastuzumab + capecitabine with or without pertuzumab in second-line HER2-positive MBC
• Enrolment stratified by:
– CNS metastases
– Measurable vs nonmeasurable disease
– Response to first-line trastuzumab therapy
• Primary endpoint:
– PFS by independent review
Trastuzumab + capecitabine
Trastuzumab + capecitabine + pertuzumab
1:1 randomisation
HER2-positive MBC (n=450)
CNS = central nervous system; MBC = metastatic breast cancer; PFS = progression-free survival
Data on file. Genentech USA, Inc., CA, USA and F Hoffmann-La Roche Ltd., Basel, Switzerland

LoRusso P M et al. Clin Cancer Res 2011;17:6437-6447
T-DM1: Trastuzumab linked to potent cytotoxic agent DM1, a derivative of maytansine, is microtubule
inhibitor 20 to 100 fold more potent than vincristine

Trastuzumab Emtansine (T-DM1): Mechanism of Action
Emtansine release
Inhibition of microtubule
polymerization
Internalization
HER2
Adapted from LoRusso PM, et al. Clin Cancer Res 2011.
T-DM1
Lysosome
Nucleus
P P
P
Trastuzumab-specific MOA • Antibody-dependent cellular
cytotoxicity (ADCC) • Inhibition of HER2 signaling • Inhibition of HER2 shedding

T-DM-1: Efficacy in phase II trials
• Two single-arm phase 2 trials in patients who received ≥1 HER2-directed therapies for MBC – ORR: 25.9% (N=112)1 and 34.5% (N=110)2
• Randomized phase 2 trial in patients without prior HER2-directed therapy for MBC – Median PFS longer with T-DM1 (n=67) vs. trastuzumab +
docetaxel (n=70)
– 14.2 vs. 9.2 months (HR=0.59; P=0.035)3
1Burris HA, et al. J Clin Oncol 2011; 2Krop I, et al. J Clin Oncol 2012; 3Hurvitz S, et al. ESMO 2011

OCTOBER 1ST, 2012

EMILIA Study Design
• Stratification factors: World region, number of prior chemo regimens for MBC or unresectable LABC, presence of visceral disease
• Primary endpoints: PFS by independent review, OS, and safety
• Key secondary endpoints: PFS by investigator, ORR, DOR
• Statistical considerations: Hierarchical statistical analysis was performed in pre-specified sequential order: PFS by independent review → OS → secondary endpoints
PFS analysis: 90% power to detect HR=0.75; 2-sided alpha 5% OS analyses: 80% power to detect HR=0.80; 2-sided alpha 5%
1:1
HER2-positive LABC or MBC (N=980)
•Prior taxane and trastuzumab
•Progression on metastatic treatment or within 6 months of adjuvant treatment
PD
T-DM1 3.6 mg/kg q3w IV
Capecitabine 1000 mg/m2 PO bid, days 1–14, q3w
+ Lapatinib
1250 mg/day PO qd
PD

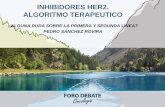
Progression-Free Survival by Independent Review
496 404 310 176 129 73 53 35 25 14 9 8 5 1 0 0
495 419 341 236 183 130 101 72 54 44 30 18 9 3 1 0
Cap + Lap
T-DM1
No. at risk by independent review:
Median (months)
No. of events
Cap + Lap 6.4 304 T-DM1 9.6 265 Stratified HR=0.650 (95% CI, 0.55, 0.77)
P<0.0001
0.0
0.2
0.4
0.6
0.8
1.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30
Pro
po
rtio
n p
rogr
ess
ion
-fre
e
Time (months)
Unstratified HR=0.66 (P<0.0001).

Progression-Free Survival Subgroup Analyses Pre-specified Stratification Factors
Median, mos
T-DM1
HR (95% CI)
Median, mos
Cap + Lap
Total n
Baseline characteristic
T-DM1 better
Cap + Lap better
Hazard ratio 0.2 0.5 1 2 5
9.6 0.66 (0.56, 0.78) 6.4 991 All patients
8.5
10.9
9.6
0.70 (0.51, 0.98)
0.56 (0.41, 0.74)
0.73 (0.56, 0.94)
5.7
6.4
6.9
270
317
404
World region US Western Europe Other
10.3
8.5
0.68 (0.55, 0.85)
0.63 (0.49, 0.82)
6.7
5.7
609
382
Number prior chemo regimens for MBC or unresectable LABC
0–1 >1
9.6
8.5
0.55 (0.45, 0.67)
0.96 (0.71, 1.30)
5.7
10.2
669
322
Disease involvement Visceral
Nonvisceral

Overall Survival: First Interim Analysis
496 469 438 364 296 242 195 155 129 97 74 52 31 17 7 3 2 1 0
495 484 461 390 331 277 220 182 149 123 96 67 46 29 16 5 2 0 0
Cap + Lap
T-DM1
No. at risk: Time (months)
Pro
po
rtio
n s
urv
ivin
g
0.0
0.2
0.4
0.6
0.8
1.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
77.0% 65.4%
47.5%
84.7%
Median (months) No. of events Cap + Lap 23.3 129 T-DM1 NR 94 Stratified HR=0.621 (95% CI, 0.48, 0.81); P=0.0005
Efficacy stopping boundary P=0.0003 or HR=0.617
Unstratified HR=0.63 (P=0.0005). NR, not reached.

Overall Survival: Confirmatory Analysis
496 471 453 435 403 368 297 240 204 159 133 110 86 63 45 27 17 7 4
495 485 474 457 439 418 349 293 242 197 164 136 111 86 62 38 28 13 5
Cap + Lap
T-DM1
No. at risk: Time (months)
78.4% 64.7%
51.8%
85.2%
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n s
urv
ivin
g
Data cut-off July 31, 2012; Unstratified HR=0.70 (P=0.0012).
Median (months) No. of events Cap + Lap 25.1 182 T-DM1 30.9 149 Stratified HR=0.682 (95% CI, 0.55, 0.85); P=0.0006
Efficacy stopping boundary P=0.0037 or HR=0.727

Cap + Lap T-DM1
Baseline characteristic
Total n
Median (mos)
Median (mos)
HR (95% CI)
T-DM1 Better
Cap + Lap Better
All patients 991 25.1 30.9 0.70 (0.56, 0.87)
World region United States 270 23.7 NR 0.62 (0.41, 0.96)
Western Europe 317 28.6 27.8 0.95 (0.65, 1.39)
Asia 158 22.7 34.3 0.48 (0.27, 0.85)
Other 246 22.7 26.1 0.68 (0.45, 1.04)
Number of prior chemotherapeutic regimens for LABC or MBC
0–1 609 28.0 29.8 0.80 (0.61, 1.07)
>1 382 22.7 31.9 0.58 (0.41, 0.81)
Disease involvement Visceral 669 21.9 28.4 0.59 (0.46, 0.76)
Nonvisceral 322 NR 33.9 1.05 (0.69, 1.61)
Overall Survival Subgroup Analyses
From confirmatory OS analysis; data cut-off July 31, 2012.
Hazard ratio 0.2 0.5 1 2 5
NR, not reached.

ORR and DOR in Patients with Measurable Disease
Objective response rate (ORR) Duration of response (DOR)
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n p
rogr
ess
ion
-fre
e
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Median, months (95% CI) Cap + Lap 6.5 (5.5, 7.2) T-DM1 12.6 (8.4, 20.8)
Difference: 12.7% (95% CI, 6.0, 19.4) P=0.0002
120 105 77 48 32 14 9 8 3 3 1 1 0 0 0 0
173 159 126 84 65 47 42 33 27 19 12 8 2 0 0 0
Cap + Lap
T-DM1
No. at risk
0
0
0
0
0
0
Time (months)
Pat
ien
ts, %
0
20
30
40
50
10
T-DM1
173/397 120/389
43.6%
30.8%
Cap + Lap

Adverse Events Grade ≥3 AEs With Incidence ≥2%
Cap + Lap (n=488)
T-DM1 (n=490)
Adverse Event All Grades, % Grade ≥3, % All Grades, % Grade ≥3, % Diarrhea 79.7 20.7 23.3 1.6 Hand-foot syndrome 58.0 16.4 1.2 0.0 Vomiting 29.3 4.5 19.0 0.8 Neutropenia 8.6 4.3 5.9 2.0 Hypokalemia 8.6 4.1 8.6 2.2 Fatigue 27.9 3.5 35.1 2.4 Nausea 44.7 2.5 39.2 0.8 Mucosal inflammation 19.1 2.3 6.7 0.2
Thrombocytopenia 2.5 0.2 28.0 12.9 Increased AST
9.4 0.8 22.4 4.3 Increased ALT
8.8 1.4 16.9 2.9 Anemia 8.0 1.6 10.4 2.7
ALT, alanine aminotransferase; AST, aspartate aminotransferase.

EARLY BREAST CANCER KAITLIN (Adjuvant study ) Study Design
Herceptin+Pertuzumab
AC/FEC
T-DM1+Pertuzumab
S U R G E R Y
3-4 Cycles
Taxane
4 Cycles or 12 Weeks
AC/FEC
3-4 Cycles
Taxane
4 Cycles or 12 Weeks
Stratification: • World region • Nodal Status • Hormonal
receptor status
Primary Endpoint: IDFS
R N = 1750
Central confirmed HER2
Follo
w u
p 1
0 y
ears

1st Line mBC Phase III MARIANNE Study: BO22589/TDM4788g
Patients with HER2 positive progressive or recurrent locally advanced breast cancer or previously untreated metastatic breast cancer
Primary endpoints: PFS as assessed by IRF; Safety Secondary endpoints: OS; PFS by investigator; PRO analyses; Biomarkers Superiority design with a Non-inferiority analysis between each of the experimental arms and the control arm Interim futility analysis: Option to drop experimental arm
Arm A
Arm B
Arm C
Planned FPI June 2010
Trastuzumab + Taxane (until PD) n=364
T-DM1+Pertuzumab (until PD) n=364
T-DM1+Pertuzumab placebo (until PD) n=364
Patients stratified by:
World region
Neo/Adjuvant therapy (Y/N)
Trastuzumab based therapy (Y/N)
Visceral disease (Y/N)
n=1092

Th3RESA: Study Design
Primary end points: OS, ORR Selected secondary end points: PFS, safety, PRO Stratification: World region, # prior therapies, presence of visceral disease Key Inclusion criteria: • Prior anthracycline, taxane, capecitabine, lapatinib, and trastuzumab • Progression on at least 2 regimens of HER2-directed therapy for MBC Treatment of physician’s choice: • Commercially available cancer therapy administered according to local practice
(may include HER2 targeted regimens)
Study treatment continues until disease progression or unmanageable toxicity
HER2 positive (Centrally confirmed)
Un-resectable locally advanced/recurrent or Metastatic breast cancer
T-DM1 q3w
Treatment of physician’s choice
Approx 795 patients 2:1 randomization
2
1

PI3K/mTOR/Akt pathway

PI3K mutation and low PTEN predict low response to trastuzumab
Patients with an activated PI3K pathway due to either PTEN loss or PIK3CA mutation have a significantly shorter PFS.
Berns et al. Cancer Cell 2007

Number at risk
Pla+T+D WT 191 164 136 114 66 46 23 17 9 3 1
Pla+T+D Mut 90 76 56 37 21 17 8 4 3 2 1
Ptz+T+D WT 190 179 159 137 90 71 46 26 16 5 3
Ptz+T+D Mut 86 71 61 44 29 25 12 6 2 1 1
21.8 12.5 13.8 8.6
Pla+T+D: WT Pla+T+D: Mut
Ind
ep
en
de
ntl
y-as
sess
ed P
FS (
%)
0
10
20
30
40
50
60
70
80
90
100
Time (months)
101 events
63 events
45 events
83 events
Ptz+T+D: WT Ptz+T+D: Mut
0 32.9 3.3 6.6 10.9 13.2 16.4 19.7 23.0 26.3 29.6
CLEOPATRA PIK3CA mutation associated with poorer prognosis
Both arms
17
Mut, mutated; WT, wild-type



Clinical trials overcoming mechanisms of trastuzumab resistance
MAPK PI3K/mTOR/Akt
Her2
Intracellular signalling pathways
SRC
LUX-Breast 1 Vinorelbine + Trastuzumab
Vs
Vinorelbine + Afatinib
BOLERO-3 Vinorelbine + Trastuzumab
Vs
Vinorelbine + Trastuzumab +
Everolimus
NALA Capecitabine + Lapatinib
Vs
Capecitabine + Neratinib
BOLERO-1 Paclitaxel + Trastuzumab +
Placebo Vs
Paclitaxel + Trastuzumab +
Everolimus

Conclusiones
• Primera línea:
– Taxano-Pertuzumab-trastuzumab
– Futuro?:
• T-DM1+Pertuzumab +/- taxano
• Paclitaxel-Trastuzumab-Everolimus
• Paclitaxel-Trastuzumab- Lapatinib
• Segunda línea
– T-DM1
– Futuro?:
• Everolimus
• Axatinib
• Neratinib
• Tercera línea
– Capecitabina-Lapatinib
• Algunas alteraciones moleculares podrán ayudar a seleccionar el tratamiento (i.e mutaciones de PI3K).

Muchas Gracias