Paraganglioma case presentation
14
An undiagnosed case of An undiagnosed case of Paraganglioma: A Paraganglioma: A nightmare for the nightmare for the Anesthesiologist Anesthesiologist Presenters: Dr Amit Sabharwal Authors: Dr Amit Kohli, Dr Sanjay Nihlani, Dr Prashanth, Dr Sunil Thakur, Dr Sonia Wadhawan, Dr Poonam Bhadoria Maulana Azad Medical College and associated LN Hospital, New Delhi.
-
Upload
prashsubbu -
Category
Documents
-
view
30 -
download
3
description
case of paragnaglioma managed peroperatively
Transcript of Paraganglioma case presentation

An undiagnosed case An undiagnosed case of Paraganglioma: A of Paraganglioma: A nightmare for the nightmare for the AnesthesiologistAnesthesiologist
Presenters: Dr Amit Sabharwal Authors: Dr Amit Kohli, Dr Sanjay Nihlani, Dr Prashanth, Dr Sunil Thakur, Dr Sonia Wadhawan, Dr Poonam BhadoriaMaulana Azad Medical College and associated LN Hospital, New Delhi.

Patient ProfilePatient ProfileA 75 yr old male,ASA-1, with an intra-abdominal swelling provisionally diagnosed as retroperitoneal tumor was posted for laprotomy under GA • Pain abdomen- 2-3 months, Mass abdomen- 4 to 5 yrs• U/S: large retroperitoneal solid cystic mass 16x9.6x10.4 cm in dimensions CECT: large heterogeneously enhancing solid cystic mass with multiple enhancing septe Diagnosis: ??retroperitoneal mesothelioma, histopath correlation advised

Pre Anaesthetic Pre Anaesthetic EvaluationEvaluation• No significant past history- no h/o of any
ailment, previous operation,drug intake, & palpitations/chest pain ,family history
• O/E –BP 124/80, Pulse 64/min, R/R 16bpm,
Pallor present.–Cardiac , GI, Renal & Pul System NAD– Inv included Xray chest, ECG, Hemogram,
KFT, SE, & LFT , Urine R,M were all WNL except Hb which was 9 gm%
Optimization: 1 unit packed cell transfusedPlan: General anesthesia with epidural
analgesia

Perioperative EventsPerioperative EventsStandard anesthesia protocol:
On manipulation of mass Vitals, Ecg changes
Inj Xylocard, Inj propofol Vent Bigeminy
repeat dose of Inj Xylocard Vent Tachycardia,Palpable
pulses,hypertension manipulation stopped,inj amiadarone
bolus,infusion NTG infusion
vitals under control Sx continued ,mass resected!

Perioperative EventsPerioperative EventsSudden hypotensionFluid resuscitation
Stable hemodynamicsMonitored over 30 min,regular respiration
Extubatiion trial attemptedShifted to ICU
Uneventful postoperative period
•Epidural care• Histopathological report- paraganglioma with concurrent tuberculosis!

Differential DiagnosisDifferential Diagnosis?Intraoperative hypertension..?Hypertensive episode precipitating an arythymia?Undiagnosed catecholamine secreting tumour•Intraoperative events in retrospect point to the mass being a silent paraganglioma.•Though Clinical suspicion is primal in aiding diagnosis, lack of any signs and symptoms preoperatively caught us off guard• Retroperitoneum, a common site of occurrence for paragangliomas.
Plausible scenario for the anesthesiologist to encounter..

Pheochromocytoma,paraganPheochromocytoma,paragangliomasgliomas tumors arising from catecholamine producing
chromaffin cells (adrenal /extra adrenal). Not under neurogenic control Account for less than 0.1% of all cases of
hypertension in adults. Eitiology: isolated (90%), inherited
(10%),both sexes of any age affected 10% can turn malignant - liver,bone,spinal
cord,lungs,brain and lymph nodes. Most tumors secrete NE either alone or more
commonly combined with a smaller amount of EP (85:15). 15% secrete EP alone.

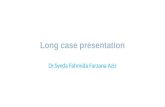
Topographic Topographic sitessites
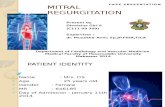
Signs and symptomsSigns and symptoms

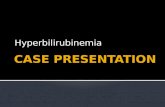
Catecholamine pathway and sites of action of various drugs

Preoperative managementPreoperative managementDetailed history,physical
examination,laboratory and cardiac evaluation.
Optimization with pharmacological agentsPreoperative blood pressure goals: no
standard guidelines: 130/80 mm Hg (while sitting),100 mm Hg systolic (while standing, not less than 80/45 mm Hg)
Heart rate: 60-70/min while sitting, 70-80/min while standing
Ref: Preoperative management of the pheochromocytoma patient. Karel Pacak. J Clin Endocrinol Metab. Nov 2007,92(11):4069-4079

Drugs used:Drugs used: Alpha adrenoceptor antagonists: phenoxybenzamine,prazosin,terazosin,doxazocin
Beta adrenoceptor antagonists: atenolol, metoprolol, propranolol
Combined alpha and beta receptor blockers: labetalol,carvedilol
Calcium channel blockers: amlodipine, nicardipine, nifedipine,varapamil
Catecholamine synthesis inhibitors

Intraoperative managementIntraoperative managementConcerns during induction, intubation, surgical
incision, abdominal exploration, manipulation, vein ligation,reversal.
Monitoring- noninvasive and invasiveAvoid morphine, atracurium, atropine,
pancuronium, succinylcholineSafe-
thiopentone,etomidate,benzodiazepines,fentanyl,
sufentanil,alfentanil,enflurane,isoflurane,nitrous oxide,vecuronium and rocuronium

Drugs useful prior to ligation SNP,phentolamine,niroglycerin,labetalol,magnesium sulphate,lidocaine,esmolol,amiadarone,diltiazem
Hypotension-most common cause of death(intra and post op) fluids,depth of anesthesia, vasopressors ( phenylephrine, norepinephrine) ,inotropes (dopamine)
Post operative:Vasopressor supportSteroid supplementationHypoglycemiaVentilatory support