Case Presentation Basha
24
CASE PRESENTATION ALAMURI KHADHAR BASHA 3 rd YEAR 1 ST SEM
-
Upload
khaderbasha2020 -
Category
Documents
-
view
240 -
download
0
Transcript of Case Presentation Basha

CASE PRESENTATION
ALAMURI KHADHAR BASHA3rd YEAR 1ST SEM

GENERAL DATA• Patient’s Name: Gil juanico Sex: M Age: 54 y.o.• Religion: Roman Catholic Occupation: Elementry school teachar• Address: Davao city Status: Single• Date Admitted: Jan.3,2014 Date of birth: Jun.15,1959• Reliability: 80%

CHIEF COMPLAINT*”PROLONGED BODY WEAKNESS & ABDOMINAL PAIN “*

HISTORY OF PRESENT ILLNESS
• Patient felt severe abdominal pain in the LUQ,pain score of 7-8/10.
• Pain was radiating back to left flank and over symphysis pubis,burning type quite near the epigastric area,where he feels/locate it significantly.
• Aggrevated at night and with empty stomach, relived by having some semi solid foods.
• Consulted a clinic,where he was diagnosed to have UTI & managed with antibiotics (can’t recall).
• Patient stated it was his starting day of unproper diet or indigestion.PARTINENT (+) =Abdominal pain,constipation
PARTINENT (-) =Fever,cough,vomiting, Haematemesis
18 Days PTA,on Dec.16

• Patient felt severe pain,over the anal region,pain score of 8/10.
• Aggrevated by walking or doing some activities & relived by resting.
• Consulted in DMSF OPD,diagnosed to have internal hemorrhids & prescribed to have policresulin + cinchocaine hcl,some pain killers (cant recall).
• Patient stated his unproper diet was continuing so,he balanced with soft diet.
4 Days PTA,on Dec.3

• Patient stated that he was not able to tolerate his unproper diet,which he mentioned it as prolonged body weakness.
• So,he admitted DMSF hospt. Stating his chief complaint as prolonged body weakness with abdominal pain and previously diagnosed UTI.
• Laboratory tests CBC(showed dec.hemoglobin and inc.glucose) ,following endoscopy was done upon admission.
ODA, Jan.3

PAST MEDICAL HISTORY
• Yr 2006 at age 45yrs -> HYPERTENSION (10) at Annual school. check up.
• Of unknown age -> ARTHRITIS.• Immunizations -> Cant recall.
CURRENT REGIMEN:• Diclofenac 50mg bid/day• Neobloc 50mg bid/day• Metoprolol 100mg bid/day• Luserten ???• Polocerculin + cinchocine hcl

PERSONAL AND SOCIAL HISTORY
• Occational drinker (kind in parties)• Somking none• Description of life style: works from 8am – 5pm,busy schedule & after reaching home relaxes himself to
relive the stress• Diet-fruits,bread,fish,vegetables.1cup rice/meal• Allergies - none

FAMILY HISTORY
• Mother(66)• father.(79)• (-) diabetes mellitus,tb,jaundice,stroke,heart disease.
HYPERTENSION

PHYSICAL EXAMINATION• VITAL SIGNS: BP 140/70, HR 72, Temp 36.8,RR 24.
• GEN APP: middle-aged MALE breathing spontaneously, answers yes or no to questions.
• HEENT: R pupil reactive 4mm 2 mm. L pupil sluggish and minimally reactive. No oral lesions. Tongue normal. No carotid bruits, JVD, thyromegaly or LAD.
• LUNGS:symmetrical ,no crackles heard.
• HEART: No gallops, murmurs, rubs, heaves or thrills.
• ABDOMEN: Hypoactive bowel sounds. burning, moderate to severe tender ness.
• EXTREMITIES: No c/c. No edema.
• SKIN: No rashes, echymoses or needle tracks.
• NEUROLOGIC: As described above. She is moving all extremities.
• RECTAL:No rectal exam done ,has hemorrhoids,tenderness.

REVIEW OF SYSTEMS• General: (+) changes in weight, (-) sweats, (+) weakness, (-) fatigue• Skin: (-) itchiness, (-) color changes, (-) pigmentation, (-) rashes, (-)
photosensitivity, changes in hairs and nails• Eye: (-) blurring of vision, (-) redness, (-) itchiness, (-) pain, (-) increased
lacrimation• Ear: (-) deafness, tinnitus, discharge• Nose: (-) epistaxis, (-) nasal discharge, obstruction, (-) postnasal drip• Mouth and throat: (-) bleeding gums, sores, fissures, tongue abnormalities,
dental caries, (-)sore throat, lump sensation• Pulmonary: (-) hemoptysis

• Cardiac: (-) easy fatigability, orthopnea, nocturnal dyspnea, syncope, edema• GI: (-) retching, hematemesis, melena, hematochezia, belching,
(+)dysphagia, indigestion, food intolerance, flatulence, (+)abdominal pain, constipation, hemorrhoids, (-) diarrhea, (-) vomiting
• GU: (-) urinary frequency, urgency, hesitancy, nocturia• Musculoskeletal: (+) joint stiffness, pain,(-) swelling, cramps, muscle pain,
weakness, wasting• Endocrine: (-) heat-cold intolerance, polyuria, polydipsia• Hematopoietic: (-) abnormal bleeding, (-) bruising• Neurologic: (-) headache, seizure, mental status changes, head trauma

DIFFERENTIAL DIAGNOSIS• Chronic gastritis• Gastric ulcer• Pancriatitis• Stomach cancer

CHRONIC GASTRITIS
• RULE IN
• RULE OUT
•Upper abdominal discomfort
•Nausea,vomiting

GASTRIC ULCER
• RULE IN
• RULE OUT
•Epigastric pain,burning or aching pain•Pain reffered to back,weight loss•Pain worsen at night & while eating
•Nausea,vomiting,bloating,belching

PANCRIATITIS
• RULE IN
• RULE OUT
•LUQ abdominal pain,radiating back,pain worsen during intake of meal
•Vomiting,nausea,fever,jaundice

STOMACH CANCER
• RULE IN
• RULE OUT
•Stomach pain,sense of fullness,loss of appetite,weight loss,trouble to swallow
•Nausea,vomiting,tarry black stools,jaundice
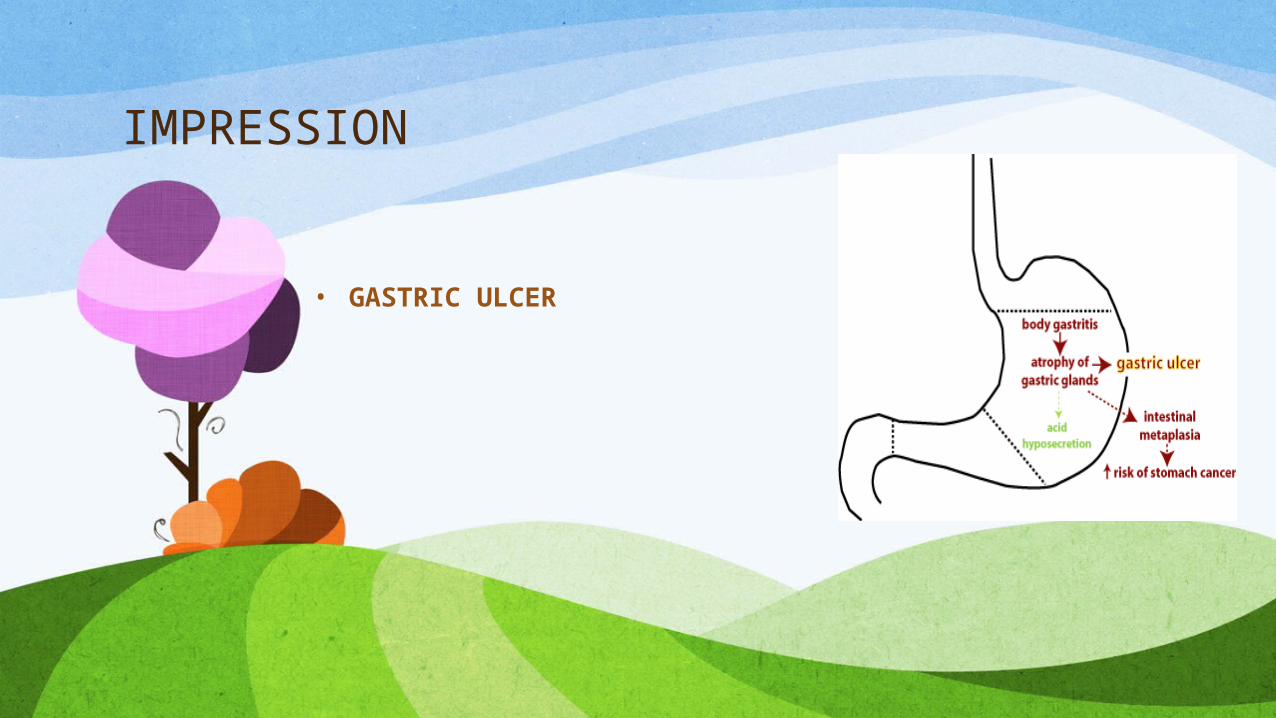
IMPRESSION
• GASTRIC ULCER
DIAGNOSTICS• Physical examination• Endoscopy• Upper gastrointestinal (UGI) series • Stool occult blood test
H.PYLORI INFX: • Non invasive -> -serology -Carbon labeled urea breath test• Invasive -> -Rapid urease test

SALIENT FEATURES - HISTORY• Epigastric pain,burning or aching pain
• Pain reffered to back
• Pain worsen at night & while eating
• Sense of fullness,loss of appetite,weight loss,trouble to swallow
• Use of pain killers and arthritis hx medications
MANAGEMENTANTI BI OTI CS
-metrodinazole , amoxicillin , clarithromycin-to eradicate h.pylori-surgical intervention
PROTON PUMP I NHI BI TORS
-clansoprazole , omeprazole
• Proton pump inhibitors (or "PPI "s) are agroup of drugs whose main action is pronounced and long-lasting reduction of gastric acid production.
Bismuth salts-suppress or eradicate h.pylori
Smoking reduction and restDietary modifi cation Surgical procedure
-vagotomy-Billroth I and Billroth I I

VAGOTOMY ANTRECTOMY (BILLROTH I)
• A vagotomy is a surgical procedure that is performed only in humans. It is resection(removal of, or at least severing) of part of the vagus nerve.
• is the resection, or surgical removal, of a part of the stomach known as the antrum. The antrum isthe lower third of the stomach that lies between the body of the stomach and the pyloric canal, which empties into the first part of the small intestine.

GASTROJEJUNOSTOMY (BILLROTH II)• A procedure in which the duodenum is excised or bypassed
and the stomach is end to end anastomosed to jejunum
• FOLLOW UP CHECK UP