Colectomia Izquierda, Anastomosis Termino-Terminal
11
Los TERRYbles BooK TeaM
-
Upload
wildor-herrera-guevara -
Category
Documents
-
view
16 -
download
1
description
colectomia izquierda.
Transcript of Colectomia Izquierda, Anastomosis Termino-Terminal

Los TERRYbles BooK TeaM

Los TERRYbles BooK TeaM

Los TERRYbles BooK TeaM
Los TERRYbles BooK TeaM

Los TERRYbles BooK TeaM

Los TERRYbles BooK TeaM

Los TERRYbles BooK TeaM
INDICATIONS
The operation is performed chiefly for tumor of the left colon or a complication of diverticulitis.
PREOPERATIVE PREPARATION
Tumors of the left colon are frequently of the stenosing type. Patients with this condition often
come to the surgeon with symptoms of impending intestinal obstruction.
When obstruction is not complete, the bowel can best be prepared over a period of days by
oral administration of the appropriate cathartics, and a clear liquid diet for the last 48 hours.
The frequency with which cathartics and cleansing agents are administered will vary
depending upon the amount of obstruction. The level and nature of the obstruction may be
confirmed by barium enema; however, colonoscopy allows biopsy for pathologic identification,
identification and removal of additional lesions such as polyps, and potential evaluation of the
proximal colon. In the presence of total obstruction, a nasogastric tube is passed for
decompression and the colon is emptied from below with enemas. Evaluation of the distal
colon with colonoscopy is valuable and a virtual colonoscopy may be obtained with special
CT imaging to evaluate the proximal colon. A baseline CEA (Corio Embryonic Antigen) blood
test is obtained. If this and enzymatic liver function tests are elevated, CT or imaging scans of
the abdomen and liver may be obtained to evaluate metastatic spread. Perioperative
antibiotics are given. A Foley catheter may be inserted, especially if a prolonged or complex
operation is anticipated.
ANESTHESIA
Either general or spinal anesthesia is satisfactory.

Los TERRYbles BooK TeaM
POSITION
The patient is placed in a comfortable supine position and rotated slightly toward the operator.
A slight Trendelenburg position may be used. If the colon tumor or process is in the lower left
colon or sigmoid region, many surgeons will position the patient in a modified lithotomy
manner using Allen stirrups supporting the knees and ankles. This will allow for prepping and
draping of the rectal region for potential passage of an EEA stapling device. The legs are
spread and the knees elevated sufficiently to provide this access to the rectum but not so high
or wide as to interfere with the abdominal portion of the operation.
OPERATIVE PREPARATION The skin is prepared in the routine manner.
INCISION AND EXPOSURE
The operator stands on the patient's left side. A liberal midline incision is made about the level
of the umbilicus. The liver as well as other possible sites for metastasis are explored. The
small intestines are then packed away medially with warm, moist gauze sponges or placed in
a plastic bag outside the abdomen on the right side. A gauze pack is placed toward the pelvis
and another along the lateral wall up to the spleen.
DETAILS OF PROCEDURE
Precautions against possible spread of the tumor should include limited manipulation of the
growth and application of a clamp, such as a Kocher, above and below the tumor to avoid
further seeding of the mucosal surfaces. As soon as possible the tumor should be covered
with gauze and its major supply clamped.
With the bowel at the point of the lesion held in the left hand, the lateral peritoneal reflection
of the mesocolon is incised close to the bowel except in the region of the tumor over as wide
an area as seems essential for its free mobilization (Figure 1). Following this, the bowel is
retracted toward the midline and the mesentery is freed from the posterior abdominal wall by
blunt gauze dissection. Troublesome bleeding may occur if the left spermatic or ovarian vein
is torn and not ligated. The left ureter is identified because it must not be drawn up with the
mesentery of the intestine and accidentally divided. A fan-shaped incision of sufficient size is
made so that the entire left colic artery and vein down to their origins can be removed so as to
maximize removal of regional lymph nodes (Figure 2). Some surgeons perform this division
as soon as possible to minimize angiolymphatic spread of tumor from manipulation and
traction of the specimen. In this technique, originally called "no touch," it is essential that the
surgeons have already identified the left ureter as well as the inferior mesenteric and sigmoid
vessels (see Anatomy of the Large Intestine, Vessels 8 and 9). At least 10 cm of margin from
the gross border on either side of the lesion should be allowed. The contents of the clamps
applied to the mesentery are tied. The mesenteric border of the bowel at the proposed site of
resection is cleared of mesenteric fat in preparation for the anastomosis (Figure 3).
In most patients, the splenic flexure of the colon is mobilized to avoid an anastomosis under
tension. This maneuver is easier and safer to accomplish if the midline incision is extended

Los TERRYbles BooK TeaM
up to the xyphoid. This technique is shown in Figures 15, 16, and 17. Alternatively, the
omentum may be removed in its relatively avascular junction along the left colon until the
splenocolic region is reached. The descending left colon is then mobilized superiorly along
the extension of the lateral line of Toldt. By approaching both ends toward the middle, the
sometimes difficult splenocolic omental attachments are safely visualized and divided with
minimal risk of splenic injury.
Paired crushing clamps of the Stone or similar type are placed obliquely across the bowel
above the lesion within 1 cm of the limits of the prepared mesentery (Figure 4). The field is
walled off with gauze, and the bowel is divided. A pair of noncrushing clamps is then applied
to the prepared area below the lesion, and the bowel is divided in a similar fashion. The ends
of the large intestine are brought end to end to determine whether the anastomosis can be
carried out without tension; The clamps are approximated and so manipulated that the
posterior serosal surface of the intestine is presented, to facilitate placement of a layer of
interrupted mattress 000 silk sutures (Figure 5). The mesenteric border should be free of fat
to achieve accurate approximation of the serosa. The sutures at the angles are not cut and
are utilized for traction (Figure 6).
Enterostomy clamps are placed several centimeters from the crushing clamps, and the
crushing clamps are removed (Figure 6). The portions of excessive bowel that were beyond
the clamps may be excised. The field is completely walled off with moist, sterile gauze packs,
and a direct open anastomosis is carried out. The mucosa is approximated with a continuous
lock suture on an atraumatic needle starting in the middle of the posterior layer (Figure 7). At
the angle, the lock suture is changed to one of the Connell type to ensure inversion of the
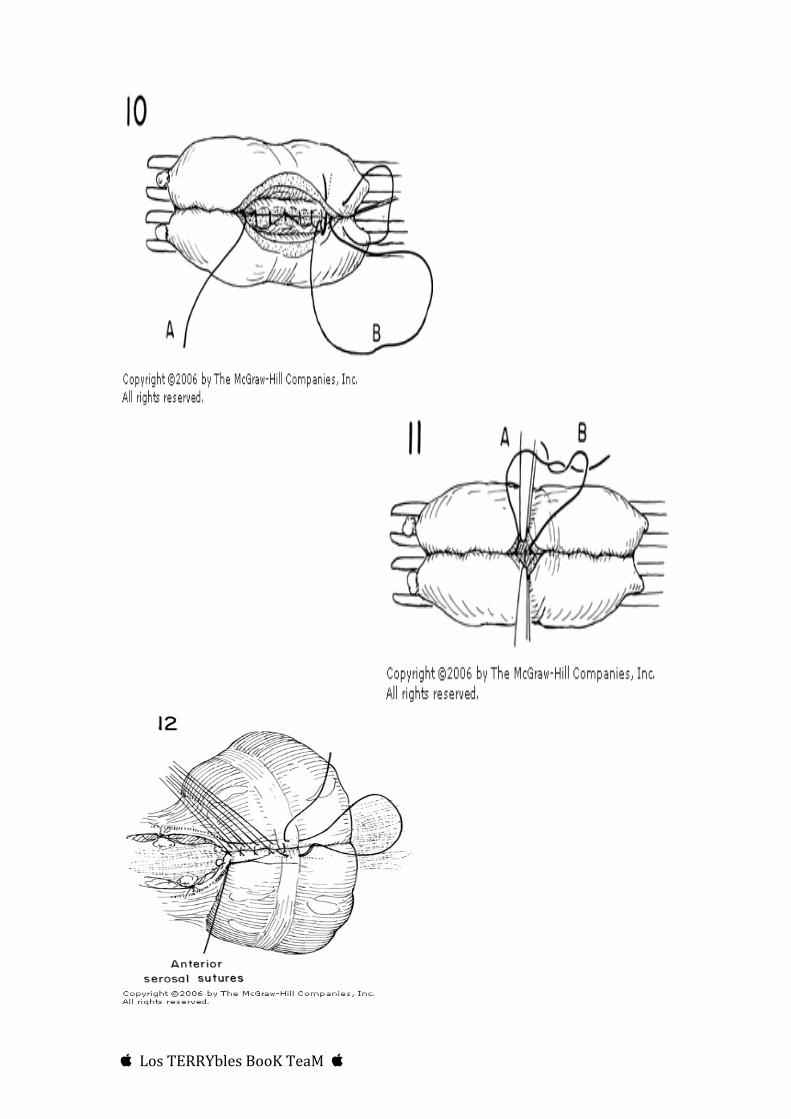
angle and the anterior mucosa (Figures 8 and 9). A second continuous suture is started
adjacent to the first one and is carried out in a similar fashion (Figure 10). After the mucosa
has been accurately approximated, the two continuous sutures, A and B, are tied with the
knot on the inside (Figure 11). A layer of interrupted 000 silk sutures or nonabsorbable
sutures is utilized to approximate the anterior serosal layer. Particular attention is given to
either angle to ensure accurate and secure approximation.
Alternative techniques for colon anastomoses include the use of single layer of delayed
absorbable interrupted sutures with knots within the lumen and the use of stapling
instruments. The latter technique is shown in Colon Anastomoses, Stapled.
Following the approximation of the mucosal layer, all contaminated instruments are
discarded. The field is covered with fresh moist gauze sponges and towels. It is desirable for
the members of the surgical team to change gloves. The anastomosis is further reinforced by
an anterior serosal layer of interrupted 000 silk sutures (Figure 12). It is sometimes advisable
to reinforce the mesenteric angle with one or two additional mattress sutures. Any remaining
opening of the mesentery is then closed with interrupted sutures of fine silk. If there is a great
deal of fat in the mesentery, which tends to hide the location of blood vessels, it is unwise to
pass a needle blindly through it lest a hematoma form between the leaves of the mesentery. It
is safer to grasp the peritoneal margins of the mesentery with small, pointed clamps and

Los TERRYbles BooK TeaM
effect a closure by simple ligation of their contents. Finally, adequacy of the blood supply to
the site of the anastomosis should be inspected. Active, pulsating vessels should be present
adjacent to the anastomosis on both sides (Figure 13). If the blood supply appears to be
interfered with and the color of the bowel is altered, it is better to resect the anastomosis
rather than risk leakage and potentially fatal peritonitis. The patency of the stoma is carefully
tested by compression between the thumb and index finger (Figure 14). It is usually possible
to obtain a two-finger stoma.
To assure easy approximation of the open ends of the large bowel, especially if the lesion is
located near the splenic flexure, it is necessary to free the intestine from adjacent structures.
The abdominal incision may have to be extended up to the costal margin, since exposure of
the uppermost portion of the splenic flexure may be difficult. After the relatively avascular
peritoneal attachments to the descending colon have been divided, it is necessary to free the
splenic flexure from the diaphragm, spleen, and stomach. The splenocolic ligament is divided
between curved clamps, and the contents are ligated to avoid possible injury to the spleen,
with troublesome hemorrhage (Figure 15). Following this, a pair of curved clamps is applied
to the gastrocolic ligament for the necessary distance required to mobilize the bowel or
remove sufficient intestine beyond the growth. Sometimes, in the presence of growths in this
area, it is necessary to carry the division adjacent to the greater curvature of the stomach.
The surgeon should not hesitate to remove a portion of the left gastroepiploic artery, if
indicated, since the stomach has such a good collateral blood supply. In some instances, a
true phrenocolic ligament can be developed, which must be divided to free the splenic flexure
(Figure 16).
If it is necessary to free a portion of the transverse colon, the omentum may be freed from the
bowel by incising its avascular attachments adjacent to the colon (Figure 17; see also
Gastrectomy, Subtotal—Omentectomy). In some instances, omentum may be involved with
the growth, and it may be desirable to remove all or part of it. The splenic flexure is reflected
medially following the division of its attachments, and care is taken to avoid the kidney and
the underlying ureter. It is usually necessary to divide a portion of the transverse mesocolon
(Figure 18). This should be done carefully, taking into consideration possible injury to the
underlying jejunum in the region of the ligament of Treitz. The large inferior mesenteric vein
will also require division and double ligation as it dips down under the inferior margin of the
body of the pancreas to join the splenic vein. The bowel is freed of all fatty attachments at the
site selected for anastomosis. Noncrushing clamps are applied, and the bowel is divided
(Figure 19). Arterial pulsations in the mesentery on both sides should be verified. The
anastomosis is carried out as previously described. If it becomes necessary to ligate the
middle colic artery, the entire transverse colon, including the hepatic and splenic flexures,
may need to be resected to ensure an adequate blood supply at the site of anastomosis. In
this situation the viability of the colon depends upon the right colic artery on one side and the
left colic artery on the other.

Los TERRYbles BooK TeaM
CLOSURE
The closure is made in the usual manner.
POSTOPERATIVE CARE
The patient is encouraged to cough, sit up, and ambulate as soon as possible. The
nasogastric tube provides decompression until bowel activity returns, usually on the first or
second day after surgery. Oral intake of clear liquids is begun and advanced as tolerated,
whereupon IV hydration and electrolytes are discontinued. Antibiotics are given in the
perioperative period or for a few days longer if gross contamination has occurred.