Patologia vascular Aneurisma Diseccion aortica Trombo embolia e infarto.
Upload
universidad-del-valle-universidad-de-antioquiaCategory
view
526download
4description

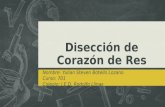
DISECCION AORTICA AGUDA
DIAGNOSTICO Y TRATAMIENTO DE LA AORTA DESCENDENTE
ESTADO DEL ARTE

DR. LEONARDO BALLESTAS MALDONADO
RESIDENTE DE CIRUGIA VASCULAR
UNIVERSIDAD DE ANTIOQUIA
DR. WILLIAM RAMIREZ
PROFESOR CIRUGIA VASCULAR
IPS UNIVERSITARIA
UNIVERSIDAD DE ANTIOQUIA

EVIDENCIA
• Se realiza una búsqueda de la evidencia en lasbases de datos Medline, Embase, Cohcrane,Tripdatabase, Scielo
• Palabras clave: Acute aortic dissection,management, surgical and endovaculartreatment, acute aortic syndrome, TEVAR

NIVELES DE EVIDENCIA

SINDROME AORTICO AGUDO
DISECCION AORTICA AGUDA
HEMATOMA INTRAMURAL
ULCERA AORTICA PENETRADA
2010 - Guidelines for the Diagnosis and Management of Patients With Thoracic AorticDisease. AHA

Desgarro espontáneo en la intima permitiendo que la sangre bajo presión se dirija entre la intima y la media de la pared
aórtica
Isselbacher EM:Diseases of the aorta. In Braunwald E, et al: heart diseases:Textbook of Cardiovascular Medicine, 6 th ed, 2001,p.1431
DEFINICION
Aguda de 2 semanas
Crónica de 2 semanas

DISECCION
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010

• Es la afección mas frecuente de la aorta quepone en peligro la vida
• Incidencia estimada en la población general esde 2.6 – 3.5 por 100.000 hab. Por año
• IRAD (International Registry of Acute AorticDissection), reporta que la mayoría de lospacientes tienen entre 60 – 80 años
DISECCION AORTICA
Hagan PG, Nienaber CA. International Registry of Acute Aortic Dissection (IRAD): new insights from an olddisease. JAMA. 2000;283:897–903.

65%
20%
10%
5%
Crawford ES, Coselli JS. Diffuse aneurysmal disease (chronic aortic dissecction, Marfan, and mega aorta syndromes)and multiple aneurysm. Ann Surg 1990; 211: 521
DISECCION AORTICA

FACTORES DE RIESGO
• Aneurisma aórtico preexistente
• Enfermedades inflamatorias que causen vasculitis
• Desordenes del colágeno (Sind. Marfan – Ehler-Danlos)
• Historia familiar
Hipertensión arterial (72% de los pacientes)
Ateroesclerosis (31% de los pacientes)
IRAD (International Registry of Acute Aortic Dissection)

CLASIFICACION
III AIII B

NUEVA CLASIFICACION
• Clase 1– Disección aortica clásica
( colgajo intimal)
• Clase 2– Disrupción de la media
– Hematoma intramural
• Clase 3– Disección sutil \ sin
hematoma
• Clase 4
– Placa rota con ulceración aortica
– Ulcera aortica penetrante con hematoma subyacente
• Clase 5
– Disección traumática o iatrogénica
Diagnosis and management of aortic dissection. Recommendations of the Task Force onAortic Dissection, European Society of Cardiology. 2001

HISTORIA NATURAL
DISECCION TIPO A
• Altamente letal
• Mortalidad 1-2% / hora
• Dolor de inicio subito
• dolor torácico 85%
• Espalda(46%)
• dolor abdominal (22%)
• Síncope (13%)
• ECV (6%)
DISECCION TIPO B
• Menos letal
• Mortalidad 20% al día 2 y del 25%al día 25 con complicacionesisquemicas y 10% en 30 días
• Inicio subito de dolor espalda (64%)
• Torax (63%)
• Abdominal (43%)
• ECV(21%)
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010

PRESENTACION CLINICA
• Dolor torácico (96%)
• Asociado a sincope (13%),ECV (6%), IAM, ICC (7%)
• Pulso ausente o débil,carotideo, braquial ofemoral
HISTORIA CLINICAEXAMEN FISICO

CARACTERISTICAS
TIPO A TIPO B
Frecuencia 60-75% 25-40%
Sexo (M:F) 1.7-2.6 : 1 2.3-3.1
Edad 50-56 60-70
hipertensión ++ +++
E. T. Conectivo ++ +
Dolor retroesternal +++ + –
Dolor interescapular
+ – +++
Síncope ++ + –

TIPO A TIPO B
ICC + –
IAM + –
Efusion pleural + – +++
Dolor abdominal + – + –
Deficit pulso periferico
Ms Inferiores y Ms Superiores
Ms Inferiores
Regurgitación valvula aórtica
++ + –
ACV + –
CARACTERISTICAS

SINDROME DE MALAPERFUSION
Localización Frecuencia
Renal 23 – 75%
Extremidades 25 – 60%
Mesentérica 10 – 20%
Coronarias 5 – 11%
Cerebral 3 – 13%
Espinal 2 – 9%

DIAGNOSTICO DIFERENCIAL
• Síndrome coronario agudo
• Regurgitación aortica sin disección
• Aneurisma aórtico sin disección
• Dolor musculo esquelético
• Pericarditis
• Tumores mediastinales
• Pleuritis
• TEP
• Colecistitis

DIAGNOSTICO
ALTO INDICE DE SOSPECHA
HISTORIA CLINICAY EXAMEN FISICO
LABORATORIO
• RX DE TORAX• AORTOGRAMA• ANGIOTAC TORAX• ANGIO RESONANCIA• ECOCARDIOGRAMA TT• ECOCARDIOGRAMA TE

RADIOGRAFIA DE TORAX
Rx de Torax:anormal en 60-90% sinespecificidad
Luker GD, Glazer HS. Aortic dissection: effect of prospective chest radiographic diagnosis on delay to definitivediagnosis. Radiology 1994; 193: 813-819. Circulation 1995; 92 (Supl 9): II107-112.

1. Ensanchamiento mediastinal 50%
1. Borramiento del botón aórtico
1. Casquete arco aórtico
1. Ensanchamiento botón aórtico distal a la subclavia izquierda
1. Engrosamiento de la pared aórtica
1. Derrame pleural usualmente izquierdo
1. Separación de la calcificación intimal del borde externo aórticomayor de 1 cm.signo del calcio
Luker GD, Glazer HS. Aortic dissection: effect of prospective chest radiographic diagnosis on delay to definitivediagnosis. Radiology 1994; 193: 813-819. Circulation 1995; 92 (Supl 9): II107-112.
RADIOGRAFIA DE TORAX

OBJETVOS DEL ESTUDIO DE IMAGEN
• Confirmar el diagnostico
• Clasificar la disección, extensión
• Diferenciar el lumen falso y verdadero
• Localizar los flap intímales
• Identificar ramas comprometidas
• Detectar el grado de regurgitación aórtico
• Detectar extravasación (hematoma peri aórtico o mediastinales,derrame pleural o pericárdico
Diagnosis and management of aortic dissection. Recommendations of the Task Force onAortic Dissection, European Society of Cardiology. 2001

Radiación y medio de contraste
Disponibilidad limitada
Sensibilidad 93 –100%,
especificidad 87 –100%
Evaluación precisa y rápida
Portátil y mínimamente invasivo
Bajo costo
Sensibilidad 77 – 88%, especificidad 93 – 96%
Técnica mas completa
No requiere medio de contraste
Sensibilidad y especificidad cercanas
al 100%
Costosa y poco disponible

COMPARACION DE ESTUDIOS DE IMAGEN
Estudio Sensibilidad Especificidad
Aortografia 80-90% 88-95%
Tomografia 90-100% 90-100%
Ultrasonido 94-100% 97-100%
Ecocardio T-T 60-80% 80-96%
Ecocardio T-E 90-99% 85-98%
Resonancia 98-100% 98-100%
Greenberg et al. Eur J Vasc Endovasc Surg .2003.26(6): 579

• Tratamiento optimo depende de undiagnostico oportuno y un entendimiento dela anatomía
• El control de la presión arterial es unelemento clave en todos los pacientes
• En las disecciones tipo A, la mortalidad en lafase aguda puede ser de 1% por hora
TRATAMIENTO
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010

TRATAMIENTO
DISECCION AORTICA AGUDA TIPO A
DISECCION AORTICA AGUDA TIPO B
MANEJO QUIRURGICOURGENTE
MANEJO QUIRURGICO O ENDOVASCULAR
MANEJO ENDOVASCULAR
COMPLICADA NO COMPLICADA
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010
TRATAMIENTO MEDICO

RECOMENDACIÓN – CLASE - RECOMENDACION I II III NE
Historia clínica y examen físico completo X C
Acceso venoso y muestras de sangre (CK, Troponina, Hemograma, Dimero D, LDH)
X C
EKG: Documentar isquemia X C
Monitorización de la presión arterial X C
Manejo del dolor (opioides) X C
Reducir la frecuencia cardiaca y presión arterial (B-bloqueadores)
X C
Traslado a UCI X C
Pacientes con HTA severa iniciar vasodilatadores X C
Pacientes con contraindicación de B-bloqueo utilizar calcio antagonistas
X C
Estudio de imagen en pacientes con EKG con signos de isquemia antes de trombolisis si se sospecha patología aortica
X C
Radiografía de Tórax X C
Diagnosis and management of aortic dissection. Recommendations of the Task Force onAortic Dissection, European Society of Cardiology. 2001

TRATAMIENTO MEDICO
• 1960 Wheat y Palmer
• El tratamiento en la unidad de cuidadosintensivos es el primer paso en todo pacientecon disección aortica aguda
• El objetivo inicial es la reducción de lasfuerzas hemodinámicas que han iniciado ypropagado el flap intimal
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010

OBJETIVO DEL TRATAMIENTO MEDICO
• Reducción de la frecuencia cardiaca
• Reducción de la presión arterial sistólica
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010
CONTRAINDICADO EN PACIENTES HIPOTENSOS

RECOMENDACIONES
1. Iniciar beta bloqueo, con la meta de una frecuencia cardiacamenor de 60 lat/min (nivel evidencia C)
2. En los pacientes que estén contraindicados los b-bloqueadores sedeben usar calcio antagonistas no dihidropiridinicos (nivelevidencia C)
3. Después de obtener un adecuado control de la frecuenciacardiaca, si la TAS es > 120 mmHg, se debe iniciar unvasodilatador intravenoso, para lograr una TAS entre 105 – 120mmHg o TAM entre 60 – 70 mmHg (nivel evidencia C)
CLASE I
2010 - Guidelines for the Diagnosis and Management of Patients With Thoracic AorticDisease. AHA

MEDICAMENTOS
BETA BLOQUEADORES
• LABETALOL (Efecto alfa y beta)
• ESMOLOL (Acción corta)
• METOPROLOL
• PROPANOLOL
VASODILATADORES
NITROPUSIATO DE SODIO
VERAPAMILO
DILTIAZEM
2010 - Guidelines for the Diagnosis and Management of Patients With Thoracic AorticDisease. AHA

MANEJO MEDICO
• La mayoría de los pacientes no se presentan concomplicaciones y responden bien al manejoinicial
• Estudios muestran que hasta el 90% de lospacientes se les realiza tratamiento medico solo
• IRAD reporta una sobrevida de 78% a tres años
• Elefteriades JA, Lovoulos CJ, Coady MA, Tellides G, Kopf GS, Rizzo JA: Management of descending aortic dissection. AnnThorac Surg 67: 2002-2005, 1999
• Hagan PG, Nienaber CA, Isselbacher EM, et al: The International Registry of Acute Aortic Dissection (IRAD): new insightsinto an old disease. JAMA 283:897-903, 2000
• Estrera AL, Miller CC, Safi HJ, et al: Outcomes of medical management of acute type B aortic dissection. Circulation114:I384-389, 2006

MANEJO QUIRURGICO
DISECCION TIPO A
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010

• Dolor torácico persistente o recurrente
• Crecimiento (expansión) aortica
• Hematoma peri aórtico
• Hematoma mediastinal
• Disección en una aorta previamente aneurismática
• Complicaciones isquémicas periféricas
MANEJO QUIRURGICO O INTERVENCIONISTA
DISECCION TIPO B AGUDA COMPLICADA
Diagnosis and management of aortic dissection. Recommendations of the Task Force onAortic Dissection, European Society of Cardiology. 2001

MANEJO QUIRURGICO
RUPTURA O AMENAZA DE RUPTURA EN EL FLAP INTIMAL AORTICO EN LA AORTA
DESCENDENTE PROXIMAL
DISECCION TIPO B
“IN OUR VIEW REMAINS THE ONLY INDICATION FOR ACUTE OPEN GRAFT REPLACEMENT IN PATIENTS WITH DISTAL DISSECTION”Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th
Edition. 2010. – Capitulo 135- Pag: 2099

TECNICA QUIRURGICA
• Resección del segmento aórtico lesionado
• Excisión desgarro intimal
• Obliteración falsa luz sutura o reaproximación de los bordes o extremos de la aorta, disecar tanto proximal como distal
• Reconstitución flujo a través de la verdadera luz
• Restablecer la continuidad de la aorta
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010

TECNICAS QUIRURGICA
• Reparo proximal de la disección
• Reemplazo aorta torácica y abdominal
• Fenestración abierta
• Puentes extra-anatómicos
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010

• La resección debe limitarse a la aorta proximal, ya quela mortalidad y la isquemia medular se incrementandrásticamente*
• El 20 – 25 % de los pacientes presentan persistencia delfalso lumen**
• Morbilidad quirúrgica significativa, resultadosequivalentes a la terapia medica y éxito variable en laresolución de los síndromes de mala perfusión
Safi HJ, Miller 3rd CC, Reardon MJ, et al: Operation for acute and chronic aortic dissection: recent outcome withregard to neurologic deficit and early death. Ann Thorac Surg 1998; 66:402-411.*
MANEJO QUIRURGICO
Sasaki S, Yasuda K, Kunihara T, et al: Surgical results of Stanford type B aortic dissection. Comparisons betweenpartial and subtotal replacement of the dissected aorta. J Cardiovasc Surg (Torino) 2000; 41:227-232.**

• 82 pacientes
• 70% tratados quirúrgicamente con sustitución de la aortadescendente, 21% reemplazo parcial del arco y 8% reemplazo totaldel arco
• Mortalidad fue del 29.3% (mas alta en los pacientes que requirieroncirugía dentro de las 24 horas del ingreso)

• Serie de 22 pacientes sometidos a reemplazo desegmento aórtico con injerto
• Lesiones isquémicas en la medula espinal en 7pacientes (32%)
• La disección aguda perse fue un predictorsignificativo de déficit neurológico postoperatorio(OR: 10.59, IC 95%, p= 0.002)
Safi HJ, Miller 3rd CC, Reardon MJ, et al: Operation for acute and chronic aortic dissection: recent outcome withregard to neurologic deficit and early death. Ann Thorac Surg 1998; 66:402-411.*
MANEJO QUIRURGICO

RECOMENDACIONES
RECOMENDACIÓN – CLASE - RECOMENDACION I II III NE
Terapia medica X C
Reemplazo quirúrgico de la aorta si: Signos persistentes o recurrentes de dolor, crecimiento temprano, complicaciones isquémicas periféricas, ruptura
X C
Manejo quirúrgico o endovascular con fenestracion y colocación de stent si persiste isquemia mesentérica, renal o de miembros inferiores o hay déficit neurológico
X C
Diagnosis and management of aortic dissection. Recommendations of the Task Force onAortic Dissection, European Society of Cardiology. 2001

• Fue descrita en 1999 *
• Se desarrollo de forma intuitiva
• Reduce la incidencia y la gravedad de los síndromes de mala perfusión
• Dake MD, Kato N, Mitchell RS, et al: Endovascular stent-graft placement for the treatment of acute aortic dissection. N Engl JMed 1999; 340:1546-1552.*
• Nienaber CA, Fattori R, Lund G, et al: Nonsurgical reconstruction of thoracic aortic dissection by stent-graft placement. NEngl J Med 1999; 340:1539-1545*
.
MANEJO ENDOVASCULAR

OBJETIVOS DEL MANEJO ENDOVASCULAR
PREVENCION DE UNA FUTURA DEGENRACION ANEURISMATICA DE LA PARED EXTERIORDE LA FALSA LUZ

RESULTADOS A CORTO PLAZO
SERIE NUMERO DE PACIENTES
INDICACIONES (%) INTERVENCION (%)
MORTALIDAD (%)
Greenberg 31 S. Maffan 77Ruptura aortica 23
Stent 94Fenestracion 6
29
Slonim 40 Stent 60Fenestracion 5Ambos 35
25
Lopera 10 Stent 100 0
Duebener 10 S. Marffan 50Ruptura aortica 30
Stent 100 20
Dake 15 Stent 100 20
Schoder 28 S. Marffan 50Ruptura aortica 30
Stent 100 11

• EuroSTAR (European Collaborators onStent/Graft Techniques for Aortic AneurysmRepair)/U.K. Registry
• En el registro, 131 pacientes con disección fuerontratados con stent
• Se logro el éxito técnico primario en el 89% y lamortalidad a 30 días fue de 8.4%, paraplejia 0.8%y la supervivencia a 1 año del 90%
RESULTADOS A CORTO PLAZO

• 609 pacientes
• Tasa de éxito 98.2%
• Mortalidad a 30 días del 5.3% (tres veces mayor en los pacientes con disección aguda
• Tasa de complicaciones neurológicas 2.9%

PROBLEMA
La historia natural de las disecciones tipo B,
controladas médicamente con
persistencia de la falsa luz son un factor de
riesgo independiente para la progresión a
dilatación
Erbel R, Oelert H, Meyer J, et al: Effect of medical and surgical therapy on aortic dissection evaluated bytransesophageal echocardiography. Implications for prognosis and therapy. The European Cooperative Study Groupon Echocardiography. Circulation 1993; 87:1604-1615.

• 19 pacientes, 4 tipo A y 15 tipo B
• Lograron trombosis de la falsa luz en el 100% de lospacientes, con alivio de los síntomas en 76% de lospacientes
• Menor tasas morbilidad y mortalidad comparadas con laintervención quirúrgica
MAYO 20 - 1999

Tsai TT, Evangelista A, Nienaber CA, et al: Partial thrombosis of the false lumen in patients with acutetype B aortic dissection. N Engl J Med 2007; 357:349-359.

Tsai TT, Evangelista A, Nienaber CA, et al: Partial thrombosis of the false lumen in patients with acutetype B aortic dissection. N Engl J Med 2007; 357:349-359.

• Durante los primeros 4 a 7 años después demanejada la disección aortica agudamedicamente, la falsa luz puede desarrollar unadegeneración aneurismática entre el 14 – 40%
• Sueyoshi demostró que un falso lumen crece 3,3mm / año, incluso en condiciones estables y sincomplicaciones*• Hagan PG, Nienaber CA, Isselbacher EM, et al: The International Registry of Acute Aortic Dissection (IRAD): new
insights into an old disease. JAMA 2000; 283:897-903.
• Hata M, Shiono M, Inoue T, et al: Optimal treatment of type B acute aortic dissection: long-term medical follow-up results. Ann Thorac Surg 2003; 75:1781-1784.
• Winnerkvist A, Lockowandt U, Rasmussen E, Radegran K: A prospective study of medically treated acute type B aorticdissection. Eur J Vasc Endovasc Surg 2006; 32:349-355.
• Sueyoshi E, Sakamoto I, Hayashi K, et al: Growth rate of aortic diameter in patients with type B aortic dissectionduring the chronic phase. Circulation 2004; 110(11 Suppl 1):II256-261.*

“ El concepto de sellamiento de la luz falsa con trombosis de esta, mediante una endoprotesis aortica puede reducir las complicaciones tempranas y tardías de la disección de tipo B”
Cronenwett JL, Johnston W. Rutherford`s Vascular Surgery. 7th Edition. 2010
False Lumen Thrombosis

140 pacientes con disección aórtica tipo B estables, aleatorizados en 2 grupos: tratamiento médico óptimo y
TEVAR (n = 72) frente a tratamiento médico óptimo sola (n = 68)

TODAS LAS CAUSAS DE MUERTE
RESULTADOS

MORTALIDAD ESPECIFICA POR CAUSAS DE LA AORTA
RESULTADOS

CRUZA LOS RESULTADOS FRENTE A LOS EVENTOS ADVERSOS
RESULTADOS
La mejoría en la supervivencia y la menor progresión de la enfermedad a los 5 años
se asocio a una trombosis de la falsa luz en el 90.6% de los
pacientes (p<0.0001)

CONCLUSION INSTEAD-XL TRIAL
• "En este estudio los sobrevivientes de la disecciónaórtica tipo B, TEVAR sumado a un tratamientomédico óptimo esta asociado con una mejoría enla supervivencia a cinco años y la progresión de laenfermedad tardía”
• “Pacientes con disección de tipo B con anatomíaadecuada, TEVAR preventivo debe serconsiderado para mejorar los resultados finales”

RESULTADOS A LARGO PLAZO
• 242 Pacientes dados de alta después de manejo de disección de aorta
• Predictores independientes de mortalidad: genero femenino, aneurismaaórtico previo, aterosclerosis, falla renal, durante la hospitalización choque
• Pendiente resultados ADSORB
PACIENTES (%) SOBREVIDA A 3 AÑOS (%)
TERAPIA MEDICA 78 77.6
CIRUGIA ABIERTA 11 82.8
TERAPIA ENDOVASCULAR 11 76.2
Tsai TT, Fattori R, Trimarchi S, et al: Long-term survival in patients presenting with type B acute aorticdissection: insights from the International Registry of Acute Aortic Dissection. Circulation 2006; 114:2226-2231.

• Obstrucción estática de las ramas: stent endovascular
• Obstrucción dinámica de las ramas: stent luz aórtica con o sin fenestración con balón
Hartnell et al. Radiographics 2005; 25: 175-189
INDICACIONES PARA FENESTRACION Y COLOCACION DE STENT


RESULTADOS
• Fenestración más stent no cubiertos en ramasterminales: se restaura el flujo en el 90% delos vasos obstruidos por la disección aórtica
Tasa de mortalidad:10% a 30 días
• Stent graft en disección aórtica: tasa desobrevida a 1 año 90%

• Terapia medica agresiva
• Visitas de seguimiento
• Imágenes seriadas
SEGUIMIENTO
Diagnosis and management of aortic dissection. Recommendations of the Task Force onAortic Dissection, European Society of Cardiology. 2001

TRATAMIENTO
DISECCION AORTICA AGUDA TIPO A
DISECCION AORTICA AGUDA TIPO B
MANEJO QUIRURGICOURGENTE
MANEJO QUIRURGICO O ENDOVASCULAR
MANEJO ENDOVASCULAR
COMPLICADA NO COMPLICADA
TRATAMIENTO MEDICO