Objetivos terapéuticos en el paciente con alto riesgo vascular · Objetivos terapéuticos en el...
39
Objetivos terapéuticos en el Objetivos terapéuticos en el paciente con alto riesgo vascular paciente con alto riesgo vascular Dr. Carlos Guijarro Herraiz Unidad de Medicina Interna
Transcript of Objetivos terapéuticos en el paciente con alto riesgo vascular · Objetivos terapéuticos en el...

Objetivos terapéuticos en el Objetivos terapéuticos en el
paciente con alto riesgo vascularpaciente con alto riesgo vascular
Dr. Carlos Guijarro Herraiz
Unidad de Medicina Interna

Objetivos terapéuticos en el paciente Objetivos terapéuticos en el paciente
con alto riesgo vascularcon alto riesgo vascular-- GUIONGUION
• ¿Qué significa ‘alto riesgo vascular’?– Riesgo vascular: bajo / alto / muy alto
• Objetivos de control– HTA
– Dislipemia
• Otras medidas: antiagregación• Valoración global – tratamiento global

Objetivos terapéuticos en el paciente Objetivos terapéuticos en el paciente
con alto riesgo vascularcon alto riesgo vascular-- GUIONGUION
• ¿Qué significa ‘alto riesgo vascular’?– Riesgo vascular: bajo / alto / muy alto
• Objetivos de control– HTA
– Dislipemia
• Otras medidas: antiagregación• Valoración global – tratamiento global

¿Qué pacientes son de ‘alto riesgo’?
• Elevación marcada de un factor de riesgo– HTA > 180/100
– Hiperlipemias genéticas (HFH)
• Estimación del ‘riesgo global’>20% Riesgo coronario Framingham>5% Mortalidad CV (SCORE)
• Prevención secundaria– Pacientes ‘de muy alto riesgo’

Objetivos de control
• Elevación marcada de un factor de riesgo– Control del FR aislado
• Alto ‘riesgo global’– Objetivo GLOBAL: REDUCIR EL RIESGO– Acción sobre TODOS LOS FACTORES
DE RIESGO
• Prevención secundaria– Pacientes ‘de muy alto riesgo’– Acción intensa sobre TODOS los FR

Alto Riesgo Clínico
Riesgo CVestimado
Reducir riesgo ObjetivoRiesgo CV
Intensidad de tratamiento
302515 205 100
Consejos generales
Consejo individual intensivo
Consejos específicos
Mo
dif
icacio
nes
esti
lo d
e v
ida
Enf. CV establecida o Diabetes *(µalb)Algunos trastornos lipídicos genéticos
Inte
rven
ció
n
farm
aco
lóg
ica
Reducir riesgo CV 5-años a < 15%
Considerar valoración especialista
Tratamiento multifactorial intenso Urgente
Tratamiento farmacológico de todos los FR

Objetivos terapéuticos en el paciente Objetivos terapéuticos en el paciente
con alto riesgo vascularcon alto riesgo vascular-- GUIONGUION
• ¿Qué significa ‘alto riesgo vascular’?– Riesgo vascular: bajo / alto / muy alto
• Objetivos de control– HTA
– Dislipemia
• Otras medidas: antiagregación• Valoración global – tratamiento global

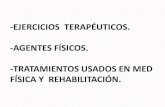
Prospective Studies Collaboration. Lancet. 2002;360:1903-1913
Usual Diastolic BP (mm Hg)Usual Systolic BP (mm Hg)
Isch
em
ic H
ea
rt D
isease M
ort
ali
ty
50-59
60-69
70-79
80-89Age at Risk (Y)
40-49
256
128
64
32
16
8
4
2
1
0120 140 160 180
50-59
60-69
70-79
80-89
Age at Risk (Y)
40-49
256
128
64
32
16
8
4
2
1
080 90 100 11070
Blood Pressure: Lower is BetterBlood Pressure: Lower is Better
Isch
em
ic H
ea
rt D
isease M
ort
ali
ty
Ischemic Heart Disease Mortality
BP=Blood pressure
a meta-analysis of individual data for one million adults in 61 prospective studies*

Bajar la presión ¿con qué fármacos?
Hypertens Res 2005; 28: 385–407
Antag Ca++
IECAARADoxazosina
GLOBAL

Bajar la presión ¿cuánto?Blood Pressure Reduction and Cardiovascular Prevention: An Update
Including the 2003–2004 Secondary Prevention Trials
Hypertens Res 2005; 28: 385–407

The J-curve phenomenon and the treatment of hypertension.
Farnett L, JAMA 1991;265:489–495.

CV
Mor
talit
yC
V E
vent
s
HOT Outcomes by Target Blood Pressure Group*
Hansson L, et al. Lancet. 1998;351:1755–1762.
≤≤≤≤ 85 ≤≤≤≤ 80
138.8
138.5 82.6
86.5

Defining the J-Curve in Hypertension and Coronary Artery Disease
INVEST Substudy Ann Intern Med. 2006;144:884-893.
nadir at 119/84 mm Hg

0
5
10
15
20
25
HOT Diabetic Subgroup Reduction in Cardiovascular Events
Hansson L, et al. Lancet. 1998;351:1755–1762.
Nu
mb
er
of
even
ts*
per
1000 p
ati
en
t-yrs
P=0.005
*Includes all myocardial infarction, all strokes, and all other cardiovascular deaths
# of patients
with diabetes
Achieved†
diastolic
BP
(mmHg)
Achieved†
systolic
BP
(mmHg)
Target
diastolic BP
(mmHg)
50185.2143.7≤≤≤≤ 90
50183.2141.4≤≤≤≤ 85
49981.1139.7≤≤≤≤ 80
†mean of all blood pressures for all study patients in BP subgroups from 6 months of follow-up to end of study

Impact of Blood Pressure Reduction on Mortality in Diabetes
66%
32%
Risk
reduction
0.016140/81144/85HOT
0.019144/82154/87UKPDS
P-valueIntensive
care
Conventional
careTrial
Turner RC, et al. BMJ. 1998;317:703-713. Hansson L, et al. Lancet. 1998;351:1755–1762.
Mortality endpoints are:UK Prospective Diabetes Study (UKPDS) – “diabetes related deaths”Hypertension Optimal Treatment (HOT) Study – “cardiovascular deaths” in diabetics

ACE Inhibitor Evidence: CAD, CVD, PVD or DMACE Inhibitor Evidence: CAD, CVD, PVD or DM
Days of Follow-Up
CV
dea
th, M
I, or
st
roke
(%
)
22% RRR, P<0.001
0.00
0.05
0.10
0.15
0.20
0 500 1000 1500
Placebo
Ramipril
HOPE Investigators. NEJM
2000;342:145-153
Heart Outcomes Prevention and Evaluation (HOPE) Study
ACE-I=Angiotensin converting enzyme inhibitors, DM=Diabetes mellitus, CV=Cardiovascular, HF=Heart failure, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction
9,297 patients with DM or vascular disease plus one additional CV risk factor, but without HF or known LVSD randomized to ramipril (10 mg) or placebo for 5 years
PA 139/79
139/77
136/76

Objetivos terapéuticos en el paciente Objetivos terapéuticos en el paciente
con alto riesgo vascularcon alto riesgo vascular-- GUIONGUION
• ¿Qué significa ‘alto riesgo vascular’?– Riesgo vascular: bajo / alto / muy alto
• Objetivos de control– HTA
– Dislipemia
• Otras medidas: antiagregación• Valoración global – tratamiento global

VA-HIT Veterans Affairs High-Density Lipoprotein Intervention Trial; LRC-CPPT, Lipids Research Clinics Coronary Primary Prevention Trial; A to Z, Aggrastat to Zocor; CDP, Coronary Drug Project; HHS, Health and Human Services; CARE, Cholesterol and Recurrent Events; POSCH, Program on the Surgical Control of the Hyperlipidemias; ASCOT-LLA, Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm; LIPS, Lescol Intervention Prevention Study; 4S, Scandinavian Simvastatin Survival Study.
Davidson: Circulation2005; 111:.2280-
EstatinasNo estatinas
Relacion entre % descenso del colesteroly enfermedad coronaria. Meta-análisis
0
-20
-40
-60
0 -5 -10 -15 -20 -25 -30
% ∆∆∆∆TC (CTL-TRT)
% de cambio de eventos CV
VA-HIT LRC-CPPT
ALLHAT-LLTCDP
A to Z
Post-CABG PROVE-IT
LIPIDHPS
WOSCOPS
AFCAPSPOSCH
CARD
LIPS
4S

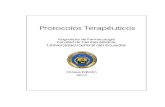
ASCOT-LLA IAM no mortal y muerte por EC
0
1
2
3
4
0,0 0,5 1,0 1,5 2,0 2,5 3,0 3,5
Años
Incidencia acumulada (%)
36 %
RR = 0,64 (0,50-0,83)
Placebo
Atorvastatina 10 mg
p=0,0005
. Lancet. 2003;361:1149-58
cLDL132 mg/dl
cLDL:126 mg/dl
cLDL:89 mg/dl
Población: 10305 hipertensos + 3 FR vascular (incluye ictus y PVP)

SIMVASTATIN: MAJOR VASCULAR EVENTin upper & lower thirds of baseline LDL
Average LDL cholesterol (mmol/l)
Statin-allocated
Placebo-allocated
% w
ith m
ajor
vas
cula
r ev
ents
UpperLDL third
20
25
30
LowerLDL third
1.5 2.0 2.5 3.0 3.5 4.0
15
Rate ratio & 95% CISTATIN better PLACEBO better
Lipid levelsat entry
LDL cholesterol
< 100
≥ 100 < 130
≥ 130
24% SE 3reduction(2P<0.00001)
ALL PATIENTS
0.4 0.6 0.8 1.0 1.2 1.4

Reduction in Death or Major Cardiovascular Event with Intensive Statin Therapy
Cannon CP et al. N Engl J Med 2004;350:1495-1504.

PROVE IT: Pravastatin or Atorvastatin Evaluation and Infection Therapy
Wiviott J Am Coll Cardiol 2005;46:1411– 6

¿todos los descensos del colesterol LDL son igual de beneficiosos?
ILLUSTRATE
N Engl J Med 2007;356:1304-16. RADIANCEN Engl J Med 2007;356:1620-1630

Relationship Between LDL-C and Event Rates in TNT and Other Statin Trials
30
25
20
15
10
5
0
0 70 90 110 130 150 170 190 210
LDL-C (mg/dL)
HPS
CARE
LIPIDLIPID
CARE
HPSEvent (%
)
Statin
Placebo
4S
4S
TNT (atorvastatin 80 mg/d)
TNT (atorvastatin 10 mg/d)
LaRosa JC et al. N Engl J Med. 2005;352:1425-1435.
?

>100 mg/dL (<100 mg/dL: consider drug
options)
≥≥≥≥100 mg/dL<100 mg/dL
if TG > 200 mg/dL,
non-HDL-C should be < 130 mg/dL
High risk:CHD or CHD risk equivalents (10-year risk >20%)
and
All patients
Initiate TLC
>100 mg/dL (<100 mg/dL: consider drug
options)
Consider Drug Therapy
<70 mg/dL,
non-HDL-C < 100 mg/dL
LDL-C and non-HDL-C Goal
Risk Category
Very high risk:
ACS or established CHD
plus: multiple major risk factors (especially diabetes) or severe and poorly controlled risk factors
Lipid Management Goals: NCEPLipid Management Goals: NCEP
ATP=Adult Treatment Panel, CHD=Coronary heart disease, LDL-C=Low-density lipoprotein cholesterol, TLC=Therapeutic lifestyle changes
AHA/ACC Guidelines for Secondary Prevention for Patients with Coronary and Other Atherosclerotic Vascular Disease: 2006 Update
Circulation 2006;113:2363-2372 and J Am Coll Cardiol 2006;47:2130-2139
¿Multiple vascular beds?
¿SUBCLINICAL?

One-year CV event rates as a function of the number of symptomatic disease locations
0,8 0,8 0,82,2
5,3
1,6 1,1 1,5
4,1
12,6
2,71,6
2,9
6,8
21,1
3,9
1,8
4,4
9,2
26,3
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
Pa
tie
nts
(%)
CV death Non-fatal MI Non-fatalstroke
CV death/MI/stroke
CV death/MI/stroke/hosp*
0
1
2
3
Patients with >3 risk factors but no symptoms are counted as 0, even in the presence of asymptomatic carotid plaque or reduced ankle brachial index
MI=myocardial infarction; *such as transient ischemic attack, unstable angina, worsening of peripheral arterial disease; adjusted for age and gender
• JAMA 2007;297(11): 1197-1206.
n=68.375

p=0.007
Estudio AIRVAG: nuevos eventos

32 eventos (12%) •9 cerebrovasculares•16 coronarios•6 periféricos•1 muerte súbita
0%
5%
10%
15%
20%
25%
CEREBRAL CORONARIO PERIFERICO
EVENTO INDICE
CEREBRAL CORONARIO PERIFERICO MUERTE CV GLOBAL
Estudio AIRVAG: nuevos eventos

32 eventos (12%) •9 cerebrovasculares•16 coronarios•6 periféricos•1 muerte súbita
0%
5%
10%
15%
20%
25%
CEREBRAL CORONARIO PERIFERICO
EVENTO INDICE
CEREBRAL CORONARIO PERIFERICO MUERTE CV GLOBAL
32 eventos (12%) •9 cerebrovasculares•16 coronarios•6 periféricos•1 muerte súbita
0%
5%
10%
15%
20%
25%
CEREBRAL CORONARIO PERIFERICO
EVENTO INDICE
CEREBRAL CORONARIO PERIFERICO MUERTE CV GLOBAL
NUEVOS EVENTOS ISQUÉMICOS
AIRVAGPERIFERICO VS OTROS
RR 2.5 IC 95% 1.07- 5.09 p <0.05
Adaptado de Guijarro Circulation 2004;110; S437 y
http://www.fesemi.org/grupos/riesgo_c/proyectos/index.php#frena 2006

Objetivos terapéuticos en el paciente Objetivos terapéuticos en el paciente
con alto riesgo vascularcon alto riesgo vascular-- GUIONGUION
• ¿Qué significa ‘alto riesgo vascular’?– Riesgo vascular: bajo / alto / muy alto
• Objetivos de control– HTA
– Dislipemia
• Otras medidas: antiagregación• Valoración global – tratamiento global

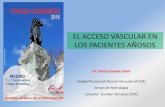
Tratamiento integral de FR
Si por cada intervención tenemos una reduccion de RR del 20%
(0.8 x 0.8 x 0.8 x 0.8) = 0.4 = RRR 60%
1
0,80
0,64
0,51
0,8
0,41 0,41
0
0,2
0,4
0,6
0,8
1
RE
DU
CC
ION
RIE
SG
O
BASAL ESTILO V HTA LIPIDOS AAS GLOBAL
FACTOR AISLADO TTO GLOBAL

Tratamiento integral de FR
• Modificaciones estilo de vidaDieta; ejercicio físico, tabaco
• Control de presión arterial• Control de dislipemia• Tratamiento antiagreganteSi por cada intervención tenemos una
reduccion de RR del 20%(0.8 x 0.8 x 0.8 x 0.8) = 0.4 =RRR 60%

Gaede P et al. N Engl J Med. 2003;348:383-393.
SBP (mm Hg)
DBP (mm Hg)
Follow-up (yr)
Steno-2: 160 DM2 patients + microalbuminuriaEffect of Therapies on Selected Risk Factors
0
5
6
7
8
9
10
11
0 1 2 3 4 5 6 7 8
0
110
120
130
140
150
160
170
0 1 2 3 4 5 6 7 8
0
65
70
75
80
85
90
95
0 1 2 3 4 5 6 7 8
HbA1c
(%)
Follow-up (yr)
Conventional therapy
Intensive therapy
Intensive therapy
Conventional therapy
Conventional therapy
Intensive therapy
0
50
100
150
200
250
300
350
0 1 2 3 4 5 6 7 8
0
50
75
100
125
150
175
200
0 1 2 3 4 5 6 7 8
0
50
100
150
200
250
300
350
0 1 2 3 4 5 6 7 8
TG (mg/dL)
LDL-C(mg/dL)
TC (mg/dL)
Conventional therapy
Intensive therapy
Intensive therapy
Conventional therapy
Intensive therapy
Conventional therapy
GLUCEMIA
P ARTERIAL
LIPIDOS

Gaede P et al. N Engl J Med. 2003;348:383-393.
No. at Risk
Conventional tx 80 72 70 63 59 50 44 41 13
Intensive tx 80 78 74 71 66 63 61 59 19
0 12 24 36 48 60 72 84 96
Follow-up (mo)
Conventional therapy
Intensive therapy
P = 0.00760
50
40
30
20
10
0
%
(log-rank test)
Steno-2: Primary Composite End Point (CV Events or Surgery for PAD)
HR 0.47 (0.24-0.73)

Proyecto MIRVAS Reducción de morbimortalidad cardiovascular mediante un control integral e intensivo de
factores de riesgo
M.A.Moreno Palanco
P. Ibáñez Sanz
Pizarro Portillo
L. Pérez Alonso
C. Ciria
C. Sánchez Luis
C. Suárez

MIRVAS Resultados: control de FRCV
Moreno Palanco MA, Ciria de Pablo C, Ibáñez Sanz P, Sánchez Luis C, Pizarro Portillo A, Suárez Fernández C. (2007).REDUCCIÓN DE MORBIMORTALIDAD CARDIOVASCULAR TRAS UN EPISODIO CARDIOVASCULAR AGUDO MEDIANTE UN TRATAMIENTO INTENSIVO DE FACTORES DE RIESGO. Manuscrito pendiente de publicación.

MIRVAS: Resultados: eventos cardiovasculares
0
5
10
15
20
25
30
SCA /IAM
Ictus /AIT
ICC MuerteCV
Muerteno CV
Intervención Control
RR 0.28 (IC 0.15-0.51)
RR 0.22 (IC 0.11-0.45)

Objetivo PRINCIPAL: REDUCCION DEL RIESGO VASCULAR
Es posible lograrlo > 50% con abordaje globalObjetivos más ambiciosos en pacientes de muy
alto riesgoObjetivos del tratamiento farmacológico• Hipotensor hasta 130/80mm Hg
– Incluidos pacientes con TA normal /alta
• Hipolipemiante hasta 70 mg/dl (LDL)– Incluidos pacientes con colesterol ‘normal’
• Tratamiento antiagregante a todo paciente de alto riesgo, salvo contraindicación