tumor oculto.pdf
9
Annals of Oncology 17 (Supplement 10): x168–x176, 2006 doi:10.1093/annonc/mdl255 Diagnostic and therapeutic management of carcinoma of unknown primary: radio-imaging investigations G. Jerusalem 1 , A. Rorive 1 , G. Ancion 2 , R. Hustinx 2 & G. Fillet 1 1 CHU Sart Tilman, Department of Medicine, Medical Oncology; 2 CHU Sart Tilman, Department of Medicine, Nuclear Medicine, Lie ` ge, Belgium introduction Metastatic cancer of unknown primary site (CUP) represents a heterogeneous group of tumors. Diagnosis is made by a biopsy of a metastatic lesion. CUP accounts for 2–3% of all malignancies. It is defined by the presence of metastatic disease for which a primary site is undetectable on presentation. Clinical presentations, histological appearances and natural histories vary widely explaining why it is impossible to define a common radio-diagnostic approach to all patients. Some specific clinical presentations will guide directly the diagnostic work-up. History, physical examination, histology of the metastases and tumor markers can sometimes suggest the primary or a specific clinico-pathological entity. Radio-imaging investigations are only part of an integrated approach aiming to find the primary and to define the best treatment for the patient. Consequently, although this review should focus on radio-imaging investigations, we have to discuss also several other issues directly related to this topic. We hope that the reader accept that our review on radio-imaging investigations reflects this integrated approach because discussing imaging techniques only outside of this clinical context does not allow to give any useful recommendation about the best use of imaging techniques in CUP. We will avoid reporting in detail the sensitivity and specificity of imaging techniques. The methodology used to evaluate the accuracy of imaging techniques is rather poor in many publications (retrospective evaluation, description of study population, description of gold standard etc.). The heterogeneit y of the study population and the defini tion of the gold standard (autopsy, other imaging techniques, follow-up etc.) have major impact on the results. The definition of CUP has changed over time. In the past, some researchers argued that the diagnosis of CUP could be made only if the primary tumor was not found at autopsy. Now we define that CUP represents a group of metastatic tumors for which no primary site can be detected following a thorough medical history, careful clinical examination and extensive diagnostic work-up. Consequentl y, the amount of work-up that has been done before accepti ng the diagnosis of CUP is an important factor. More importantly, only a few investigators have been interested in detailed studies of these patients. Past information suffers from many generalizations and is not representative of the entire patient population or specific subgroups of patients. Furthermore, the sensitivity of all imaging techniques has rapidly increased over time with technical improvements. On the other hand, pathological evaluation of the metastasis with recent immunohistochemical markers allows more frequently the identification of the primary. Consequently, results published 10 or 20 years ago give not much useful information on the impact of imaging techniques in patient management in 2006. Unfortunately, the false positive rate of some imaging procedures equalled or exceeded the true positive rate [1]. Extensive work-up with modern imaging technology such as computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET) has resulted in some improvements in diagnosis, showing sometimes the primary and allowing a better definition of the extent of the disease. For example, in retrospective studies from the Mayo Clinic and the University of Kansas, CT of the abdomen and/or chest was able to correctly identify the primary tumor in 35% and 32% of patients, respectively [2, 3]. However, the primary remains unknown in many patients, even on autopsy. Autopsies performed between 1984 and 1999 at the Mayo Clinic in 64 patients without primary tumor identified during the patient’ s lifeti me showed the primary site in 35 patients (55%). Common primary tumor locations were the lung, the pancreaticobiliary system and the upper and lower gastrointestinal tract [4]. The detection rate was lowest among the poorly differentiated carcinomas. clinical presentation Patients usually present symptoms related to the localization of the metastases and constitutional symptoms including anorexia, weight loss, weakness and fatigue. Physical examination frequently reveals peripheral adenopathy, pleural effusions, ascites and hepatomegaly. Common sites of metastatic spread are the lung, the liver and the bones. Unfortunately, the overall survival for this patient population remains poor with a median survival time of 11 months and only an 11% 5-year survival rate [5]. Male gender, the presence of liver metastases and an increasing number of organs involved were all independent predictors for poor outcome [6]. Patient’s performance status is also a critical prognostic variable. Searching for the primary site in patients with rapidly progressing disease and poor performance status is not indicated when best supportive care is the only treatment option. ª 2006 European Society for Medical Oncology b y g u e s t o n J a n u a r y 1 8 , 2 0 1 4 h t t p : / / a n n o n c . o f o r d j o u r n a l s . o r g / D o w n l o a d e d f r o
-
Upload
lilian-sousa -
Category
Documents
-
view
221 -
download
0
Transcript of tumor oculto.pdf

8/12/2019 tumor oculto.pdf
http://slidepdf.com/reader/full/tumor-ocultopdf 1/9
Annals of Oncology 17 (Supplement 10): x168–x176, 2006
doi:10.1093/annonc/mdl255
Diagnostic and therapeutic management of carcinoma
of unknown primary: radio-imaging investigations
G. Jerusalem1, A. Rorive1, G. Ancion2, R. Hustinx2 & G. Fillet1
1CHU Sart Tilman, Department of Medicine, Medical Oncology; 2CHU Sart Tilman, Department of Medicine, Nuclear Medicine, Lie ge, Belgium
introduction
Metastatic cancer of unknown primary site (CUP) representsa heterogeneous group of tumors. Diagnosis is made by a biopsy of a metastatic lesion. CUP accounts for 2–3% of allmalignancies. It is defined by the presence of metastatic diseasefor which a primary site is undetectable on presentation. Clinicalpresentations, histological appearances and natural histories
vary widely explaining why it is impossible to define a commonradio-diagnostic approach to all patients. Some specific clinicalpresentations will guide directly the diagnostic work-up.History, physical examination, histology of the metastases andtumor markers can sometimes suggest the primary or a specificclinico-pathological entity. Radio-imaging investigations areonly part of an integrated approach aiming to find the primary and to define the best treatment for the patient. Consequently,although this review should focus on radio-imaginginvestigations, we have to discuss also several other issuesdirectly related to this topic. We hope that the reader accept thatour review on radio-imaging investigations reflects thisintegrated approach because discussing imaging techniques only
outside of this clinical context does not allow to give any usefulrecommendation about the best use of imaging techniques inCUP. We will avoid reporting in detail the sensitivity andspecificity of imaging techniques. The methodology used toevaluate the accuracy of imaging techniques is rather poor inmany publications (retrospective evaluation, description of study population, description of gold standard etc.). Theheterogeneity of the study population and the definition of thegold standard (autopsy, other imaging techniques, follow-upetc.) have major impact on the results. The definition of CUPhas changed over time. In the past, some researchers arguedthat the diagnosis of CUP could be made only if the primary tumor was not found at autopsy. Now we define that CUP
represents a group of metastatic tumors for which no primary site can be detected following a thorough medical history,careful clinical examination and extensive diagnostic work-up.Consequently, the amount of work-up that has been donebefore accepting the diagnosis of CUP is an important factor.More importantly, only a few investigators have been interestedin detailed studies of these patients. Past information suffersfrom many generalizations and is not representative of the entirepatient population or specific subgroups of patients.Furthermore, the sensitivity of all imaging techniques hasrapidly increased over time with technical improvements. On
the other hand, pathological evaluation of the metastasis withrecent immunohistochemical markers allows more frequently the identification of the primary. Consequently, resultspublished 10 or 20 years ago give not much usefulinformation on the impact of imaging techniques in patientmanagement in 2006.
Unfortunately, the false positive rate of some imaging
procedures equalled or exceeded the true positive rate [1].Extensive work-up with modern imaging technology such ascomputed tomography (CT), magnetic resonance imaging(MRI) and positron emission tomography (PET) has resultedin some improvements in diagnosis, showing sometimes theprimary and allowing a better definition of the extent of thedisease. For example, in retrospective studies from the MayoClinic and the University of Kansas, CT of the abdomenand/or chest was able to correctly identify the primary tumorin 35% and 32% of patients, respectively [2, 3]. However, theprimary remains unknown in many patients, even on autopsy.Autopsies performed between 1984 and 1999 at the MayoClinic in 64 patients without primary tumor identified duringthe patient’s lifetime showed the primary site in 35 patients
(55%). Common primary tumor locations were the lung, thepancreaticobiliary system and the upper and lowergastrointestinal tract [4]. The detection rate was lowestamong the poorly differentiated carcinomas.
clinical presentation
Patients usually present symptoms related to the localizationof the metastases and constitutional symptoms includinganorexia, weight loss, weakness and fatigue. Physicalexamination frequently reveals peripheral adenopathy, pleuraleffusions, ascites and hepatomegaly. Common sites of
metastatic spread are the lung, the liver and the bones.Unfortunately, the overall survival for this patient populationremains poor with a median survival time of 11 months andonly an 11% 5-year survival rate [5]. Male gender, thepresence of liver metastases and an increasing number of organs involved were all independent predictors for pooroutcome [6]. Patient’s performance status is also a criticalprognostic variable. Searching for the primary site in patientswith rapidly progressing disease and poor performance statusis not indicated when best supportive care is the only treatment option.
ª 2006 European Society for Medical Oncology

8/12/2019 tumor oculto.pdf
http://slidepdf.com/reader/full/tumor-ocultopdf 2/9
biology of CUP
The primary site may either remain microscopic and escapeclinical detection or disappear after seeding the metastases[7–9]. If only one tumor site is identified, it may also representan unusual primary tumor mimicking metastatic disease.Advances in the understanding of the basic biology of CUPmay have a direct impact on clinical care [10]. One can regardCUP as common metastases of an unrecognized primary. Inthis case diagnostic evaluation should concentrate on theidentification of the primary origin of the tumor. Itsidentification would lead to a disease-directed treatment anda better defined prognosis. Consequently, research should focuson developing tools for better detection and/or classificationof primary tumors such as MRI or PET. However, some studieshave shown that the prognosis is not better when the primary tumor has been identified [11, 12]. In contrast, when we takeinto account the concept of a specific biology of CUP, the searchfor a primary is of minor importance and diagnostic evaluationshould focus on the detection of specific biochemical andmolecular targets. In fact, CUP are characterized by an early dissemination and an unpredictability of metastatic pattern
and aggressiveness [13]. CUP primaries, when found, tend tospread in a manner different from that of known primaries of the same organ. Lung cancer presenting as known primary involves the bones in 30–50%, while presenting as CUP theosseous involvement is 5%. Pancreatic cancer presenting as CUPhas as 4-fold higher incidence of affecting bones, whereasprostate cancer presenting as CUP has a 3-fold less incidenceof affecting bones compared with known primaries [14].
searching for the primary tumor site
The costs, in terms of time and money, as well as the final benefitin the outcome of the patients have to be taken into
consideration. In oncology, predictions about prognosis anddecisions about therapy are mainly based on knowledge of the primary site. However, a critical review of the literaturedoes not indicate the value of an exhaustive and expensivesearch for the primary tumor site. It is only recommended toidentify treatable and in some cases potentially curable subsetsof patients with CUP. In the past, approximately 5–10% of patients with CUP benefited from a specific treatment approach.However, new drugs are now available and palliativechemotherapy is recommended for most solid tumors, evenin advanced stage. More patients benefit now from disease-directed treatments. Furthermore, even when no beneficialtumor-specific therapeutic option exists, patients and their
physician often desire to know the source and type of neoplasm.The absence of a primary generates anxiety and results infeelings that the evaluation has been inadequate. There is alsoan unproven feeling that the prognosis can be improved whenthe primary is identified [12]. With the increasing availability of new diagnostic modalities and better palliative treatmentoptions, physicians must determine how much diagnosticworkup is sufficient before accepting a diagnosis of CUP [9].It is important to define a practical guideline for the diagnosticwork-up of patients suffering from CUP but, unfortunately,not anyone has been prospectively evaluated.
A careful pathologic evaluation plays an increasing role insearching for the primary tumor site. Immunohistochemicaltechniques allow the physician to clarify tumor subtypes in upto 40% of patients [15]. Cytokeratins 7 and 20 and thyroidtranscription factor are some of the usefulimmunohistochemical markers in adenocarcinoma. Potentially treatable or curable tumors (i.e. breast cancer, prostate cancer,lymphomas, germ cell tumors, Ewing’s sarcoma) have to be
ruled-out by specialized modern pathologic techniques.Molecular identification of tumor origin is a successful new approach [8, 16]. The use of gene expression data generatedfrom micro-array technology may also help to identify theprimary site in patients with CUP [17, 18].
All patients should have an evaluation including a completehistory, physical examination and basic blood and biochemistry survey. It is very important to point out that an appropriateevaluation begins with a thorough history [19]. A review of the past medical history should include questions regardingprior surgeries for ‘benign’ skin lesions and moles becausefurther investigation may reveal these to be the source of thecurrent metastatic disease. Family history of breast, ovarian or
colorectal cancers may suggest the presence of an underlyingheritable cancer syndrome and an increased risk for specificmalignancies. Also a social history focused on prior exposures(such as tobacco or asbestos) and risk factors for HIV infectionmay suggest an underlying risk for certain tumors. Basiclaboratory tests will not identify the primary tumor but may provide information regarding potential unrecognized sites of metastatic disease. They offer also an assessment of organfunction that can be used to predict the patient’s ability totolerate chemotherapy.
If a specific clinicopathological entity is not suspected, allpatients should have a standard diagnostic work-up includingat least urinalysis, fecal occult blood test, chest X-ray and CTof the abdomen and pelvis [20] (Table 1). Assessment of serum
alpha-foetoprotein (AFP), human chorionic gonadotropin(HCG) and prostate-specific antigen (PSA) is suggested inmale patients to exclude potentially curable extragonadalgerm cell tumor or prostate cancer amenable to hormonetreatment. The use of tumor markers except AFP, HCGand PSA in this special circumstance is discouraged because
Table 1. Diagnostic work-up in CUP
First step:
• Identification of risk factors
•
Clinical history • Physical examination
• Pathologic evaluation
Second step:
• A specific clinicopathological entity is suspected or the
predominant site of disease will guide radiodiagnostic
procedures
• All the other patients should have a standard evaluation
including at least urinalysis, fecal occult blood test,
chest-X-ray and CT of the abdomen and pelvis. A CT
of the thorax and a PET scan may also be useful
Annals of Oncology
Volume 17 | Supplement 10 | September 2006 doi:10.1093/annonc/mdl255 | x
169

8/12/2019 tumor oculto.pdf
http://slidepdf.com/reader/full/tumor-ocultopdf 3/9
of a low specificity [21]. Furthermore, no association betweena particular marker elevation and response to therapy orsurvival has been observed.
Further evaluation and endoscopies should be sign- orsymptom-guided. The diagnostic work-up in specificclinicopathological entities is discussed later in this review (Tables 2–3).
CT of the chest
Although CT of the chest is not part of the standard evaluation[20], one can discuss its role in CUP. Chest X-ray is able todifferentiate between primary and secondary malignancies inonly one third of the patients [22, 23]. CT of the chest canprovide several useful pieces of information [2, 3]. Involvementof the mediastinum is best evaluated by CT. It can alsodetermine the extent of the metastatic disease and it may provide guidance in selecting the optimal site for biopsy.Furthermore, lung cancer is one of the most commonidentifiable primary tumors that present with CUP.Consequently, a CT thorax is usually performed.
positron emission tomography
PET using 18F-fluorodeoxyglucose (18F-FDG) merits alsofurther evaluation [24]. 18F-FDG PET allows whole-body screening. 18F-FDG PET can correctly identify a primary siteof disease in some patients. In particular, it may be helpful inlocalizing head and neck tumors in patients with a cervicallymphadenopathy from an unknown primary [25–32]. Some
investigators have observed that the false positive rate of PETin this setting may be extremely high [33]. Even thoughwhole-body 18F-FDG PET has several advantages overconventional imaging techniques, there are some limitations.18F-FDG is excreted by the kidneys and the ability to detecttumors in the urinary tract may be limited. Physiologic uptakein the digestive tract may mimic a primary tumor leading tounnecessary gastrointestinal endoscopies. 18F-FDG uptake may
be low in well-differentiated slowly growing tumors suchas prostate cancer or neuroendocrine tumors. 18F-FDG PETis also limited by spatial resolution for the detection of very small primary tumors. The likelihood of finding a primary tumor in patients who already underwent extensive work-upwith CT, MRI, US and endoscopy seems low. Of course, thesensitivity of PET depends on the number of other imagingprocedures done in addition to standard evaluations, definingCUP. Although most investigators have performed PET aftera thorough negative diagnostic work-up, its high sensitivity could indicate that it should be used as a first-line modality in order to guide the diagnostic procedures (Figures 1–4).From the patients point of view, a one-day non-invasive
procedure is usually preferable to repeated visits to thehospital, especially when the single procedure is more effective,as shown in two recent studies [34, 35]. Both retrospectivestudies included only a few patients with cervical lymph nodemetastases but a high number of patients with brain metastases.They reported an advantage of PET over CT in particular inthe detection of lung cancer and pancreaticobiliary systemtumors. However, the performance of PET can be overestimatedcompared to conventional imaging methods because PET
Table 2. Diagnostic work-up in a specific clinicopathological entity:
Peripheral lymph nodes
Upper or mid-cervical lymph node involvement by squamous cell
carcinoma, in particular in middle-aged or elderly patients who
frequently have abused tobacco or alcohol: head and neck tumor?
• CT of the head and neck
• 18F-FDG PET (?)
• Panendoscopy
Lower cervical or supraclavicular lymph node involvement, in
particular in middle-aged or elderly patients who frequently
abused tobacco: lung tumor?
• CT of the thorax
• Panendoscopy if the CT of the thorax is negative
Axillary lymph node involvement by adenocarcinoma in a woman:
breast cancer?• Mammography
• Ultrasound of the breast
• MRI of the breast
Inguinal lymph nodes involved by squamous cell carcinoma:
primary in the perineal region?
• Examination of the vulva, vagina and cervix in women, of the
penis and scrotum in men
• Colposcopy in women
• Digital rectal examination
• Anoscopy
Table 3. Diagnostic work-up in a specific clinicopathological
entity: Other presentations
Young men with poorly differentiated carcinoma predominantly
localized in the mediastinum and retroperitoneum: testicular cancer
or extragonadal germ-cell tumor syndrome?
• Serum HCG and AFP tumor marker level
• Scrotal ultrasonography
• CT of the thorax
• CT of the abdomen and pelvis
• CT of the brain
Metastases of an adenocarcinoma or a poorly differentiated
carcinoma only in the liver: colon cancer?
• Colonoscopy
Pleural effusions: well or moderately differentiated adenocarcinoma
• CT of the thorax: lung cancer?
• Mammography in woman: breast cancer?
• Gynecological examination, ultrasound of the pelvis,
CT of abdomen and pelvis
• Ovarian cancer or primary peritoneal carcinomatosis?
Patient with an isolated metastasis before considering
local treatment
• CT of the thorax
• CT of the abdomen and pelvis
• Bone scintigraphy
• 18F-FDG PET (?)
Annals of Oncology
x
170 | Jerusalem et al. Volume 17 | Supplement 10 | September 2006

8/12/2019 tumor oculto.pdf
http://slidepdf.com/reader/full/tumor-ocultopdf 4/9
scan were analyzed by a team of experienced physicians whileconventional imaging methods were performed in differentlocations and conditions, not standardized and their resultswere not analyzed by the same radiologists. PET was alsosuperior to mammography in the detection of breast cancer.False positive findings were observed in the digestive tract andin the head and neck region [34]. No conclusion can bedrawn from these retrospective studies about the
cost-effectiveness of using PET as a first-line imagingprocedure in patients with CUP.
The potential role of PET is not only to identify an occultprimary. It can direct a biopsy of other metastatic lesions whena larger biopsy is needed for further pathologic evaluationavoiding sometimes a more invasive procedure. PET can alsoimprove the staging of the disease in showing more advanceddisease than the conventional investigations. Sometimesa specific histologic pattern with a particular anatomicdistribution identifies a clinical presentation with still a curativeapproach. For example, an isolated lymph node metastasis of melanoma without an obvious primary can be cured by lymphadenectomy. In patients with metastases evident only in
one site based on conventional imaging technique, PET may indicate who is not candidate for a local treatment by detectingfurther unknown metastatic sites.
the radio-diagnostic evaluation of
different clinicopathological entities
Optimal pathologic evaluation is critical because it may allow identification of the primary site, of specific cancer types (e.g.,lymphomas) and of patients subtypes with specific treatmentimplications (e.g., poorly differentiated neuroendocrinetumors). Patients should be evaluated based on one of fivehistologies: undifferentiated neoplasm, well or moderately differentiated adenocarcinoma, squamous cell carcinoma,
poorly differentiated carcinoma/adenocarcinoma andcarcinoma with neuroendocrine differentiation. Thelocalization of the metastasis and other clinical informationwill guide the radiodiagnostic work-up in each of thesehistologies [36].
poorly or undifferentiated neoplasm of
unknown primary
This is a group of patients where the pathologist is unableto distinguish a general category of neoplasm (carcinoma,lymphoma, melanoma, sarcoma, neuroendocrine tumors,germ cell tumor, melanoma). It accounts for less than 5% of all CUP. Specialized modern pathologic techniques can now aid in tumor characterization. This is extremely important
because many patients have responsive tumors. Furtherpathologic evaluation revealed in older studies that 34–66% of poorly differentiated or anaplastic neoplasms are lymphomas[37]. Most of the remaining tumors were poorly differentiatedcarcinoma; other tumors, including melanoma and sarcoma,accounted for less than 15% of all patients. The most commoncause of a nonspecific light microscopic diagnosis is aninadequate biopsy specimen. Radiodiagnostic procedures may allow identification of sites where a larger biopsy can beobtained more easily. Immunohistochemistry and otherspecialized modern pathologic techniques should be routinely applied in poorly differentiated cases to exclude chemosensitiveand potentially curable tumors (i.e. lymphoma and germ cell
tumors). Close cooperation between the pathologist andclinician optimizes the chances of making a specific diagnosisin patients with CUP [37]. All patients should have a standarddiagnostic work-up at baseline including CT of the thorax and CT of the abdomen and pelvis. The role of imagingtechniques is mainly staging and response evaluation in thisgroup of patients.
well or moderately differentiated
adenocarcinoma of unknown primary
About 50% of all patients with CUP fall in this category. Mostpatients are elderly and have multiple sites of metastases
including liver, lungs and bones. The primary site is only identified in 15–20% of patients during life in older studies priorto the availability of CT [38]. The most common primary identified at autopsy were lung and pancreas (about 40% of cases) followed by other gastrointestinal sites (stomach, colon
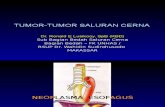
Figure 1. 45-year old woman with left cervical lymph nodes. PET shows that the primary is localized in the nasopharynx (Figure 1A:CT, Figure 1B:PET,
Figure 1C:PET/CT). No distant metastases are observed (images of whole-body PET not shown). The biopsy of the primary revealed an undifferentiated
carcinoma.
Annals of Oncology
Volume 17 | Supplement 10 | September 2006 doi:10.1093/annonc/mdl255 | x
171

8/12/2019 tumor oculto.pdf
http://slidepdf.com/reader/full/tumor-ocultopdf 5/9

8/12/2019 tumor oculto.pdf
http://slidepdf.com/reader/full/tumor-ocultopdf 6/9
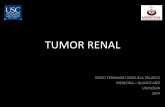
Figure 4. 49-year old woman with metastases of an undifferentiated carcinoma infiltrating the lung. PET shows multiple lung lesions (Figure 4A, 4D:CT,
Figure 4B, 4E:PET, Figure 4C, 4F:PET/CT).Whole-body PET (Figure 4G) indicates no extrathoracic lesions. Physiological radiotracer uptake is seen in the
muscles, in the digestive tract and in the bladder. Radio-imaging investigations are in favour of metastases from a primary localized in the lung.
Annals of Oncology
Volume 17 | Supplement 10 | September 2006 doi:10.1093/annonc/mdl255 | x
173

8/12/2019 tumor oculto.pdf
http://slidepdf.com/reader/full/tumor-ocultopdf 7/9
This syndrome is now called primary peritoneal carcinomatosis.The clinical features are similar to ovarian cancer or abdominalcarcinomatosis. It can be seen in women who previously hadtheir ovaries removed, in particular in patients harboringBRCA1 mutations.
prostate cancer
In men with skeletal metastases, a metastatic prostate
carcinoma should be suspected in particular when the patientpresents an adenocarcinoma involving predominantly thebones, when the metastases are blastic or when the serum PSAor acid phosphatase level is increased. Some men have moreunusual radiological presentations and the diagnosis is only suggested by tumor staining for PSA [42, 43]. Usually they have metastases in the lung, in mediastinal lymph nodes orin upper abdominal lymph nodes but they do not haveinvolvement of pelvic lymph nodes or of the bones.
colon cancer
Colon cancer has to be excluded in patients presenting only liver metastases. A colonoscopy should be done even if fecal
occult blood tests are negative.
only one identified metastasis
Local treatment should be administered to the unusual patientwho presents with tumor at only one identifiable site. A PETmay be useful to exclude more extensive metastatic spread.Some of these patients have prolonged survival after localtherapy particularly those who present with a sole metastasisin an isolated peripheral lymph node group.
Sometimes the predominant site of disease will guide furtherdiagnostic work-up.
pleural effusion
In the case of pleural effusion, a CT of the thorax is indicatedto search for a primary lung cancer. A bronchoscopy will bedone if the CT of the thorax shows abnormalities suggestiveto be the primary tumor. In a woman, breast cancer, ovariancancer or primary peritoneal carcinomatosis should alsobe excluded.
lung metastases
Most patients with multiple lung lesions suffer from lungcancer. A CT of the thorax and a bronchoscopy should bedone but a CT of the abdomen and pelvis should also beperformed in order to exclude a primary outside of the lung.
bone metastases
A CT of the thorax and of the abdomen and pelvis will identify the primary in most cases. In men, in particular when metastasesare osteoblastic, prostate cancer is frequently the origin (seeabove). Digital rectal examination and dosage of PSA serumlevel should be done. In a woman osteoblastic metastases aremost times related to a primary breast cancer. Clinicalexamination of breast, a mammography, an ultrasound andan IRM of the breast should be performed. A bone scintigraphy will guide further imaging studies (radiography, CT, IRM) of
the bones. Prophylactic interventions and palliative systemictreatments are now available decreasing the morbidity associated with bone metastases.
CNS metastases
A CT of the thorax is indicated because an asymptomaticprimary lung tumor is frequently identified.
squamous cell carcinoma
This histology represents only 15% of unknown primary carcinoma. Appropriate evaluation of these patients isessential because effective treatment is available for certainclinical syndromes.
cervical and supraclavicular lymph node
metastases
Most patients are middle-aged or elderly and frequently haveabused tobacco or alcohol. Upper or mid-cervical lymph nodesare usually related to a primary tumor in the head and neck region. All patients should undergo a thorough search for
a primary site in the head and neck region, including a CT of the head and neck and panendoscopy (laryngoscopy,bronchoscopy and esophagoscopy). Routine blind biopsiesof common potential primary sites, including the base of thetongue, piriform sinus and tonsils and of any suspiciousmucosal area are performed. Ipsilateral or bilateraltonsillectomy are often performed because they will be foundto harbor an occult primary in 10–25% of patients [30].18F-FDG PET may be useful in identifying a primary tumorin the head and neck area [29, 31]. Some studies indicate that18F-FDG PET identifies an occult primary site in the head andneck area in approximately one-third of patients [26, 28, 30, 32].However, the real sensitivity of PET in an unselected patient
population after an appropriate standard evaluation includingear-nose-throat endoscopy remains unknown. 18F-FDG PEThas also some limitations. 18F-FDG uptake can be variable inthe tonsils, adenoid, salivary glands and in muscles of thehead and neck which can render image analysis difficult.False-positive and false-negative findings can result underthese circumstances [24, 34]. When no primary site isidentified and lymph node resection alone is used as the primary treatment modality, a primary tumor in the head and neck subsequently becomes obvious in 20–40% of patients [37].
Lower cervical or supraclavicular lymph node involvementis frequently related to a primary lung cancer. A CT thorax and bronchoscopy should be performed. When the CT of the thorax is negative, a primary tumor of the oesophagusor of the head and neck region should be excluded by a panendoscopy.
inguinal lymph nodes
Almost all patients have a primary tumor identifiable in theperineal region. Identification of a primary site in the vulva,vagina, cervix and anus is important because even after spreadto regional nodes a curative approach remains possible.A careful examination of the vulva, vagina and cervix inwomen or the penis and scrotum in men is indicated.
Annals of Oncology
x
174 | Jerusalem et al. Volume 17 | Supplement 10 | September 2006

8/12/2019 tumor oculto.pdf
http://slidepdf.com/reader/full/tumor-ocultopdf 8/9
A colposcopy should always be performed in women. Digitalrectal examination and anoscopy is also indicated to excludea primary in the anorectal area.
bone metastases
A CT of the thorax should be performed. If the CT isnegative, a panendoscopy should be done. A bone scintigraphy will guide further imaging studies (radiography, CT, IRM) of
the bones. Prophylactic interventions and palliative systemictreatments are now available decreasing the morbidity associated with bone metastases.
other sites
Most times these patients have an occult primary lung cancer.A CT of the chest and a bronchoscopy should be performed.Other rare presentations include primary tumors from thehead and neck, esophagus, anus and skin.
poorly differentiated carcinoma
About 30% of all patients with an unknown primary havepoorly differentiated carcinoma or poorly differentiatedadenocarcinoma. Clinical and pathological evaluation is criticalbecause some patients can be cured by cisplatin-basedchemotherapy. Tumor location is the most useful clinicalfeature in predicting response to therapy and survival [44].Patients have a rapid progression of symptoms and objectiveevidence of rapid tumor growth. Lymph nodes in themediastinum and retroperitoneum are more frequently among the predominant sites of disease compared with welldifferentiated adenocarcinoma. The median age of this group of patients is also younger although a wide age range has beenobserved. CT of the chest and abdomen should be performed inall patients because of the frequency of mediastinal and
retroperitoneal involvement. Significant increase of serumlevels of HCG and alphafetoprotein suggest the diagnosisof germ cell tumor. A scrotal ultrasonography should beperformed in particular in young men.
Most patients with multiple lung lesions suffer froma primary lung cancer. A CT of the abdomen and pelvis isperformed to search for a primary in this region. It is alsoimportant to exclude testicular cancer in a young man(HCG and AFP serum level, scrotal ultrasound) or unsuspectedgestational choriocarcinoma in a young woman (history of recent pregnancy, spontaneous abortion or missed menstrualperiods, HCG serum level).
In the case of pleural effusion, a biopsy allows to exclude
mesothelioma. A primary lung cancer can be detected by a CT of the thorax. In women, it is also indicated to performa mammography (breast cancer?), a gynecological examinationand an ultrasound of the pelvis (ovarian cancer?).
The most frequent causes of malignant peritoneal effusionshave yet been discussed in the section about well and moderately differentiated adenocarcinoma.
The possibility of an unusual primary tumor mimickingmetastatic disease should be considered when only one siteof neoplasm is identified. Merkel cell tumors, skin adnexaltumors or sarcomas can have this kind of presentation.
Patients with undifferentiated neuroendocrine tumors withvery limited involvement at only one site treated with only local modalities can have a good long term outcome [37].Radio-imaging studies (CT of the thorax, CT of the abdomenand pelvis, bone scintigraphy) are indicated to exclude thepresence of other tumor sites.
The diagnostic work-up for patients suffering from poorly differentiated adenocarcinoma is the same than for patients
with well or moderately differentiated adenocarcinoma.
carcinomas with neuroendocrine
differentiation
An octreoscan (well differentiated tumors) or a PET-scan(poorly differentiated tumors) may be useful to search for theprimary but further prospective evaluations of the impact onpatient management and outcome are needed.
conclusions and perspectives
Unfortunately, no practical guideline for the diagnosticwork-up of patients suffering from CUP has been prospectively evaluated. A reasonable clinical and pathologic evaluation of these patients and their tumors is indicated. The methodology used for the evaluation of radio-imaging techniques is ratherpoor and results from older studies give little useful informationon the accuracy of modern radiological equipments.Furthermore, the study population has rapidly changed becauseof improvements in pathology allowing more frequently theidentification of the primary tumor site. With all theselimitations in mind, we conclude after a critical review of theliterature, that an integrated approach taking into accounthistory, clinical examination, histology and sometimes tumormarkers is indicated when searching for a primary tumor site.
Sometimes specific clinical presentations can be identified andwill guide directly the diagnostic work-up. If a specificclinicopathological entity is not suspected, all patients shouldhave a standard diagnostic work-up including at least urinalysis,fecal occult blood test, chest X-ray and CT of the abdomenand pelvis. Although CT of the thorax is not part of the standardevaluation, it is usually performed. Imaging techniques arenot only useful for searching the primary tumor site but canalso sometimes guide a biopsy. They are also performed todefine extend of disease and to monitor response totreatment. In the future, a whole-body PET/CT may be usedas first-line imaging procedure guiding further radio-diagnosticevaluation. Prospective studies with an improved methodology
(definition of study population, definition of gold standard,interpretation of new imaging techniques and reference studiesboth by experienced investigators, etc.) are needed to betterevaluate the role and cost-effectiveness of imaging techniquesin CUP. A prospective validation of practical guidelines isalso needed.
references
1. Greco FA, Hainsworth JD. Cancer of unknown primary site. In DeVita VT Jr,
Hellman S, Rosenberg SA (eds) : Cancer: principles and practice of
Annals of Oncology
Volume 17 | Supplement 10 | September 2006 doi:10.1093/annonc/mdl255 | x
175

8/12/2019 tumor oculto.pdf
http://slidepdf.com/reader/full/tumor-ocultopdf 9/9
oncology (6th Edn). Philadelphia, PA: Lippincott Williams & Wilkins 2001;
pp 2537–2560.
2. Karsell PR, Sheedy PF, O’Connell MJ. Computed tomography in search of cancer
of unknown origin. JAMA 1982; 248: 340–343.
3. McMillan JH, Levine E, Stephens RH. Computed tomography in the evaluation
of metastatic adenocarcinoma from an unknown primary site. A retrospective
study. Radiology 1982; 143: 143–146.
4. Blaszyk H, Hartmann A, Bjornsson J. Cancer of unknown primary:
clinicopathologic correlations. APMIS 2003; 111: 1089–1094.
5. Hess KR, Abbruzzese MC, Lenzi R et al. Classification and regression treeanalysis of 1000 consecutive patients with unknown primary carcinoma. Clin
Cancer Res 1999; 5: 3403–3410.
6. Abbruzzese JL, Abbruzzese MC, Hess KR et al. Unknown primary carcinoma:
natural history and prognostic factors in 657 consecutive patients. J Clin Oncol
1994; 12: 1272–1280.
7. Jordan WE, III, Shildt RA. Adenocarcinoma of unknown primary site. The Brooke
Army Medical Center experience. Cancer 1985; 55: 857–860.
8. Califano J, Westra WH, Koch W et al. Unknown primary head and neck
squamous cell carcinoma: molecular identification of the site of origin. J Natl
Cancer Inst 1999; 91: 599–604.
9. Varadhachary GR, Abbruzzese JL, Lenzi R. Diagnostic strategies for unknown
primary cancer. Cancer 2004; 100: 1776–1785.
10. van de Wouw AJ, Jansen RL, Speel EJ et al. The unknown biology of the
unknown primary tumour: a literature review. Ann Oncol 2003; 14: 191–196.
11. Stewart JF, Tattersall MH, Woods RL et al. Unknown primary adenocarcinoma:
incidence of overinvestigation and natural history. Br Med J 1979; 1:
1530–1533.
12. Abbruzzese JL, Abbruzzese MC, Lenzi R et al. Analysis of a diagnostic strategy
for patients with suspected tumors of unknown origin. J Clin Oncol 1995; 13:
2094–2103.
13. Pavlidis N, Briasoulis E, Hainsworth J et al. Diagnostic and therapeutic
management of cancer of an unknown primary. Eur J Cancer 2003; 39:
1990–2005.
14. Nystrom JS, Weiner JM, Heffelfinger-Juttner J et al. Metastatic and histologic
presentations in unknown primary cancer. Semin Oncol 1977; 4: 53–58.
15. Hainsworth JD, Greco FA. Management of patients with cancer of unknown
primary site. Oncology (Williston Park) 2000; 14: 563–574.
16. Summersgill B, Goker H, Osin P et al. Establishing germ cell origin of
undifferentiated tumors by identifying gain of 12p material using comparative
genomic hybridization analysis of paraffin-embedded samples. Diagn Mol Pathol
1998; 7: 260–266.
17. Giordano TJ, Shedden KA, Schwartz DR et al. Organ-specific molecular
classification of primary lung, colon, and ovarian adenocarcinomas using gene
expression profiles. Am J Pathol 2001; 159: 1231–1238.
18. Su AI, Welsh JB, Sapinoso LM et al. Molecular classification of human
carcinomas by use of gene expression signatures. Cancer Res 2001; 61:
7388–7393.
19. Dowell JE. Cancer from an unknown primary site. Am J Med Sci 2003; 326:
35–46.
20. ESMO Minimum Clinical Recommendations for diagnosis, treatment and
follow-up of cancers of unknown primary site (CUP). Ann Oncol 2005; 16:
i75–i76.
21. Pavlidis N, Kalef-Ezra J, Briassoulis E et al. Evaluation of six tumor markers
in patients with carcinoma of unknown primary. Med Pediatr Oncol 1994; 22:162–167.
22 . Nystrom JS, Weiner JM, Wolf RM et al. Identifying the primary site in
metastatic cancer of unknown origin. Inadequacy of roentgenographic
procedures. JAMA 1979; 241: 381–383.
23. Le Chevalier T, Cvitkovic E, Caille P et al. Early metastatic cancer of unknown
primary origin at presentation. A clinical study of 302 consecutive autopsied
patients. Arch Intern Med 1988; 148: 2035–2039.
24. Delgado-Bolton RC, Fernandez-Perez C, Gonzalez-Mate A et al. Meta-analysis
of the performance of 18F-FDG PET in primary tumor detection in unknown
primary tumors. J Nucl Med 2003; 44: 1301–1314.
25. AAssar OS, Fischbein NJ, Caputo GR et al. Metastatic head and neck cancer:
role and usefulness of FDG PET in locating occult primary tumors. Radiology
1999; 210: 177–181.
26. Lassen U, Daugaard G, Eigtved A et al. 18F-FDG whole body positron emission
tomography (PET) in patients with unknown primary tumours (UPT). Eur J Cancer
1999; 35: 1076–1082.
27. Kole AC, Nieweg OE, Pruim J et al. Detection of unknown occult primary
tumors using positron emission tomography. Cancer 1998; 82:
1160–1166.
28. Bohuslavizki KH, Klutmann S, Kroger S et al. FDG PET detection of unknownprimary tumors. J Nucl Med 2000; 41: 816–822.
29. Grau C, Johansen LV, Jakobsen J et al. Cervical lymph node metastases
from unknown primary tumours. Results from a national survey by the
Danish Society for Head and Neck Oncology. Radiother Oncol 2000; 55:
121–129.
30. Jungehulsing M, Scheidhauer K, Damm M et al. 2[F]-fluoro-2-deoxy-D-glucose
positron emission tomography is a sensitive tool for the detection of occult
primary cancer (carcinoma of unknown primary syndrome) with head and
neck lymph node manifestation. Otolaryngol Head Neck Surg 2000; 123:
294–301.
31. Nieder C, Gregoire V, Ang KK. Cervical lymph node metastases from occult
squamous cell carcinoma: cut down a tree to get an apple? Int J Radiat Oncol
Biol Phys 2001; 50: 727–733.
32. Rades D, Kuhnel G, Wildfang I et al. Localised disease in cancer of unknown
primary (CUP): the value of positron emission tomography (PET) for individualtherapeutic management. Ann Oncol 2001; 12: 1605–1609.
33. Greven KM, Keyes JW, Jr., Williams DW III et al. Occult primary tumors of the
head and neck: lack of benefit from positron emission tomography imaging with
2-[F-18]fluoro-2-deoxy-D- glucose. Cancer 1999; 86: 114–118.
34. Lonneux M, Reffad A. Metastases from Unknown Primary Tumor. PET-
FDG as Initial Diagnostic Procedure? Clin Positron Imaging 2000; 3:
137–141.
35. Alberini JL, Belhocine T, Hustinx R et al. Whole-body positron emission
tomography using fluorodeoxyglucose in patients with metastases of
unknown primary tumours (CUP syndrome). Nucl Med Commun 2003; 24:
1081–1086.
36. Standards, Options et Recommandations pour la prise en charge des patients
atteints de carcinomes de site primitif inconnu: http://www.fnclcc.fr/
Recommandations pour la pratique clinique/acce ` s aux RPC SOR/Cancer de
l’adulte/divers/carcinome de site inconnu/Strate gie diagnostique (online acces
15 february 2006)
37. Greco FA, Hainsworth JD: Tumors of unknown origin. CA Cancer J Clin 1992;
42: 96–115.
38. Shildt RA, Kennedy PS, Chen TT et al. Management of patients with metastatic
adenocarcinoma of unknown origin: a Southwest Oncology Group study. Cancer
Treat Rep 1983; 67: 77–79.
39. Baron PL, Moore MP, Kinne DW et al. Occult breast cancer presenting
with axillary metastases. Updated management. Arch Surg 1990; 125:
210–214.
40. Orel SG, Weinstein SP, Schnall MD et al. Breast MR imaging in patients with
axillary node metastases and unknown primary malignancy. Radiology 1999;
212: 543–549.
41. Kirsten F, Chi CH, Leary JA et al. Metastatic adeno or undifferentiated carcinoma
from an unknown primary site–natural history and guidelines for identification
of treatable subsets. Q J Med 1987; 62: 143–161.
42. Tell DT, Khoury JM, Taylor HG et al. Atypical metastasis from prostate cancer.
Clinical utility of the immunoperoxidase technique for prostate-specific antigen.
JAMA 1985; 253: 3574–3575.
43. Gentile PS, Carloss HW, Huang TY et al. Disseminated prostatic carcinoma
simulating primary lung cancer. Indications for immunodiagnostic studies. Cancer
1988; 62: 711–715.
44. Greco FA, Vaughn WK, Hainsworth JD. Advanced poorly differentiated carcinoma
of unknown primary site: recognition of a treatable syndrome. Ann Intern Med
1986; 104: 547–553.
Annals of Oncology
x
176 | Jerusalem et al. Volume 17 | Supplement 10 | September 2006