GP+HFMA+presentation
42
‘Medicine for Managers; General Practice’ Presented by Dr. Michael Gregory, Clinical Director for Strategy and Policy for Trafford CCG Chaired by Andrew Wood Chief Finance Officer at Fareham & Gosport and South Eastern Hampshire Clinical Commissioning Groups 23 rd January 2014 - 11.00am-12.00pm
-
Upload
michael-gregory -
Category
Documents
-
view
154 -
download
0
Transcript of GP+HFMA+presentation

‘Medicine for Managers; General Practice’ Presented by Dr. Michael Gregory, Clinical Director for Strategy and Policy for Trafford CCG Chaired by Andrew Wood Chief Finance Officer at Fareham & Gosport and South Eastern Hampshire Clinical Commissioning Groups 23rd January 2014 - 11.00am-12.00pm

Housekeeping Guy Mitson, e-learning manager, hfma • Do put your questions to our speakers!
• Type your questions in as you think of them, rather than waiting
until then end.
• Try refreshing your browser if you have any audio problems and check your internet connection. -For more technical help, click on the ‘Test your System’ at the bottom of the screen.
• Please leave a rating so that we can maintain and improve your webinar experience.
• Webinar and presentation will be available on the HFMA site straight after this webinar finishes .

Primary Care
Dr Michael Gregory General Practitioner West Timperley Medical Centre Altrincham, Cheshire. Clinical Director Trafford CCG.

• An introduction to general practice. • The role of GPs in healthcare and the services
provided • How general practice is financed • Current challenges for general practice • Future developments that will impact on general
practice.

A bit of history….. National Insurance Act 1911

1946 - Creation of NHS

1950 -Collings Report 1952 - Danckwerts Award 1966 - General Medical Services Contract

1952 – Creation of RCGP

1980s - increased scrutiny 1990s - evolving roles 2004 - GP contract 2013 - Health and Social Care Act

The Importance of Primary Care
Questions

Role of GPs
‘personal doctors, primarily responsible for the provision of comprehensive and continuing generalist care to every individual seeking medical care irrespective of age, sex and state of health’.

GP Training Primary Care Management Person centred care Specific problem solving skills Comprehensive approach Community orientation Holistic approach

GP Training Medical Degree 5 years Foundation training (usually in medicine and surgery) 2 years Speciality Registrar Specialities 18 months Practice 18 months
Prescriptions
Consultations Treatments
Referrals
Screening
Imms
LTCs Health Promotion


HSCIC 2009
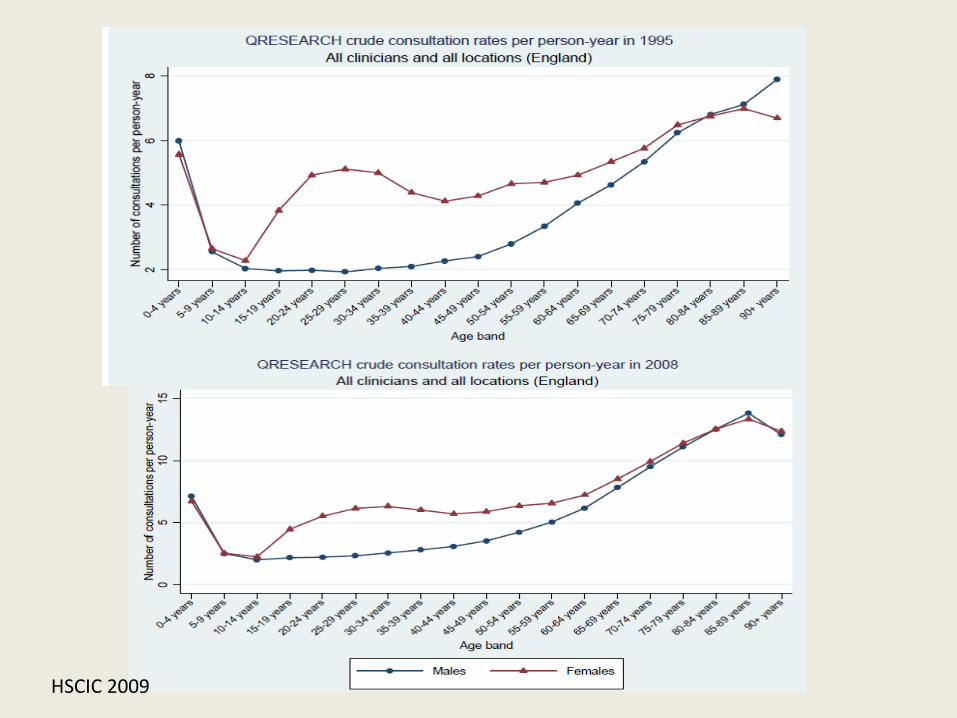
HSCIC 2009
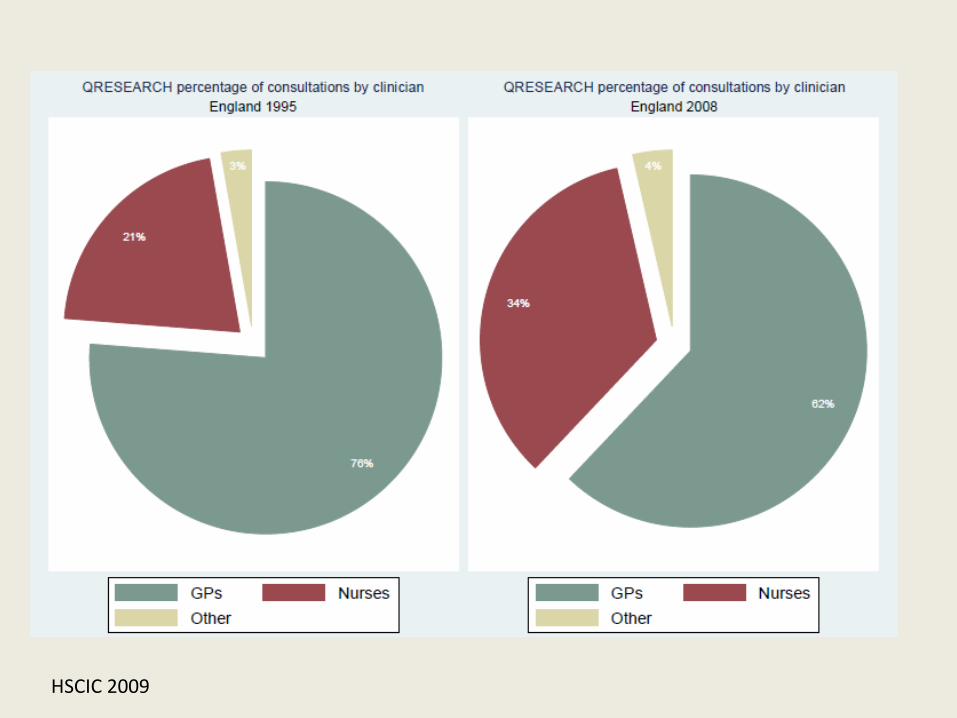
HSCIC 2009

HSCIC 2009

Question

2004 Contract
General Medical Services Personal Medical Services Alternative Personal Medical Services

Global Sum
• MPIG • Correction Factor

Quality and Outcomes Framework
• Clinical Domain • Public Health Domain • Quality and Productivity Domain • Patient Experience

Question
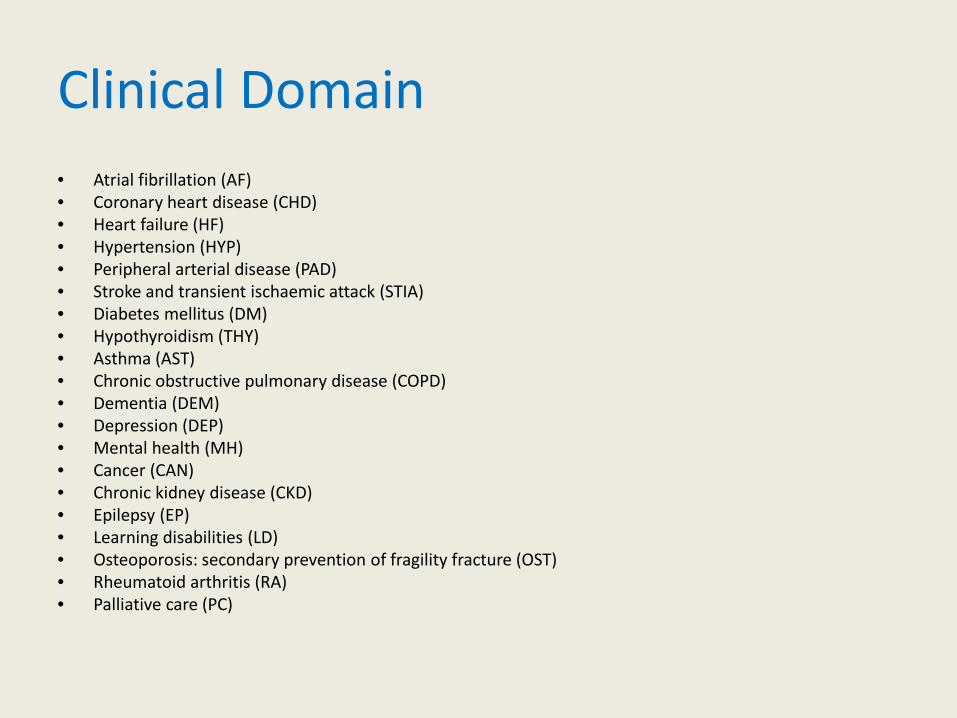
Clinical Domain • Atrial fibrillation (AF) • Coronary heart disease (CHD) • Heart failure (HF) • Hypertension (HYP) • Peripheral arterial disease (PAD) • Stroke and transient ischaemic attack (STIA) • Diabetes mellitus (DM) • Hypothyroidism (THY) • Asthma (AST) • Chronic obstructive pulmonary disease (COPD) • Dementia (DEM) • Depression (DEP) • Mental health (MH) • Cancer (CAN) • Chronic kidney disease (CKD) • Epilepsy (EP) • Learning disabilities (LD) • Osteoporosis: secondary prevention of fragility fracture (OST) • Rheumatoid arthritis (RA) • Palliative care (PC)
Public Health Domain
• Cardiovascular disease – primary prevention (CVD-PP)
• Blood pressure (BP) • Obesity (OB) • Smoking (SMOK) • Cervical screening (CS) • Child health surveillance (CHS) • Maternity (MAT) • Sexual health (CON)

Other Domains
• Quality and Productivity Domain • Patient Experience

Quality and Outcomes Framework

The physical activity index categorises patients’ level of activity, which is correlated to CVD risk. Patients are categorised as: 1. Inactive – sedentary job and no physical exercise or cycling 2. Moderately inactive – sedentary job and some but less than one hour of physical exercise and/or cycling per week or standing job and no physical exercise or cycling 3. Moderately active – sedentary job and one to 2.9 hours of physical exercise and/or cycling per week or standing job and some but less than one hour of physical exercise and/or cycling per week or physical job and no physical exercise or cycling 4. Active – sedentary job and three hours or more of physical exercise and/or cycling per week or standing job and one to 2.9 hours of physical exercise and/or cycling per week or physical job and some but less than one hour of physical exercise and/or cycling per week or heavy manual job. It is advised that all patients who receive a score of 'less than active' are offered a brief intervention supporting behaviour change to increase physical activity.
Exception Reporting
• Explicit rejection • No response to invitations • Patient unsuitable • On maximum tolerated therapy

Enhanced Services
• Direct Enhanced Services • National Enhanced Services • Local Enhanced Services

Contract Changes 2013/14
• New vaccination programmes
• Enhanced Services (NHS England):
• High risk of admission patients
• Dementia • Remote care monitoring
preparation • Electronic booking

Contract Changes 2014/15
• Enhanced services: • People at risk of admission • Abolition of risk profiling DES, patient online
booking DES and Remote care monitoring DES. • 341 QoF points retired • 238 points into core funding and remaining to
fund enhanced services • MPIG phase out • Seniority phased out

GP Income
• 20% decline since 2005/6
• Expense rise of 56.5% of earnings in 2004/5 to 61.6% in 2011/12.

Clinical Commissioning Groups


Barriers
• Prescribing • Secondary care activity • Choice agenda • Competition and collaboration • IT


Nuffield – Securing the Future of General Practice 2013.
• improving population health, particularly among those at greatest risk of illness or injury
• managing short-term, non-urgent episodes of minor illness or injury
• managing and coordinating the health and care of those with long-term conditions
• managing urgent episodes of illness or injury
• managing and coordinating care for those who are nearing the end of their lives.


Future of General Practice
• From solo practitioner to multi professional team • Value generalism whilst embracing specialist
knowledge • Developing shared care • Wider range of integration • From gatekeeper to navigator • Support SDM and self care