Case Presentation

of 82
description
CKD
Transcript of Case Presentation
-
7/15/2019 Case Presentation
1/82
Chronic Kidney Disease 2to Diabetes Mellitus IIrelated to Hypertension,
Anemia 2 to Nephropathy
Group 1
-
7/15/2019 Case Presentation
2/82
GROUP 1
-
7/15/2019 Case Presentation
3/82
Arceo, Mari
Aguirre, Kim Leonard
Bermudez, Joanna Marie
Bongkingki, Janela Cassandra
De Guzman, Fredaline Dayle
De Guzman, Maria Cristina
Desvarro, Eric
Domingo, JenniferLeyva, Allan Mario
Seminiano, Haidy
Socias, Christian Anthony
-
7/15/2019 Case Presentation
4/82
-
7/15/2019 Case Presentation
5/82
-
7/15/2019 Case Presentation
6/82
OUR LOVELY CLINICAL INSTRUCTOR
-
7/15/2019 Case Presentation
7/82
Mrs.Angelica Hernandez
-
7/15/2019 Case Presentation
8/82
Introduction
-
7/15/2019 Case Presentation
9/82
I. Background of the studyPresenting a case of Patient H.F., 51 year-old female
admitted on the 24th of September , 2012 at 7:30 PMwith baseline vital signs of T- 37.1 C, PR-92bpm, RR-23
bpm, and a BP of 160/90mmHg. The patient was
admitted to the Mandaluyong City Medical Center, and
was given a final diagnosis of Chronic Kidney Disease 2to Diabetes Mellitus II related to Hypertension,
Anemia 2 to Nephropathy
Diabetes mellitus (DM) is a set of related diseases in
which the body cannot regulate the amount of sugar(specifically, glucose) in the blood. The blood delivers
glucose to provide the body with energy to perform all of
a person's daily activities.
-
7/15/2019 Case Presentation
10/82
The liver converts the food a person eats into glucose. The glucose isthen released into the bloodstream.
In a healthy person, the blood glucose level is regulated by several
hormones, primarily insulin. Insulin is produced by the pancreas, a small
organ between the stomach and liver. The pancreas also makes other
important enzymes released directly into the gut that helps digest food.
Insulin allows glucose to move out of the blood into cells throughout
the body where it is used for fuel.
People with diabetes either do not produce enough insulin (type 1
diabetes) or cannot use insulin properly (type 2 diabetes), or both (which
occurs with several forms of diabetes).
In diabetes, glucose in the blood cannot move efficiently into cells, soblood glucose levels remain high. This not only starves all the cells that
need the glucose for fuel, but also harms certain organs and tissues
exposed to the high glucose levels.
-
7/15/2019 Case Presentation
11/82
Type 2 diabetes (T2D): Although the pancreas still secretes insulin,the body of someone with type 2 diabetes is partially or completelyunable to use this insulin. This is sometimes referred to as insulin
resistance. The pancreas tries to overcome this resistance by secreting
more and more insulin. People with insulin resistance develop type 2
diabetes when they fail to secrete enough insulin to cope with their
higher demands.At least 90% of adult individuals with diabetes have type 2 diabetes.
Type 2 diabetes is typically diagnosed in adulthood, usually after age 45
years. It used to be called adult-onset diabetes mellitus, or non-insulin-
dependent diabetes mellitus. These names are no longer used because
type 2 diabetes does occur in younger people, and some people withtype 2 diabetes require insulin therapy. Type 2 diabetes is usually
controlled with diet, weight loss, exercise, and oral medications.
However, more than half of all people with type 2 diabetes require
insulin to control their blood sugar levels at some point in the course of
their illness.
-
7/15/2019 Case Presentation
12/82
A. RATIONALE FOR CHOOSING THE CASE1. To know the anatomy and physiology of the pancreas and the associated
organs.
2. To know the pathophysiology of Diabetes Mellitus Type 2, its signs and
symptoms and its further complications.
3. To know the appropriate nursing intervention in accordance with itsscientific rationales.
4. To know the appropriate medical management in the treatment of the
disease.
-
7/15/2019 Case Presentation
13/82
B. OBJECTIVES OF THE STUDYThis case study aims to identify and determine general health problems and
needs of the patient with a diagnosis Chronic Kidney Disease 2 to Diabetes
Mellitus II related to Hypertension, Anemia 2 to Nephropathy. This work
also intends to promote health and medical understanding of such condition
through the application of nursing process and skills.
Specific Objectives:The students will be able to improve their skills in conducting appropriate
assessment on the clients health condition.
The students will enhance their knowledge on the disease process and its
effect to the human body.The students will be able to formulate a scientific-based pathophysiology
based on the clients health history and presenting signs and symptoms.
The students will be able to formulate appropriate Nursing Care plan based
on the clients presented health problems and risks and effectively
improve/alleviate clients health condition.
-
7/15/2019 Case Presentation
14/82
The students will be able to utilize the nursing process and critical
thinking skills in the management and care of the common problems
of the patient.
The students will be able to render quality care to patients guided
with scientific based rationale.
The students will be able to expand their knowledge on the drugs
through identification of its indication, side effects, adverse reactions
and mechanism of action on why it was prescribed to the patient and
specific nursing considerations.
-
7/15/2019 Case Presentation
15/82
ASSESSMENT
Clients Profile Name : Patient F.H.
Age : 51 years old
Gender : Female
Birth Date : December 22, 1960
Civil status : Married
Occupation : Housewife
Nationality : Filipino
Religion : Catholic
-
7/15/2019 Case Presentation
16/82
Date of Admission : September 24, 2012
Time of admission : N/A
Admitting Diagnosis : Chronic Kidney Disease 2 to
Diabetes Mellitus II related toHypertension, Anemia 2 to
Nephropathy
B. Chief Complaint : Generalized body weakness
-
7/15/2019 Case Presentation
17/82
C. History of Present Illness : Three days prior to admission, client
experienced loss of Appetite, generalized
body weakness and easy fatigability.
Symptoms persisted which promptedconsult.
D. Past Medical History : DM Type II for ten yearsPeripheral Vascular Disease
Accidents : N/A
Hospitalization : Last hospitalization: July, 2012.
Medications taken : Glucovance 2.5 mg
Losartan 50mg
-
7/15/2019 Case Presentation
18/82
GrandfatherGrandmother
Father
Mother
Patient
Brother 1
SisterBrother 2
Hypertension
Diabetes
Heart Disease
Deceased
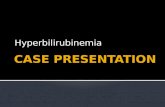
E. Family History
Legends
-
7/15/2019 Case Presentation
19/82
E. Family HistoryThe following figure shows the family genogram of the patient.
GrandfatherGrandmother Grandfather
Grandmother
FatherMother
Patient
H.F
Husband
Fatherside Motherside
LEGEND:
Deceased
Diabetes Mellitus
Colon Cancer
Hypertension
Nephropathy
Male
Female
-
7/15/2019 Case Presentation
20/82
F. Gordons Functional Health Pattern Health Perception and Health Management
Before hospitalization, she knows that being healthy is important, but she is
not fond of doing exercise. Her perception of a healthy person is anyone who
can perform their daily task and one who doesnt have a disease. She drinks
alcoholic beverages occasionally and does not smoke. When the patient is
hospitalized, she perceived herself as an unhealthy person.
Nutrition and Metabolism
Before hospitalization, the client states that she loves to eat. She loves to
eat everything including those foods that are not advisable for her to eat.
During hospitalization, the client is advised to be on a Low salt, low fat, DM
Diet. She becomes more aware of her condition and states that she will try
her best to follow the advised diet.
-
7/15/2019 Case Presentation
21/82
24 Hour Diet-Recall
Meal Food QuantityBreakfast Rice Half cup
Chicken Breast Small serving
Coffee 1 cup
Lunch Lugaw with egg 1 bowl
Orange juice 1 glass (250 ml)
-
7/15/2019 Case Presentation
22/82
EliminationPrior to hospitalization, the client defecates brownish, formed stool 6-7
times a week. She urinates clear-yellowish urine 6-7times a day. During
hospitalization, client stated that she defecates once in every two days and
she urinates 6-7 times per shift. She also stated that she perspires just right.
Activity ExerciseBefore hospitalization, clients household chores serve as her way of
exercising. Whenever she is doing something like cleaning the house or
washing the chores, she gets tired easily. During hospitalization, walking is
her only activity.
Sleep RestPrior to hospitalization, client normally gets 6-7 hours of sleep. She does
not have any difficulty sleeping. She claimed that hospitalization affects her
sleeping pattern; she cannot sleep comfortably and wakes up easily.
-
7/15/2019 Case Presentation
23/82
Cognitive PerceptualThe client can recall past memories when being asked. She has no
hearing problems. The client is oriented with time, place, people and date.
She is able to follow instructions. Client claimed that her memory hasnt
changed even during hospitalization.
Self Perception / Self ConceptClient claimed that she was already satisfied with her life. She states that
prior to hospitalization, she perceives herself as a loving wife and mother.
She perceives herself as a healthy person. Upon hospitalization, client sees
herself as unhealthy.
Role Relationship PatternPrior to hospitalization, client lives with her husband and they have 7
children. Their child supports their financial needs. She and her husband
take part in decision-making. They have open communication with each
other. The client presently feels the support of her family and she is happy
about it. Upon hospitalization, clients husband takes responsibility indecision-making.
-
7/15/2019 Case Presentation
24/82
Sexuality ReproductiveThe client stated that they do not practice family planning ever since.
Despite of their age, theyre still able to maintain a satisfying sexual
relationship. The couple engages in sexual activity once or twice a month.
During hospitalization, client doesnt engage with sexual activity anymore.
Coping Stress TolerancePrior to hospitalization, Clients usual cause of stress is misunderstandingwith her husband and children. She easily gets irritated with arguments and
cries whenever depressed. During hospitalization, she claims that she gets
stressed whenever she experiences body weakness. Client would just vent out
to her husband and try to sleep.Value BeliefThe client states that she is a religious person and usually goes to
church every Sunday. During hospitalization, client claimed that she becomes
closer to God and that she never forgets to pray for her faster recovery.
-
7/15/2019 Case Presentation
25/82
G. Physical ExaminationGeneral SurveyThe patients body built is proportionate with coordinated posture and gait.
Client is lethargic but coherent and oriented to time, place and person. Clientappears to be physically weak upon assessment.
Vital SignsHer temperature is 37.1 C, axillary with a regular pulse rate of 75 bpm. The
respiratory rate is 34 cpm, deep and her bp is 180/110 mmHg taken in a lyingposition.
Anthropometric MeasurementsHer height is 52 and her weight is 136 lbs (upon admission), 129lbs (upon
referral).
-
7/15/2019 Case Presentation
26/82
SkinHer skin color is pale, with venoclysis on right metacarpal vein .She has no
edema. She has dry skin, cool upon touch and show poor turgor.
HairHer hair is evenly distributed, thick and silky. There is presence of sparse
leg hair. There is no presence of infestations.
NailsHer nails are convex 160 in curvature and angle. The texture is smooth
with pale nail beds. The surrounding tissues are intact and capillary refills in
4 seconds.
Skull and FaceThe skull is normocephalic, has smooth contour, has symmetrical facial
features.
-
7/15/2019 Case Presentation
27/82
Eye Structures and Visual AcuityHer eyebrows are evenly distributed, eyelashes are equally distributed, intact
skin, and eyes close symmetrically and have 15-20 involuntary blinks. She
has pale conjunctiva and has transparent cornea, PERRLA. Her eye is
coordinated in extraocular movement and she is able to read newspaper.There is a presence of peritorbital edema on both eyes.
Ears and HearingThe pinna of her ears has a uniform skin color and symmetrical. The ear
canal has presence of dry cerumen .The tympanic membrane is pearly gray
and the hearing acuity is intact.
Nose and SinusesShe has symmetrical nasolabial fold. Her septum is in midline, non-deviated
and has no perforation. Its mucosa is dry but has no discharges. It is both
patent. She has symmetrical gross smell. Sinuses are not tender.
-
7/15/2019 Case Presentation
28/82
Mouth and OropharynxHer lips are dry, pale and with few lesions. She has 4 missing teeth; 1right,
upper lateral incisor, 1st right, upper premolar, 2nd left, lower molar, 3rd left,
lower molar. Tongue is in midline, pinkish, smooth and movable. Her
palate is light pink and smooth with uvula is in midline. The oropharynx isalso pink and smooth. Tonsils are not inflamed. The gag reflex is intact.
NeckHer neck muscles are equal in size with a coordinated movement, full range
of motion and equal muscle strength. The lymph nodes are not palpable.
The trachea is in midline, the thyroid gland is not visible with a symmetrical
carotid pulse. The jugular veins are not visible.
Thorax and LungsHer breathing pattern is rapid and deep. The shape and symmetry of the
thorax and lungs is symmetrical, the spine is aligned with a smooth skin. The
respiratory excursion is full and symmetric.
-
7/15/2019 Case Presentation
29/82
Breast and Axilla
Her breast and axillas shape is rounded. The skin is smooth with round
areola. The nipples are round.
AbdomenThe abdomen contour is rounded and the symmetry is symmetrical. The
bowel sounds are normoactive with a tymphanic percussion and relaxed
palpation.
Upper and Lower ExtremitiesThe upper and lower extremities have an equal muscle size, firm muscle
tone with equal muscle strength. Her range of motion is limited.
-
7/15/2019 Case Presentation
30/82
H. Laboratory and Diagnostic Study
-
7/15/2019 Case Presentation
31/82
PROBLEM IDENTIFICATION
-
7/15/2019 Case Presentation
32/82
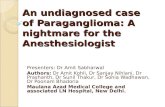
A. Anatomy of PancreasThe pancreas is an elongated, tapered organ located across the ba
ck of theabdomen, behind the stomach. The right side of the organ(called the head) is the widest part of the organ and lies in the curve
of the duodenum (the first section of the small Intestine). The
tapered left side extends slightly upward (called the body of the
pancreas) and ends near the spleen (called the tail).The pancreas are
made up of two types of tissue:
-
7/15/2019 Case Presentation
33/82
-
7/15/2019 Case Presentation
34/82
Exocrine tissue the exocrine tissue secretes digestive enzymes. These
enzymes are secreted into network of ducts that join the main pancreatic duct,which runs the length of the pancreas.
Endocrine tissue the endocrine tissue, which consists of the islets of
Langerhans, secretes hormones into the bloodstream.
Functions of the pancreas:
The pancreas has digestive and hormonal functions:
The enzymes secreted by the exocrine tissue in the pancreas help break down
carbohydrates, fats, proteins, and acids in the duodenum. These enzymes travel
down the pancreatic duct into the bile duct in an inactive form. When they
enter the duodenum, they are activated. The exocrine tissue also secretesbicarbonate to neutralize stomach acid in the duodenum.
The hormones secreted by the endocrine tissue in the pancreas are insulin
and glucagon (which regulate the level of glucose in the blood), and somatostatin
(which prevents the release of the other two hormones.
-
7/15/2019 Case Presentation
35/82
Anatomy of kidney
The kidneys play key roles in body function, not only by filtering the blood
and getting rid of waste products, but also by balancing levels
of electrolytes in the body, controlling blood pressure, and stimulating
the production of red blood cells.
-
7/15/2019 Case Presentation
36/82
The kidneys are located in the abdomen toward the back,
normally one of each side of the spine. They get their blood supply
through the renal arteries directly from the aorta and send blood back
to the heart via the renal veins to the vena cava. (The term renal" is
derived from the Latin name for kidney.)The kidneys have the ability
to monitor the amount of body fluid, the concentrations of
electrolytes like sodium and potassium, and the acid-base balanceof the body. They filter waste products of body metabolism, like urea
from protein metabolism and uric acid from DNA breakdown. Two
waste products in the blood can be measured: blood urea
nitrogen (BUN) and creatinine (Cr).Kidneys are also the source
of erythropoietin in the body, a hormone that stimulates the bonemarrow to make red blood cells. Special cells in the kidney
monitor the oxygen concentration in blood. If oxygen levels fall,
erythropoietin levels rise and the body starts to manufacture more red
blood cells.
-
7/15/2019 Case Presentation
37/82
Diabetes Mellitus
Diabetes Mellitus type 2 is the most common form of Diabetes.
Formerly known as adult
onset diabetes, it usually affects people aged over 40 and progresses
gradually. In this type the pancreas has not ceased to produce insulin, butthe quantity is insufficient, or the hormone is not stimulating the glucose
uptake in muscles and tissues required for energy. The result is a build-upof glucose in blood and urine.
Although the cause of this malfunctioning is unclear, non-insulin dependent
diabetes mellitus tends to run in families. Other risk factors, such as
increasing age, obesity, and a sedentary lifestyle, probably contribute to its
increased incidence in developed countries. Non-insulin dependent diabetes
mellitus can often be controlled initially by diet alone, or in combinationwith tablets that reduce the amount of blood
glucose. There are two main types of blood glucose-reducing drugs:
sulphonylureas work mainly by stimulating the pancreass islet cells (known
as the islets of Langerhans) to produce more insulin and iguanids increase
the effectiveness of insulin on cells. Eventually, however, patients may need
insulin injections.
-
7/15/2019 Case Presentation
38/82
Signs and Symptoms with Rationale Diabetes Mellitus
HYPERGLYCEMIA (INCREASED BLOOD SUGAR LEVEL)
May be due to lack of physiologically
active insulin that transportsglucose from extracellular to intracellular leadingto accumulation of glucose in the intravascular space. The glucose is not
utilized by the body and it remains in the blood streams.
POLYURIA
Increased frequency of urination. This may be due to the osmoticdiuretic effect of the glucose, wherein it attracts water during urination.
POLYDIPSIA
Increased thirst and fluid intake. This may be due to the activation of
thethirst center in the hypothalamus resulting form the intracellular dehydration or volume depletion.
-
7/15/2019 Case Presentation
39/82
POLYPHAGIA
Increased hunger and food intake. This may be due to the decrease
glucose uptake by the cells leading the stimulation of the satiety center in
the hypothalamus resulting to the hunger sensation.
WEAKNESS/ FATIGUE
This is due to the decreased glucose uptake by the cells leading to
decreased energy production.
GLYCOSURIA
The kidney filters the blood, making it to its normal state. Glucose
was filtered out and excreted in the urine.
Due to the excess glucose ad compared to the kidney threshold,
which results to the excretion of glucose in the urine. GASTROPARESIS
(Stomach fullness)
-
7/15/2019 Case Presentation
40/82
CONSTIPATION and BLOATING
This is due to changes in nerves and damages the blood vessels that
carry oxygen and nutrients to the nerves. Over time, high blood glucose
can damage the vagus nerve. The stomach fails to empty properly and is
likely due to the generalized neuropathy.
NAUSEA/ VOMITING
Due to stomach fullness, there will be an involuntary emptying
of stomach contents that are forcefully expelled by the mouth.
A compensatory mechanism due to acidity of body because of
decrease excretion of metabolic waste.
PALE
Due to decreased production of erythropoietin.
-
7/15/2019 Case Presentation
41/82
B. Pathophysiology
C P bl Li t
-
7/15/2019 Case Presentation
42/82
C. Problem List
-
7/15/2019 Case Presentation
43/82
PLANNING
A Problem Prioriti ation
-
7/15/2019 Case Presentation
44/82
A. Problem Prioritization
NURSING PROBLEM RANK JUSTIFICATION
1
2
3
-
7/15/2019 Case Presentation
45/82
C. Discharge PlanningMedication Instruct the patient the importance of regularly taking of prescribed home
medications.
Amlodipine 10mg 1 tab / OD
Cefuroxime 500 mg 1 tab / BID
NaHCO3 1 tab / TID
CaCO3 1 tab / TID
Ferrous sulfate + Folic acid 1 tab / OD
Insulin
Ensure safety by providing health teaching about the side effects and adverse
effects of the drug.
Instruct the patient to continue with follow up medical care.
Advise the patient not to miss the intake of medication given by his physician.
-
7/15/2019 Case Presentation
46/82
Exercise and Environment Encourage the patient mild exercise such as walking it is best to start slowly and
more as the patient get stronger. Exercising can make the heart stronger, lower
blood pressure and keep healthy. Exercise can benefit patient with CKD/DM
Nephropathy. Resistance training in particular helps reduce the catabolic effectsof a low-protein (0.6g/kg/day) diet, whereas aerobic exercise may help control
blood pressure and lipid level.Treatment Since the patient due to the loss of renal erythropoietin production and should
be treated with supplement iron and synthetic erythropoietin to reach a target
hemoglobin of 11-12g/ dL. Phosphate binders and dietary phosphorus restriction
are indicated to keep phosphate,
-
7/15/2019 Case Presentation
47/82
Health Teaching Encourage the patient also have adequate rest periods and to have an adequate sleep
of at least of 8-10hrs.
Encourage the patient to eat a low-protein diet.
Instruct the patient to limit fluid intake.
Instruct the patient regarding limiting the amount of salt (sodium), potassium,
phosphorus and other electrolytes, getting enough calories, especially if patient is
losing weight.
Encourage the patient also have to Monitor of blood glucose levels.
Help the patient/ Family learn self-observational skills (Temperature, Pulse,Respirations, Blood Pressure, intake and output and weight) and record keeping.
Explain the benefits of consuming simple, basic foods such as lean meat, fresh orfrozen vegetables, and whole grained breads. Processed or prepared foods should
be avoided.
-
7/15/2019 Case Presentation
48/82
Encourage the patient keep a food diary for several days. It should include
food eaten, portion size, and time of consumption so that together you canmodify the diet as needed.
Explain avoidance of infection.
Out patient Instruct the patient to come back for follow up check-up.
Emphasize the need to be present in medical procedure schedule.
-
7/15/2019 Case Presentation
49/82
Diet Low total and animal protein
A prolonged high-protein intake is accompanied by an increase in GFR, 4
which in turn may cause intraglomerular hypertension and eventual loss of renal
function.
Sodium Restriction
Patient with CKD are often salt-sensitive, responding to elevated intakes of
sodium chloride with increase in glomerular filtration and proteinuria.
Water-Soluble Vitamins
Low-protein diets may increase the risk for deficiency of thiamine, riboflavin
and especially pyridoxine, and vitamin C levels are also often low in DM.
-
7/15/2019 Case Presentation
50/82
Vitamin D Supplementation
Deficiency of vitamin D is present early in the course of DM, and
correction may prevent activation of key pathogenic mechanism in
cardiovascular disease. (e.g. Inflammation, Myocardial cell hypertrophy
and Proliferation and the renin-angiotensin system).
A Diet in Fiber and Low in saturated Fat and cholesterol
Most patients with Chronic Kidney Disease die from cardiovascular
causes before developing DM Nephropathy. Dietary and supplemental
source of fiber may be helpful for reducing the build up of nitrogenous
waste products in the blood that cause many symptoms of uremia.
Maintain on low salt and low fat.
Limit sodium, potassium, phosphorus and other electrolytes.
Limit fluid intake.
-
7/15/2019 Case Presentation
51/82
The following table is a proposed 1 week diet of the patient:
Sunday Monday Tuesday Wednesday
Thursday Friday Saturday
BreakfastApple slices
Bread w/
tuna spread
Pineapple
juice.
Cereals
Fresh
milk
Oatmeal
Orange
juice
Brown
Rice
1/2cup
1 serving
of tinolang
manok
Grape
juice 1
glass
1 cup
fiber one
Original
cereal
1 cup
Skim milk
slice of
melon and
strawberrie
1 cup
Prepared
Oatmeal
cup
Skim milk
2 tbsp.
Seedless
raisins
1 servings
of oranges
2 oz cheddar
cheese, low
fat
2 slices of
wheat bread
Watermelon
2 servings
A glass of
Orange juice
Sunday Monday Tuesday Wednesd Thursday Friday Saturday
-
7/15/2019 Case Presentation
52/82
ayLUNCH
Toast,
hardboiledeggs &
Orange.
Slices (340
calories)
1 slice whole
wheat toast
2 tsp. Jam
2 large Hard-
boiled eggs
1 mediumOrange, cut
into segments
100g Non-fat
fruit yogurt
Glass ofWater
Brown
Rice
1/2cup
Chicken
(280
calories)
2
servings
of
Papaya
slice
Steam
rice 1
cup
Ampalay
a with
scramble
s egg 2servings
Glass of
water
2 slices
whole
wheatbread
90g tuna,
canned
in water
1 tbsp.
Mayonn
aise
2 leaveslettuce
2 serving
of
pinakbet
Steam rice
1 cup
1 glass of
2 servings
of ripe
Kiwifruit
Glass of
water
1 serving
of
sinigangna
bangus
Brown
Rice1/2cup
1 glass of
Orange
juice
2 servings
of apple
slices
2 servings of
tortang talong
Steam rice 1
cup
Pineapple
juice
2 servings of
slices melon
-
7/15/2019 Case Presentation
53/82
Sunday Monday Tuesday Wednesday
Thursday Friday Saturday
DINNER1
servings
Vegetabl
es salad
with tuna
Orange
juice
100 g
chicken
breast,
boneless,
skinless
cooked
1 cup
medium
grain
brown rice
(cooked)
2 cups
Green
beans,
steamed
1
servings
Pesang
dalag
with
miso
Brown
Rice
cup
2
servings
of ripe
mangoe
s
1
serving
s of
chopsue
y
Brown
Rice
cup
1 servings
Shrimp
sinigang
With
vegetables
BrownRice
cup
Pineapple
juice
1 servings
Paksiw
na isda
Brown
Rice
cup
2 servings
of
Papaya
slice
Glass of
water
100 g
chicken
breast,
boneless,
skinless
cooked
Brown Rice
cup
-
7/15/2019 Case Presentation
54/82
Spiritual Counseling Encourage the patient not to lose hope and have faith in GOD.
Encourage the patient to seek the LORDs guidance and pray in
times of hopeless.
-
7/15/2019 Case Presentation
55/82
IMPLEMENTATION
-
7/15/2019 Case Presentation
56/82
GENERIC NAME : AmlodipineBRANDNAME : NorvascCLASSIFICATION : Cardiovascular agent
; Calcium channel
blocker; antihypertensive agent.
DOSAGE : 10 mg 1 tab//ODDRUG ACTION : These medications block the transport ofcalcium into the smooth muscle cells lining the coronary arteries and other arteries
of the body. Since calcium is important in muscle contraction, blocking calcium
transport relaxes artery muscles and dilates coronary arteries and other arteries of
the body.INDICATION : Chest pain or heart pain (angina) occursbecause of insufficient oxygen delivered to the heart muscles. Insufficient oxygen
may be a result of coronary artery blockage or spasm, or because of physicalexertion which increases heart oxygen demand in a patient with coronary artery
narrowing. Amlodipine is used for the treatment and prevention of angina resulting
from coronary spasm as well as from exertion. Amlodipine is also used in thetreatment of hi h blood ressure.
A. Drug Study
-
7/15/2019 Case Presentation
57/82
ADVERSE REACTION: The two most common side effectsare headache and edema (swelling) of the lower extremities. Less common
side effects include dizziness, flushing, fatigue, nausea, and palpitationsNURSING RESPONSIBILITY: Monitor BP for therapeutic effectiveness. BP reduction is greatest after
peak levels of amlodipine are achieved 69 h following oral doses.
Monitor for S&S of dose-related peripheral or facial edema.
Monitor BP with postural changes. Report postural hypotension.
Monitor more frequently when additional anti hypertensives or diuretics
are added.
-
7/15/2019 Case Presentation
58/82
GENERIC NAME : Cefuroxime
BRANDNAME : Zinacef
CLASSIFICATION : Cephalosporin
DOSAGE : 500mg 1 tab//BID
DRUG ACTION : Decreases or control the infection.
INDICATION : For the treatment of many different typesof bacterial infections such as bronchitis, sinusitis, tonsillitis, ear
infections, skin infections, gonorrhea, and urinary tract infections.
CONTRAINDICATION : Contraindicated in patients hypersensitive
to drug or other cephalosporin. CV: phlebitis, thrombophlebitis. GI:
diarrhea, anorexia, vomiting. Hematologic: hemolytic anemia,
thrombocytopenia, transient neutropenia, eosinophilia
-
7/15/2019 Case Presentation
59/82
NURSING RESPONSIBILITY: Determine history of hypersensitivity reactions to cephalosporins, penicillins,
and history ofallergies, particularly to drugs, before therapy is initiated.
Report onset of loose stools or diarrhea
Monitor for manifestations of hypersensitivity. Discontinue drug and report
their appearance promptly.
Monitor I&O rates and pattern: Especially important in severely ill patients
receiving high doses. Report any significant changes.
-
7/15/2019 Case Presentation
60/82
DRUG : NaHCO3
BRANDNAME : bakinSoda, Bell-Ans, Citrocarbonate, Neut, SodaMint
CLASSIFICATION : antiulcer agents, alkalinizing agent
DOSAGE : 1 tab//TID
DRUG ACTION : Sodium Bicarbonate acts as an alkalinizing agent by
releasing bicarbonate ions. Following oral administration of this medication, itreleases bicarbonate which is capable of neutralizing gastric acid.
INDICATION : > Management of metabolic acidosis
>Used to alkalinize urine and promote excretion of
certain drugs in over dosage situations.
>Used as an antacid
CONTRAINDICATION : Metabolic or respiratory alkalosisHypocalcemia, Excessive chloride loss. It is not recommended as an antidote
following ingestion of strong mineral acids. Patients on sodium restricted diet.
Renal failure, Severe abdominal pain of unknown cause especially if associated
with fever, Edema, Flatulence, Gastric distention, Metabolic alkalosis,
Hypernatremia, Hypocalcemia, Hypokalemia, Sodium and water retention,
Irritation at IV site, Tetany
-
7/15/2019 Case Presentation
61/82
NURSING RESPONSIBILITY: Assess the clients fluid balance throughout the therapy.
Symptoms of fluid overload should be reported such as hypertension,
edema, difficulty breathing or dyspnea, rales or crackles and frothy sputum.
Signs of acidosis should be assessed such as disorientation, headache,
weakness, dyspnea and hyperventilation.
Assess for alkalosis by monitoring the client for confusion, irritability,
paresthesia, tetany and altered breathing pattern.
Hypernatremia clinical manifestations should be assessed and monitored
which includes: edema, weight gain, hypertension, tachycardia, fever, flushedskin and mental irritability.
http://nursingcrib.com/case-study/hypertension/http://nursingcrib.com/case-study/hypertension/ -
7/15/2019 Case Presentation
62/82
Hypokalemia should also be assessed by monitoring signs and
symptoms such as: weakness, fatigue, U wave on ECG, arrhythmias,polyuria and polydipsia.
Monitor the clients serum calcium, sodium, potassium, bicarbonate
concentrations, serum osmolarity, acid-base balance and renal
function before and throughout the therapy. Tablets must be taken with a full glass of water.
For clients taking the medication as a treatment for peptic ulcers it
may be administered 1 and 3 hours after meals and at bedtime.
-
7/15/2019 Case Presentation
63/82
DRUG : CaCO3 Calcium CarbonateCLASSIFICATION : Class of calcium-containing preparations. Used as
dietary supplements.
DOSAGE : 500mg 1tab//TID
DRUG ACTION : Decreases total acid load of GI tract. Increase
esophageal sphincter tone.
INDICATION : Antacid, calcium supplement, osteoporosis.CONTRAINDICATION : Patients with Ca renal calculi or history of renal
calculi; hypercalcaemia; hypophosphataemia. Patients with suspected digoxin
toxicity. Constipation, flatulence; hypercalcaemia; metabolic alkalosis; milk-alkalisyndrome, tissue-calcification. Gastric hypersecretion and acid rebound (with
prolonged use).
NURSING RESPONSIBILITY:
Administer as antacid 1 hour after meal and at bed time
Administer as supplement 1 hrs after meal and at bed time
Advice patient to increase fluids to 2L unless contraindicated
-
7/15/2019 Case Presentation
64/82
DRUG : FeSO4 + Folic
CLASSIFICATION : Iron preparationDOSAGE : 1tab//OD
DRUG ACTION : Elevates the serum iron concentration on which then helps
to form high or trapped in the reticulo endothelial cells for storage and eventual
conversion to a usable form of iron.
INDICATION : Prevention and treatment of iron deficiency
anemia. Dietary supplement for iron.
CONTRAINDICATION : Hypersensitivity, Severe Hypotension, Dizziness, N & V,
Nasal Congestion, Dyspnea, Hypotension, CHF, MI,
Muscle cramps, Flushing
NURSING RESPONSIBILITY :
Advice patient to take medicine as prescribed.
Caution patient to make position changes slowly to minimize orthostatic hypotension.
Instruct patient to avoid concurrent use of alcohol or OTC medicine without consulting
the physician.
Advise patient to consult physician if irregular heartbeat, dyspnea, swelling of hands and
feet and hypotension occurs.
-
7/15/2019 Case Presentation
65/82
Inform patient that angina attacks may occur 30 min. after
administration due reflex tachycardia.
Encourage patient to comply with additional intervention for
hypertension like proper diet, regular exercise, and lifestyle
changes and stress management.
-
7/15/2019 Case Presentation
66/82
GENERIC NAME : Glipizide
BRANDNAME : GlucotrolCLASSIFICATION : It belongs to the sulfonylurea class of drugs
which also includes glimepiride (Amaryl), glyburide (Micronase, Diabeta),
tolbutamide (Orinase) and tolazamide (Tolinase).
DOSAGE : 2.5mg 1tab//OD
DRUG ACTION : Patients with type 2 diabetes have high
glucose (sugar) levels in their blood because the cells in their bodies are
resistant to the glucose-removing effect of the insulin, and the liver
produces too much glucose. In addition, in type 2 diabetes the pancreas is
unable to produce the increased amounts of insulin that are necessary toovercome the resistance. Glipizide reduces blood glucose by stimulating the
pancreas to produce more insulin
INDICATION : Glipizide is used together
with diet and exercise to reduce blood glucose in patients with type 2
diabetes.
http://www.medicinenet.com/script/main/art.asp?articlekey=755http://www.medicinenet.com/script/main/art.asp?articlekey=755 -
7/15/2019 Case Presentation
67/82
CONTRAINDICATION : Contraindicated with allergy to sulfonylureas;
diabetes with ketoacidosis, sole therapy of type 1 diabetes or diabetescomplicated by pregnancy, diabetes complicated by fever, severe infections,
severe trauma, major surgery, ketosis, acidosis, coma (insulin is indicated); type
1 diabetes, serious hepatic impairment, serious renal impairment. Side effects of
glipizide are possible, such as dizziness, diarrhea, and nervousness. In many
cases, these side effects are minor and easily treated by you or your healthcare
provider. However, some glipizide side effects should be reported to your
doctor, including chest pain, shortness of breath, or signs of an allergic reaction.
NURSING RESPONSIBILITY:
Give drug 30 min before breakfast; if severe GI upset occurs or more than
15 mg/day is required, dose may be divided and given before meals.Monitor urine or serum glucose levels frequently to determine drug
effectiveness and dosage.
C. Course in the ward
-
7/15/2019 Case Presentation
68/82
September 24, 2012 (7:45pm)Diagnostic Procedure: CBC, Na, K, Crea , BUN, RBS, U/A, CXR
Diet: Diabetic diet/ low fat, low salt
Exercise/Activity: Ambulatory
Treatment: (not yet handled)A Patient 51 yr. old female admitted to FMW under charity. Received by a
wheel chair; Endorsed by ER nurse and transferred to bed safely with
(+) generalized body weakness and (+) dyspnea. With on going IVF PNSS 1L
x 6 regulated as ordered. Treatment given D50-50 1 vial TIV
NaHCO3 or CaCO3 500 mg / tab TID. FeSO4 + FA 1 tab TID, Clonidine75 mg/tab PRN for BP 140 / 90mmHg it is administered by NOD.
-
7/15/2019 Case Presentation
69/82
September 25 2012 (12: 45pm)Diagnostic Procedure: CBG, BT s/p
Diet: Low Salt, Low Fat diet, Diabetic diet
Exercise/Activity: Ambulatory
Treatment: (not yet handled)
CBG monitored And done cross matched for BT. V/ S q4
monitored and recorded. Informed in ROD and referred
accordingly.
-
7/15/2019 Case Presentation
70/82
September 25 2012 (12: 45pm)Diagnostic Procedure: CBG
Diet: Low Salt, Low Fat diet, Diabetic diet
Exercise/Activity: Ambulatory
Treatment: (not yet handled)
With venoclysis PNSS 1l x 12 regulated as ordered.
-
7/15/2019 Case Presentation
71/82
September 27, 2012 (6:00pm)Diagnostic Procedure: Repeat U/A ,CBC TID , BT,
Diet: Low Salt, Low Fat diet, Diabetic diet
Exercise/Activity: Ambulatory
Treatment: (not yet handled)
Hooked and regulated IVF PNSS 1L x KVO. For BT 1U and
2 U PRBC properly typed and crossed matched. Repeated
CBC for 2ndU of BT. Each unit to run for 4 hours with 4
hours intervals. Pre-BT meds given prior to first unit of PRBC.paracetamol 500 mg/tab 1 tab PO and Diphenhydramine 25
mg/IV given by the NOD. Cefuroxime 500 mg/ 1 tab BID.
-
7/15/2019 Case Presentation
72/82
September 28, 2012Diagnostic Procedure: Hgb & Hct,
Diet: Low Salt, Low Fat diet, Diabetic diet
Exercise/Activity: Ambulatory
Treatment: (not yet handled)
With the same venoclysis regulated @ desired amount.
Administered plasil 10 mg TIV q 8 PRN for vomiting. Given
furosemide 80 mg TIV for BT. Done repeated UTZ.
-
7/15/2019 Case Presentation
73/82
September 29, 2012 (2:00pm)Diagnostic Procedure: Repeat CBC, Hct & Hgb
Diet: Low Salt, Low Fat diet, Diabetic diet
Exercise/Activity: Ambulatory
Treatment: (not yet handled)
Transfused 3 U PRBC with IVF PNSS 1l x KVO. After the
last PRBC has been transfused, CBC and Hgb & Hct
repeated. Treatment of NaHCO3 1 tab TIDAmlodipine 10 g/ 1 tab OD, Cefuroxime 500 mg/ 1 tab BID x 5
days , Glipizide 2.5 mg/ 1 tab OD CaCO3 500 mg/ 1 tab TID ,
FeSO4 + Folic 1 tab TID , given by the NOD.
-
7/15/2019 Case Presentation
74/82
September 30, 2012 (2:00pm)Diagnostic Procedure: ABG
Diet: Low Salt, Low Fat diet, Diabetic diet
Exercise/Activity: Ambulatory
Treatment: (not yet handled)
With the same venoclysis and regulated at the same ordered.
Treatment given is Amlodipine 10 g/ 1 tab OD, Cefuroxime
500 mg/ 1 tab BID x 5 days , NaHCO3 1 tab TID, Glipizide 2.5mg/ 1 tab OD CaCO3 500 mg/ 1 tab TID , FeSO4 + Folic 1
tab OD , given by the NOD.
-
7/15/2019 Case Presentation
75/82
October 1, 2012 (2:00pm)Diagnostic Procedure: Repeat CBC , Na , K , CBG, Urinalysis
Diet: Low Salt, Low Fat diet, Diabetic diet
Exercise/Activity: Ambulatory
Treatment: (not yet handled)
Client is conscious and coherent, on DM diet, low salt, low
fat. V/S taken and recorded. Due meds. given. I & O
measured and recorded.
-
7/15/2019 Case Presentation
76/82
EVALUATION
A. Summary
-
7/15/2019 Case Presentation
77/82
This study is about 51 year old women, who was admitted at theMandaluyong City Medical Center and was diagnosed with Chronic Kidney
Disease 2 to Diabetes Mellitus II related to Hypertension, Anemia 2 to
Nephropathy, her suspicious and concern about her condition led her to seek
for medical assistance together with her relatives. Her chief complaint
generalized body weakness. The patient examined by her attending physician.
Her diagnosis is worthy to study to find out how she end up on having thatkind of condition with her permission and blessing, We as a student nurse of
BSN level 4 (Old curriculum) Group 1A and 1B have decided to make a study
regarding her condition. Patients having this kind of condition serve as achallenge not just in the health care system but also in the field of nursing. More
than caring, caring is the essential component of nursing the best way to help
patient is to render a service that is honesty and full of compassion.This study also aims to widen the knowledge about the problem known in
the pathophysiology of the study, the appropriate interventions and
management for patient who are under this condition.
B C l i
-
7/15/2019 Case Presentation
78/82
This data was studied and gathered by the BSN 4 (Old Curriculum)
Group 1A and 1B to present a simple but yet concise information based on casestudy presentation. Nursing students were able to apply the proper nursing
action to the patient during assessment. Students were able to identify causes of
patient condition with the use of different taught of the group base on the
knowledge gain.
Students were able to formulate a scientific based pathophysiology that is
parallel with the patient condition from the risk factors to the disease process
manifesting signs and symptoms based on the physical assessment, medical
procedure and Laboratory results.
Actual and probable health problems to determine based from the highestto the least priority in order to prevent further complications caused by
conditions. Nursing care plans to classified using SMART, specific, measurable,
attainable, realistic, and time bounded. Nursing interventions was rendered to
give the proper care that client needed. As the Student nurses tried their best in
rendering the ideal and not just the ordinary care that can be seen in the hospital
now days.
B. Conclusion
-
7/15/2019 Case Presentation
79/82
We, the nursing students determined the actions, classifications,
indications, contraindications, side effects and adverse reaction and
most importantly the appropriate nursing considerations. We future
nurse need to know that in giving medications prioritizing the 10Rs is
needed to avoid medication error. We need to assure that obligation
to our patient is not just giving the medication and preparing it but to
know the essential classification of the drugs and its effectiveness that
soon will help to the patient for their fast recovery.
-
7/15/2019 Case Presentation
80/82
REFERENCES
-
7/15/2019 Case Presentation
81/82
MOSBYS Clinical Nursing (4th edition)
Saunders manual of Nursing Carehttp://www.Creativehealthinstitute.com
Kozier, B.,et al. (2007) Kozier & Erbs Fundamentals of Nursing: Concepts,
Process & Practice. (8th Edition, Vol. 1). Philippines.Pearson Education South
Asia PTE. LTD.
Marieb, E. (2006). Essentials of Human Anatomy and Physiology. (8th
Edition) Philippines. Pearson Education Inc., Prentice Hall Smeltzer, Suzanne C., et.al (2010). Medical-Surgical Nursing.(12th Edition).
Philadelphia. Wolters Kluwer Health & Lippincott Williams &Wilkins
Doenges, Marilynn, Moorhouse, M.F, & Alice Murr. (2008) Nurses Pocket
Guide:Diagnoses, Prioritized Interventions and Rationales. (11th Edition).
Taiwan.F.A.Davis CompanyBrunner and Suddharts, et al. (2008) Textbook of Medical-Surgical Nursing
(11th Edition) PhiladelpiaWolters Kluwer, Lippin Colt Williams and Wilkins.
MIMS.com (2010) Philippines Index of Medical Specialties (123rd Edition
2010)
http://www.scribd.com/ -
7/15/2019 Case Presentation
82/82