Modul Dyspneu

of 19
-
Upload
zarah-alifani-dzulhijjah -
Category
Documents
-
view
225 -
download
0
Transcript of Modul Dyspneu
-
7/27/2019 Modul Dyspneu
1/19
COMPLETE REPORT
MODUL Dypsnoe
Scenario 1
System Cardiovaskular
1A Group
Maria Ulfah (1102090049) Irfan Thamrin (1102090056) Rizki Rahmadhan (1102090063) Akhmad Edwin Indra Pratama (1102090064) Fakhrurrazi (1102090065) Muh. Fadly Aditya (1102090070)
Muhammad Assadul Malik (1102090072) Inna Mthmainnah Musa (1102090084) Andi Firman Mubarak (1102090088) Ainun Martoni (1102090093) Andi Fajar Apriani (1102090106) Dzul Ikram (1102090108) Zarah Alifani Dzulhijjah (1102090115) Sigit Dwi Pramono (1102090133) Andi Anugrah Suci (1102090142)Nur Sabriany Lihawa (1102090156)
FAKULTAS KEDOKTERAN
UNIVERSITAS MUSLIM INDONESIA
2010
-
7/27/2019 Modul Dyspneu
2/19
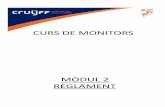
A. SCENARIOB. ANATOMY
Position
Left : linea medioclavicularis
sinistra
Right : linea parasternalis
dextraTop : intercostal II
Bottom : intercostal V
-
7/27/2019 Modul Dyspneu
3/19
Morphology
ApexA part of left ventricle
Position :
-intercostalis space 5 kiri
- 9 cm from left mediana line
- 2 fingers left medioclavicularis line in medial site
BasisTop : craniodorsal in the left orientationBuilt by:
- some parts of left and right atrium
- proximal part of large blood vessels
sternocostalis facies sinister diaphragmatica facies
Walls layers :
Epicardium (outher)
-
7/27/2019 Modul Dyspneu
4/19
Myocardium (middle) Endocardium (inner)
Chembers of the heart:
Right atriumThe right atrium receives the superior vena cava in its upper and posterior part, the
inferior vena cava and coronary sinus in its lower part, and the anterior cardiac vein
(draining much of the front of the heart) anteriorly.Running more or less vertically
downwards between the venae cavae is a distinct muscular ridge, the crista
terminalis (indicated on the outer surface of the atrium by a shallow groovethe
sulcus terminalis). This ridge separates the smooth-walled posterior part of the
atrium, derived from the sinus venosus, from the rough-walled anterior portion
which is prolonged into the auricular appendage and which is derived from the true
fetal\atrium. The openings of the inferior vena cava and the coronary sinus are
guarded by rudimentary valves; that of the inferior vena cava being continuous withthe annulus ovalis around the shallow depression on the atrial
Right ventricle
The right ventricle is joined to the right atrium by the way of the vertically disposed
tricuspid valve, and with the pulmonary trunk through the pulmonary valve. A
muscular ridge, the infundibuloventricular crest, between the atrioventricular and
pulmonary orifices, separates the inflow and outflow tracts of the ventricle. The
inner aspect of the inflow tract path is marked in the presence of a number of
irregular muscular elevations (trabeculaecarneae) from some of which the papillary
muscles project into the lumen of the ventricle and find attachment to the freeborders of the cusps of the tricuspid valve by way of the chordae tendineae. The
moderator band is a muscular bundle crossing the ventricular cavity from the
interventricular septum to the anterior wall and is of some importance since it
conveys the right branch of the atrioventricular bundle to the ventricular muscle.
The outflow tract of the ventricle or infundibulum is smooth-walled and is directed
upwards and to the right towards the pulmonary trunk. The pulmonary orifice is
guarded by thepulmonary valves, comprising three semilunar cusps.
Left atrium
The left atrium is rather smaller than the right but has somewhat thicker walls. On
the upper part of its posterior wall it presents the openings of the four pulmonary
veins and on its septal surface there is a shallow depression corresponding to the
fossa ovalis of the right atrium. As on the right side, the main part of the cavity is
smooth-walled but the surface of the auricle is marked by a number of ridges due to
the underlying pectinate muscles.
Left ventricle
The left ventricle communicates with the left atrium by way of the mitral (so-called
because it vaguely resembles a bishops mitre), which possessesa large anterior and
a smaller posterior cusp attached to papillarymuscles by chordae tendineae. With
the exception of the fibrous vestibule immediately below the aortic orifice, the wall
-
7/27/2019 Modul Dyspneu
5/19
of the left ventricle is marked by thick trabeculae carneae. The aortic orifice is
guarded by the three semilunar cusps of the aortic valve, immediately above which
are the dilated aortic sinuses. The mouths ofthe right and left coronary arteries are
seen in the anterior and left posteriorsinus respectively.
The conducting system of the heart
This consists of specialized cardiac muscle found in the sinuatrial node and in the
atrioventricular node and bundle. The heart-beat is initiated in the sinuatrial node (the
pacemaker of the heart), situated in the upper part of the crista terminalis just to the
right of the opening of the superior vena cava into the right atrium. From there the
cardiac impulse spreads the atrial septum immediately above the opening of the
coronary sinus. The impulse is then conducted to the ventricles by way of the
specialized tissue of the atrioventricular bundle (of His). This bundle divides at the
junction of the membranous and muscular parts of the interventricular septum into its
right and left branches which run immediately beneath the endocardium to activateall parts of the ventricular musculature
The blood supply to the heart
The hearts blood supply is derived from the right and left coronary arteries whose
main branches lie in the interventricular and atrioventricular grooves. The right
coronary arteryarises from the anterior aortic sinus and passes forwards between the
pulmonary trunk and the right atrium to descend in the right part of the
atrioventricular groove. At the inferior border of the heart it continues along the
atrioventricular groove to anastomose with the left coronary at the posterior
interventricular groove. It gives off a marginalbranch along the lower border of theheart and the posterior interventricular branch which runs forward in the inferior
interventricular groove and to anastomose near the apex of the heart with the
corresponding branch of the left coronary artery. The left coronary artery, which is
larger than the right, rises from the left posterior aortic sinus. Passing first behind and
then to the left of the pulmonary trunk, it reaches the left part of atrioventricular
groove in which it runs laterally round the left border of the heart as the circumflex
arteryto reach the posterior interatrial groove. Its most important branch, given off
about 2 cm from its origin, is the anterior interventricular artery which supplies the
anterior aspect of both ventricles and passes around the apex of the heart to
anastomose with the posterior interventricular branch of the right coronary. Note thatthe sinuatrial node is usually supplied by the right coronary artery, although the left
coronary artery takes over this duty in about one-third of subjects. Although
anastomoses occur between the terminations of the right and left coronary arteries,
these are usually inefficient. Thrombosis in one or other of these vessels leads to
death of the area of heart muscle supplied (a myocardial infarction).
The venous drainage of the heart
The bulk of the venous drainage of the heart is achieved by veins which accompany
the coronary arteries and which open into the right atrium. The rest of the blood
drains by means of small veins (venae cordis minimae) directly into the cardiac cavity.
-
7/27/2019 Modul Dyspneu
6/19
The coronary sinus lies in the posterior atrioventricular groove and opens into the
right atrium just to the left of the mouth of the inferior vena cava.
It receives:
1the great cardiac vein in the anterior interventricular groove;
2the middle cardiac vein the inferior interventricular groove;
3the small cardiac vein accompanying the marginal artery along the lower border
of the heart;
4the oblique vein descends obliquely on the posterior aspect of the left
atrium.
The anterior cardiac veins (up to three or four in number) cross the anterior
atrioventricular groove, drain much of the anterior surface of the heart and open
directly into the right atrium.
Nerve supply
The nerve supply of the heart is derived from the vagus (cardio-inhibitor) and the
cervical and upper 5 thoracic sympathetic ganglia (cardioaccelerator) by way ofsuperficial and deep cardiac plexuses.
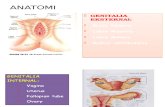
C. FISIOLOGIHeart Cycle
-
7/27/2019 Modul Dyspneu
7/19
The cardiac events that occur from the beginning of one heartbeat to the beginningof the next are called the cardiac cycle. Each cycle is initiated by spontaneous
generation of an action potential in the sinus node. This node is located in the
superior lateral wall of the right atrium near the opening of the superior vena cava,
and the action potential travels from here rapidly through both atria and then
through the A-V bundle into the ventricles. Because of this special arrangement of
the conducting system from the atria into the ventricles, there is a delay of more
than 0.1 second during passage of the cardiac impulse from the atria into the
ventricles.This allows the atria to contract ahead of ventricular contraction, thereby
pumping blood into the ventricles before the strong ventricular contraction
begins.Thus, the atria act as primer pumps for the ventricles, and the ventricles inturn provide the major source of power for moving blood through the bodys
vascular system. The cardiac cycle consists of a period of relaxation called diastole,
during which the heart fills with blood, followed by a period of contraction called
systole.
Function of the Atria as Primer Pumps
Blood normally flows continually from the great veins into the atria; about 80 per
cent of the blood flows directly through the atria into the ventricles even before the
atria contract. Then, atrial contraction usually causes an additional 20 per cent fillingof the ventricles. Therefore, the atria simply function as primer pumps that increase
-
7/27/2019 Modul Dyspneu
8/19
the ventricular pumping effectiveness as much as 20 per cent. However, the heart
can continue to operate under most conditions even without this extra 20 per cent
effectiveness because it normally has the capability of pumping 300 to 400 per cent
more blood than is required by the resting body.Therefore, when the atria fail to
function, the difference is unlikely to be noticed unless a person exercises; then
acute signs of heart failure occasionally develop, especially shortness of breath.
Function of the Ventricles as Pumps
Filling of the Ventricles. During ventricular systole, large amounts of blood
accumulate in the right and left atria because of the closed A-V valves. Therefore, as
soon as systole is over and the ventricular pressures fall again to their low diastolic
values, the moderately increased pressures that have developed in the atria during
ventricular systole immediately push the A-V valves open and allow blood to flow
rapidly into the ventricles, as shown by the rise of the left ventricularvolume curve inThis is called the period of rapid filling of the ventricles. The period of rapid filling
lasts for about the first third of diastole. During the middle third of diastole, only a
small amount of blood normally flows into the ventricles; this is blood that continues
to empty into the atria from the veins and passes through the atria directly into the
ventricles. During the last third of diastole, the atria contract and give an additional
thrust to the inflow of blood into the ventricles; this accounts for about 20 per cent
of the filling of the ventricles during each heart cycle.
Emptying of the Ventricles During Systole
Period of Isovolumic (Isometric) Contraction. Immediately after ventricularcontraction begins, the ventricular pressure rises abruptly. Then an additional 0.02 to
0.03 second is required for the ventricle to build up sufficient pressure to push the
semilunar (aortic and pulmonary) valves open against the pressures in the aorta and
pulmonary artery.Therefore, during this period, contraction is occurring in the
ventricles, but there is no emptying. This is called the period of isovolumic or
isometric contraction, meaning that tension is increasing in the muscle but little or
no shortening of the muscle fibers is occurring.
Period of Ejection. When the left ventricular pressure rises slightly above 80 mm Hg
(and the right ventricular pressure slightly above 8 mm Hg), the ventricular pressures
push the semilunar valves open. Immediately, blood begins to pour out of the
ventricles, with about 70 per cent of the blood emptying occurring during the first
third of the period of ejection and the remaining 30 per cent emptying during the
next two thirds. Therefore, the first third is called the period ofrapid ejection, and
the last two thirds, theperiod ofslow ejection.
Period of Isovolumic (Isometric) Relaxation. At the end of systole, ventricular
relaxation begins suddenly, allowing both the right and left intraventricular pressures
to decrease rapidly. The elevated pressures in the distended large arteries that have
just been filled with blood from the contracted ventricles immediately push blood
back toward the ventricles, which snaps the aortic and pulmonary valves closed. For
another 0.03 to 0.06 second, the ventricular muscle continues to relax, even though
-
7/27/2019 Modul Dyspneu
9/19
the ventricular volume does notchange, giving rise to the period of isovolumic or
isometricrelaxation. During this period, the intraventricular
pressures decrease rapidly back to their low diastolic levels. Then the A-V valves
open to begin a new cycle of ventricular pumping.
End-Diastolic Volume, End-Systolic Volume, and Stroke Volume
Output. During diastole, normal filling of the ventricles increases the volume of each
ventricle to about 110 to 120 milliliters. This volume is called the end-diastolic
volume. Then, as the ventricles empty during systole, the volume decreases about 70
milliliters, which is called the stroke volume output.The remaining volume
in each ventricle, about 40 to 50 milliliters, is called the end-systolic volume. The
fraction of the end-diastolic volume that is ejected is called the ejection fraction
usually equal to about 60 per cent. When the heart contracts strongly, the end-
systolic volume can be decreased to as little as 10 to 20 milliliters. Conversely, when
large amounts of blood flow into the ventricles during diastole, the ventricular end
diastolic volumes can become as great as 150 to 180 milliliters in the healthy heart.
By both increasing the end-diastolic volume and decreasing the end-systolic volume,the stroke volume output can be increased to more than double normal.
Function of the Valves
Atrioventricular Valves. The A-V valves (the tricuspid and mitral valves) prevent
backflow of blood from the ventricles to the atria during systole, and the semilunar
valves (the aortic andpulmonary arteryvalves) prevent backflow from the aorta and
pulmonary arteries into the ventricles during diastole. These valves, for the left
ventricle, close and open passively. That is, they close when a backward pressure
gradient pushes blood backward, and they open when a forward pressure gradient
forces blood in the forward direction. For anatomical reasons, the thin, filmy A-Vvalves require almost no backflow to cause closure, whereas the much heavier
semilunar valves require rather rapid backflow for a few milliseconds.
Aortic and Pulmonary Artery Valves.
The aortic and pulmonary artery semilunar valves function quite differently from the
A-V valves. First, the high pressures in the arteries at the end of systole cause the
semilunar valves to snap to the closed position, in contrast to the much softer
closure of the A-V valves. Second, because of smaller openings, the velocity of blood
ejection through the aortic and pulmonary valves is far greater than that through the
much larger A-V valves. Also, because of the rapid closure and rapid ejection, the
edges of the aortic and pulmonary valves are subjected to much greater mechanicalabrasion than are the A-V valves. Finally, the A-V valves are supported by the
chordae tendineae, which is not true for the semilunarvalves. It is obvious from the
anatomy of the aortic and pulmonary valves that they must be constructed with an
especially strong yet very pliable fibrous tissue base to withstand the extra physical
stresses.
-
7/27/2019 Modul Dyspneu
10/19
Conducting System
Origin and Spread of Excitation within the Heart
The heart consists of two kinds of muscle cells: contractile cells and conducting cells.
Contractile cells constitute the majority of atrial and ventricular tissues and are the
working cells of the heart. Action potentials in contractile cells lead to contraction and
generation of force or pressure. Conducting cells constitute the tissues of the SA node,the atrial internodal tracts, the AV node, the bundle of His, and the Purkinje system.
Conducting cells are specialized muscle cells that do not contribute significantly to
generation of force; instead, they function to rapidly spread action potentials over the
entire myocardium. Another feature of the specialized conducting tissues is their
capacity to generate action potentials spontaneously. Except for the SA node, however,
this capacity normally is suppressed.
The action potential spreads throughout the myocardium in the following sequence:
1. SA node. Normally, the action potential of the heart is initiated in the specializedtissue of the SA node, which serves as the pacemaker. After the action potential isinitiated in the SA node, there is a very specific sequence and timing for the
-
7/27/2019 Modul Dyspneu
11/19
conduction of action potentials to the rest of the heart.
2. Atrial internodal tracts and atria. The action potential spreads from the SA node tothe right and left atria via the atrial internodal tracts. Simultaneously, the action
potential is conducted to the AV node.
3. AV node. Conduction velocity through the AV node is considerably slower than inthe other cardiac tissues. Slow conduction through the AV node ensures that theventricles have sufficient time to fill with blood before they are activated and contract.
Increases in conduction velocity of the AV node can lead to decreased ventricular
filling and decreased stroke volume and cardiac output.
4. Bundle of His, Purkinje system, and ventricles. From the AV node, the actionpotential enters the specialized conducting system of the ventricles. The action
potential is first conducted to the bundle of His through the common bundle. It then
invades the left and right bundle branches and then the smaller bundles of the Purkinje
system. Conduction through the His-Purkinje system is extremely fast, and it rapidly
distributes the action potential to the ventricles. The action potential also spreads from
one ventricular muscle cell to the next, via low-resistance pathways between the cells.
Rapid conduction of the action potential throughout the ventricles is essential andallows for efficient contraction and ejection of blood.
Action Potential of the Heart
1. Phase 0, upstroke. In ventricular, atrial, and Purkinje fibers, the action potential
-
7/27/2019 Modul Dyspneu
12/19
begins with a phase of rapid depolarization, called the upstroke. As in nerve and
skeletal muscle, the upstroke is caused by a transient increase in Na+
conductance
(gNa), produced by depolarization-induced opening of activation gates on the Na+
channels. When gNa increases, there is an inward Na+
current (influx of Na+
into the
cell), or INa, which drives the membrane potential toward the Na+
equilibrium
potential of approximately +65 mV. The membrane potential does not quite reach
the Na+
equilibrium potential because, as in nerve, the inactivation gates on the Na+
channels close in response to depolarization (albeit more slowly than the activation
gates open). Thus, the Na+
channels open briefly and then close. At the peak of the
upstroke, the membrane potential is depolarized to a value of about +20 mV.
The rate of rise of the upstroke is called dV/dT. dV/dT is the rate of change of the
membrane potential as a function of time, and its units are volts per second (V/sec).
dV/dT varies, depending on the value of the resting membrane potential. This
dependence is called the responsiveness relationship. Thus, dV/dT is greatest (the
rate of rise of the upstroke is fastest) when the resting membrane potential is most
negative, or hyperpolarized (e.g., -90 mV), and dV/dT is lowest (the rate of rise of theupstroke is slowest) when the resting membrane potential is less negative, or
depolarized (e.g., -60 mV). This correlation is based on the relationship between
membrane potential and the position of the inactivation gates on the Na+
channel
When the resting membrane potential is relatively hyperpolarized (e.g., -90 mV), the
voltage-dependent inactivation gates are open, and many Na+
channels are available
for the upstroke. When the resting membrane potential is relatively depolarized
(e.g., -60 mV), the inactivation gates on the Na+
channels tend to be closed, and
fewer Na+
channels are available to open during the upstroke. dV/dT also correlates
with the size of the inward current (i.e., in ventricular, atrial, and Purkinje fibers, the
size of the inward Na+
current).2. Phase 2, plateau. During the plateau, there is a long period (150 to 200 msec) of
relatively stable, depolarized membrane potential, particularly in ventricular and
Purkinje fibers. (In atrial fibers, the plateau is shorter than in ventricular fibers.)
Recall that for the membrane potential to be stable, inward and outward currents
must be equal such that there is no net current flow across the membrane.
How is such a balance of inward and outward currents achieved during the plateau?
There is an increase in Ca2+
conductance (gCa), which results in an inward Ca2+
current. Inward Ca2+
current is also called slow inward current, reflecting the slower
kinetics of these channels (compared with the fast Na+
channels of the upstroke).
The Ca2+
channels that open during the plateau are L-type channels ("L," for long-lasting) and are inhibited by the Ca
2+channel blockers nifedipine , diltiazem, and
verapamil. To balance the inward Ca2+
current, there is an outward K+
current,
driven by the electrochemical driving force on K+
ions (as described for phase 1).
Thus, during the plateau, the inward Ca2+
current is balanced by the outward K+
current, the net current is zero, and the membrane potential remains at a stable
depolarized value.The significance of the inward Ca2+
current extends beyond its
effect on membrane potential. This Ca2+
entry during the plateau of the action
potential initiates the release of more Ca2+
from intracellular stores for excitation-
contraction coupling. This process of so-called Ca2+
-induced Ca2+
release will be
discussed in the section on cardiac muscle contraction.3. Phase 3, repolarization. Repolarization begins gradually at the end of phase 2, and
-
7/27/2019 Modul Dyspneu
13/19
then there is rapid repolarization to the resting membrane potential during phase 3.
Recall that repolarization is produced when outward currents are greater than
inward currents. During phase 3, repolarization results from a combination of a
decrease in gCa (previously increased during the plateau) and an increase in g K (to
even higher levels than at rest). The reduction in gCa results in a decrease in the
inward Ca2+ current, and the increase in gK results in an increase in the outward K+
current (IK), with K+
moving down a steep electrochemical gradient (as described for
phase 1). At the end of phase 3, the outward K+
current is reduced because
repolarization brings the membrane potential closer to the K+
equilibrium potential,
thus decreasing the driving force on K+.
CIRCUITRY
The left heart and right heart have different functions. The left heart and the
systemic arteries, capillaries, and veins are collectively called the systemic
circulation. The left ventricle pumps blood to all organs of the body except the lungs.
The right heart and the pulmonary arteries, capillaries, and veins are collectively
called the pulmonary circulation. The right ventricle pumps blood to the lungs. The
-
7/27/2019 Modul Dyspneu
14/19
left heart and right heart function in series so that blood is pumped sequentially
from the left heart to the systemic circulation, to the right heart, to the pulmonary
circulation, and then back to the left. The rate at which blood is pumped from either
ventricle is called the cardiac output. Because the two sides of the heart operate in
series, the cardiac output of the left ventricle equals the cardiac output of the rightventricle in the steady state. The rate at which blood is returned to the atria from
the veins is called the venous return. Again, because the left heart and the right
heart operate in series, venous return to the left heart equals venous return to the
right heart in the steady state. Finally, in the steady state, cardiac output from the
heart equals venous return to the heart.
Step of the circuicity:
1. Oxygenated blood fills the left ventricle. Blood that has been oxygenated in thelungs returns to the left atrium via the pulmonary vein. This blood then flows fromthe left atrium to the left ventricle through the mitral valve (the AV valve of the left
heart).
2. Blood is ejected from the left ventricle into the aorta. Blood leaves the left ventriclethrough the aortic valve (the semilunar valve of the left side of the heart), which is
located between the left ventricle and the aorta. When the left ventricle contracts,
the pressure in the ventricle increases, causing the aortic valve to open and blood to
be ejected forcefully into the aorta. (As noted previously, the amount of blood
ejected from the left ventricle per unit time is called the cardiac output.) Blood then
flows through the arterial system, driven by the pressure created by contraction ofthe left ventricle.
3. Cardiac output is distributed among various organs. The total cardiac output of theleft heart is distributed among the organ systems via sets of parallel arteries. Thus,
simultaneously, 15% of the cardiac output is delivered to the brain via the cerebral
arteries, 5% is delivered to the heart via the coronary arteries, 25% is delivered to
the kidneys via the renal arteries, and so forth. Given this parallel arrangement of
the organ systems, it follows that the total systemic blood flow must equal the
cardiac output.
The percentage distribution of cardiac output among the various organ systems is
not fixed, however. For example, during strenuous exercise, the percentage of thecardiac output going to skeletal muscle increases, compared with the percentage at
rest. There are three major mechanisms for achieving such a change in blood flow to
an organ system. In the firstmechanism, the cardiac output remains constant, but
the blood flow is redistributed among the organ systems by the selective alteration
of arteriolar resistance. In this scenario, blood flow to one organ can be increased at
the expense of blood flow to other organs. In the second mechanism, the cardiac
output increases or decreases, but the percentage distribution of blood flow among
the organ systems is kept constant. Finally, in a thirdmechanism, a combination of
the first two mechanisms occurs in which both cardiac output and the percentage
distribution of blood flow are altered. This third mechanism is used, for example, in
the response to strenuous exercise: Blood flow to skeletal muscle increases to meet
-
7/27/2019 Modul Dyspneu
15/19
the increased metabolic demand by a combination of increased cardiac output and
increased percentage distribution to skeletal muscle.
4. Blood flow from the organs is collected in the veins. The blood leaving the organs isvenous blood and contains waste products from metabolism, such as carbon dioxide
(CO2). This mixed venous blood is collected in veins of increasing size and finally in
the largest vein, the vena cava. The vena cava carries blood to the right heart.
5. Venous return to the right atrium. Because the pressure in the vena cava is higherthan in the right atrium, the right atrium fills with blood, the venous return. In the
steady state, venous return to the right atrium equals cardiac output from the left
ventricle.
6. Mixed venous blood fills the right ventricle. Mixed venous blood flows from theright atrium to the right ventricle through the AV valve in the right heart, the
tricuspid valve.
7. Blood is ejected from the right ventricle into the pulmonary artery. When the rightventricle contracts, blood is ejected through the pulmonic valve (the semilunar valve
of the right side of the heart) into the pulmonary artery, which carries blood to thelungs. Note that the cardiac output ejected from the right ventricle is identical to the
cardiac output that was ejected from the left ventricle. In the capillary beds of the
lungs, oxygen (O2) is added to the blood from alveolar gas, and CO2 is removed from
the blood and added to the alveolar gas. Thus, the blood leaving the lungs has more
O2 and less CO2 than the blood that entered the lungs.
8. Blood flow from the lungs is returned to the heart via the pulmonary vein. Oxygenated blood is returned to the left atrium via the pulmonary vein to begin a
new cycle.
D. HISTOLOGYArteries
General considerations_ Carry blood away from the heart and toward capillary beds
_ Have thicker walls and smaller lumens than veins of similar size
_ Tunica media is the predominate tunic.
_ Cross-sectional outlines are more circular in arteries than in veins.
Types Elastic (large) arteries (aorta, pulmonary arteries)
_ Internal elastic lamina is present but difficult to distinguish.
_ Tunica media is composed of fenestrated sheets of elastic tissue (elastic lamellae)
and smooth muscle.
_ Passively maintain blood pressure by distension and recoil of the elastic sheets
Muscular (medium, distributing)_ Tunica media is composed of smooth muscle.
_ Internal elastic lamina. Single, fenestrated, elastic sheet; lies internal to the
smooth muscle of the tunica media.
_ External elastic laminae. Multiple elastic sheets; lie external to the smooth
muscle of the tunica media
-
7/27/2019 Modul Dyspneu
16/19
_ Regulate blood pressure and blood distribution by contraction and relaxation of
smooth muscle in the tunica media
Small arteries and arterioles_ Less than 200 microns in diameter
_ Small arteries have an internal elastic lamina and up to eight layers of smooth
muscle in the tunica media.
_ Arterioles usually lack an internal elastic lamina and have one to two layers of
smooth muscle in the tunica media.
_ Arterioles are the vessels that regulate blood pressure and deliver blood under
low pressure to capillaries.
Capillaries
General considerations_ Function to exchange oxygen and carbon dioxide and nutrients and metabolic
wastes between blood and cells
_ Lumen is approximately 8 microns in diameter, thus only largeenough for RBCsto move through in a single row.
_ Composed of the endothelium (simple squamous epithelium) and its
underlying basal lamina
TypesContinuous capillaries
_ Most common
_ Endothelium is continuous (i.e., has no pores)
Fenestrated capillaries_ Endothelium contains pores that may or may not be spanned by a
diaphragm. If present, the diaphragm is thinner than two apposed plasma
membranes.
_ Pores with diaphragms are common in capillaries in the endocrine organs
and portions of the digestive tract. Pores lacking diaphragms are uniquely
present in the glomerular capillaries of the kidney.
_ Pores facilitate diffusion across the endothelium
Discontinuous sinusoidal capillaries_ Larger diameter and slower blood flow than in other capillaries
_ Endothelium has large pores that are not closed by a diaphragm.
_ Gaps are present between adjacent endothelial cells.
_ Partial or no basal lamina present.
_ Prominent in spleen and liver
-
7/27/2019 Modul Dyspneu
17/19
Veins General considerations
_ Return blood from capillary beds to the heart
_ Have thinner walls and larger lumens than arteries of similar size; cross-
sectional outlines are more irregular
_ Tunica adventitia is the predominate tunic.
_ Larger veins possess valves, that are extensions of the tunica intima
that serve to prevent back-flow of blood.
TypesVenules and small veins_ Tunica media is absent in venules. Smooth muscle fibers appear in the tunica
media as venules progress to small veins.
_ High endothelial venules. Venules in which the endothelium is simple
cuboidal; facilitate movement of cells from the blood into the surrounding
tissues (diapedesis). This type of venule is found in many of the lymphatic
tissues.
Medium veins. Smooth muscle forms a more definitive and continuous tunicamedia; most named veins are in this category
Large veins, includes superior and inferior venae cavae; have well-developed,longitudinally oriented smooth muscle in the tunica adventitia in addition tothe smooth muscle in the tunica media.
-
7/27/2019 Modul Dyspneu
18/19
Heart
Develops by a vessel folding back on itself to produce four chambers
in the adult. Two upper chambers, atria (singular, atrium), receiveblood from the body and lungs; two ventricles pump blood out of the
heart.
Impulse conducting system. Formed of specialized cardiac muscle
fibers that initiate and coordinate the contraction of the heart
_ Sinoatrial (SA) node in the right atrium is the electricalpacemakerthat initiates
the impuse.
_ Fibers spread the impulse throughout the atria as well as transferring it to the
atrioventricular node.
_ The atrioventricular (AV) node is located in the interatrial septum.
_ An atrioventricular bundle extends from the AV node in the septummembranaceum and bifurcates into right and left bundle branches that lie
beneath the endocardium on both sides of the interventricular septum.
_ Purkinje fibers, modified, enlarged cardiac muscle fibers leave the bundle
branches to innervate the myocardium.
Tunics
Endocardium_ Homologous to the tunica intima of vessels Consists of an endothelium
(simple squamous epithelium) plus underlying connective tissue
_ Cardiac valves. Folds of the endocardium
_ Semilunar valves at the base of the aortic and pulmonary trunks preventbackflow of blood into the heart.
-
7/27/2019 Modul Dyspneu
19/19
_ Atrioventricular valves (bicuspid and tricuspid) prevent backflow of blood
from the ventricles into the atria.
Myocardium_ Composed of cardiac muscle
_ Fibers insert on components of the cardiac skeleton.
_ Thickest layer of the heart
_ Variation in thickness depends on the function of each chamber; thicker in
ventricles than atria and thicker in left ventricle than right ventricle
Epicardium (visceral pericardium)_ Serous membrane on the surface of the myocardium
_ Consists of a simple squamous epithelium and a loose connective tissue, with
adipocytes, adjacent to the myocardium.
_ Coronary blood vessels are located in the connective tissue.
Cardiac skeleton. Thickened regions of dense connective tissue thatprovide support for heart valves and serve as insertion of cardiac
muscle fibers
_ Annuli fibrosi are connective tissue rings that surround and stabilize each
valve.
_ Septum membranceum is a connective tissue partition forming the upper
portion of the interventricular septum; this connective tissue also separates
the left ventricle from the right atrium.
E. PATOFISIOLOGIF. DD