16. Enfermedad Inflamatoria Intestinal

of 13
-
Upload
hugo-gonzalez -
Category
Documents
-
view
220 -
download
0
Transcript of 16. Enfermedad Inflamatoria Intestinal
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
1/13
MEDICAL PROGRESS
N Engl J Med, Vol. 347, No. 6 August 8, 2002 www.nejm.org
417
Review Article
Medical Progress
I
NFLAMMATORY
B
OWEL
D
ISEASE
D
ANIEL
K. P
ODOLSKY
, M.D.
From the Gastrointestinal Unit and the Center for the Study of Inflam-matory Bowel Disease, Massachusetts General Hospital and Harvard Med-ical School, Boston.
N the decades since the major forms of idiopath-ic inflammatory bowel disease were defined onthe basis of clinical manifestations, investigators
have been challenged to identify the fundamental
pathophysiologic processes underlying these enigmaticdisorders, and clinicians have struggled to provide ef-fective therapy for the often dismaying clinical man-ifestations. Clinical experience has led to the generallyaccepted notion that Crohns disease and ulcerativecolitis are distinct, if not discrete, entities. However,
whether these are fundamentally different diseases orpart of a mechanistic continuum remains an unan-swered question, with both conceptual and practicalmanagement implications.
ETIOLOGY AND PATHOPHYSIOLOGY
Inflammatory bowel disease is thought to resultfrom inappropriate and ongoing activation of the mu-
cosal immune system driven by the presence of normalluminal flora. This aberrant response is most likelyfacilitated by defects in both the barrier function ofthe intestinal epithelium and the mucosal immunesystem.
Genetic Factors
Several clinical observations suggest that geneticfactors contribute to susceptibility to inflammatorybowel disease (Table 1). These include wide variationsin the incidence and prevalence of Crohns diseaseand ulcerative colitis among different populations, co-segregation of inflammatory bowel disease in rare kin-dreds with a variety of uncommon genetic disorders,and more directly, familial aggregation of inflamma-tory bowel disease. Multiple studies have suggestedthat first-degree relatives of an affected patient havea risk of inflammatory bowel disease that is 4 to 20times as high as that among the background popu-
I
lation; the absolute risk of inflammatory bowel dis-ease is approximately 7 percent among first-degreefamily members.
1,2
A substantially higher rate of dis-ease concordance has been observed in monozygotictwins than in dizygotic twins, especially in those withCrohns disease.
1
Collectively, these findings lend compelling sup-port to the inference that susceptibility is inheritedand that the genetic contribution to the developmentof disease is more important in Crohns disease thanin ulcerative colitis. However, the absence of simplemendelian inheritance suggests that multiple geneproducts contribute to a persons risk of inflammatorybowel disease.
Over the past 15 years, a wide variety of candidategenes have been studied. Most associations identifiedbetween specific candidate genes, including major-histocompatibility-complex loci, and inflammatorybowel disease have not been reproducible, have notshed new light on pathogenesis, or have not facilitateddiagnosis.
3-5
However, substantial progress has nowbeen made with use of the less biased approach of ge-nome-wide screening with microsatellite DNA mark-ers. Screening of DNA from members of kindreds
with multiple affected members identified an area ofapparent linkage on chromosome 16 among kindreds
with Crohns disease but not those with ulcerativecolitis.
6
Although the relative risk associated withthis putative locus, designated IBD1,
was small, theassociation was replicated in all but one independentstudy. These studies also provided evidence that in-flammatory bowel disease is linked to several othergenomic regions.
7-10
Most of these sites are equallylinked to both major forms of inflammatory boweldisease, suggesting that Crohns disease and ulcerativecolitis share many common genetic and, therefore,mechanistic features.
Detailed mapping of chromosome 16 has recentlyresulted in the identification of a gene responsible,at least in part, for this linkage.
11,12
This gene encodesa cytoplasmic protein designated NOD2 (also referredto as CARD 15 [caspase activation and recruitmentdomain]), which is expressed in macrophages and mayserve as a so-called pattern-recognition receptor forbacterial lipopolysaccharide, perhaps regulating nu-clear factor-
k
B activation and macrophage apoptosis.European and North American patients with Crohnsdisease, including those without a family history ofinflammatory bowel disease, are more likely to have
variants of NOD2 than are persons without Crohnsdisease. Paradoxically, these NOD2 variants appear
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
2/13
418
N Engl J Med, Vol. 347, No. 6
August 8, 2002
www.nejm.org
The New England Journal of Medic ine
to result in reduced macrophage activation of nucle-ar factor-
k
B in response to lipopolysaccharide. Per-sons who are homozygous for variant NOD2 mayhave a 20-fold or more increase in susceptibility toCrohns disease, with a particular predilection for il-eal disease.
13-15
Heterozygotes are also at increasedrisk. However, fewer than 20 percent of patients withCrohns disease are homozygous for these NOD2
variants. A putative locus associated with early-onsetCrohns disease appears to be present on chromo-some 5 in the vicinity of genes encoding a varietyof cytokine receptors.
16
Environmental Precipitants and Disease Cofactors
Whatever part genetic loci play in conferring sus-ceptibility to inflammatory bowel disease, studies ofidentical twins (in which only 45 percent of pairsof identical twins are concordant for Crohns disease)make it clear that the development of disease dependson additional factors. Among myriad factors studied,the most consistent are the use of nonsteroidal anti-
inflammatory drugs, which can lead to disease flares,possibly related to an altered intestinal barrier, andearly appendectomy, which is associated with a re-duced incidence of ulcerative colitis.
17,18
Smoking maymodify the phenotype; it protects against ulcerativecolitis but increases the risk of Crohns disease.
19,20
Accumulating evidence suggests that the luminalflora is a requisite and perhaps central factor in thedevelopment of inflammatory bowel disease. This in-ference is supported by studies in murine models ofcolitis established through genetic manipulation andreinforced by a variety of clinical observations in pa-tients (Table 2). For example, the development ofspontaneous colitis in rats and mice appears to re-quire the presence of luminal flora; colitis does notoccur in any of several mutant strains when they aremaintained in a germ-free environment, but it devel-ops rapidly when these mice are colonized by com-mensal bacteria.
21,22
Studies of murine models resonate with clinicalexperience. Broad-spectrum antibiotics and probiot-
*Although HLA antigens have been studied extensively, the resulting associations have been vari-ably reproducible.
The IBD1 locus encodes NOD2(also designated CARD 15
).
T
ABLE
1. E
VIDENCE
OF
G
ENETICALLY
D
ETERMINED
S
USCEPTIBILITY
TO
I
NFLAMMATORY
B
OWEL
D
ISEASE
.
Human studies
The prevalence varies among different populations.
The risk is increased among first-degree relatives of affected patients.
There is greater concordance among monozygotic than dizygotic twins.
Syndromes resembling inflammatory bowel disease cosegregate in families with rare genetic disorders(e.g., glycogen storage disease type IB, WiskottAldrich syndrome, HermanskyPudlaksyndrome).
There is usually concordance in the type and site of disease among members of families with multipleaffected members.
Numerous candidate genes have been identified with putative allelic associations with inflammatorybowel disease, including genes that encode HLA antigens,* tumor necrosis factor (promoter-sequence polymorphisms), mucin, interleukin-10, interleukin-1receptor antagonist, intercellu-lar adhesion molecule 1, kinin B1, inhibitor ofk
B kinase, and natural-resistanceassociated mac-rophage protein 2.
Screening with microsatellite DNA markers has identified genomic linkage on chromosomes 16(
IBD1
locus; linkage with Crohns disease only), 3, 5, 7, 12 (linkage with ulcerative colitis only),18, and 19 and the X chromosome.
Animal studies
Experiments in rodent lines with genetic alterations conferred by transgenic or gene-deletiontechniques led to the heritable development of inflammatory bowel diseaselike colitis.
Transgenic overexpression or deletion of a single gene by means of homologous recombination canlead to inflammatory bowel disease.
The phenotype resulting from a single genetic alteration is modulated by other genetic loci (e.g., theseverity and age at onset vary depending on the background strain).
No single gene is uniquely associated with the development of inflammatory bowel disease; colitisresults from alterations in a subgroup of genes that encode proteins involved in either the epi-thelial mucosal barrier or the mucosal immune response.
Genetic alteration confers susceptibility but is not sufficient to result in disease (e.g., mutant murinelines maintained in a germ-free state do not manifest inflammatory bowel disease).
Commensal bacteria are required for the development of inflammatory bowel disease in susceptiblehosts.
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
3/13
MEDICAL PROGRESS
N Engl J Med, Vol. 347, No. 6
August 8, 2002
www.nejm.org
419
ics have proven clinical efficacy in specific subgroupsof patients. Studies have demonstrated the presenceof an increased number of surface-adherent and intra-cellular bacteria in the colonic epithelium of patients
with inflammatory bowel disease.
23,24
Such observa-tions underscore the importance of further definingthe mechanisms of interaction between the normalmucosa and luminal microflora and their alterationin association with inflammatory bowel disease.
Immune Response and Inflammatory Pathways
The aggregate effect of genetic, environmental, andother processes is the sustained activation of mucosalimmune responses (Fig. 1). It remains unclear whetherthe immune system is activated as a result of an intrin-
sic defect (either constitutive activation or the failureof down-regulatory mechanisms) or because of con-tinued stimulation resulting from a change in theepithelial mucosal barrier.
25,26
Substantial progress has been made in character-izing immune-cell populations and inflammatory me-diators in patients with inflammatory bowel diseaseand murine models.
22,27
There is reasonable consensusthat the mucosa of patients with established Crohnsdisease is dominated by CD4+ lymphocytes with atype 1 helper-T-cell (Th1) phenotype, characterizedby the production of interferon-
g
and interleukin-2.In contrast, the mucosa in patients with ulcerative coli-tis may be dominated by CD4+ lymphocytes with anatypical type 2 helper-T-cell (Th2) phenotype, char-
T
ABLE
2. K
EY
F
EATURES
OF
M
AJOR
F
ORMS
OF
I
NFLAMMATORY
B
OWEL
D
ISEASE
.
F
EATURE
U
LCERATIVE
C
OLITIS
C
ROHN
S
D
ISEASE
Clinical features
FeverAbdominal painDiarrheaRectal bleeding
Weight lossSigns of malnutritionPerianal disease
Abdominal massGrowth failure in children and adolescents
Fairly commonVariesVery commonVery commonFairly commonFairly common
AbsentAbsentOccasional
CommonCommonFairly commonFairly commonCommonCommonFairly commonCommonCommon
Site
ColonIleumJejunumStomach or duodenumEsophagus
ExclusivelyNeverNeverNeverNever
2/3 of patients2/3 of patientsInfrequentInfrequentInfrequent
Intestinal complications
Stricture
FistulasToxic megacolonPerforationCancer
Unknown
AbsentUnknownUnknownCommon
Common
Fairly commonAbsentUncommonFairly common
Endoscopic findings
FriabilityAphthous and linear ulcersCobblestone appearancePseudopolypsRectal involvement
Very commonAbsentAbsentCommon
Very common
Fairly commonCommonCommonFairly commonFairly common
Radiologic findings
Distribution
Ulceration
FissuresStrictures or fistulas
Ileal involvement
Continuous
Fine, superficial
AbsentRare
Dilated (backwash ileitis)
Discontinuous, seg-mented
Deep, with submucosalextension
CommonCommon
Narrowed, nodular
Laboratory findings
Perinuclear-staining antineutrophilcytoplasmic antibodies
Anti
Saccharomyces cerevisiaeantibodies
70% of patients
Occasional
Occasional
50% of patients
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
4/13
420
N Engl J Med, Vol. 347, No. 6
August 8, 2002
www.nejm.org
The New England Journal of Medic ine
acterized by the production of transforming growthfactorb
(TGF-
b
) and interleukin-5 but not interleu-kin-4.
28
In murine models, the effects of the activationof Th1 cells may be enhanced by the concomitantdecrease in subgroups of suppressor T cells, variouslydesignated Th3 or Tr1, which produce the down-reg-ulatory cytokines interleukin-10 and TGF-
b
.
29
In-depth characterization of murine lines suggests
that the stereotypical Th1 cytokines activate macro-phages, which in turn, produce interleukin-12, inter-leukin-18, and macrophage migration inhibitor factorand thus further stimulate Th1 in a self-sustainingcycle. Just as important, activated macrophages pro-duce a potent mix of broadly active inflammatorycytokines, including tumor necrosis factor (TNF),interleukin-1, and interleukin-6.
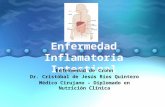
Figure 1.
Pathogenesis of Inflammatory Bowel Disease.
Normal epithelium, with its highly evolved tight junctions and products of goblet-cell populations, most notably trefoil peptides
and mucin glycoproteins, provides an effective barrier against luminal agents. The integrity of the barrier may be compromised bygenetic variations in key molecular determinants, a diminished reparative response to injury, or exogenous agents, such as non-steroidal antiinflammatory drugs. Chronic, recurrent intestinal inflammation appears to result from stimulation of the mucosal im-
mune system by products of commensal bacteria in the lumen. Antigens from dietary sources may also contribute. Stimulation
may occur as a result of the penetration of bacterial products through the mucosal barrier, leading to their direct interaction withimmune cells, especially dendritic cells and lymphocyte populations, to promote a classic adaptive immune response. Alternatively,
bacterial products may stimulate the surface epithelium, possibly through receptors that are components of the innate immune-response system; the epithelium can, in turn, produce cytokines and chemokines that recruit and activate mucosal immune cells.Activation of classic antigen-presenting cells, such as dendritic cells, or direct stimulation through pattern-recognition receptors
promotes the differentiation of type 1 helper T cells (Th1) in patients with Crohns disease (shown here) or, possibly, atypical type 2helper T cells in patients with ulcerative colitis. The stereotypical products of Th1 promote a self-sustaining cycle of activation withmacrophages. In addition to producing the key cytokines that stimulate Th1 (interleukin-12, interleukin-18, and macrophage migra-
tion inhibitor factor), macrophages produce a mix of inflammatory cytokines, including interleukin-1, interleukin-6, and most nota-bly tumor necrosis factor, which target a broad variety of other types of cells. The latter include endothelial cells, which then facil-itate the recruitment of leukocytes to the mucosa from the vascular space, as well as fibroblasts and epithelium, modulating their
functional properties. Most important, these functions may be altered either by genetically determined variants, as exemplified bygerm-line mutations in the gene encoding NOD2, the product of the IBD1 locus, in some patients with Crohns disease, or by envi-ronmental factors.
Epithelial
barrier
Normal epithelium
Tumor necrosis factor
Interleukin-1
Interleukin-6
Interferon-
Macrophagemigration inhibitorfactor
Interleukin-12
Interleukin-18
Macrophage
Bacteria Type 1 helperT cell
Antigen-presenting
cell
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
5/13
MEDICAL PROGRESS
N Engl J Med, Vol. 347, No. 6
August 8, 2002
www.nejm.org
421
The activation of central immune-cell populationsis eventually accompanied by the production of a wide
variety of nonspecific mediators of inflammation (Fig.2). These include many other cytokines, chemokines,and growth factors as well as metabolites of arachi-
donic acid (e.g., prostaglandins and leukotrienes) andreactive oxygen metabolites such as nitric oxide.
24,27
These mediators enhance the inflammatory processitself and tissue destruction, which eventuate in theclinical manifestations of disease. Recruitment of ad-ditional leukocytes from the vascular space to sitesof disease activity is especially important in maintain-ing inflammation and depends on the expression ofadhesion molecules in the local microvasculatureand counterligands on the various leukocyte popu-lations.
30,31
TREATMENT
Treatment must begin with accurate diagnosis. The
diagnosis of inflammatory bowel disease depends onthe aggregate constellation of the clinical history,physical findings, and endoscopic, radiologic, and his-tologic features, as well as the results of routine lab-oratory tests (Table 2). Typically, these features per-mit a firm diagnosis of inflammatory bowel diseaseand distinction between ulcerative colitis and Crohnsdisease. However, in as many as 10 percent of pa-tients with inflammatory bowel disease that is limitedto the colon, it may not be possible to distinguishulcerative colitis from Crohns disease, at least initially;thus, these patients are considered to have indeter-minate colitis. Serologic markers, including perinu-clear-staining antineutrophil cytoplasmic antibodies,
present in up to 70 percent of patients with ulcerativecolitis, and anti
Saccharomyces cerevisiae
antibodies,present in 50 percent or more of those with Crohnsdisease.
32-35
Although these markers may help in thedifferential diagnosis of the few patients in whom thenature of colitis cannot be determined according tothe usual criteria, they are not recommended for rou-tine diagnosis.
The long-term management of inflammatory bow-el disease must be multidimensional and governed bythe type of disease and sites involved (Table 3). Ad-
junctive agents, such as antidiarrheal agents, that aredirected primarily at relieving symptoms rather thancontrolling inflammation itself can be important. El-emental diets have also been advocated as a primarytreatment for Crohns disease, but patients poor com-pliance often limits the practicality of this approach.
35,36
Proper nutrition and attention to related secondarycomplications such as osteoporosis resulting from mal-absorption, corticosteroid therapy, or both are alsoimportant. Supplemental nutrition is especially im-portant in the treatment of growth failure in children.Surgery can have an important role in management,
though a full consideration is beyond the scope of thisreview.
Notwithstanding the importance of other treat-ments, an expanding number and variety of drugsthat target the inflammatory processes broadly or se-
lectively are usually effective in controlling active dis-ease in most patients and in sustaining symptomaticremission for prolonged periods in many. In general,most clinicians use a stepped approach to therapy in
which more potent agents are added to the regimenif less active drugs fail to achieve an adequate response.
5-Aminosalicylic Acid
The 5-aminosalicylatebased compounds have re-mained mainstays of treatment for patients with mildto moderately active ulcerative colitis and Crohnsdisease since the recognition of the therapeutic effi-cacy of the prototypical agent sulfasalazine (see Sup-plementary Appendix 1, available with the full text
of this article at http://www.nejm.org). Early studiesdemonstrated that 5-aminosalicylate was the func-tionally active moiety of this sulfapyridine congener.5-Aminosalicylate may act by blocking the productionof prostaglandins and leukotrienes, inhibiting bacterialpeptideinduced neutrophil chemotaxis and adeno-sine-induced secretion, scavenging reactive oxygenmetabolites, and perhaps inhibiting the activation ofnuclear factor-
k
B.Over the past 15 years, a variety of newer 5-ami-
nosalicylatebased compounds have become avail-able.
37-43
In general, a 5-aminosalicylatebased agentshould be selected principally on the basis of diseaselocation. For patients with distal colonic disease, a sup-
pository or enema form will be most appropriate. Oralcompounds in which 5-aminosalicylic acid (mesal-amine) is conjugated to prevent absorption by thesmall bowel are appropriate for colonic disease. Theseinclude sulfasalazine, olsalazine (a 5-aminosalicylic aciddimer), and the recently approved balsalazide. Topicalformulations may be used alone or in combination
with oral formulations for patients with left-sidedcolonic disease. Oral formulations in which 5-amino-salicylic acid is in a slow-release or pH-dependent ma-trix can deliver therapeutic concentrations to the moreproximal small bowel or distal ileum, respectively, toexpand the spectrum of patients with Crohns disease
who may be treated with this class of agent. Mainte-nance treatment with a 5-aminosalicylic acid can beeffective for sustaining remission in ulcerative colitisbut is of questionable value in Crohns disease.
Corticosteroids
Corticosteroids have been commonly used when5-aminosalicylatebased compounds are inadequate.They presumably act through the same functionalproperties relevant to other inflammatory processes,
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
6/13
422
N Engl J Med, Vol. 347, No. 6
August 8, 2002
www.nejm.org
The New England Journal of Medic ine
though which among these may be especially impor-tant in inflammatory bowel disease has not been de-termined.
Topical corticosteroids (hydrocortisone enemas orfoam) can be used as an alternative to 5-aminosalicy-latebased compounds for patients with ulcerative
proctitis or distal ulcerative colitis. Oral prednisoneor prednisolone is used for moderately severe ulcer-ative colitis or Crohns disease, in doses ranging upto 60 mg per day for patients with the most severedisease. Intravenous administration is warranted forpatients who are sufficiently ill to require hospital-
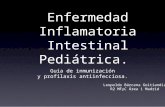
Figure 2.
Common Cellular Pathways of Activation in Inflammatory Bowel Disease.
Activation of the protean transcriptional regulatory factor nuclear factor-
k
B (NF-
k
B) is acommon pathway central to cell activation and the production of diverse inflammatory me-
diators, including a variety of cytokines and chemokines. It also modulates resistance toprogrammed cell death (apoptosis). Several inflammatory factors implicated in inflamma-tory bowel disease activate NF-
k
B by eventually stimulating an intermediate kinase suchas NF-
k
Binducing kinase (NIK) or mitogen-activated protein kinase kinase 1 or 3 (MEKK1
or MEKK3) or by binding to receptor-interacting protein 2. These lead to phosphorylation ofthe inhibitor ofkB kinase (IKK) and subsequent dissociation of NF-kB (itself a dimer). NF-kBthen travels to the nucleus, where it can effect gene transcription. The phosphorylated con-
stituents are subject to degradation by proteosomes after ubiquitination. The spectrum ofmediators that activate this pathway includes inflammatory cytokines such as interleukin-1and tumor necrosis factor (TNF), which bind to their respective cell-surface receptors, as
well as microbial products such as lipopolysaccharide, which bind to cell-surface receptorsthat are members of the toll-like receptor family of pattern-recognition receptors. The path-way is also activated by NOD2 (also referred to as CARD 15), an intracytoplasmic receptor
that is activated by the entry, through mechanisms yet to be defined, of bacterial lipopoly-saccharide into the cytoplasm. NOD2 is the product of the IBD1 gene; germ-line mutations,
which are present in many patients with Crohns disease, appear to alter the activation ofthe NF-kB pathway. MyD88 denotes myeloid differentiation factor 88.
Bacterial
lipopolysaccharide
Geneenetranscriptionranscription
InterleukinsnterleukinsCytokinesytokinesChemokineshemokines
NF-F-B
NOD2OD2MyD88yD88MyD88MyD88
Toll-like
receptor
TNF and
receptor
Interleukin-1
and receptor
Antiapoptosis
Gene
transcription
Interleukins
Cytokines
Chemokines
NF-B
IBIB
NOD2
NIK, MEKK1,IK, MEKK1,or MEKK3r MEKK3NIK, MEKK1,or MEKK3
IKKKKcomplexomplexIKKcomplex
Receptor-interactingeceptor-interactingprotein 2rotein 2Receptor-interactingprotein 2
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
7/13
MEDICAL PROGRESS
N Engl J Med, Vol. 347, No. 6 August 8, 2002 www.nejm.org 423
ization; the majority of such patients, even those withfulminant ulcerative colitis, will have a response with-in 7 to 10 days. Optimal administration schedules foreither oral or intravenous corticosteroids have notbeen defined. Corticosteroids, irrespective of the routeof administration, should be continued only as longas needed to control acute inflammatory activity, sincethey have no proven maintenance benefit in the treat-ment of either ulcerative colitis or Crohns disease.Optimal tapering schedules have not been definedand are generally guided by clinical experience.44
Although corticosteroids are frequently, thoughnot invariably, effective, these effects must be balancedagainst their many and often serious side effects. Ingeneral, side effects correlate with the dose and du-ration of treatment. Some side effects may be partiallyoffset by careful management (e.g., early administra-tion of supplemental calcium, vitamin D, and bisphos-phonates to reduce corticosteroid-induced osteoporo-sis and careful monitoring of blood pressure and bloodglucose for corticosteroid-induced hypertension anddiabetes). For some patients, the side effects may bepartially circumvented by the use of budesonide, whichhas recently become available in the United States ina controlled-ileal-release formulation; an enema formis also available elsewhere.45-47 However, concern per-sists that patients who take budesonide for prolongedperiods remain at risk for systemic side effects; al-though first-pass metabolism may eliminate more than90 percent of the drug, budesonide has an affinity forthe glucocorticoid receptor that is 50 to 100 timesthat of prednisone. Moreover, its use is limited primar-ily to patients with distal ileal and right-sided colonic
disease, and its efficacy somewhat less than that of con-ventional corticosteroids.
Immunosuppressive and Immunoregulatory Agents
There is an expanding role for immunomodulatorydrugs in the care of patients with inflammatory boweldisease. These agents are generally appropriate for pa-tients in whom the dose of corticosteroids cannot betapered or discontinued. All these agents (as well ascorticosteroids) put patients at risk for opportunisticinfections.
Azathioprine and its active metabolite mercapto-purine have been the most extensively used immuno-suppressive agents, despite early hesitation arising fromconcern about an increased risk of lymphoma and oth-er side effects. Indeed, this issue remains unresolved,in part owing to uncertainty about the possibility ofa small, underlying increase in the risk of lymphomain patients with inflammatory bowel disease.48-50 Theactual mechanisms of action responsible for the ther-apeutic effect of these drugs remain largely unknownbut may include suppressing the generation of a spe-cific and long-lived subgroup of T cells, which mightaccount for the prolonged time needed to achieve atherapeutic response.
Clinical studies have shown that these agents areefficacious when they are given in adequate doses inpatients with ulcerative colitis or Crohns disease, al-lowing a gradual decrease in the corticosteroids andprolonging remission.51-53 The onset of benefit typ-ically takes several weeks and may require up to sixmonths, so that these drugs are not useful in the con-trol of acute disease activity and, conversely, should
TABLE 3. THERAPEUTIC OPTIONSFOR ULCERATIVE COLITISAND CROHNS DISEASE.
VARIABLE DISTAL ULCERATIVE COLITIS EXTENSIVE ULCERATIVE COLITIS CROHNS DISEASE
Mild disease Oral or rectal aminosalicylates Oral aminosalicylates Oral aminosalicylatesRectal corticosteroids Oral metronidazolePossibly oral budesonide or ciprofloxacin
Moderate disease Oral or rectal aminosalicylatesRectal cort icosteroids
Oral aminosalicylates Oral corticosteroids (budesonide for ilealor right-sided colonic disease)
Oral azathioprine or mercaptopurine
Severe disease Oral or parenteral corticosteroids Oral or parenteral corticosteroids Oral or parenteral corticosteroidsRectal corticosteroids Intravenous cyclosporine Subcutaneous or intravenous methotrexate
Intravenous infliximab
Refractory disease Oral or intravenous corticosteroids,in addition to oral azathioprine ormercaptopurine
Oral or intravenous cor ticosteroids,in addition to oral azathioprine ormercaptopurine
Intravenous infliximab
Perianal disease Oral antibiotic (metronidazole or cipro-floxacin)
Intravenous infliximabOral azathioprine or mercaptopurine
Remission Oral or rectal aminosalicylatesOral azathioprine or mercaptopurine
Oral aminosalicylatesOral azathioprine or mercaptopurine
Possibly oral azathioprine or mercaptopur-ine, mesalamine, metronidazole
Oral azathioprine or mercaptopurine
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
8/13
424 N Engl J Med, Vol. 347, No. 6 August 8, 2002 www.nejm.org
The New England Journal of Medic ine
be used only when prolonged therapy is planned.Although no firm guidelines for initiating the use ofthese agents have been established, many cliniciansconsider their use if it has not been possible to weanpatients from corticosteroids after six weeks.
Toxic effects, some quite serious, frequently limit theuse of azathioprine and mercaptopurine. Dose-relat-ed suppression of bone marrow is uniformly observed,and the white-cell count must be monitored closely
when therapy is initiated and periodically thereafter(typically every two to three months). Considerableprogress has been made in delineating the pathwaysof metabolism of mercaptopurine, and these findingshave highlighted the importance of genetic variants ofthe key enzyme thiopurine S-methyltransferase in de-termining susceptibility to life-threatening bone mar-row suppression.54-56 Approximately 0.1 percent of pa-tients are homozygous for a functionally null allele thatleads to the accumulation of toxic metabolites derived
from alternative degradative pathways. Neither bloodcounts nor metabolite concentrations reliably predictother toxic effects, which include pancreatitis anddrug-induced hepatotoxicity. In both instances, theseinitially asymptomatic effects are usually reversible withdiscontinuation of the medication and rapidly recur
with greater severity if treatment is resumed.Methotrexate is effective in the treatment of cor-
ticosteroid-dependent active Crohns disease and inmaintaining remission.57-59 Typically, the drug is ad-ministered as a weekly injection, either intramuscu-lar (15 mg per week) or subcutaneous (25 mg per
week), and the response becomes evident over a pe-riod of several weeks. The mechanism of action of
this agent also remains mostly uncertain. Aside fromthe generic risks of immunosuppression, methotrex-ate may lead to interstitial pneumonitis, which is firstmanifested by nonproductive cough and dyspnea,and there is a dose-related risk of hepatic fibrosis.
Cyclosporine can be effective in the treatment ofpatients with severe ulcerative colitis who are hospi-talized and otherwise in need of urgent proctocolec-tomy.60-62 This agent is presumed to work by block-ing lymphocyte activation. High doses can achieve atleast short-term control of disease sufficient to allowup to 80 percent of hospitalized patients who havebeen unresponsive to corticosteroids to be switchedto a tapering oral regimen of cyclosporine. Cyclospor-ine is usually added after an initial 7-to-10-day trialof intravenous high-dose corticosteroids. A recentstudy has shown essentially equivalent response ratesin patients given either cyclosporine or corticoster-oids as initial intravenous therapy after hospitaliza-tion.62 Although, as noted above, short-term controlof disease will result from the addition of cyclospor-ine in a substantial number of patients, approximately50 percent will undergo proctocolectomy within a
year as a result of either the inability to taper medi-cations or recurrent disease activity. Azathioprine ormercaptopurine may help sustain the cyclosporine-induced response. In general, cyclosporine should notbe used in the treatment of patients with Crohns
disease, with the possible exception of patients withsymptomatic and severe perianal or cutaneous fistu-las.63 Recent trials have suggested that the related com-pound tacrolimus, as well as mycophenolate mofetil,is also effective in the treatment of patients with in-flammatory bowel disease, though direct comparativestudies with cyclosporine have not been carried out.
Anti-TNF Therapy
The availability of the prototypical anti-TNF agentinfliximab has offered an important advance in ther-apy for patients with Crohns disease.64 Infliximabsmechanism of action is incompletely understood. Itseffectiveness suggests that TNF, a product of activat-
ed macrophages, may have a pivotal role among themany regulatory peptides with altered expression inassociation with inflammatory bowel disease.65,66 Thischimeric monoclonal antibody, composed of a com-plement-fixing human IgG1 constant region and amurine-derived antigen-binding variable region, bindssoluble TNF; however, its action is thought to de-pend in part on its ability to bind precursor cell-sur-face TNF, perhaps leading to monocyte apoptosis.
Two pivotal trials demonstrated the efficacy of in-fliximab in patients with Crohns disease.67,68 In thefirst, approximately two thirds of patients with mod-erately active Crohns disease who received a singleinfusion of infliximab had a significant reduction in
their score on a standard Crohns Disease ActivityIndex; of these, approximately half (one third of thetotal) achieved actual clinical remission. The response
was generally quite prompt (usually within two weeks).However, the durability of the response ranged froma few weeks to six months or more. This pattern ofresponse was mirrored in the second reported studyin which patients with perianal and cutaneous fistu-las received three infusions over a period of six weeks.Since this drug was approved for use in the UnitedStates, the experience in treating patients in routinepractice has largely resembled that observed in con-trolled studies.69-71
Important questions remain to be addressed to de-fine the most appropriate use of infliximab. Recentlycompleted trials suggest the effectiveness of serial ad-ministration of the drug to maintain the initial re-sponse, but this indication is not yet approved.72 Fur-thermore, although responses have been reported insmall numbers of patients with a variety of other in-testinal inflammatory conditions (e.g., Behets syn-drome), the usefulness of infliximab in patients withulcerative colitis remains uncertain.
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
9/13
MEDICAL PROGRESS
N Engl J Med, Vol. 347, No. 6 August 8, 2002 www.nejm.org 425
The optimal timing of infliximab administrationand the value of maintenance therapy must be deter-mined in rigorous studies, for several reasons. First,patients may not remain responsive to infliximab ther-apy indefinitely, and in some, the duration of responseafter an infusion becomes progressively shorter. Sec-ond, some patients who received infliximab during tri-als and who resumed treatment after a prolonged hia-tus had a serum sicknesslike reaction, suggesting that
the drug should not be used intermittently. Collec-tively, these two observations necessitate judicious useof this agent in patients with a lifelong condition.Third, the therapy is quite costly in terms of boththe cost of the drug itself and the logistics of infusingit (the average third-party reimbursement per dose ad-ministered to a 70-kg patient is more than $5,200).Fourth, though it is generally safe, serious complica-tions can ensue. In addition to occasional hypersensi-
TABLE 4. POTENTIAL THERAPEUTIC AGENTSFOR INFLAMMATORYBOWEL DISEASE.
AGENT RATIONALEOR TARGET STATUS
Growth hormone Stimulates production of insulin-likegrowth factor 1; trophic for theintestinal mucosa
Superior to placebo in patients withactive Crohns disease in a singletrial
Heparin Binds relevant growth factors (e.g.,fibroblast growth factor); blocksprothrombotic state; has anti-thrombotic activity
Some activity in suppressing activeulcerative colitis in multiple trials
Fish oil Modulates metabolism of arachidonicacid and its products
Reduced postoperative recurrenceof Crohns disease over a 2-yearperiod in a controlled trial
Nicotine patch Agent in tobacco that may accountfor the protective effect of smokingin patients with ulcerative colitis
Reduced some symptoms of ulcer-ative colitis but caused no objectivechanges in a controlled trial
Thalidomide Inhibits intracellular processingof tumor necrosis factor
Response in patients with activeCrohns disease in two pilot trials
Short-chain fattyacids
Presumptive optimal metabolic fuelfor colonic epithelium
Enema formulation improved distalulcerative colitis; results vary
Elemental diet Modulates antigenic load either di-
rectly or through altered flora
Improvement in active Crohns dis-
ease in multiple studiesMycophenolate
mofetilInhibits pathogenic T cell s Response in pat ients with Crohns
disease, but not ulcerative colitis, insmall series and controlled trials
Tacrolimus Inhibits activation pathways in lym-phocytes and other cell popula-tions
Benefit similar to that afforded by cy-closporine in small series; healingof fistulas
Interleukin-11 Enhances epithelial integrity Phase 23 studies in patients withCrohns disease
Interleukin-10 Down-regulates lymphocyte activa-tion
Minimal activity in patients withCrohns disease in phase 3 trials
Antiinterferon-g Antagonizes activation of macro-phages by interferon-g
Phase 2 trial in patients with Crohnsdisease
Antiinterleukin-12 Antagonizes interleukin-12 activationof type 1 helper T cells
Phase 2 studies in patients withCrohns disease
Keratinocyte growthfactor
Stimulates epithelial proliferation andrepair
Phase 2 studies in patients with ulcer-ative colitis
p38 Inhibitor Inhibits signal pathway leading tonuclear factor-kB Phase 12 studies in patients withCrohns disease
Antia4 integrin Inhibits leukocyte recruitment Variable activity in pat ients withCrohns disease in phase 3 studies
Antia4b7 integrin Inhibits leukocyte recruitment Phase 3 studies in patients with ulcer-ative colitis and Crohns disease
Bactericidalperme-ability-increasingprotein
Inhibits bacterial stimulation Phase 2 studies in patients withCrohns disease
Rosiglitazone Inhibits peroxisome-proli feratoractivated receptor-g
Phase 2 trial in patients with ulcer-ative colitis
Probiotic mixture Replaces pathogenic endogenousflora
Prevented pouchitis in studies ofpatients with ulcerative colitis; re-duced activity in Crohns disease
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
10/13
426 N Engl J Med, Vol. 347, No. 6 August 8, 2002 www.nejm.org
The New England Journal of Medic ine
tivity and infusion reactions, a number of deaths havebeen reported as a result of tuberculosis or sepsis.Complications have included the reactivation of tuber-culosis with atypical features; thus, all patients shouldbe screened for tuberculosis before beginning therapy.
Although a lupus-like syndrome has been reported in-frequently after treatment with infliximab, the clinicalsignificance of the more frequently detected antinucle-ar antibodies and antichimeric monoclonal antibodiesis uncertain. Finally, lymphoma has developed in asmall number of patients receiving infliximab, thougha causal relation has not been established.
A number of other agents that target TNF are inadvanced stages of clinical evaluation. These includeCDP571, a humanized monoclonal antibody in whichonly the small number of residues necessary to conferantigen specificity remain from the original murineantibody. The overall usefulness of CDP571 in clin-ical trials involving patients with active Crohns dis-
ease appears to be generally similar to that observedwith infliximab.73,74 These results contrast with thevery limited efficacy of etanercept, a fusion proteincomposed of the ligand-binding domain of the solu-ble receptor for TNF and an IgG common region, inpatients with Crohns disease.75
There has been recent interest in the use of thalid-omide in the treatment of Crohns disease, because ofits presumptive action in blocking the production ofTNF through the inhibition of intracellular path-
ways.76 Two small pilot trials have suggested thera-peutic effectiveness.77,78 However, given the infamoushistory of this agent as a teratogen, its use requiresrigorous supervision, including confirmation of ade-
quate contraception in patients of childbearing age.
Antibiotics and Probiotics
Empirical clinical experience has led to the recog-nition that antibiotics are useful in the treatment ofsubgroups of patients with Crohns disease.79 In con-trast, antibiotics have very limited use in patients withulcerative colitis, suggesting a differential role of theluminal flora in the two forms of inflammatory boweldisease.80 Metronidazole can be effective in the treat-ment of patients with Crohns disease who have per-ianal fistulas. However, high doses are usually neces-sary (up to 750 mg three times daily), and the sideeffects may be limiting, most notably neurotoxicity.Despite its lack of effectiveness in the treatment ofulcerative colitis, metronidazole can control colonic(but not small-bowel) Crohns disease. Ciprofloxacinand clarithromycin have been advocated as alterna-tives to metronidazole, but only small trials have beenreported.
The effectiveness of nonspecific antibiotics and ex-perimental evidence of the central role of the lumi-nal flora as an essential cofactor for the development
of disease in the susceptible host have provided animpetus to the development of alternative strategiesto manipulate the intestinal flora for therapeutic ben-efit. Probiotics, the administration of healthy bac-teria, appears to be one promising approach.81 Pa-
tients with pouchitis or active Crohns disease whowere treated with a mixture of commensal bacteriahad a positive therapeutic response; these findingsshould prompt increased efforts to define the valueof this approach, which could be free of systemic sideeffects.82
Investigational Agents
Advances in the understanding of the pathophys-iology of inflammatory bowel disease, even if theyare still incomplete, have led to great interest in theevaluation of a variety of new therapeutic agents withnovel actions (Table 4). The explication of the cyto-kine network in inflammatory bowel disease and the
seemingly central role of macrophage-produced in-terleukin-12, as described above, have led to ongoingtrials with antibodies against interleukin-12. Interleu-kin-10, a cytokine that generally down-regulates theactivation of Th1 cells, was found to have minimalactivity in Crohns disease.83-85 Preliminary studies ofinterleukin-11, a cytokine that is thought to act byenhancing the epithelial barrier as well as through theinhibition of inflammatory cytokines, showed an ap-parent benefit. Larger trials of interleukin-11 in pa-tients with ulcerative colitis and Crohns disease arein progress.86
Strategies that block the recruitment of leukocytesto the sites of mucosal inflammation have produced
promising results for example, a large-scale studyof patients with Crohns disease who were treated
with a monoclonal antibody directed against the a4integrin subunit. This integrin is part of a heterodimerthat functions as a homing molecule for mucosal lym-phocytes.87 Studies in both patients with ulcerativecolitis and those with Crohns disease are also under
way after the demonstration, in pilot studies, that achimeric antibody specific for the a4b7 integrin het-erodimer reduced disease activity in patients withmoderate-to-severe ulcerative colitis.88
Increasing attention is being directed at efforts toblock the intracellular signaling pathways central tothe activation of lymphocytes and macrophages withthe use of p38 antagonists and agents that target thetranscription factor nuclear factor-kB. A few patientshave already received a p38-blocking small molecule,
with apparent benefit. However, most of these agentsare in a relatively early stage of development,89 andthe overall safety of disrupting ubiquitous signalingmechanisms remains to be determined. In addition,a variety of more conventional agents, includinggrowth hormone,90 transdermal nicotine,91 fish oil,92
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
11/13
MEDICAL PROGRESS
N Engl J Med, Vol. 347, No. 6 August 8, 2002 www.nejm.org 427
and rosiglitazone,93 have been found to have someeffect in trials of variable sizes (Table 4). Finally, sev-eral patients with Crohns disease had a prolongedremission after undergoing allogeneic bone marrowtransplantation for unrelated reasons; this effect was
presumably the result of reconstitution with non-pathogenic T cells.94 However, this approach cannotbe considered established therapy.
CONCLUSIONS
Considerable progress has been made recently inboth defining the mechanisms underlying the devel-opment of inflammatory bowel disease and expand-ing the spectrum of effective therapies. It is reasonableto expect that, as the spectrum of genes that confersusceptibility to inflammatory bowel disease is iden-tified, attention will be focused on the mechanismsthrough which they lead to ulcerative colitis andCrohns disease. A definitive understanding will re-
quire the delineation of the nature of the interactionswith environmental factors, especially microflora.Progress in achieving these goals should lead to moreprecise genetic-based diagnosis, including presymp-tomatic risk assessment in family members of affectedpatients. In the interim, progress in our understand-ing of facets of the pathophysiology of inflammatorybowel disease has led to the development of usefulnew therapies.
The Center for the Study of Inflammatory Bowel Disease is supportedby funds from the National Institutes of Health (P30 DK43351).
I am indebted to Drs. Lawrence Friedman, Stephen Goldfinger,and Bruce Sands for comments and suggestions.
REFERENCES
1. Tysk C, Lindberg E, Jarnerot G, Floderus-Myrhed B. Ulcerative colitisand Crohns disease in an unselected population of monozygotic and dizy-gotic twins: a study of heritability and the influence of smoking. Gut 1988;29:990-6.2. Orholm M, Munkholm P, Langholz E, Nielsen OH, Srensen TIA,Binder V. Familial occurrence of inflammatory bowel disease. N Engl JMed 1991;324:84-8.3. Cariappa A, Sands B, Forcione D, Finkelstein D, Podolsky DK, Pillai S.
Analysis of MHC class II DP, DQ and DR alleles in Crohns disease. Gut1998;43:210-5.4. Satsangi J, Welsh KI, Bunce M, et al. Contribution of genes of the ma-
jor histocompatibility complex to susceptibility and disease phenotype ininflammatory bowel disease. Lancet 1996;347:1212-7.5. Negoro K, Kinouchi Y, Hiwatashi N, et al. Crohns disease is associated
with novel polymorphisms in the 5'-flanking region of the tumor necrosis
factor gene. Gastroenterology 1999;117:1062-8.6. Hugot JP, Laurent-Puig P, Gower-Rousseau C, et al. Mapping of a sus-ceptibility locus for Crohns disease on chromosome 16. Nature 1996;379:821-3.7. Satsangi J, Parkes M, Louis E, et al. Two stage genome-wide search ininflammatory bowel disease provides evidence for susceptibility loci onchromosomes 3, 7 and 12. Nat Genet 1996;14:199-202.8. Ma Y, Ohmen JD, Li Z, et al. A genome-wide search identifies potentialnew susceptibility loci for Crohns disease. Inflamm Bowel Dis 1999;5:271-8.9. Brant SR, Fu Y, Fields CT, et al. American families with Crohns diseasehave strong evidence for linkage to chromosome 16 but not chromosome12. Gastroenterology 1998;115:1056-61.
10. Rioux JD, Daly MJ, Green T, et al. Absence of linkage between in-flammatory bowel disease and selected loci on chromosomes 3, 7, 12, and16. Gastroenterology 1998;115:1062-5.11. Hugot JP, Chamaillard M, Zouali H, et al. Association of NOD2 leu-cine-rich repeat variants with susceptibility to Crohns disease. Nature2001;411:599-603.12. Ogura Y, Bonen DK, Inohara N, et al. A frameshift mutation in
NOD2 associated with susceptibility to Crohns disease. Nature 2001;411:603-6.13. Ahmad T, Armuzzi A, Bunce M, et al. The molecular classification ofthe clinical manifestations of Crohns disease. Gastroenterology 2002;122:854-66.14. Cuthbert AP, Fisher SA, Mirza MM, et al. The contribution of NOD2gene mutations to the risk and site of disease in inflammatory bowel dis-ease. Gastroenterology 2002;122:867-74.15. Lesage S, Zouali H, Cezard JP, et al. CARD15/NOD2 mutationalanalysis and genotype-phenotype correlation in 612 patients with inflam-matory bowel disease. Am J Hum Genet 2002;70:845-57.16. Rioux JD, Daly MJ, Silverberg MS, et al. Genetic variation in the 5q31cytokine gene cluster confers susceptibility to Crohn disease. Nat Genet2001;29:223-8.17. Andersson RE, Olaison G, Tysk C, Ekbom A. Appendectomy and pro-tection against ulcerative colitis. N Engl J Med 2001;344:808-14.18. Evans JM, McMahon AD, Murray FE, McDevitt DG, MacDonaldTM. Non-steroidal anti-inflammatory drugs are associated with emergencyadmission to hospital for colitis due to inflammatory bowel disease. Gut
1997;40:619-22.19. Cosnes J, Beaugerie L, Carbornnel F, Gendre JP. Smoking cessationand the course of Crohns disease: an intervention study. Gastroenterology2001;120:1093-9.20. Lindberg E, Tysk C, Andersson K, Jarnerot G. Smoking and inflam-matory bowel disease: a case control study. Gut 1988;29:352-7.21. Rath HC, Schultz M, Freitag R, et al. Different subsets of enteric bac-teria induce and perpetuate experimental colitis in rats and mice. Infect Im-mun 2001;69:2277-85.22. Elson CO. Experimental models of intestinal inflammation: new in-sights into mechanisms of mucosal homeostasis. In: Ogra PL, Mestecky J,Lamm ME, Strober W, Bienenstock J, McGhee JR, eds. Mucosal immu-nology. 2nd ed. San Diego, Calif.: Academic Press, 1999:1007-24.23. Darfeuille-Michaud A, Neut C, Barnich N, et al. Presence of adherentEscherichia coli strains in ileal mucosa of patients with Crohns disease.Gastroenterology 1998;115:1405-13.24. Swidsinski A, Ladhoff A, Pernthaler A, et al. Mucosal flora in inflam-matory bowel disease. Gastroenterology 2002;122:44-54.25. Mashimo H, Wu DC, Podolsky DK, Fishman MC. Impaired defense
of intestinal mucosa in mice lacking intestinal trefoil factor. Science 1996;274:262-5.26. Schmitz H, Barmeyer C, Fromm M, et al. Altered tight junction struc-ture contributes to the impaired epithelial barrier function in ulcerativecolitis. Gastroenterology 1999;116:301-9.27. Fiocchi C. Inflammatory bowel disease: etiology and pathogenesis.Gastroenterology 1998;115:182-205.28. Fuss IJ, Neurath M, Boirivant M, et al. Disparate CD4+ lamina pro-pria (LP) lymphokine secretion profiles in inflammatory bowel disease:Crohns disease LP cells manifest increased secretion of IFN-gamma,
whereas ulcerative colitis LP cells manifest increased secretion of IL-5.J Immunol 1996;157:1261-70.29. Toms C, Powrie F. Control of intestinal inflammation by regulatoryT cells. Microbes Infect 2001;3:929-35.30. Sans M, Salas A, Soriano A, et al. Differential role of selectins in ex-perimental colitis. Gastroenterology 2001;120:1162-72.31. Koizumi M, King N, Lobb R , Benjamin C, Podolsky DK. Expressionof vascular adhesion molecules in inflammatory bowel disease. Gastroen-terology 1992;103:840-7.
32. Saxon A, Shanahan F, Landers C, Ganz T, Targan S. A distinct subsetof antineutrophil cytoplasmic antibodies is associated with inflammatorybowel disease. J Allergy Clin Immunol 1990;86:202-10.33. Peeters M, Joossens S, Vermeire S, Vlietinck R , Bossuyt X, RutgeertsP. Diagnostic value of anti-Saccharomyces cerevisiae and antineutrophil cy-toplasmic autoantibodies in inflammatory bowel disease. Am J Gastroen-terol 2001;96:730-4.34. Vermeire S, Joossens S, Peeters M, et al. Comparative study of ASCA(anti-Saccharomyces cerevisiae antibody) assays in inflammatory bowel dis-ease. Gastroenterology 2001;120:827-33.35. Rigaud D, Cosnes J, Le Quintrec Y, Rene E, Gendre JP, Mignon M.Controlled trial comparing two types of enteral nutrition in treatment ofactive Crohns disease: elemental versus polymeric diet. Gut 1991;32:1492-7.
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
12/13
428 N Engl J Med, Vol. 347, No. 6 August 8, 2002 www.nejm.org
The New England Journal of Medic ine
36. Griffiths AM, Ohlsson A, Sherman PM, Sutherland LR. Meta-analysisof enteral nutrition as a primary treatment of active Crohns disease. Gas-troenterology 1995;108:1056-67.37. Sutherland LR, Rothy DE, Beck PL. Alternatives to sulfasalazine:a meta-analysis of 5-ASA in the treatment of ulcerative colitis. InflammBowel Dis 1997;3:65-78.38. Sutherland LR, Martin F, Greer S, et al. 5-Aminosalicylic acid enema
in the treatment of distal ulcerative colitis, proctosigmoiditis, and proctitis.Gastroenterology 1987;92:1894-8.39. Green JR, Lobo AJ, Holdsworth CD, et al. Balsalazide is more effec-tive and better tolerated than mesalamine in the treatment of acute ulcer-ative colitis. Gastroenterology 1998;114:15-22.40. Prantera C, Cottone M, Pallone F, et al. Mesalamine in the treatmentof mild to moderate active Crohns ileitis: results of a randomized, multi-center trial. Gastroenterology 1999;116:521-6.41. Hanauer SB, Krawitt EL, Robinson M, Rick GG, Safdi MA. Long-term management of Crohns disease with mesalamine capsules (Pentasa).
Am J Gastroenterol 1993;88:1343-51.42. Hanauer SB, Robinson M, Pruitt R , et al. Budesonide enema for thetreatment of active, distal ulcerative colitis and proctitis: a dose-rangingstudy. Gastroenterology 1998;115:525-32.43. Mahmud N, Kamm MA, Dupas JL, et al. Olsalazine is not superiorto placebo in maintaining remission of inactive Crohns colitis and ileocoli-tis: a double blind, parallel, randomised, multicentre study. Gut 2001;49:552-6.44. Faubion WA Jr, Loftus EV Jr, Harmsen WS, Zinsmeister AR, Sandborn
WJ. The natural history of corticosteroid therapy for inflammatory boweldisease: a population-based study. Gastroenterology 2001;121:255-60.45. Danielsson A, Lofberg R, Persson T, et al. A steroid enema, budeso-nide, lacking systemic effects for the treatment of distal ulcerative colitis orproctitis. Scand J Gastroenterol 1992;27:9-12.46. Greenberg GR, Feagan BG, Martin F, et al. Oral budesonide as main-tenance treatment for Crohns disease: a placebo-controlled, dose-rangingstudy. Gastroenterology 1996;110:45-51.47. Thomsen O, Cortot A, Jewell D, et al. A comparison of budesonideand mesalamine for active Crohns disease. N Engl J Med 1998;339:370-4. [Erratum, N Engl J Med 2001;345:1652.]48. Lewis JD, Bilker WB, Brensinger C, Deren JJ, Vaughn DJ, Strom BL.Inflammatory bowel disease is not associated with an increased risk of lym-phoma. Gastroenterology 2001;121:1080-7.49. Loftus EV Jr, Sandborn WJ. Lymphoma risk in inflammatory boweldisease: influences of referral bias and therapy. Gastroenterology 2001;121:1239-42.50. Farrell RJ, Ang Y, Kileen P, et al. Increased incidence of non-Hodg-kins lymphoma in inflammatory bowel disease patients on immunosup-
pressive therapy but overall risk is low. Gut 2000;47:514-9.51. Present DH, Korelitz BI, Wisch N, Glass JL, Sachar DB, PasternackBS. Treatment of Crohns disease with 6-mercaptopurine: a long-term, ran-domized, double-blind study. N Engl J Med 1980;302:981-7.52. Lewis JD, Schwartz JS, Lichtenstein GR. Azathioprine for mainte-nance of remission in Crohns disease: benefits outweigh the risk of lym-phoma. Gastroenterology 2000;118:1018-24.53. Bouhnik Y, Lemann M, Mary JY, et al. Long-term follow-up of pa-tients with Crohns disease treated with azathioprine or 6-mercaptopurine.Lancet 1996;347:215-9.54. Corominas H, Domenech M, Gonzalez D, et al. Allelic variants of thethiopurine S-methyltransferase deficiency in patients with ulcerative colitisand in healthy controls. Am J Gastroenterol 2000;95:2313-7.55. Dubinsky MC, Lamothe S, Yang HY, et al. Pharmacogenomics andmetabolite measurement for 6-mercaptopurine therapy in inflammatorybowel disease. Gastroenterology 2000;118:705-13.56. Colombel JF, Ferrari N, Debuysere H, et al. Genotypic analysis of thi-opurine S-methyltransferase in patients with Crohns disease and severemyelosuppression during azathioprine therapy. Gastroenterology 2000;
118:1025-30.57. Feagan BG, Fedorak RN, Irvine EJ, et al. A comparison of methotrex-ate with placebo for the maintenance of remission in Crohns disease.N Engl J Med 2000;342:1627-32.58. Feagan BG, Rochon J, Fedorak RN, et al. Methotrexate for the treat-ment of Crohns disease. N Engl J Med 1995;332:292-7.59. Oren R, Arber N, Odes S, et al. Methotrexate in chronic active ulcer-ative colitis: a double-blind, randomized, Israeli multicenter trial. Gastro-enterology 1996;110:1416-21.60. Lichtiger S, Present DH, Kornbluth A, et al. Cyclosporine in severe ul-cerative colitis refractory to steroid therapy. N Engl J Med 1994;330:1841-5.61. Kornbluth A, Present DH, L ichtiger S, Hanauer S. Cyclosporin for se-
vere ulcerative colitis: a users guide. Am J Gastroenterol 1997;92:1424-8.
62. DHaens G, Lemmens L, Geboes K, et al. Intravenous cyclosporineversus intravenous corticosteroids as single therapy for severe attacks of ul-cerative colitis. Gastroenterology 2001;120:1323-9.63. Stange EF, Modigliani R, Pena AS, Wood AJ, Feutren G, Smith PR.European trial of cyclosporine in chronic active Crohns disease: a 12-month study. Gastroenterology 1995;109:774-82.64. van Dullemen HM, van Deventer SJ, Hommes DW, et al. Treatment
of Crohns disease with anti-tumor necrosis factor chimeric monoclonal an-tibody (cA2). Gastroenterology 1995;109:129-35.65. ten Hove T, van Montfrans C, Peppelenbosch MP, van Deventer SJ.Infliximab treatment induces apoptosis of lamina propria T lymphocytes inCrohns disease. Gut 2002;50:206-11.66. Lugering A, Schmidt M, Lugering N, Pauels HG, Domschke W, Ku-charzik T. Infliximab induces apoptosis in monocytes from patients withchronic active Crohns disease by using a caspase-dependent pathway. Gas-troenterology 2001;121:1145-57.67. Targan SR, Hanauer SB, van Deventer SJH, et al. A short-term studyof chimeric monoclonal antibody cA2 to tumor necrosis factor a forCrohns disease. N Engl J Med l997;337:1029-35.68. Present DH, Rutgeerts P, Targan S, et al. Infliximab for the treatment offistulas in patients with Crohns disease. N Engl J Med 1999;340:1398-405.69. Cohen RD, Tsang JF, Hanauer SB. Infliximab in Crohns disease: firstanniversary clinical experience. Am J Gastroenterol 2000;95:3469-77.70. Ricart E, Panaccione R, Loftus EV, Tremaine WJ, Sandborn WJ. In-fliximab for Crohns disease in clinical practice at the Mayo Clinic: the first100 patients. Am J Gastroenterol 2001;96:722-9.
71. Rutgeerts P, DHaens G, Targan S, et al. Efficacy and safety of retreat-ment with anti-tumor necrosis factor antibody (infliximab) to maintain re-mission in Crohns disease. Gastroenterology 1999;117:761-9.72. Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance inflix-imab for Crohns disease: the ACCENT I randomised trial. Lancet 2002;359:1541-9.73. Sandborn WJ, Feagan BG, Hanauer SB, et al. An engineered humanantibody to TNF (CDP571) for active Crohns disease: a randomized dou-ble-blind placebo-controlled trial. Gastroenterology 2001;120:1330-8.74. Stack WA, Mann SD, Roy AJ, et al. Randomised controlled trial ofCDP571 antibody to tumour necrosis factor-alpha in Crohns disease. Lan-cet 1997;349:521-4.75. Sandborn WJ, Hanauer SB, Katz S, et al. Etanercept for active Crohnsdisease: a randomized, double-blind, placebo-controlled trial. Gastroenter-ology 2001;121:1088-94.76. Bauditz J, Wedel S, Lochs H. Thalidomide reduces tumour necrosisfactor alpha and interleukin 12 production in patients with chronic activeCrohns disease. Gut 2002;50:196-200.77. Vasiliauskas EA, Kam LY, Abreu-Martin MT, et al. An open-label pilot
study of low-dose thalidomide in chronically active, steroid-dependentCrohns disease. Gastroenterology 1999;117:1278-87.78. Ehrenpreis ED, Kane SV, Cohen LB, Cohen RD, Hanauer SB. Tha-lidomide therapy for patients with refractory Crohns disease: an open-labeltrial. Gastroenterology 1999;117:1271-7.79. Sutherland L, Singleton J, Sessions J, et al. Double blind, placebo con-trolled trial of metronidazole in Crohns disease. Gut 1991;32:1071-5.80. Turunen UM, Farkkila MA, Hakala K, et al. Long-term treatment ofulcerative colitis with ciprofloxacin: a prospective, double-blind, placebo-controlled study. Gastroenterology 1998;115:1072-8.81. Rembacken BJ, Snelling AM, Hawkey PM, Chalmers DM, Axon AT.Non-pathogenic Escherichia coli versus mesalazine for the treatment of ul-cerative colitis: a randomised trial. Lancet l999;354:635-9.82. Gionchetti P, Rizzello F, Venturi A, et al. Oral bacteriotherapy asmaintenance treatment in patients with chronic pouchitis: a double-blind,placebo-controlled trial. Gastroenterology 2000;119:305-9.83. van Deventer SJ, Elson CO, Fedorak RN. Multiple doses of intrave-nous interleukin 10 in steroid-refractory Crohns disease. Gastroenterology1997;113:383-9.
84. Schreiber S, Fedorak RN, Nielsen OH, et al. Safety and efficacy of re-combinant human interleukin 10 in chronic active Crohns disease. Gastro-enterology 2000;119:1461-72.85. Fedorak RN, Gangl A, Elson CO, et al. Recombinant human inter-leukin 10 in the treatment of patients with mild to moderately activeCrohns disease. Gastroenterology 2000;119:1473-82.86. Sands BE, Bank S, Sninsky CA, et al. Preliminary evaluation of safetyand activity of recombinant human interleukin 11 in patients with activeCrohns disease. Gastroenterology 1999;117:58-64.87. Gordon FH, Lai CW, Hamilton MI, et al. A randomized placebo-con-trolled trial of a humanized monoclonal antibody to alpha4 integrin in ac-tive Crohns disease. Gastroenterology 2001;121:268-74.88. Feagan BG, McDonald J, Greenberg G, et al. An ascending dose trial
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.
Copyright 2002 Massachusetts Medical Society. All rights reserved.
-
7/28/2019 16. Enfermedad Inflamatoria Intestinal
13/13
MEDICAL PROGRESS
N Engl J Med, Vol. 347, No. 6 August 8, 2002 www.nejm.org 429
of a humanized A4B7 antibody in ulcerative colitis (UC). Gastroenterology2000;118:Suppl 2:A874. abstract.89. Hommes D, van den Blink B, Plasse T, et al. Inhibition of stress-acti-
vated MAP kinases induces clinical improvement in moderate to severeCrohns disease. Gastroenterology 2002;122:7-14.90. Slonim AE, Bulone L, Damore MB, Goldberg T, Wingertzahn MA,McKinley MJ. A preliminary study of growth hormone therapy for Crohns
disease. N Engl J Med 2000;342:1633-7.91. Sandborn WJ, Tremaine WJ, Offord KP, et al. Transdermal nicotine formildly to moderately active ulcerative colitis: a randomized, double-blind,placebo-controlled tr ial. Ann Intern Med 1997;126:364-71.
92. Belluzzi A, Brignola C, Campieri M, Pera A, Boschi S, Miglioli M.Effect of an enteric-coated fish-oil preparation on relapses in Crohns dis-ease. N Engl J Med 1996;334:1557-60.93. Lewis JD, Lichtenstein GR, Stein RB, et al. An open-label trial of thePPAR-gamma ligand rosiglitazone for active ulcerative colitis. Am J Gas-troenterol 2001;96:3323-8.94. Lopez-Cubero SO, Sullivan KM, McDonald GB. Course of Crohns
disease after allogeneic marrow transplantation. Gastroenterology 1998;114:433-40.
Copyright 2002 Massachusetts Medical Society.
POSTING PRESENTATIONS AT MEDICAL MEETINGS ON THE INTERNET
Posting an audio recording of an oral presentation at a medical meeting on theInternet, with selected slides from the presentation, will not be considered priorpublication. This will allow students and physicians who are unable to attend themeeting to hear the presentation and view the slides. If there are any questionsabout this policy, authors should feel free to call the Journals Editorial Offices.
Downloaded from www.nejm.org by PEDRO MAGGIOLO on March 31, 2004.