DOLOR ABDOMINAL PRIMARIA...DIAGNOSTICO DEFINITIVO DEL DOLOR ABDOMINAL REMITIDO DESDE ATENCIÓN...
19
DOLOR ABDOMINAL CRÓNICO MANEJO Y CRITERIOS DE DERIVACIÓN. ROSMARI VÁZQUEZ GOMIS Octubre 2019 Hospital General universitario de Elche
Transcript of DOLOR ABDOMINAL PRIMARIA...DIAGNOSTICO DEFINITIVO DEL DOLOR ABDOMINAL REMITIDO DESDE ATENCIÓN...
DOLOR ABDOMINAL CRÓNICO MANEJO Y CRITERIOS DE
DERIVACIÓN.
ROSMARI VÁZQUEZ GOMISOctubre 2019
Hospital General universitario de Elche
• Síntomas agudos que pueden ser mas o menos intensos
• Cuadro extenso dx diferencial
DOLOR ABDOMINAL
AGUDO
DOLOR ABDOMINAL PERSISTENTE
DOLOR ABDOMINAL
CRÓNICOMÁS DE 2 MESES DE EVOLUCIÓN

TODO DOLOR ABDOMINAL CRONICO TIENE QUE LLEGAR A UN DIAGNÓSTICO
PRIMARIA ESPECIALIZADA

¿PUEDE EL PEDIATRA DE ATENCIÓN PRIMARIA LLEGAR A UN DIAGNÓSTICO DE ESE DOLOR ABDOMINAL CRÓNICO?

TRASTORNOS FUNCIONALES DIGESTIVOS• Los trastornos funcionales se definen como una asociación
de síntomas gastrointestinales crónicos o recurrentes no explicados por alteraciones estructurales, bioquímicas o metabólicas.
• Constituyen un espectro amplio de enfermedades, incluyendo algunas que se relacionan con el nivel de desarrollo madurativo normal de los niños.
• ¿NO CAUSA=FUNCIONAL ?
HISTORIA DE LOS TFD
Consensos�de�RomaConsensos�de�Roma
ROMA�IIROMA�II1999�1999�((GutGut)) ROMA�IIIROMA�III
20062006((GastroenterologyGastroenterology))
ROMA�IROMA�I19941994
ROMA�IVROMA�IV????
1º Clasificaciónde�TFD1990
1º Criteriosde�SII1989
ROMA IV
2016

PREVALENCIA TFDpatients who had their initial diagnosisconfirmed at the end of the follow-upperiod.
RESULTS
Among 9291 children examined once inthe first 3 months of enrollment by 21pediatricians, 261 (2.8%) met theRome II criteria and were included inthe study. Ten patients (3.8%) werelost at follow-up. In all cases but 4 (1celiac disease, 1 ascaridiasis, 1 giardi-asis, and 1 gastroesophageal refluxdisease), diagnosis of FGIDs was con-firmed at the end of follow-up (98.4%).The distribution of each disorderamong 247 patients with FGIDs at theend of follow-up are shown in Table 2.
For 3 patients, the diagnosis of FGIDswas changed at the end of follow-upperiod: 2 with initial diagnosis of func-tional abdominal pain, and 1 with dys-pepsia were given a diagnosis of IBS.
Constipation was the most commondisorder. Two patients underwent pan-colonoscopy and rectosigmoidoscopy,
respectively, for rectal bleeding, and in1 patient, nodular lymphoid hyperpla-sia was found. All patients weretreated with polyethylene glycol or lac-tulose. Among 11 patients with func-tional fecal retention, who were on av-erage older than those patients withfunctional constipation, 4 had poor
compliance with treatment, with noimprovement in 2 of them.
The second most common disorderwas functional abdominal pain. Thelargest number of instrumental inves-tigations was recorded in this group:20 abdominal ultrasounds; 3 bariumradiograph digestive tract completeseries; and 1 upper gastrointestinalendoscopy. In this latter patient, a di-agnosis of gastroesophageal refluxesophagitis was given. Four childrenhad alarm symptoms (2 lateral local-ized pain, 1 poor growth, and 1 famil-ial history of inflammatory bowel dis-ease): in all but 1 (who moved tothe IBS group) the diagnosis wasconfirmed.
The third most common disorder wasinfant regurgitation. This is an exam-ple of gastroesophageal reflux. Whenthe latter causes or contributes totissue damage or inflammation (eg,esophagitis, obstructive apnea, reac-tive airway disease, pulmonary aspira-
TABLE 1 Definition of Compliance With Diagnostic and Therapeutic Protocols of FGID in Children
Disorders Laboratory Examination Instrumental Examination Drugs
Infant regurgitation None None No drugFunctional constipation None None Macrogol for fecal impaction; macrogol
or lactulose for maintenanceFunctional dyspepsia Amylase, lipase, aminotransferase, htTG
for allAcceptable: abdominal ultrasound Anti-H2 blockers or proton-pump
inhibitor drugs; acceptable:domperidone
Functional abdominalpain
Blood cell count, ESR, urinalysis, fecalsearch of ova and parasites, humantissue transglutaminase antibodies forall
Acceptable: abdominal ultrasound No drug
IBS Blood cell count, ESR, search of ova,parasites and microbes, human tissuetransglutaminase antibodies for allOptional: fecal calprotectin
In complicated cases: colonoscopy with biopsy Macrogol for fecal impaction; macrogolor lactulose for maintenance
Functional fecalretention
None None Macrogol for fecal impaction; macrogolor lactulose for maintenance
Functional diarrhea Not mandatory: blood cell count, ESR,urine test, search of ova andparasites, human tissuetransglutaminase antibodies
None No drug; acceptable: empiricaltreatment with 1 dose of tinidazole
Cyclic vomitingsyndrome
Serum glucose, urea, aminotransferases,amylase, lipase, electrolyte, lactic acid,pyruvic acid, creatine phosphokinase,ammonium, acid-base equilibrium
After referral to tertiary level centre for uppergastrointestinal contrast radiographstudies, abdominal ultrasound, uppergastrointestinal endoscopy, brain MRI, atdiscretion of senior gastroenterologist
No validated drug; at the beginning, atrial with gastric acid inhibitors andlorazepam was allowed
ESR indicates erythrocyte sedimentation rate.
TABLE 2 FGID Distribution in Study Population
Disorder No. ofChildren
% ofPopulation
%AmongFGID
Functionalconstipation
92 0.99 37.24
Functionalabdominalpain
58 0.62 23.48
Infantregurgitation
41 0.44 16.59
Functionaldyspepsia
20 0.21 8.09
IBS 13 0.14 5.26Functional fecalretention
11 0.11 4.45
Functionaldiarrhea
7 0.07 2.83
Cyclic vomitingsyndrome
5 0.05 2.02
Total 247 2.63 100
ARTICLES
PEDIATRICS Volume 125, Number 1, January 2010 e157 at H Universitario La Fe on October 12, 2014pediatrics.aappublications.orgDownloaded from
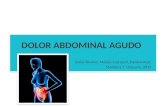
Prevalencias de�TFD/ Estudio�multicéntrico/ 13�pediatras/ n=�9660�niños�/ Período�de�estudio:�3�meses/ Seguimiento:�1�3�12�meses/ Rango�edad:�0�12�años/ TFD:�194�niños/ A�los�12�meses�97.5%�continuaban�
cumpliendo�criterios�de�Roma�II.
MieleMiele E,�E,�StaianoStaiano A�et�al.�A�et�al.�PediatricsPediatrics 20042004
/ Estudio�multicéntrico/ 21�pediatras/ n=�9291�niños�/ Período�de�estudio:�3�meses/ Seguimiento:�1�3�12�meses/ Rango�edad:�0�14�años/ TFD:�261�niños/ A�los�12�meses�98.4%�continuaban�
cumpliendo�criterios�de�Roma�II.
Primavera�G�et�al.�Primavera�G�et�al.�PediatricsPediatrics 20102010
ESTUDIO MULTICÉNTRICO21 PEDIATRASN= 9291 niñosPeriodo de estudio: 3 mesesSeguimiento:1-3-12 mesesRango de edad:0-14 añosTFD: 247 niños
TFD 2,6%
A los 12 meses 98,4%, continuaban cumpliendo Roma III
DOI: 10.1542/peds.114.1.73 2004;114;73Pediatrics
Steven J. Novek and Annamaria StaianoErasmo Miele, Domenico Simeone, Antonio Marino, Luigi Greco, Renata Auricchio,
Functional Gastrointestinal Disorders in Children: An Italian Prospective Survey
http://pediatrics.aappublications.org/content/114/1/73.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2004 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Hospital Lluis Alcanyis on October 12, 2014pediatrics.aappublications.orgDownloaded from at Hospital Lluis Alcanyis on October 12, 2014pediatrics.aappublications.orgDownloaded from
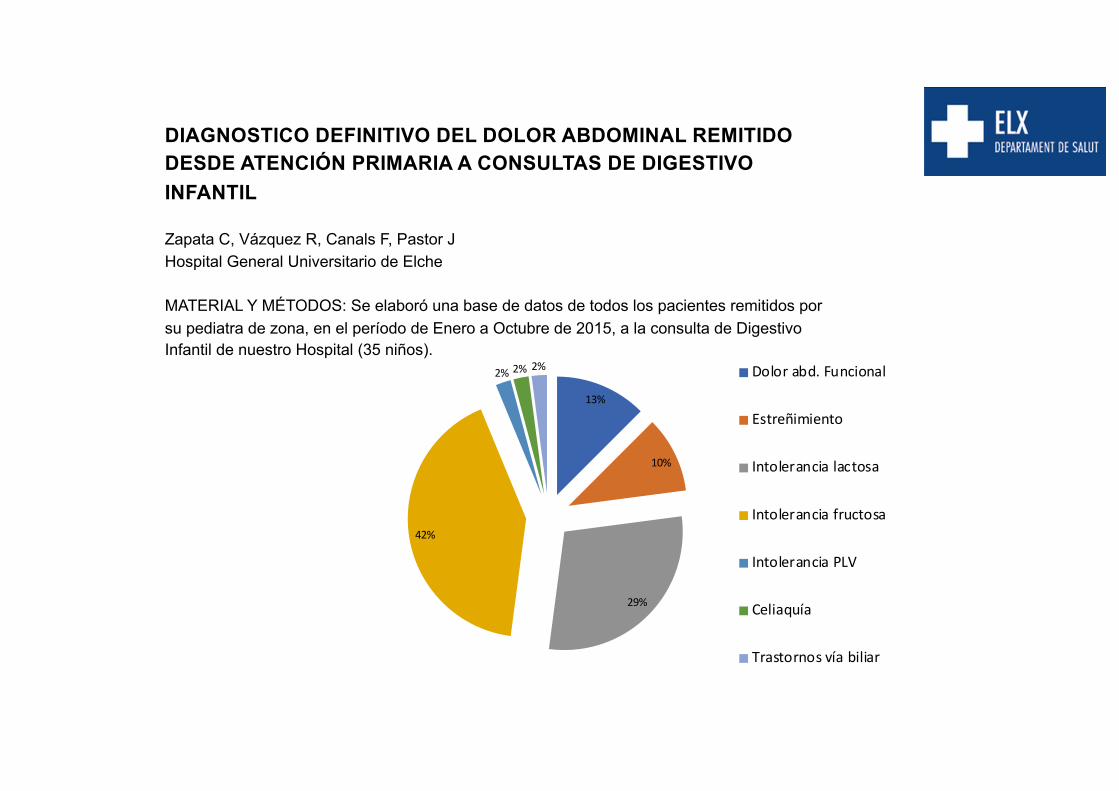
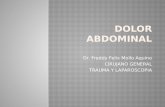
DIAGNOSTICO DEFINITIVO DEL DOLOR ABDOMINAL REMITIDO DESDE ATENCIÓN PRIMARIA A CONSULTAS DE DIGESTIVO INFANTIL
Zapata C, Vázquez R, Canals F, Pastor JHospital General Universitario de Elche
MATERIAL Y MÉTODOS: Se elaboró una base de datos de todos los pacientes remitidos por su pediatra de zona, en el período de Enero a Octubre de 2015, a la consulta de Digestivo Infantil de nuestro Hospital (35 niños).
13%
10%
29%
42%
2% 2% 2% Dolor abd. Funcional
Estreñimiento
Intolerancia lactosa
Intolerancia fructosa
Intolerancia PLV
Celiaquía
Trastornos vía biliar

G1 Regurgitación del lactante
G2 Síndrome de rumiación
G3 Síndrome de vómitos cíclicos
G4 Cólico del lactante
G5 Diarrea funcional
G6 Disquecia del lactante
G7 Estreñimiento funcional
TRASTORNOS FUNCIONALES NIÑO 1-4 AÑOS. ROMA IV IV
CLASIFICACIÓN DE LOS TFD

TRASTORNOS FUNCIONALES MAYORES DE 5 AÑOS Y ADOLESCENTES. ROMA IVV
Nauseas y vómitos
• Síndrome de vómitos cíclicos• Nauseas funcionales y vómitos funcionales• Síndrome de rumiación• Aerofagia
DOLOR ABDOMINAL
• Dispepsia funcional• Síndrome de intestino irritable• Migraña abdominal• Dolor abdominal funcional
DEFECACIÓN
• Estreñimiento funcional• Incontinencia fecal no retentiva
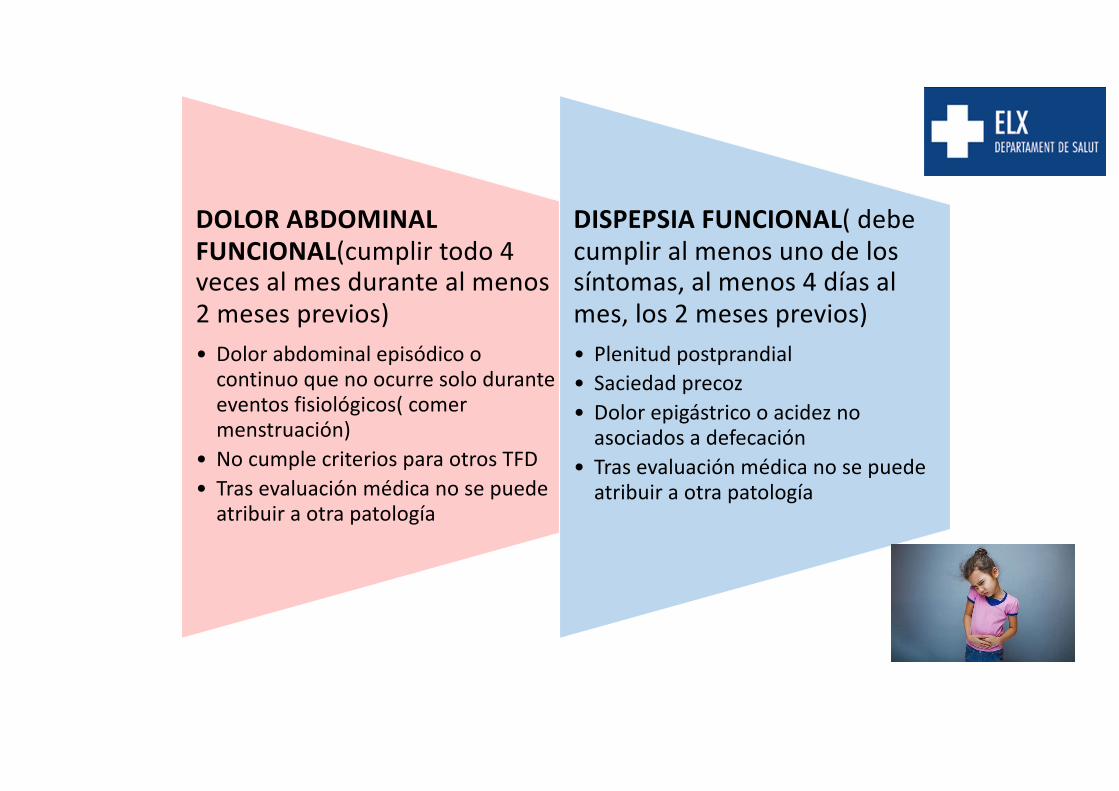
DOLOR ABDOMINAL FUNCIONAL(cumplir todo 4 veces al mes durante al menos 2 meses previos)• Dolor abdominal episódico o
continuo que no ocurre solo durante eventos fisiológicos( comer menstruación)
• No cumple criterios para otros TFD • Tras evaluación médica no se puede
atribuir a otra patología
DISPEPSIA FUNCIONAL( debe cumplir al menos uno de los síntomas, al menos 4 días al mes, los 2 meses previos)• Plenitud postprandial• Saciedad precoz• Dolor epigástrico o acidez no
asociados a defecación• Tras evaluación médica no se puede
atribuir a otra patología
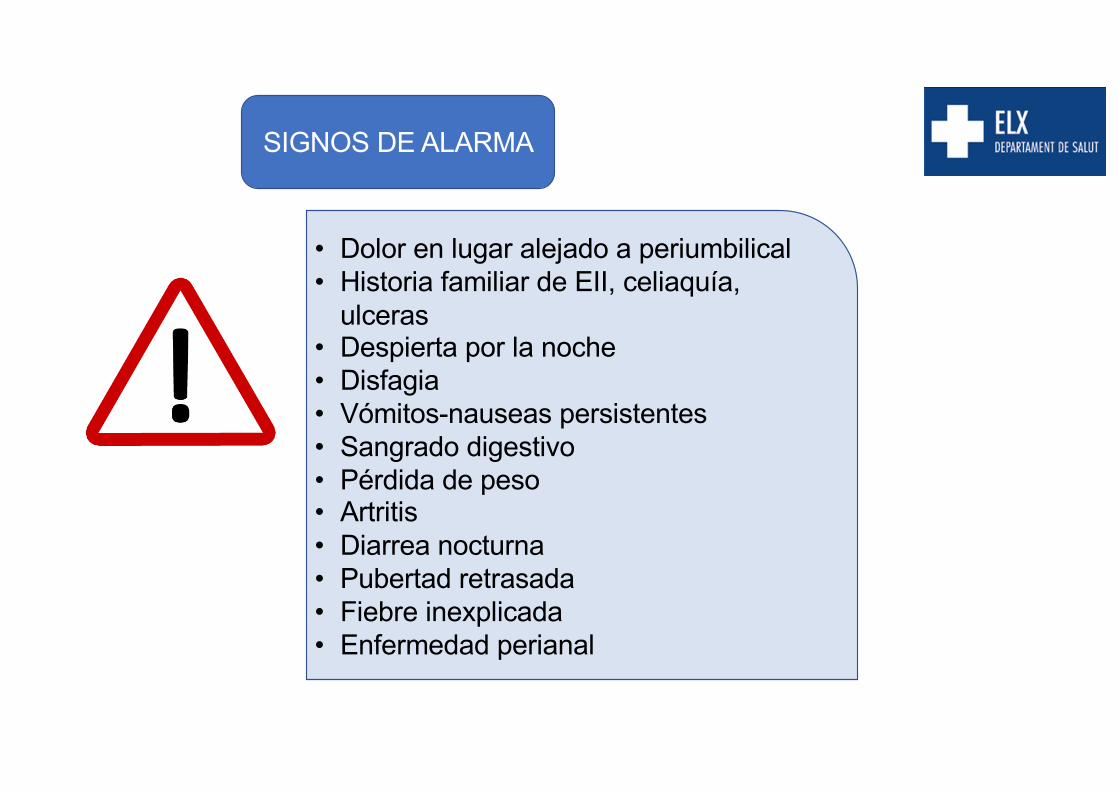
SIGNOS DE ALARMA
• Dolor en lugar alejado a periumbilical• Historia familiar de EII, celiaquía,
ulceras• Despierta por la noche• Disfagia• Vómitos-nauseas persistentes• Sangrado digestivo• Pérdida de peso• Artritis• Diarrea nocturna• Pubertad retrasada• Fiebre inexplicada• Enfermedad perianal
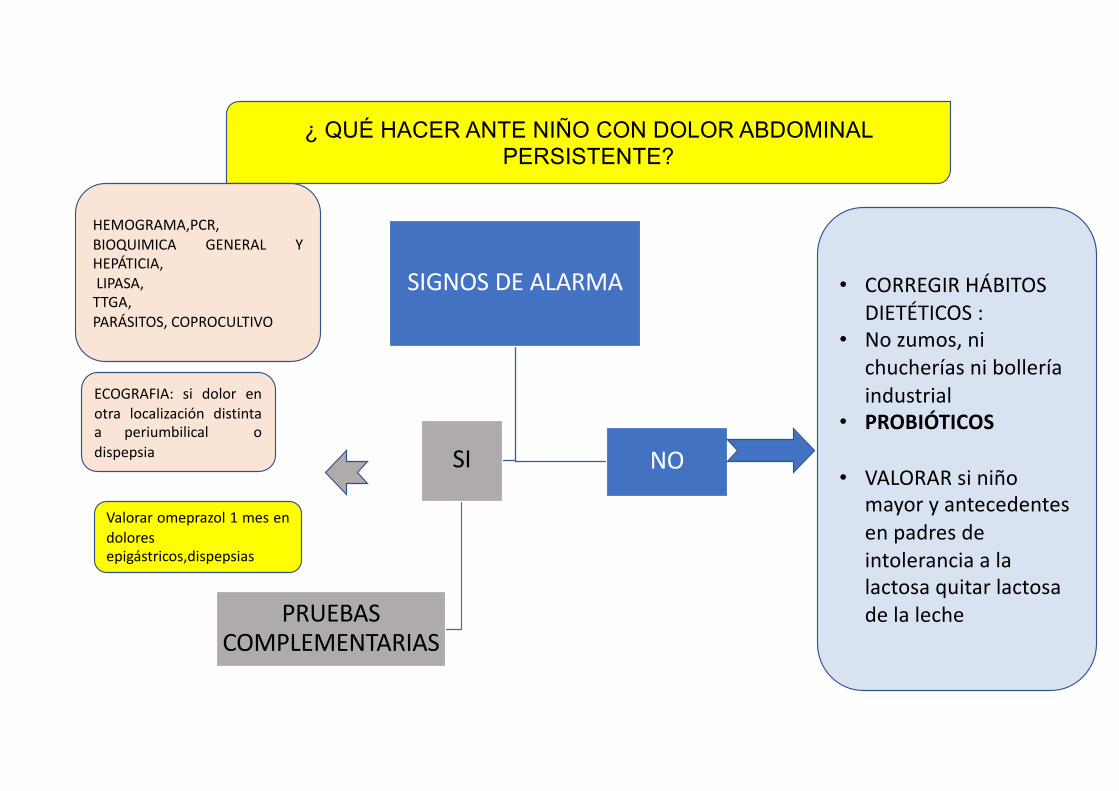
¿ QUÉ HACER ANTE NIÑO CON DOLOR ABDOMINAL PERSISTENTE?
SIGNOS DE ALARMA
SI
PRUEBAS COMPLEMENTARIAS
NO
HEMOGRAMA,PCR,BIOQUIMICA GENERAL YHEPÁTICIA,LIPASA,TTGA,PARÁSITOS, COPROCULTIVO
ECOGRAFIA: si dolor enotra localización distintaa periumbilical odispepsia
• CORREGIR HÁBITOS DIETÉTICOS :
• No zumos, ni chucherías ni bollería industrial
• PROBIÓTICOS
• VALORAR si niño mayor y antecedentes en padres de intolerancia a la lactosa quitar lactosa de la leche
Valorar omeprazol 1 mes endoloresepigástricos,dispepsias

¿ QUÉ HACER ANTE NIÑO CON DOLOR ABDOMINAL CRÓNICO?> 2 MESES
SIGNOS DE ALARMA
SI
PRUEBAS COMPLEMENTARIAS
REMITIR A DIGESTIVO
NO
HEMOGRAMA,PCRBIOQUIMICA GENERAL YHEPÁTICIALIPASA,TTGA,PARÁSITOS, COPROCULTIVO
ECOGRAFIA: si dolor enotra localizacióndistinta a periumbilical/epigastrico
• CORREGIR HÁBITOS DIETÉTICOS :
• No zumos, ni chucherías ni bollería industrial
• PROBIÓTICOS
• VALORAR si niño mayor y antecedentes en padres de intolerancia a la lactosa quitar lactosa de la leche

¿CUÁNDO PEDIR HELICOBACTER PILORY EN UN DOLOR ABDOMINAL?
CASI NUNCA¡¡¡¡¡¡
• Recordar que en niños en principio no se hace el test and treat. HABRÍA QUE HACER ENDOSCOPIA ....
• Aunque esté el HP ,El dolor abdominal la mayor parte de las veces no lo causa el HP, independientemente de discutir si es bueno o no tener HP....
• SÓLO PEDIRLO EN DOLORES TIPO ULCEROSOS , EPIGÁSTRICOS.

¿CUÁNDO PEDIR CALPROTECTINA EN UN DOLOR ABDOMINAL?
POCAS VECES¡¡¡¡¡¡
• CUANDO SOSPECHES UNA ENFERMEDAD DE CROHN O COLITIS ULCEROSA
• NIÑOS MENORES DE 6 AÑOS TIENEN VALORES MÁS ALTOS
• INESPECÍFICO, SE ELEVA EN INTOLERANCIAS , INFECCIONES....

Y DESPUÉS DEL DIAGNÓSTICO POR DIGESTIVO INFANTIL, ALTA Y CONTROL POR PEDIATRA EN ESTOS CASOS
• DOLOR ABDOMINAL FUNCIONAL• ESTREÑIMIENTO FUNCIONAL• DISPEPSIA FUNCIONAL• PARASITOSIS• SOBRECRECIMIENTO BACTERIANO• MALABSORCIÓN/INTOLERANCIA A LA LACTOSA• MALABSORCIÓN/INTOLERANCIA A FRUCTOSA
SEGUIMIENTO HOSPITALARIO:
• ENFERMEDAD INFLAMATORIA INTESTINAL• CELIAQUÍA• SINDROME DE INTESTINO IRRITABLE/MIGRAÑA
ABDOMINAL/VÓMITOS CÍCLICOS• INTOLERANCIA A LA HISTAMINA• INTOLERANCIA A FRUCTOSA CON MAL CONTROL DE
SINTOMAS Y/O CON DEFICIT NUTRICIONALES• PATOLOGÍA HEPATICA, PANCREATICA Y BILIAR

GRACIAS ¡¡¡¡¡¡