PTI-Henoch Schonlein
19
PURPURA TROMBOCITOPENICA IDIOPÁTICA( TROMBOCITOPENIA INMUNE) - PURPURA DE SCHÖNLEIN - HENOCH Cátedra de pediatría Universidad de Nariño Alvaro Javier Córdoba Villota
-
Upload
alvaro-cordoba-villota -
Category
Healthcare
-
view
138 -
download
0
Transcript of PTI-Henoch Schonlein

PURPURA TROMBOCITOPENICA IDIOPÁTICA(TROMBOCITOPENIA INMUNE)-PURPURA DE SCHÖNLEIN-HENOCH
Cátedra de pediatría Universidad de NariñoAlvaro Javier Córdoba Villota
PTI- Generalidades
• Resolución
• 3-6 mesesBenigno
Común
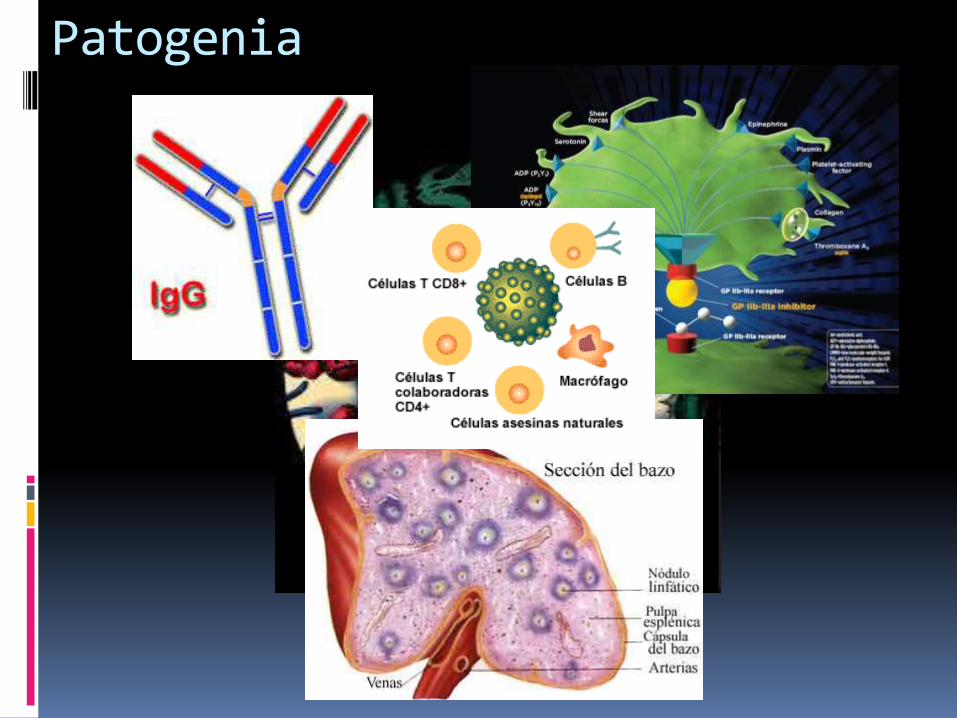
Patogenia
Epidemiologia
2-5 años
1-6.4
80%<8
Sexo

Manifestaciones Clínicas

Examen físico
Evolución de la enfermedad
●Newly diagnosed ITP – ITP within three months from diagnosis
●Persistent ITP –Ongoing ITP between 3 and 12 months from the initial diagnosis
●Chronic ITP – ITP lasting for more than 12 months
http://www.uptodate.com.sci-hub.org/contents/immune-thrombocytopenia-itp-in-children-clinical-manifestations-and-diagnosis?source=search_result&search=itp&selectedTitle=3~150

Diagnostico
• Platelet count <100,000/microL (often <20,000/microL).
• Otherwise normal complete blood count (CBC) with differential white count, and reticulocyte count
• No abnormalities on the peripheral blood smear after review by an experienced practitioner. In particular, there should be no evidence of hemolysis or of blast cells
• No clinically apparent associated conditions that may cause thrombocytopenia, after a thorough history and physical examination. Findings that suggest a diagnosis other than ITP include enlargement of lymph nodes, liver, or spleen; systemic symptoms

Manejo

Manejo

Indicaciones tto farmacológico
●NO pharmacologic intervention ("watchful waiting") formost children with no bleeding or mild bleeding (defined asskin manifestations only, such as bruising and petechiae),regardless of platelet count.
●Pharmacologic intervention for any child with severe orlife-threatening bleeding (eg, severe or prolongedepistaxis, gastrointestinal bleeding, or intracranialhemorrhage [ICH]); this occurs in about 3 percent ofchildren with ITP. These patients also should be admitted tothe hospital for treatment and monitoring. Patients withhead trauma or suspected ICH also should be urgentlyevaluated with computerized tomography (CT) of the head
Opciones farmacológicas
Inmunoglobulinas intravenosas (IGIV). Las IGIV en dosis de 0,8-1 g/kg/día durante 1 o 2 días
Tratamiento anti-D intravenoso i.v. de 50-75 mg/kg de anti-D a pacientes Rh positivos
1-4 mg/kg/24 horas de prednisona induce una elevación del recuento plaquetario
Purpura de SCHÖNLEIN-HENOCH
Vasculitis IgA
90%Auto
limitada
Patogenia

Manifestaciones Clínicas

Diagnostico Diferencial
El edema hemorrágico agudo (EHA
Manejo
Medidas generales
Prednisona Segumiento