Servicio Medicina Interna CAULE - … · Protocolos y guías clínicas de NeumoSur.
Servicio de Medicina In
terna CAULE
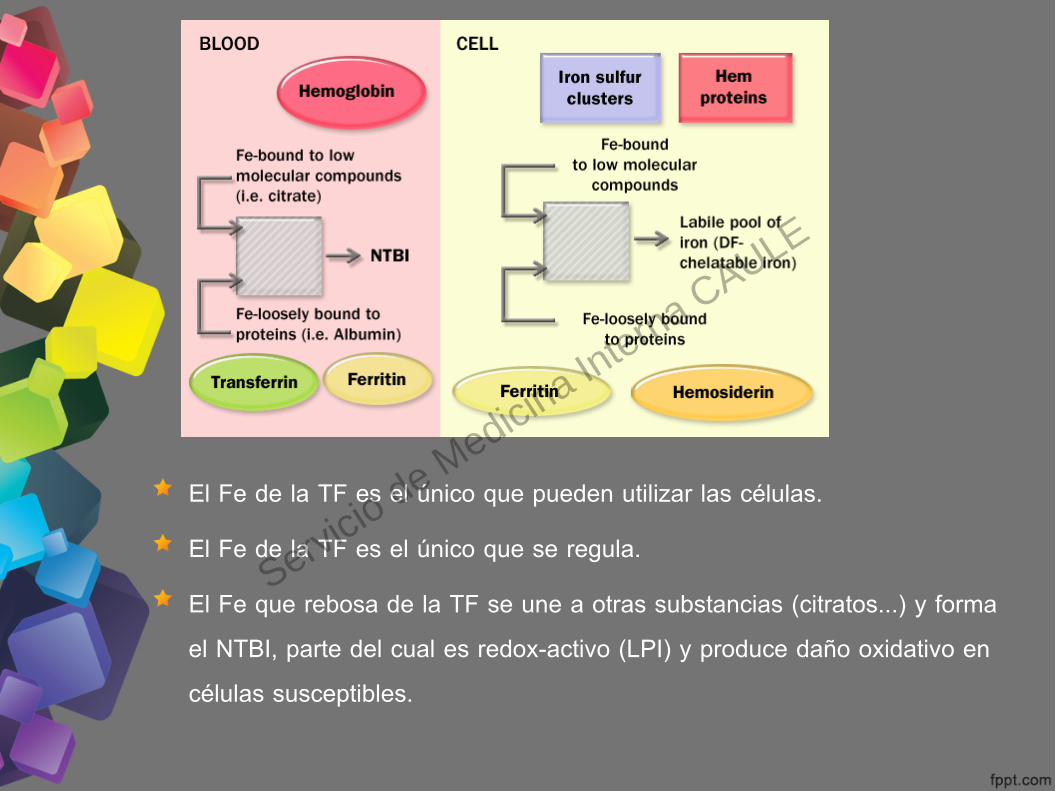
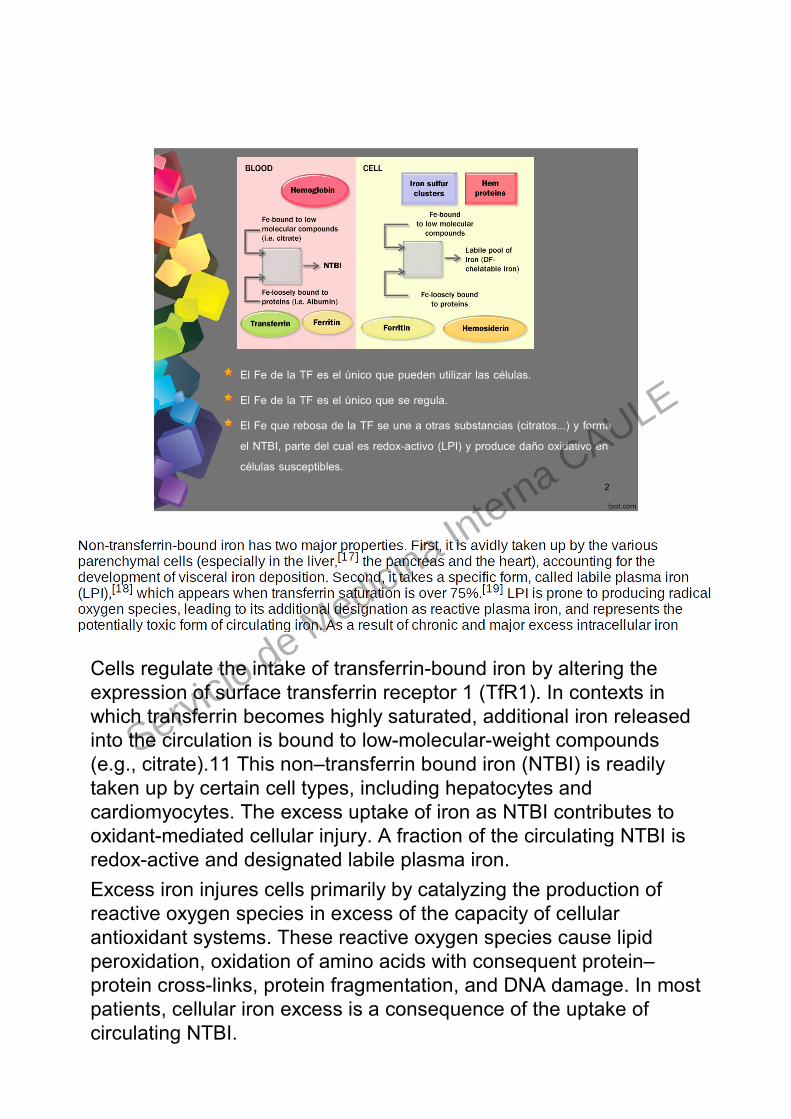
El Fe de la TF es el único que pueden utilizar las células.El Fe de la TF es el único que se regula.El Fe que rebosa de la TF se une a otras substancias (citratos...) y forma el NTBI, parte del cual es redox-activo (LPI) y produce daño oxidativo en células susceptibles.
Servicio de Medicina In
terna CAULE
Servicio de Medicina In
terna CAULE

Servicio de Medicina In
terna CAULE
Servicio de Medicina In
terna CAULE
Servicio de Medicina In
terna CAULE
Servicio de Medicina In
terna CAULE
Regulación de la hepcidina
Servicio de Medicina In
terna CAULE
Servicio de Medicina In
terna CAULE

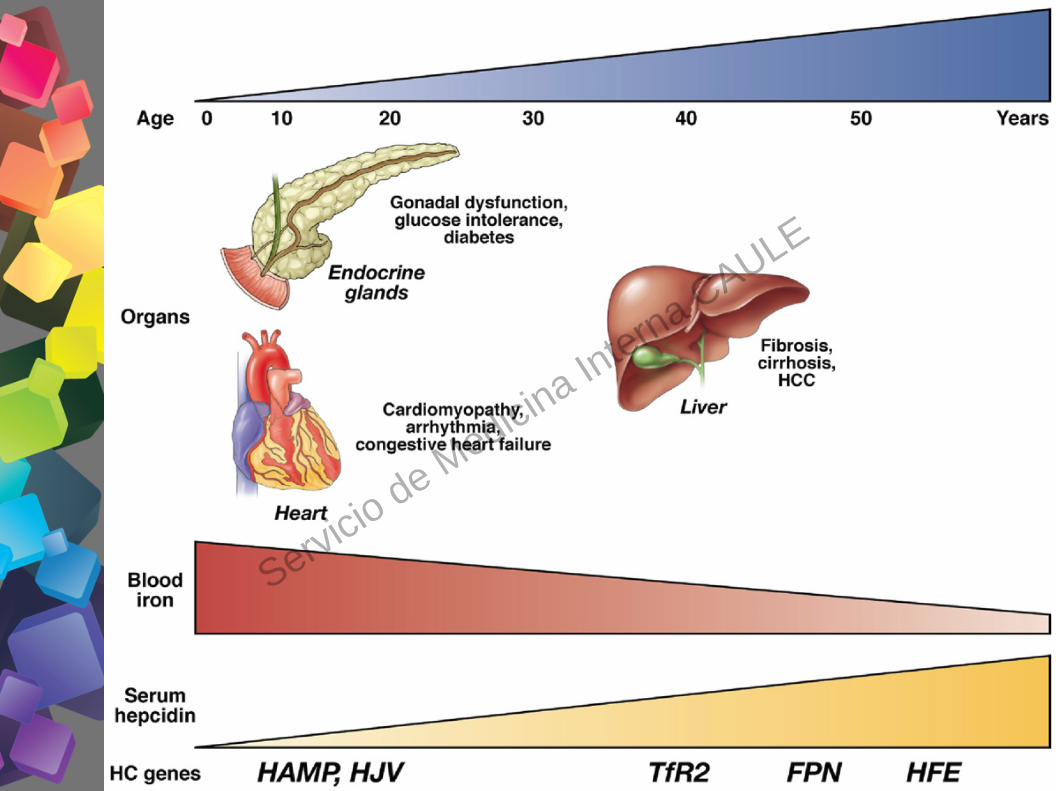
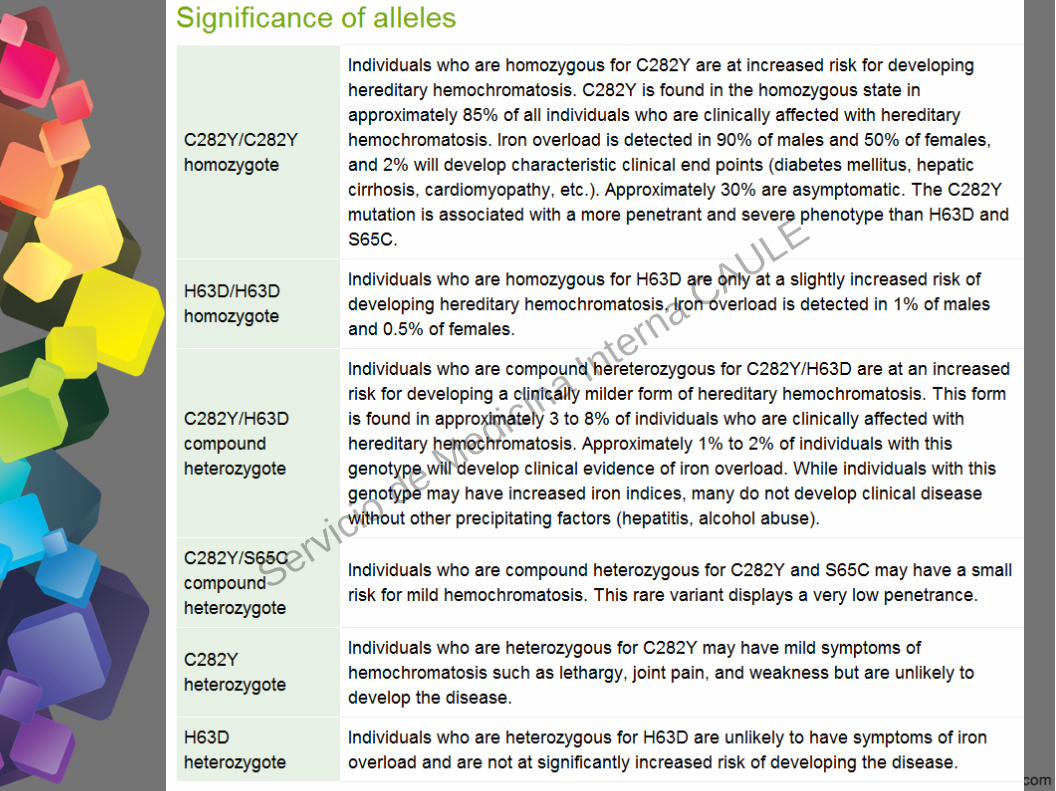
El 10% de la población blanca es portadora del gen C282Y.Penetrancia bioquímica del C282Y +/+ del 36-76%.Penetrancia de la enfermedad del C282Y +/+ del 2-38% en ♂ y del 1-10% en .♀El H63D ocasiona sobrecarga férrica solo si coincide con otra mutación trascendente (p. ej.: H63D/C282Y).
Servicio de Medicina In
terna CAULE

Servicio de Medicina In
terna CAULE
Servicio de Medicina In
terna CAULE

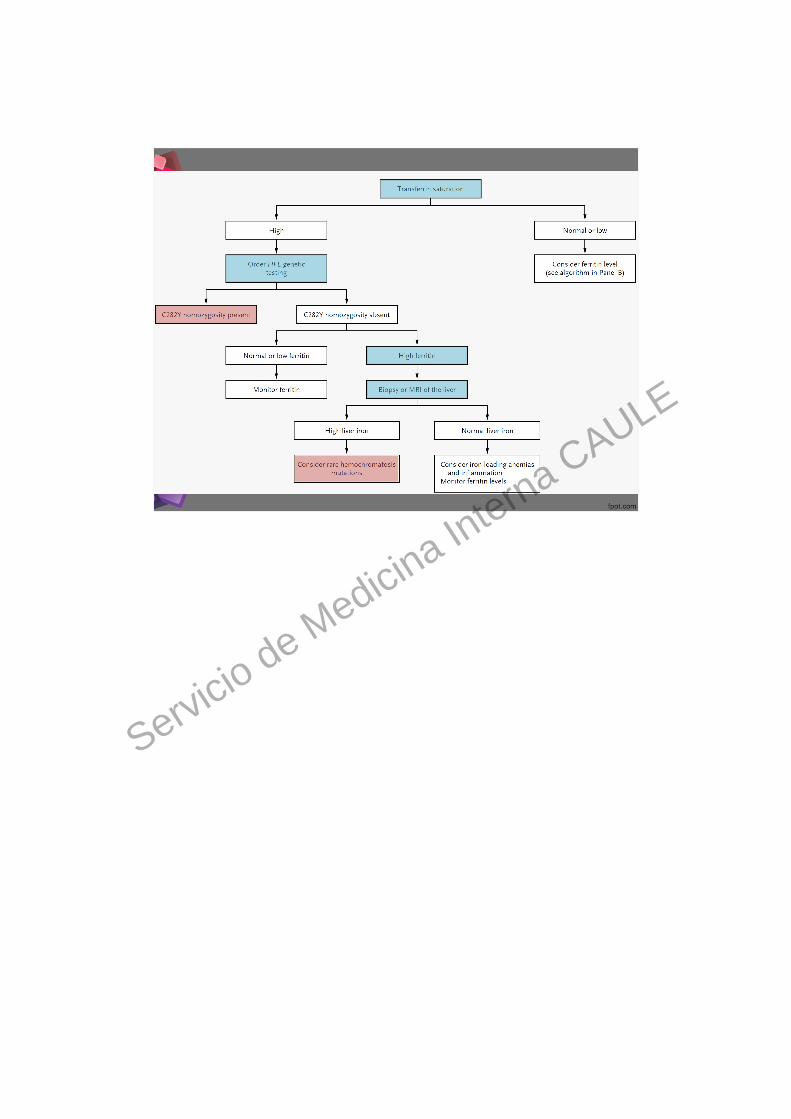
SEÑALES DE ALARMAFerritina >200 ng/ml en mujeres ó 300 ng/ml en varones.%TF >45% en + ó >50 en varones (más sensible y especifica).↓ hepcidina: para el futuro (marcador genético subrogado).
SITUACIONES CONCRETASSITUACIONES CONCRETAS↑ Ferritina + ↓ %TF: Descartar inflamación, autoinmunes, neoplasias, ERC, hepatopatias, alcoholismo, s. metabólico ⇒ la %TF suele ser normal ó baja (RFA inverso).↑ Ferritina + ↓ %TF: no descarta del todo la HC. Formas aceruloplasminemia y mutaciones FP con PF (probable/ sin trascencencia).↑ Ferritina + ↑ %TF + C282Y/C282Y: HC.↑ Ferritina + ↑ %TF + C282Y/wt, H63D/wt, H63D/H63D, wt/wt ⇒ RM ó biópsia.
Servicio de Medicina In
terna CAULE

Servicio de Medicina In
terna CAULE

Servicio de Medicina In
terna CAULE
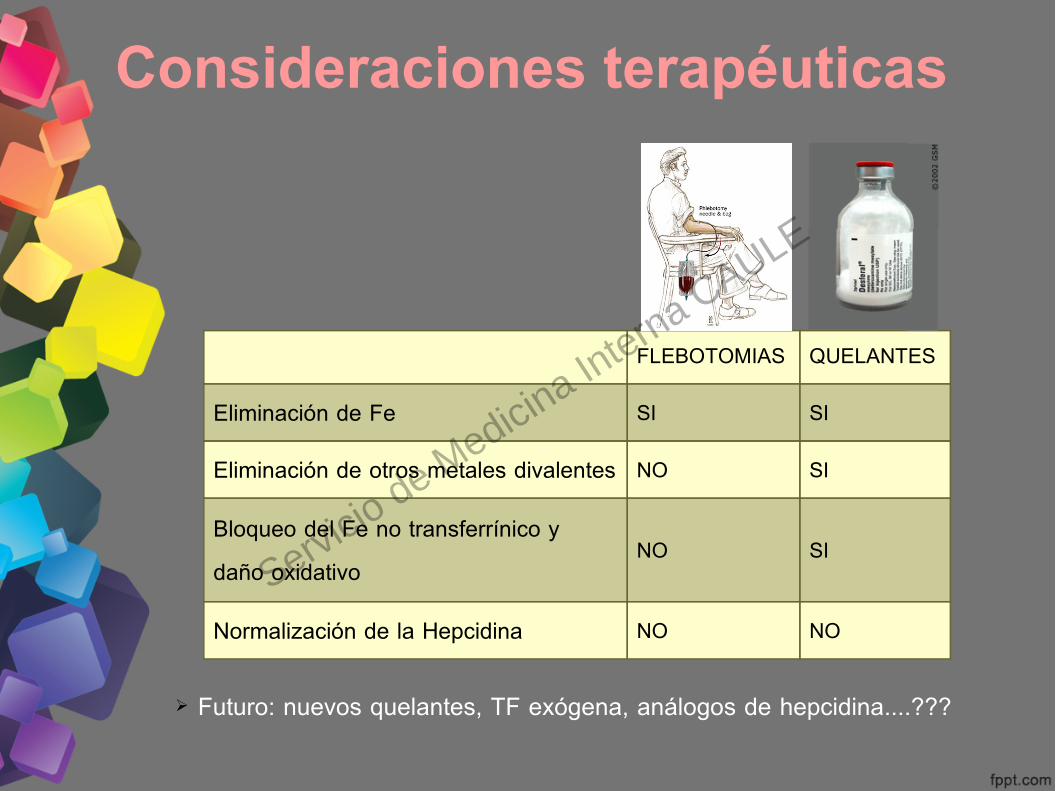
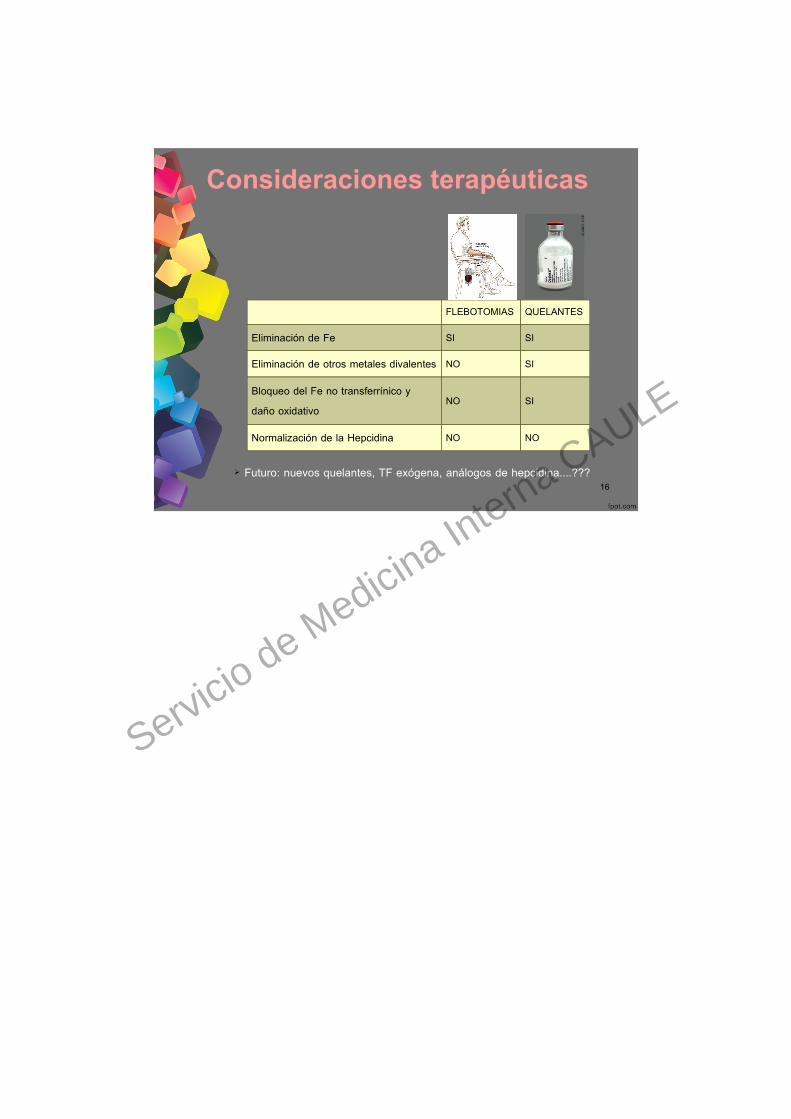
Consideraciones terapéuticas
FLEBOTOMIAS QUELANTES
Eliminación de Fe SI SI
Eliminación de otros metales divalentes NO SI
Bloqueo del Fe no transferrínico y daño oxidativo
NO SI
Normalización de la Hepcidina NO NO
➢ Futuro: nuevos quelantes, TF exógena, análogos de hepcidina....???
Servicio de Medicina In
terna CAULE

1
Servicio de Medicina In
terna CAULE
2
El Fe de la TF es el único que pueden utilizar las células.El Fe de la TF es el único que se regula.El Fe que rebosa de la TF se une a otras substancias (citratos...) y forma el NTBI, parte del cual es redox-activo (LPI) y produce daño oxidativo en células susceptibles.
Cells regulate the intake of transferrin-bound iron by altering the expression of surface transferrin receptor 1 (TfR1). In contexts in which transferrin becomes highly saturated, additional iron released into the circulation is bound to low-molecular-weight compounds (e.g., citrate).11 This non–transferrin bound iron (NTBI) is readily taken up by certain cell types, including hepatocytes and cardiomyocytes. The excess uptake of iron as NTBI contributes to oxidant-mediated cellular injury. A fraction of the circulating NTBI is redox-active and designated labile plasma iron.Excess iron injures cells primarily by catalyzing the production of reactive oxygen species in excess of the capacity of cellular antioxidant systems. These reactive oxygen species cause lipid peroxidation, oxidation of amino acids with consequent protein–protein cross-links, protein fragmentation, and DNA damage. In most patients, cellular iron excess is a consequence of the uptake of circulating NTBI.
Servicio de Medicina In
terna CAULE
3
Servicio de Medicina In
terna CAULE
4
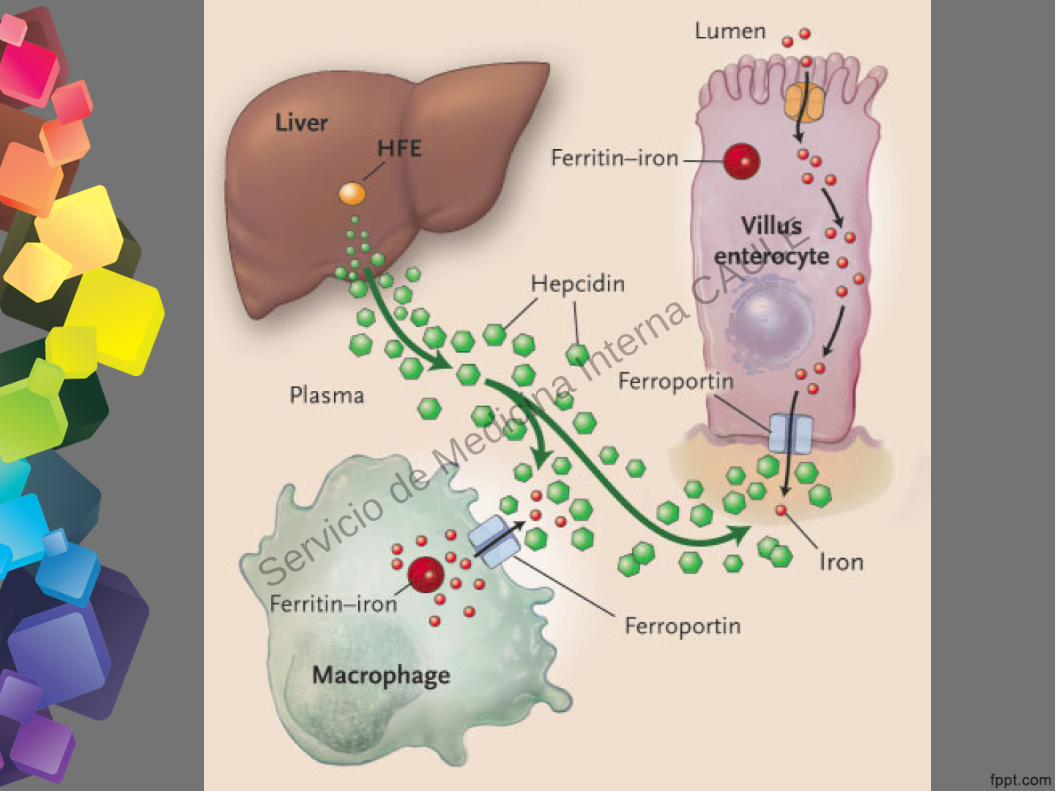
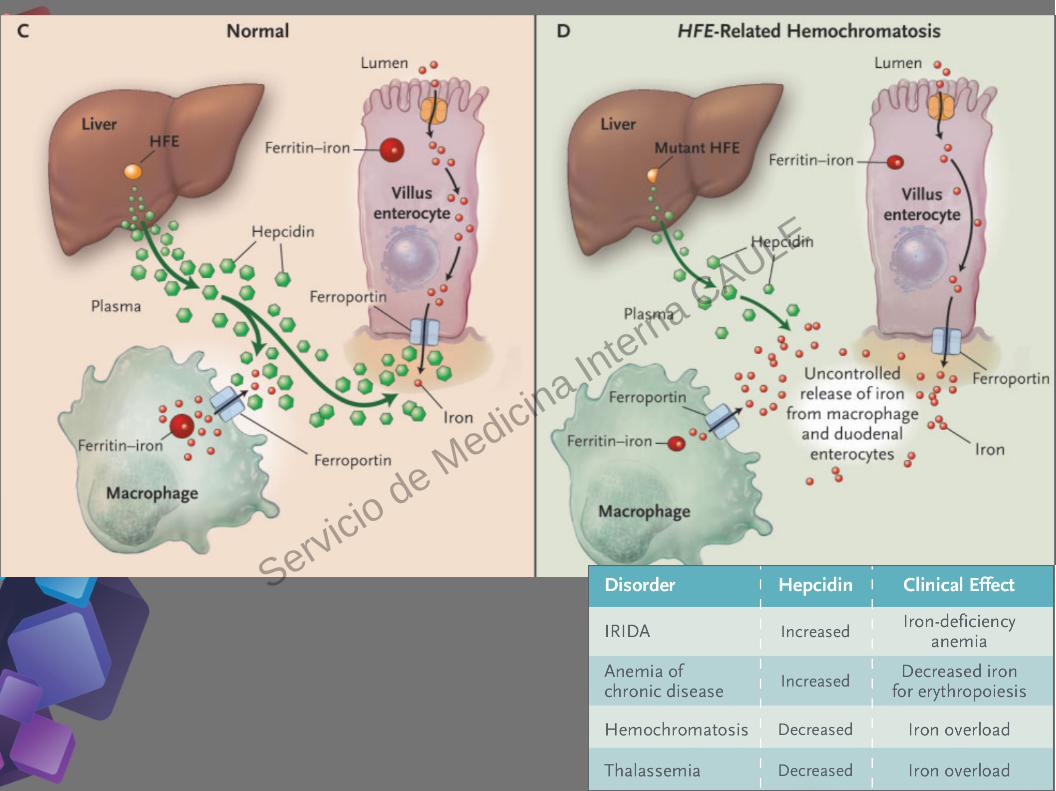
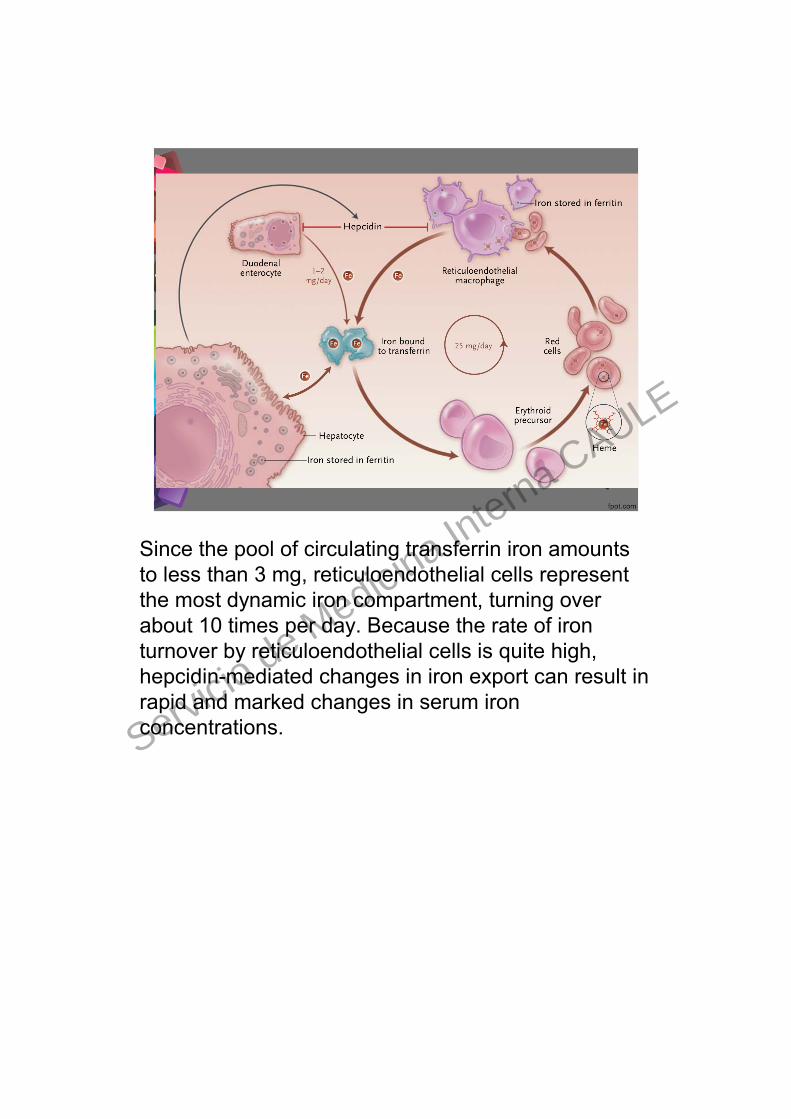
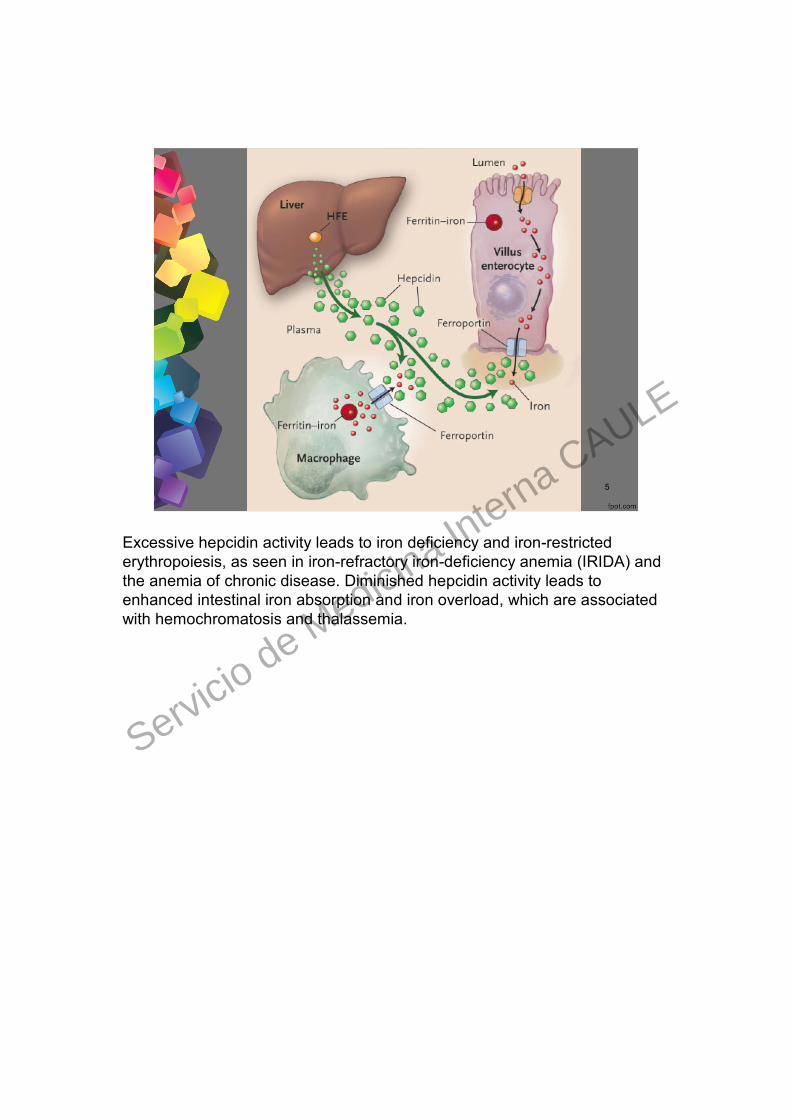
Since the pool of circulating transferrin iron amounts to less than 3 mg, reticuloendothelial cells represent the most dynamic iron compartment, turning over about 10 times per day. Because the rate of iron turnover by reticuloendothelial cells is quite high, hepcidin-mediated changes in iron export can result in rapid and marked changes in serum iron concentrations.Servicio de M
edicina Interna CAULE
5
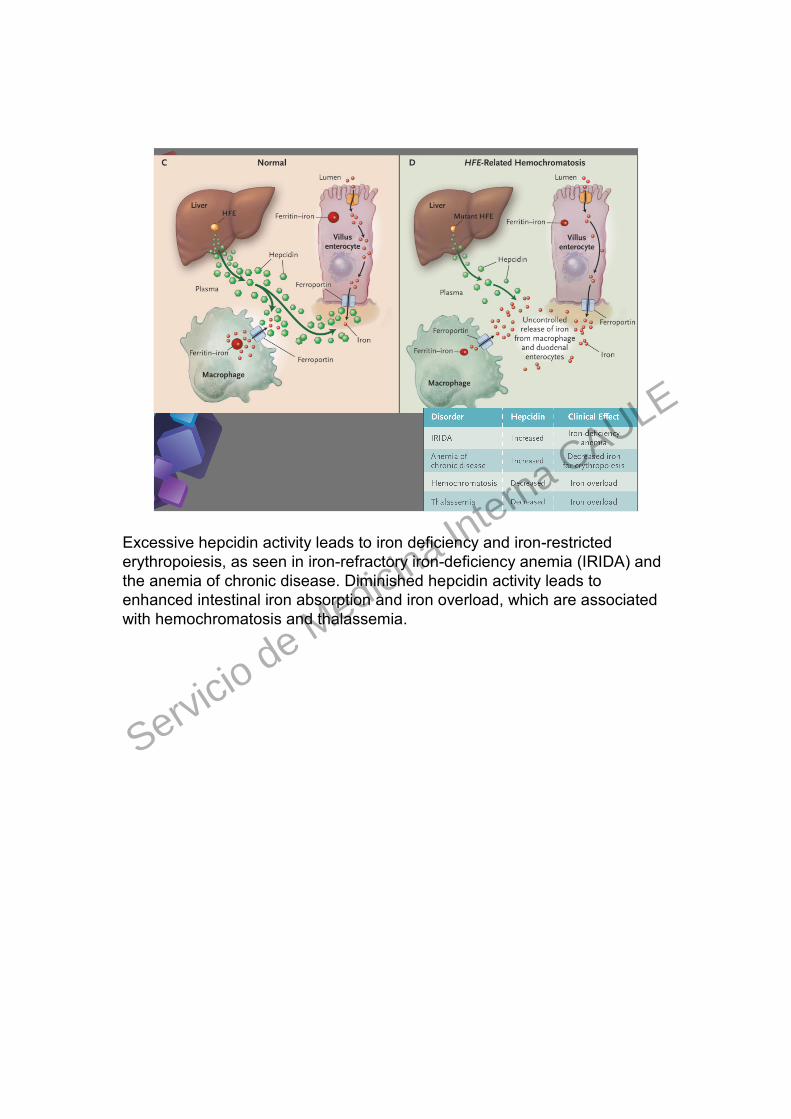
Excessive hepcidin activity leads to iron deficiency and iron-restricted erythropoiesis, as seen in iron-refractory iron-deficiency anemia (IRIDA) and the anemia of chronic disease. Diminished hepcidin activity leads to enhanced intestinal iron absorption and iron overload, which are associated with hemochromatosis and thalassemia.
Servicio de Medicina In
terna CAULE

6
Servicio de Medicina In
terna CAULE
7
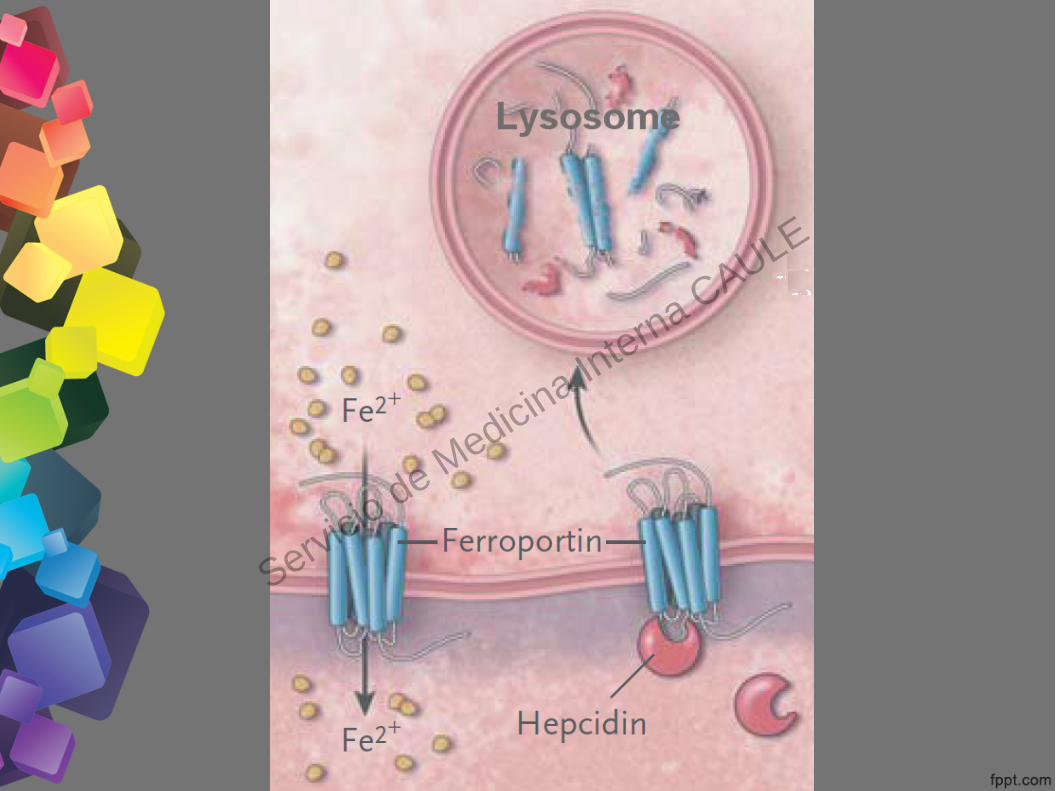
Excessive hepcidin activity leads to iron deficiency and iron-restricted erythropoiesis, as seen in iron-refractory iron-deficiency anemia (IRIDA) and the anemia of chronic disease. Diminished hepcidin activity leads to enhanced intestinal iron absorption and iron overload, which are associated with hemochromatosis and thalassemia.
Servicio de Medicina In
terna CAULE

8
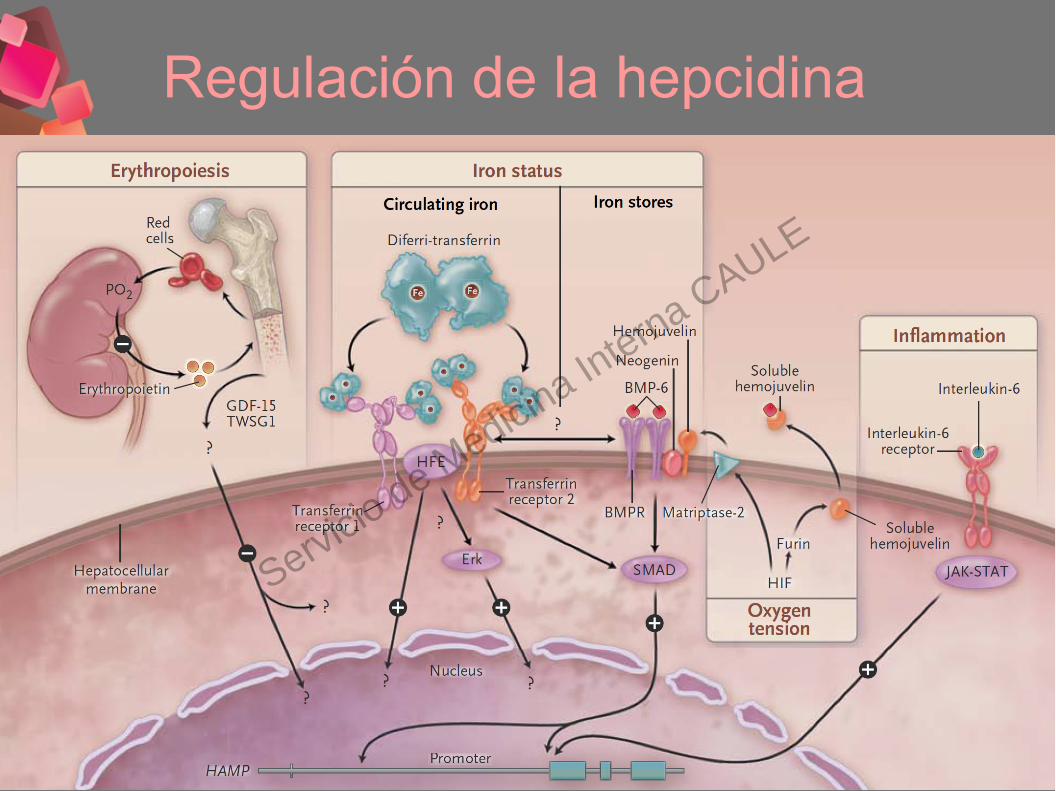
Regulación de la hepcidina
Four functionally defined hepcidin regulatory pathways are depicted: erythropoiesis, iron status, oxygen tension, and inflammation. Increased erythropoiesis is associated with decreased hepcidin expression by mechanisms that remain to be defined. Candidate signaling molecules from the marrow include growth differentiation factor 15 (GDF-15) and twisted gastrulation protein homolog 1 (TWSG1). Increased body iron status increases hepcidin expression through two mechanisms: a circulating-iron signal provided by ferri-transferrin and a cellular-iron-stores signal provided by bone morphogenetic protein 6 (BMP-6). The ferri-transferrin signal acts through transferrin receptors 1 and 2 and is modulated by the hemochromatosis protein HFE. The BMP-6 signal acts through its receptor and is modulated by the BMP coreceptor hemojuvelin and by neogenin. Decreased oxygen tension leads to decreased hepcidin expression by increasing the transcription of two genes, matriptase-2 and furin, that are responsive to hypoxia-inducible factor (HIF). Matriptase-2 cleaves hemo juvelin from the cell surface, preventing its function as a coreceptor. Furin cleaves hemojuvelin during processing to produce a soluble form that serves as a BMP-6 decoy. Infections and other forms of inflammation increase hepcidin expression by the cytokine interleukin-6. BMPR denotes bone morphogenetic protein receptor, HAMP hepcidin gene, JAK-STAT Janus-associated kinase–signal transducers and activators of transcription, and PO2 partial pressure of oxygen.
Servicio de Medicina In
terna CAULE
9
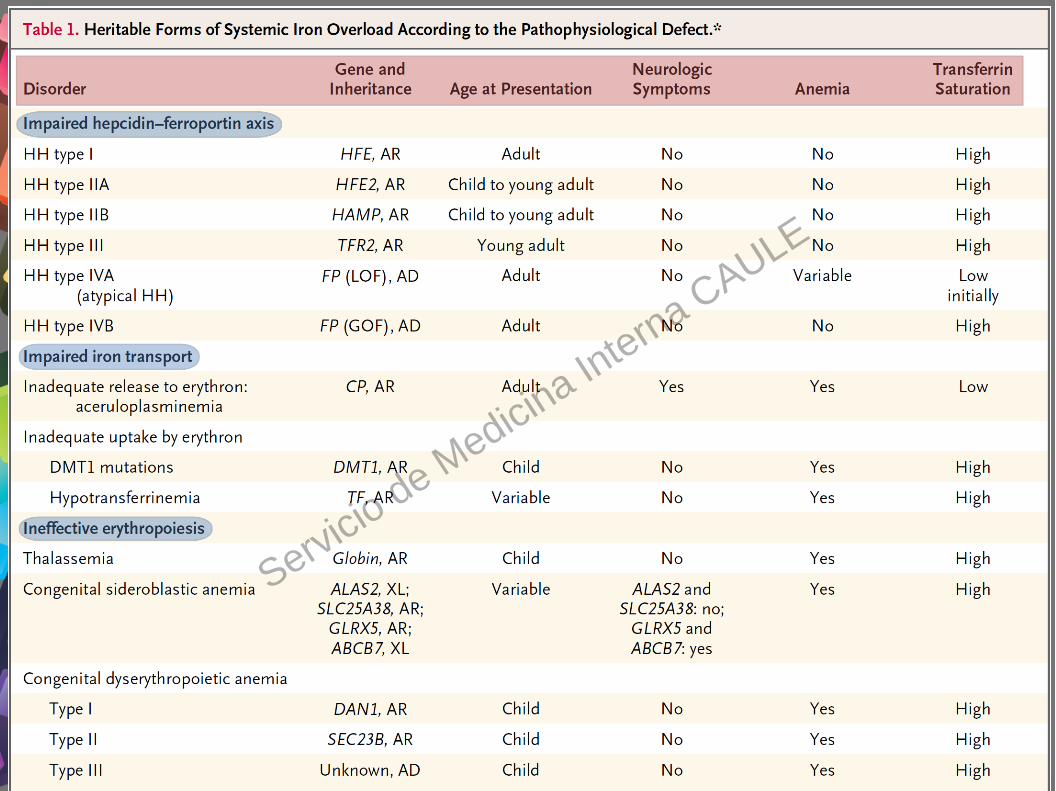
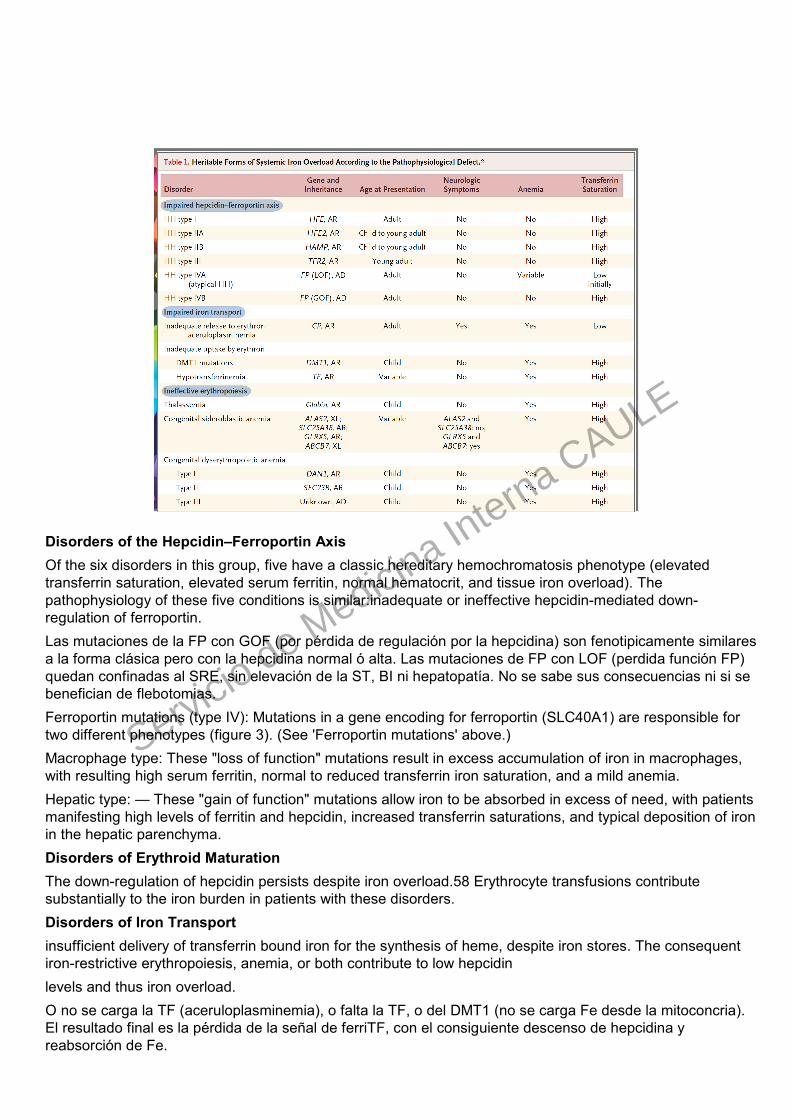
Disorders of the Hepcidin–Ferroportin AxisOf the six disorders in this group, five have a classic hereditary hemochromatosis phenotype (elevated transferrin saturation, elevated serum ferritin, normal hematocrit, and tissue iron overload). The pathophysiology of these five conditions is similar:inadequate or ineffective hepcidin-mediated down-regulation of ferroportin.Las mutaciones de la FP con GOF (por pérdida de regulación por la hepcidina) son fenotipicamente similares a la forma clásica pero con la hepcidina normal ó alta. Las mutaciones de FP con LOF (perdida función FP) quedan confinadas al SRE, sin elevación de la ST, BI ni hepatopatía. No se sabe sus consecuencias ni si se benefician de flebotomias.Ferroportin mutations (type IV): Mutations in a gene encoding for ferroportin (SLC40A1) are responsible for two different phenotypes (figure 3). (See 'Ferroportin mutations' above.)Macrophage type: These "loss of function" mutations result in excess accumulation of iron in macrophages, with resulting high serum ferritin, normal to reduced transferrin iron saturation, and a mild anemia.Hepatic type: — These "gain of function" mutations allow iron to be absorbed in excess of need, with patients manifesting high levels of ferritin and hepcidin, increased transferrin saturations, and typical deposition of iron in the hepatic parenchyma.Disorders of Erythroid MaturationThe down-regulation of hepcidin persists despite iron overload.58 Erythrocyte transfusions contribute substantially to the iron burden in patients with these disorders.Disorders of Iron Transportinsufficient delivery of transferrin bound iron for the synthesis of heme, despite iron stores. The consequent iron-restrictive erythropoiesis, anemia, or both contribute to low hepcidinlevels and thus iron overload.O no se carga la TF (aceruloplasminemia), o falta la TF, o del DMT1 (no se carga Fe desde la mitoconcria). El resultado final es la pérdida de la señal de ferriTF, con el consiguiente descenso de hepcidina y reabsorción de Fe.
Servicio de Medicina In
terna CAULE

10
El 10% de la población blanca es portadora del gen C282Y.Penetrancia bioquímica del C282Y +/+ del 36-76%.Penetrancia de la enfermedad del C282Y +/+ del 2-38% en ♂ y del 1-10% en .♀El H63D ocasiona sobrecarga férrica solo si coincide con otra mutación trascendente (p. ej.: H63D/C282Y).
Servicio de Medicina In
terna CAULE

11
Servicio de Medicina In
terna CAULE

12
Servicio de Medicina In
terna CAULE

13
SEÑALES DE ALARMAFerritina >200 ng/ml en mujeres ó 300 ng/ml en varones.%TF >45% en + ó >50 en varones (más sensible y especifica).↓ hepcidina: para el futuro (marcador genético subrogado).
SITUACIONES CONCRETASSITUACIONES CONCRETAS↑ Ferritina + ↓ %TF: Descartar inflamación, autoinmunes, neoplasias, ERC, hepatopatias, alcoholismo, s. metabólico ⇒ la %TF suele ser normal ó baja (RFA inverso).↑ Ferritina + ↓ %TF: no descarta del todo la HC. Formas aceruloplasminemia y mutaciones FP con PF (probable/ sin trascencencia).↑ Ferritina + ↑ %TF + C282Y/C282Y: HC.↑ Ferritina + ↑ %TF + C282Y/wt, H63D/wt, H63D/H63D, wt/wt ⇒ RM ó biópsia.
Servicio de Medicina In
terna CAULE
14
Servicio de Medicina In
terna CAULE

15
Servicio de Medicina In
terna CAULE
16
Consideraciones terapéuticas
FLEBOTOMIAS QUELANTES
Eliminación de Fe SI SI
Eliminación de otros metales divalentes NO SI
Bloqueo del Fe no transferrínico y daño oxidativo
NO SI
Normalización de la Hepcidina NO NO
➢ Futuro: nuevos quelantes, TF exógena, análogos de hepcidina....???
Servicio de Medicina In
terna CAULE