Servicio de Medicina Interna - CAULE · % Servicio de Medicina Interna - CAULE...
26
Sesión Bibliográfica Octubre 2010 a Febrero de 2011 José Antonio Herrera Rubio Servicio de Medicina Interna Complejo Asistencial Universitario de León SACYL Servicio de Medicina Interna - CAULE
Transcript of Servicio de Medicina Interna - CAULE · % Servicio de Medicina Interna - CAULE...
Sesión Bibliográfica Octubre 2010 a Febrero de 2011
José Antonio Herrera Rubio Servicio de Medicina Interna
Complejo Asistencial Universitario de León SACYL
Servic
io de
Med
icina
Inte
rna
- CAULE
Fundamento y ObjeCvos: Inhibidores directos de la trombina son tan eficaces como dicumarínicos, y < hemorragias intracraneales Prevención de ictus isquémico en > 65 con FA no valvular y CHADS2 score 1 ó > Supervivencia ajustada a la calidad de vida Costes Coste-‐EfecCvidad de Dabigatran / warfarina Métodos: Randomized EvaluaCon of Long-‐Term AnCcoagulaCon Therapy trial y otros Tiempo: Toda la vida
Intervención: Warfarin INR 2.0 -‐ 3.0); Dabigatran, 110 mg twice daily (low dose); / Dabigatran, 150 mg twice daily (high dose).
Servic
io de
Med
icina
Inte
rna
- CAULE
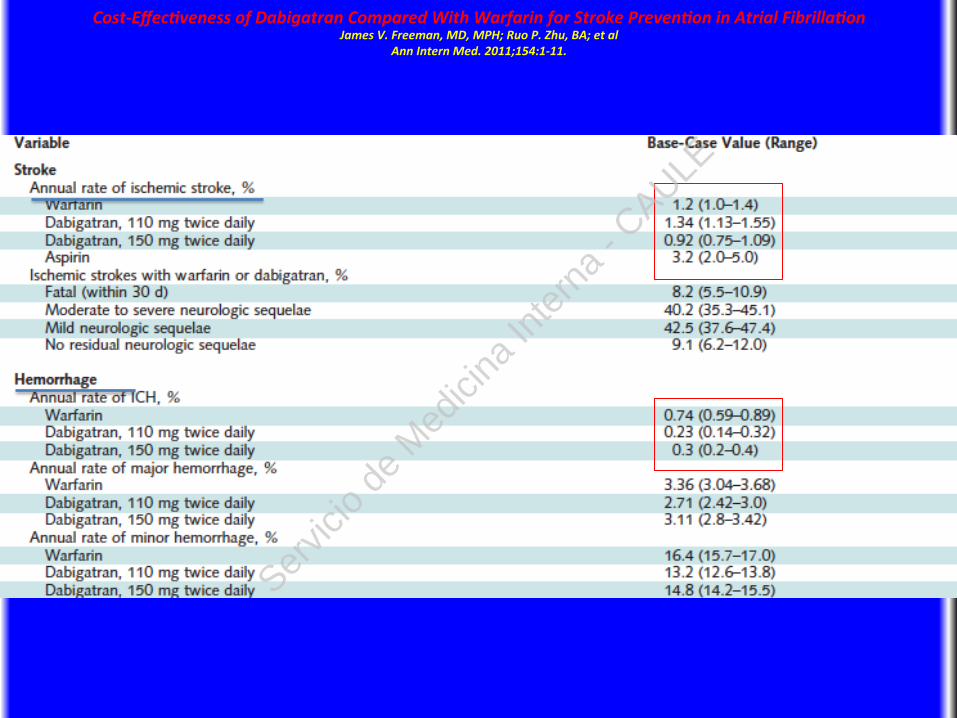
Cost-‐Effec>veness of Dabigatran Compared With Warfarin for Stroke Preven>on in Atrial Fibrilla>on James V. Freeman, MD, MPH; Ruo P. Zhu, BA; et al
Ann Intern Med. 2011;154:1-‐11.
Servic
io de
Med
icina
Inte
rna
- CAULE
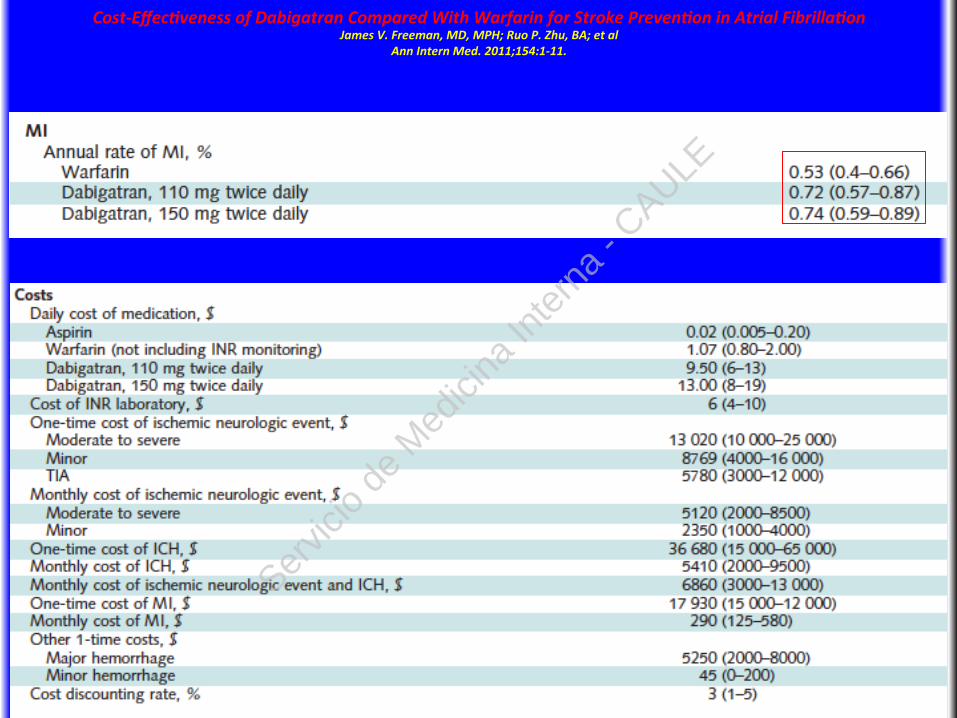
Cost-‐Effec>veness of Dabigatran Compared With Warfarin for Stroke Preven>on in Atrial Fibrilla>on James V. Freeman, MD, MPH; Ruo P. Zhu, BA; et al
Ann Intern Med. 2011;154:1-‐11.
Servic
io de
Med
icina
Inte
rna
- CAULE
Cost-‐Effec>veness of Dabigatran Compared With Warfarin for Stroke Preven>on in Atrial Fibrilla>on James V. Freeman, MD, MPH; Ruo P. Zhu, BA; et al
Ann Intern Med. 2011;154:1-‐11.
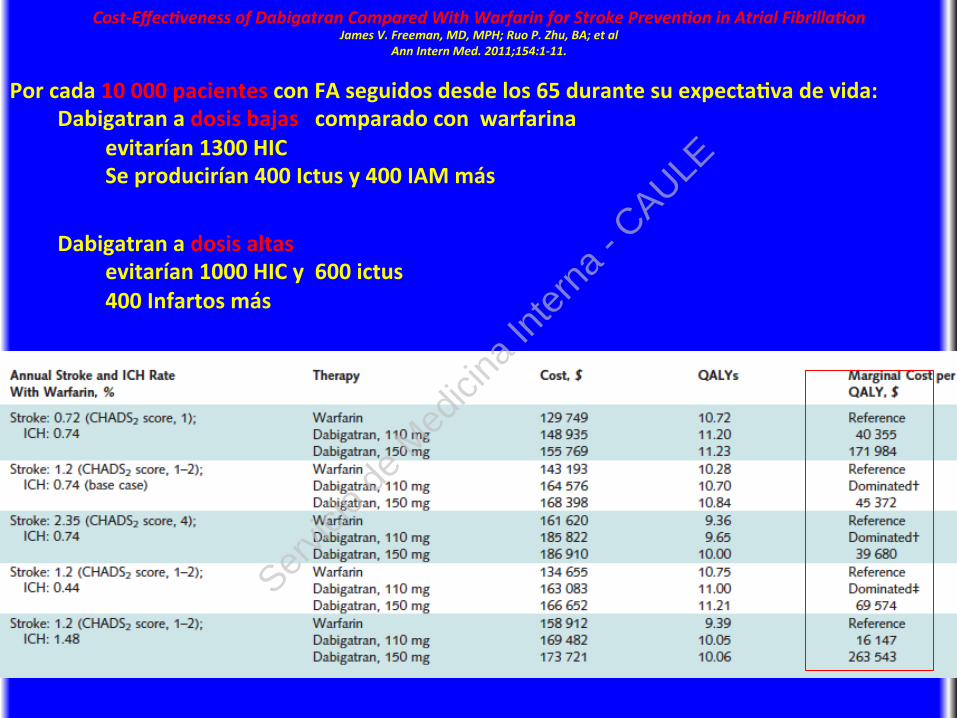
Por cada 10 000 pacientes con FA seguidos desde los 65 durante su expectaCva de vida: Dabigatran a dosis bajas comparado con warfarina evitarían 1300 HIC Se producirían 400 Ictus y 400 IAM más
Dabigatran a dosis altas evitarían 1000 HIC y 600 ictus 400 Infartos más
Servic
io de
Med
icina
Inte
rna
- CAULE
Cost-‐Effec>veness of Dabigatran Compared With Warfarin for Stroke Preven>on in Atrial Fibrilla>on James V. Freeman, MD, MPH; Ruo P. Zhu, BA; et al
Ann Intern Med. 2011;154:1-‐11.
Limitaciones: El estudio recogió datos de 2 años y extrapoló las consecuencias a 35 años Conclusion: In paCents aged 65 years or older with nonvalvular AF at increased risk for stroke (CHADS2 score 1 or equivalent), dabigatran may be a cost-‐effecCve alternaCve to warfarin depending on pricing in the United States. Primary Funding Source: American Heart AssociaCon and Veterans Affairs Health Services Research & Development Service.
Servic
io de
Med
icina
Inte
rna
- CAULE
Cost-‐Effec>veness of Dabigatran Compared With Warfarin for Stroke Preven>on in Atrial Fibrilla>on James V. Freeman, MD, MPH; Ruo P. Zhu, BA; et al
Ann Intern Med. 2011;154:1-‐11.
DISCUSSION We demonstrated that in paCents aged 65 years or older with AF who are at increased risk for stroke (CHADS2 score 1 or equivalent), dabigatran could be a cost-‐effecCve alternaCve to warfarin. High-‐dose dabigatran was also the most effecCve treatment opCon we evaluated, yielding an addiConal 0.56 QALY compared with warfarin. In addiCon,for paCents at higher risk for ischemic stroke or ICH, including those with CHADS2 scores of 2 or greater, the ICER for high-‐dose dabigatran compared with warfarin improved. Our analysis suggests that at a willingness-‐to-‐pay threshold of $50 000 per QALY, low-‐dose dabigatran may be the preferred therapy for paCents with a low absolute risk for ischemic stroke (for example, CHADS2 score of 0 or 1), especially if their concurrent risk for ICH is high. For paCents with low absolute risk for ICH, warfarin may be the preferred therapy. However, for some low-‐risk paCents, anCplatelet therapy rather than anCcoagulaCon may be a reasonable alternaCve, but further clinical study is needed to determine opCmal treatment for paCents who are at low risk for stroke and ICH.
Servic
io de
Med
icina
Inte
rna
- CAULE
Cost-‐Effec>veness of Dabigatran Compared With Warfarin for Stroke Preven>on in Atrial Fibrilla>on James V. Freeman, MD, MPH; Ruo P. Zhu, BA; et al
Ann Intern Med. 2011;154:1-‐11.
Limitaciones: El estudio recogió datos de 2 años y extrapoló las consecuencias a 35 años Conclusion: In paCents aged 65 years or older with nonvalvular AF at increased risk for stroke (CHADS2 score 1 or equivalent), dabigatran may be a cost-‐effecCve alternaCve to warfarin depending on pricing in the United States. Primary Funding Source: American Heart AssociaCon and Veterans Affairs Health Services Research & Development Service.
RESUMIENDO ALTO RIESGO DE ICTUS Y DE HEMORRAGIA: DABIGATRAN BAJO RIESGO DE HEMORRAGIA: WARFARINA BAJO RIESGO DE ICTUS Y DE HEMORRAGIA ANTIAGREGANTES
Servic
io de
Med
icina
Inte
rna
- CAULE
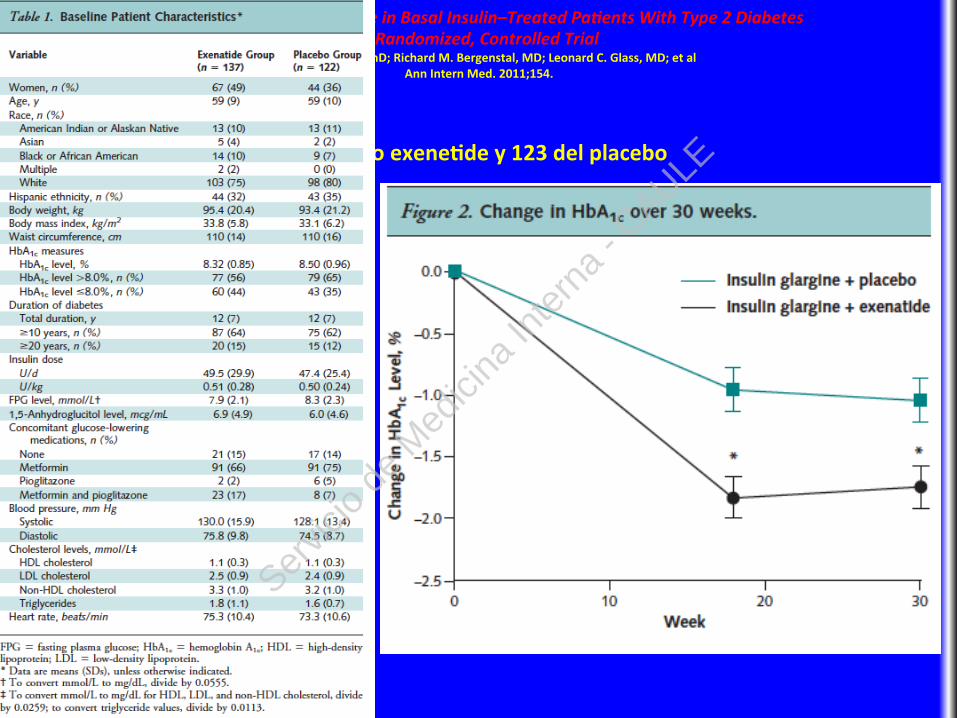
Pacientes con Insulina Glargina y mal control. Se estudia el efecto de añadir exenaCde dos veces al día Design: Parallel, randomized, placebo-‐controlled trial, blocked and straCfied by HbA1c level at site, October 2008 -‐ January 2010. ParCcipants, invesCgators, and personnel conducCng the study were masked to treatment assignments. Senng: 59 centers in 5 countries. Pacientes: Adultos con DM2 y HbA1c entre 7,1 y 10,5% en ro con insulina glargina, sóla o con mesormina y/o pioglitazona.
Servic
io de
Med
icina
Inte
rna
- CAULE
Use of Twice-‐Daily Exena>de in Basal Insulin–Treated Pa>ents With Type 2 Diabetes A Randomized, Controlled Trial
John B. Buse, MD, PhD; Richard M. Bergenstal, MD; Leonard C. Glass, MD; et al Ann Intern Med. 2011;154.
Intervención: Randomización a exenaCde 5 mcg/12 horas durante 4 y semanas y luego 10mcg/12 horas hasta 30 semanas o placebo.
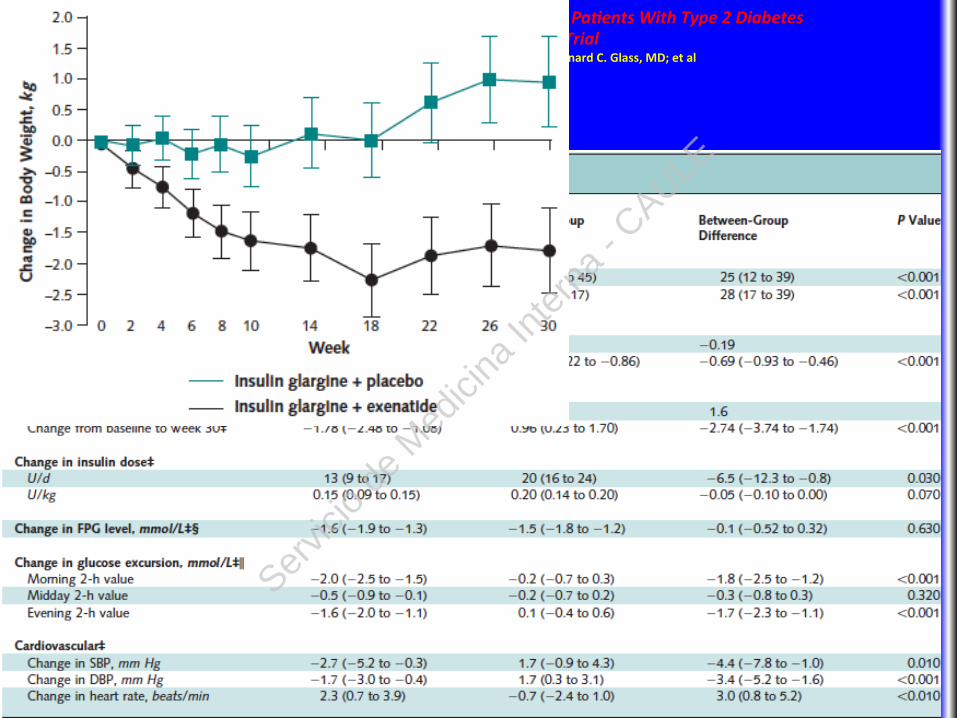
Medidas: Primario: Cambio en el nivel basal de HbA1c . Secundarios
% the parCcipants with HbA1c values of 7.0% or less and 6.5% or less, 7-‐point selfmonitored glucose profiles, body weight, waist circumference, insulin dose, hypoglycemia, and adverse events.
Servic
io de
Med
icina
Inte
rna
- CAULE
Use of Twice-‐Daily Exena>de in Basal Insulin–Treated Pa>ents With Type 2 Diabetes A Randomized, Controlled Trial
John B. Buse, MD, PhD; Richard M. Bergenstal, MD; Leonard C. Glass, MD; et al Ann Intern Med. 2011;154.
Resultados: Completaron el estudio 112 del grupo exeneCde y 123 del placebo
Servic
io de
Med
icina
Inte
rna
- CAULE
Use of Twice-‐Daily Exena>de in Basal Insulin–Treated Pa>ents With Type 2 Diabetes A Randomized, Controlled Trial
John B. Buse, MD, PhD; Richard M. Bergenstal, MD; Leonard C. Glass, MD; et al Ann Intern Med. 2011;154.
Resultados:
Servic
io de
Med
icina
Inte
rna
- CAULE
Use of Twice-‐Daily Exena>de in Basal Insulin–Treated Pa>ents With Type 2 Diabetes A Randomized, Controlled Trial
John B. Buse, MD, PhD; Richard M. Bergenstal, MD; Leonard C. Glass, MD; et al Ann Intern Med. 2011;154.
Resultados:
Servic
io de
Med
icina
Inte
rna
- CAULE
Use of Twice-‐Daily Exena>de in Basal Insulin–Treated Pa>ents With Type 2 Diabetes A Randomized, Controlled Trial
John B. Buse, MD, PhD; Richard M. Bergenstal, MD; Leonard C. Glass, MD; et al Ann Intern Med. 2011;154.
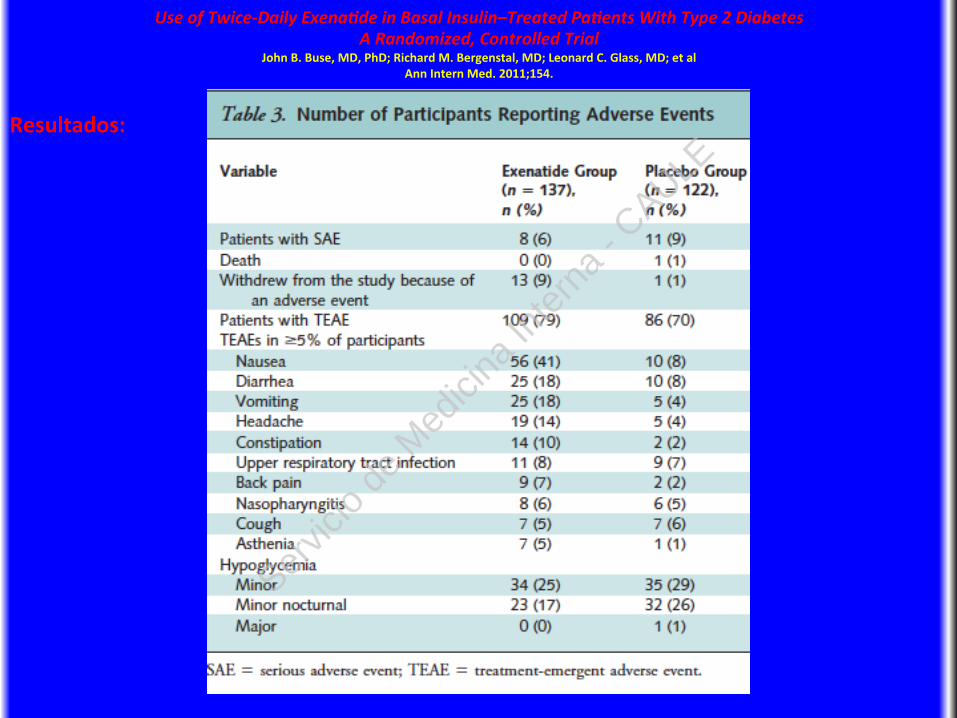
LimitaCons: The study was of short duraCon. There were slight imbalances between groups at baseline in terms of sex, use of concomitant glucose-‐lowering medicaCons, and HbA1c levels, and more exenaCde recipients than placebo recipients withdrew because of adverse events.
Conclusion: Adding twice-‐daily exenaCde injecCons improved glycemic control without increased hypoglycemia or weight gain in parCcipants with uncontrolled type 2 diabetes who were receiving insulin glargine treatment. Adverse events of exenaCde included nausea, diarrhea, vomiCng, headache, and consCpaCon. Primary Funding Source: Alliance of Eli Lilly and Company and Amylin PharmaceuCcals Ser
vicio
de M
edici
na In
tern
a - C
AULE
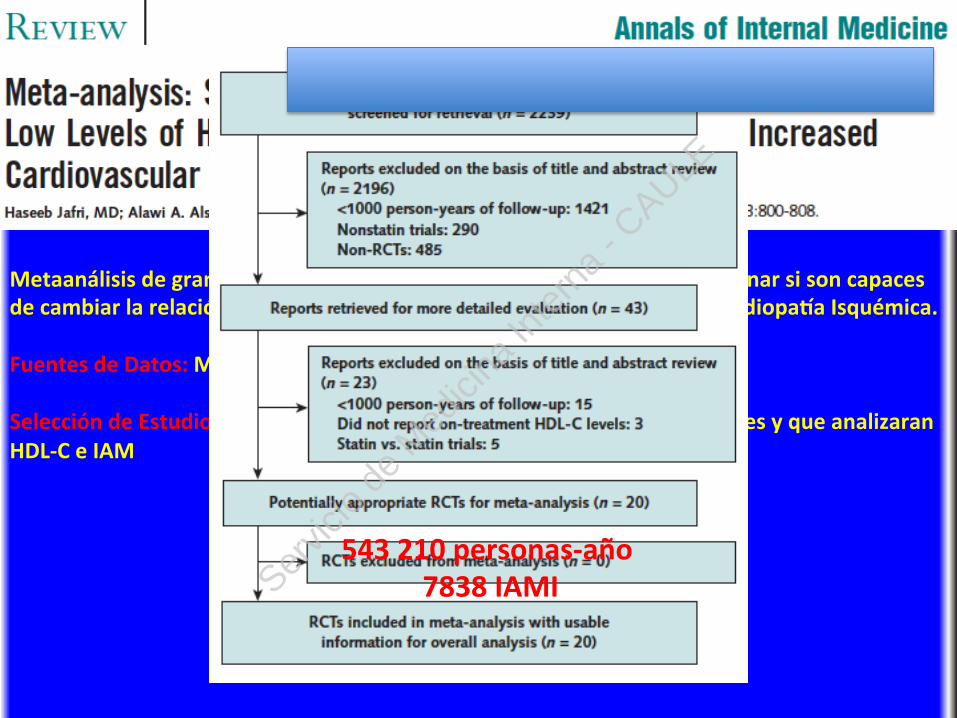
Metaanálisis de grandes estudios randomizados de estaCnas para determinar si son capaces de cambiar la relación existente entre los niveles bajos de HDL-‐col y la Cardiopaua Isquémica. Fuentes de Datos: MEDLINE hasta febrero de 2010 Selección de Estudios: En Inglés, RCTs con un mínimo de 1000 parCcipantes y que analizaran HDL-‐C e IAM
543 210 personas-‐año 7838 IAMI Ser
vicio
de M
edici
na In
tern
a - C
AULE
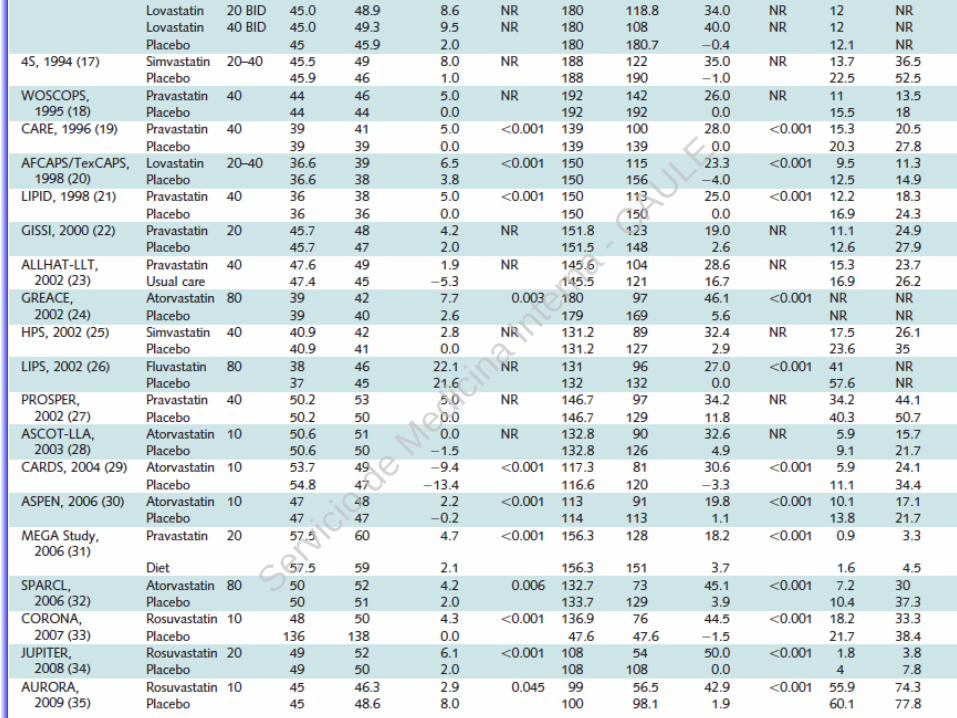
Meta-‐analysis: StaCn Therapy Does Not Alter the AssociaCon Between Low Levels of High-‐Density Lipoprotein Cholesterol and Increased Cardiovascular Risk
Haseeb Jafri, MD; Alawi A. Alsheikh-‐Ali, MD, MS; and Richard H. Karas, MD, PhD Ann Intern Med. 2010;153:800-‐808.
Servic
io de
Med
icina
Inte
rna
- CAULE
Meta-‐analysis: StaCn Therapy Does Not Alter the AssociaCon Between Low Levels of High-‐Density Lipoprotein Cholesterol and Increased Cardiovascular Risk
Haseeb Jafri, MD; Alawi A. Alsheikh-‐Ali, MD, MS; and Richard H. Karas, MD, PhD Ann Intern Med. 2010;153:800-‐808.
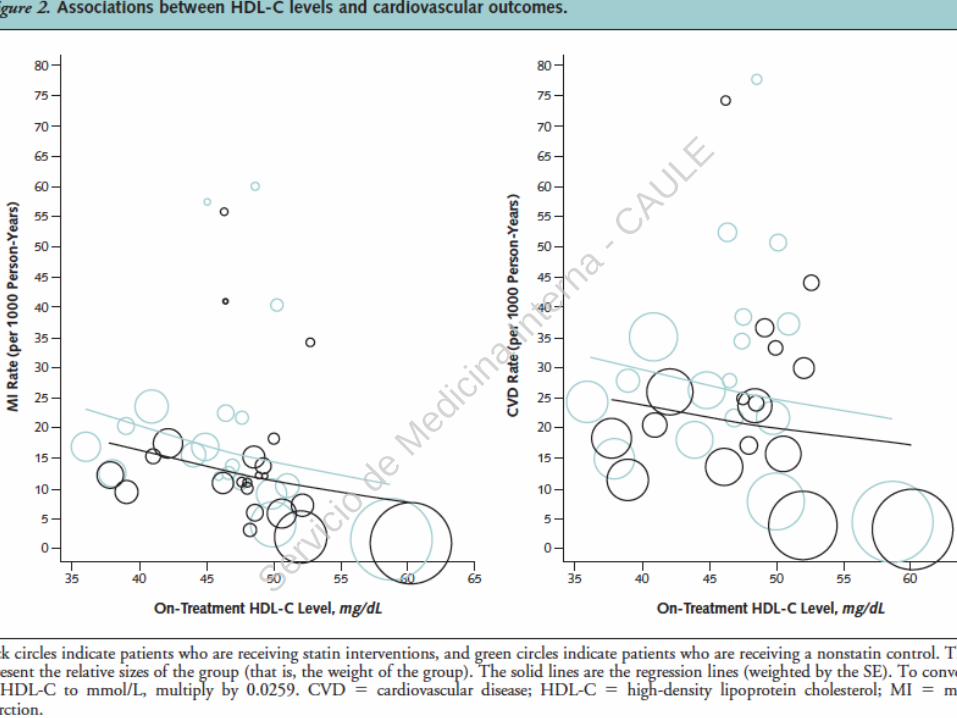
Awer adjustment for on-‐treatment LDL-‐C levels, age, hypertension, diabetes, and tobacco use, there was a significant inverse associaCon between HDL-‐C levels and risk for MI in staCn-‐
treated paCents and control parCcipants.
Servic
io de
Med
icina
Inte
rna
- CAULE
Meta-‐analysis: StaCn Therapy Does Not Alter the AssociaCon Between Low Levels of High-‐Density Lipoprotein Cholesterol and Increased Cardiovascular Risk
Haseeb Jafri, MD; Alawi A. Alsheikh-‐Ali, MD, MS; and Richard H. Karas, MD, PhD Ann Intern Med. 2010;153:800-‐808.
LimitaCon: The observed associaCons may be explained by unmeasured confounding and do not imply causality in the relaConship between HDL-‐C level and cardiovascular risk. Conclusion: StaCns do not alter the relaConship between HDL-‐C level and cardiovascular risk, such that low levels of HDL-‐C remain significantly and independently associated with increased risk despite staCn treatment. The remaining risk seen in staCn-‐treated paCents may be partly explained by low HDL-‐C levels or other, factors associated with low levels of HDL-‐C. Primary Funding Source: None.
Servic
io de
Med
icina
Inte
rna
- CAULE
ObjeCvo: Determinar si existe diferencia e intentar establecer las causas Diseño: Estudio de cohortes, observacional, en 164 hospitales de Nueva York. ParCcipantes: 5319 negros y 18 340 blancos > 18 años, ingresados por ictus isquémicos entre Enero 2005 y Diciembre 2006 Medidas: Influencia de la raza en la mortalidad
aspectos del tratamiento en el fin de la vida Uso de fibrinolisis Gasto Hospitalario Estancia
El seguimiento fue de 1 año desde el ingreso
Servic
io de
Med
icina
Inte
rna
- CAULE
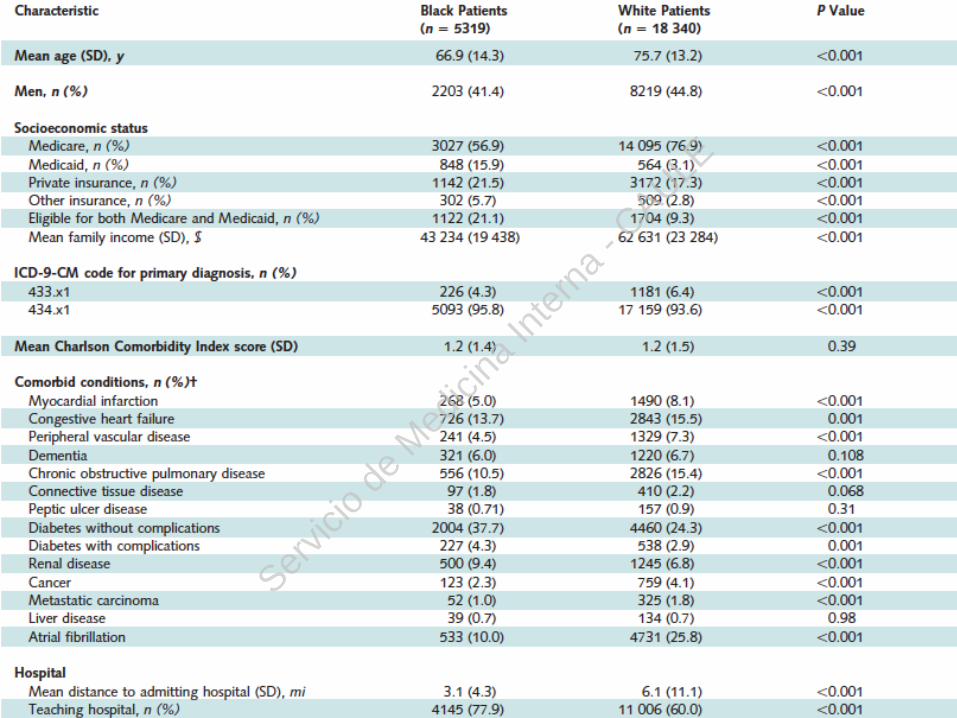
Racial Differences in Mortality Among PaCents With Acute Ischemic Stroke An ObservaConal Study
Ying Xian, MD, PhD; Robert G. Holloway, MD, MPH; KaCa Noyes, PhD, MPH; Manish N. Shah, MD, MPH; and Bruce Friedman, PhD, MPH Ann Intern Med. 2011;154:152-‐159.
Servic
io de
Med
icina
Inte
rna
- CAULE
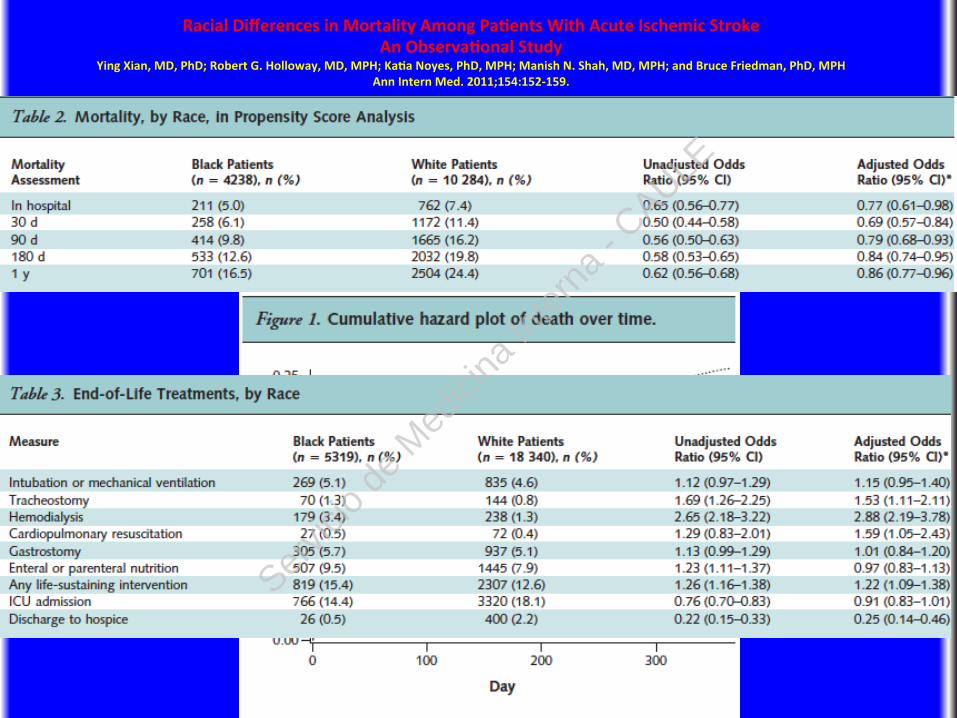
Racial Differences in Mortality Among PaCents With Acute Ischemic Stroke An ObservaConal Study
Ying Xian, MD, PhD; Robert G. Holloway, MD, MPH; KaCa Noyes, PhD, MPH; Manish N. Shah, MD, MPH; and Bruce Friedman, PhD, MPH Ann Intern Med. 2011;154:152-‐159.
Servic
io de
Med
icina
Inte
rna
- CAULE
Racial Differences in Mortality Among PaCents With Acute Ischemic Stroke An ObservaConal Study
Ying Xian, MD, PhD; Robert G. Holloway, MD, MPH; KaCa Noyes, PhD, MPH; Manish N. Shah, MD, MPH; and Bruce Friedman, PhD, MPH Ann Intern Med. 2011;154:152-‐159.
Limitaciones: The study used hospital administraCve data that lacked a stroke severity measure. The study design precluded determinaCon of causality. Conclusión: Among paCents with acute ischemic stroke, black paCents had lower mortality than white paCents. This could be the result of differences in receipt of life-‐sustaining intervenCons and end-‐of-‐life care. Primary Funding Source: American Heart AssociaCon Founders Affiliate
Servic
io de
Med
icina
Inte
rna
- CAULE
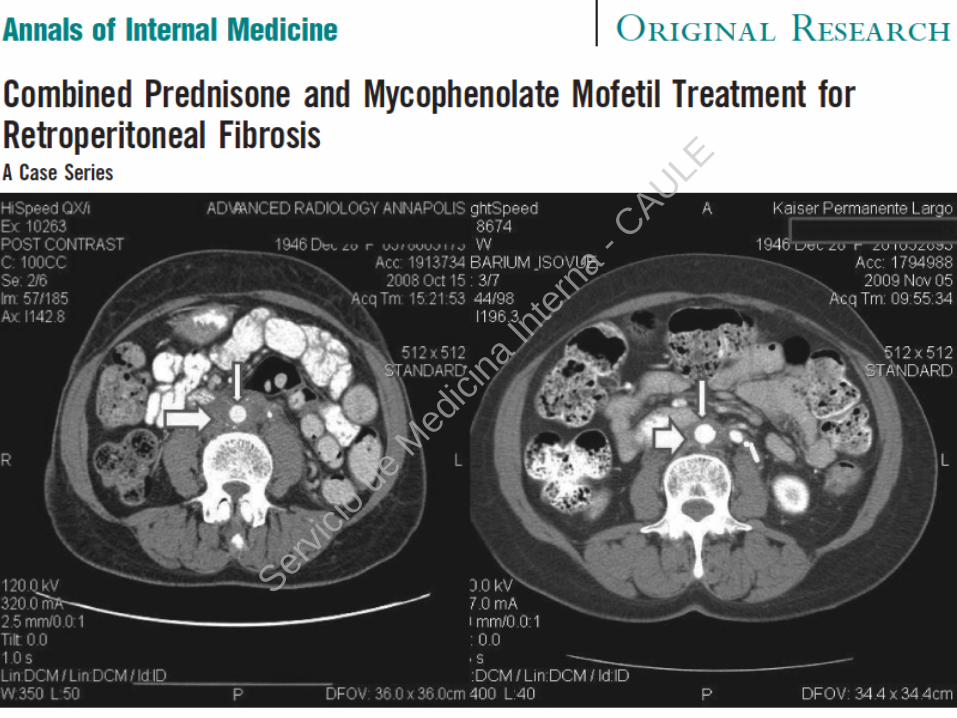
ObjeCvo: Evolución de adultos con FRP en ro con prednisona y micofenolato. Diseño: ProspecCvo. Serie de casos. 1 Abril 2005 y 1 de Julio de 2009 Un Hospital de Tercer nivel 28 pacientes Intervención: Prednisona, 40 mg/d, durante más de 6 meses y mycophenolate mofeCl, 1000 mg/12horas twice daily, durante una media de 24.3 meses Medidas: Evolución clínica, datos de laboratorio y medida de masa paraaórCca. Media de seguimiento 1012 días
Servic
io de
Med
icina
Inte
rna
- CAULE
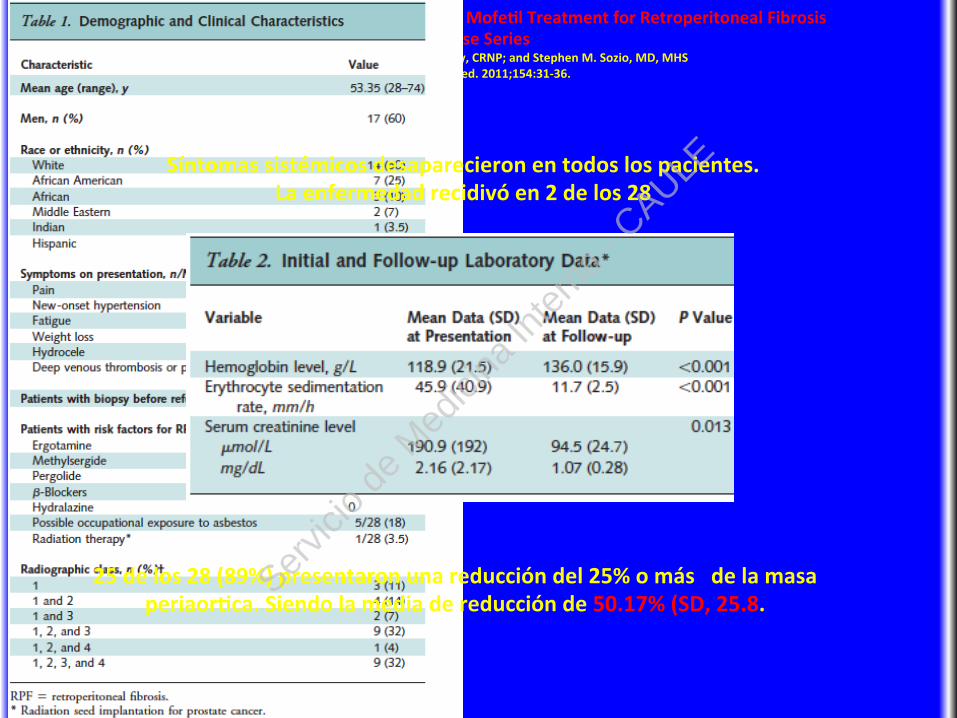
Combined Prednisone and Mycophenolate MofeCl Treatment for Retroperitoneal Fibrosis A Case Series
Paul J. Scheel Jr., MD; Nancy Feeley, CRNP; and Stephen M. Sozio, MD, MHS Ann Intern Med. 2011;154:31-‐36.
Resultados:
25 de los 28 (89%) presentaron una reducción del 25% o más de la masa periaorCca. Siendo la media de reducción de 50.17% (SD, 25.8.
Síntomas sistémicos desaparecieron en todos los pacientes. La enfermedad recidivó en 2 de los 28
Servic
io de
Med
icina
Inte
rna
- CAULE
Combined Prednisone and Mycophenolate MofeCl Treatment for Retroperitoneal Fibrosis A Case Series
Paul J. Scheel Jr., MD; Nancy Feeley, CRNP; and Stephen M. Sozio, MD, MHS Johns Hopkins University School of Medicine
Ann Intern Med. 2011;154:31-‐36.
LimitaCon: Pequeña serie Conclusion: Combined prednisone and mycophenolate mofeCl therapy is a potenCally effecCve treatment for retroperitoneal fibrosis that warrants evaluaCon in randomized trials. Primary Funding Source: Ninguno.
Servic
io de
Med
icina
Inte
rna
- CAULE
Servic
io de
Med
icina
Inte
rna
- CAULE