Servicio de Medicina Interna CAULE · Servicio de Medicina Interna CAULE Mayores de 66 años, con...
14
Sesión Bibliográfica 22 de Julio de 2011 Annals of Internal Medicine José A. Herrera Rubio Servicio de Medicina Interna CAULE
Transcript of Servicio de Medicina Interna CAULE · Servicio de Medicina Interna CAULE Mayores de 66 años, con...
Sesión Bibliográfica 22 de Julio de 2011
Annals of Internal Medicine José A. Herrera Rubio
Servic
io de
Med
icina
Inte
rna
CAULE
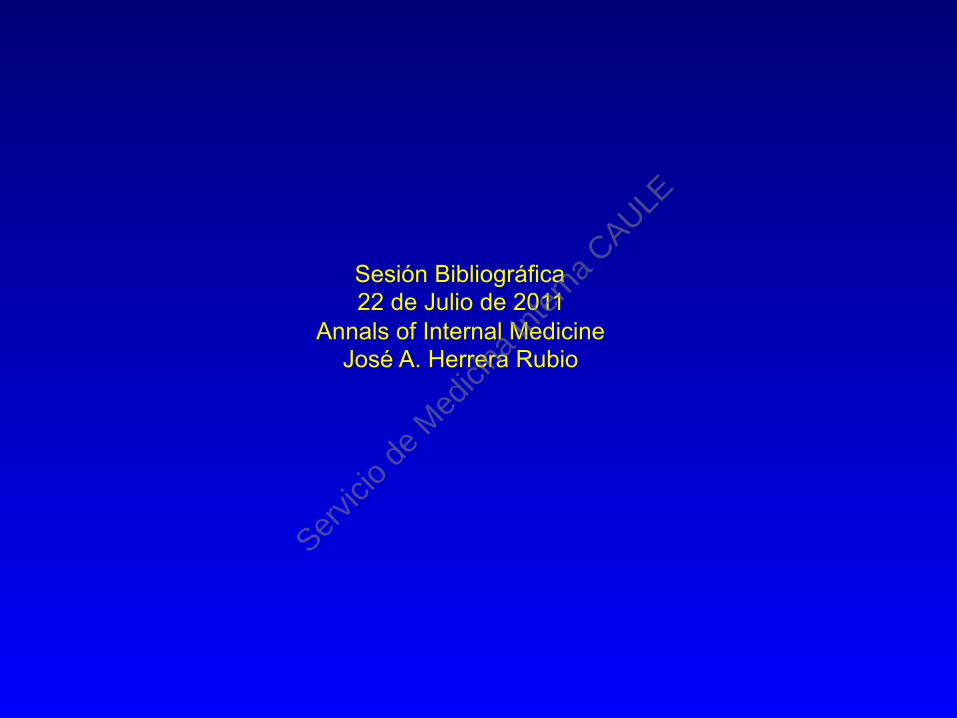
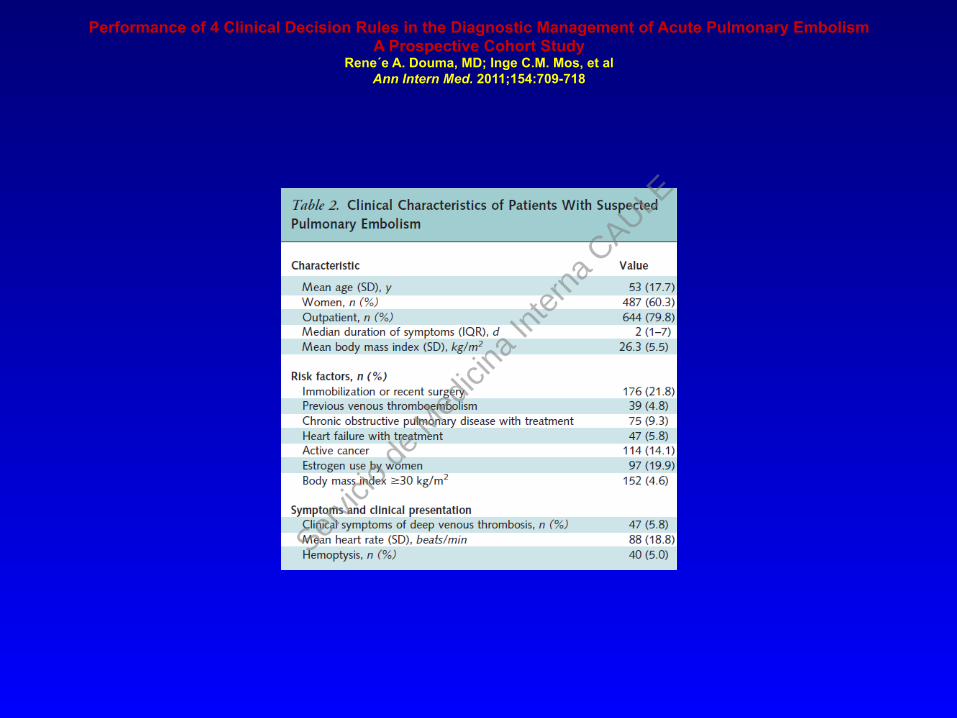
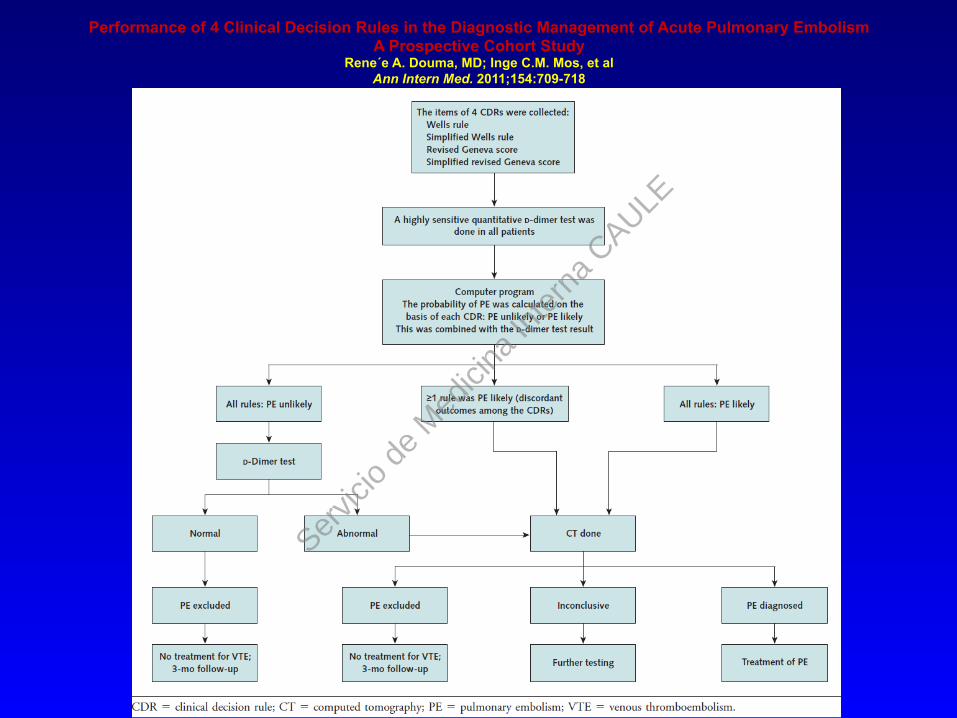
Objetivo: Comparar la eficacia de los 4 marcadores junto al dímero D en la exclusión del TEP Estudio prospectivo en 7 Hospitales de Holanda incluyendo 807 enfermos consecutivos con sospecha de TEP
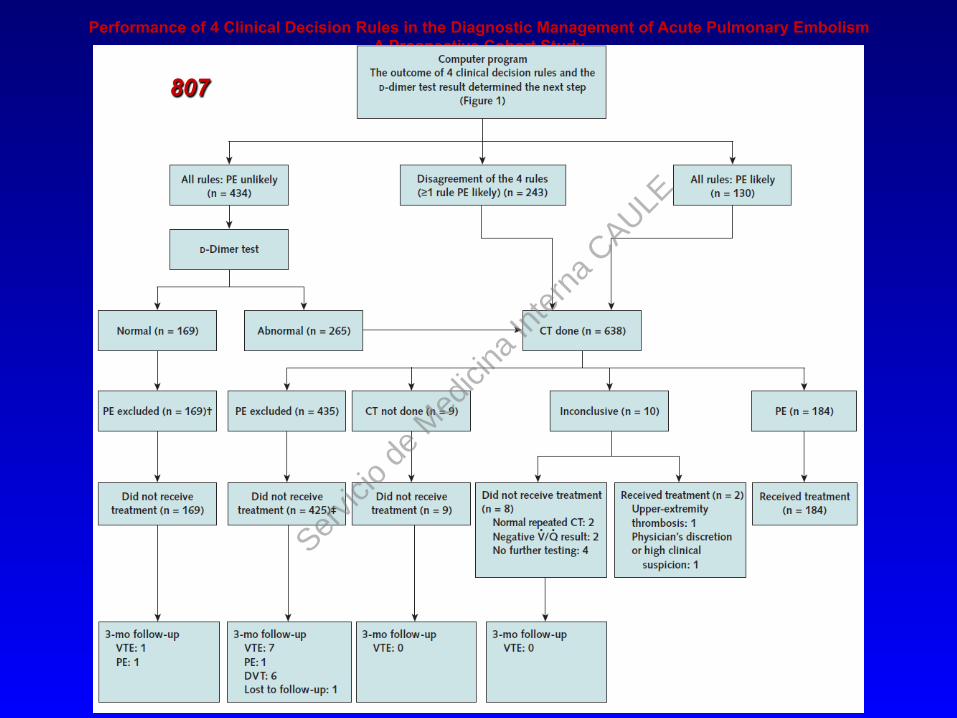
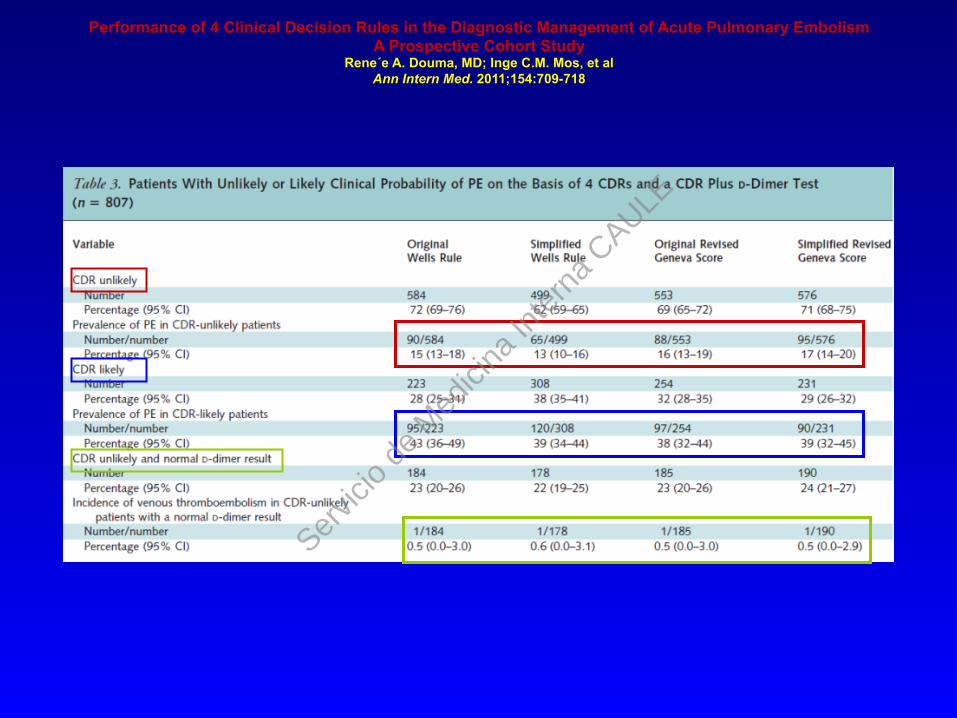
Medidas: Los Resultados de los scores se compararon entre sí según la prevalencia de TEP demostrado por TAC o TVP a los tres meses.
Servic
io de
Med
icina
Inte
rna
CAULE
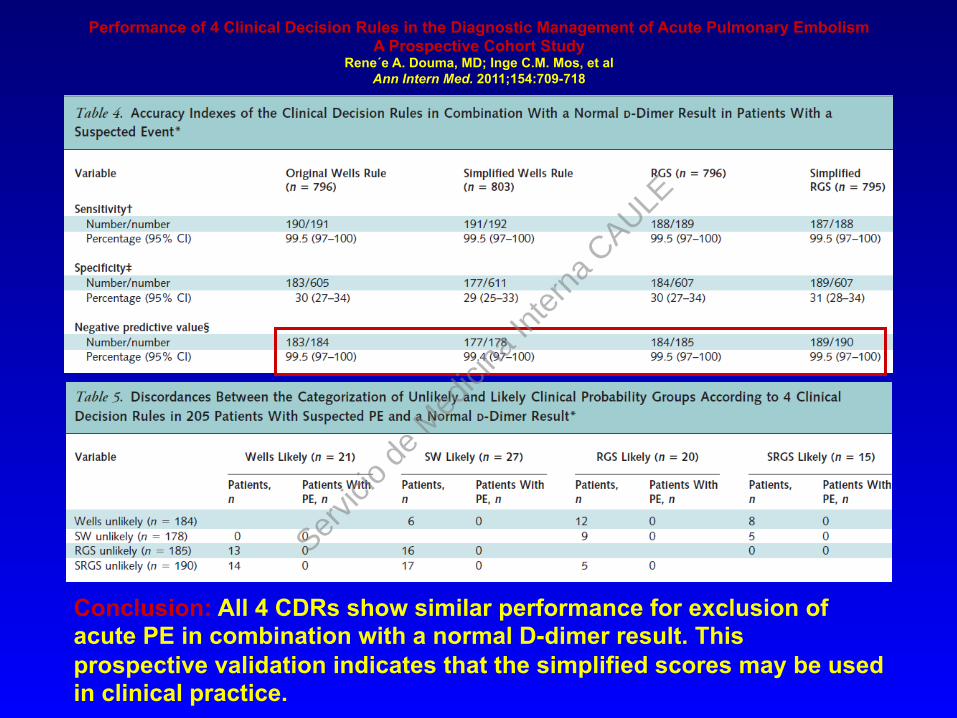
Performance of 4 Clinical Decision Rules in the Diagnostic Management of Acute Pulmonary Embolism A Prospective Cohort Study
Rene´e A. Douma, MD; Inge C.M. Mos, et al Ann Intern Med. 2011;154:709-718
Servic
io de
Med
icina
Inte
rna
CAULE
Performance of 4 Clinical Decision Rules in the Diagnostic Management of Acute Pulmonary Embolism A Prospective Cohort Study
Rene´e A. Douma, MD; Inge C.M. Mos, et al Ann Intern Med. 2011;154:709-718
Servic
io de
Med
icina
Inte
rna
CAULE
Performance of 4 Clinical Decision Rules in the Diagnostic Management of Acute Pulmonary Embolism A Prospective Cohort Study
Rene´e A. Douma, MD; Inge C.M. Mos, et al Ann Intern Med. 2011;154:709-718 807
Servic
io de
Med
icina
Inte
rna
CAULE
Performance of 4 Clinical Decision Rules in the Diagnostic Management of Acute Pulmonary Embolism A Prospective Cohort Study
Rene´e A. Douma, MD; Inge C.M. Mos, et al Ann Intern Med. 2011;154:709-718
Servic
io de
Med
icina
Inte
rna
CAULE
Performance of 4 Clinical Decision Rules in the Diagnostic Management of Acute Pulmonary Embolism A Prospective Cohort Study
Rene´e A. Douma, MD; Inge C.M. Mos, et al Ann Intern Med. 2011;154:709-718
Conclusion: All 4 CDRs show similar performance for exclusion of acute PE in combination with a normal D-dimer result. This prospective validation indicates that the simplified scores may be used in clinical practice.
Servic
io de
Med
icina
Inte
rna
CAULE

Diseño: Se compararon las imágenes obtenidas con el dispositivo portátil con las proporcionadas por un Ecógrafo transtorácico convencional en 97 pacientes ingresados y ambulatorios, remitidos para realizar un ETT convencional. Posteriormente dos ecografistas informaron y compararon las imágenes Lugar: Scripps Clinic Torrey Pines and Scripps Green Hospital, La Jolla, California. Medidas: Visualización y precisión en la determinación de: FE, Anomalías en la contractilidad de la pared, Tamaño ventricular telediastólico, tamaño de la vena cava inferior, morfología mitral y aórtica y presencia de derrame pericárdico.
Servic
io de
Med
icina
Inte
rna
CAULE
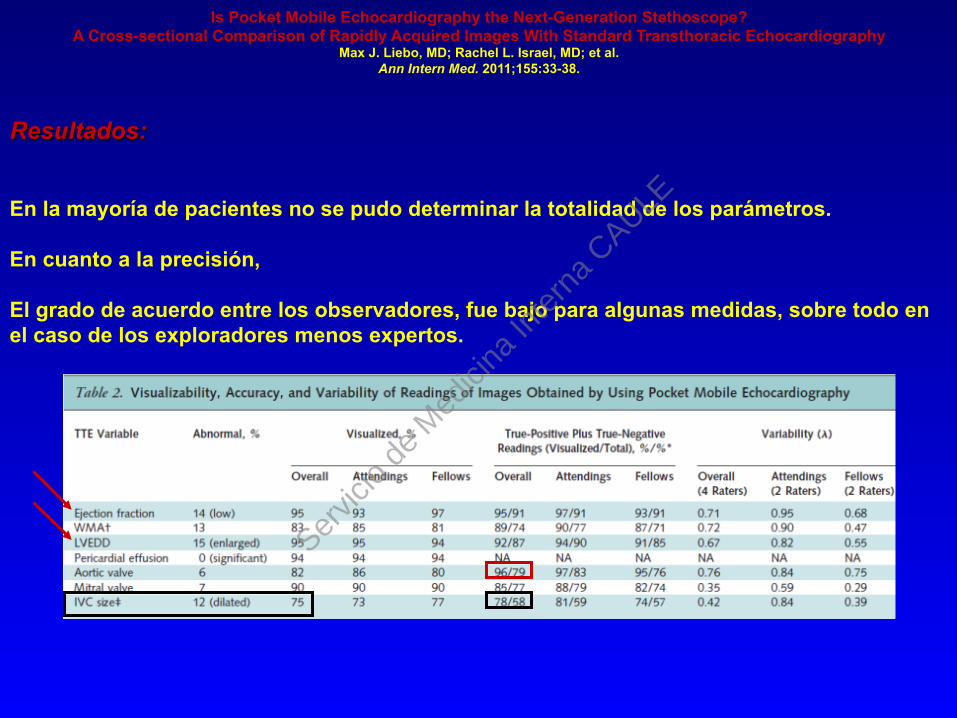
Resultados: En la mayoría de pacientes no se pudo determinar la totalidad de los parámetros. En cuanto a la precisión, El grado de acuerdo entre los observadores, fue bajo para algunas medidas, sobre todo en el caso de los exploradores menos expertos.
Is Pocket Mobile Echocardiography the Next-Generation Stethoscope? A Cross-sectional Comparison of Rapidly Acquired Images With Standard Transthoracic Echocardiography
Max J. Liebo, MD; Rachel L. Israel, MD; et al. Ann Intern Med. 2011;155:33-38.
Servic
io de
Med
icina
Inte
rna
CAULE
Is Pocket Mobile Echocardiography the Next-Generation Stethoscope? A Cross-sectional Comparison of Rapidly Acquired Images With Standard Transthoracic Echocardiography
Max J. Liebo, MD; Rachel L. Israel, MD; et al. Ann Intern Med. 2011;155:33-38.
Conclusion: The rapid acquisition of images by skilled ultrasonographers who use PME yields accurate assessments of ejection fraction and some but not all cardiac structures in many patients. Further testing of the device in larger patient cohorts with diverse cardiac abnormalities and with untrained clinicians obtaining and interpreting images is required before wide dissemination of its use can be recommended. Primary Funding Source: National Institutes of Health.
Limitation: The study was conducted at a single setting, there was no formal estimate of accuracy given the small convenience sample of patients, and few abnormal echocardiographic measurements occurred.
Servic
io de
Med
icina
Inte
rna
CAULE
Fuentes: MEDLINE, EMBASE, Cochrane Library, LILACS, y ClinicalTrials.gov. Selección de Estudios: Randomizados de al menos 24 semanas de duración, que valoren la eficacia que supone añadir un tercer fármaco en el tratamiento de la diabetes tipo 2 en > de 18 años con HbA1c > 7.0% y en tratamiento con MTF y SFU Datos Extraidos: End points primarios: variación de HbA1c, cambio en el peso y episodios de hipoglucemia severa. Grupos Estudiados: Insulina. Acarbosa, Tiazolindionas, Agonistas GLP-1 e inhibidores DPP4
Servic
io de
Med
icina
Inte
rna
CAULE
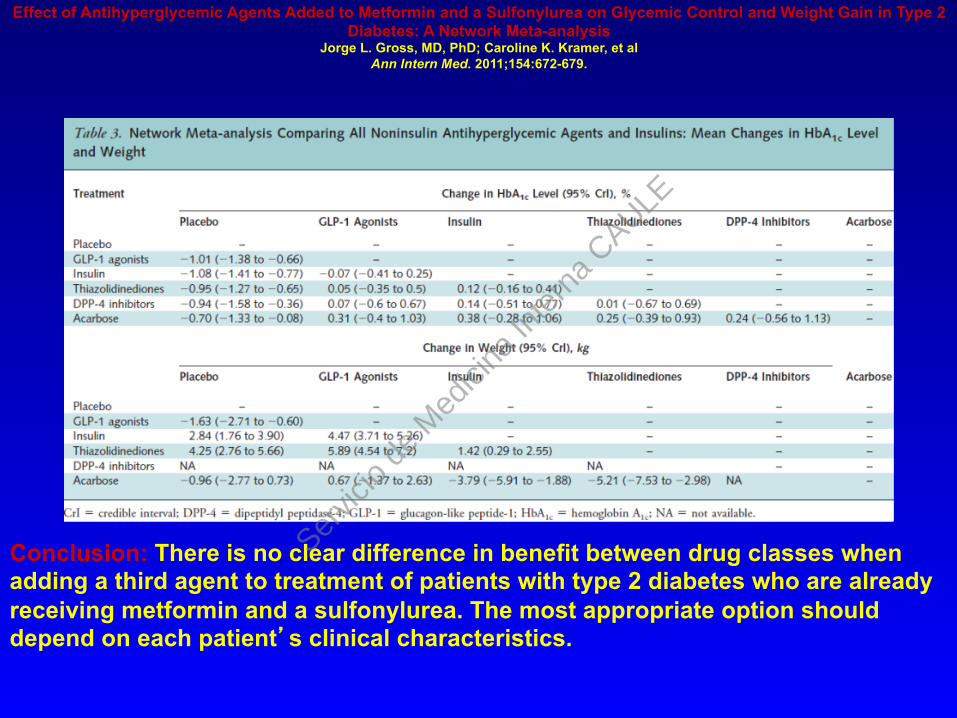
Conclusion: There is no clear difference in benefit between drug classes when adding a third agent to treatment of patients with type 2 diabetes who are already receiving metformin and a sulfonylurea. The most appropriate option should depend on each patient’s clinical characteristics.
Effect of Antihyperglycemic Agents Added to Metformin and a Sulfonylurea on Glycemic Control and Weight Gain in Type 2 Diabetes: A Network Meta-analysis
Jorge L. Gross, MD, PhD; Caroline K. Kramer, et al Ann Intern Med. 2011;154:672-679.
Servic
io de
Med
icina
Inte
rna
CAULE
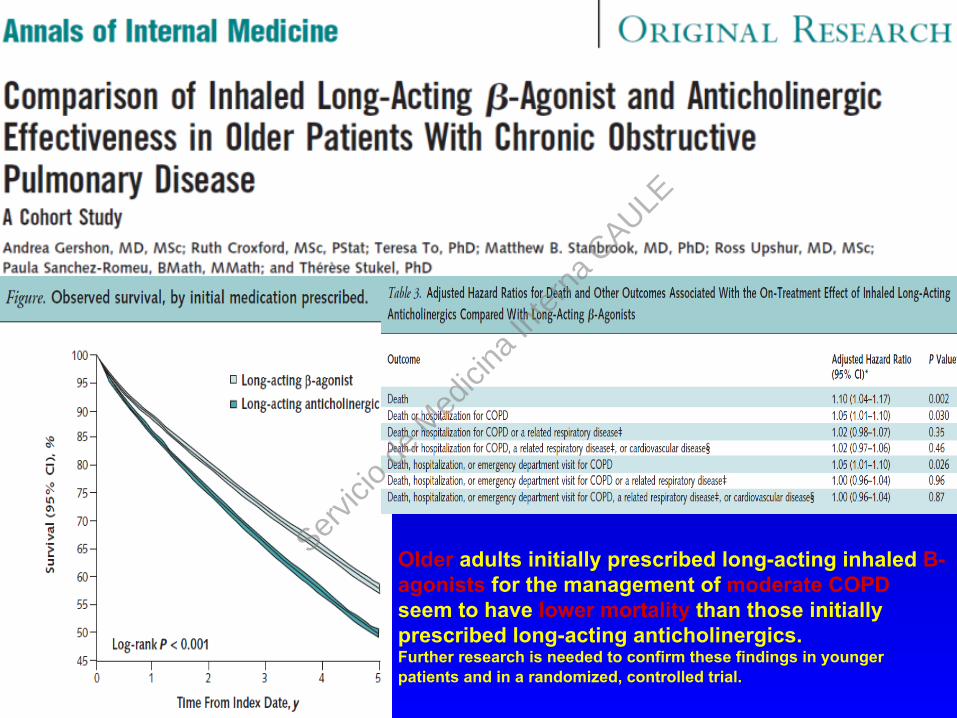
Mayores de 66 años, con diagnóstico espirométrico de EPOC y a los que se les receta de novo un Beta2 de larga duración ó un anticolinérgico, pero no ambos, entre 2003 y 2007. Fueron seguidos más de 5,5 años. Medidas: Mortalidad por cualquier causa
46 403 patients with COPD (mean age, 77 years; 49% women) were included. Overall mortality was 38.2%.
Older adults initially prescribed long-acting inhaled B-agonists for the management of moderate COPD seem to have lower mortality than those initially prescribed long-acting anticholinergics. Further research is needed to confirm these findings in younger patients and in a randomized, controlled trial.
Servic
io de
Med
icina
Inte
rna
CAULE
Conclusion: Compared with usual care, PST with or without PSM is associated with significantly fewer deaths and thromboembolic events, without increased risk for a serious bleeding event, for a highly selected group of motivated adult patients requiring longterm anticoagulation with vitamin K antagonists. Whether this care model is cost-effective and can be implemented successfully in typical U.S. health care settings requires further study.
Servic
io de
Med
icina
Inte
rna
CAULE